training tool box - uwsp · slide 32 why it is important to be gender responsive •...
TRANSCRIPT

8/28/2017
1
Addressing the Gender-specific Service Needs of Women with
Substance Use Disorders
Training Tool Box
AcknowledgmentThis Training Tool Box was developed for the Substance Abuse and Mental Health Services Administration (SAMHSA) by Advocates for Human Potential, Inc., (AHP) under contract number 283-07-3807 with SAMHSA, U.S. Department of Health and Human Services (HHS). The contents do not necessarily reflect the views or policies of SAMHSA or HHS.
DisclaimerThe views, opinions, and content of this Training Tool Box are those of the authors and contributors and do not necessarily reflect the views, opinions, or policies of SAMHSA or HHS. The Training Tool Box provides introductory information and should not be considered clinical guidance. It is not to be considered a substitute for individualized client care or as a protocol for treatment decisions. Resources listed in this Tool Box are not all inclusive. Inclusion as a resource does not constitute an endorsement by SAMHSA or HHS.
Public Domain NoticeAll material appearing in this Training Tool Box is in the public domain and may be used without permission from SAMHSA or HHS. Citation of this source is appreciated. However, the training modules and resources may not be reproduced, presented, or distributed for a fee without the specific, written authorization of SAMHSA, HHS. 2017.
Slide 3
Learning Objectives
Participants will be able to:
• Gain an understanding of the unique needs of women in the context of substance abuse treatment and recognize the value of coordinated care
• Learn about guidelines for the use of MAT during the perinatal period
• Appreciate the role that appropriate care of women plays in the health of families and communities
Slide 5

8/28/2017
2
Telescoping and Other Sex-related Differences
Telescoping, in this use of the term, refers to an effect whereby women “progress faster than men from initial use to alcohol- and drug-related problems, even when
using a similar or lesser amount of substances.”
(Substance Abuse and Mental Health Services Administration [SAMHSA], 2009, p. 27; Piazza et al., 1989)
Slide 8
Culture and SUDs
“The complex interplay of culture and health—as well as the influence of differing attitudes toward,
definitions of, and beliefs about health and substance use among cultural groups—affects the psychosocial
development of women and their alcohol, drug, and tobacco use and abuse.”
(SAMHSA, 2009, pp. xxi–xxii)
Slide 14
Women and the Military
• Women make up approximately 15 percent of the armed forces. (Office of the Deputy Assistant Secretary of Defense, 2013)
• Women who are in the military are at risk of additional trauma, including military sexual trauma (MST). Many also experience trauma prior to joining the military.
• Substance use among women veterans is high.
• Women with military experience often have higher than average work experience and education levels.
Slide 16

8/28/2017
3
Across the Life Span
• Suzi is 15 and smoking marijuana.
• Joanne is 22 and using opioids.
• Jessica is a 40-year-old mother of three who is a poly drug user.
• Charlisa is a 70-year-old widow who is dependent on alcohol.
Each woman has different assessment, treatment, and recovery needs.
Slide 17
Substance Use: Women vs. Men
Women have lower rates of substance use and SUDs than men.
8.5
10.2
3.44.4
3.31.9
0
2
4
6
8
10
12
past year alcoholdependence
past month heavyalcohol use
past year illicitdrug dependence
or abuse
men
women
Pe
rce
nta
ge
Source: Substance Abuse and Mental Health Services Administration. (2015a). Behavioral health barometer: United States, 2015. HHS Publication No. SMA-16-Baro-2015. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Slide 18
Substance Use: Adolescents
Past Month Use of Selected Illicit Drugs and Alcohol among Youths Aged 12 to 17, by Gender and Age Group: 2012
# Difference between this estimate and the male estimateis statistically significant at the .05 level.
Source: SAMHSA. (2013c). Results from the 2012 National Survey on Drug Use and Health: Mental health findings, NSDUH Series H-47.
Slide 19

