topic 2 toxicology prof aa - · pdf filetopic 2 toxicology prof aa 1. ... route of entry for...
TRANSCRIPT
Topic 2
Toxicology
Prof AA
1
Toxicology & Industrial Hygiene
Toxicology
– A qualitative and quantitative study of the adverse
effects of toxicants on biological organism.
Industrial Hygiene
– Industrial hygiene is the science of anticipating, recognizing, evaluating, and controlling workplace conditions that may cause workers' injury or illness.
Definition
Toxicology
The way toxicants enter biological
organism
The way toxicants are eliminated from
biological organism
The effect of toxicants on biological
organism
Fundamental Principle of
Toxicology
There are no harmless substance,
only harmless ways of using
substances
Toxicants
A chemical agents
A physical (dusts, fibers, noise, and radiation) agents, e.g. asbestos
Toxicity is a property of toxicant that describe its effect on biological organism.
Toxic hazards is the likelihood of damage to biological organism based on exposure resulting from the use/transport/storage of the toxicants (property of hazardous material).
7
Toxic Effect can be classified
according to:
Reversible Vs Irreviersible
Acute Vs Chronic (Duration of Exposure)
Local (Sk-dermal) Vs Systemic (Sk-systemic) (Location of the effect)
Reversible/Irreversible
Irreversible– Carcinogen-cause cancer
– Mutagen-cause chromosome (gene) damage
– Teratogen- cause birth defects
May or may not be irreversible– Dermatotoxic – affects skin
– Hemotoxic – affects blood
– Hepatotoxic- affects liver
– Nephrotoxic – affects kidneys
– Neutotoxic – affects nervous system
– Pulmonotoxic- affects lungs
9
Acute / Chronic
Acute exposure
– High Dosage (e.g. due to accidental release)
– The effect is immediate
Chronic Exposure
– Normally lower dose
– The effect only noticed/detected following long exposure
– Sometimes, the worker could not recall the exposure.
Local/Systemic
Local
Damage to the part of the body that comes in contact with the substance.
Systemic
Chemical is absorbed by the body and attacks a target organ.
11
Source of Toxicants
Toxic Release (emissions, rupture etc)
– Vapour/gas/liquid release from source
Fire and Explosion
– Fire and radiation
– Toxic release following fire/explosion (as products
of fire & explosion)
Route of Entry
Route of Entry
Injection: through cuts or hypodermic needles into the skin, usually cause highest blood level concentration.
Inhalation: through mouth/nose into the lungs (respiratory system), 2nd highest blood level concentration.
Ingestion: through mouth into stomach and gastrointestinal tract, 2nd lowest in blood level concentration.
