tissue engineering in congenital heart...
TRANSCRIPT

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
2
Abstract— Congenital heart disease is one of the most
prevalent birth defects. Approximately 1% of babies are born
with a structural heart defect. Components of the
cardiovascular system that may be affected by congenital heart
disease include the cardiac wall, septum, heart valves and blood
vessels. Many of these cardiac anomalies require surgical
correction; however current methods have some limitations.
Pediatric patients often require multiple operations as they
grow to replace their grafts, which may be either failing or
becoming too small in size. Additionally, current materials for
organ reconstruction can still not fully integrate with the host
tissue and lack regenerative properties. Tissue engineering
potentially offers a solution to the pressing problem of tissue
damage and shortage of transplant organs. This review article
provides an overview of congenital heart defects and outlines
the unique needs of children as a patient population. Advances
in tissue engineering of cardiac patches, heart valves and blood
vessels relevant to congenital heart disease are described.
Furthermore, this report outlines the challenges in the field that
need to be overcome before tissue engineered myocardium,
septum, valves and vessels can become clinical reality for the
treatment of pediatric cardiac patients.
Keywords — Biomaterial, cardiac defect, congenital heart
disease, regenerative medicine, tissue engineering
1. INTRODUCTION
Congenital heart defects (CHDs) affect approximately 1 in
100 children born in the United States, which equates to nearly
40,000 births per year [1, 2]. These statistics are a conservative
estimate, and can vary depending on the classification and
detection of the defect [1]. As a result, CHDs are the leading
cause of infant illness and death [3]. From 1999 to 2006, the
US census reported nearly 41,500 CHD-related deaths with
almost 28,000 deaths resulting directly from CHDs [4]. While
the exact mechanisms that cause each CHD are unclear, it is
estimated that at least 15% are related to certain genetic
disorders [5-7]. The type and severity of defects are vast and
often occur as a combination of defects [8]. The spectrum of
CHDs is very broad, with some minor defects not requiring any
form of therapy, to very complex cases, where time-sensitive
1 Department of Pediatrics, Baylor College of Medicine, One Baylor Plaza,
Houston, TX, 77030, USA, 2 Department of Bioengineering, Rice University,
PO Box 1892, MS-142, Houston, TX 77251-1892, USA 3 Congenital Heart
Surgery Services, Texas Children’s Hospital, Houston, TX, USA
*Correspondence to Jeffrey G. Jacot (e-mail: [email protected]).
surgical interventions are needed to sustain the life of the child.
The cost of healthcare for CHDs is massive, with nearly $1.4
billion reported in the United States in 2004 [9]. This is more
than half of the entire hospital costs for birth defects reported
that year. Therefore early detection and strategies to repair
CHDs and prevent long-term therapy and multiple operations
are important areas of research that would have significant
return.
In recent years, tissue engineering has emerged as a major
field of research for the regeneration and restoration of injured
or defective native tissue. Where some regenerative success in
years prior has come from autografts and homografts [10, 11]
restoring structure similar to native tissue, the majority of
approaches lack the restoration of native function. In the case
of CHDs, especially those involving cardiac wall repair, the
ability to contract synchronously is essential for proper blood
circulation. Tissue engineering is an appealing alternative that
can overcome the shortfalls of grafts in terms of availability and
rejection if used in conjunction with autologous cells. Tissue
engineered constructs for CHDs would not only provide
structural support, but also restore native function. Therefore
classical tissue engineering strategies [12, 13] to accomplish
this goal are typically composed of the following key elements:
a scaffold for mechanical support, mechanical stimuli to
provide conditioning, biochemical stimuli to promote cellular
signaling and function, and cells to assist in new tissue
formation as well as signaling. Ideally, the construct would
also be biodegradable with the degradation rate in tune with the
new tissue ingrowth.
The developing cardiopulmonary system is unique and
dynamic. This system is essential to sustaining life, and does so
by means of its structural and functional complexity. Cardiac
tissue is unique in itself, where cardiac muscle is distinct from
skeletal and smooth muscle. Components of the cardiovascular
system are regionally and functionally different, containing
different cells and extracellular matrix molecules.
Understanding the complexity of this system is the first step
towards designing regenerative techniques. In the case of
pediatric patients, CHDs pose further unique issues compared
to adult chronic cardiovascular diseases, such as
atherosclerosis, and therefore one must also consider the
distinctive needs of children as a patient population.
