transfusion associated dyspnea (tad) · at the conclusion of this presentation, the audience should...
TRANSCRIPT

Transfusion Associated Dyspnea (TAD):“A ROSE”* by Many Other Names?
International Haemovigilance Seminar Meeting
Manchester, UK July 10,2018
Chester Andrzejewski, Ph.D., M.D., F.C.A.P.Director of System Blood Banking & Transfusion/Apheresis Medicine Services
Baystate Health, Springfield, MA 01199 USAAssistant Professor, Department of Pathology
University of Massachusetts Medical School-Baystate, Worcester, MA USA
“…What’s in a name? that which we call a rose
By any other name would smell as sweet;…”Romeo and Juliet, Act II, Scene I,
William Shakespeare English Playwright & Poet, 1564-1613
* = “Adverse Respiratory Outcomes & Sanguine Excess”
Copyright 2018 Chester Andrzejewski/Baystate Health

At the conclusion of this presentation, the audience should be able to:
1. Describe a brief history of Transfusion Associated Dyspnea (TAD) & appreciate the “existential nature” of it.
2. Identify various issues, strategies & "tools” to further our understanding of TAD.
3. Define possible models of TAD that may explain selected aspects relating to it.

Disclosures
No Financial Conflicts of Interest
Please Note:
Presenter’s discussion of data provided by various haemovigilance entities does not represent any
formal endorsements by these entities regarding his comments and solely reflects the views and opinions
of the Presenter.

Presentation Outline• Opening Comments /Historical Overview
• Defining Transfusion Associated Dyspnea (TAD)
• TAD Standard Reporting Criteria
• Modeling TAD
• Summary
• Closing Comments & Questions/Answers

Acknowledgements
AABB Department of Research, AABB Center for Patient Safety (CPS), &AABB Patient Safety Organization (PSO) Advisory Committee,
Barbee Whitaker, Ph.D.Gabriela E. Perez, M.S.Srijana Rajbhandary, M.PH.Maximilienne Mbinack
Massachusetts Department of Public Health (MDPH)
Melissa Cumming, M.S.Christina Brandeburg, M.P.H.Alexandra De Jesus, M.P.H.
Baystate Medical Center Transfusion Medicine Services
Lynne O’Hearn,MT,(ASCP)Kelly Passanisi, MT(ASCP)
UMMS-Baystate | Pathology Residency ProgramSajjad Hassan, M.D.
UMMS-Baystate | Medicine-Pediatrics Residency ProgramNura El Haj ,M.D.
“Where no counsel is, the people fall: but in the multitude of counsellors there is safety.” Proverbs 11:14.

Answer: Maybe …
But perhaps a more fundamental & appropriate question should be…
So What Exactly are We Observing in Patients We Classify as Experiencing TAD ?
Genesis of the Session

Genesis of the Session
“… A little learning is a dangerous thing;
Drink deep, or taste not the Pierian spring …”
“… For fools rush in where angels fear to tread …”
An Essay on CriticismAlexander Pope, English Poet (1688–1744).
`Would you tell me, please, which way I ought to go from
here?'
`That depends a good deal on where you want to get to,'
said the Cat.
`I don't much care where--' said Alice.
`Then it doesn't matter which way you go,' said the Cat.
`--so long as I get somewhere,' Alice added as an
explanation.
`Oh, you're sure to do that,' said the Cat, `if you only walk
long enough.‘
― Lewis Carroll, Alice in Wonderland
Answer: Unclear;
Hence, a need to embark on a Journey of Discoverythat examines this entity more closely.
Down the Rabbit Hole We Go…

https://www.google.com/search?source=hp&ei=tUi-WoGuA4z2zgKygq2IBA&q=rabbithole&oq=rabbithole&gs_l=psy-ab.3..0i46k1j46l2j0l2j0i10k1l3j0l3j0i10k1.2567.5822.0.8607.10.9.0.1.1.0.170.1143.0j9.9.0....0...1c.1.64.psy-ab..0.10.1171...0i131k1.0._3pd2zW74gk. Accessed 2018.03.30.
So Welcome on Our Journey Downthe “TAD’s Rabbit Hole …
orperhaps from another perspective…
Adventures in Biovigilance Wonderland ?
But remember…Chance favors the prepared mind.
Louis Pasteur (1822-1895)
Our First Stop:The Concept of "Frames of Reference”
a
https://www.merriam-webster.com/dictionary/frame%20of%20reference. Accessed 2018.02.22.
Framing the Subject Context & Questionsto be Addressed
Frames of Reference: A Bottom-line Take-Home Message
(Not Just for TAD, but Everything We Do Regarding Haemovigilance)