Dermal (Skin) absorption: through skin membrane, lowest in blood level concentration, note: absorption of phenol could result in death
14
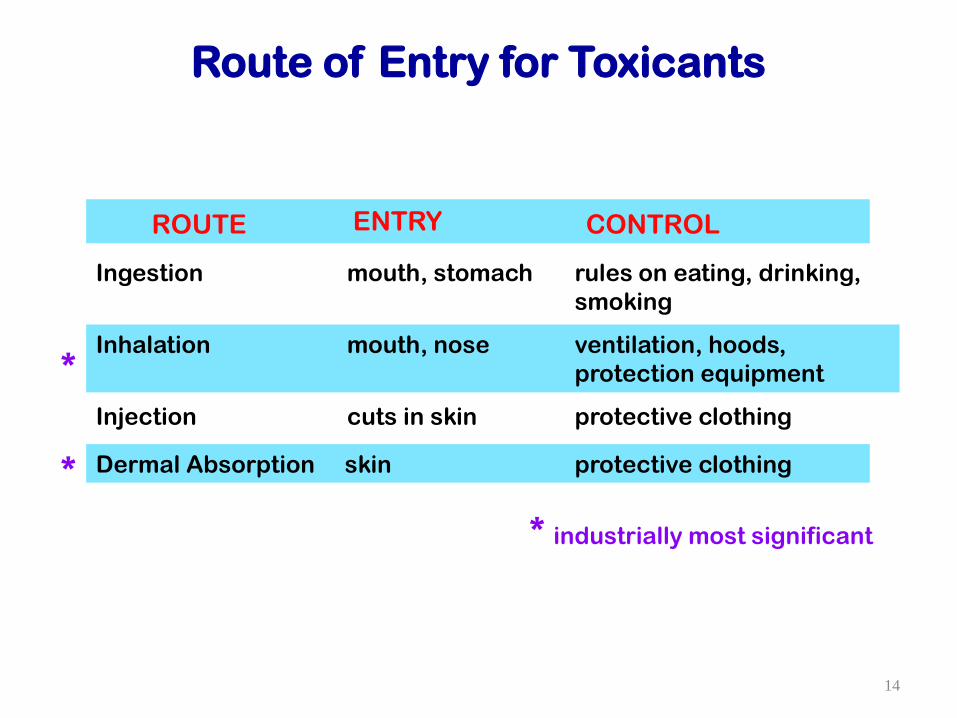
Inhalation mouth, nose ventilation, hoods,
protection equipment
Injection cuts in skin protective clothing
Dermal Absorption skin protective clothing
Ingestion mouth, stomach rules on eating, drinking,
smoking
ROUTE ENTRY CONTROL
*
*
* industrially most significant
Route of Entry for Toxicants
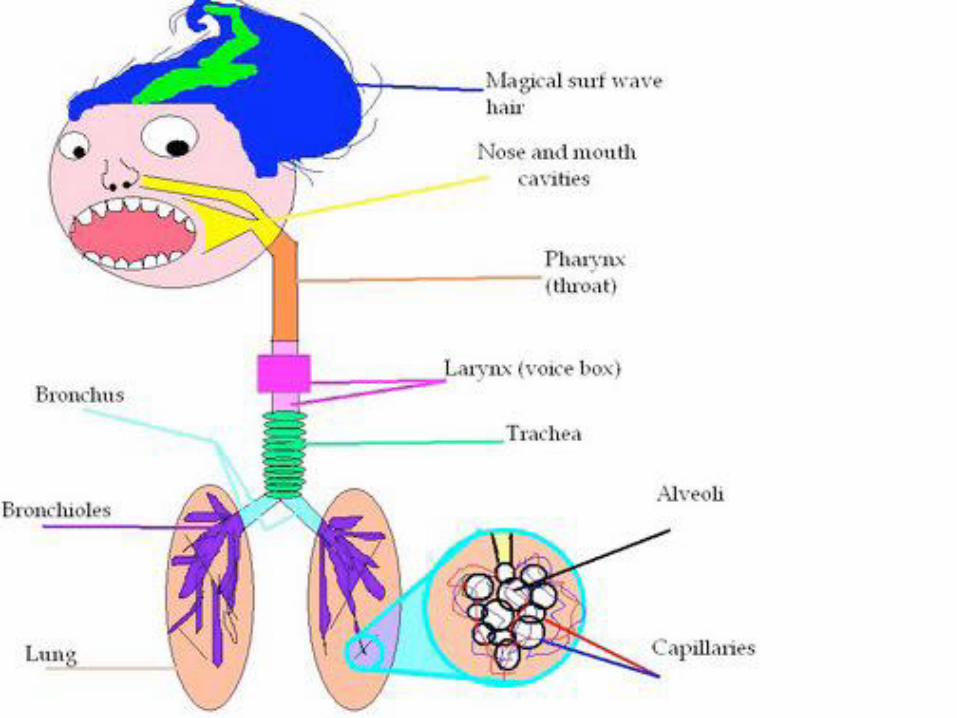
RESPIRATORY SYSTEM
Upper respiratory
– Nose, sinuses, mouth, pharynx, larynx and tracea
– Filtering, heating, and humidifying the air
– Affected by toxicants that are soluble in water
– These toxicants will react or dissolve in the mucus to form acids or bases
– E.g. hydrogen halides, oxides, hydroxides, sodium dusts
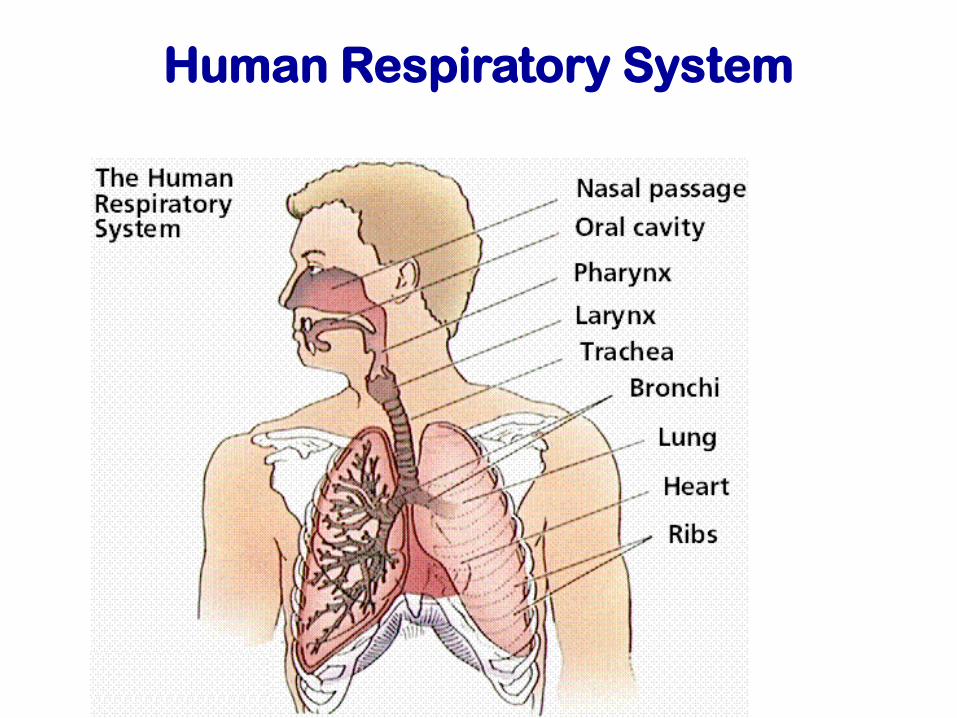
Human Respiratory System

Respiratory System: Lower Respiratory
System
Lungs (bronchial tubes and alveoli for gas exchange with blood)
Toxicants affect the function of alveoli by blocking the transfer of gases or by reaction with alveoli wall to produce corrosive/toxic substances.
E.g. monomers (acrylonitrile), halides (Chlorine),hydrogen sulfide, methyl cynaide etc
Respiratory System
Effect of dust and insoluble materials
– The smaller the dust particles, the farther it
penetrate into respiratory system
– Particles >5 μ m are filtered in the upper respiratory
system.
– 5μm>Particles>2 μm can reach bronchial system
– Particles<1 μm can reach the alveoli
How toxicant are eliminated from
biological organism
Excretion- through kidneys (blood to urine), liver (selectively excrete certain chemicals indigestive tract to bile), lungs , skin (sweats), hair, nail or other organ
Detoxification-change the chemical into something less harmful by biotransformation through liver, can also occur in blood, intestinal wall, skin, kidney
Storage- in fatty tissue. Can create problem when fatty deposits are metabolized and released the toxic (e.g. during reduced food supply). Also store in bone, blood, liver, and kidney.
Massive exposure to hazardous chemical can damage majororgans (kidney, lung, liver), reduces their ability to excrete.
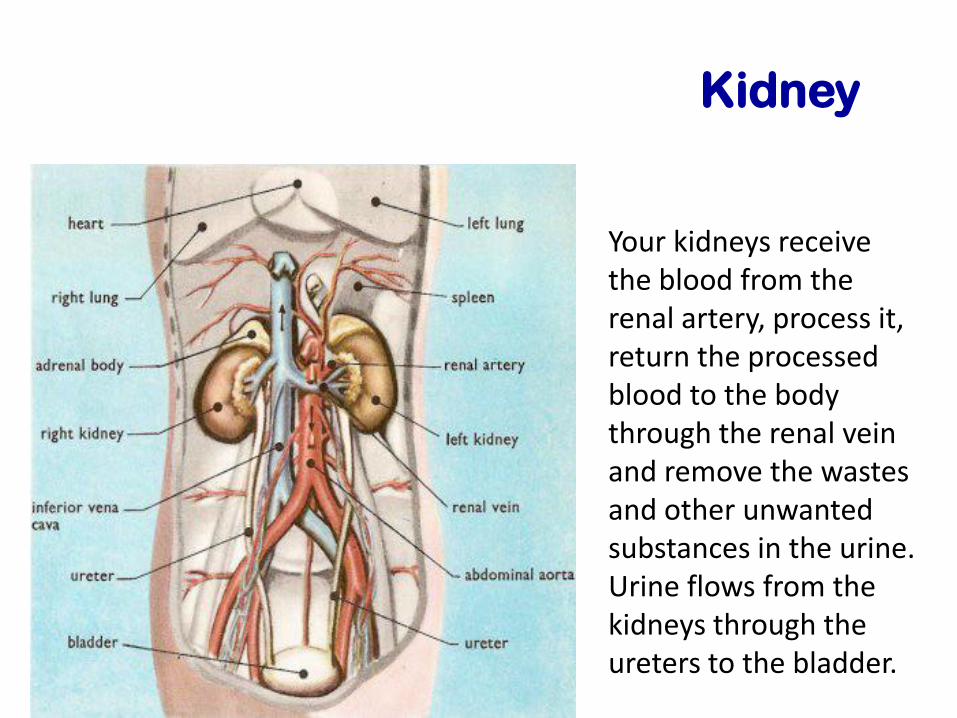
Kidney
Your kidneys receive the blood from the renal artery, process it, return the processed blood to the body through the renal vein and remove the wastes and other unwanted substances in the urine. Urine flows from the kidneys through the ureters to the bladder.
