transfusion medicine iii complications and safety of transfusion practices
DESCRIPTION
Transfusion Medicine III Complications and Safety of Transfusion Practices. Salwa Hindawi Medical Director of Blood Transfusion Services KAUH. Donor Patient. The risks associated with transfusion can be reduced by: - Effective blood donor selection. - PowerPoint PPT PresentationTRANSCRIPT
4th year medical students 2nd Feb,2008
Transfusion Medicine IIIComplications and Safety of Transfusion
Practices
Salwa Hindawi
Medical Director of Blood Transfusion ServicesKAUH
4th year medical students2nd Feb,2008
The risks associated with transfusion can be reduced by: - Effective blood donor selection.- Screening for TTI in the blood donor population. high quality blood grouping, compatibility testing. - Component separation and storage.
- Appropriate clinical use of blood and blood products. - Quality assurance
Donor Patient
4th year medical students 2nd Feb,2008
Principles of Clinical Transfusion Practices
Avoid blood transfusion Transfusion is only one part of the
patient’s management. Prevention and early diagnosis and
treatment of Anemia & underlying condition
Use of alternative to transfusion.eg. IV fluids
Good anesthetic and surgical management to minimized blood loss.
4th year medical students 2nd Feb,2008
– Prescribing should be based on Prescribing should be based on national guidelines on the clinical use national guidelines on the clinical use of of blood taking individual patient blood taking individual patient needs into needs into account.account.
– Hb level should not be the sole Hb level should not be the sole deciding Factor Clinical evaluation is deciding Factor Clinical evaluation is importantimportant
4th year medical students 2nd Feb,2008
– Consent form to be obtained from the patient before transfusion.
– The clinician should record the reason for transfusion clearly.
– A trained person should monitor the transfused patient and if any adverse effects occur respond immediately.
4th year medical students 2nd Feb,2008
Paid Directed Volunteers
4th year medical students 2nd Feb,2008
Blood Donation
• WB every 8 weeks, Hct > 38%
• Plateletpheresis every 3 days or 24 times per year, Hct > 38%
• Autologous Blood– WB every 3 days (twice/week)– up to 3 days prior to surgery– Hct > 33%
4th year medical students 2nd Feb,2008
Donor Selection
Is Important
To Be Sure That The Donor Is Fit To DonateThe Required Amount Of BloodBlood Donation Will Not Harm The Donor
The Donated Blood Should Be Safe And FreeFrom Transfusion Transmitted Infections TTI
4th year medical students 2nd Feb,2008
Donor Selection
I. Interview
II. Questionnaires
III. Physical examination
Donor safety
Patient safety
4th year medical students 2nd Feb,2008
Single Donation Testing
Different countries screen for different organisms.Each country has to set its own policies for screeningof donors.
i. Serological screeningii. Microbiological screening
HIV I & II (Ag-Ab), HBV, HCV, Syphilis
HTLV-I & IIHBcAb
Special donors for CMVMalaria screen (in some countries)
4th year medical students 2nd Feb,2008
Confirmatory tests
Any reactive donation should repeat testing in duplicate. If any of the repeated tests is reactive, a sample should be send to a reference laboratory and the donation will be destroyed by autoclaving or used for batch validation or quality control purposes.
