transportation. section 1: blood cardiovascular system – includes: fluid (blood) – includes ~75...
TRANSCRIPT
Transportation

Section 1: Blood
• Cardiovascular system– Includes:• Fluid (blood)
– Includes ~75 trillion cells
• Series of conducting hoses (blood vessels)• Pump (heart)

VeinArtery
Capillaries
Heart
The Components of the Cardiovascular System
THE HEART propels blood and maintains blood pressure.
BLOOD VESSELS
Capillaries
Arteries
Veins
BLOOD
distribute blood around the body.
permit diffusion between blood andinterstitial fluids.
carry blood away from the heart to thecapillaries.
return blood from capillaries to theheart.
distributes oxygen, carbon dioxide, andblood cells; delivers nutrients and hormones;transports waste products; and assists intemperature regulation and defense against disease.
Figure 17 Section 1 1
Section 1: Blood
• Functions of blood– Transportation of dissolved gases, nutrients,
hormones, and metabolic wastes– Regulation of the pH and ion composition of
interstitial fluids– Restriction of fluid loss at injury sites– Defense against toxins and pathogens– Stabilization of body temperature

Module 17.1: Blood components
• Blood– Is a fluid connective tissue– About 5 liters (5.3 quarts) in body
• 5–6 in males, 4–5 in females (difference mainly body size)– Consists of:
• Plasma (liquid matrix)• Formed elements (cells and cell fragments)
– Properties• Temp is roughly 38°C (100.4°F)• Is 5× more viscous than water (due to solid components)• Is slightly alkaline (average pH 7.4)
Module 17.1: Blood components
• Whole blood– Term for removed blood when composition is
unaltered• May be fractionated or separated
– Plasma» 46%–63% of blood volume
– Hematocrit (or packed cell volume [PCV])» Percentage of whole blood contributed by formed elements
(99% of which are red blood cells)» Average 47% for male (range 40%–54%)» Average 42% for female (range 37%–47%)

Module 17.1: Blood components
• Plasma– Composition resembles interstitial fluid in many ways
• Exists because exchange of water, ions, and small solutes• 92% water• 7% plasma proteins• 1% other solutes
– Primary differences• Levels of respiratory gases (oxygen and carbon dioxide)• Concentrations of dissolved proteins (cannot cross capillary
walls)
Module 17.1: Blood components
• Plasma proteins– In solution rather than as fibers like other
connective tissues– Each 100 mL has ~7.6 g of protein• ~5× that of interstitial fluid
– Large size and globular shapes prevent leaving bloodstream
– Liver synthesizes >90% of all plasma proteins

Module 17.1: Blood components
• Plasma proteins (continued)– Albumins
• ~60% of all plasma proteins• Major contributors to plasma osmotic pressure
– Globulins• ~35% of all plasma proteins• Antibodies (immunoglobulins) that attack pathogens• Transport globulins that bind ions, hormones, compounds
– Fibrinogen• Functions in clotting and activate to form fibrin strands
– Many active and inactive enzymes and hormones
Module 17.1: Blood components
• Plasma solutes– Electrolytes
• Essential for vital cellular activities• Major ions are Na+, K+, Ca2+, Mg2+, Cl–, HCO3
–, HPO4–, SO4
2–
– Organic nutrients• Used for cell ATP production, growth, and maintenance• Includes lipids, carbohydrates, and amino acids
– Organic wastes• Carried to sites of breakdown or excretion• Examples: urea, uric acid, creatinine, bilirubin, NH4
+

Figure 17.1 1
Wholeblood
consists of
Plasma(46–63%)
Formedelements(37–54%)

Module 17.1: Blood components
• Formed elements– Platelets
• Small membrane-bound cell fragments involved in clotting– White blood cells (WBCs)
• Also known as leukocytes (leukos, white + -cyte, cell)• Participate in body’s defense mechanisms• Five classes, each with different functions
– Red blood cells (RBCs)• Also known as erythrocytes (erythros, red + -cyte, cell)• Essential for oxygen transport in blood
Module 17.1 Review
a. Define hematocrit.
b. Identify the two components constituting whole blood, and list the composition of each.
c. Which specific plasma proteins would you expect to be elevated during an infection?
Module 17.2: Red blood cells
• RBCs in blood– Most numerous cell type in blood• Roughly 1/3 of all cells in the body
– Red blood cell count (standard blood test) results• Adult males: 4.5–6.3 million RBCs/1 µL or 1 mm3 of whole
blood• Adult females: 4.2–5.5 million RBCs/1 µL or 1 mm3 of
whole blood• One drop = 260 million RBCs

