transcatheter options for mr - aats.org · transcatheter options for mr howard c. herrmann, md,...
TRANSCRIPT

Transcatheter Options for MR
Howard C. Herrmann, MD, FACC, MSCAI
John Bryfogle Professor of Cardiovascular Medicine and SurgeryHealth System Director for Interventional Cardiology
Director, Cardiac Cath Labs, Hospital of the Univ of PA
Perelman School of Medicine University of Pennsylvania
Philadelphia

Disclosure Statement of Financial InterestWithin the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
Discussion may include unapproved and off-label devices, procedures, and indications
Major Stock Shareholder/Equity
MicrointerventionalDevices
Consulting Fees/Honoraria
SiemensEdwards LifesciencesGlaxoSmithKlineMerck
Grant/Research Support
Abbott Vascular Edwards LifesciencesSt. Jude MedicalMedtronicGoreSiemens
Boston SciRegado BiosciCordisCardiokinetxUniv LavalMitraspan

Adapted from Herrmann and Maisano, Circulation 2014;130:1712-22
ANATOMIC TARGET DEVICE NAME MANUFACTURER STATUS
LEAFLET / CHORDAL MitraClip Abbott Vascular (IL) CE Mark, FDA approved
NeoChord NeoChord (MN) Phase 1 (OUS)
Mitra-Spacer Cardiosolutions (MA) Phase 1 (OUS)
MitraFlex TransCardiac Ther (GA) Preclinical
Middle Peak Medical Middle Peak Med (CA) Preclinical
Pascal Edwards Lifesciences Phase 1 (OUS)
INDIRECT ANNULOPLASTY Carillon XE2 Cardiac Dimensions (CA) CE Mark
ARTO system MVRx (CA) Phase 1 (OUS)
Cerclage NHLBI (MD) Phase 1 (OUS)
DIRECT/LV ANNULOPLASTY Perc Annulo System Mitralign (MA) Phase 1 (OUS)
Accucinch Ancora (CA) Phase 1 (OUS)
Boa RF QuantumCor (CA) Preclinical
Cardioband Valtech (Israel) Phase 1 (OUS)
Tasra MitraSpan (MA) Preclinical
Millipede Millipede (TX) Preclinical
HYBRID SURGICAL Adjustable Ring St Jude Med (MN) CE Mark
enCor Dynaplasty MiCardia (CA) CE Mark
Cardinal Valtech (Israel) CE Mark, Phase 1 (US)
LV REMODELING Basal annuloplasty Mardil (MN) Phase 1
Parachute CardioKinetix (CA) CE Mark, Phase III (US)
TMVR CardiAQ, Caisson Edwards, Caisson US EFS

MitraClip Catheter-Based Repair

18Investigational device limited by Federal (U.S.) law to investigational use only. PML02827 Rev. A 03/2010
0 20 40 60 80 100
EVEREST II RCT: Primary EndpointsPer Protocol Cohort
0 20 40 60
9.6%
Device Group, n=136
Control Group, n=79
57.0%
Met superiority hypothesisMet superiority hypothesis• Pre-specified margin = 6% • Observed difference = 47.4%• 97.5% LCB = 34.4%
72.4%
87.8%Control Group, n=74
Device Group, n=134
Met nonMet non--inferiority hypothesisinferiority hypothesis• Pre-specified margin = 31% • Observed difference = 15.4%• 95% UCB = 25.4%
SafetyMajor Adverse Events
30 days
EffectivenessClinical Success Rate*
12 months
LCB = lower confidence boundUCB = upper confidence bound
pSUP <0.0001 pNI =0.0012
* Freedom from the combined outcome of death, MV surgery or re-operation for MV dysfunction, MR >2+ at 12 months
55%
73%
ITT p=0.007

MitraClip vs Surgery 30 Day OutcomesSystematic Review of High Risk Pts (21 studies)
3.31.1
4.21.7 3
7
16.2
4.5
59
36.3
15
26
0
10
20
30
40
50
60
70
Death Stroke Bleeding ProlongedVent
ICU Days HospitalDays
MitraClipSurgery
Philip F et al, Cathet Cardiovasc Intervent 84:581, 2014
n=3198
n=3265


