towards in vivo microimaging of lung inflammation … in vivo microimaging of lung inflammation and...
TRANSCRIPT

Towards In Vivo microimaging of Lung Inflammation and Repair:
Current issues and future directions
O. Lesur1, P.G. Charette
2, Ph Jouvet
3, F. Cheriet
4, and F. Chagnon
1
1Medical Intensive Care Unit, CRC-CHU Sherbrooke, Faculty of Medicine, University of Sherbrooke, Quebec, Canada 2Department of Electrical and Computer Engineering, Faculty of Engineery, University of Sherbrooke, Quebec, Canada 3Pediatric Intensive Care Unit, Sainte-Justine Hospital, University of Montreal, Quebec, Canada 4Department of Computer Engineering, Ecole Polytechnique de Montreal, University of Montreal, Quebec, Canada
Rationale: a new lung imaging technique based on endoscopic confocal fluorescence microscopy (ECFM) is presented,
which is a new method able to provide cellular and structural assessment of living tissue using a miniaturized confocal
probe in direct contact with the visceral pleura or introduced through the airways down-to the airspaces.
Objectives: To observe distal airspace structure and cellular&molecular conditions in normal and injured lungs (hyperoxic
and bleomycin challenged), using fluorescent-specific marker contrast and ECFM. To avoid surgical open lung biopsies
and tissue fixation procedures, and directly visualize real-time condition of selected regions of interest.
Methods: Alveolar space ECFM (using a Five-1® system) with spectral analyses are performed at 488-nm excitation
using FITC-labeled markers or naturally fluorescent dyes. The normal lung is compared with the sick lung, where in vivo
imaging experiments correlated well with results obtained with corresponding ex vivo conventional histological assays.
Comparisons with current radiological lung imaging procedures, and with alternative ECFM techniques presently
available are given.
Data: Main elements pertaining to the acute lung injury/ acute respiratory distress syndrome (ALI/ARDS)
pathophysiology and established early key events, such as inflammation and repair, can be specifically studied: alveolar
epithelial membrane phenotype, lung cell apoptosis, neutrophil recruitment, and edema. ECFM allows visualization of : i)
fine-tuned ultrastructural lectin (RCA-1, PSA) epithelial cell membrane expression, ii) YO-PRO®-1-related DNA linking
of lung cell apoptosis, iii) PKH2 green fluorescent cell linker-labeled neutrophil tracking in lung microcirculatory network
and airspaces, iv) FITC-dextran plasma contrast and extravasation with edema formation. ECFM provides reliable and
comparable results to corresponding ex vivo fluorescent methods.
Conclusions: ECFM, using a minimally invasive optical instrument and specific fluorescent markers, is able to provide
real-time revolutionary imaging of live unfixed normal and injured lung tissue with promising developments for
improving bedside diagnostic and decision-making therapeutic strategy in patients with acute lung injury (ALI). Works are
in progress to establish a user-friendly multimodal interface of macro- and microimaging of the lung, including ECFM,
and using a “google earth” approach.
Keywords: Lung microimaging in vivo, ALI/ARDS, epithelium, neutrophils, edema
Implementing better methods for understanding tissue repair and regeneration is necessary to further scientific
knowledge about human disease and is especially required to develop new therapeutic approaches for use by bedside
physicians. Some human tissue properties, such as the skin, have been extensively studied, but lung repair is still a
developing and promising field. This non-exhaustive review discusses current knowledge of lung inflammation and
repair, methods of assessing this condition in the clinical setting, as well as commonly used lung imaging techniques
and their use in the evaluation of lung repair and imaging techniques currently in development. In particular, new
technologies allowing in vivo imaging of lung inflammation/repair are now available, opening many new research
possibilities and eventually new clinical tools for the assessment and treatment of acute lung diseases at bedside. In this
respect, the 2007 American Thoracic Society (ATS) proceedings on small animal imaging of the lung includes among
its recommendations for future directions, to “utilize imaging modalities to investigate intracellular lung
pathophysiology in vivo and in real time”[1]. This new technology area shows several advantages over older imaging
procedures, but obstacles must still be overcome before it integrates regular medical practice.
Current understanding of lung inflammation/ repair stems from the knowledge acquired in the study of several lung
diseases whose physiopathology involves inadequate, dysfunctional or inappropriate tissue repair. Examples include
acute lung injury (ALI) and acute respiratory distress syndrome (ARDS), chronic obstructive lung disease (COPD),
asthma, idiopathic pulmonary fibrosis and other interstitial lung diseases. Specifically, knowledge acquired from the
study of ALI using animal models (e.g. the bleomycin rat model) has given us greater insight into lung repair.
Therefore, much of the information on the mechanisms of lung repair provided in this article is derived from ALI
animal model studies [2-4].
