top 5 pediatric hospital journal articles - azaap lecture... · top 5 journal club articles . ......
TRANSCRIPT
40 TH ANNUAL PEDIATRICS IN THE RED ROCKS CONFERENCE
S A M U E L F L O R E S , M D – P E D I A T R I C H O S P I T A L I S T ,
K I D S L I N K H O S P I T A L I S T G R O U P , P H O E N I X C H I L D R E N ’ S H O S P I T A L
B R I T T A N Y W O L D M D – P E D I A T R I C H O S P I T A L I S T F E L L O W , K I D S L I N K H O P S I T A L I S T G R O U P , P H O E N I X
C H I L D R E N ’ S H O S P I T A L
T E R E S A B L A S K O V I C H – P L 3 P E D I A T R I C R E S I D E N T , P C H / M M C R E S I D E N C Y P R O G R A M
S A R A H F R A N C I X – P L 2 P E D I A T R I C R E S I D E N T , P C H / M M C
R E S I D E N C Y P R O G R A M
W H I T N E Y G U T I E R R A Z – P L 2 P E D I A T R I C R E S I D E N T , P C H / M M C R E S I D E N C Y P R O G R A M
Top 5 Journal Club Articles

Disclosure
We have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in the CME activity.
We do not intend to discuss an unapproved/investigative use of a commercial product/device in our presentation.
Literature Review
Journals
Journal of Pediatrics
Journal of Pediatric Infectious Diseases
Journal of Pediatric Gastroenterology
Journal of Hospital Pediatrics

A L E X A N D E R W . H I R S C H , M D , M I C H A E L C . M O N U T E A U X , S C D , G E N N A F R U C H T M A N , B A , R I C H A R D G . B A C H U R ,
M D , M A R K I . N E U M A N , M D , M P H
H O S P I T A L P E D I A T R I C S V O L 1 3 8 , I S S U E 2 , A U G U S T 2 0 1 6
Characteristics of Children Hospitalized with Aspiration
Pneumonia

Case

Aspiration Pneumonia
Aspiration pneumonia is an infectious process due to the aspiration of pharyngeal secretions that are colonized by pathogenic bacteria.
It is an important cause of serious morbidity and mortality, particularly among children with chronic medical conditions

Pathophysiology and Bacteriology
A study revealed that half of all healthy adults aspirate small amounts of oropharyngeal secretions during sleep.
There are multiple protective mechanisms to prevent aspiration: During aspiration the airway is exposed to oropharyngeal saliva or
acidic gastric contents, along with enteric bacteria. Traditionally been attributed to anaerobic bacteria. Brook I, Finegold SM. Bacteriology of aspiration pneumonia in children. Pediatrics. 1980;65(6):1115–1120 Average of 5 bacteria isolated per specimen with a mixture of anaerobes and
aerobes.
Conditions that increase the volume of aspirated oropharyngeal contents lead to an increased risk of aspiration pneumonia. Reduced level of consciousness: chronic neurological impairment, seizure,
anesthesia, alcohol or substance abuse Dysphagia Gastroesophageal reflux Foreign body aspiration Use of a NG tube

Objective
Study Aim: To evaluate the difference in disease entities (aspiration pneumonia vs CAP) in regards to:
Patient characteristics: median age, sex, race, proportion of patients with a complex chronic condition (CCC).
Hospitalization characteristics: length of stay, ICU admission, cost, 30-day readmission rate, and median hospitalization costs.
Pharmacological treatment: antibiotics or corticosteroid administration.
Seasonal variability
Methods
Retrospective cohort study
Pediatric Health Information System: administrative database that contains encounter-level data from more than 47 tertiary care pediatric hospitals.
Inclusion Criteria: discharged from inpatient or observation with a diagnosis of aspiration pneumonia or CAP between 1/2009 – 12/2014.
Exclusion Criteria: Children with cystic fibrosis and children who died during their hospitalization.

Methods – Further Classification
Proportion of patient’s with complex chronic conditions Dx expected to last > 12 months Involve several organ systems or 1 organ system severely
enough to require specialty care and hospitalization. Presence of technology dependence: gastrostomy,
tracheostomy, cerebrospinal fluid ventricular shunt, permanent indwelling catheter and pacemaker.
ICD-9 diagnosis codes for complicated pneumonia and related procedures.
Illness severity (measured using the severity scale defined as part of the All Patient Refined Diagnosis Related Groups Classification).

