total ankle arthroplasty - coa · anatomy and biomechanics of the ankle joint ... revision rate...
TRANSCRIPT

Total Ankle Arthroplasty
David Thordarson, MD Professor, Division of
Orthopedics Cedars Sinai Medical Center

Disclosures
I have none relevant for this talk All should be listed in the program

Background First attempted in the early 1970s Abandonment of first and second generation total
ankle replacements (TAR) due to unacceptably high complication and failure
Early designs struggled to find balance between constraints and stability

Introduction Ankle has one third the surface area of the knee, yet
carries almost twice the load of the knee. TAR can be used to treat post-traumatic, idiopathic
(primary), and rheumatoid arthritis. TARs has been performed in selected patients with
arthritis since the 1970s as an alternative to arthrodesis with mixed results.
Recently, increasing patient demand due to improved outcomes and desire to maintain normal joint ROM.
Almost all current TARs have two common features: porous coated for bone ingrowth and made of a titanium alloy with a cobalt chrome–polyethylene articulation.

Problems of Total Ankle Replacement

Background 1st Generation of implants
Two part systems Polyethylene part was placed in
the tibia and the metal part in the talus or sometimes the arrangement was reversed
Highly constrained Cemented components that
required significant bony resection for implantation
Although stable, designs loosened, subsided and caused osteolysis

Background 2nd Generation of implants
Agility ankle prosthesis (semi-constrained, two part prosthesis)
Required less bone resection and avoided cement fixation
Less constraint reduced the shear forces and torsion at the bone-prosthesis interface
Increases polyethylene wear and failure and compromised stability
Failures due to painful impingements, subluxation or complete dislocation

Anatomy and Biomechanics of the Ankle Joint The bony anatomy, ligaments, and joint capsule guide and
restrain movement between the talus and the mortise Talus has a continuously changing axis of rotation as it moves
from maximum dorsiflexion to maximum plantar flexion relative to the mortise.
The talus and mortise widen slightly from posterior to anterior. When the talus is plantarflexed, its narrowest portion sits in the
ankle mortise and allows rotatory movement between the talus and mortise.
When the talus is maximally dorsiflexed, the tibiofibular syndesmosis spreads, and the wider portion of the talar articular surface locks into the ankle mortise, allowing little or no rotation between the talus and the mortise.

Patient Selection and Evaluation Ideal patient is still up for debate Older, thin, low demand individual with minimal
deformity may be considered the optimal candidates for TAR
Chronological age and body weight as independent threshold remains controversial

Patient Selection and Evaluation
Expanded indication • Ipsilateral arthritis • Inflammatory or osteoarthritis of multiple, adjacent
joints • Arthrodesis of hindfoot and/or contralateral
arthrodesis of the ankle

Patient Selection and Evaluation
Absolute contraindication • Active infection • Extensive avascular necrosis of talar dome • Compromised bone stock or soft tissue • Peripheral neuropathy • Peripheral vascular disease • Charcot neuroarthropathy

Patient Selection and Evaluation
Relative contraindications • Remote history of infection • Ligamentous instability • Subluxation of talus • Presence of severe deformities above or beneath the ankle • Absence of the medial and/or lateral malleoli; • Poor skin condition secondary to surgical scars or trauma.

Modern TAR Designs Three component
• A metallic baseplate fixed to the tibia • A domed or condylar shaped metallic component that
resurfaces the talus • Bearing surface made of ultra-high molecular weight
polyethylene interposed between tibial and talar components
• Only one FDA approved 3 component design in US but essentially all in Europe

Modern TAR Designs Two-piece designs (fixed bearing systems) lock the
polyethylene component into the baseplate Mobile or meniscal bearing systems do not attach
the polyethylene to either component Both systems use similar semi-constrained design Increased conformity between the bearing surface
and the talar component in sagittal plane while permitting more motion in the transverse and axial planes.

Modern TAR Designs The reduction in the shear and torsional forces at
the bone-implant interface is an accepted advantage of the three piece design
Insufficient data exist to offer recommendation regarding the choice of fixed or mobile-bearing design for modern TAR
Recent study suggested that 3 component design allowed for mild inaccuracies in implantation alignment but really did not move after implantation

Modern TAR Designs Four 2 component designs approved by FDA
• Agility Total Ankle System (Depuy Orthopaedics) • Salto Talaris Anatomic Ankle Prosthesis (Tornier) • Inbone Total Ankle System (Inbone Technologies) • Eclipse Total Ankle Implant (Kinetikos) • Zimmer Total Ankle Replacement
Single 3 component design approved STAR(Scandinvian Total Ankle Replacement System)