Module 17.2: Red blood cells
• RBC characteristics– Biconcave disc– Average diameter ~8 µm– Large surface area-to-volume ratio• Greater exchange rate of oxygen
– Can form stacks (rouleaux)• Facilitate smooth transport through small vessels
– Are flexible• Allow movement through capillaries with diameters
smaller than RBC (as narrow as 4 µm)
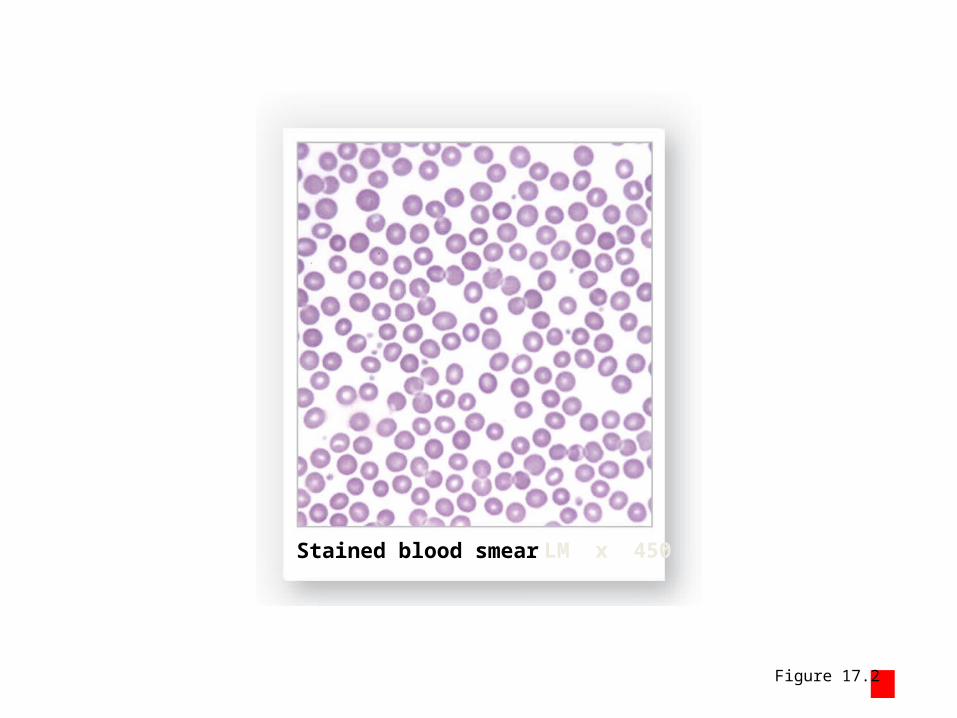
Figure 17.2 1
Stained blood smear LM x 450

Figure 17.2 2
The size and biconcave shape of an RBC
RBCs Colorized SEM x 1800
7.2–8.4 μm
0.45–1.16 μm 2.31–2.85 μm

Figure 17.2 3
The advantages of the biconcave shape of RBCs
Functional Aspects of Red Blood Cells
• Large surface area-to-volume ration. Each RBC carries oxygen bound to intracellular proteins, and that oxygen must be absorbed or released quickly as the RBC passes through the capillaries. The greater the surface area per unit volume, the faster the exchange between the RBC’s interior and the surrounding plasma. The total surface area of all the RBCs in the blood of a typical adult is about 3800 square meters, roughly 2000 times the total surface area of the body.
• RBCs can form stacks. Like dinner plates, RBCs can form stacks that ease the flow through narrow blood vessels. An entire stack can pass along a blood vessel only slightly larger than the diameter of a single RBC, whereas individual cells would bump the walls, bang together, and form logjams that could restrict or prevent blood flow.
• Flexibility. Red blood cells are very flexible and can bend and flex when entering small capillaries and branches. By changing shape, individual RBCs can squeeze through capillaries as narrow as 4 μm.
Sectional view of capillaries LM x 1430
Red blood cell (RBC)
Nucleus of endothelial cell
Blood vessels (viewedin longitudinal section)
Rouleaux(stacks of RBCs)

Module 17.2: Red blood cells
• RBC characteristics (continued)– Lose most organelles including nucleus during development
• Cannot repair themselves and die in ~120 days– Contain many molecules (hemoglobin) associated with
primary function of carrying oxygen• Each cell contains ~280 million hemoglobin (Hb) molecules• Normal whole blood content (grams per deciliter)
– 14–18 dL (males), 12–16 dL (females)
• ~98.5% of blood oxygen attached to Hb in RBCs– Rest of oxygen dissolved in plasma

