towards malaria elimination in indonesia · - mass blood survey - malaria treatment and bednet...
TRANSCRIPT

Towards Malaria Elimination in Indonesia
Executive Board Meeting, ACT MALARIA
Dr. Rita Kusriastuti, M.ScDirector of VBDC, DG DC&EH, MOH INDONESIA
VIENTIENE, 16 – 18th March 2009
Indonesia : COUNTRY IN BRIEF
Jakarta
• 220 million people• 1.9 million square km• 33 provinces• 471 districts• 17,000 islands (transportation includes flight, road, boat)• cultural diversity• since 2003 shifting to decentralized system
7 hours flight
#
#
#
# #
# ##
#
#
##
#
#
# #
# ###
#
#
####
###
## ## ##### #
#
#
#
#
##
##
#
#
#
#
##
#
#
# ##
##
#
#
#
#
#
##
#
#
#
#
#
#
##
# #
#
#
##
##
#
#
##
#
##
### # ##
#
#
##
#
##
##
#
#
# ##
##
#
#
#
## ##
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
##
#
#
#
##
#
### ##
#
#####
##
#
#
## #
#
#
##
##
## ##
#
#
###
###################### ######
#######
#####################
##
#
#
#
#
#
##
# ##
###
# # ##
### ##
##
##
# ##
###
#####
# ####
####
#######
# ###
## ###
###
#
##
#
# #
## # ##
####
# ###
# ## # ##
######
####
#####
# #####
##########
####
#
#
S
N
EW
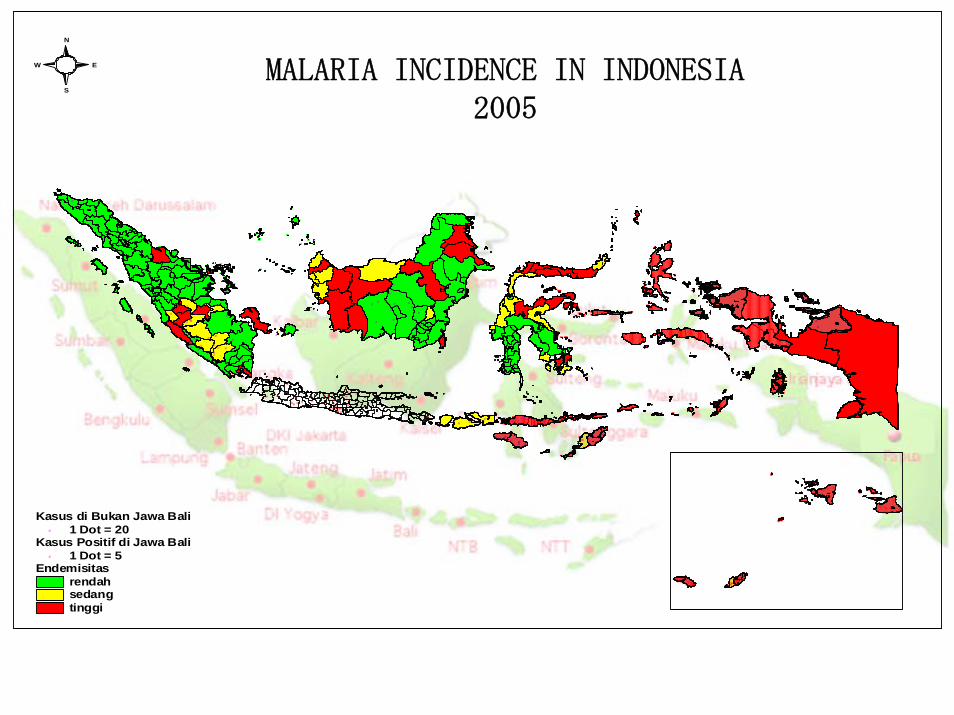
Endemisitas rendahsedangtinggi
Kasus Positif di Jawa Bali# 1 Dot = 5
Kasus di Bukan Jawa Bali# 1 Dot = 20
MALARIA INCIDENCE IN INDONESIA2005
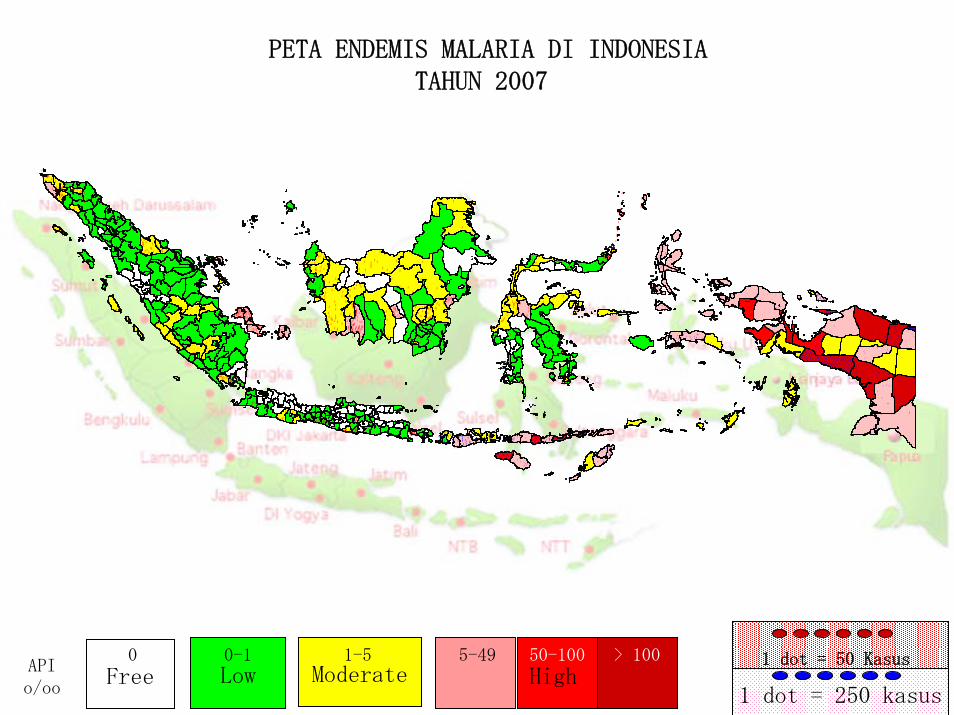
PETA ENDEMIS MALARIA DI INDONESIATAHUN 2007
#
#
##
#
##
##
#
#
##
#
#
#
#
## #
## #
##
##
#
#
#
#
##
#
##
#
#
#
#
#
#
##
##
#
#
#
#
###
###
## ##
##
##
# #
#
##
## ## #
#
#
#
#
#
#
#
#
#
#
#
#
# #
## #
#
##
#
##
#
#
#
#
#
#
#
#
#
## #
#
##
#
#
#
##
#
# # ## #
#
# #
#
#
#
#
#
#
#
#
#
#
#
# #
#
#
# #
#
#
##
##
#
##
#
##
#
#
#
#
#
#
##
# ## ##
### # ####
# #
##
## # ### ### # ##
### #
##
# ## # #
### ## #
##
#
####