Major Frames of Reference Regarding TADThat Need to Be Considered
1. Bedside “Practitioners” - Physicians/Nurses/Ancillary Staff/Patients
2. Blood Banks/Transfusion Medicine Services- Product/Process/Person
3. Haemovigilance Networks- Multiple Perspectives
4. Professional/Regulatory/Accreditation Entities- Multiple Perspectives
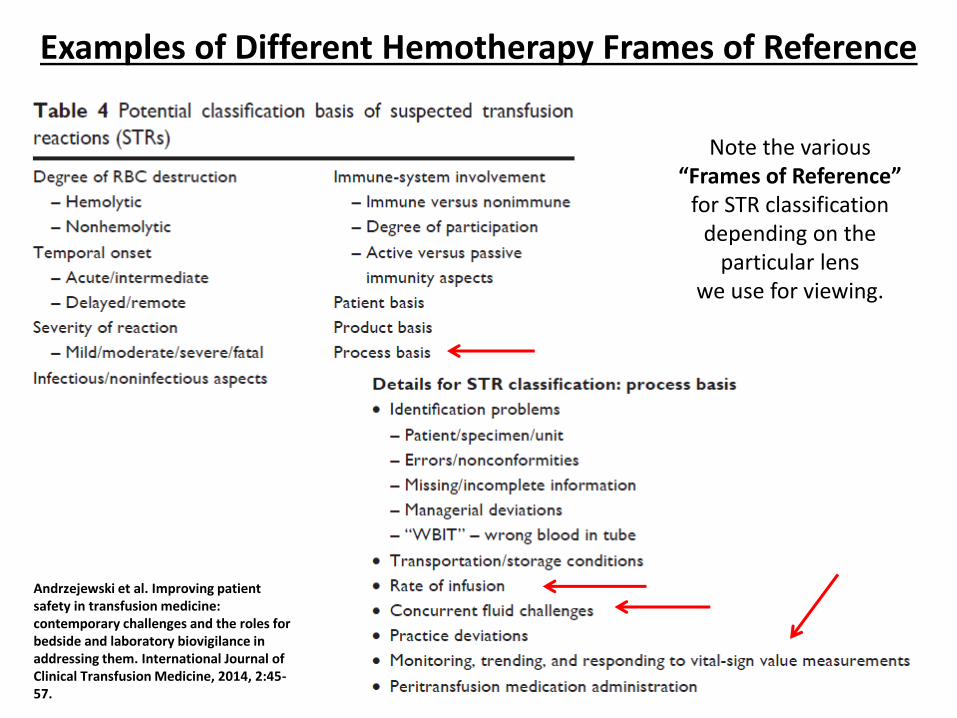
Examples of Different Hemotherapy Frames of Reference
Andrzejewski et al. Improving patient safety in transfusion medicine: contemporary challenges and the roles for bedside and laboratory biovigilance in addressing them. International Journal of Clinical Transfusion Medicine, 2014, 2:45-57.
Note the various “Frames of Reference”
for STR classificationdepending on the
particular lenswe use for viewing.