Results: Demographics
Exclusion: CF (7723) and children that died during the hospitalization (623) Mortality was more likely among
children with aspiration pneumonia. (1.6% vs 0.4%, P < 0.001).
Children with aspiration pneumonia were older and more likely to have public insurance than children with CAP.

Results: comorbidities
Children with aspiration pneumonia where more likely to have a CCC and more likely to have multiple chronic conditions.
54.8% of children with aspiration pneumonia had a neurological comorbidity compared with 10% of children with CAP.
Most common type of chronic condition: technology dependence.

Results
Aspiration pneumonia was associated with: Longer median hospital length
of stay (5 days vs 2 days). Hospitalization > 1 week. 3 times as likely to require ICU
care (33% vs 12%).
Hospital readmission within 30 days occurred in 36% of patients (vs 16%)
Median cost of hospitalization was $14,963 vs $6,115 for CAP.

Results
Controlling for confounding variables:
Analyses were performed between children with aspiration pneumonia vs CAP without complex chronic conditions.
Aspiration pneumonia continued to have:
Longer hospital stays (3 vs 2 days, P < .001).
More likely to require ICU admission ( 22.9% vs 7.4%, P < .001).
Higher median hospital costs ($8127 vs $4793, P < .001).

Results: Pharmacological Treatment
Antibiotic prescribing patterns differed between children hospitalized with aspiration pneumonia and those with CAP.

Results: Seasonal Variation

Discussion
Children with aspiration pneumonia are hospitalized for longer durations of time, have higher rates of mortality, more likely to require ICU level care and have higher 30-day readmission rates
These differences reflect different disease processes but are also reflective of vastly different patient populations.
Patients with aspiration pneumonia are more likely to have complex chronic conditions.
Antibiotic strategies reflect an attempt to capture the different microbial profiles that distinguish CAP from aspiration pneumonia.

Strengths and Limitations
Strengths Large population Secondary analysis performed that was restricted to children
without complex chronic conditions. Statistically significant differences were determine between the
two groups. Limitations Misclassification of patients
There is little clinical information available in the Pediatric Health Information System administrative database.
Does not demonstrate a generalized population. Only examined inpatient encounters. Likely inherent bias in the labeling of a diagnosis of aspiration in a
child with a chronic condition. Treatment initiation and duration.

Conclusion
This study supplements a growing body of literature suggesting health outcomes are worse and hospital resources use is higher in patient’s diagnosed with aspiration verses non-aspiration pneumonia.
There needs to be further research to improve coordination of care and treatment of children at risk for aspiration pneumonia.

B O R J A G O M E Z , M D , A , B S A N T I A G O M I N T E G I , M D , P H D , A , B S I L V I A B R E S S A N , M D , P H D , C L I V I A N A D A D A L T ,
M D , D A L A I N G E R V A I X ,
M D , E L A U R E N C E L A C R O I X , M D
J O U R N A L O F P E D I A T R I C S , V O L U M E 1 3 8 , N U M B E R 2 , A U G U S T 2 0 1 6
Validation of the “Step-by-Step” Approach in the Management of
Young Febrile Infants

Objective
Prospectively validate the Step-by-Step approach
Compare it to the Rochester criteria and the Lab-score for identifying low risk febrile infants
Why do we Care?
National ongoing goal (Project REVISE) to differentiate high vs low risk febrile infants
Reduce risk of procedures (LP)
Reduce risk of unnecessary antibiotic exposure
Reduce length of hospitalization
Reduce healthcare costs
Study Design
Multicenter Study: 11 European pediatric emergency departments
Infants ≤ 90 days old presenting with fever without a source
September 2012 – August 2014
Study Design
Urine dipstick, urine culture, WBC, CRP, PCT, and blood culture were collected on every patient
Further testing, treatment, and admission at discretion of attending physician
Step-by-Step, Rochester criteria, and Lab-score were applied to each patient and compared
Exclusion Criteria
1. Clear source of fever identified after a careful medical history
2. No fever on arrival at the PED and fever that had only been subjectively assessed by parents on touch, without the use of a thermometer
3. Absence of 1 or more of the mandatory ancillary tests (blood culture, urine culture collected by an aseptic technique, urine dipstick, PCT, CRP, or WBC count)
4. Refusal of the parents or caregiver to participate
Rochester Criteria
Infant appears well
Infant is previously healthy
Term, no perinatal/postnatal antibiotics, no hospitalizations, no chronic illness, no unexplained hyperbilirubinemia)
No evidence of skin, soft tissue, bone, joint or ear infection
Labs:
WBC 5,000 – 15,000
Bands </= 1,500
</= 10 WBC on urine microscopy
</= 5 WBC on stool microscopy if diarrhea