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 633
______________________________________________

Mechanisms of lung repair
The human respiratory system is composed of airways leading to a fine network of blood vessels and alveoli. This
fragile system must act as an efficient barrier to fight exterior microorganisms and chemical aggressors, as well as to
retain its intended function in maintaining gas exchange and homeostasis. When needed, normal lung tissue must
respond to exterior aggression and initiate repair while preserving the delicate interface between the epithelial and
endothelial lumen. In addition, all cellular components must function in the constantly mobile environment of the
breathing lung, in contrast to the mostly static environment of most tissues.
Lung repair is made of a series of complex processes that begins with a response to aggression and involves tissue
inflammation with recruitment of white blood cells, migration of epithelial cells and fibroblasts and extracellular matrix
deposition. Interactions between these committed cells are mediated through cytokines and growth factors which are
still being studied and elucidated. Known mechanisms of lung repair in the setting of different disease models have
been extensively reviewed, and it is beyond the scope of this article to describe in detail the different healing pathways.
Nevertheless, the general mechanisms will be discussed as a starting point for future directions in in vivo lung imaging.
Lung injury and repair can be divided into 3 phases; the triggering event, an initial inflammatory and exudative phase,
and finally a fibroproliferative phase during which lung architecture is restored.
The initial triggering event may take diverse forms such as microorganisms (chemical and physical), aggressors,
allergens or circulating immune complexes. Whichever the triggering event, it results in a disruption of the integrity of
the alveolar-capillary membrane complex, with alveolar type I, type II and endothelial cell damage, necrosis and
apoptosis as well as basement membrane exposure. Regulation of apoptosis is thought to play a major role in tissue
repair [5, 6]. All lung cell types can undergo apoptosis in particular settings. Initial injury, especially if of an
inflammatory nature, may induce apoptosis rather than necrosis of alveolar epithelial cells, such as in ALI. Clearance of
excess neutrophils, fibroblasts and alveolar epithelial type II cells is thought to be regulated by apoptosis. The apoptotic
pathways (such as Fas/FasL ligand, bax/bcl-2 and myc proto-oncogen systems) are extremely complex and the role and
mechanisms of each throughout the process of lung repair are largely unknown. Structural cell apoptosis (i.e. epithelial
and endothelial) occurs very rapidly, making it very difficult to study with traditional methods, whereas neutrophil
apoptosis is delayed in ARDS as well in sepsis [7-8]. In this respect, real-time in vivo microscopy of apoptotic cells may
provide more insight in this process.
The inflammatory phase is initiated by the damaged, necrotic and apoptotic cells and exposed extracellular matrix
components. It is usually characterized by a protein rich exudate and infiltration of white blood cells such as neutrophils
and macrophages. The type of white blood cell infiltrate will be influenced by the type of triggering event. All
implicated cell types (type I and II alveolar epithelium, endothelium and white blood cells) will produce the cytokines
and other molecules responsible for the initiation of the repair process and the influx of other cells. Tumor necrosis
factor (TNF-α) and interleukins (e.g. IL-1β, IL-6, IL-8) play major roles in promoting inflammation while IL-10 is
thought to play an anti-inflammatory role. The balance of pro- and anti-inflammatory mediators will then determine if
the response is appropriate, self-limited or inappropriate and inadequately sustained.
The proliferative phase is characterized by epithelial type II cell proliferation and influx of fibroblasts. Alveolar type
II cells proliferate, migrate to the damaged area, recreate and remodel the underlying basement membrane (partly with
the help of fibroblasts) and finally differentiate into type I cells. Extracellular matrix deposition and remodelling is a
careful balance mediated by alveolar type II cells, fibroblasts and macrophages through molecules such as transforming
growth factor (TGF-β), macrophage derived platelet derived growth factor (PDGF), interferon-γ, TNF-α and IL-1β.
This is a crucial phase which leads to restoration of tissue integrity and function or, in examples such as ARDS and
interstitial lung diseases, to pulmonary fibrosis.
In summary, lung repair is composed of complex, dynamic and partly understood processes which occur at the
cellular and molecular levels. Only by studying it at this microscopic and molecular level can we truly aim to
comprehend and influence it.
Evaluation of lung repair in the clinical setting
There are currently no methods for direct assessment of lung repair in the clinical settings. Clinical tools are directed at
correct diagnosis in order to proceed to adequate treatment. Response is then assessed by history, physical exam,
imaging and function tests. There are no available methods to evaluate the state of lung repair in a patient, either to use
as guidance for the best timing in initiating treatment or to monitor treatment response. All current evaluation methods
do not permit a clear understanding of the repair process, only showing the initial consequences of loss of function, then
monitoring the return to normal function or further deterioration.
Bedside clinical evaluation tells the physician how much the lung function is deteriorating after the initial insult or
inadequate repair. In a highly simplified example, as a patient shows increasing dyspnea, low blood oxygen saturation
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
634 ©FORMATEX 2010
______________________________________________

and arterial blood gas indicating hypoxemia, his treating physician will suspect impaired oxygen exchange, and direct
further investigation at identifying the cause and treatment at restoring the lung’s impaired function. Patient’s
symptoms, vitals, and blood gases will inform the physician if lung function is improving or has returned to normal. It
will be assumed that the lung has repaired, without any direct assessment of lung repair itself. Commonly used
investigative tools have the same weakness, showing consequences of injury and repair in greater detail, but not the
underlying state and mechanisms of repair itself.