Presentation Outline• Opening Comments /Historical Overview
• Defining Transfusion Associated Dyspnea (TAD)
• TAD Standard Reporting Criteria
• Modeling TAD
• Summary
• Closing Comments & Questions/Answers

Our Next Stop Down the Rabbit-Hole:A Potential Way to Classify the BIRDS*
Transfusion Associated Adverse Pulmonary Sequelae (TAAPS)
A TAAPS Taxonomy Field Guide: “BIRDS” of a Feather Flocking Together?
Rare “BIRDS”…Canaries in Coal Mines…
or… Both?
*= Blood Induced Respiratory Distress Syndromes

TRALI TADTACO
T e
The Transfusion Associated Adverse Pulmonary Sequelae (TAAPS) Umbrellaand the “Clouds of Uncertainty”
“The Sequelae Umbrella”
C. Andrzejewski, 2018
Allergic / Anaphylactic ReactionsBacterial Sepsis /Air Emboli
Intra-Vascular Hemolysis Pre-Existing / Intercurrent Disease
Idiopathic / Combination of Above
RARE BIRDS*
Really Rare BIRDS* ?
* = Blood Induced Respiratory Distress Syndromes

https://www.google.com/search?q=optical+illusions&tbm=isch&tbs=rimg:CRMrmdyYY2-QIjiAqpzBFsMmSk9_1dmU9AOgYLq1yvskyzkC_1CMlz4II_1CUWOmb7kMLq287r8KeUD2n13SxF_1XLKHqioSCYCqnMEWwyZKETVK5MGXxtV3KhIJT392ZT0A6BgRyz2NG1dpzlIqEgkurXK-yTLOQBHDHXxSFOekyyoSCb8IyXPggj8JEWUazstnjEeTKhIJRY6ZvuQwurYRuecr20594PgqEgnzuvwp5QPafREx9_1NjWRpTSyoSCXdLEX9csoeqEb87ILwRhTYY&tbo=u&sa=X&ved=2ahUKEwjApuODz9raAhXOtlkKHSlvCLwQ9C96BAgAEBg&biw=1280&bih=922&dpr=1#imgrc=87r8KeUD2n0x7M:&spf=1524837714110.Accessed 2018.04.27.
TAD: A Rare BIRD?If It Looks Like a Duck, Walks Like a Duck, and Quacks Like a Duck,
It’s a Duck ………. or Is It?

Next Stop: Confronting Some Fundamental Questions
1. Really basic issues: How is it spelled, pronounced, & what does it literally mean?
2. How much medical literature actually exits related to it?
3. When/where did the terminology first appear in the medical literature?
4. How is it defined by HV Networks, Blood Banks, & at the bedside?
5. What is its etiopathogenesis?
6. How does TAD relate to other Transfusion Associated Adverse Pulmonary Sequelae (TAAPS)?
7. How can it be prevented or mitigated?
8. How can a knowledge of TAD help inform our inquiries into other TAAPS conditions and enhance blood safety?

https://www.google.com/search?source=hp&ei=phuDWuuMMIi45gLJmp6gBw&q=tad&oq=tad&gs_l=psy-ab.3..0j0i131k1j0j0i131k1l3j0l4.2542.14239.0.18981.18.9.8.1.2.0.98.607.9.9.0....0...1c.1.64.psy-ab..0.18.837...0i10k1.0.qaRup_DgDc0.Accessed 2018.02.13.
Q1. Really basic issues: How is it spelled, pronounced, & what does it literally mean?
https://www.google.com/search?source=hp&ei=CAr_WpWdKJH45gK_363YCg&q=dyspnea&oq=dypn&gs_l=psy-ab.1.0.0i10k1l10.2015.5918.0.7514.4.4.0.0.0.0.116.429.1j3.4.0....0...1c.1.64.psy-ab..0.4.426...0j0i131k1.0.MqHvOCsTH0Q.Accessed2018.05.18.
TransfusionAssociatedDyspnoea

https://www.ncbi.nlm.nih.gov/pubmed/?term=Transfusion+Associated+Dyspnea.Accessed 2018.03.23.
Q2. How much medical literature actually exits related to it ?
WOW !!!