Agility Total Ankle System Approved in the US for
approx 20 years Semi-constrained fixed
bearing prosthesis An ultra-high molecular
weight polyethylene bearing surface locks into a titanium tibial component
Both components utilize a beaded surface to achieve fixation through bony ingrowth

Agility Total Ankle System
Requires arthrodesis of the distal syndesmosis Application of an external fixator for distraction of the
joint during implantation Large resection of the bone from the tibia for
implantation approx 2.6 cm

Agility Total Ankle System Result from one study (cohort) including 100 arthroplasties
between 1984 to 1994 performed by a single surgeron • 90% reported decreased pain and satisfaction with the outcome of
the surgery • 83% reported functional improvement • 11% required major revision (one half received another
arthroplasty and the other half underwent arthodesis) • 76% of surviving arthroplasties demonstrated lucency around
implants • Majority of these were either focal, stable mechanical lysis along
interface between fibula and tibial component

Agility Total Ankle System
Reports from 400 cases yields consistently high rates of satisfaction and pain relief
Survival of implants and a good functional outcome appear to depend on patient age
Nonunion of the syndesmosis fusion and specific specific patterns of progressive lucency around the implants may herald subsidence and migration of the components and failure of the arthoplasty

Salto Talaris Anatomic Ankle Prosthesis
Semi-constrained, fixed bearing 3 universal tibial base sizes and 4 talar
component sizes, wider anteriorly for better bone coverage
Two distinct radii of curvature, medially and laterally, avoid overstressing the deltoid ligaments
Based upon anatomy, the flexion/extension axis is the axis of a cone to allow normal external rotation of the foot during dorsiflexion
Stability is provided by a hollow fixation plug and three bone cuts (anterior, posterior, lateral) to resurface the talus with minimal bone removal
Salto Talaris Anatomic Ankle Prosthesis
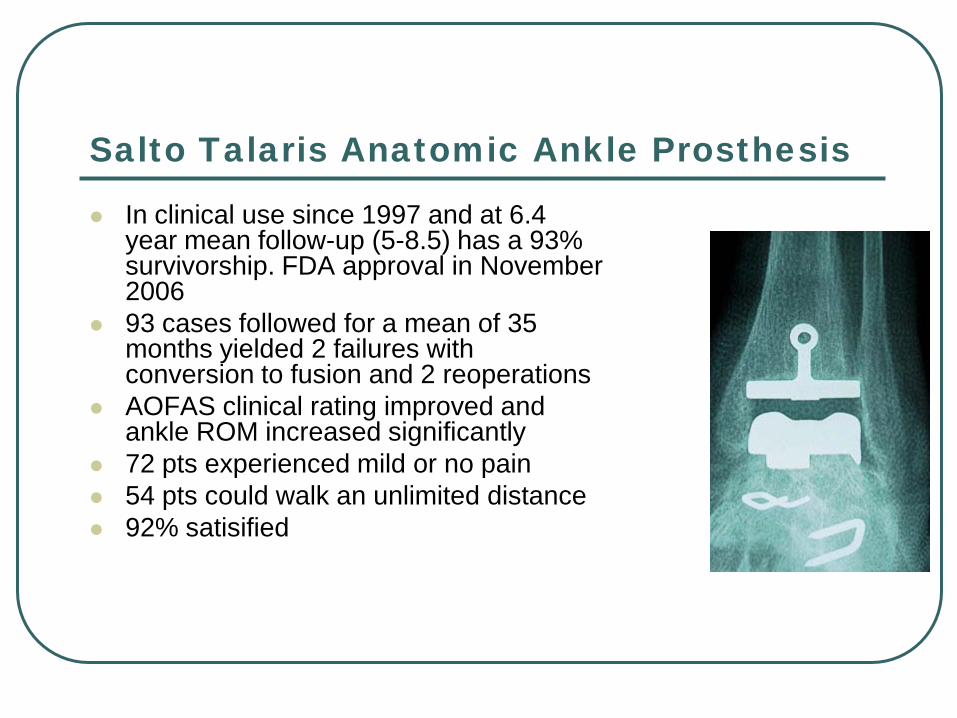
In clinical use since 1997 and at 6.4 year mean follow-up (5-8.5) has a 93% survivorship. FDA approval in November 2006
93 cases followed for a mean of 35 months yielded 2 failures with conversion to fusion and 2 reoperations
AOFAS clinical rating improved and ankle ROM increased significantly
72 pts experienced mild or no pain 54 pts could walk an unlimited distance 92% satisified

Inbone Total Ankle System
FDA approved in 2005 Utilizes an intramedullary
guide for osseous cuts System is modular, allowing
mismatch between the talar and tibial components
System employs an ultra-high molecular weight polyethylene bearing slotted into a modular coated, stemmed tibial component