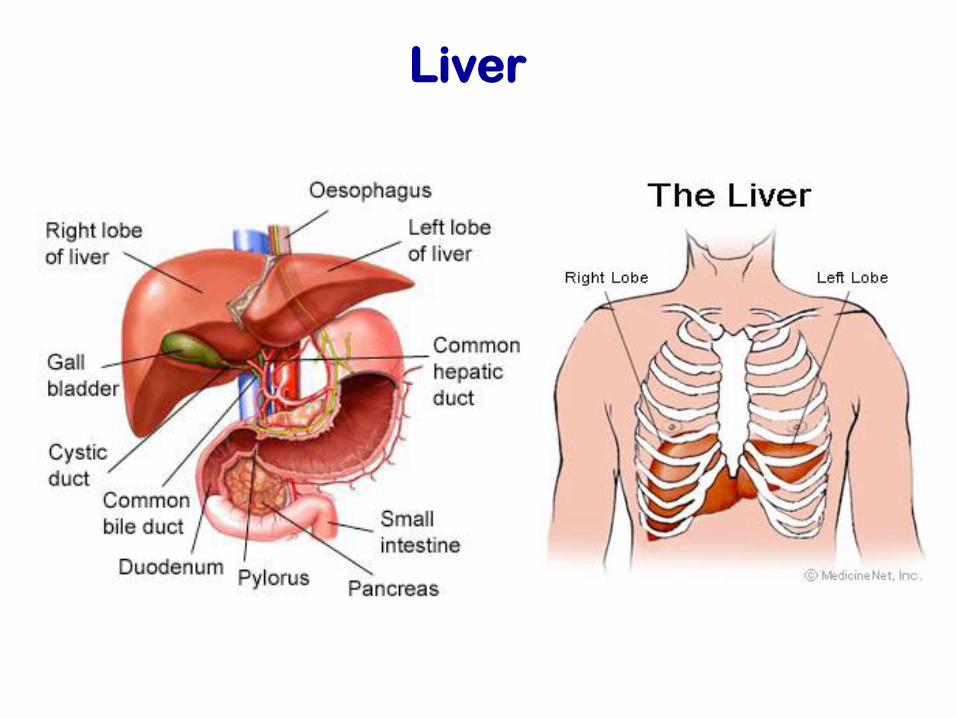
Liver
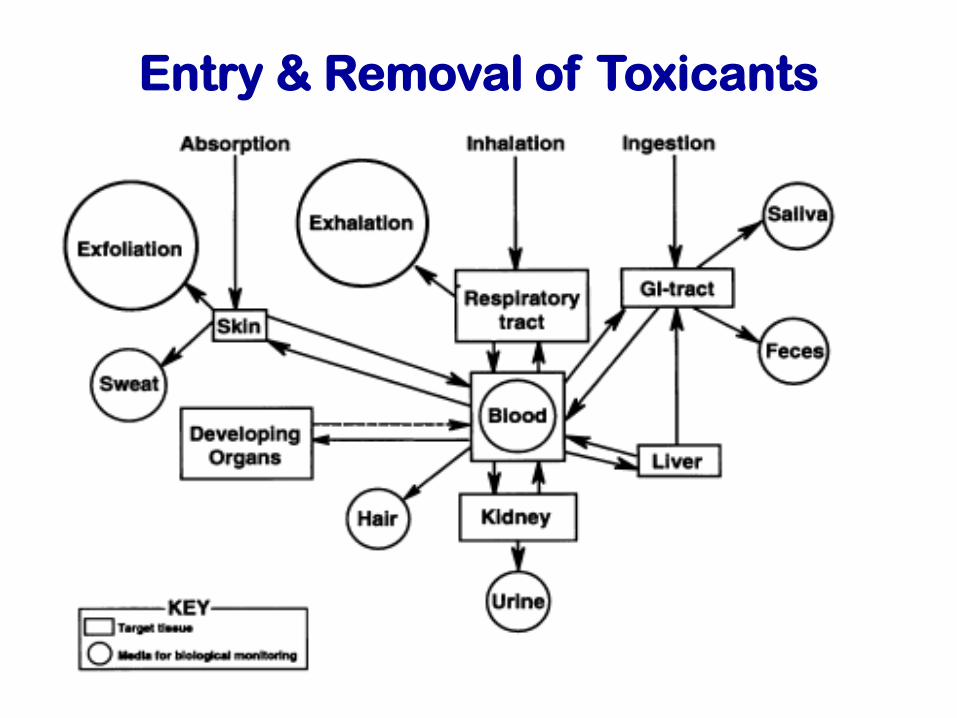
Entry & Removal of Toxicants

Dose-Response
Relationships
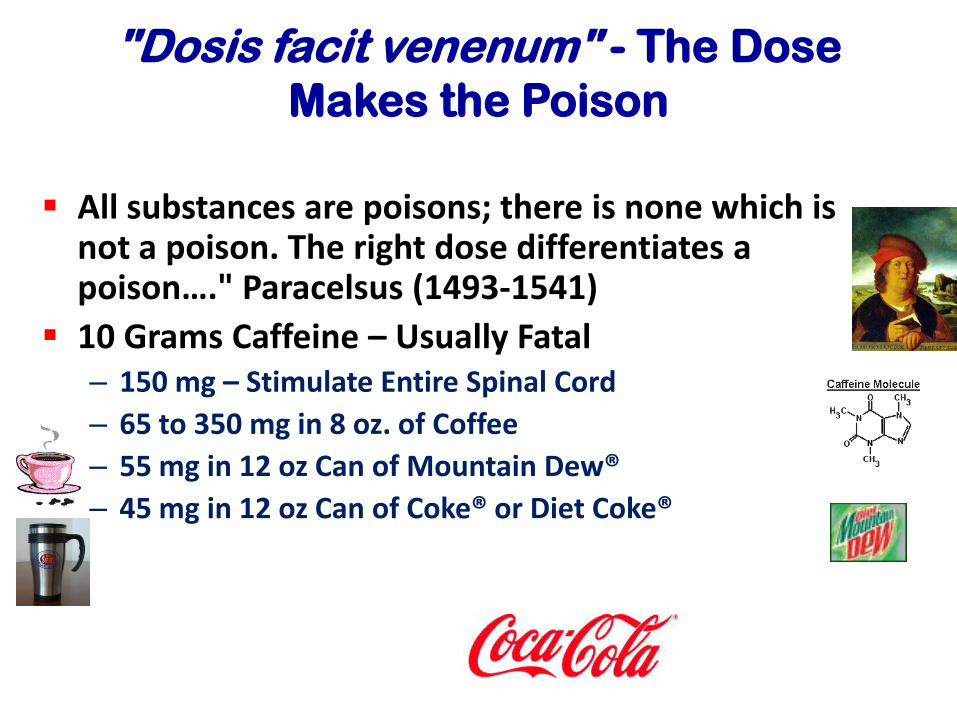
"Dosis facit venenum" - The Dose
Makes the Poison
All substances are poisons; there is none which is not a poison. The right dose differentiates a poison…." Paracelsus (1493-1541)
10 Grams Caffeine – Usually Fatal– 150 mg – Stimulate Entire Spinal Cord
– 65 to 350 mg in 8 oz. of Coffee
– 55 mg in 12 oz Can of Mountain Dew®
– 45 mg in 12 oz Can of Coke® or Diet Coke®
Key Factors Related to Dose
Response
The dose-response curve may differ for different populations.