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3076325/.Accessed 2018.04.03.
Q3. When/where did the terminology first appear in the medical literature?
OCTOBER 2008

Transfusion Associated Dyspnea (TAD):Fundamental Questions
1. Really basic issues: How is it spelled, pronounced, & what does it literally mean?
2. How much medical literature actually exits related to it?
3. When/where did the terminology first appear in the medical literature?
4. How is it defined by HV Networks, Blood Banks, & at the bedside?
5. What is its etiopathogenesis?
6. How does TAD relate to other Transfusion Associated Adverse Pulmonary Sequelae (TAAPS)?
7. How can it be prevented or mitigated?
8. How can a knowledge of TAD help inform our inquiries into other TAAPS conditions and enhance blood safety?

http://www.ihn-org.com/wp-content/uploads/2011/06/ISBT_definitions_final_2011_TRALIcorrection2013.pdf. Accessed 2018/02/13.
A “ TAD” Too Far, a “TAD” Too Less …or a “TAD” Just Right?
Q4. How is it defined by HV Networks, Blood Banks, & at the bedside?
Answer: Somewhat Nebulously.

Limited data from various HV networks.
Published reports typically indicate that TAD is a milder, less frequent entity potentially occurring within a broad spectrum
of underlying clinical conditions.
More severe expressions of it may be encountered.3,4,5
TAD can occur in patients of all ages with all types of blood products.
Pediatric patients may be more susceptible to TAD especially with respect to platelet transfusions.4
What Does the Literature Tell Us ?

Analyses of aggregated data from the ISTARE database(25 countries; 2006 to 2012 timeframe) revealed:
TAD frequencies of 2.2% of all reactions and 4.8% of all serious reactions.5
349 reported deaths (58% related to three acute reactions involving the respiratory system, i.e., TACO, TRALI, TAD);
27% Attributed to TACO19% Attributed to TRALI
12% Attributed to TAD
International Surveillance database of Adverse Reactions and Events (ISTARE) Report (2016)

Information from Some Haemovigilance Entities
1. Massachusetts Department of Public Health
State Mandated Participation Program
(via CDC NHSN Hemovigilance Module since June 2014)
2. AABB Center for Patient Safety
Patient Safety Organization (PSO)
3. Baystate Medical Center, Springfield, MA USA
Hospital Based Haemovigilance Program


Data Source: MDPH
1.MDPH 2016 Annual Report
2. MDPH TAD ReactionsFocused Review 2015-2017
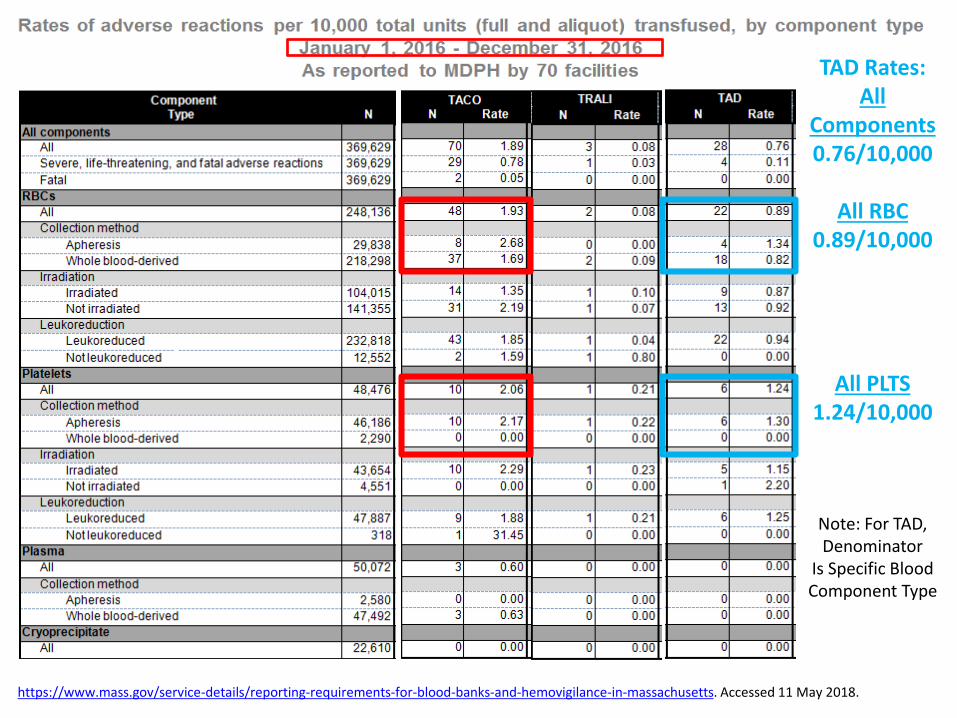
https://www.mass.gov/service-details/reporting-requirements-for-blood-banks-and-hemovigilance-in-massachusetts. Accessed 11 May 2018.
TAD Rates:All
Components0.76/10,000
All RBC0.89/10,000
All PLTS1.24/10,000
Note: For TAD,Denominator
Is Specific Blood Component Type