Module 17.2: Red blood cells
• Hemoglobin– Protein with complex quaternary structure– Each molecule has 4 chains (globular protein subunits)
• 2 alpha (α) chains• 2 beta (β) chains
– Each chain contains a single heme pigment molecule• Each heme (with iron) can reversibly bind one molecule of oxygen
– Forms oxyhemoglobin (HbO2) (bright red)
» Deoxyhemoglobin when not binding O2 (dark red)
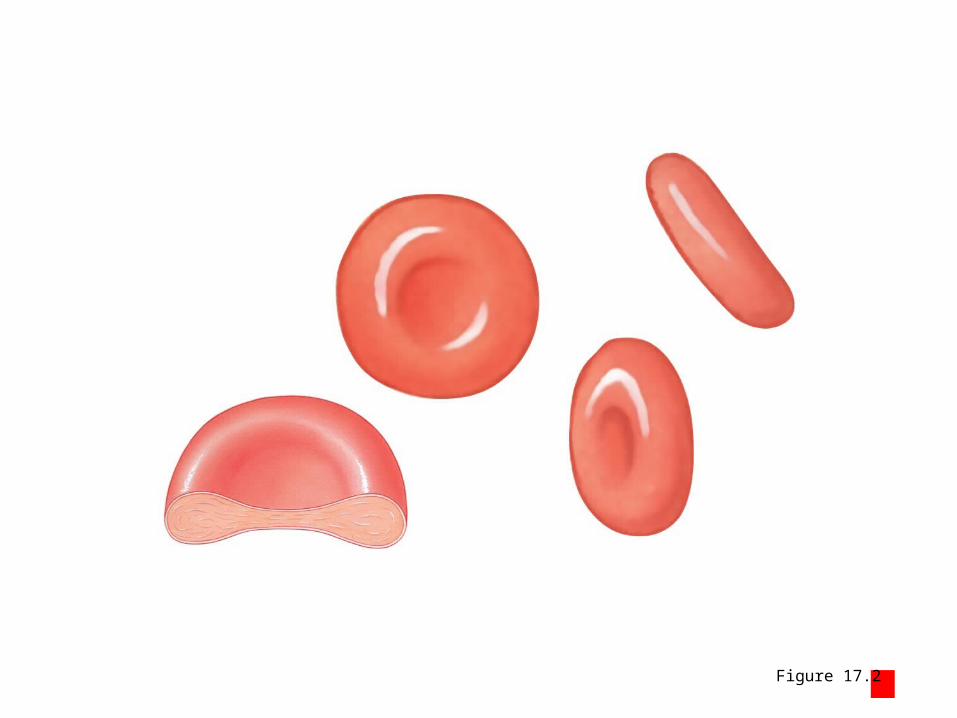
Figure 17.2 4
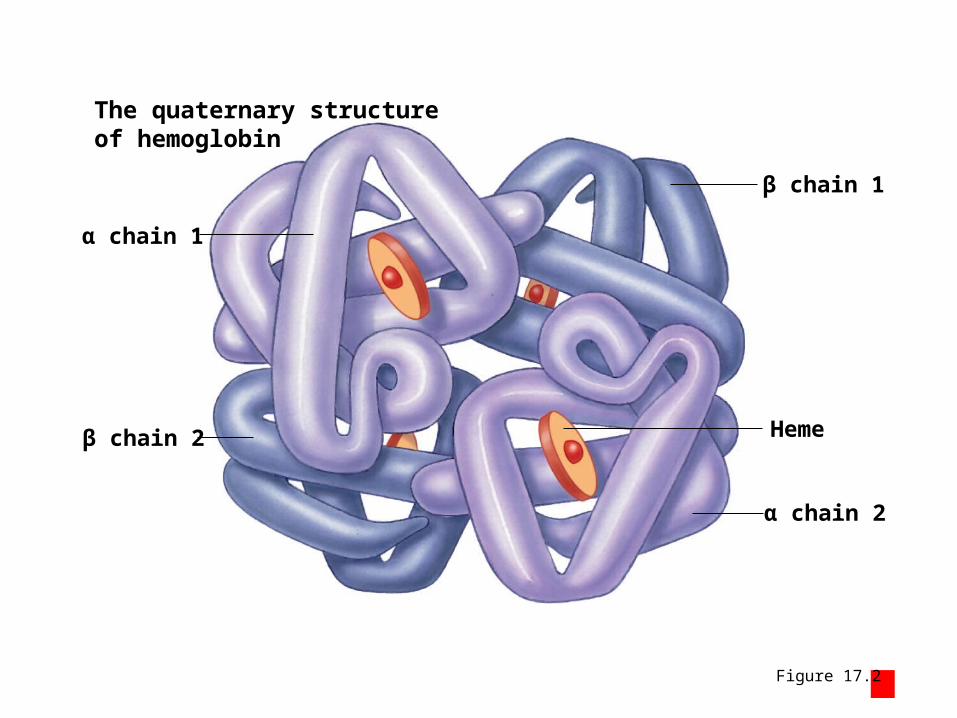
Figure 17.2 5
The quaternary structureof hemoglobin
α chain 1
β chain 2
β chain 1
α chain 2
Heme
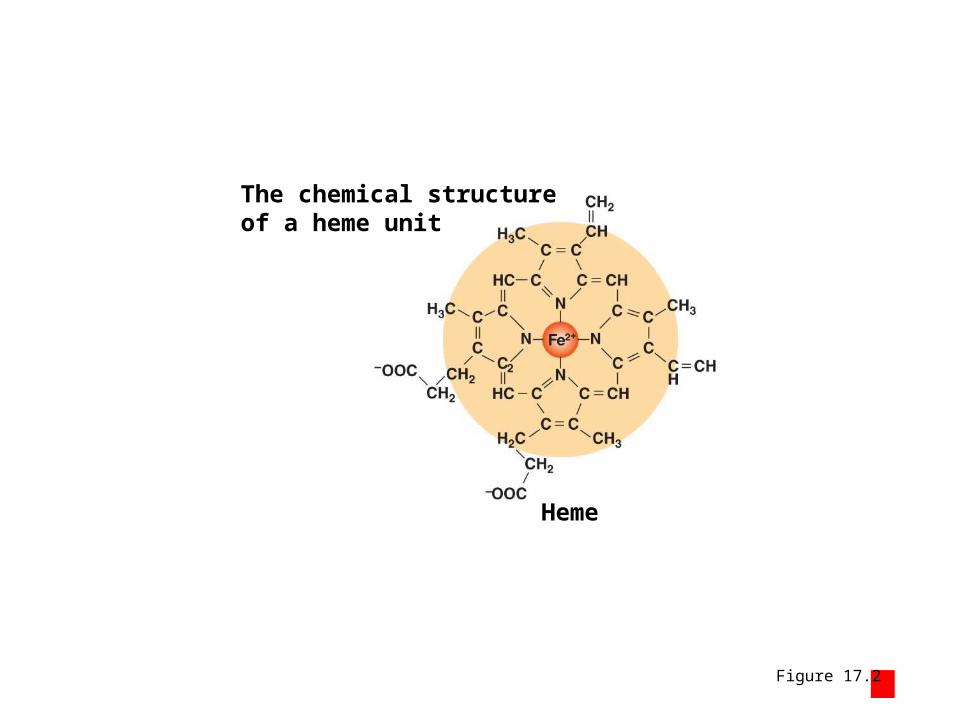
Figure 17.2 6
The chemical structureof a heme unit
Heme

Module 17.2 Review
a. Define rouleaux.
b. Describe hemoglobin.
c. Compare oxyhemoglobin with deoxyhemoglobin.