Lab-Score criteria
Assigns points for pro-calcitonin, CRP, and UA

Step-By-Step

Results
Discussion
The Step by Step approach was the most accurate at ruling out an invasive bacterial infection.
High sensitivity
High NPV
Best negative LR
Due to the low prevalence of IBI, the specificity, PPV, and positive LR were poor for all 3 approaches

Missed IBI’s
6 of the 7 invasive bacterial infections missed by the Step by Step approach, had fever duration of less than 2 hours

Conclusions
Step-by-Step approach appears to be a useful tool for risk stratifying febrile infants.
Caution should be used in infants with very short fever duration. These infants may require additional observation.
J E F F R E Y R I E S E , M D , A T I M O T H Y P O R T E R , M D , A J A M I E F I E R C E , M D , A A L I S O N R I E S E , M D , M P H , A T R O Y
R I C H A R D S O N , M S , M P H , P H D , B B R I A N K . A L V E R S O N , M D A
J O U R N A L O F H O S P I T A L P E D I A T R I C S , V O L U M E 7 , I S S U E 4 , A P R I L 2 0 1 7
Clinical Outcomes of Bronchiolitis After Implementation of a General Ward High
Flow Nasal Cannula Guideline
Study Question
Is there an association between using high-flow nasal cannula on general wards and clinical outcomes of infants with bronchiolitis?

Study Design
Retrospective, interrupted time series analysis of pre and post-implementation of HFNC guideline
Hasbro Children’s Hospital (tertiary center in Providence, RI)
Allowed admission to floor on HFNC
Allowed initiation of HFNC on floor patient
Allowed transfer of PICU to floor on HFNC
Patient Selection
Inclusion:
Infants <24 months admitted from 2010 – 2014 with bronchiolitis
Exclusion:
<37 weeks prematurity
CLD, asthma, heart disease, neurologic disease, chromosomal abnormalities
Admitted >21 days


Clinical Outcomes
Primary Outcome: Hospital length of stay
Secondary Outcome:
PICU transfer from wards
PICU length of stay
Adverse outcomes (intubation and 30 day readmission)

Study Results
Looked at unadjusted vs adjusted clinical outcomes
Adjusted = takes into account pre-intervention trends of improvement in bronchiolitis management
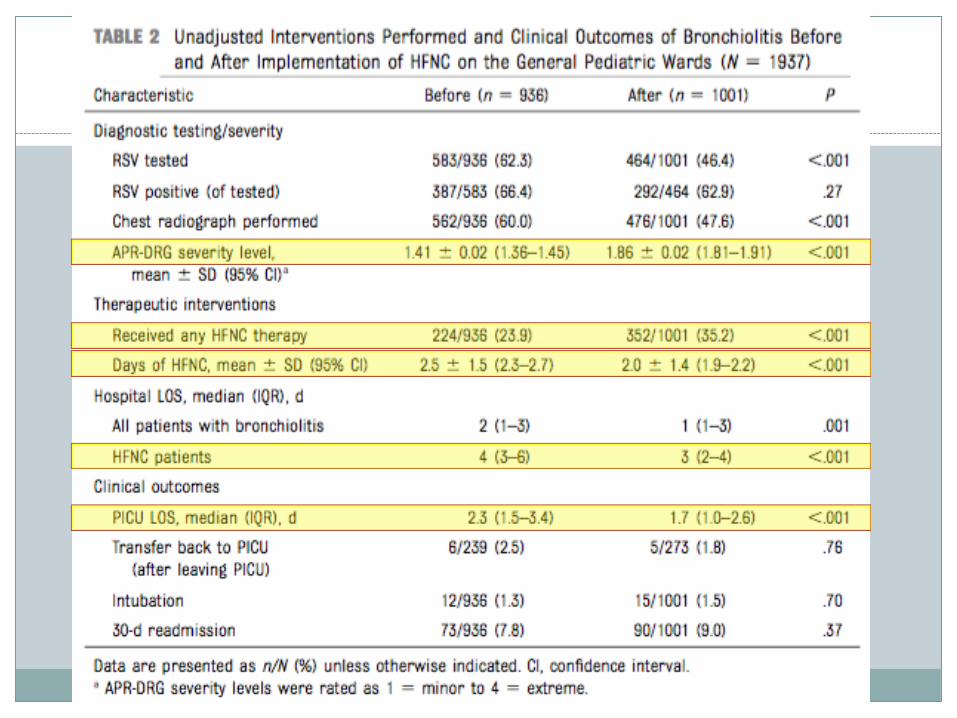