https://www.mass.gov/service-details/reporting-requirements-for-blood-banks-and-hemovigilance-in-massachusetts. Accessed 11 May 2018.
Note TAD Gender Difference: F >>> M (~3X); F > M seen over most Age Ranges.

Data Source MDPH
1.MDPH 2016 Annual Report
2. MDPH TAD ReactionsFocused Review 2015-2017

MDPH TAD Reactions Focused Review: 2015-2017
Data Source: MDPH 2015-17 Extended Data Analyses
Majority of TAD reactions (~72%) occur with RBC units (51/71)in hospitals with large transfusion volumes and/or of bed sizes >= 300 beds.
Fairly Constant
Frequency
One TAD Fatality
(3/2017):Granulocytes

MDPH TAD Reactions Focused Review: 2015-2017
Data Source: MDPH 2015-17 Extended Data Analyses
With regard to:Gender & TAD: F >> M (~2X); Peak Age Incidence Range: 60-89 years.

MDPH TAD Reactions Focused Review: 2015-2017Conditions Reported as Symptoms in TAD Reactions
Data Source: MDPH 2015-17 Extended Data Analyses
Somewhat Surprisingly
is theSecond Most
Common Symptom
Encountered,i.e., “Other”.

MDPH TAD Reactions Focused Review: 2015-2017Conditions Reported in “Other” Symptom Category
Data Source: MDPH 2015-17 Extended Data Analyses
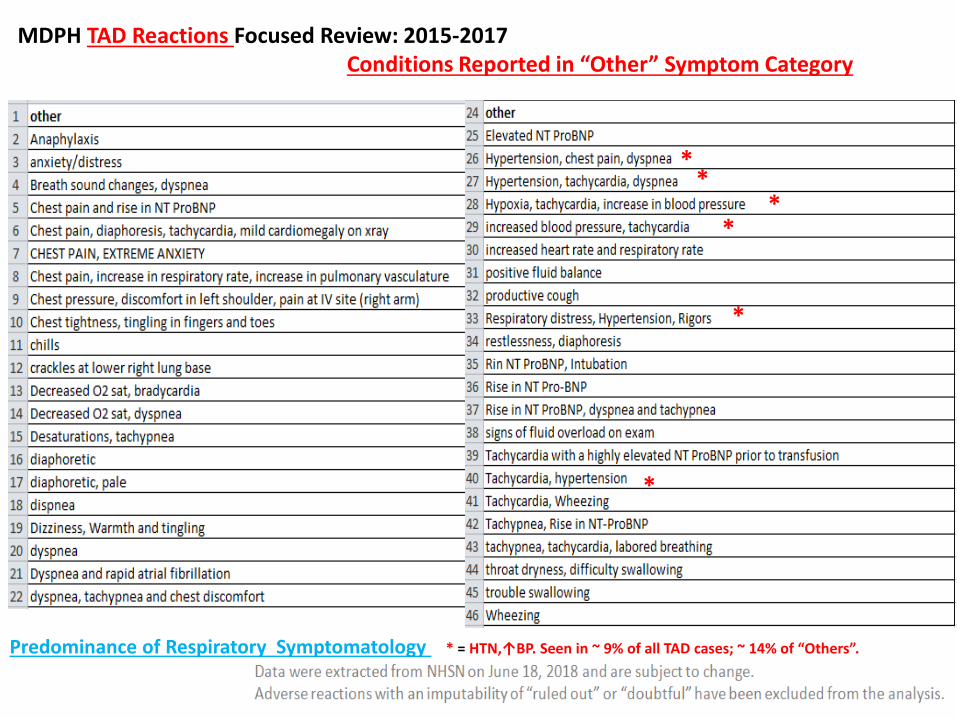
MDPH TAD Reactions Focused Review: 2015-2017Conditions Reported in “Other” Symptom Category
Predominance of Respiratory Symptomatology * = HTN,↑BP. Seen in ~ 9% of all TAD cases; ~ 14% of “Others”.
*
**
**
*
Data from AABB Center for Patient Safety (CPS)
Focused Review Study Regarding Pulmonary Transfusion Reactions