8/28/2017
4
Protective Factors for Girls/Young Women
• Feeling connected to family, cared about, and supported; high parental warmth
• Parent disapproval of substance use
• Religious/spiritual practices
• Coping skills
Slide 20
Substance Use: During Pregnancy
• 9.4% of pregnant women ages 15–44 report current alcohol use, 2.3% reported binge drinking, and .4% report heavy drinking.
• 5.4% of pregnant women in this age range reported illicit drug use.
• 15.4% of pregnant women in this age range reported past month tobacco use.
• Rates of alcohol, drug, and tobacco use are lower among pregnant women than non-pregnant women.
• Rates of alcohol, drug, and tobacco use are lower during second and third trimesters than during the first.
Slide 21Source: Substance Abuse and Mental Health Services Administration. (2014). Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings.
Opioid Epidemic
• In just one decade, deaths from prescription pain killers (opioids) rose by more than 400% among women. (CDC, 2013)
• Every 3 minutes, a woman goes to the emergency room for prescription painkiller misuse. (CDC, 2013)
• The number of drug overdose deaths has never been higher, and the majority of these deaths (more than 6 out of 10 in 2014) involved opioids. (CDC, 2015d)
• At least half of opioid deaths involve a prescription opioid. When pregnant women use opiates, the fetus can also become dependent on them. (CDC, 2016d)
Slide 22

8/28/2017
5
Common Reasons/Risks Factors for Initiation of Substance Use
• Influence of relationships
• Co-occurring disorders
• Trauma history
• Prescription medications
Slide 23
Substance Use, Trauma, and Mental Health Cycle
Slide 24
© Institute for Health and Recovery
Other Risk Factors for Substance Use and SUDs
• Easy access
• Positive effects
• Mood disorders
• Lack of positive activities
• Home atmosphere
Slide 25

8/28/2017
6
Consequences/Risks of Substance Use and SUDs
Women with SUDs may experience:
• Loss of their children
• Loss of relationships
• Increased trauma or violence, including rape, assault, or intimate partner violence
Slide 27
Consequences/Risks of Substance Use and SUDs (con.)
Women with SUDs risk:
• Health problems, including:
o SUD-related health conditionso HIV, hepatitis, and other infectionso Pregnancy complications
• Economic hardship and homelessness
Slide 28
Involvement with the Criminal Justice System
• Increasing numbers of women and girls are becoming involved with the criminal justice system.
• Many have SUDs, SUD-related arrests, and trauma histories.
Slide 29
8/28/2017
7
Barriers to Accessing Help
Top barrier
• Self (is not ready or does not feel she needs help)
Other common barriers for women:
• Cost (socioeconomic hardship)
• Feelings of shame and guilt
• Family
• Partner
• Systemic
• Practical
Slide 30
How Women Access Help
The primary sources of referral to SUD treatment for women are:
• Self-referral, often with the help or support of family
• Social service agencies, such as child protective services
• Criminal justice system
Slide 32
Why It Is Important to Be Gender Responsive
• Gender-responsive services create an environment that reflects the understanding of the reality of women’s lives and addresses women’s issues.
• Gender-responsive services help improve the effectiveness of services for women and girls.
Slide 34
8/28/2017
8
MODULE 2Gender-responsive Services for Women: Principles and Core Components
History of Women’s Services
• There is now a robust body of research on women’s substance use disorder (SUD) treatment and recovery needs.
• Knowledge of person-centered approaches and how to address the specific needs of women continues to grow and evolve.
(Grella, 2000)Slide 5
What is “Gender Responsive”?
Gender responsive is described as:
• “Creating an environment through site selection, staff selection, program development, content, and material that reflects an understanding of the realities of women’s lives and is responsive to the issues of the clients.” (Covington, 2007)
Slide 6

8/28/2017
9
Gender-responsive Principles
The knowledge, models, and strategies of gender-responsive principles are grounded in five core components:
1. Addresses women’s unique experiences
2. Is trauma informed
3. Uses relational approaches
4. Is comprehensive to address women’s multiple needs
5. Provides a healing environment
Slide 7
Component 1: Addresses Women’s Unique Experiences
• Person-centered and relevant to each woman’s experiences
• Gender-responsive and culturally responsive; respectful
• Acknowledges that treatment needs of women are different and more complex than men
• Addresses those treatment needs of women
Slide 8
Component 1: Addresses Women’s Unique Experiences 2
• Focuses on each woman’s experiences, motivation, and self-efficacy and uses strengths-based approaches
• Discovers and addresses a woman’s individual motivations for and barriers to staying in treatment and achieving recovery, such as outside caregiving responsibilities or the relationship with her partner
Slide 9