## # #
# ## ## #
##
# ##
##
# ## ## # ##
##
## ##
##
# ####
#
#
##
#
##
# #
##
#
##
#
#
#
#
###
#
# #
##
#
#
#
#
#
##
#
#
#
#
#
#
#
# #
#
##
#
### #
##
#
##
#
# #
#
##
#
#
#
###
##
##
##
##
#
#
# #
##
#
#
##
#
#
#
##
##
#
#
#
## # #
#
#
##
#
#
#
#
##
##
##
#
## ##
##
#
# ##
#
#
#
#
##
##
#
#
#
#
#
#
###
##
##
#
##
##
#
# ###
#
#
#
##
##
#
## #
#
##
#
#
#
#
#
#
##
#
## #
#
## #
###
# #
#
#
##
### ##
#
#
##
#
##
#
#
#
#
#
#
#
###
#
##
# ##
#
#
##
#
#
#
##
#
#
#
#
#
#
## #
# #
#
#
#
#
#
#
#
#
##
#
##
##
##
#
#
#
#
#
#
##
##
## #
#
#
##
#
#
#
#
##
#
#
#
##
##
#
#
#
#
#
##
#
# #
#
#
#
#
#
#
#
#
# # ##
## # ## ##
####
##
##
#
#
#
#
#
##
#
##
#
#
##
##
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
###
# #
# #
##
##
#
#
#
##
#
##
#
#
#
#
#
#
##
#
#
#
#
##
#
#
#
#
#
#
##
#
#
#
##
#
#
#
#
# #
#
#
###
## #####
###
## #
##
## ## #
#
##
#
#
# # ## #
# #
#
#
#
#
##
# # #
#
###
#
##
#
## #
#
#
##
#
#
## #
##
#
##
#
#
#
#
#
#
# #
#
#
#
##
#
#
#
##
##
#
#
#
#
#
#
#
#
#
#
#
#
##
##
#
#
### ##
#
# #
#
# ##
#
#
#
###
#
# ##
###
#
#
#
#
#
#
#
####
## #
## ##
##
## #
#
#
##
##
##
##
#
#
#
## #
##
### #
##
##
### #
#
##
#
##
# #
##
##
##
# ###
## # #
#
##
#
##
# # #
#
##
#
### ###
#
##
#
##
# ###
# #
#
###
#
## ##
# ##
# # ###
##
##
## ## ##
####
#
### ###
# ####
##
# #
# ## # ##
##
#### #
# #
#
##
## #
#
##
##
#
##
#
#
#
##
#
#
### #
# # ##
#
#
# ##
##
# #
#
#
###
#
#
#
## #
###
#
#
#
#
##
#
##
#
#
#
### #
###
##
# ##### #####
##
##
### ##
##
######
##### ## ## ##
# ## ###
## ###
#
#
#
##
#
## #
##
# ##
######
#
#
#
#
#
#
# #
#
#
##
##
#
# #
##
###
###
#
#
#
# ##
#
#
##
#
#
##
##
##
#
#
#
####
#
#
##
#####
##
#
###
####
#
#
#
##
#
##
##
#
#
## #
#
##
#
# #
## ##
##
#
#
# ##
#
###
###
#
##
##
#
##
#
#
#
#
#
##
# #
#
#
# ##
## ###
#
### #