4th year medical students 2nd Feb,2008
Complications of Blood Transfusion
Immediate Delayed
HTR GVHD
FNTR PTP
TRALI Iron overload
Bacterial Infectious
contamination diseases
Allergic, Anaphylaxis Alloimmunization
4th year medical students 2nd Feb,2008
Acute Hemolytic Transfusion Reaction
• a clerical error (wrong specimen, wrong patient)
• 1 in 6,000 to 25,000 transfusions
• back pain, chest pain, fever, red urine, oliguria, shock, DIC, death in 1 in 4
• stop the transfusion
4th year medical students 2nd Feb,2008
Work up of An AHTR
• start normal saline
• treat patient symptomatically
• send blood bag and tubing to culture
• send red top and purple top tubes
• urine specimen for hemoglobinuria
• DAT is positive
4th year medical students 2nd Feb,2008
Non Hemolytic Febrile Transfusion Reaction
• NHFTR (1:100)
• Recipient has WBC antibodies to Donor WBCs contained within RBCs and Plateletpheresis products
• DAT is negative
• rise in temperature by 2F or 1C
• other causes for fever are eliminated

4th year medical students 2nd Feb,2008
Allergic (Urticarial) Transfusion Reaction
• Recipient has antibodies to the Donor’s plasma proteins (1 in 1000)
• offending protein is not identified
• urticaria, itching, flushing, wheezing
• this is the only transfusion reaction where the blood that is hanging can be restarted after treatment with Benadryl
• if symptoms continue then STOP
4th year medical students 2nd Feb,2008
Anaphlyactic Transfusion Reaction
• anaphylactic reaction (1 in 150,000)
• 1 in 700-900 people never made IgA
• occurs when exposed to normal blood products which contain IgA
• bronchospasm, vomiting and diarrhea and vascular collapse
• treat with Epinepherine, Solu-Medrol,
4th year medical students 2nd Feb,2008
Circulatory Overload
• marginal cardiovascular status
• given blood components too rapidly
• develops acute shortness of breath, heart failure, edema (1: 10,000)
• systolic BP increases 50 mm
• infuse slowly, not to exceed 4 hours
• split the unit of RBC and give half
4th year medical students 2nd Feb,2008
Transfusion Related Acute Leukocyte Lung Injury
• TRALI reaction (1:10,000)
• Donor plasma contains WBC antibodies that when transfused to the recipient cause agglutination of recipient’s WBC in the pulmonary capillary beds
• Chest X ray looks like ARDS
• Donor removed from donating blood

4th year medical students 2nd Feb,2008
Transfusion - Related Acute Lung Injury (TRALI)
A potentially fatal transfusion reactionManifested usually within 6hrs after transfusionCharacterised by
Hypoxemia PaO2/ FiO2< 300mmhg O2 sat <90% on room air
Chest X-ray:Bilateral hilar infiltratesAbsence of evidence of circulatory overload
Toronto TRALI Concensus Conference 1 April 2004Transfusion,44;1774-91 Dec 2004
4th year medical students 2nd Feb,2008
Diagnosis
High Index of suspicion / Timing of Transfusion
Blood Gases
Chest X-ray
hypoxia and pulmonary oedema ; most consistent findings.
Diagnosis of exclusion
4th year medical students 2nd Feb,2008
TRALI Non-cardiogenic pulmonary oedema(result of increased vascular permeability)
The first sign of the reaction can be“Production of copious quantities of frothyblood-tinged fluid” from the endotracheal tubeduring intubation
4th year medical students 2nd Feb,2008
Other courses of pulmonary oedema
• Volume Overload• Congestive heart failure• Myocardial infarction
Response to diuretics?
Differential Diagnosis
4th year medical students 2nd Feb,2008
Other Differential Diagnosisacute reaction
• Acute haemolytic transfusion reaction
• Bacterial infection(TTI)
• Acute anaphylaxis IgA def with anti-IgA
4th year medical students 2nd Feb,2008
Management
• Adequate respiratory support
100% patients need O2 support
71% required mechanical ventilation
Steroids not beneficial
Important to distinguish TRALI from volume overload
Treatment with diuretics may have a detrimental effect /reduced cardiac out put.May need fluid support.