Days of HFNC
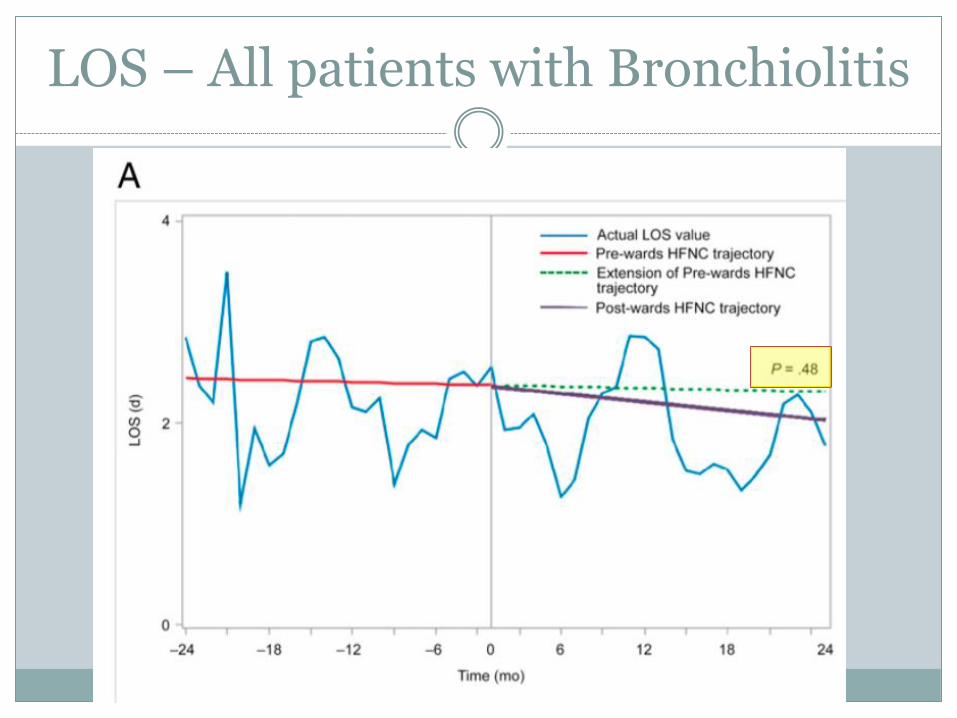
LOS – All patients with Bronchiolitis

LOS – Patients receiving HFNC

LOS – Patients not receiving HFNC

PICU Length of Stay

Transfer rate to PICU
Author’s Conclusions
Implementing use of HFNC on general ward was associated with increase in use, but no significant changes in measured clinical outcomes of bronchiolitis

Study Limitations
Did the guideline actually change practice? Despite claim that use of HFNC increased, there is
no adjusted data on patients who “Received any HFNC therapy”
Interrupted time series can be difficult to interpret when it takes time for change to actually come into effect
Interrupted time series requires extrapolation of data
Inability to control confounding variables Hospital LOS calculated in whole days
J O E L S . T I E D E R , M D , M P H , F A A P , J O S H U A L . B O N K O W S K Y , M D , P H D , F A A P , R U T H A . E T Z E L , M D , P H D , F A A P , W A Y N E , H . F R A N K L I N , M D , M P H , M M M ,
F A A P , D A V I D A . G R E M S E , M D , F A A P , B R U C E H E R M A N , M D , F A A P , E L I O T S . K A T Z , M D , F A A P , L E O N A R D R .
K R I L O V , M D , F A A P , J . L A W R E N C E M E R R I T T I I , M D , F A A P , C H U C K N O R L I N , M D , F A A P , J A C K P E R C E L A Y , M D ,
M P H , F A A P , R O B E R T E . S A P I E N , M D , M M M , F A A P , R I C H A R D N . S H I F F M A N , M D , M C I S , F A A P , M I C H A E L
B . H . S M I T H , M B , F R C P C H , F A A P
J O U R N A L O F P E D I A T R I C S V O L U M E 1 3 7 , N U M B E R 5 , M A Y 2 0 1 6 :
What are the Clinical Practice Guidelines for Brief Resolved Unexplained Events(BRUE)?
ALTE
ALTE originated from 1986 National Institutes of Health Consensus Conference on Infantile Apnea
Intended to replace “Near-miss sudden infant death syndrome”
ALTE: episode that is frightening to the observer and that is characterized by some combination of apnea (central or occasionally obstructive), color change (usually cyanotic or pallid but occasionally erythematous or plethoric), marked change in muscle tone (usually marked limpness), choking, or gagging