### #
##
##
####
#
#
#
#
## # #
#
##
#
###
##
#
#
#
# #
#
##
#
#
#
# #
#
## #
#
#
##
#
#
##
#
#
#
#
#
#
#
# #
#
#
#
##
#
#
#
#
##
# #####
## ##
## ##
#
##
#
# ## ##
###
#
#
#
#
#
#
#
##
#
##
#
#
#
#
#
##
# ##
##
###
####
#
#
# ###
##
##
###
## #
##
##
# #
####
##
#
#
#
#
#
# ## ## ##
## ##
#
##
#
#
##
###
##
#
##
##
#
###
# #
##
#
#
##
##
#
##
#
#
#
#
#
#
#
#
##
#
#
#
#
##
#
#
###
###
#
## #
#
##
#
###
#
#
#
# ##
#
##
### # #
####### ######### ## ##### ##
### ###
### #
###
###
### #
# #
###
## #
###
#
##
# ### ## ##
##
###
##
#
# ## ## #####
#### #### #######
#
## ### ##
#####
##
#### ###
##
#
# #######
## #
##
###
## ##
##
#### #
##
#
#####
###
#### #
#
####
#
##
# ##
#### # #
####
### ## #
#
##
#
##
#
## ##
# ##
#
###
#
## #
#
###
### #
##
###
#
#
###
# #
#
#
#
#
##
##
###
#
# #
###
#
##
##
##
##
#
#
## ##
#
#
#
##
#
#
#
#
#
#
# #### ##
#
#
#
##
### ##
##
#
#
#
#
##
#
#
#
###
#
#
#
#
##
#
#
##
#
#
#
##
#
#
# #
#
##
# #
#
# ##
#
##
#
#
# #
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
## #
#
#
#
#
#
#
#
##
##
#
#
###
#
#
#
#
#
#
## ##
#
# #
#
#
#
##
##
#
#
#
###
#
##
#
#
#
#
# #
#
#
##
##
#
#
#
#
###
##
##
#
#
####
#
##
##
#
#
#
##
##
#
#
##
# ###
##
#
###
#
### ##### #
#
### #
#
##
##
#
# #
#
#
## #
#
#
#
##
#
#
###
##
###
# #
## #
####
#
##
##
#
## ###
## #
#
#
##
# #
#
#
#
##
#
##
## #
###
#
##
#
#
#
##
###
###
#
# ##
## ##
#
##
# #
## #
## ##
#
####
## #
###
###
# ### #
##
#
#
#
#
#
####
##
# # ##
## #
#
##
##
##
#
# ## ##
#
##
#
###
## #
###
# ##
###
#
#
#
##
##
#
## #
# ## ## ## ### ####
# # ## # ## ## #### # ## ## ## ##
##
# ### ## ## ## ## ### ##### ###
##
####
##
##
# #### ####
###
#
#
#
# #
#
#
#
#
#
#
#
#
#
#
#
#
#
##
##
# #
#
#
#
####
#
##
#
#
#
#
##
## #
#
#
##
#
#
##
#
#
#
## #### ## ##### # #
## ###