Individuals vary with regard to response to drugs or toxins.
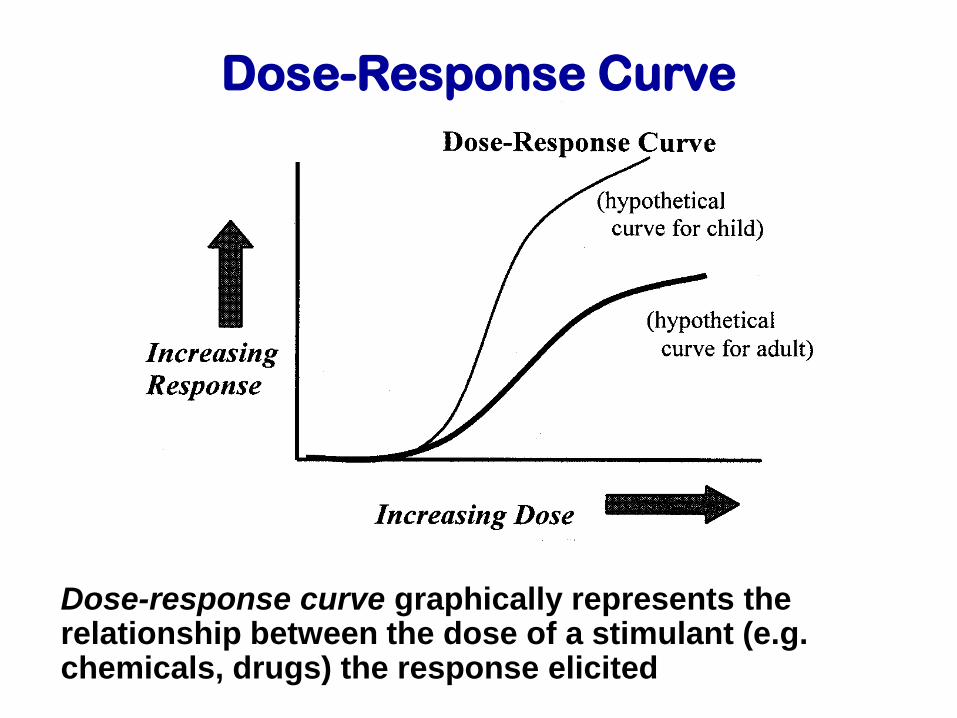
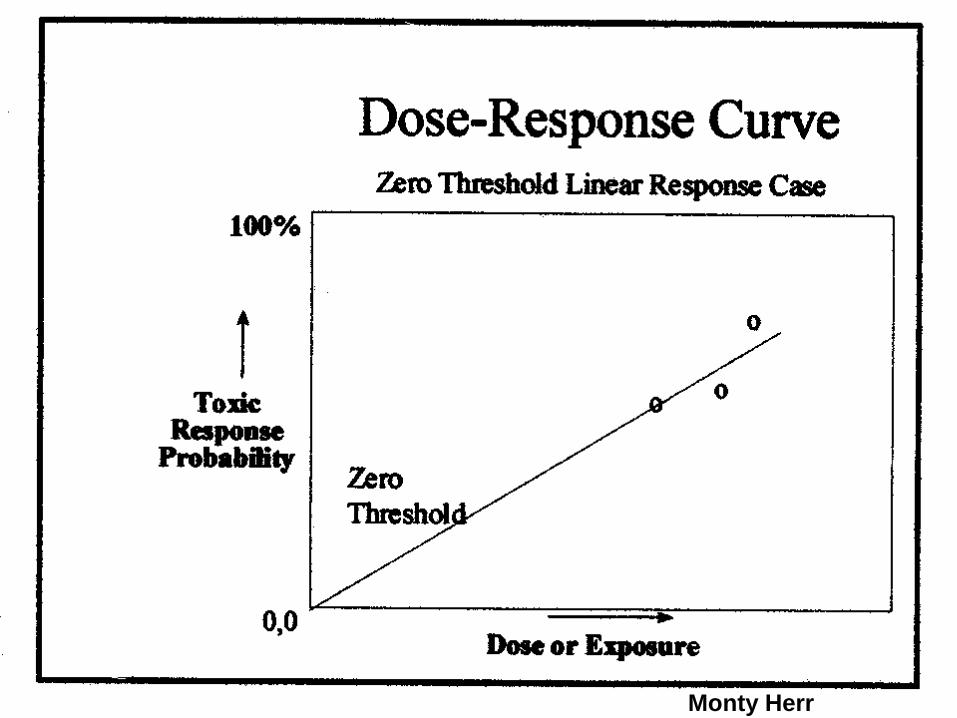
Dose-Response Curve
Dose-response curve graphically represents the relationship between the dose of a stimulant (e.g. chemicals, drugs) the response elicited
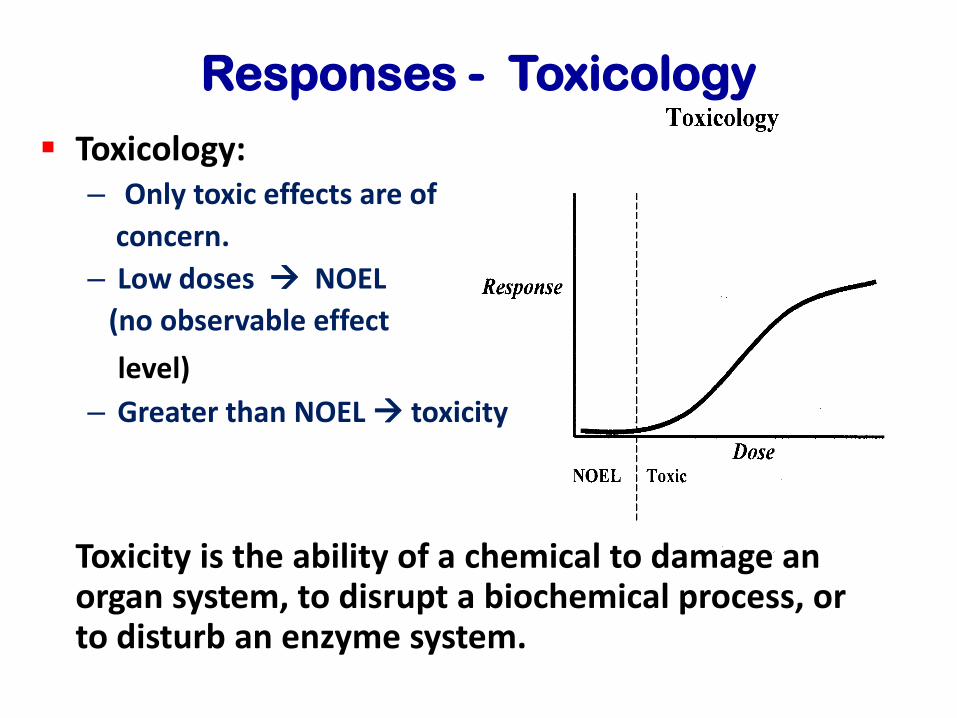
Responses - Toxicology
Toxicology:– Only toxic effects are of
concern.