First one June 2007-RA with triple

Postop- Very happy at 22months

Eclipse Total Ankle Implant
Use of medial or lateral malleolar osteotomy The designers contend that this feature aviods the
anterior angiosome of the ankle and allows for easier bony resections keep the components congruent with the load bearing surface

New Zimmer TAR
1st prosthesis to be implanted via lateral malleolar osteotomy to allow for less bone resection introduced 2013 AAOS meeting

Scandinvian Total Ankle Replacement System (STAR)
Semi-constrained prosthesis with cobalt-chrome-molybdenum components and an ultra-high molecular weight polyethylene mobile bearing
A porous plasma spray coating of hydroxyapatite applied to the nonbearing surface of the components facilitates bony ingrowth

72 yo female who refused ankle fusion with early TN DJD

2 year postop films

Arthroplasty versus Arthrodesis
Arthrodesis • Gold standard for relieving pain and restoring
function in individuals with symptomatic arthrosis, deformity or severe instability of the tibiotalar joint
• Multiple studies have documented its efficacy in long term pain relief
• Maintain approx. 1/3 sagittal plane motion after fusion

Arthroplasty versus Arthrodesis
• Disadvantages of ankle fusion • Onset of arthrosis of joints adjacent to the fusion
approx 20 years later • Alterations in gait • The limb with the arthrodesis also has higher
incidence of pain, disability and activity limitation • In one study, cadence and stride length were
significantly decreased

Arthroplasty versus Arthrodesis No studies exist that currently compare participation
in sporting activities following these two procedures However, one study compared activity level before
and after 147 TAR • After mean of 2.8 years follow up the percentage of patients
actively participating in sports increased from 36% to 56% • Pts who were active in sports after TAR demonstrated
higher AOFAS scores than those that were sedentary

How Successful are Current Ankle Replacements? A Systematic Review of the Literature Nikolaos Gougoulias MD, PhD, Anil Khanna MD, Nicola Maffulli MD, PhD; Clin Orthop Relat Res (2010) 468:199–208
13 level IV studies, 1105 TAR 234 AgilityTM, 344 STAR, 153 Buechel-Pappas, 152
HINTEGRA, 98 Salto, 70 TNK, 54 Mobility Overall failure 10% at 5 years (range 0-32%) Current through Oct 2008 Current study Level IV since only a review of Level
IV studies-despite being well done can’t make Chicken salad out of it

How Successful are Current Ankle Replacements? A Systematic Review of the Literature Nikolaos Gougoulias MD, PhD, Anil Khanna MD, Nicola Maffulli MD, PhD; Clin Orthop Relat Res (2010) 468:199–208
Residual pain was common (range, 27%–60%) Superficial wound complications in 0% to 14.7% Deep infections in 0% to 4.6% of ankles Ankle function consistently improved after total ankle
arthroplasty

Intermediate and Long-Term Outcomes of Total Ankle Arthroplasty and Ankle Arthrodesis A Systematic Review of the Literature S.Haddad, J.C. Coetzee, et al. J Bone Joint Surg Am. 2007;89:1899-905
10 TAR (852 pts), 39 fusion (1262 pts) studies through 2005 included
Five-year implant survival rate was 78% (95% confidence interval, 69.0% to 87.6%) and the ten-year survival rate was 77% (95% confidence interval, 63.3% to 90.8%)
Revision rate following total ankle arthroplasty was 7% (95% confidence interval, 3.5% to 10.9%) with the primary reason for the revisions being loosening and/or subsidence

Intermediate and Long-Term Outcomes of Total Ankle Arthroplasty and Ankle Arthrodesis A Systematic Review of the Literature S.Haddad, J.C. Coetzee, et al. J Bone Joint Surg Am. 2007;89:1899-905 Mean AOFAS Ankle-Hindfoot Scale score was 78.2
points for TAR and 75.6 points for arthrodesis Meta-analytic mean 38% TAR had an excellent
result, 30.5% had a good result, 5.5% had a fair result, and 24% had a poor result
Arthrodesis group, corresponding values were 31%, 37%, 13%, and 13%
Intermediate outcome of TAR appears to be similar to ankle arthrodesis
Level IV study due to quality of studies reviewed-better than previous study