#
#
#
#
#
#
#
#
#
#
#
##
#
##
#
#
#
#
#
##
#
#
#
#
#
###
#
#
#
#
#
#
###
# #####
###
# #
### ###
##
##
# #
##
## #
##
#
#
#
#
####
## #
#
## #
##
#
# ##
##
# ##
##
### #
#### ###
##
#
### #
#####
###
#
# ##
###
# ##
##
#
#
##
####
#
### #
## #
##
#
# #
##
# #
#
# #
## ##
#
#
#
##
##
###
##
###
##
#
#
#
##
#
# ###
##
### ##
##
###
### #
#
## #
##
#
#
Low ModerateFree1 dot = 50 Kasus
1 dot = 250 kasusHigh
0 0-1 1-5 5-49 50-100 > 100API o/oo
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
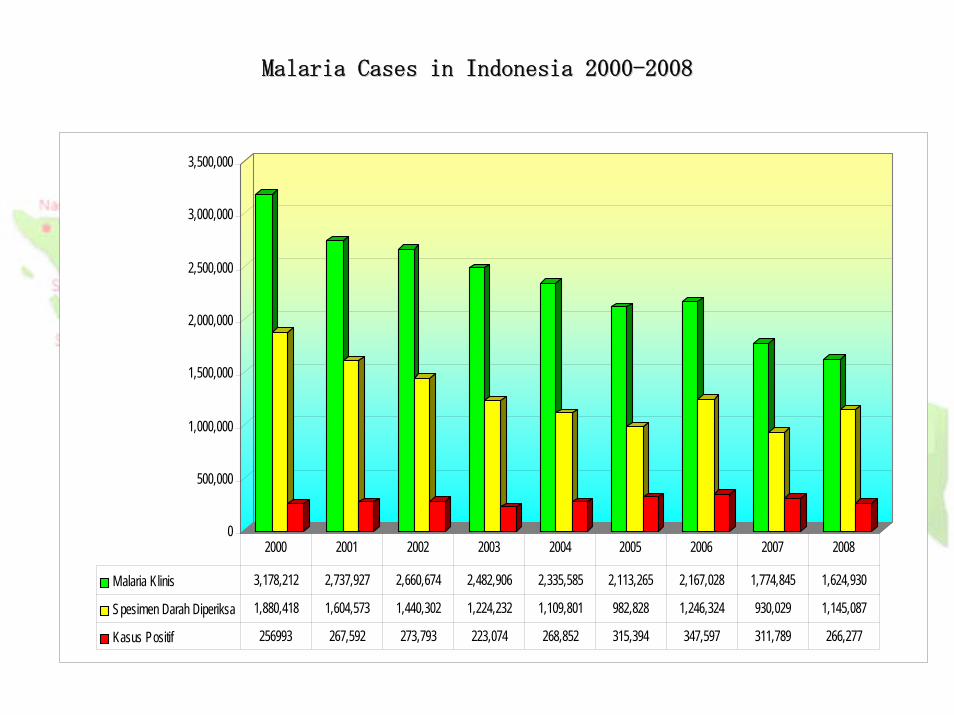
Malaria Klinis 3,178,212 2,737,927 2,660,674 2,482,906 2,335,585 2,113,265 2,167,028 1,774,845 1,624,930
Spesimen Darah Diperiksa 1,880,418 1,604,573 1,440,302 1,224,232 1,109,801 982,828 1,246,324 930,029 1,145,087
Kasus Positif 256993 267,592 273,793 223,074 268,852 315,394 347,597 311,789 266,277
2000 2001 2002 2003 2004 2005 2006 2007 2008
Malaria Cases in Indonesia 2000Malaria Cases in Indonesia 2000--20082008

1
1
2
3
4
5
6
7
89
10
11
12
13
14
1 4
1 515
16
1 6
16
17
17
18 19
202 0
20
20
21
2121
21
2 2
22
23
24
24
25
25
PENYEBA RA N V EK TOR MA LA RIA DI INDONESIA 2008VECTOR MALARIA IN INDONESIA
Keterangan : 1. An.aconitus 6. An. flavirostris 11. An. ludlowi 16.An.sinensis 2. An.balabacensis 7. An. koliensis 12. An.maculates 17. An. .subpictus3. An.bancrofti 8. An.letifer 13. An.minimus 18 An.sundaicus 4. An.barbirostris 9. An.leucosphyrus 14.An.nigerrimus 19. An. vagus 5. An.farauti 10. An.karwari 15. An.punctulatus 20. An. umbrosus21. An.tesellatus 22. An.parangensis 23.An. kochi 24.An.ludlowi 25.An.annullaris
OBJECTIVES : Indonesia
1.1. By the year 2010 be able By the year 2010 be able to decreaseto decrease all HCI all HCI areas (villages with malaria positive areas (villages with malaria positive ≥≥ 5 per 5 per 1000 pop) 1000 pop) by 50 %by 50 %