Section 1: Heart Structure
• Location of the heart– Near anterior chest wall, directly posterior to
sternum– Center lies slightly to the left of midline– Entire heart is rotated slightly left

Section 1: Heart Structure
• Gross anatomy– Base (superior surface where major vessels attach)– Apex (inferior pointed tip)– Borders• Superior border (formed by base) • Right border (formed by right atrium)• Left border (formed by left ventricle and small part of left
atrium)• Inferior border (formed mainly by inferior wall of right
ventricle)

The location of the heartin the chest cavity
1 1
2 2
3 3
4 4
5 5
6 6
7 7
88
9 910 10
Apex
Ribs
Base
Figure 18 Section 1 1

Figure 18 Section 1 2
An anterior view showing theborders of the heart
Right border
Superior border
Inferior border
Left border

Module 18.1: Heart wall and tissue
• Layers of heart wall1. Epicardium (visceral pericardium)• Covers surface of heart• Serous membrane made of exposed mesothelium and
underlying areolar tissue (attaching to myocardium)
– Parietal pericardium• Not a heart wall layer but is continuous serous
membrane with visceral pericardium• Lines pericardial cavity and fibrous pericardial sac
Module 18.1: Heart wall and tissue
• Layers of heart wall (continued)2. Myocardium• Middle, muscular layer forming atria and ventricles• Contains cardiac muscle tissue, blood vessels, and
nerves– Concentric muscle tissue layers
» Form a figure-eight around the atria» Superficial muscle layers wrap both ventricles» Deep muscle layers form figure-eight around ventricles
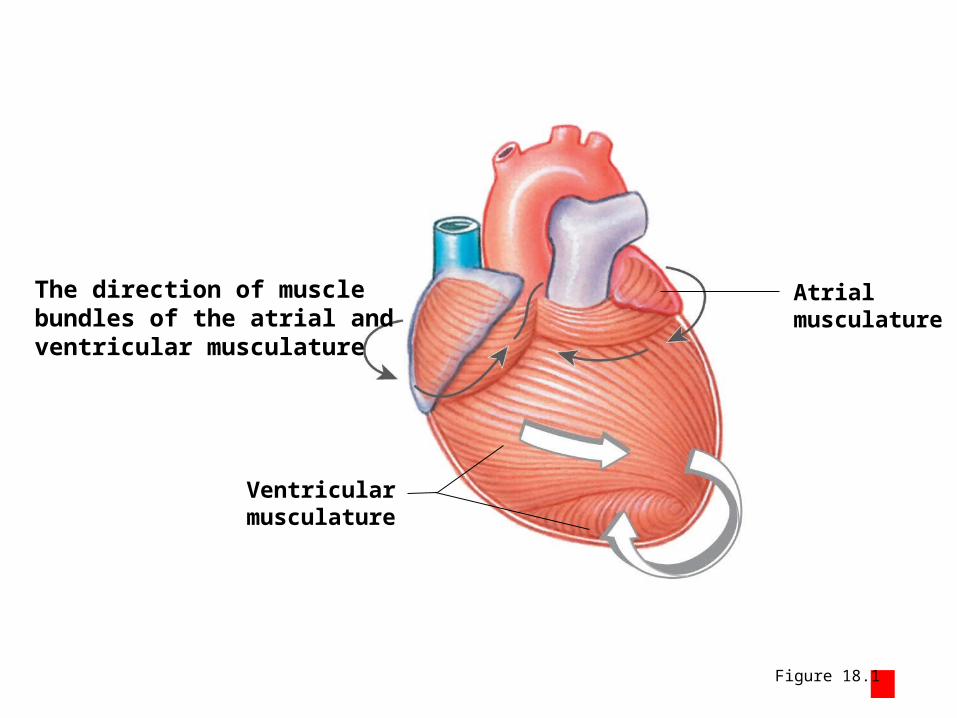
Figure 18.1 2
The direction of musclebundles of the atrial andventricular musculature
Ventricularmusculature
Atrialmusculature
Module 18.1: Heart wall and tissue
• Layers of heart wall (continued)3. Endocardium• Covering inner surfaces of heart, including valves• Composed of simple squamous epithelial tissue and
underlying areolar tissue– Forms endothelium continuous with blood vessel
endothelium

Figure 18.1 1
A section of the heart showing its three layers: epicardium,myocardium, and endocardium
Myocardium
Endocardium
Epicardium
Parietal Pericardium
Dense fibrous layer
Areolar tissue
Mesothelium
Mesothelium
Areolar tissue
Connective tissues
Pericardial cavity(contains serous fluid)
Muscular wall of the heartconsisting primarily ofcardiac muscle cells
Areolar tissue
Covers the inner surfaces ofthe heart
Endothelium
Covers the outer surface of the heart; also calledthe visceral pericardium
The serous membrane thatforms the outer wall of thepericardial cavity; it and adense fibrous layer form thepericardial sac surroundingthe heart
Module 18.1: Heart wall and tissue
• Cardiac muscle tissue– Compared to skeletal muscle tissue
1. Small cell size2. Single, centrally located nucleus3. Branching interconnections4. Specialized intercellular connections
– Intercalated discs
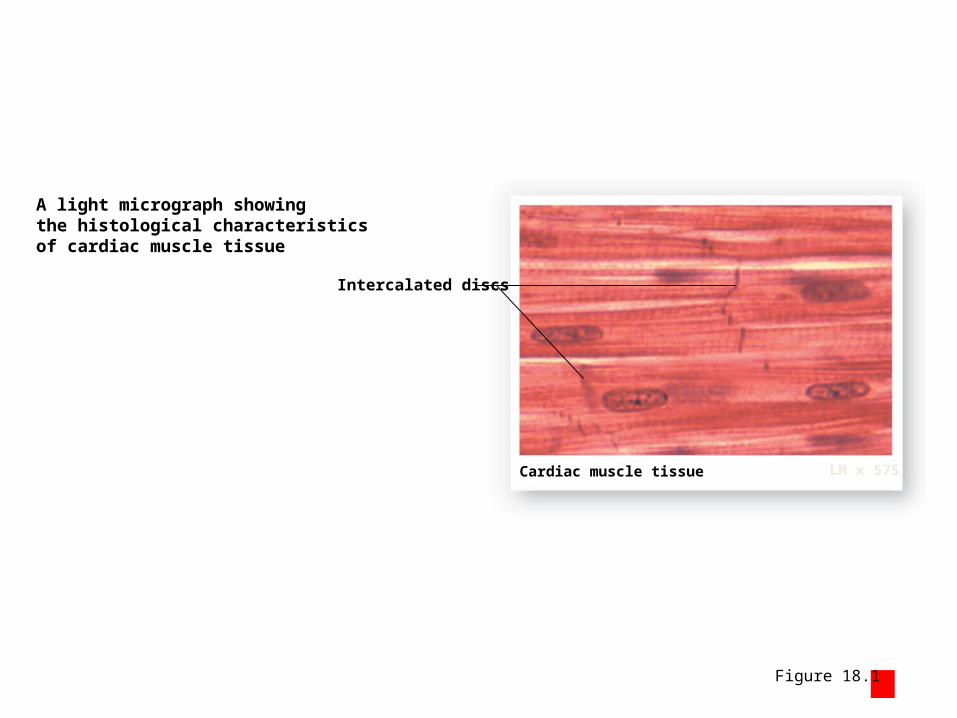
Figure 18.1 3
Intercalated discs
A light micrograph showingthe histological characteristicsof cardiac muscle tissue
Cardiac muscle tissue LM x 575