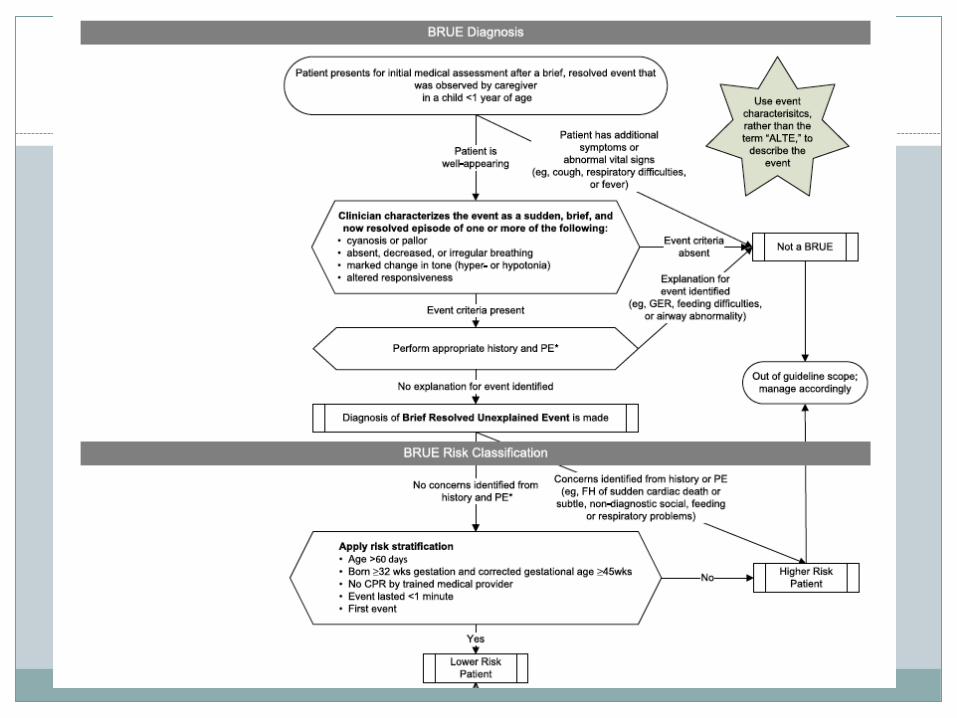
BRUE
BRUE:
Occurs in infants < 1 year of age when the observer reports a sudden, brief, and now resolved episode of >1 of the following:
Cyanosis or pallor
Absent, decreased, or irregular breathing
Marked change in tone (hypertonia or hypotonia)
Altered level of consciousness
Diagnose a BRUE only when there is no explanation for a qualifying event after conducting an appropriate history and physical examination

History Considerations
Considerations for child abuse
History of the event
State during the event
End of event
State after event
Recent history
Past medical history
Family history
Environmental history
Social history

Physical Exam Considerations
General appearance Growth variables Vital signs Skin HEENT Neck Chest Heart Abdomen Genitalia Extremities Neurologic
Lower Risk Group
Age > 60 days
Gestational age > 32 weeks and post-conceptional age > 45 weeks
First BRUE
Duration of event < 1 minute
No CPR required by trained medical provider
No concerning historical features
No concerning physical examination findings

Methods
A multidisciplinary subcommittee including doctors, methodologist, epidemiologist and parent representatives performed a systematic review of literature of ALTEs from 1970-2014
Evidence-based recommendations were graded based on benefit vs. harm