– Low doses NOEL
(no observable effect
level)
– Greater than NOEL toxicity
Toxicity is the ability of a chemical to damage an organ system, to disrupt a biochemical process, or to disturb an enzyme system.
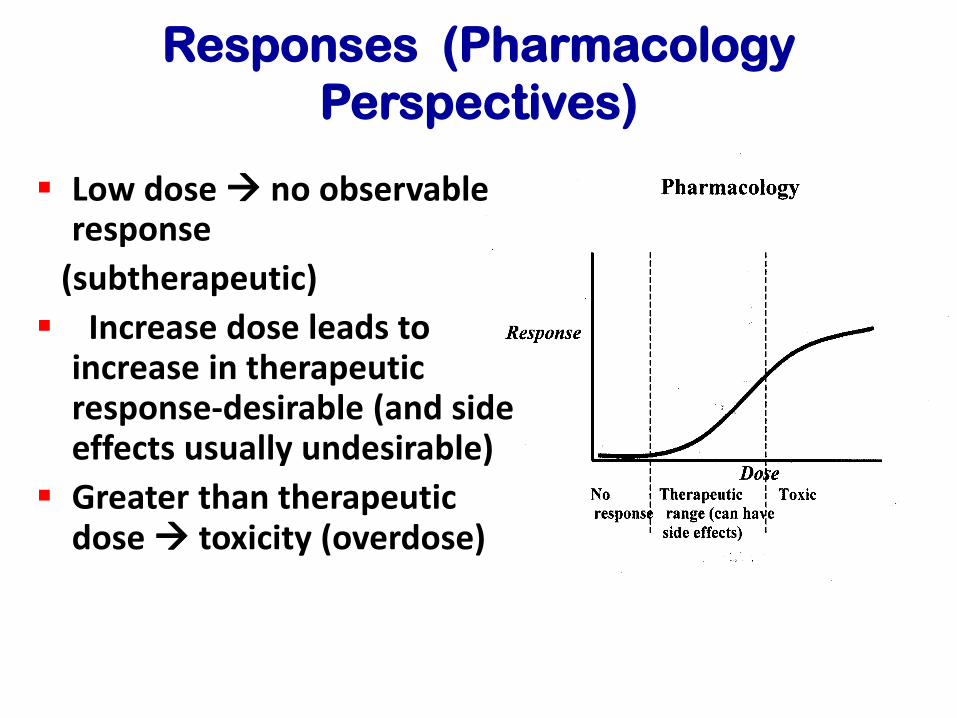
Responses (Pharmacology
Perspectives)
Low dose no observable response
(subtherapeutic)
Increase dose leads to increase in therapeutic response-desirable (and side effects usually undesirable)
Greater than therapeutic dose toxicity (overdose)
Factor Influencing a Dose-Response
Curve?
Species
Gender
Genetic strain
Age
Route of administration
Environmental conditions
Nutritional status
Effects of More Than One
Chemical
Additive Effect: the combined effect of the two chemicals is equal to the sum of the effects of each agent given alone. This is the most commonly observed effect when two chemicals are given together. (2 + 2 = 4)
Effects of More Than One
Chemical – Continued
Synergistic Effect: occurs when the combined effects of two chemicals are much greater than the sum of the effects of each agent given alone.
– CCl4 and ethanol are hepatotoxic alone but when given together produce much more liver injury than the mathematical sum of their individual effects. (2 + 2 = 20).
– Smoking and asbestos exposure is another example.
– Cocaine use with alcohol is the third example.
Effects of More Than One
Chemical – Continued
Potentiation: occurs when one compound does not have a toxic effect on a certain organ or system but when added to another chemical makes that chemical much more toxic.
– CCl4 is hepatotoxic, isopropanol is not hepatotoxic, when given together the effect of CCl4 is more than expected. (0 + 2 = 10)
Effects of More Than One
Chemical – Continued
Antagonism: occurs when two chemicals administered together interfere with each other’s action. Antagonistic interactions are very often desirable in toxicology and are the basis of many antidotes. (2 + (-2) = 0).
Types of Antagonism
Functional antagonism occurs when two chemicals counterbalance each other by producing opposite effects on the same physiological function.
Chemical antagonism is a chemical reaction between two compounds that produces a less toxic product. Example = a chelator and a metal.
Determination
of Exposure Limits
Toxicology study
To quantify the effects of toxicant on target organism
Usually done on animals (lung, kidney, liver) and the results are extrapolated to human. For genetic effect, the study is on single-cell organism.