Many congenital heart defects are detected during prenatal
testing [14], or diagnosed during the first days of life. The most
severe lesions may require treatment very soon after birth. The
timing of intervention is a critical step, both in terms of surgical
decision-making, but also because of the availability of tissue
grafts. Sometimes a procedure cannot be undertaken until a
donor tissue of the right size is found, or because a surgeon
elects to postpone treatment until the patient grows and can
receive a larger implant so that multiple repeat surgical
procedures can be avoided. Tissue engineering could
Tissue Engineering in Congenital Heart Disease
Leda Klouda1, PhD, Christopher Tsao
2, MS, and Jeffrey G. Jacot*
2, 3, PhD

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
3
circumvent these concerns by providing a made-to-order
solution that can grow with the child. In the case that cells will
be included in the tissue engineered construct, prenatally
harvested cells could be expanded and be ready for
implantation quickly after the baby is born. Also, considering
the young age of patients receiving a graft, it is important to
stress the unique need for the implant to remodel and grow
during the child’s stages of development. A child undergoes
incremental growth phases, and the increase in size of most
organs follows that of the general body size [15]. Ideally, a
construct should be fully integrated with the host and be
durable and functional for life. Studies are presently underway
to determine the life span of some solutions employed for the
treatment of congenital cardiovascular disease, and in many
cases, reoperations and replacements are necessary. For
example, existing surgical prostheses for heart valve disease
have a limited functional life, which may be adequate for a
middle-aged person, but often prove problematic for young
recipients. Moreover, differences in the immune system of
infants, children and adults must be carefully evaluated
[16-18]. Previous studies have suggested that the performance
of bioprostheses is linked to the immune response which can
vary between age groups, particularly infants [19-21]. The
latter age category is important due to the large volume of
congenital cardiac surgeries performed in early infancy.
Therefore the use of immunosuppressants in pediatric patients
needing bioprostheses becomes a delicate balance of implant
rejection, side effects of long term exposure, and risk of
infection. When designing treatment strategies, one must
consider the detrimental effects of certain compounds or
medications on the developing systems of young children, and
also their active lifestyles, which make anticoagulant drugs for
example often dangerous. Overall, these are some of the factors
that may differentiate management of pediatric versus adult
patients, and have potential implications in tissue engineering.
This review provides an overview of the most common
congenital heart defects, as well as highlight current tissue
engineering research strategies used to correct these defects.
From this literature examination, current challenges in the field
are elucidated and therefore give insight into future research
directions for more successful treatment strategies.
2. OVERVIEW OF CONGENITAL HEART DEFECTS
Based on clinical studies, CHD is believed to affect around
1% of live births [1]. Ultrasound procedures allow for
approximately 39% of major CHDs, such as tetralogy of Fallot
or hypoplastic left heart syndrome, to be diagnosed in utero
during the second trimester [14], while the diagnosis of acute
CHDs, such as small atrial septal defects (ASDs) or ventricular
septal defects (VSDs), may not occur until birth or later.
Typically a trivial cardiac lesion that has eluded detection will
naturally close during infancy [22]. Also, many CHDs do not
manifest themselves until there is mixing of oxygenated and
deoxygenated blood after birth. This results from incomplete
closure of fetal circulatory vessels, such as the ductus
arteriosus. Therefore the actual reported percentage of births
with CHDs is likely to be slightly higher than reported [1].
The heart is a complex organ and myriad diseases can
result from lesions or malfunctions. As suggested by the
statistical occurrence of CHDs, the degree of severity in CHDs
is very diverse. There are a number of risk factors that can lead
to CHD, including but not limited to, maternal diabetes and
maternal lithium, phenytoin and alcohol use. In cases of
maternal diabetes, the risk of having a newborn with a
structural heart defect increases by 30% [23]. Family history
of CHD can also play a role, about 1-4% of babies born to
parents with CHDs are affected [1]. The exact causes for the
majority of CHDs are unknown, but are proposed to be linked
to causative genes in developing fetuses [7]. From the
perspective of tissue engineering for CHDs, corrective action
attempts to treat different lesions associated with a given
congenital heart disease. A brief overview of clinically
relevant lesion specific CHDs will help to better understand the
engineering challenges in creating a viable construct. Table 1
summarizes some specific CHDs with associated causes and
current treatment options.
TABLE OF ABBREVIATIONS AFSC amniotic fluid derived stem cells
ASD atrial septal defect
CHD congenital heart defect/disease
ECM extracellular matrix
EPC endothelial progenitor cells
GAG glycosaminoglycan
HA hyaluronic acid
IGF insulin growth factor
MSC mesenchymal stromal cells
P4HB poly(4-hydroxybutyrate)
ePTFE expanded polytetrafluoroethylene
PA pulmonary artery
PCL polycaprolactone
PDA patent ductus arteriosus
PEG poly (ethylene glycol)
PEUU polyester urethane urea
PGA poly(glycolic acid)
PGS poly(glycerol sebacate)
PLGA poly(lactide-co-glycolide)
PLLA poly(L-lactic acid)
PU polyurethane
RVOT right ventricular outflow tract
SIS small intestinal submucosa
TEHV tissue engineered heart valve
VEGF vascular endothelial growth factor
VIC valvular interstitial cell
VSD ventricular septal defect

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
4
Table 1: Congenital Heart Defects
Defect Estimated
% of Total
Congenital
Heart
Defects in
the US [1,
2]
Causes Diagnosis Treatment
Options
Ventricular
septal defects
20% Hole in ventricular
septum
Cardiac auscultation,
chest x-ray,
echocardiogram
Occlusion devices
[24-26],
patch closure materials
[27]
Tetralogy of
Fallot
10% 1. Large
ventricular defect 2.