HPI • 90 yo• Progressive DOE (1/2 block, Class III-IV)• PH:
• COPD (50 pk-yr): FEV1 1.56 (111%), DLCO (50%)• PVD (AAA and carotid (>70% R))• DVD (cervical)• R diaph paralysis
• Echo: large P2 flail• STS risk for replacement = 16.5%

Images courtesy of Frank Silvestry, MD
Procedural Echo Guidance Must be Fully Integrated
• Transseptal puncture• Guide and delivery catheter insertion in LA• Alignment of the system axial to the valve plane
and over MR origin• Proper alignment of the Clip arms• Grasping of the leaflets• Release of the Clip• Steering system out of LA• Assessment of MR and leaflet insertion
Essential for:

Procedure


How are Patients with Isolated FMR Treated? Duke Databank: 1,538 pts with echocardiographic 3+ - 4+ FMR and LVEF ≥20% between 2000 and 2010 not undergoing CABG
Management:
11.4% 5.9% 8.4% 11.8% 18.4%
0%
25%
50%
75%
100%
All pts 20%-30% 30%-40% 40%-50% 50%-60%
Conservative management Isolated MV surgery
LVEFN=1538 N=440 N=298 N=313 N=479
8 other pts had LVEF >60%; none underwent MV surgery c/o Mitch Krucoff

2 Year F/U of 116 Repair PatientsJ Thoracic Cardiovasc Surg 2015;149:752
40%48%

HPI
• 74 yo
• CC: DOE, fatigue, CP (NYHA Class III)
• s/p CABG 1976• s/p re-do CABG 1991 • HTN, HL, PVD, AF, OSA, DM• VT s/p Biv ICD

Echocardiogram
Findings:
• Mod-severe MR (3+)
• VC 0.72, EROA 0.5, blunted to rev pul v flow
• 2-3 jets: largest medial to A2, smaller lateral to A2
• EF 30-35% (Inf AK, AS, AL, and apical HK)
• Normal RV, PASP 31 mmHg
• Dilated annulus with post leaflet tethering and anterior override
• Calcified aorta
• Pedicle RIMA crossing the midline

3D Echocardiogram

Procedure: Mitraclip X2

Follow up at 6 mos• No SOB limitation. Walks 1 ½ blocks to claudication• Has more energy• Class II• TTE: mild MR• Continues to do well (now at 15 mos)

EVEREST II REALISM High Risk by Etiology 25
Mitral Regurgitation SeverityEcho Core Lab Assessed
High Risk FMR(N=439)
High Risk DMR(N=189)
Paired Data (N=232) Paired Data (N=108)
N=survivors with paired data at 1 year; p-values for descriptive purposes only
4+4+
4+
4+
3+
3+
3+
3+
2+
2+
2+
2+
1+
1+ 1+
0+
0%
20%
40%
60%
80%
100%
Baseline 1 Year Baseline 1 Year
Patie
nts (
%)
83%
9%
83%
22%
p < 0.0001p < 0.0001

EVEREST II REALISM High Risk by Etiology 26
Hospitalizations for Heart Failure
0.67
0.460.56
0.120.0
0.2
0.4
0.6
0.8
1.0
1 Year Prior toMitraClip
1 Year Post-Discharge
1 Year Prior toMitraClip
1 Year Post-Discharge
HF
Hos
pita
lizat
ion
Rate
Per
Pa
tient
Yea
r
(N=189)
31% reductionp = 0.0002
(N=183)(N=439) (N=422)
79% reductionp < 0.0001
High Risk FMR(N=439)
High Risk DMR(N=189)

2710/17/2017
Edwards PASCAL Mitral Valve Repair System
Not approved for sale in any country. Edwards PASCAL is a trademark of Edwards Lifesciences.
Transseptal approach
Spacer is clasped between mitral valve leaflets
Independent leaflet clasping
Simple, intuitive delivery system