Key Action Statement: Cardiopulmonary
Clinicians need not admit infants presenting with a lower risk BRUE to the hospital solely for cardiorespiratory monitoring (Grade B, Weak Recommendation)
Clinicians may briefly monitor infants presenting with a lower risk BRUE with continuous pulse oximetry and serial observations (Grade D, Weak Recommendation)
Clinicians should not obtain a chest radiograph in infants presenting with a lower risk BRUE (Grade B, Moderate Recommendations)
Clinicians should not obtain measurement of venous or arterial blood gases in infants presenting with a lower-risk BRUE (Grade B, Moderate Recommendation)

Key Action Statement: Cardiopulmonary Cont.
Clinicians should not obtain an overnight polysomnograph in infants presenting with Lower-Risk BRUE (Grade B, Moderate Recommendation)
Clinicians may obtain a 12-lead electrocardiogram for infants presenting with lower-risk BRUE (Grade C, Weak Recommendation)
Clinicians should not obtain an echocardiogram in infants presenting with lower-risk BRUE (Grade C, Moderate Recommendation)
Clinicians should not initiate home cardiorespiratory monitoring in infants presenting with a lower-risk BRUE (Grade B, Moderate Recommendations)

Key Action Statement: Child Abuse
Clinicians need not obtain neuroimaging (computed tomography, MRI, or ultrasonography) to detect child abuse in infants presenting with a lower-risk BRUE (Grade C, Weak Recommendation)
Clinicians should obtain an assessment of social risk factors to detect child abuse in infants presenting with a lower-risk BRUE (Grade C, Moderate Recommendation)
Child Abuse History and Physical
History: Developmentally inconsistent or discrepant history provided by the caregivers, a previous ALTE, a recent emergency service telephone call, vomiting, irritability, or bleeding from nose or mouth
Social risk factors: unrealistic expectations, mental health problems, domestic violence/intimate partner violence, social service involvement, law enforcement involvement, and substance abuse
Physical exam: large or full/bulging anterior fontanel, scalp bruising or bogginess, oropharynx, frenula damage, skin findings such as bruising or petechiae

Key Action Statement: Neurology
Clinicians should not obtain neuroimaging (computed tomography, MRI, or ultrasonography) to detect neurologic disorders in infants presenting with a lower-risk BRUE (Grade C, Moderate Recommendation)
Clinicians should not obtain an EEG to detect neurologic disorders in infants presenting with a lower-risk BRUE (Grade C, Moderate Recommendation)
Clinicians should not prescribe antiepileptic medications for potential neurologic disorders in infants presenting with a lower-risk BRUE (Grade C, Moderate Recommendation)

Key Action Statement: Infectious Disease
Clinicians should not obtain a white blood cell count, blood culture, or cerebrospinal fluid analysis or culture to detect an occult bacterial infection in infants presenting with a Lower-Risk BRUE (Grade B, Strong Recommendation)
Clinicians need not obtain a urinalysis (bag or catheter) in infants presenting with a Lower Risk BRUE (Grade C, Weak Recommendation)
Clinicians should not obtain a chest radiograph to assess for pulmonary infection in infants presenting with a Lower-Risk BRUE (Grade B, Moderate Recommendation)

Key Action Statement: Infectious Disease Cont.
Clinicians need not obtain respiratory viral testing if rapid testing is available in infants presenting with a Lower-Risk BRUE (Grade C, Weak Recommendations)
Clinicians may obtain testing for pertussis in infants presenting with a Lower-Risk BRUE (Grade B, Weak Recommendation)
Key Action Statement: Gastroenterology
Clinicians should not obtain investigations for GER (eg. Upper Gastrointestinal Series, pH probe, Endoscopy, Barium Contrast Study, Nuclear Scintigraphy, and Ultrasonography) in infants presenting with a Lower-Risk BRUE (Grade C, Moderate Recommendation)
Clinicians should not prescribe acid suppression therapy for infants presenting with a Lower-Risk BRUE (Grade C, Moderate Recommendation)

Key Action Statement: Inborn Errors of Metabolism
Clinicians need not obtain measurements in lower-risk BRUE:
Serum lactic Acid
Serum bicarbonate
Electrolytes
Calcium
Ammonia
Venous or arterial blood gases
Blood glucose
Urine organic acids, plasma amino acids, or plasma acylcarnitines
Key Action Statement: Anemia
Clinicians should not obtain laboratory evaluation for anemia in infants presenting with a Lower-Risk BRUE (Grade C, Moderate Recommendation)