Module 18.1: Heart wall and tissue
• Cardiac muscle tissue (continued)– Found only in the heart– Cells are striated due to organized myofibrils– Almost totally dependent on aerobic
metabolism for ATP• Large numbers of mitochondria and myoglobin to
store O2
• Has large number of capillaries to supply nutrients and O2

Module 18.1: Heart wall and tissue
• Intercalated discs– Contain: • Desmosomes• Gap junctions
– Allow ions and molecules to move directly between cells» Create direct electrical connection so an action potential
can pass directly between cells
– Stabilize relative positions of adjacent cells– Allow cells to “pull together” for maximum
efficiency– All cells to function “as one” (functional syncytium)
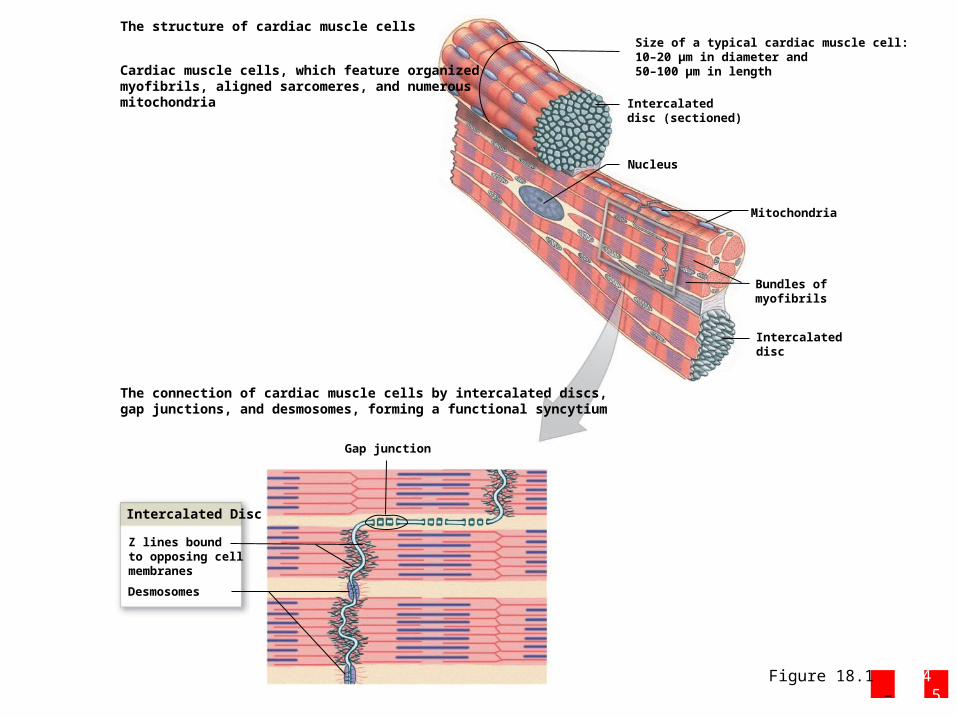
Figure 18.1 4 – 5
The connection of cardiac muscle cells by intercalated discs,gap junctions, and desmosomes, forming a functional syncytium
Intercalated Disc
Gap junction
Z lines boundto opposing cellmembranes
Desmosomes
Intercalateddisc
Bundles ofmyofibrils
Mitochondria
Nucleus
Intercalateddisc (sectioned)
Size of a typical cardiac muscle cell:10–20 μm in diameter and50–100 μm in lengthCardiac muscle cells, which feature organized
myofibrils, aligned sarcomeres, and numerousmitochondria
The structure of cardiac muscle cells