8/28/2017
10
Component 1: Addresses Women’s Unique Experiences 3
Women’s treatment needs differ from men’s, so it is helpful for programs to consider the following:
• Offering gender-specific groups
• Exploring gender-specific curricula
• Addressing women’s issues in planning and services
Slide 10
Component 2: Trauma Informed 1
• According to several studies, among women, a trauma history is significantly associated with the initiation of substance use and development of an SUD. (SAMHSA, 2009, p. 22)
Slide 11
Component 2: Trauma Informed 2
“Trauma results from an event, series of events, or set of circumstances that is experienced by an
individual as physically or emotionally harmful or life threatening and that has lasting adverse
effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being.”
(SAMHSA, TIP 57, p. 7)
Slide 12

8/28/2017
11
Component 2:Trauma Informed 3
• Trauma can affect a woman’s perceptions about the world.
• Problem behavior may be an adaptation to coping with trauma.
Slide 13
Activity 1
Grounding Exercises
Slide 14
Component 2:Trauma Informed 4
SAMHSA’s four Rs of a trauma-informed approach:
• Realizes the widespread impact of trauma and understands potential paths for recovery
• Recognizes the signs and symptoms of trauma
• Responds by fully integrating knowledge about trauma into policies, procedures, and practices
• Resists re-traumatization
Slide 15

8/28/2017
12
Component 2:Trauma Informed 5
SAMHSA’s six principles of trauma-informed care:
1. Safety
2. Trustworthiness and transparency
3. Peer support and mutual self-help
4. Collaboration and mutuality
5. Empowerment, voice, and choice
6. Cultural, historical, and gender issues
Slide 16
1
2
3
4
5
6
Component 3: Relational – Overall
• Many women are relational and tend to prioritize relationships as a means of growth and development.
• Relational model = focus on connections
• Women recover in connection, not isolation. Relationships play a significant role in both the development and recovery from SUDs.
• Relationships or connections are central in women’s lives as:
– Part of their identities– Sources of self-esteem– The context for decision-making and choices– Support for day-to-day living and growth
Slide 18
Component 3: Relational – Connections
Connection vs. Disconnection
Slide 19

8/28/2017
13
Component 3: Relational –Therapeutic Alliance
• “A strong therapeutic relationship with a counselor is one of the largest factors in an individual’s ability to recover from the overwhelming effects of trauma.” (TIP 57, p. 176)
• It has been suggested that women may value relationships differently than men.
– Women: Trust and warmth is of primary importance.– Men: Relationships that help them solve problems
are of primary importance.
Slide 21
Component 3: Relational – Peers
• Peers are important for:
– Establishing safety and hope
– Building trust
– Enhancing collaboration
– Sharing stories (experience, strength, and hope)
Slide 23
Component 3: Relational – Family/Partners
Relational approaches to service:
• Are sensitive to the relationship/family history women bring into treatment—both positive and negative.
• Take a family-focused perspective using a broad definition of family and encouraging a woman to define her family/support system.
• Are welcoming to children.
• Help a woman understand roles and dynamics, including examining her partner’s influence on her substance use.
Slide 24

8/28/2017
14
Component 4: Comprehensive – Overall
• A comprehensive approach treats the whole woman and her comprehensive needs, including the following:
– Physical and mental health
– Overall wellness
– Survival needs
– Child and family
– Employment/education
– Criminal justice requirements
– Recovery supports
Slide 26
Component 4: Comprehensive – Mental Health
• Women are more likely than men to have co-occurring mental and substance use disorders. (SAMHSA, 2005a)
• Women are more likely than men to have multiple comorbidity, which is three or more psychiatric diagnoses in addition to an SUD. (Zilberman et al., 2003)
• Effective services include comprehensive assessment and either onsite integrated care or established relationships for referral to mental health services.
Slide 27
Component 4: Comprehensive – Physical Health
• Women with SUDs are at an increased risk of many health-related consequences.
• Women with SUDs often do not receive routine exams or needed health services.
• Comprehensive services include physical health assessments and onsite, or referral to, primary health care to address health issues.
Slide 28

8/28/2017
15
Component 4: Comprehensive – Family
• Women often have care-taking responsibilities for children, siblings, or elders.
• Children and family members may need services.
• Women often need parenting education, family strengthening, relationship counseling, and other family resources.
Slide 29
Component 5: Healing Environment
• Provide services in a safe and comfortable environment
• Offer women-only groups and activities
• Be open to feedback from participants
• Offer staff training and development
Slide 30
Addressing Gender Dynamics in Treatment Settings
• Women benefit from:
– Support and activities that develop their voices and self-identities
– Having opportunities to share their stories
• Gender-responsive treatment acknowledges potential subconscious and unintended biases that lead both men and women to defer to men.
Slide 32