2810/17/2017
Edwards PASCAL Mitral Valve Repair System

2910/17/2017
Compassionate use of the PASCAL transcatheter mitral valve repair system for patients with severe mitral regurgitation: a multicentre, prospective, observational, first-in-man study
Fabien Praz, MD, Konstantinos Spargias, MD, Michael Chrissoheris, MD, Lutz Büllesfeld, MD, Prof Georg Nickenig, MD, Florian Deuschl, MD, Robert Schueler, MD, Neil P Fam, MD, Robert Moss, MD, Moody Makar, MD, Robert Boone, MD, Jeremy Edwards, MD, Aris Moschovitis, MD,
Saibal Kar, MD, Prof John Webb, MD, Ulrich Schäfer, MD, Prof Ted Feldman, MD, Prof Stephan Windecker, MD
The LancetVolume 390, Issue 10096, Pages 773-780 (August 2017)
DOI: 10.1016/S0140-6736(17)31600-8
3410/17/2017
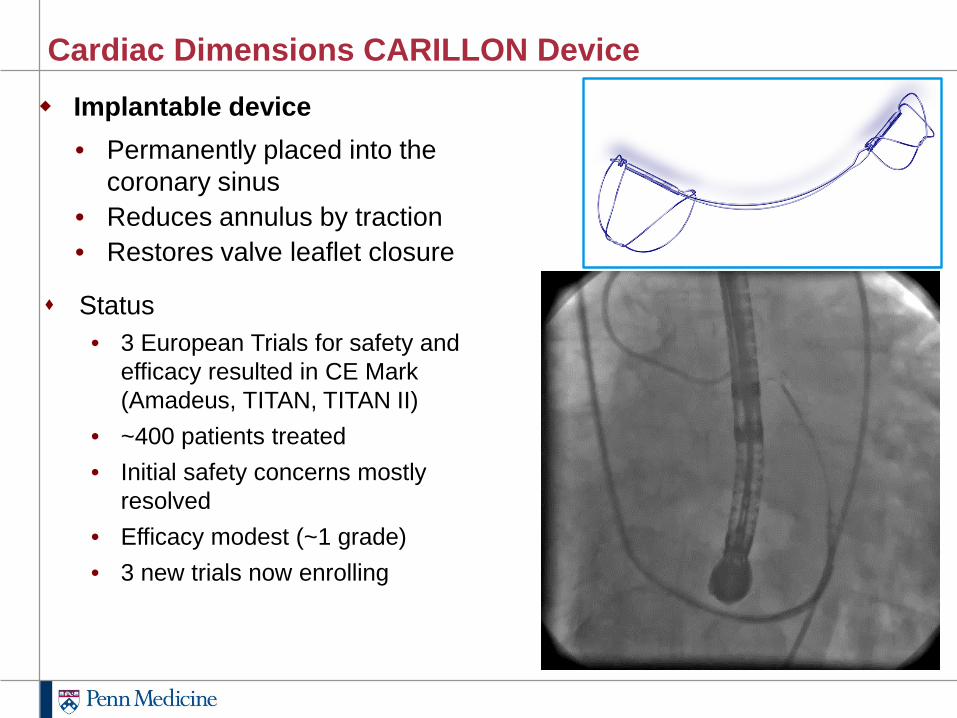
Cardiac Dimensions CARILLON Device Implantable device
• Permanently placed into the coronary sinus
• Reduces annulus by traction• Restores valve leaflet closure
Status• 3 European Trials for safety and
efficacy resulted in CE Mark (Amadeus, TITAN, TITAN II)
• ~400 patients treated• Initial safety concerns mostly
resolved• Efficacy modest (~1 grade)• 3 new trials now enrolling

3510/17/2017
New Trials with Carillon
Reduce FMR Clinch US Pivotal
PI Sievert Schofer / HaudeVan Bardeleben
Kapadia / StarlingGillinov
Sites Europe/Australia Germany (3) 50 centers (US, Canada, Europe, Australia)
Inclusion FMR FMR Symptomatic FMR, 2-4+ MR
N 120 30 400
Randomization 3:1 1:1 2:1 (blinded)
1o Efficacy Endpoint
Regurg Volume 6 min walk distance Co-10 at 12 mos:Death, HF hosp, 6MWD
andRegurg Volume
Comparator Med manage Mitraclip with built in crossover for persistent
MR/Sx
GDMT

Confidential• Implant with no cinch • Implant with partial cinch • Completed Implant
AccuCinch®
Ventriculoplasty System