Module 18.1 Review
a. From superficial to deep, name the layers of the heart wall.
b. Describe how the cardiac muscle cells ‘talk’ to one another.
c. Why is it important that cardiac tissue be richly supplied with mitochondria and capillaries?
Module 18.2: Pericardial cavity
• Heart lies within pericardial cavity, a subdivision of the mediastinum
• Mediastinum also contains:– Great vessels (entering and exiting the heart)– Thymus– Esophagus– Trachea
• Because heart is closely associated with many organs, trauma can lead to fluid accumulation that can restrict heart movement (cardiac tamponade)
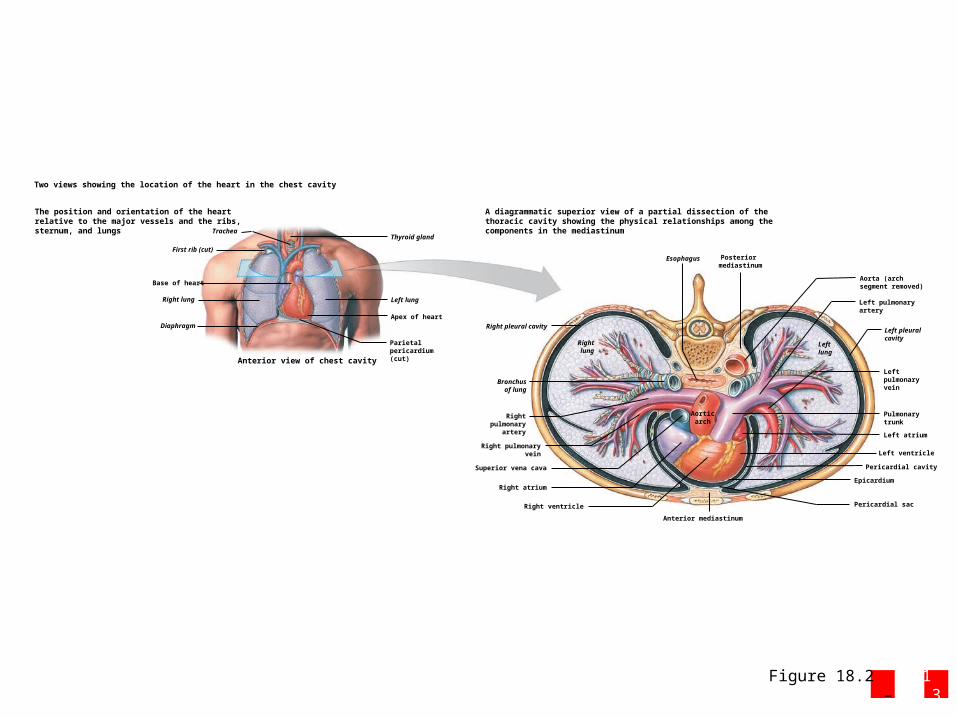
Figure 18.2 1 – 3
The position and orientation of the heartrelative to the major vessels and the ribs,sternum, and lungs
A diagrammatic superior view of a partial dissection of thethoracic cavity showing the physical relationships among thecomponents in the mediastinumTrachea
First rib (cut)
Right lung
Diaphragm
Left lung
Thyroid gland
Base of heart
Apex of heart
Parietalpericardium(cut)Anterior view of chest cavity
Rightlung
Leftlung
Bronchusof lung
Rightpulmonary
artery
Right pulmonaryvein
Right pleural cavity
Esophagus
Right ventricle
Right atrium
Superior vena cava
Anterior mediastinum
Left atrium
Left ventricle
Left pulmonaryvein
Left pleural cavity
Left pulmonaryartery
Pericardial sac
Pericardial cavity
Epicardium
Pulmonarytrunk
Aorticarch
Posterior mediastinum
Aorta (archsegment removed)
Two views showing the location of the heart in the chest cavity
Module 18.2: Pericardial cavity
• Pericardial cavity and fluid– Lined with parietal pericardium• Continuous with visceral pericardium (like balloon
with fist in it)– Contains 10–15 mL of pericardial fluid secreted
by membranes• Acts as lubricant when heart beats
– Swelling of pericardial surfaces can occur with infection causing friction (pericarditis)
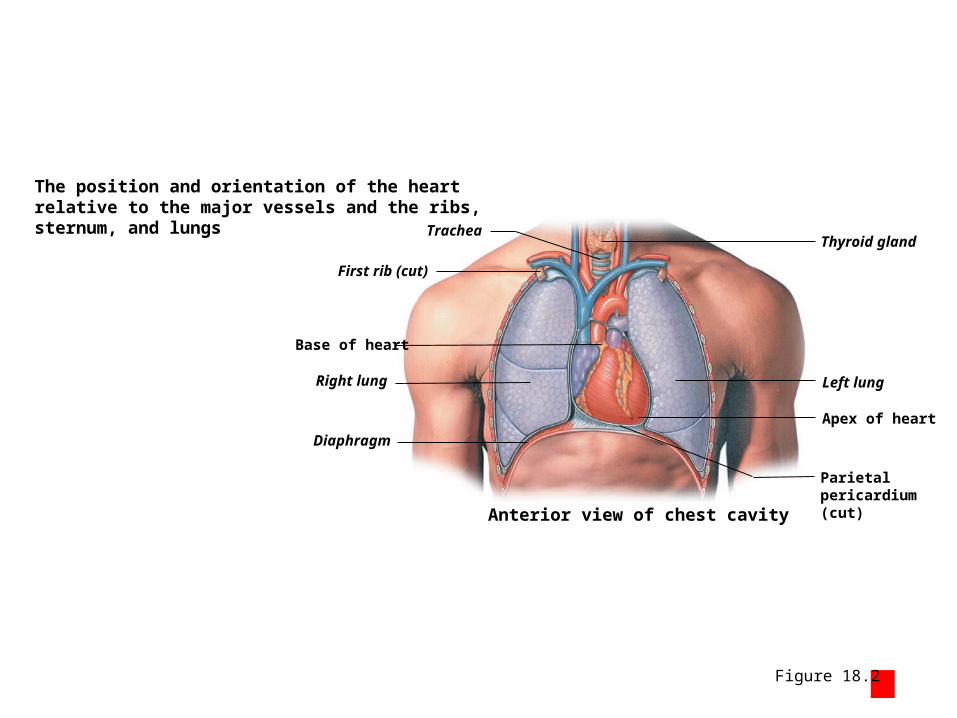
Figure 18.2 1
The position and orientation of the heartrelative to the major vessels and the ribs,sternum, and lungs Trachea
First rib (cut)
Right lung
Diaphragm
Left lung
Thyroid gland
Base of heart
Apex of heart
Parietalpericardium(cut)Anterior view of chest cavity