2.2. In year 2010 all districts and cities able to In year 2010 all districts and cities able to conduct conduct confirmationconfirmation of malaria suspected cases of malaria suspected cases and 100% treat withand 100% treat with ACTACT
3. In year 2010 all Indonesia’s endemic areas conduct intensification and integration in malaria control.
4. By the year 2010 begin elimination of malaria in stepwise by Islands

OBJECTIVES :ELIMINATION
1. Elimination in DKI, Bali, Batam: 2010
2. Elimination in Jawa and Aceh : 2015
3. Elimination in Sumatra, NTB, Kalimantan, Sulawesi: 2020
4.Elimination in Papua, WestPapua, Maluku,, NTT, North Maluku : 2030
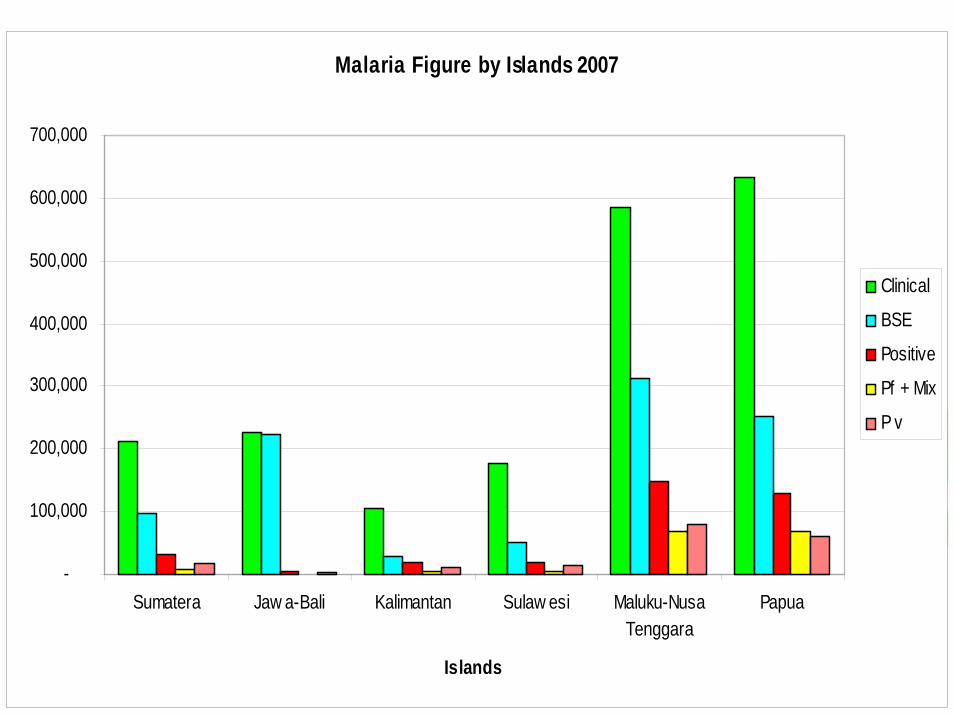
Malaria Figure by Islands 2007
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
Sumatera Jaw a-Bali Kalimantan Sulaw esi Maluku-NusaTenggara
Papua
Islands
Clinical
BSE
Positive
Pf + Mix
P v
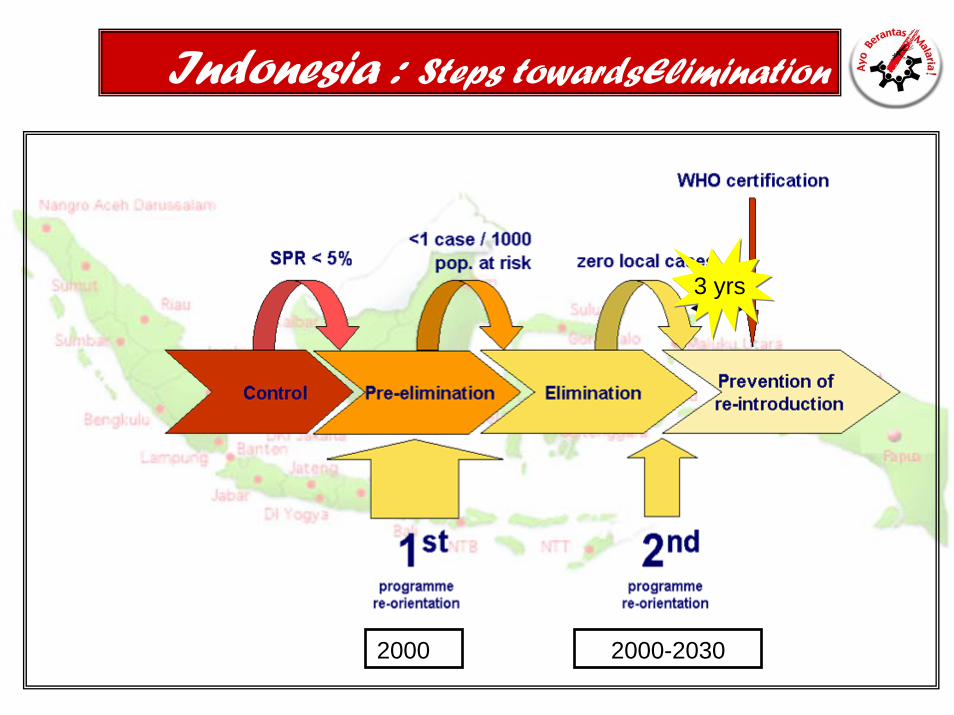
Indonesia : Steps towardsElimination
2000
3 yrs3 yrs
2000-2030
Indonesia : Elimination
CONTROL PHASE :-No or limited confirmation activities, limited microscopist.- Diagnosis :Clinical Malaria-Predominantly Plasmodium falciparum-Weak in surveillance , outbreak often occur and late in control it - prevalence still high, SPR > 5 %
-PRE ELIMINATION- Good confirmation activities-Good surveillance activities, towards the zero transmission (indigenous)-API < 1 / 1000 population at village level

Intervention towards Elimination
• Confirmation of all malaria cases by quality malaria microscopy
• Full coverage by effective antimalarial drugs given free of charge
• Total coverage by IRS the main prevention measure in active foci (coverage >85%)