8/28/2017
16
Summary
• Following gender-responsive principles and creating treatment environments that are both gender responsive and trauma informed will improve the experience of women with SUDs and lead to more effective services and recovery.
• Providing staff members with ongoing gender-specific and trauma-informed training and supervision will help ensure they all understand and can implement the core competencies noted in this module.
Slide 34
MODULE 5
Pregnant and Parenting Women
Activity 1
How do you feel when you see a pregnant woman drinking or smoking?
Slide 48
8/28/2017
17
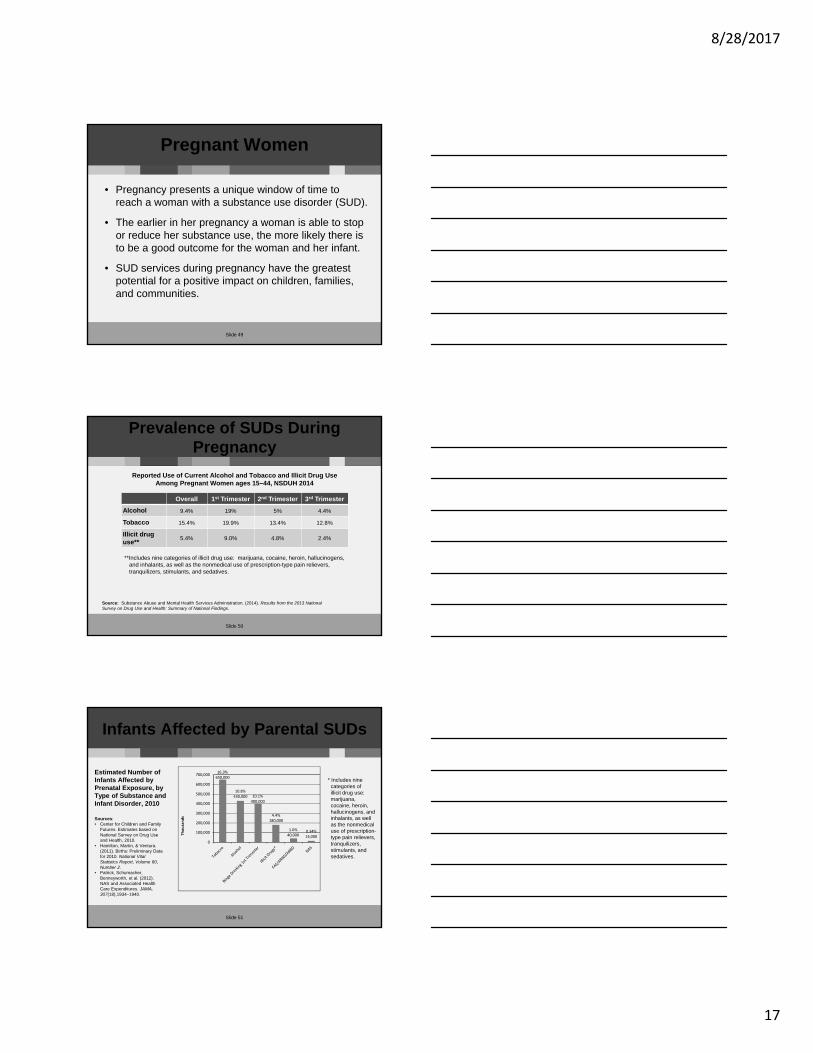
Pregnant Women
• Pregnancy presents a unique window of time to reach a woman with a substance use disorder (SUD).
• The earlier in her pregnancy a woman is able to stop or reduce her substance use, the more likely there is to be a good outcome for the woman and her infant.
• SUD services during pregnancy have the greatest potential for a positive impact on children, families, and communities.
Slide 49
Prevalence of SUDs During Pregnancy
Reported Use of Current Alcohol and Tobacco and Illicit Drug Use Among Pregnant Women ages 15–44, NSDUH 2014
**Includes nine categories of illicit drug use: marijuana, cocaine, heroin, hallucinogens, and inhalants, as well as the nonmedical use of prescription-type pain relievers,tranquilizers, stimulants, and sedatives.
Overall 1st Trimester 2nd Trimester 3rd Trimester
Alcohol 9.4% 19% 5% 4.4%
Tobacco 15.4% 19.9% 13.4% 12.8%
Illicit drug use**
5.4% 9.0% 4.8% 2.4%
Source: Substance Abuse and Mental Health Services Administration. (2014). Results from the 2013 NationalSurvey on Drug Use and Health: Summary of National Findings.
Slide 50
Infants Affected by Parental SUDs
Estimated Number of Infants Affected by Prenatal Exposure, by Type of Substance and Infant Disorder, 2010
16.3%650,000
10.8%430,000 10.1%
400,000
4.4%180,000
1.0%40,000
0.34%14,000
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
Thousands
* Includes nine categories of illicit drug use: marijuana,cocaine, heroin, hallucinogens, and inhalants, as wellas the nonmedical use of prescription-type pain relievers, tranquilizers, stimulants, and sedatives.
Sources: • Center for Children and Family
Futures. Estimates based on National Survey on Drug Use and Health, 2010.
• Hamilton, Martin, & Ventura. (2011). Births: Preliminary Data for 2010. National Vital Statistics Report, Volume 60, Number 2.
• Patrick, Schumacher, Benneyworth, et al. (2012). NAS and Associated Health Care Expenditures. JAMA,307(18),1934–1940.
Slide 51