Figure 18.2 2
Apex of heart
Base of heart
Inner wall (correspondsto epicardium)
Air space (correspondsto pericardial cavity)
Outer wall (correspondsto parietal pericardium)
Balloon
Wrist (correspondsto base of heart)
The positions of and relationshipbetween the heart and thepericardial cavity
The relationship between the heartand the pericardial cavity, which canbe linked to a fist pressed into thecenter of a partially inflated balloon
The location of the pericardialcavity relative to the heart
Pericardial cavitycontainingpericardial fluid
Fibrous attachmentto diaphragm
Fibrous tissue ofpericardial sac
Cut edge ofparietal pericardium
Parietal Pericardium
Cut edge of epicardium
Areolar tissueMesothelium
Module 18.2 Review
a. Define mediastinum.
b. Describe the heart’s location.
c. Why can cardiac tamponade be a life-threatening condition?

Module 18.3: Heart surface anatomy
• Heart surface anoatomy– Sulci (singular, sulcus)
• Surface grooves separating heart chambers– Often with cardiac vessels covered with fat
• Anterior interventricular sulcus– Anterior groove separating ventricles
• Posterior interventricular sulcus– Posterior groove separating ventricles
• Coronary sulcus– Separates atria from ventricles – On posterior surface, contains coronary sinus (collects blood from
myocardium and conveys to right atrium)

Module 18.3: Heart surface anatomy
• Other surface features– Auricles • Expandable extensions of atria
– Ligamentum arteriosum• Fibrous remnant of fetal connection between aorta
and pulmonary trunk

Figure 18.3 1 – 3
A photograph of an anterior view ofa heart from a preserved cadaver
Rightventricle Anterior
interventricularsulcus
Leftventricle
Coronarysulcus
Right atrium
Auricle ofright atrium
Rightatrium
Auricle ofleft atrium
Left ventricle
Auricle of left atrium
Anteriorinterventricularsulcus
Coronarysulcus
Superiorvena cava
Superiorvena cava
Aortic arch
Rightventricle
Ascending aorta
Auricle
Fat
Anterior surface
Cadaver dissection, anterior view
Ascendingaorta
Pulmonarytrunk
Pulmonary trunk
Parietalpericardium
A diagrammatic view of theanterior surface of the heart
Ligamentumarteriosum
Two views of the anterior surface of the heart
Module 18.3 Review
b. Name and describe the shallow depressions and grooves found on the heart’s external surface.
c. Which structures collect blood from the myocardium, and into which heart chamber does this blood flow?

Module 18.4: Coronary circulation
• Coronary circulation– Provides cardiac muscle cells with reliable supplies
of oxygen and nutrients– During maximum exertion, myocardial blood flow
may increase to 9× resting levels– Blood flow is continuous but not steady
• With left ventricular relaxation, aorta walls recoil (elastic rebound), which pushes blood into coronary arteries
Module 18.4: Coronary circulation
• Coronary arteries– Right coronary artery (right atrium, portions of both ventricles
and conduction system of heart)• Marginal arteries (right ventricle surface)• Posterior interventricular artery (interventricular septum and
adjacent ventricular portions)– Left coronary artery (left ventricle, left atrium, and
interventricular septum)• Circumflex artery (from left coronary artery, follows coronary
sulcus to meet right coronary artery branches)• Anterior interventricular artery (interventricular sulcus)
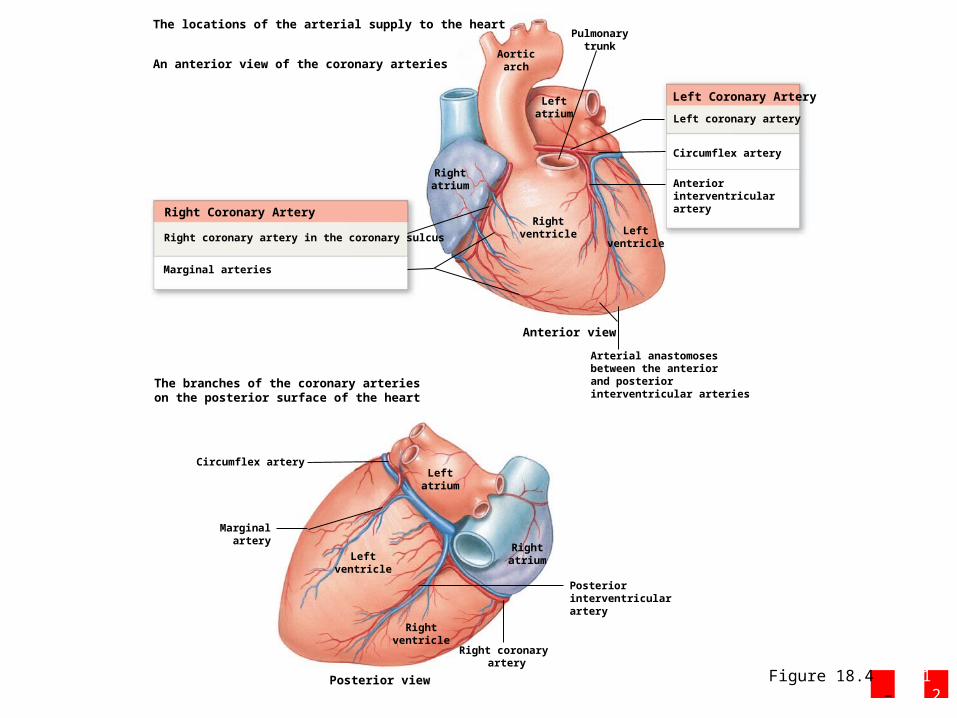
Figure 18.4 1 – 2
The locations of the arterial supply to the heart
An anterior view of the coronary arteries
Right Coronary Artery
Right coronary artery in the coronary sulcus
Marginal arteries
The branches of the coronary arterieson the posterior surface of the heart
Marginalartery
Right coronary artery
Rightatrium
Rightventricle
Leftatrium
Leftventricle
Rightatrium
Rightventricle
Leftatrium
Leftventricle
Posteriorinterventricularartery
Anteriorinterventricularartery
Left coronary artery
Circumflex artery
Arterial anastomosesbetween the anteriorand posteriorinterventricular arteries
Left Coronary Artery
Aorticarch
Pulmonarytrunk
Circumflex artery
Posterior view
Anterior view