• Use LLN as prevention and vector control• Strong malaria information system covering all health
facilities including community surveillance• Surveillance system to classify all cases and all foci with
their present functional status (in real time) • Active case detection• Geographical reconnaissance
ACTIVITIES
TrainingsTrainingsActive case detection (MBS. MFS).Active case detection (MBS. MFS).
Case management: diagnosis and treatment.Case management: diagnosis and treatment.Vector control/IVM ( IRS and LLIN).Vector control/IVM ( IRS and LLIN).Village Malaria Posts with Village Mal Village Malaria Posts with Village Mal Cadres.Cadres.Procurement of laboratory facilities Procurement of laboratory facilities (Microscope and RDT) laboratory supplies , (Microscope and RDT) laboratory supplies , LLIN and ACT. LLIN and ACT. Advocacy : RBM forum , partnership NGOAdvocacy : RBM forum , partnership NGO’’s , s , Private, expert organizationPrivate, expert organization

Indonesia: SCALLING UP
Integration and Intensification of Malaria Control ActivitiesIntegration and Intensification of Malaria Control Activities. . -- Mass Blood SurveyMass Blood Survey-- Malaria treatment and bednet distribution to pregnant women.Malaria treatment and bednet distribution to pregnant women.-- Malaria treatment and Bednet distribution during immunization Malaria treatment and Bednet distribution during immunization
program. program. -- Bednet distribution during Mass Drug Administration for FillariaBednet distribution during Mass Drug Administration for Fillariasis sis
control program and conduct mass campaign.control program and conduct mass campaign.-- Establishment of Village Malaria PostsEstablishment of Village Malaria Posts
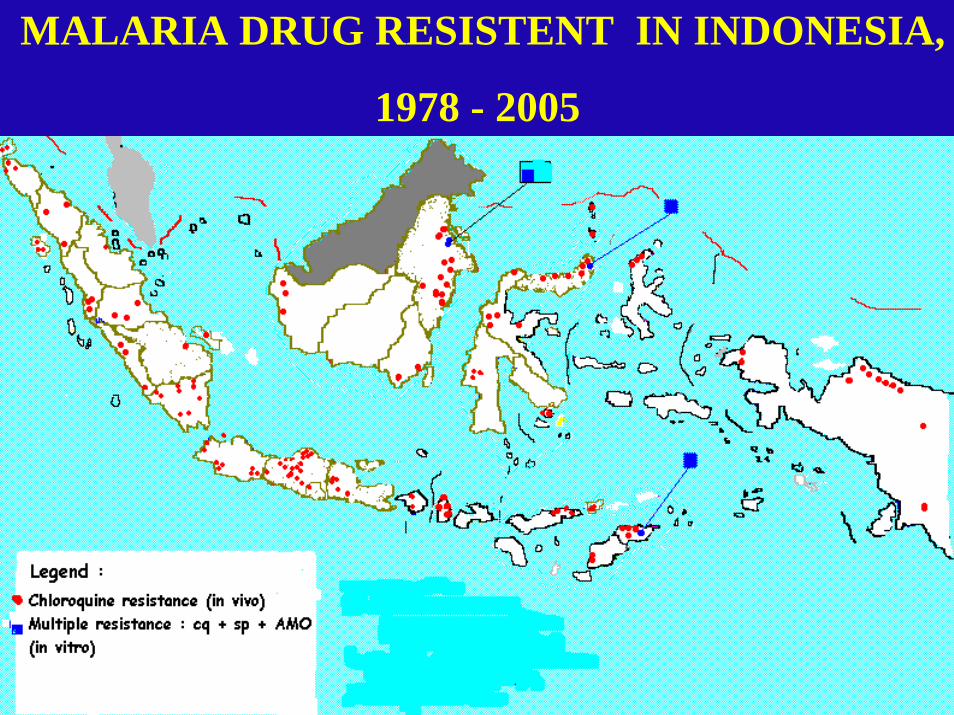