Chest imaging is an essential part of the lung diagnostic workup [9-11]. Standard chest x-ray will show infiltrates,
patterns of fibrosis or changes in lung volumes. Alveolar or interstitial infiltrates suggest local inflammation or
increases of membrane permeability. Indicators of fibrosis show the end-point of tissue repair, such as adequate healing
response and minimal scarring or completely pathological and disorganized healing progressing to diffuse alveolo-
interstitial fibrosis. Computerized tomography (CT) of the lung provides similar information, thus allowing better
characterization of parenchymal abnormalities. For instance, it is possible to radiologically differentiate the early
exudative with the late proliferative and fibrotic phases of ALI, the former showing ground-glass attenuation and
alveolar consolidation and the latter traction bronchiectasis and interstitial fibrosis. CT scanning of the lung provides
essential diagnostic information, making it possible to identify and differentiate many lung diseases, such as the
interstitials pneumonias, ALI, atelectasis, bacterial pneumonias and pulmonary edema. It provides better clues than
bedside assessment pertaining to the stage and progression of lung repair or misrepair but, like the previous methods
described, gives not much insight into the underlying cellular or molecular processes and most often requires the patient
to be mobilized with potential related morbidity.
Non-imaging methods of lung investigation include bronchoalveolar lavage and open lung biopsy. Broncholaveolar
lavage is diagnostically useful by providing white blood cell counts and most importantly adequate material for
microbiological cultures. In the research setting, it is often used to isolate inflammatory molecules such as TNF-α or IL-
1β. The clinical relevance of identifying inflammatory marker patterns is yet to be determined, but shows promise as a
future method in assessment of lung repair. Open lung biopsy and video assisted thoracoscopy are used for patients with
persisting respiratory failure without a clear underlying cause [12-14]. It allows the histological examination of actual
lung tissue, thus providing extremely accurate diagnosis. Microscopic lung architecture and diagnostic elements such as
hyaline membranes, white blood cell infiltrates, and collagen distribution are directly visualized. Immunohistochemistry
and immunofluorescence may also be performed on the collected specimens. Some groups have described advantages
to use open lung biopsy in this context [14]. However, disadvantages limiting the clinical use of surgical lung biopsy are
mainly the potential morbidity related to the use of an invasive technique on already critically ill patients, and the
effective setup availability of expert advice from a lung pathologist. Other disadvantages compared to in vivo
microscopy are the questionable representativity and specificity of the selected sampled lung portion with regards to the
frequent patchy nature of the insult, the static nature of the specimen and the potential architectural and molecular
alterations related to the fixation process.
Recently developed imaging modalities
Micro-CT. Computed tomography (CT) is doubtlessly the most used technique, because of its very good resolution and
its good acquisition speed. High resolution CT (HRCT), which has very good spatial resolution (1mm slices), is
gradually being replaced by a new technique called Multi-detector CT (MDCT). MDCT even allows the segmentation
of the bronchial tree to the 5th
generation. This new technology advance in CT permits new approaches in imaging of
the lung, with more and more resolution and allows local measurement of the lung (lung ventilation, lung volume and
no more for the entire lung with the Xenon-enhanced CT (XE-MDCT). With new contrast methods, the visualisation of
vascular and lung perfusion is made possible. In the future, CT imaging will be associated with a magnetic resonance
(MR) scanner, to complement the information obtained with CT [15].
MRI. Magnetic resonance imaging (MRI) is also a progressively more widespread technique. In its beginnings, MRI
had low intensity, due to low density of protons and tissue inhomogeneity. These problems are very present in the air-
filled lung, as the air itself is not easily detectable by MRI. Furthermore, the fluid-air interfaces cause a phenomenon
called susceptibility artefacts [16]. When two tissues at an interface have different magnetic susceptibility (intern
animation due to magnetic field) it creates a magnetic distortion. In some cases, the low proton density in lung can be an
advantage because certain inflammatory and neoplastic processes increase the number of protons [15]. Hyperpolarized
gases, the most used being 129
Xe, have further increased the MRI resolution. The polarization of these gases has been
enhanced by a factor of up to 100,000 to extend their detection [1]. Another technique used to increase the resolution is
Fast-MRI. The lung is constantly in motion, therefore causing movement artefacts. Fast-MRI uses new receptors and an
HF antenna to attenuate these artefacts. MRI is also used to ascertain more complex lung characteristics, by
measurements of local lung physiology. For example, the pulmonary blood flow can be measured, but this presents its
own difficulties due to low proton density [17]. MRI’s advantages over CT include the improved acquisition speed and
absence of radiation.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 635
______________________________________________

Micro-PET. New positron emission tomography (PET) technology, especially the combined CT/PET, has permitted
new results in small animal imagery. PET allows the visualisation of in vivo mechanisms and has numerous applications
(e.g. brain injury, bone degeneration) [1]. The main problem with PET is its low sensitivity to small signals.
