toxicokinetics 2 crispin pierce, ph.d. university of washington [email protected] (206)...
TRANSCRIPT


Exposure to Exogenous Substances
Food Drugs Toxicants
ABSORPTION THROUGH THE GI TRACT, LUNGS, SKIN AND
VENOUS CIRCULATION
DISTRIBUTION WITHIN THE BODY
METABOLISM
ELIMINATION
PHYSIOLOGIC EFFECT AT A TARGET SITE STORAGE
SECRETION OF ENDOGENOUS SUBSTANCES
Pharmaco- and Toxicodynamics
Pharmaco- and Toxicokinetics
Purposes of Toxicokinetics
To quantify toxicant absorption, distribution, metabolism, and excretion (ADME).
To provide an exposure framework for risk assessment.

The Value of Modeling
Understand biologic systemsDrive data collectionInterpolateExtrapolatePredictReduce animal usage
?
Models are an abstraction of reality. To establish dose-risk relationships, we can choose anything between a completely theoretical model, and massive testing of humans to toxic chemicals. What are the hallmarks of a model/testing paradigm that you would mandate?

Four Modeling Approaches
Hand-Waving
Non-Compartmental
Compartmental
Physiologic

Hand Waving
The same dose/kg gives the same blood concentration.
Use a 10-fold safety factor for test animal-human differences.
Use a 10-fold safety factor for interindividual differences.
Use a 1-10-fold modifying factor for additional uncertainties.

?
For what kinds of substances, exposures, and test costs would the hand-waving approach be appropriate?

Non-Compartmental ModelsEmpiric
observation of volume, clearance, and half-life.
No structural model of where the toxicant goes.
AUCTime
Blood (or
plasma)
Concentration
CL = F·Dose/AUC
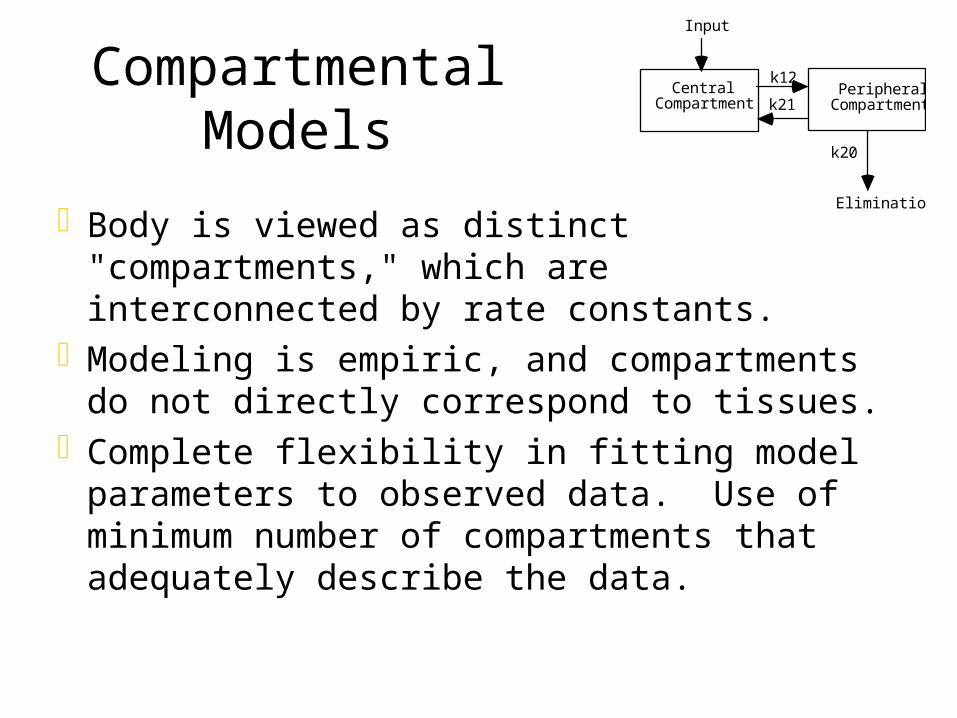
Compartmental Models
Body is viewed as distinct "compartments," which are interconnected by rate constants.
Modeling is empiric, and compartments do not directly correspond to tissues.
Complete flexibility in fitting model parameters to observed data. Use of minimum number of compartments that adequately describe the data.
Central Compartment
Peripheral Compartment
Input
k12
k21
k20
Elimination

One Compartment Model
One compartment model: xenobiotic distributes into a single, homogenous "vessel" (example: methanol).
Central Compartment
Input
k10
Elimination
(blood or plasma)
Time
ln Conc
Non-i.v. dose
i.v. doseCo
slope = -k
C C0e kt
?
How would you define an adequate fit of your model to the data?