Different routes requires different toxicological study
Toxicological study
Involve identifying,
– The toxicant
– The target or test organism
– The effect or response to be monitored
– The dose range
– Ingestion or injection , mg toxicant/kg of body weight
– Gaseous Inhalation, ppm or mg/m3 air
– Particle inhalation, millions of particle per cubic foot (mppcf) or mg/m3 air
– The period of the test (mostly acute tocixity study)
– Acute toxicity, single exposure or series of exposure in a short time
– Chronic toxicity, multiple exposure over a long period of time, also difficult to perform
Acute Exposure - Continued
Mouse and rat are the species most commonly used for testing
Both sexes are used
Food is withheld the night before testing
The number of animals that reach a prescribed endpoint at each dose are tabulated
10 animals per dose
5 dose levels
Acute Exposure - Continued
If larger animals are used the dose is increased in the same animal until the prescribed endpoint is reached
Endpoints could be
– Lethal dose (death)
– Toxic dose (ex. Liver injury)
– Effective dose (ex. Relief from itching)
Subchronic Testing
90 days is the most common test duration but 30 days to 90 days can be used
Usually oral administration of the chemical via food; also implant
Used to further characterize the specific organs affected by test compound after repeated administration of the chemical
Subchronic Exposure
At least 3 doses
– A high dose that produces toxicity but death in less than 10% of the animals
– A low dose that does not produce apparent toxic effects during an acute exposure
– An intermediate dose
For Drugs Under Development
Acute and Subchronic studies must be completed before company can file an IND (Investigate New Drug) application with the FDA (Food and Drug Administration).
If the application is approved then Clinical Trials can begin. Chronic tests can begin at the same time.
Chronic Exposure
Exposure to a chemical for a period longer than 3 months, usually 6 months to 2 years in rodents
Drug Testing – 6 months
Food Additives with potential lifetime human exposure – 2 years required
Chronic Exposure - Continued