Furthermore, the dose of radiation can have an influence on the results. To obtain the radioisotope, a cyclotron is
needed, and the cost is high. One of its derived techniques is single photon emission CT (SPECT) [18]. In spite of
having decreased resolution and a longer acquisition time compared to CT, SPECT allows the simultaneous
visualisation of some mechanisms such as blood and air circulation. A significant advantage of SPECT is 3D
reconstruction which gives tridimensional information on the pulmonary structure or on the precise configuration of
abnormalities such as lung tumours. PET is used to get some lung parameters, such as the regional effective alveolar
ventilation-perfusion (VA˙/Q˙), and even the degree of bronchoconstriction [19].
Echography. Echography can also be used to image the lung, but it is mostly restricted to the visualisation of the
pleural space because of the poor echogenicity of air in the lung. A new technique, called ultra sound lung comets
(ULCs), allows the measurement of the extra vascular water in the lung. This imaging modality is well adapted with
ARDS because water is very present, due to the thickening of the alveolar wall. With a pulmonary injury model
reproducing the first stage ARDS, Gargani has proven that ULCs are capable of quickly detecting the extra vascular
water in pigs [20]
Molecular markers. The lung has a low background signal, allowing the use of molecular markers. There are two types
of molecular imaging: one uses the endogenous targets (direct imaging), and the other uses a reporter gene (indirect
imaging). The principle of direct imaging hinges upon the presence of receptors such as enzymes or kinases in the target
tissue. Indirect imaging is based on gene expression or protein-protein interactions [1]. This technique can be compared
with PET (with FDG) and is very useful in several lung diseases. The molecular markers are particularly useful in
staging non-small cell lung cancer and searching for metastasis [21].
The above techniques are very useful to obtain structural and physiological information of the lung, but they don’t
allow the evaluation of the state of pulmonary repair. Microscopic in vivo imaging shows great promise in
complementing these techniques.
Imaging modality: microscopic in vivo imaging
Developments in microscopic in vivo imaging are booming. Its potential to evaluate pulmonary repair is high. The
molecular or cellular information that physicians can obtain from this technique is very important in ARDS. It is with
the presence (or the absence) and number of certain cells that the physicians can evaluate with precision if the lung is
repairing or not. This technique can be divided in two subcategories: transthoracic and endobronchial imaging. The
approach in both cases is totally different but the information is quite similar. Two companies have developed systems
that can be used to lung in vivo microscopy: Mauna Kea (France) and Optiscan (Australia). Both systems are fibered
confocal fluorescence microscopes (FCFMs).
Mauna Kea has chosen the endobronchial approach. They have introduced the “alveoloscopy” term, because their
instrument can go down the lung airways to the alveoli. The system is equipped with very small probes (350 to
1800µm, depending of the probe), allowing physicians to observe very small airspaces. This system can record video
sequences due to its fast acquisition rate (12 frames/sec) [22]. It mainly depends on endogenous fluorescence produced
by the elastin component of the basement membrane zone [23]. It has a good spatial resolution (lateral resolution of
3.5µm) and a field of view of 600µm, allowing the observation of very small structures.
The Optiscan instrument has two configurations: a flexible endoscopic system for clinical use marketed by Pentax
and a rigid pen-like probe (6mm diameter) for research applications. In both cases, a transthoracic approach is required.
The size and rigidity of the probe precludes an endobronchial approach, so the probe must be applied directly on the
pleura. Lateral resolution is 0.7µm and axial resolution is 7µm. Due to the acquisition speed (0.7 to 1.4 frames/sec), the
recording of video sequences is not allowed, but with several successive images and appropriate software, video
sequence reconstruction is possible. An advantage of this system is its ability to image through tissue, as it is a true
confocal microscope with adjustable imaging depth. Indeed, the focal plane can be moved from the surface to 250µm in
depth, allowing the tridimensional structure of the lung to be better observed. However, the system cannot detect
endogenous fluorescence, so that the injection of contrast agents is necessary.
Other advances in intravital microscopy (IVM) require a window-based preparation for the visualisation of
subpleural lung microvessels, for example the implantation of flanged steel windows in the thoracic wall. Stabilisation
is assured via suction through a borehole. With window approaches, blood flow and blood cells can be visualised more
easily [24].
Real-time fluorescence imaging (RFI) allows the visualisation of lung cellular or molecular responses, e.g. the
determination of cytosolic Ca2+
levels. RFI has been coupled with immunofluorescence, for observation of leukocyte
adhesion in lung [24].
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
636 ©FORMATEX 2010
______________________________________________
Microscopic in vivo technique is a judicious choice for imaging the lung in the setting of lung injury, such as in
ARDS. This technique brings important information not only concerning the structure of the lung, but especially its
state of repair.