8/28/2017
18
Importance of Outreach
• Pregnant women with SUDs benefit from early identification of pregnancy and an informed team response.
• Pregnant women with SUDs have better outcomes when they:
– Obtain SUD services
– Receive prenatal care
• Prioritize outreach to pregnant women to prevent prenatal substance exposure.
• Provide information about Screening, Brief Intervention, and Referral to Treatment (SBIRT) to local health providers.
Slide 52
Priority for Services
• Pregnant women with SUDs have priority admission status for SUD services in block-grant funded programs.
• Pregnant women need timely access to prenatal care, eitherby the program or by referral to the appropriate healthcare providers.
Slide 53
Risks of Substance Use to Pregnant Women and Their Babies
• Substance use during pregnancy can result in health concerns and risks for the woman and unborn fetus.
• Risks include miscarriage, low birth weight, FASD, and NAS.
• Some complications are drug oralcohol specific.
• Others risks are linked to a substance use lifestyle, social environmental risk factors, or poverty.
Slide 54

8/28/2017
19
Risks of Tobacco/Smoking
• Smoking during pregnancy can disrupt fetal development. (The American College of Obstetricians and Gynecologists [ACOG], 2013)
• Cognitive, emotional, and behavioral problems in children are associated with a woman’s smoking during pregnancy. (SAMHSA, 2011d)
• Children of mothers who smoked during pregnancy are more likely to have asthma, colic, and childhood obesity. (ACOG, 2013)
• The effectiveness of nicotine replacement therapy (NRT) in pregnant women is inconclusive. (ACOG, 2013)
Slide 55
FASD
• Fetal alcohol spectrum disorder (FASD) is a term describing the range of effects caused by neonatal exposure to alcohol.
• FASD is an umbrella term referring to conditions such as:– Prenatal alcohol exposure (PAE)
– Fetal alcohol syndrome (FAS)
– Partial FAS (pFAS)
– Alcohol-related neurodevelopmental disorder (ARND)
– Alcohol-related birth defects (ARBDs)
– Neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE)
Slide 56
FASD Statistics
• Prenatal exposure to alcohol is one of the leading causes of developmental disabilities and birth defects in children.
• Up to 1 in 20 U.S. school children may have a FASD. (CDC, 2016a)
• Data estimates are that 2–5% of children in the United States have a FASD. (CDC, 201ba; May et al., 2014)
• It is estimated that almost 70% of the children in foster care are affected by prenatal alcohol exposure in varying degrees (NOFAS, 2016). Among those, 1–1.5% have FAS. (Williams et al., 2015)
Slide 57