4th year medical students 2nd Feb,2008
Sepsis from Bacterial Comtamination
• Platelets:– skin contaminants most common cause– plateletpheresis 1 in 5000– pooled platelets 1 in 1000
• RBC:– Sepsis from RBC due to Yersinia,
Enterics or Gram Positive 1 in 3,000,000
4th year medical students 2nd Feb,2008
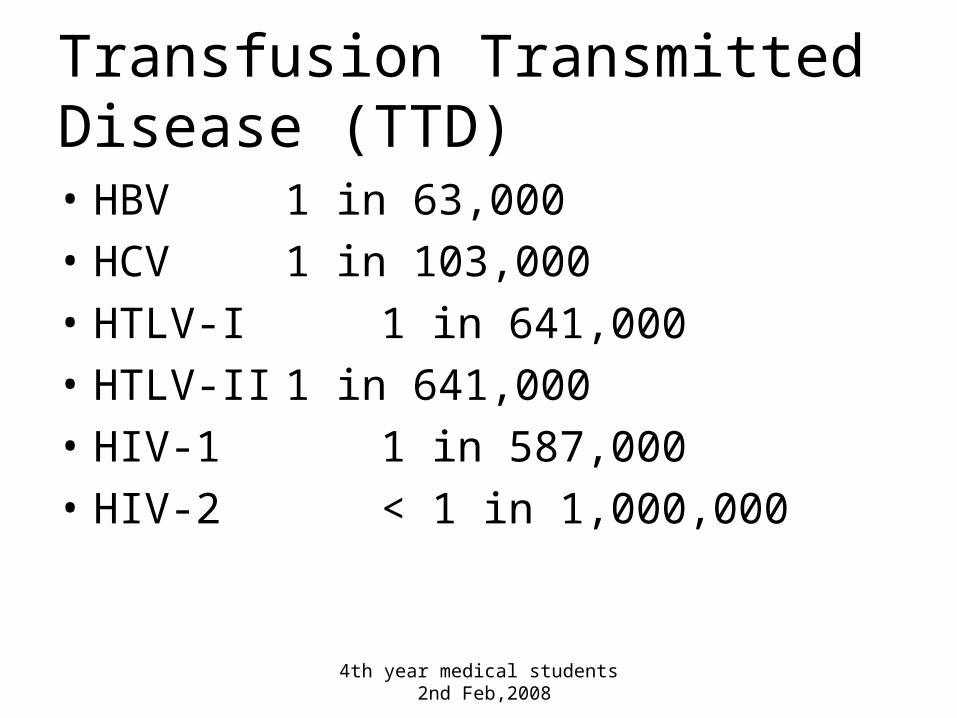
Transfusion Transmitted Disease (TTD)• HBV 1 in 63,000
• HCV 1 in 103,000
• HTLV-I 1 in 641,000
• HTLV-II 1 in 641,000
• HIV-1 1 in 587,000
• HIV-2 < 1 in 1,000,000
4th year medical students 2nd Feb,2008
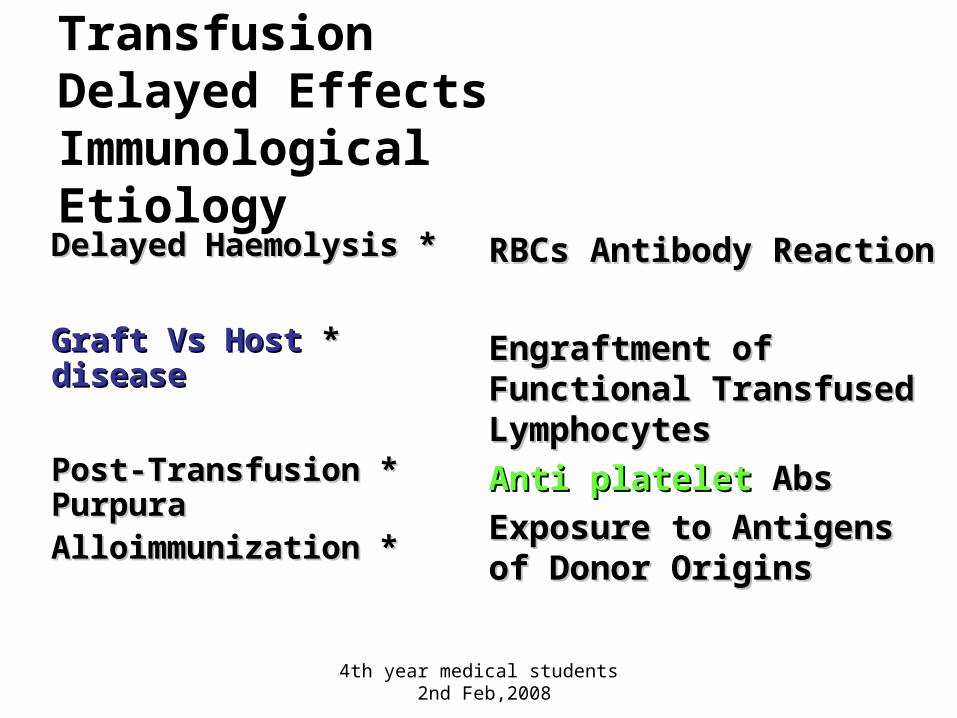
Adverse Effects of TransfusionDelayed Effects Immunological Etiology
* *Delayed HaemolysisDelayed Haemolysis
* *Graft Vs Host Graft Vs Host diseasedisease
* *Post-Transfusion Post-Transfusion PurpuraPurpura