Advantages, limits and future directions for in vivo microimaging
In the study of lung inflammation/ repair, microscopic in vivo imaging shows major advantages over traditional imaging
techniques as well as techniques still in development. It is the only imaging modality able to visualise microscopic lung
architecture without the need for collecting actual tissue, as in open lung biopsy. With the use of in vivo markers, it has
the potential of providing at least as much information as a biopsy specimen, with the added benefit of visualising
actual live tissue. An in vivo image is not altered in any way, showing cells in their natural homeostasis. Surrounding
molecules such as cytokines, growth factors and hormones are also intact. In vivo imaging eliminates confounding
factors related to laboratory in vitro techniques. With the additional benefit of real-time imaging, potentially any in vivo
cell movement is visible to the examiner. Migrating leucocytes, creeping/repairing type II alveolar epithelial cells,
apoptosis and edema could be studied directly (e.g. figure 1 A-E). With the use of modern fluorescent biomarkers,
images of targeted circulating molecules and their site of action may someday be obtained for real-time functional
studies. The potential for acquiring new knowledge of lung repair and eventually using it for the benefit of patients is
immense, making in vivo microscopy a promising new research tool.
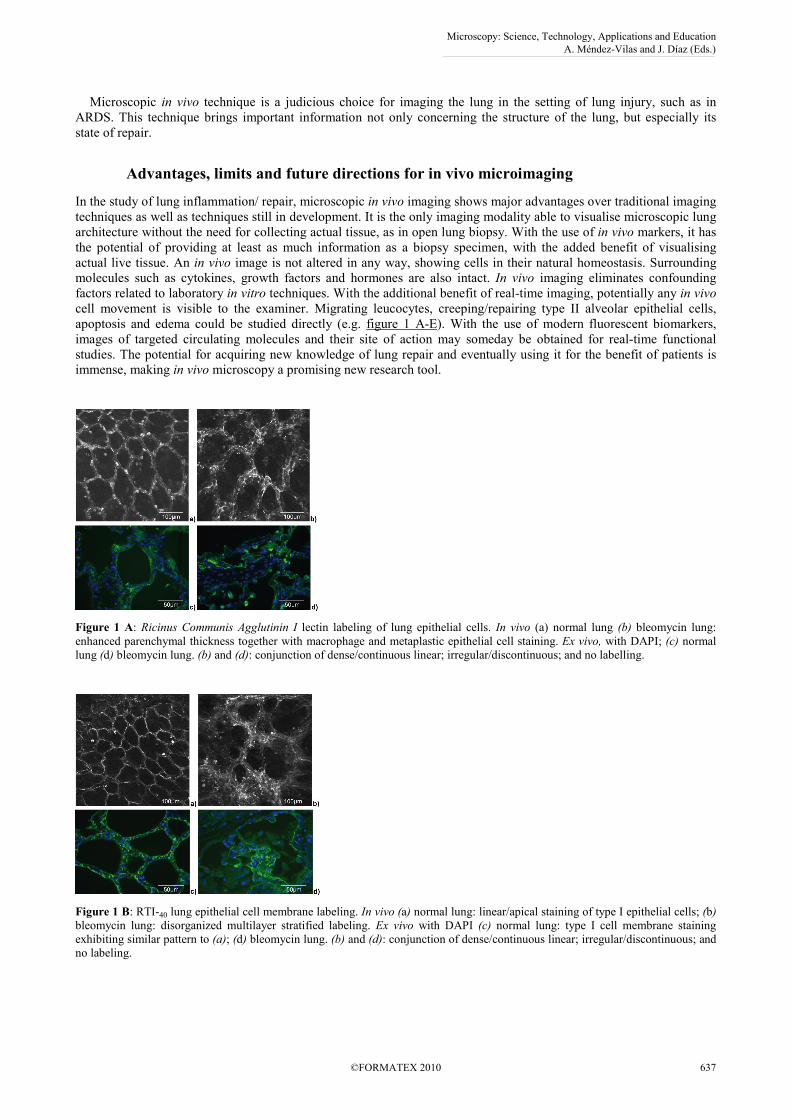
Figure 1 A: Ricinus Communis Agglutinin I lectin labeling of lung epithelial cells. In vivo (a) normal lung (b) bleomycin lung:
enhanced parenchymal thickness together with macrophage and metaplastic epithelial cell staining. Ex vivo, with DAPI; (c) normal
lung (d) bleomycin lung. (b) and (d): conjunction of dense/continuous linear; irregular/discontinuous; and no labelling.