MALARIA DRUG RESISTENT IN INDONESIA,
1978 - 2005
16
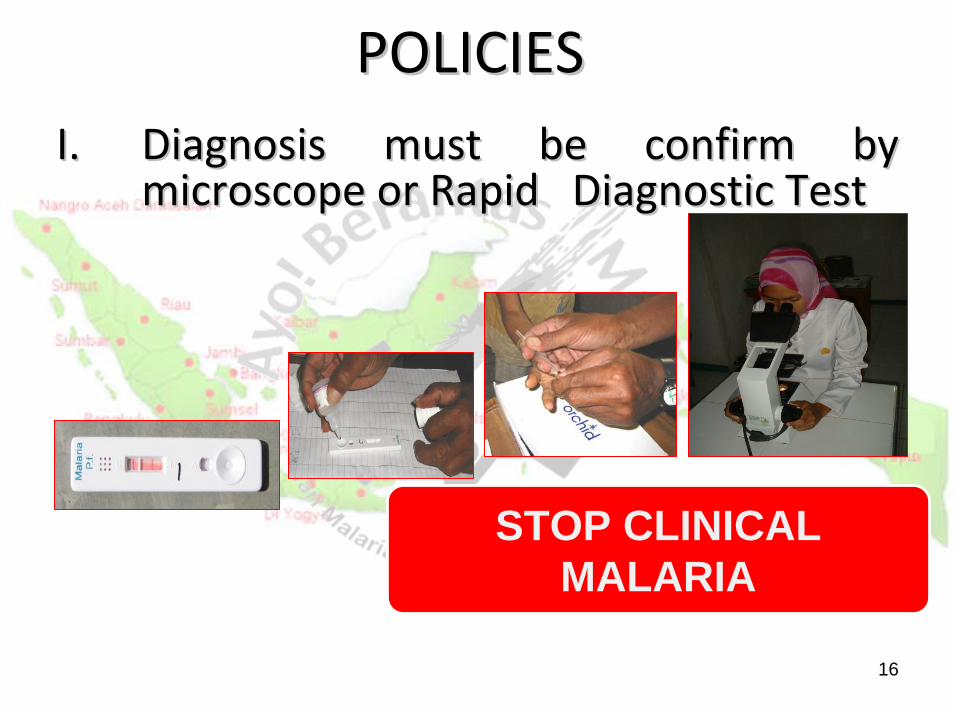
POLICIES POLICIES I.I. DiagnosDiagnosis must be confirm by is must be confirm by
mimiccrosrosccopopee oror Rapid Diagnostic TestRapid Diagnostic Test
STOP CLINICAL MALARIA

17
POLICIESPOLICIESII.TREATMENTII.TREATMENT
ArtemisininArtemisinin--basedbased Combination TherapyCombination Therapy (ACT)(ACT)
STOP MONOTHERAPY
18
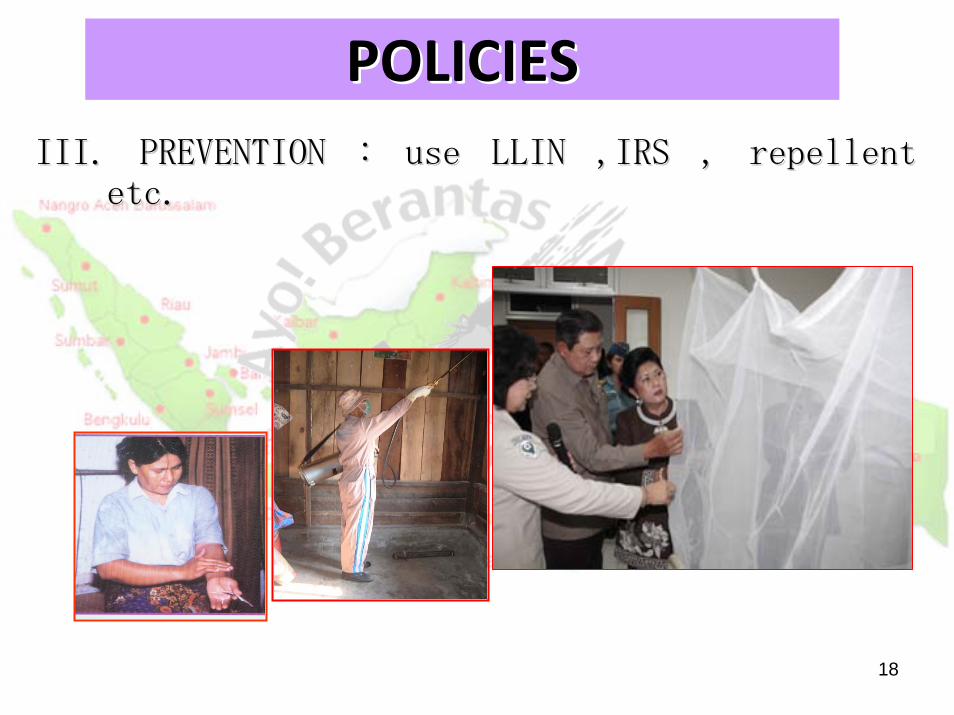
III. PIII. PREVENTION : useREVENTION : use LLIN ,LLIN ,IRSIRS ,, repellentrepellentetc.etc.
POLICIESPOLICIES

19
IV.IV. Intersectoral collaboaration in RBM Intersectoral collaboaration in RBM forum.forum.
PoliciesPolicies
20
V.V. Community participation through Community participation through strengthening the Village Malaria Post strengthening the Village Malaria Post and Village Malaria Cadre/volunteers.and Village Malaria Cadre/volunteers.
PoliciesPolicies
PKK Kabupaten PKK Kabupaten Banjarnegara Banjarnegara Peserta Paduan Peserta Paduan Suara Lagu Suara Lagu ““Gebrak Gebrak MalariaMalaria””

Indonesia : ACHIEVEMENT IN PILOT DISTRICT
• 897 midwives out of 1034 has been trained and equiped in 2007. (86.7%)
• 38,688 new pregnant women out of 49,371 received LLIN when visiting ANC in 2007. (78.8%)
• 16,736 new pregnant women out of 32,786 screened for malaria (51%)
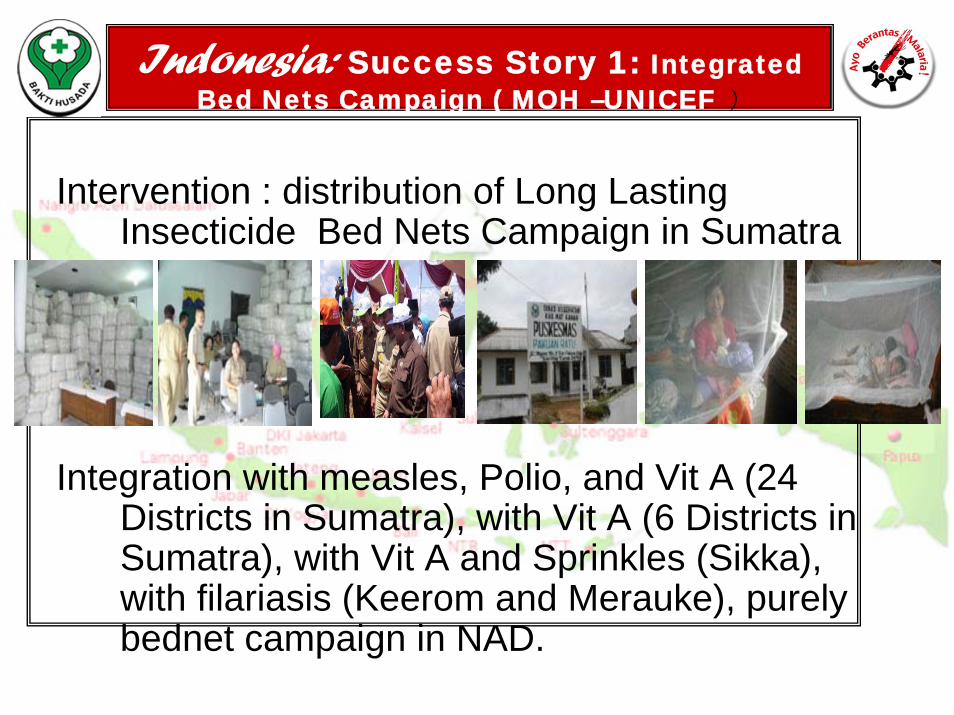
Indonesia: Success Story 1: Integrated Bed Nets Campaign ( MOH –UNICEF )
Intervention : distribution of Long Lasting Insecticide Bed Nets Campaign in Sumatra
Integration with measles, Polio, and Vit A (24 Districts in Sumatra), with Vit A (6 Districts in Sumatra), with Vit A and Sprinkles (Sikka), with filariasis (Keerom and Merauke), purely bednet campaign in NAD.