Confidential 42
U.S.Clinical Sites
St. LouisBarnes HospitalJohn Lasala, MD
New York CityColumbia UniversitySusheel Kodali MD/Marty Leon, MD
Salt Lake CityIntermountain Medical Center Brian Whisenant, MD
New York CityNYU Langone Medical CenterMathew Williams, MD
HoustonSt. Luke’s / Texas Heart InstituteGuilherme Silva, MD
LincolnNebraska HeartHosakote Nagaraj, MD
SeattleUniversity of WashingtonMark Reisman, MD
MinneapolisMinn. HeartPaul Sorajja, MD
Favorable FDA interactions
CMS reimbursement for IDE
8 centers15 patients
UW Medicine
Columbia University
St. Luke’s
NYU Langone
Intermountain Medical Center
Nebraska Heart
Barnes
Minn. Heart
• IDE EFS U.S.o 8 centerso 15 patients
• Cinch 2 EFS Europeo 10 centerso 27 patients

/
Update from European trial - 61 patients results
A single arm, multi-center, prospective study with intra-subject comparisons to evaluate the performance and safety of the Cardioband for repair of functional mitral regurgitation.
Courtesy of F. Maisano, MD

/
LIVE ADJUSTMENT OF ANNULAR SIZE TO OPTIMIZE COAPTATIONB
asel
ine
Fina
l siz
e Po
st
Adju
stm
ent

/
*Dr. Paul Grayburn – Baylor University
94% MR ≤ 2+at 12 Months
92% MR ≤ 2+at 24 Months
92% MR ≤ 2+at 6 Months
92% patients with MR ≤2+ At 24 Months By Core Lab*
87% MR ≤ 2+at 30 Days
3-4+
3-4+ 3-4+ 3-4+ 3-4+ 3-4+
2+
2+ 2+ 2+ 2+ 2+
0-1+ 0-1+ 0-1+ 0-1+ 0-1+
0%
20%
40%
60%
80%
100%
BaselineN=61
DischargeN=57
30 daysN=53
6 Months N=40 12 MonthsN=31
24 MonthsN=12
46

/
Annular Reconstruction by SignificantReduction in Septo Lateral (A-P) Dimension
30% average reduction in A-P
*P<0.01
20
25
30
35
40
Baseline Discharge
A-P
Dis
men
sion
[mm
]
37±4(29-46)
26±4(18-35)
17
22
27
32
37
42
47
Baseline Discharge
Sept
o La
tera
l Dim
ensi
on [m
m]

/
Functional Improvement at 12 Months
304
376
200225250275300325350375400
41
18
0
10
20
30
40
Baseline 12 MonthsBaseline 12 MonthsN = 24 N = 28
6MWTP<0.01Δ = 72
MLHFQ ScoreP<0.01Δ = -23
Met
ers
Wal
ked
MLH
FQ S
core
IV
III
III
II
II
I
0%
20%
40%
60%
80%
100%
Baseline 24 MonthsN = 34
79% N
1YHA
I/II
% o
f pop
ulat
ion
NYHA ClassP<0.01
48
ACTIVE pivotal trial imminent in the US

Considerations for Transcatheter Therapy of 2o MR
• Most patients don’t get surgery
• Surgical repair, when successful, has better LV remodeling than replacement, but has a high recurrence rate
• Transcatheter repair therapies are limited to certain anatomies and, though safer, generally less effective than surgery
• There is a need for a less invasive therapy than surgery that can improve symptoms better than medical management

Transcatheter MV Replacement:The Rationale:• Avoid risks and discomfort of surgery (CPB and
sternotomy/thoracotomy)• Avoid slower recovery of surgery• Must balance efficacy and safety (consider age,
frailty, co-morbidities, goals of care)• Results with transcatheter repair disappointing
(and sobering compared with TAVR)
The Hope for TMVR:• Feasibility demonstrated VIV, Phase 1• Better efficacy (more consistent MR reduction)• Less dependent on anatomy (more predictable
results)
1 Maisano and Herrmann, EHJ 20152 Herrmann and Chitwood, JACC 2017

Transcatheter Mitral Therapy at Penn