Figure 1 B: RTI-40 lung epithelial cell membrane labeling. In vivo (a) normal lung: linear/apical staining of type I epithelial cells; (b)
bleomycin lung: disorganized multilayer stratified labeling. Ex vivo with DAPI (c) normal lung: type I cell membrane staining
exhibiting similar pattern to (a); (d) bleomycin lung. (b) and (d): conjunction of dense/continuous linear; irregular/discontinuous; and
no labeling.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 637
______________________________________________
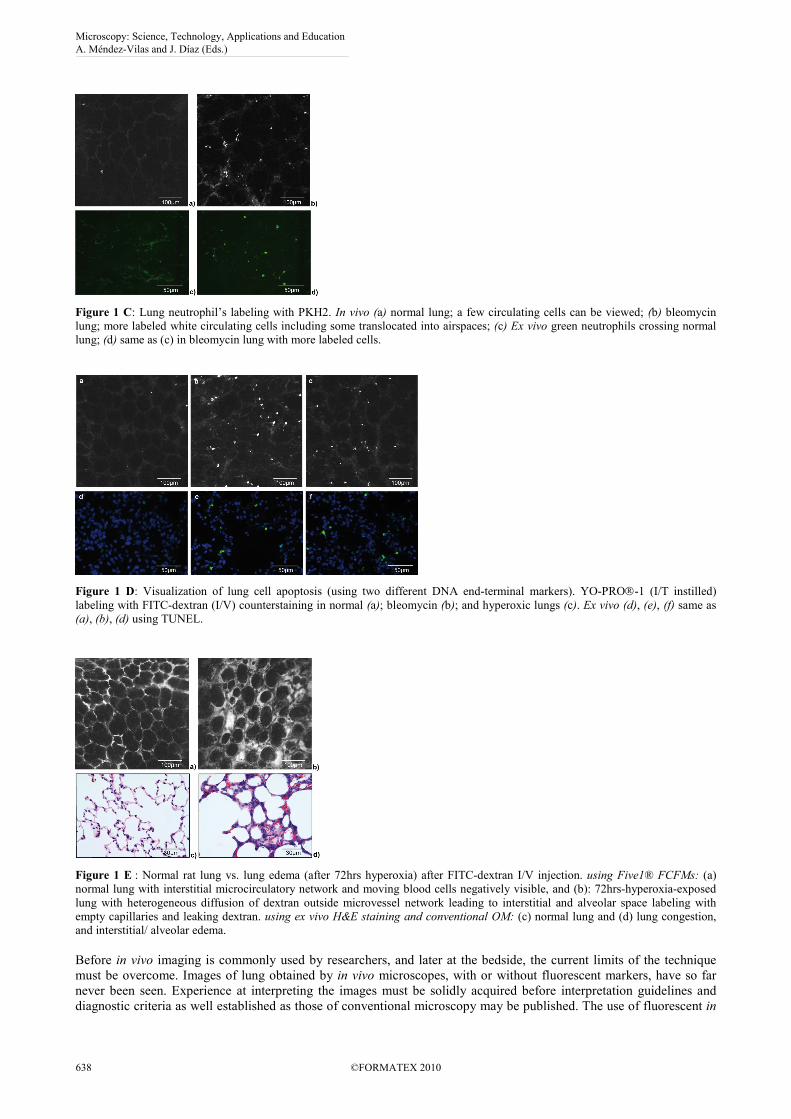
Figure 1 C: Lung neutrophil’s labeling with PKH2. In vivo (a) normal lung; a few circulating cells can be viewed; (b) bleomycin
lung; more labeled white circulating cells including some translocated into airspaces; (c) Ex vivo green neutrophils crossing normal
lung; (d) same as (c) in bleomycin lung with more labeled cells.
Figure 1 D: Visualization of lung cell apoptosis (using two different DNA end-terminal markers). YO-PRO-1 (I/T instilled)
labeling with FITC-dextran (I/V) counterstaining in normal (a); bleomycin (b); and hyperoxic lungs (c). Ex vivo (d), (e), (f) same as
(a), (b), (d) using TUNEL.
Figure 1 E : Normal rat lung vs. lung edema (after 72hrs hyperoxia) after FITC-dextran I/V injection. using Five1® FCFMs: (a)
normal lung with interstitial microcirculatory network and moving blood cells negatively visible, and (b): 72hrs-hyperoxia-exposed
lung with heterogeneous diffusion of dextran outside microvessel network leading to interstitial and alveolar space labeling with
empty capillaries and leaking dextran. using ex vivo H&E staining and conventional OM: (c) normal lung and (d) lung congestion,
and interstitial/ alveolar edema.
Before in vivo imaging is commonly used by researchers, and later at the bedside, the current limits of the technique
must be overcome. Images of lung obtained by in vivo microscopes, with or without fluorescent markers, have so far
never been seen. Experience at interpreting the images must be solidly acquired before interpretation guidelines and
diagnostic criteria as well established as those of conventional microscopy may be published. The use of fluorescent in
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
638 ©FORMATEX 2010
______________________________________________

vivo markers is still recent and much research is needed before an extensive and well studied panel is available.
Compared with traditional histology, in vivo marking is faced with the major challenge of having to contend with the
lung’s natural epithelial, endothelial and cellular membrane barriers. In addition the markers must also be proven safe
for human use. Other limitations of in vivo imaging are mechanical. The constant movement of live breathing lung
renders stabilisation of probes on a particular segment of tissue difficult. Also, the speed of image capture is often too
slow for rapid breathing movements, creating a kinetic blur and rendering image acquisition of the lung problematic.