Two Compartment Model
Two compartment model: xenobiotic distributes into a central, and then a peripheral compartment.
Central Compartment
Peripheral Compartment
Input
k12
k21
k10
Elimination
Central Compartment
Peripheral Compartment
Input
k12
k21
k20
Elimination

Rate of change of toxicant in central compartment = ka*Amount at absorption site - k12*Amount in Central Compartment + k21*Amount in Peripheral Compartment - k10*Amount in Central Compartment
Central Compartment
Peripheral Compartment
Input
k12
k21
k10
Elimination
ka

Time
ln Conc
Non-i.v. dose
i.v. dose
or
A
B
slope = -
slope = -
C Ae t Be t

t1/2, = ln2/, t1/2, = ln2/AUC = A/ + B/t1/2,, t1/2,, , and are constant with
dose.A and B vary with dose.
Time
ln Conc
i.v. doseA
B
slope = -
slope = -

?
How would you test whether the kinetics of a chemical is better described by one or two compartments?

Physiologically-Based Kinetic (PBK) Modeling
An attempt to simulate toxicant disposition in the body by using measured values: Tissue volumes and blood flows Toxicant-specific tissue partition
coefficients and elimination rates

Body is viewed as grouped tissue compartments which are interconnected by blood flows.
Modeling is mechanistic, and compartments are defined by physiologic volumes and partition coefficients.
Model parameters are fit within physiologic bounds to observed data. Use of minimum number of compartments that adequately describe the data.

Lung Blood
Q tCven
Q t = CO
Cart
Cva
Q a = .09*CO
Cvr
Qr=.49*CO
Cvs
Qs=.15*CO
Cvl
Ql=.25*CO
Rapidly Perfused Tissues
Slowly Perfused Tissues
Adipose Tissues
IV, dermal
dose
Oral DoseLiver
Inhalation dose

Flow-Limited DeliveryFlow-limited delivery of xenobiotics to
tissue groups:
Vt
Qt QtKp
Venous blood Arterial blood
dA t
dt= Qt Ca -
Qt A t
Kp V t
where: At = Amount in tissue, Qt = Blood flow to tissue, Ca = Arterial blood concentration, Kp = Tissue/blood partition coefficient, Vt = Tissue volume

Michaelis-Menten Metabolism
Vt
Qt Qt
Km Vmax
Kp
Venous blood Arterial blood
Metabolite Formation
dA t
dt= Qt Ca -
Qt A t
Kp V t
-Vmax A t
(KmV t +At )Kp
Vmax = Maximum metabolic rate, Km = Michaelis constant (toxicant concentration at half-maximum metabolic rate)

?
Which kind of model would you use to study identical dosing in a very homogeneous group (e.g., vaccinations in two year-olds)?
Which kind of model would you use to study varied dosing in a heterogeneous group (e.g., genetically modified food in the general population)?

Uses of the PBK Model
Use across a wide range of doses - low to saturating.
Interspecies scaling, in particular with regards to risk.
Determination of target tissue dose.Simulating complex risk assessment conditions.Searching for relevant interindividual differences.
Toxicant-Specific Considerations
Molecular weight, conformation, charge >>> Flow- or diffusion-limited delivery and filtration by kidney.
Vapor pressure over blood >>> Elimination by exhalation.
Molecular weight, conformation, charge (lipophilicity) >>> Tissue distribution and accumulation.

Human Physiologic Considerations
Genetic polymorphism >>> Metabolic ratesSex and age differences >>> Blood flows and
metabolic ratesWeight >>> Blood flows and tissue volumesBody fat percentage >>> Adipose tissue volumeWorking conditions >>> Alveolar ventilation rate,
cardiac output, blood flowsRoute of administration >>> First-pass effects
?
Which PBK model parameters are likely known with greatest certainty? Which with least certainty? Which would you allow to vary within physiologic bounds to describe the data?
Might the PBK model be used to question the accuracy of data between studies?