Long-Term Results Following Ankle Arthrodesis for Post-Traumatic Arthritis L COESTER, C. SALTZMAN,et al. J BONE JOINT SURG 83-A (2): 219-228,2001
23 pts avg F/U 22 yrs (range12-44 ) DJD ipsilateral subtalar (p < 0.0001), TN(p <
0.0001), CC (p <0.0001), NC (p = 0.0012), TMT(p = 0.0009), and 1st MTP (p = 0.0012) more severe than contralateral side. Osteoarthritis did not develop more frequently in the
ipsilateral knee or lesser MTP Level of Evidence IV as it was a retrospective case
series but with excellent follow up

Long-Term Results Following Ankle Arthrodesis for Post-Traumatic Arthritis L COESTER, C. SALTZMAN,et al. J BONE JOINT SURG 83-A (2): 219-228,2001
Significant differences between the two sides were found with regard to overall activity limitation (p < 0.0001), pain (p < 0.0001), and disability (p < 0.0001), with the involved side consistently more symptomatic
16 (67%) were happy with the overall outcome 21 (88%) would have the ankle arthrodesis again Although ankle arthrodesis may provide good early
relief of pain, it is associated with premature deterioration of other joints of the foot and eventual arthritis, pain, and dysfunction.

Surgeon randomized IDE trial since FDA felt 3 component TAR not equivalent to previous 2 component approved designs
606 STAR, 66 fusion 24 mo min F/U 57.9 vs 44.6 point pain VAS improvement TAR vs
fusion If success defined as 40 point BP score increase
then STAR much more effective than fusion Study data lead to FDA approval Level of Evidence II Prospective Comparative Case
Controlled Study
Charles L. Saltzman, Roger A. Mann, et al Prospective Controlled Trial of STAR Total Ankle Replacement versus Ankle Fusion: Initial Results Foot Ankle Int 2009 30: 579-596

Comparison of Reoperation Rates Following Ankle Arthrodesis and Total Ankle Arthroplasty; N SooHoo, D Zingmond, C Ko; J Bone Joint Surg Am. 2007;89:2143-9
Calif hospital discharge database 1994-2005 4705 fusion, 480 TAR Rates of major revision surgery after ankle
replacement were 9% at 1 year and 23% at 5 years compared with 5% and 11% following ankle arthrodesis
Ankle arthrodesis had a higher rate of subtalar fusion at five years postoperatively (2.8%) than did those treated with ankle replacement (0.7%)
Level of Evidence III Retrospective Case Series

Ankle Replacement versus Arthrodesis: A Comparative Gait Analysis Study P Piriou, P Culpan, et al; Foot Ankle Int Vol. 29 (1) 2008:3-9
12 pts; min 2 year F/U Ankle arthrodesis faster gait with greater
asymmetry TAR had greater movement at the ankle,
symmetrical timing of gait and restored ground reaction force pattern
Overall more normal gait in TAR group Level of Evidence III Therapeutic

Hahn, ME; Wright, ES; Segal, AD, et al.: Comparative gait analysis of ankle arthrodesis and arthroplasty: initial findings of a prospective study. Foot Ankle Int. 2012;(33): 282-289.
19 pts, 9 Salto Talaris, 9 ankle arthrodesis Nonsignificant improved temporal-spatial
measurements Fusion pts had greater hip ROM Salto pts had greater ankle and knee ROM Both groups had less pain Level of Evidence III Comparative Case Series

What can go wrong?

Postop TAR impinging/malposition

bone prosthetic interface/medial translation



50 yo male told he would be playing
basketball 4 months postop now 1 year
out with chronic pain

Loose talar component salvaged with fusion

83 yo female with DM now 18 months postop with draining fistula, refuses BKA with vascular calcifications

3 months postop

Preop isolated ankle DJD does not want fusion

Talar cut too low-did well for 6 months

6 months postop talar fracture

Revised with long stem talar component

Failed again, then got infected salvaged with PMMA Abx spacer

Failed TAR with fx both malleoli

Salvaged with TC fusion

PRE-OP RA, 65 yo with previous triple arthrodesis-perfect candidate for TAR

POST-OP Vertical split of medial malleolus needed intraop ORIF with buttress plate

POST-OP
40 yo with stiff hindfoot was considering BKA but wanted to try TAR

POST-OP

6 weeks postop with exposed tib. Ant. tendon

“Rotational” retinacular flap to cover tendon

Fortunately healed

Personal Preference
Single joint involvement offer/encourage ankle fusion
Bilateral ankle DJD, preexisting hindfoot fusion/DJD encourage consideration for TAR
Economically not very viable currently as cost of prosthesis exceeds $10,000 to hospital which is more than Medicare reimbursement for whole procedure to hospital

Conclusion
Ankle fusion more predictable Definite role for TAR TAR will never have same role as knee
or hip replacements as 1/10 the incidence of symptomatic ankle DJD and knee and hip fusions function much more poorly than replacement