Future advances in the probe technologies should soon correct these limitations. Greater mechanical limits are those
imposed by lung diseases with a patchy damage pattern such as ALI/ARDS. An ideal site of damaged lung must be
correctly identified before applying the probe. This is especially relevant in the case of the transthoracic approach, in
which a small opening in the thorax must be performed. Once the ideal site is identified and the first images are
obtained, the same site must be found again in order to conduct follow-up imaging, representing yet another significant
challenge at the microscopic level. Combination of traditional imaging technique like CT scanning with in vivo
microscopy may be useful in this setting. These are only some examples of the obstacles that must be overcome. New
challenges will likely surface as the technology and research continue to develop.
In the path to developing new treatments in lung diseases, better understanding of lung repair is a logical step.
Current imaging technologies are incapable of adequately assessing lung repair by the clinician. This clearly
demonstrates a great gap in bedside assessment that may be filled with in vivo microimaging. Continuing research will
determine its role in diagnosis. Increasing knowledge of the complex mechanisms involved in lung inflammation/
repair, will lead to the identification of more precise turning points in the repair stages, as well as description of precise
molecular inflammatory patterns and their variations depending on stage and disease. In cases of acute respiratory
failure or chronic lung diseases in which diagnosis is unclear, in vivo microimaging might prove to be a new
indispensible tool, especially in patients whose condition precludes more invasive procedures. In patients with clear
diagnosis, in vivo microimaging might be used as a prognostic indicator and as a guide in the timing of treatment
initiation. For example, the use of corticosteroids is ARDS has been the subject of debate, with large studies showing no
clear benefit [25]. Corticosteroids might still be useful in certain subsets of patients and in vivo imaging may aid in
identifying them. A similar example of a chronic disease would be in the case of idiopathic pulmonary fibrosis.
Identification of specific inflammatory patterns and lung repair stages could also guide the use of future treatment
options such as biologicals and other immunomodulators. Better evaluation of tissue repair may help the physician
decide which treatment to use, when to initiate and when to cease or modify it.
The study of lung repair shows great potential benefit in aiding patients stricken with acute and chronic lung
diseases. It is in the interest of these patients that research involving in vivo microimaging of the lung be pursued.
References
[1] H. Brown, C.G. Irvin, G.B. Allen, III, S.D. Shapiro, W.J. Martin, M R. J. Kolb, D.M. Hyde, G.F. Nieman, D.D. Cody, M. Ishii,
S.J. Kadlecek, B. Driehuys, R.R. Rizi, A.M. Wu, W.A. Weber, D.B. Stout on behalf of the ATS Small Animal Imaging
Subcommittee: An official ATS conference proceedings: advances in small-animal imaging application to lung
pathophysiology. Proc Am Thorac Soc Vol. 5 (2008) pp. 591-600.
[2] D.H. Ingbar: Mechanisms of repair and remodeling following acute lung injury. Clin Chest Med Vol. 21(2000) pp. 589-616.
[3] M.S. Razzaque, T. Taguchi: Pulmonary fibrosis: cellular and molecular events. Pathol Int Vol. 53 (2003) pp. 133-45.
[4] D.W. Shimabukuro, T. Sawa, M.A. Gropper: Injury and repair in lung and airways. Crit Care Med Vol. 31(2003)(Suppl) pp.
S524-31.
[5] B.D. Uhal: Apoptosis in lung fibrosis and repair. Chest Vol. 122 (2002)(Suppl): pp. 293S-298S.
[6] X. Li, R Shu, G Filippatos, BD Uhal: Apoptosis in lung injury and remodeling. J Appl Physiol Vol. 97 (2004) pp. 1535-42.
[7] O. Lesur, A. Kokis, C. Hermans, T. Fülöp, A. Bernard, D. Lane: IL-2 involvement in early ARDS: relationship with
polymorphonuclear neutrophil apoptosis and patient survival. Crit Care Med Vol.28 (2000) pp. 3814-3822.
[8] G. Matute-Bello, W.C. Liles, F. 2nd Radella, K.P. Steinberg, J.T. Ruzinski, L.D. Hudson, T.R. Martin: Modulation of neutrophil
apoptosis by granulocyte colony-stimulating factor and granulocyte/macrophage colony-stimulating factor during the course of
acute respiratory distress syndrome. Crit Care Med Vol. 28 (2000) pp. 1-7.
[9] A.N. Rubinowitz, M.D. Siegel, I. Tocino: Thoracic imaging in the ICU. Crit Care Clin Vol. 23 (2007) pp. 539-73.
[10] J.R. Hill, P.E. Horner, S.L. Primack: ICU imaging. Clin Chest Med Vol. 29 (2008) pp. 59-76, vi.
[11] T. Johkoh: Imaging of idiopathic interstitial pneumonias. Clin Chest Med Vol. 29 (2008) pp. 133-47, vi.