Indonesia : Success story : Continued
-In total 3,8 million nets were distributed
-Achievement in Sumatra (rapid assessment 1 month after campaign) :
-% HH who has 1 or more ITNs, increased from 2.2% (2/91) before the campaign to 94.5% (86/91) after the campaign. -But the % ITNs that was used/hanged = 44.8% (64/143) -% children under five years of age who slept using ITN increased from 1.9% (2/106) to 51% (54/106) after the campaign
-Figures from other districts were more or less similar
-Benefit for other program was noted and appreciated (high coverage of EPI, nutrition, and mass drug administration of filariasis)

Success story 2 : Vector control program through community mobilization
Intervention : Community based vector control, using PLA (Participatory Learning and Action) approach/Mr. Bangkit (workshop management of vector
control programs, Cambodia, August 2008).Achievement : together with Sub Dit Vector/Mr.Winarno, WHO, PHO, and DHO develop training and activities in the villages in South Halmahera
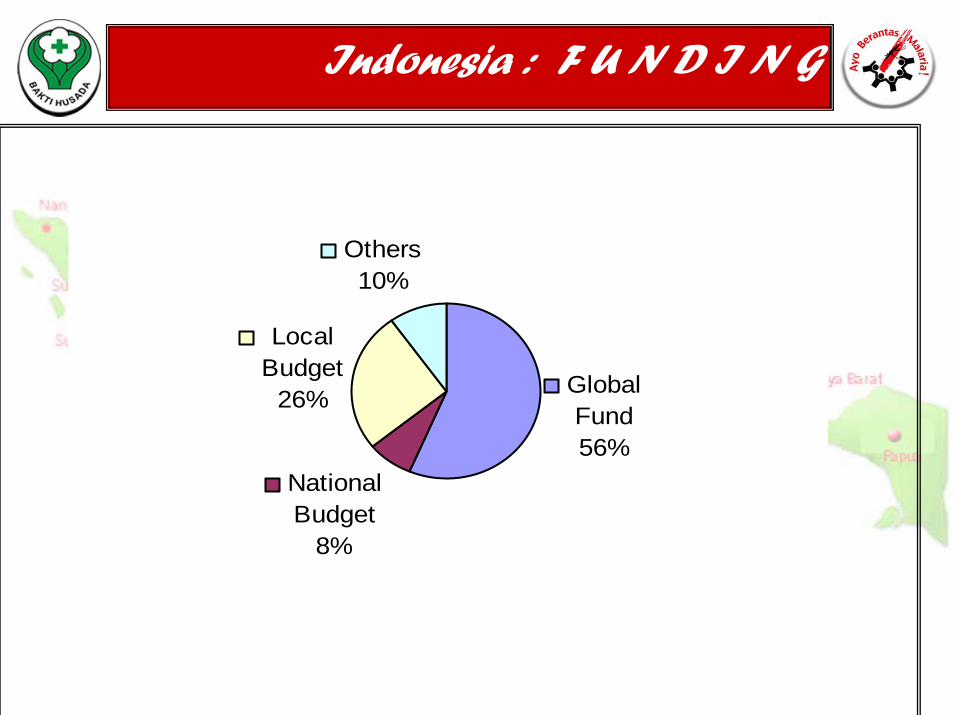
Indonesia : F U N D I N G
Global Fund 56%
Others 10%
Local Budget
26%
National Budget
8%

Indonesia : F U N D I N G needed
National Bednets Availability 2008-2012
-10,000,00020,000,00030,000,00040,000,00050,000,00060,000,00070,000,00080,000,00090,000,000
Needs (5 yrs ) Actual (3 yrs) Gaps (Needs-Actual)
Plans GF R8 (5 yrs)
Indonesia : Challenges
Lack of access to health facilities in Lack of access to health facilities in very remote areas and hard to reach very remote areas and hard to reach islands.islands.Inequality of health development (Java VS Inequality of health development (Java VS Outer Java). Outer Java). Limitation of adequate Malaria Human Limitation of adequate Malaria Human Resources mostly microscopist & Resources mostly microscopist & entomologistentomologist (Ms.Hasni & Ms(Ms.Hasni & Ms..MelvinawatiMelvinawati,,both both
are participants from strengthening training in Malaria are participants from strengthening training in Malaria microscopy & quality assurance in Philippines, Sept 2008)microscopy & quality assurance in Philippines, Sept 2008)
Environmental changes relates to Environmental changes relates to increasing of mosquito breeding placesincreasing of mosquito breeding placesLimited Operational research Limited Operational research

Indonesia : Challenges
1. Quality of midwives performing RDT needs to be closely evaluated and improved
2. Poor distribution of health workers (midwives) in remote places (in this setting, IPT needed? )

Indonesia : Challenges & opportunities
1. Expansion to 101 district for malaria in pregnancy and 70 district for integration of routine EPI is huge and will need strong technical capacity and strong collaboration to have good quality program.
2. Expansion will need to be continued beyond GF funding.
3. Campaign is effective to reduce malaria in most endemic area, though, expensive.
4. Most malaria endemic area are remote and difficult to reach, logistic and coverage is a challenge
`THANK YOUTerima kasih