Designed to assess cumulative toxicity of chemicals including consideration of carcinogenic potential
Mice – 18 months to 2 years
Rats – 2 to 2.5 years
Start with 60 animals/sex/dose to end up with 30 animals to survive study (LD50/LC50)
What Can Be Learned From A Dose-
Response Curve?
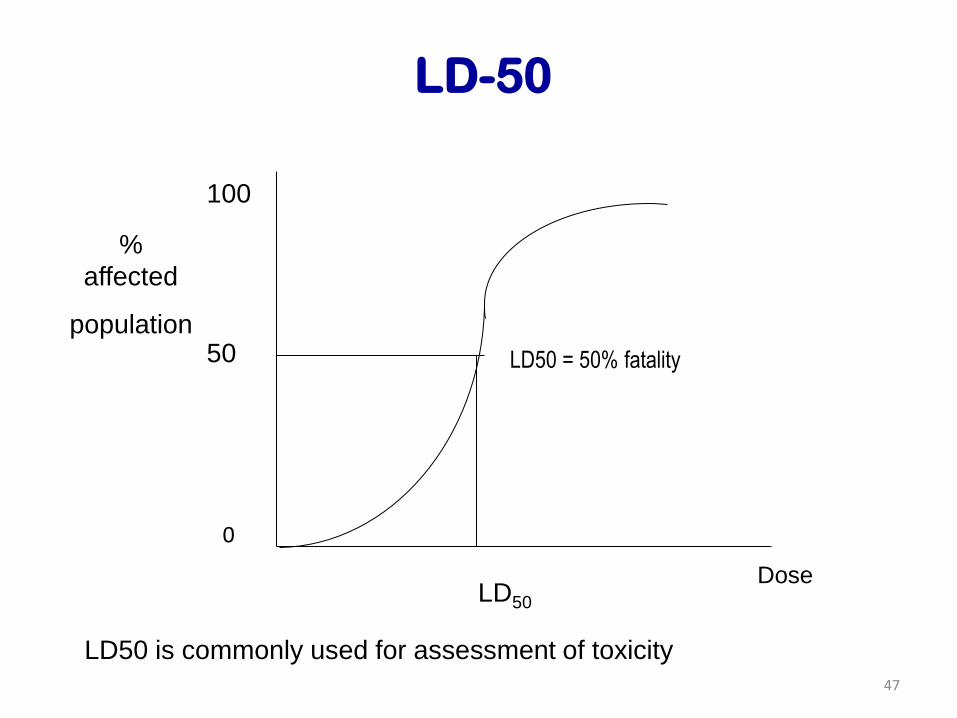
LD50 – Median Lethal Dose, quantity of the chemical that is estimated to be fatal to 50% of the organisms
– LD50 values are the standard for comparison of acute toxicity between chemical compounds and between species
TD50 – Median Toxic Dose
ED50 – Median Effective Dose
LC50 – Median Lethal Concentration
47
LD50 is commonly used for assessment of toxicity
%
affected
population
100
50
0
LD50
Dose
LD50 = 50% fatality
LD-50
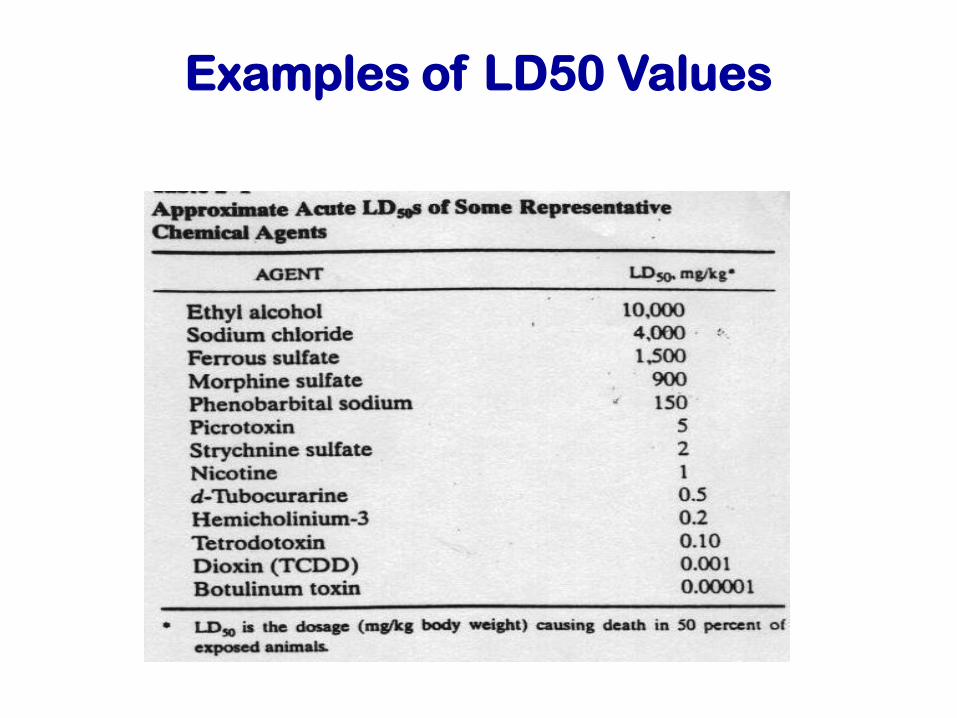
Examples of LD50 Values
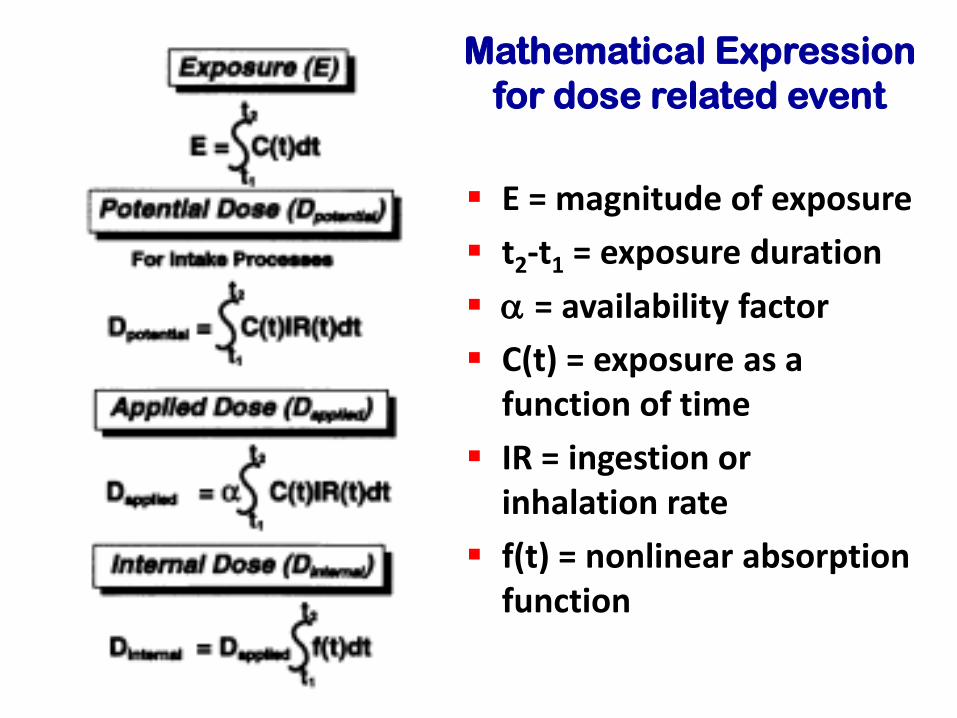
Mathematical Expression
for dose related event
E = magnitude of exposure
t2-t1 = exposure duration
a = availability factor
C(t) = exposure as a function of time
IR = ingestion or inhalation rate
f(t) = nonlinear absorption function

Probit Analysis
Probit Analysis
The dose level of the various hazard events
against fatality can be conveniently determined
using Probit Analysis.
It is a graphical and Look-up Table approach to
determine probability of fatality
51
Probit Analysis
The probit variable Y is computed from:
Y = k1 + k2 ln V
Values of constants k1, k2 and causative
variable V (representing the dose) are
given in table
Once the probit is obtained, it can be
converted into % fatality
52
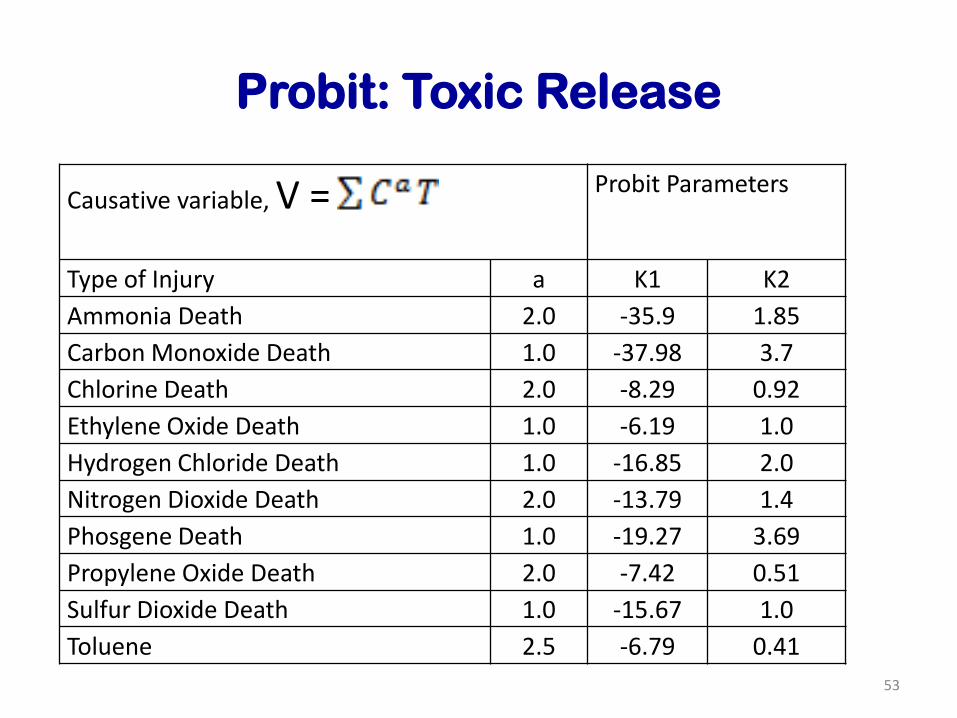
Probit: Toxic Release
53
Causative variable, V = Probit Parameters
Type of Injury a K1 K2
Ammonia Death 2.0 -35.9 1.85
Carbon Monoxide Death 1.0 -37.98 3.7
Chlorine Death 2.0 -8.29 0.92
Ethylene Oxide Death 1.0 -6.19 1.0
Hydrogen Chloride Death 1.0 -16.85 2.0
Nitrogen Dioxide Death 2.0 -13.79 1.4
Phosgene Death 1.0 -19.27 3.69
Propylene Oxide Death 2.0 -7.42 0.51
Sulfur Dioxide Death 1.0 -15.67 1.0
Toluene 2.5 -6.79 0.41
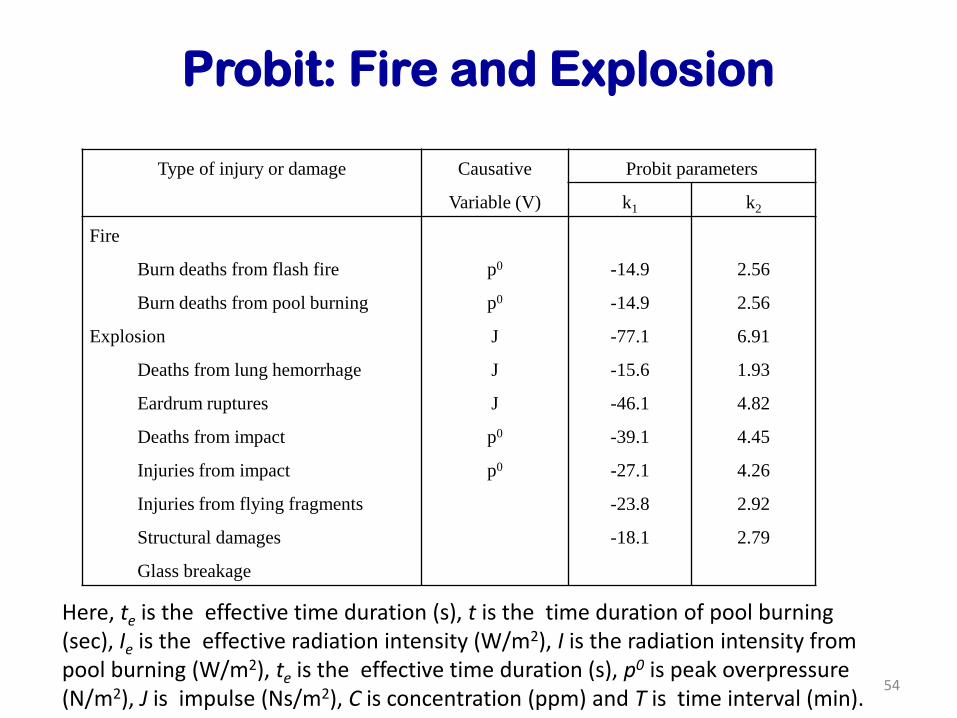
Probit: Fire and Explosion
Type of injury or damage Causative
Variable (V)
Probit parameters
k1 k2
Fire
Burn deaths from flash fire
Burn deaths from pool burning