Key Action Statement: Patient-and Family-Centered Care
Clinicians should offer resources for CPR training to caregivers (Grade C, Moderate Recommendation)
Clinicians should educate caregivers about BRUEs (Grade C, Moderate Recommendation)
Clinicians should use shared decision-making for infants presenting with a Lower-Risk BRUE (Grade C, Moderate Recommendation)


Conclusion
Efforts and education needed to facilitate BRUE guideline across medical community
Guideline created to give physicians definition and appropriate work-up given many situations.
Further research required to determine incidence of BRUEs and effective of BRUE definition

A L E X A N D E R W . H I R S C H , M D , M I C H A E L C . M O N U T E A U X , S C D , G E N N A F R U C H T M A N , B A , R I C H A R D G . B A C H U R , M D ,
M A R K I . N E U M A N , M D , M P H
H O S P I T A L P E D I A T R I C S V O L U M E 6 , I S S U E 1 1 , N O V E M B E R 2 0 1 6
Are Proton Pump Inhibitors Effective for Treating GERD in
Infants Ages 1-11 months?

GER: A Physiological Manifestation
Gastroesophageal reflux (GER) defined as retrograde passage of gastric contents into the esophagus or extra-esophageal regions
Associated with transient relaxation of the lower esophageal sphincter
Typically presents as recurrent vomiting or persistent regurgitation

When GER Becomes Pathological
Physiological GER can become pathologic when it produces adverse symptoms or histologic and/or endoscopic visible changes
Clinical symptoms: Recurrent vomiting
Poor weight gain
Irritability
Dysphagia
Discomfort
Esophagitis
Respiratory Disorders

Goal of Study
Evaluate the efficacy and safety of esomeprazole in infants ages 1-11 months with signs and symptoms of GERD.

Methods
Randomized, double-blind, placebo-controlled parallel-group, treatment-withdrawal study conducted in 33 centers in the United States, France, Germany, and Poland
A 2-week open-label treatment phase followed by a 4-week randomized, double-blind, placebo-controlled treatment phase

Study Design
During 2-week open-label phase, all patients received esomeprazole once daily dosed per weight
After open-label phase, infants were randomized 1:2 to double-blind treatment with esomeprazole (at the open-label dose) or placebo for up to 4 weeks

Methods: Assessments
Primary efficacy endpoint was time from randomization to discontinuation owing to symptoms worsening in double-blind phase.
Secondary endpoints included time from randomization to discontinuation for any reason, proportion of patients achieving treatment success, daily symptoms assessed by parent/guardian, and PGA symptom severity
Safety and tolerability also evaluated through recording of adverse events

Results: Double-Blind Treatment Open-Label Phase

Results: Double-blind Treatment Withdrawal Phase
Primary analysis: Discontinuation from study secondary to symptom worsening in placebo group 48.8% (20/41 patient) compared with 38.5% (15/39) patients who received esomeprazole
No statistical significance (HR 0.69%, 95% CI 0.35-1.35%, P=0.28) but numerically favored esomeprazole group
More infants in placebo (n=17) than in the esomeprazole group (n=10) discontinued from the study

Results: Safety and Tolerability
In open-label phase, 47 of 98 patients (48%) had adverse events; 4 patients (4.1%) considered treatment related
During the double-blind phase, 23 of 39 (59%) of esomeprazole-treated patients and 27 of 41 (66%) of placebo patients had adverse events
Discussion
Patients treated with esomeprazole had a 31% reduced risk of discontinuing from the study owing to worsening of symptoms compared with infants who received placebo. No statistical difference.
Most infants (83%) had improvement of GERD symptoms within 2 weeks of starting open-label esomeprazole therapy

Discussion: Limitations
Inclusion of mixed-type study population
Patients with a variety of symptoms enrolled
No assessment of time to symptom resolution during the open-label phase
No insight as to whether patients who improved during the open-label phase would have improved with or without treatment

Discussion: Summary
No statistically significant difference between PPI treatment and placebo
Infants with more severe symptoms and confirmed GERD may benefit more from PPI therapy
No clinical studies of infants < 1 year old have demonstrated a statistical benefit in treating with PPIs
PPIs are well tolerated by infants
Discussion: Future Research
PPIs and their role in treating infants < 1 year old with severe disease symptoms and confirmed GERD
Clarification in identifying patients most likely to respond favorably to PPIs