8/28/2017
20
Long-term Effects of FASD
• Of all commonly used substances, alcohol produces the most serious lasting neurobehavioral effects in the fetus.
• Children exposed to alcohol in the womb can have a range of serious life-long issues, including delayed developmental outcomes.
• Lifetime costs for one individual with FASD are estimated to be up to $244 million. (CDC, 2015b; Williams & Smith, 2015)
Slide 58
NAS/NOW
• Neonatal abstinence syndrome (NAS) is a postnatal drug withdrawal syndrome, mainly caused by maternal opioid use. It most is most often evident between 24–48 hours after birth.
• The term neonatal opioid withdrawal (NOW) is also commonly used.
• NAS is treatable. Medication-assisted treatment (MAT) is most often recommended for pregnant women rather than withdrawal or abstinence, which can result in premature labor, fetal distress, or miscarriage. (SAMHSA, in press)
• Treatment for NAS/NOW may be pharmacological or non-pharmacological.
Slide 59
Clinical Features/Outcomes of NAS/NOW
• NAS/NOW has a variety of possible symptoms, which typically develop in the first few days of birth.
• Infants with NAS/NOW have an average hospital stay of 17 days overall; 23 days when treatment is needed.
• Long-term adverse outcomes are possible.
• Early intervention is recommended for children with NAS/NOW.
Slide 60

8/28/2017
21
Screening and Support for Pregnant Women
It is recommended that SUD centers:
• Conduct a comprehensive screening to determine the stage of pregnancy and alcohol or drug use.
• Link women with the appropriate medical services and other supports.
• Ask a pregnant woman about, and listen to, her fears.
• Explore options to access treatment and recovery, including medication-assisted treatment and recovery (MATR).
• Screen for intimate partner violence.
Slide 61
CAPTA
• The Child Abuse Prevention and Treatment Act (CAPTA) is key federal legislation on child abuse and neglect.
• The Comprehensive Addiction and Recovery Act of 2016 (CARA) amended CAPTA.
• CAPTA requires health providers and child welfare to respond when infants are born affected by caregiver substance use or with prenatal exposure, including the development of an infant safe care plan.
Slide 62
Anxiety and Fear about Seeking Treatment
• Pregnant women with SUDs often feel anxiety and fear that if they admit to having a substance use problem, they will lose their children.
• Pregnant women may also have anxiety that their infant will be born healthy and that they will be able to be good parents or anxiety regarding changes in the family or economics.
Slide 63

8/28/2017
22
Engagement in Services
• Women with SUDs have a range of feelings related to pregnancy:• Love• Ambivalence• Guilt and shame• Fear of losing their child• Hope for the future
• Pregnant women need supportive relationships to address SUD problems, access other supports, and prepare for pregnancy.
• Engagement can occur in a lot of settings and through many different relationships.
Slide 64
Medication-assisted Treatment (MAT) for Pregnant Women
• Pregnant women using opioids are usually advised to enter medication-assisted treatment (MAT) and recovery (MATR).
• MAT prevents the onset of withdrawal, reduces or eliminates drug cravings, and blocks the euphoric effects of opioids.
• Babies born to mothers on methadone maintenance or buprenorphine may still experience NAS, but their health is comparable to the general population and much better than those who continue to be exposed to illicit substances.
Slide 65
MAT (con.)
• Comprehensive MAT services include more than just the administration of methadone or buprenorphine.
• Both SAMHSA and the American College of Obstetricians and Gynecologists have issued guidelines around MAT for women.
Slide 66

8/28/2017
23
Complications for Women Taking Psychotropic Medications
• Prescription medications for CODs may have an effect on the pregnant woman, her fetus, and breastfeeding infants. (Armstrong, 2008)
• There may be potential complications related to prescription changes or discontinuing medications.
• Treatment providers should work closely with prescribers of psychotropic medications to ensure women have the most current information about the relative benefits/risks of continuing these medications.
• Ongoing mental health consultations are advised.
Slide 67
Treatment/Recovery Planning with Pregnant Women
• Pregnancy affects all aspects of a woman’s life. • Considerations include the following:
– Health and nutrition needs– HIV testing and early intervention/prevention– Mental health screening including pregnancy-related
mood and anxiety disorders. Feelings and options regarding pregnancy
– Possible grief and loss counseling– Preparation for parenting (or alternatives)– Concerns with other children/family and fathers– Possible work with child welfare
– Economic needs
Slide 68
Delivery
• Staff can help women prepare for birth and know what to expect.
• She may need support to address discrimination and judgements and to alleviate her fears about the well-being of her infant.
• Advance planning allows the medical facility and personnel to prepare for her delivery, which will likely be deemed a high-risk birth.
• Most women recovering from SUDs who are abstaining from alcohol and illicit drugs are able to breastfeed, including those using MATR.
Slide 69