[12] K-C. Kao, Y-H. Tsai, Y-K. Wu, N-H. Chen, M-J. Hsieh, S-F. Huang, C-C. Huang: Open lung biopsy in early-stage acute
respiratory distress syndrome. Crit Care.Vol. 10 (2006) pp. R106.
[13] S.Y. Lim, G.Y. Suh, J.C. Choi, W.J. Koh, S.Y. Lim, J. Han, K.S.Lee, Y.M. Shim, M.P. Chung, H. Kim, O.J. Kwon: Usefulness
of open lung biopsy in mechanically ventilated patients with undiagnosed diffuse pulmonary infiltrates: influence of
comorbidities and organ dysfunction. Crit Care Vol. 11 (2007) pp. R93.
[14] L. Papazian, C. Doddoli, B. Chetaille, Y. Gernez, X. Thirion, A. Roch, Y. Donati, M. Bonnety, C. Zandotti, P. Thomas: A
contributive result of open-lung biopsy improves survival in acute respiratory distress syndrome patients. Crit Care Med.Vol.
35 (2007) pp. 755-62.
[15] E.J. van Beek, E.A. Hoffman: Functional imaging: CT and MRI. Clinics in Chest Med Vol. 29 (2008): pp. 195-216.
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
©FORMATEX 2010 639
______________________________________________

[16] M. Eichinger, R. Tetzlaff, M. Puderbach, N. Woddhouse, H.U. Kauczor: Proton magnetic resonance imaging for assessment of
lung function and respiratory dynamics. Eur J of Radiol Vol. 64 (2007) pp. 329-334.
[17] S.R. Hopkins, D.R. Levin, K. Emami, S. Kadlecek, J. Yu, M. Ishii, R.R. Rizi: Advances in magnetic resonance imaging of lung
physiology. J of Appl Physiol Vol. 102 (2007) pp. 1244-1254.
[18] J. Petersson, A. Sanchez-Crespo, S.A. Larsson, M. Mure: Physiological imaging of the lung: single-photon-emission computed
tomography (SPECT). J of Appl Physiol Vol. 102 (2007) pp. 468-476.
[19] R.S. Harris, D.P. Schuster: Visualizing lung function with positron emission tomography. J of Appl Physiol Vol. 102 (2007) pp.
448-458.
[20] L. Gargani, V. Lionetti, C. Di Cristofano, G. Bevilacqua, F.A. Recchia, E. Picano: Early detection of acute lung injury
uncoupled to hypoxemia in pigs using ultrasound lung comets. Crit Care Med Vol. 35 (2007) pp. 2769-2774.
[21] T.A. D'Amico, T.A.Aloia, M-B.H. Moore, D.H. Conlon, J.E. Harpole Jr: Predicting the sites of metastases from lung cancer
using molecular biologic markers. Annals of Thoracic Surgery Vol. 72 (2001) pp. 1144-1148.
[22] A. Perchant, G. Le Goualher, M. Genet, B. Viellerobe, F. Berier: An integrated fibered confocal microscopy system for in vivo
and in situ fluorescence imaging - applications to endoscopy in small animal imaging, in Biomedical Imaging: Nano to Macro,
2004. IEEE International Symposium Vol. 1 (2004) pp. 692-695.
[23] L. Thiberville, S. Moreno-Swirc, T. Vercauteren, E. Peltier, C. Cavé, G. Bourg Heckly: In vivo imaging of the bronchial wall
microstructure using fibered confocal fluorescence microscopy. Am J Respir Crit Care Med Vol.175 (2007) pp. 22-31.
[24] W.M. Kuebler, K. Parthasarathi, J. Lindert, J. Bhattachrya: Real-time lung microscopy. J of Appl Physiol Vol. 102 (2007) pp.
1255-1264.
[25] K.P. Steinberg, L.D. Hudson, R.B. Goodman, C.L. Hough, P.N. Lanken, R. Hyzy, B.T. Thompson, M. Ancukiewicz National
Heart, Lung and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network: Efficacy and safety of
corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med Vol. 354 (2006) pp. 1671-84.
[26] L. Thiberville, M. Salaün, S. Lachkar, S. Dominique, S. Moreno-Swirc, C. Vever-Bizet, G. Bourg Heckly: Human in vivo
fluorescence microimaging of the alveolar ducts and sacs during bronchoscopy. Eur Respir J Vol. 33 (2009) pp. 974-85.
[27] F. Chagnon, C. Fournier, P.G. Charette, L. Moleski, D.M. Payet, L.G. Dobbs, O. Lesur. Pulmonary In vivo intravital fibered-
bundle fluorescence microscopy: travelling abyssal zones of normal lung and acute lung injury. Lab Invest (2010) Apr 12.
[Epub ahead of print]
Microscopy: Science, Technology, Applications and Education A. Méndez-Vilas and J. Díaz (Eds.)
640 ©FORMATEX 2010
______________________________________________