Data from AABB Center for Patient Safety (CPS)Patient Safety Organization(PSO)
Reaction Rates: 1 Jan 2015 – 30 June 2017
www.aabb.org 2
• A total of 415 respiratory reactions were reported to the AABB Center for Patient Safety PSO from January 2015 to June 2017. – 257 TACO reactions (Rate of 0.14 per 1,000 units + aliquots
transfused)– 133 TAD reactions (Rate of 0.07 per 1,000 units + aliquots
transfused) (~ 32 % of all respiratory reactions)– 25 TRALI reactions (Rate of 0.01 per 1,000 units + aliquots
transfused)
• 1,840,748 transfusions were reported during this period of time.

TACO,TRALI, TAD Reaction Rates
www.aabb.org 3
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
2015Q1(n=21)
2015Q2(n=8)
2015Q3(n=8)
2015Q4(n=15)
2016Q1(n=16)
2016Q2(n=21)
2016Q3(n=29)
2016Q4(n=17)
2017Q1(n=17)
2017Q2(n=13)
Rea
ctio
n R
ate
per
1,0
00
un
its
tran
sfu
sed
Calendar Quarter (n = reporting organizations)
Respiratory Reaction Rates Q1 2015 - Q2 2017
TACO TRALI TAD
TACO
TAD
TRALI

AABB CPS Tool: Respiratory Reactions Supplemental Form
Adverse Pulmonary Reaction Tool
Requesting Additional Data Elements

AABB CPS Tool: Respiratory Reactions Supplemental Form

Timing of Onset of Symptoms
www.aabb.org
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
TACO (N=64)
TRALI(N=9)
TAD(N=50)
61%56%
72%
20%
11%
18%
16%
33%
6%
3% 4%
Per
cen
t o
f To
tal I
nd
icat
ed R
eact
ion
s
Time of Onset of Symptoms
>6 <24 hours aftercessation of transfusion
1-6 hours aftercessation of transfusion
Within 1 hour oftransfusion cessation
During the transfusion
Majority of all patients exhibited symptoms onset
during HT: [TACO (61%); TRALI (56%);
TAD (72%)].
Minority of TAD patients (6%)
exhibited symptoms onset
1-6 hours after HT cessation.

Questions Related to Fluid Status
24% of TAD Patients (12/50)with Positive Fluid Balance
46% of TAD Patients (23/50)with Suspected Volume Overload