Module 18.4: Coronary circulation
• Coronary veins– Great cardiac vein (drains area supplied by
anterior interventricular artery, empties into coronary sinus on posterior)
– Anterior cardiac veins (drains anterior surface of right ventricle, empties into right atrium)

Figure 18.4 3
Leftatrium
Leftventricle
Rightatrium
Rightventricle
Aorticarch
Anterior view
Greatcardiac vein
Anterior cardiac veins
The major collecting vessels on the anteriorsurface of the heart
Module 18.4: Coronary circulation
• Coronary veins (continued)– Coronary sinus (expanded vein, empties into right
atrium)– Posterior cardiac vein (drains area supplied by
circumflex artery)– Small cardiac vein (drains posterior right atrium
and ventricle, empties into coronary sinus)– Middle cardiac vein (drains area supplied by
posterior interventricular artery, drains into coronary sinus)

Figure 18.4 4
Leftventricle
Rightventricle
Rightatrium
Leftatrium
Posterior view
Posteriorcardiac vein
Greatcardiac vein
Middlecardiac vein
Smallcardiac vein
Coronary sinus
The major collecting vessels onthe posterior surface of the heart
Module 18.4 Review
a. List the arteries and veins of the heart.
b. Describe what happens to blood flow during elastic rebound.
c. Identify the main vessel that drains blood from the myocardial capillaries.
Module 18.5: Internal heart anatomy
• Internal heart anatomy– Four chambers• Two atria (left and right separated by interatrial
septum)• Two ventricles (left and right separated by
interventricular septum)– Left atrium flows into left ventricle– Right atrium flows into right ventricle

Module 18.5: Internal heart anatomy
• Right atrium– Receives blood from superior and inferior
venae cavae and coronary sinus– Fossa ovalis (remnant of fetal foramen ovale)– Pectinate (pectin, comb) muscles (muscular
ridges on anterior atrial and auricle walls)• Left atrium– Receives blood from pulmonary veins
Module 18.5: Internal heart anatomy
• Right ventricle– Receives blood from right atrium through right
atrioventricular (AV) valve• Also known as tricuspid (tri, three)
– Has three flaps or cusps attached to tendinous connective fibers (chordae tendineae)
– Fibers connect to papillary muscles» Innervated to contract through moderator band which
keeps “slamming” of AV cusps
• Prevents backflow of blood to atrium during ventricular contraction

Module 18.5: Internal heart anatomy
• Left ventricle– Receives blood from left atrium through right atrioventricular
valve• Also known as bicuspid and mitral (mitre, bishop’s hat) valve• Prevents backflow of blood to atrium during ventricular
contraction• Has paired flaps or cusps
– Trabeculae carneae (carneus, fleshy)• Muscular ridges on ventricular walls
– Aortic valve • Allows blood to exit left ventricle and enter aorta

Figure 18.5 1
The internal anatomy of the heart andthe direction of blood flow betweenthe chambers
Inferiorvena cava
Left AtriumRight Atrium
Left Ventricle
Aortic arch
Pulmonarytrunk
Superiorvena cava
Aortic valve
Ascendingaorta
Moderatorband
Interventricularseptum
Fossa ovalis
Pectinate muscles on the innersurface of the auricle
Opening of the coronary sinus
Receives blood from the superiorand inferior venae cavae and fromthe cardiac veins through thecoronary sinus
Right Ventricle
Left pulmonary veins
Receives blood fromthe pulmonary veins
Thick wall of left ventricle
Left atrioventricular (AV)valve (bicuspid valve)
Trabeculae carneae
Chordae tendineae
Right atrioventricular (AV)valve (tricuspid valve)
Papillary muscle
Pulmonary valve (pulmonarysemilunar valve)

Module 18.5: Internal heart anatomy
• Ventricular comparisons– Right ventricle has relatively thin wall
• Ventricle only pushes blood to nearby pulmonary circuit• When it contracts, it squeezes against left ventricle wall forcing
blood out pulmonary trunk– Left ventricle has extremely thick wall and is round in cross
section• Ventricle must develop 4–6× as much pressure as right to push
blood around systemic circuit• When it contracts
1. Diameter of chamber decreases2. Distance between base and apex decreases

Figure 18.5 2
A sectional view of the heart showingthe thicknesses of the ventricle wallsand the shapes of the ventricularchambers
The relatively thin wallof the right ventricleresembles a pouchattached to the massivewall of the left ventricle
The left ventricle hasan extremely thickmuscular wall and isround in cross section.
Fat in anteriorinterventricular sulcus
Posteriorinterventricular sulcus

Figure 18.5 3
Leftventricle
Rightventricle
The changes in ventricleshape during ventricularcontraction
Dilated (relaxed)
Contracted
Contraction of rightventricle squeezesblood against the thickwall of the left ventricle.
Contraction of left ventricledecreases the diameter of theventricular chamber and reducesthe distance between the baseand apex
Module 18.5 Review
a. Damage to the semilunar valves on the right side of the heart would affect blood flow to which vessel?
b. What prevents the AV valves from swinging into the atria?
c. Why is the left ventricle more muscular than the right ventricle?
d. Name the four cardiac chambers.