8/28/2017
24
Postpartum Depression
• Women should be screened for maternal and postpartum emotions and disorders, such as anxiety, depression, and psychosis.
• Take appropriate action when needed.
• Plan for long-term engagement in treatment and recovery supports.
Slide 70
PART 2
Family-centered Approaches
Intergenerational Cycle of Substance Use
• Substance use disorders affect the entire family unit and all individual members.
• Parental substance use increases the likelihood that a family will experience: – Financial problems – Shifting of adult roles onto children – Child abuse and neglect; inconsistent parenting– Violence and disrupted environments
• Children of parents with SUDs have a significantly higher likelihood of developing substance use problems themselves.
Slide 72

8/28/2017
25
Werner, D., Young, N. K., Dennis, K, & Amatetti, S. (2007). Family-centered treatment for women with substance use disorders—history, key elements, and challenges. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration.
Continuum of Family Services
Slide 73
Comprehensive Model for Women and Children
Center for Substance Abuse Treatment. (2009). Substance abuse treatment: Addressing the specific needs of women. Treatment Improvement Protocol (TIP) Series, No. 51. HHS Publication No. (SMA) 15-4426. Rockville, MD: Center for Substance Abuse Treatment. p. 284 Slide 74
Attachment
• The level of early childhood attachment is a significant predictor of developmental delays, emotional disturbance, and mental health conditions and incarceration.
• Providing women with education about infant and child development may help them understand the important role of attachment.
• Encourage time holding, touching, feeding, and talking with their babies.
• Include other children in welcoming the infant to the family.
Slide 75

8/28/2017
26
Parenting Skills
• Building satisfying relationships with her infants and children can increase a woman’s motivation to abstain from substance use.
• Improving parenting helps child development and resilience.
• Women who are pregnant shouldbe connected with available community resources for parents.
Slide 76
Family-centered Recovery Supports
• Recovery supports can consider whole family needs:– Health– Home– Purpose– Community
• Women often have to prioritize family needs.
• Family-focused recreational activities help with healthy relationships and parenting.
Slide 77
Family Responsibilities
• Life skills training and supports, including:
– Addressing daily life with children, such as establishing regular meal and sleep schedules
– Establishing and maintaining parent and child roles and responsibilities
• Case management and family counseling may be needed to help women address their family’s economic needs
• Peers with similar lived experience may share effective strategies for meeting family needs
Slide 78
8/28/2017
27
Working with Child Welfare
• Many parenting women who enter treatment are involved with the child welfare agency and family/dependency court to decide whether their children may safely remain in their care.
• Communication with these agencies is vital.
Slide 79
Addressing the Needs of Children
• Children of mothers with active SUDs have often experienced instability in relationship to their mothers.
• Children sometimes communicate their fears and trauma through behaviors that can be difficult to handle.
Slide 80
Children’s Educational Needs
• Women may need support to navigate the primary education system.
• Women should know the educational rights of their children, or at least know how to obtain advocates and assistance with navigating the public school system.
Slide 81

8/28/2017
28
Identifying Family and Family Support
• Family is important for all women, not just parenting women.
• Family support and education assist women with reaching and maintaining gains made in treatment and recovery.
• Women may need support in communicating with family members who may be estranged and who they want to reconnect and rebuild relationships.
• Some family members are not supportive of a woman’s recovery.
Slide 82
Activity 6
How families can influence treatment and recovery:
• Some women with SUDs abandon familial connections with people close to them who do not use substances or who disapprove of their drug and alcohol use. Other women maintain relationships with partners and family members that revolve around drinking and using.
• Fostering the connections with people that support recovery and taking steps to limit the threat that unsafe relationships pose in early recovery is a fundamental task recovering women must undertake. Staff can help women evaluate, cultivate, and manage the positive and negative influences that family and significant relationships assert on the recovery process.
Slide 83
Intimate Partner Violence
• Programs can assess the risk of intimate partner violence (IPV), discuss risks and safety with women, and help with safety planning.
• Women with histories of trauma need support to avoid re-traumatization and develop healthy coping skills.
• Training is available to teach women how to specifically handle situations with, or with risk of, IPV.
Slide 84

8/28/2017
29
Family Counseling and Therapy
Slide 85
• Family participation and family connections are important for women.
• Substance use and related behaviors often lead to disconnectedness, a lack of trust, and unhealthy relationship dynamics.
• Family counseling and family groups are often an important element of SUD services.
Conclusion
• Pregnancy is a time of great potential for change and growth that can be capitalized on to assist a woman with entering recovery.
• Family-centered services help women, their children, and families toward health and wellness.
Slide 86