Explosion
Deaths from lung hemorrhage
Eardrum ruptures
Deaths from impact
Injuries from impact
Injuries from flying fragments
Structural damages
Glass breakage
p0
p0
J
J
J
p0
p0
-14.9
-14.9
-77.1
-15.6
-46.1
-39.1
-27.1
-23.8
-18.1
2.56
2.56
6.91
1.93
4.82
4.45
4.26
2.92
2.79
54
Here, te is the effective time duration (s), t is the time duration of pool burning (sec), Ie is the effective radiation intensity (W/m2), I is the radiation intensity from pool burning (W/m2), te is the effective time duration (s), p0 is peak overpressure (N/m2), J is impulse (Ns/m2), C is concentration (ppm) and T is time interval (min).
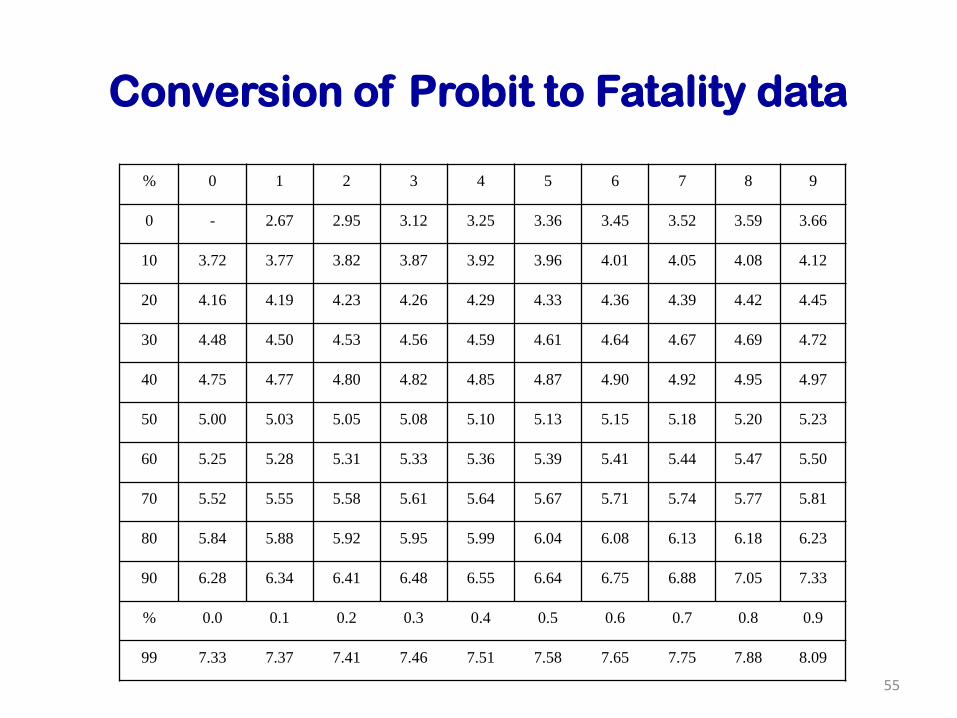
Conversion of Probit to Fatality data
55
% 0 1 2 3 4 5 6 7 8 9
0 - 2.67 2.95 3.12 3.25 3.36 3.45 3.52 3.59 3.66
10 3.72 3.77 3.82 3.87 3.92 3.96 4.01 4.05 4.08 4.12
20 4.16 4.19 4.23 4.26 4.29 4.33 4.36 4.39 4.42 4.45
30 4.48 4.50 4.53 4.56 4.59 4.61 4.64 4.67 4.69 4.72
40 4.75 4.77 4.80 4.82 4.85 4.87 4.90 4.92 4.95 4.97
50 5.00 5.03 5.05 5.08 5.10 5.13 5.15 5.18 5.20 5.23
60 5.25 5.28 5.31 5.33 5.36 5.39 5.41 5.44 5.47 5.50
70 5.52 5.55 5.58 5.61 5.64 5.67 5.71 5.74 5.77 5.81
80 5.84 5.88 5.92 5.95 5.99 6.04 6.08 6.13 6.18 6.23
90 6.28 6.34 6.41 6.48 6.55 6.64 6.75 6.88 7.05 7.33
% 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
99 7.33 7.37 7.41 7.46 7.51 7.58 7.65 7.75 7.88 8.09
Monty Herr
Types of Antagonism-Continued
Dispositional antagonism occurs when the disposition of a chemical is altered so that the concentration and/or duration of the chemical at the target organ are diminished. Ex. Metabolism is increased –Excretion is increased, therefore half-life is decreased
Receptor antagonism occurs when two chemicals that bind to the same receptor produce less of an effect when given together than the addition of their separate parts. Receptor antagonists are often termed blockers.
Chronic Exposure - Continued
Highest administered dose = “Estimated Maximum Tolerable Dose (MTD) derived from subchronic study
The National Toxicology Program defines the MTD as “a dose that suppresses body weight slightly (i.e. 10%) in a 90 day study
Also use ½ MTD, ¼ MTD, and a control group