26% of TAD Patients (13/50) Had History of CHF
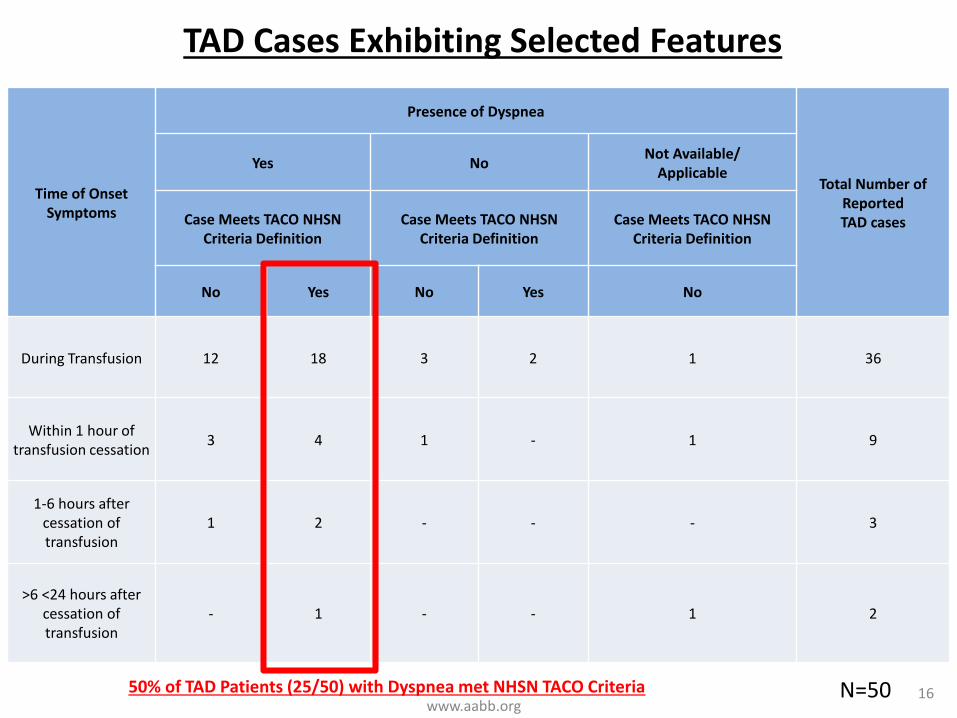
TAD Cases Exhibiting Selected Features
www.aabb.org16
Time of Onset Symptoms
Presence of Dyspnea
Total Number of Reported TAD cases
Yes NoNot Available/
Applicable
Case Meets TACO NHSN Criteria Definition
Case Meets TACO NHSN Criteria Definition
Case Meets TACO NHSN Criteria Definition
No Yes No Yes No
During Transfusion 12 18 3 2 1 36
Within 1 hour of transfusion cessation
3 4 1 - 1 9
1-6 hours after cessation of transfusion
1 2 - - - 3
>6 <24 hours after cessation of transfusion
- 1 - - 1 2
50% of TAD Patients (25/50) with Dyspnea met NHSN TACO Criteria N=50

Time of Recovery
www.aabb.org 13
RespiratoryReaction
<1 day after onset of symptoms
>1 <7 days afteronset of
symptoms*
>7 <28 days after onset of symptoms
>28 days after onset of symptoms
No recovery (death)
TACO(N=64)
42% 47% 6% 5%
TRALI (N=9)
33% 56% 11%
TAD (N=50)
70% 20% 6% 4%
*The following categories were combined: > 24 hours after onset of symptoms and >1 <7 days after onset of symptoms.
A TAD Tail?Although 70% of TAD patients recover in < 1 day,
~ 30% manifest longer recovery periods.

Transfusion Associated Dyspnea (TAD): Some Fundamental Questions
1. Really basic issues: How is it spelled, pronounced, & what does it literally mean?
2. How much medical literature actually exits related to it?
3. When/where did the terminology first appear in the medical literature?
4. How is it defined by HV Networks, Blood Banks, & at the bedside?
5. What is its etiopathogenesis?
6. How does TAD relate to other Transfusion Associated Adverse Pulmonary Sequelae (TAAPS)?
7. How can it be prevented or mitigated?
8. How can a knowledge of TAD help inform our inquiries into other TAAPS conditions and enhance blood safety?

So What Does It All Mean?
Our Next Stop in the Rabbit Hole:
Constructing and Examining a
Potential Model*
for
Transfusion Associated Dyspnea (TAD)
* Via an Interchange with a “Budding”
Transfusion Medicine Specialist, TACO Aficionado &
my Trusted Buddy, much younger Colleague, “Dr. Sunshine”.

TAD
Laying the Foundation for a Potential Model of TAD:
“The Quantum Cheshire Cat of TAAPS”?
TAD

Transfusion.53:3037-3047.2013.

A Multiphasic Model for TACO
Post-TACO: A Postdromal State of TACO
That postcedent condition on the TACO/Fluid
Challenges continuum involving changes within the
pulmonary space, chiefly characterized by
respiratory system alterations, occurring in the
paucity/absence of and/or after
initial cardiovascular system manifestations.
Can some cases of TAD be postcedent states of TACO,
i.e., Does Post–TACO = TAD?