* * AlloimmunizationAlloimmunization
RBCs Antibody ReactionRBCs Antibody Reaction
Engraftment of Engraftment of Functional Transfused Functional Transfused LymphocytesLymphocytes
Anti platelet Anti platelet AbsAbs
Exposure to Antigens of Exposure to Antigens of Donor OriginsDonor Origins
4th year medical students 2nd Feb,2008
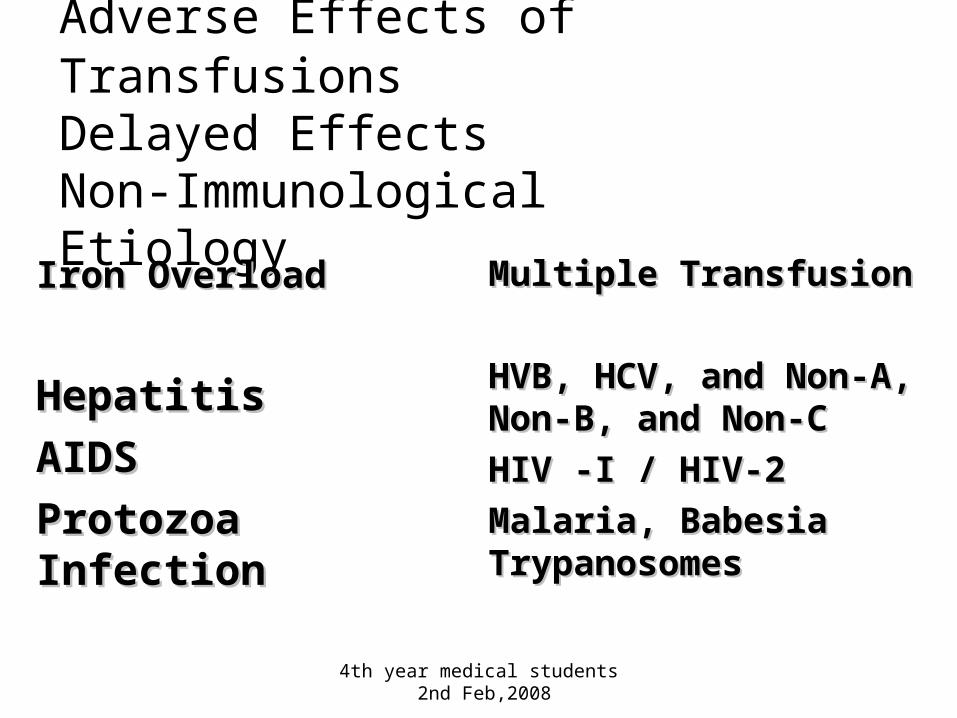
Adverse Effects of TransfusionsDelayed EffectsNon-Immunological Etiology
Iron OverloadIron Overload
HepatitisHepatitis
AIDSAIDS
Protozoa Protozoa InfectionInfection
Multiple TransfusionMultiple Transfusion
HVB, HCV, and Non-A, HVB, HCV, and Non-A, Non-B, and Non-CNon-B, and Non-C
HIV -I / HIV-2HIV -I / HIV-2
Malaria, Babesia Malaria, Babesia TrypanosomesTrypanosomes
4th year medical students 2nd Feb,2008