Transfusion.53:3037-3047.2013.
Is TAD a Postdromal Condition or Cataphoric State of TACO (“cTACO”) ?
TAD
TACO, i.e., the preceding or predicate state, is a cataphor when it points to its right toward a latter or postcedent condition, i.e., TAD.

https://onlinelibrary.wiley.com/doi/pdf/10.1111/vox.12262. Accessed on 2018.03.02.

Answer:
Remains to be determined
but …
is there a possibility that certain
endotypes of TADmay have unique
features associated with them,
e.g., a seasonality aspect?

Data Source: MDPH / All Hospitals 2015-17 (36 months); 1=January
Tota
l Nu
mb
er
of
Eve
nts
(N
)Figure 1: Number of TAD Adverse Events (N) by Month & Year
(Years 2015-17 (36 Months); All MA Hospitals)
Calendar Year Month
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10 11 12
2015
2016
2017
Total N = 71
2016
2017
2015
JAN DEC

Data Source: MDPH 2015-17 (36 months); 1=January
Tota
l Nu
mb
er
of
Eve
nts
(N
)Figure 2: Number of TAD Adverse Events (N) by Month & Year
Years 2015-17 (N=36 Months)
Calendar Year Month
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 10 11 12
ALL MA
ALL (-BMC)
BMC Only
BMC Only
ALL (-BMC)
ALL MA
JAN DEC

0
2
4
6
8
10
12
14
Tota
l Eve
nts
Month
TAD Adverse Events by Month and Year (Excluding Baystate)
2015-2017ALL (-BMC)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Tota
l Eve
nts
Month
TAD Adverse Events by Month and Year (Baystate Only)2015-2017
BMC Only
TAD: A Disease for All Seasons?
Note differingpeaks and valleysin TAD occurrence depending on the
institutional “Frame of Reference” …
suggesting perhaps,Metrological, Geographical,
or possibly Meteorological
contributors to itsetiopathogenesis?

BMC Monthly Aggregated Data; ~ 68% occurring in Fall/Winter Seasons (October-March).N=19 TAD Reactions Source Data: Baystate Medical Center, Springfield,MA USA; Biovigilance Monitoring Data.

Q. So What Exactly are We Observing in Patients We Classify as Experiencing TAD ?
Back to the Beginning: Genesis of the Session

Q. So What Exactly are We Observing in Patients We Classify as Experiencing TAD ?
A. Your Guess is as Good as Mine
Back to the Beginning: Genesis of the Session

A Comparison of or for the “BIRDS” ?

Summary & Closing Comments
1. Transfusion Associated Dyspnoea (TAD) is a poorly understood adverse consequence of HT with an obscure etiopathogenesis that remains to be fully
elucidated.
2. Compared to TACO and TRALI, it is typically perceived as being milder in its clinical expression, although severe and even fatal cases may be encountered.
3. Data from various haemovigilance networks and other investigatorsare limited but provide important insights into its nature.
4. Depending on one’s frame of reference, one potential model of TAD positing the existence of certain subsets or endotypes of it can be constructed.
5. Based on such a model and data from the literature, a not infrequent TAD endotype may really be reflective of unrecognized fluid overloads, i.e., TACO.
6. Further research is needed to increase our understanding of thisunder- appreciated condition and how it interfaces with other
adverse respiratory sequelae related to transfusion.

Transfusion Associated Dyspnea (TAD):“A ROSE” by Many Other Names?
“…There are more things in heaven and earth, Horatio,
Than are dreamt of in your philosophy….”Hamlet, Act I, Scene v, William Shakespeare
Which Leads Us Back to the Foundational Concept of:
“Frames of Reference”
Keeping in Mind the Various Frames of Reference We Use,
So That in Our Continuing Explorations in
Haemovigilance Wonderland … We Don’t End Up
in Biovigilance Blunderland!
Frames of Reference: A Bottom-line Take-Home Message

State of the Research Symposium on TACO, TRALI, and TAD
Friday, October 12 | 8:30 am - 5:30 pmBoston, USA
Immediately before the 2018 AABB Annual Meeting
Sponsored by:
IHN and ISBT members will receive the AABB member rate for the Symposium.