Severe right
ventricular outflow tract
obstruction 3.
Overriding of the aorta 4.
Right
ventricular hypertrophy
Echocardiogra
m, chest x-ray, pulse
oximetry, MRI
Right
ventricular outflow tract
reconstructio
n [28] VSD closure
device [29,
30]
Coarctation
of the aorta
10% Mild-complete
obstruction of
aorta
Magnetic
resonance
angiography, echocardiogra
m
Patch for
aortoplasty
[31]
Patent
ductus
arteriosus
10% Ductus arteriosus
remains open
after birth
Chest x-ray, echocardiogra
m
PDA occlusion
device [32],
occlusion spring coil
[33]
Atrial septal
defect
5% Hole in atrial
septum
Echocardiogra
m, cardiac
auscultation, chest x-ray,
Occlusion
devices [34, 35], patch
closure
materials [36, 37]
Transpositio
n of the
great vessels
5% Abnormal
spatial
arrangement of great
vessels
Echocardiogra
m, X-ray
Arterial
switch
operation [38], septal
occlusion
device
Aortic valve
stenosis
5% Narrowing across aortic
valve
Echocardiogram
Surgical or balloon
valvuloplast
y [39], bioprosthese
s [40]
Ebstein
anomaly
1% Abnormal
tricuspid valve and
atrialization of
ventricle
Echocardiogra
m, ECG, chest x-ray
Valve
reconstruction,
Bioprostheti
c or mechanical
valve,
surgical or transcatheter
placement
[41, 42]
Anomalies
of the
1% Mild-complete obstruction of
Pulse oximetry,
Venous connection
pulmonary
veins
pulmonary
artery
Cardiac
catheterization
reconstructio
n, patch
closure materials
[43, 44]
Tricuspid
atresia
1% Absence of
tricuspid valve
Echocardiogra
m, chest x-ray, ECG
Valve
reconstruction,
Bioprostheti
c or mechanical
valve,
surgical or transcatheter
placement
[42, 45]
Interrupted
aortic arch
1% Underdeveloped aorta
Echocardiogram, loss of
appetite, pale
Patch for aortoplasty
[31]
Hypoplastic
left heart
syndrome
1% Varying
degrees of underdevelope
d aorta, aortic
valve, left ventricle,
mitral valve,
and left atrium
Echocardiogra
m
Left heart
total repair, shunts [46],
aortoplasty
[31]
3. TISSUE ENGINEERING STRATEGIES FOR CARDIAC WALL
REPAIR IN CONGENITAL HEART DISEASE
In congenital heart disease, common abnormalities requiring
surgical intervention involve a lesion or hole in septal heart
tissue requiring closure. Small defects (<5mm) often do not
require surgical intervention and will spontaneously close [54].
However, when the hole is too large, surgeons will place
patches or occlusion materials in a patient to help bridge the
native heart tissue and allow for restored structure. In terms of
an ideal tissue engineering construct, restoring structural
support is only part of the challenge. A biomaterial may meet
the mechanical properties needed to withstand the fatigue of a
contracting heart, but if the material is inert it will not
completely restore native function. Vascularization is also a
limiting factor in current cardiac patches [55]. Unless the
cardiac patch is prevascularized or able to have neovascular
ingrowth, the patch will be diffusion limited and therefore
limited to the overall thickness [56]. Another requirement in
restoring native function is the synchronized beating of an
implanted cardiac patch with the native heart pace [57].
Following the restoration of natural function is the ability of
living tissue to grow and expand. This is particularly important
in pediatric patients, where their continued growth can lead to
implant failure, requiring reoperations [22]. This necessity to
grow and expand presents a unique engineering challenge
which is not as relevant in adult applications. A number of
CHDs require cardiac wall repair, the most common being
ventricular/atrial septal wall repairs using occlusion devices
termed “baffles”, which are defined as materials that direct the
flow of blood between desired chambers while sealing blood
from other chambers [58]. This is contrary to full-thickness
cardiac wall patches where the goal is to augment free wall
structures. Examples of full-thickness cardiac patches needed
during surgical intervention include: ventricular outflow patch

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
5
for tetralogy of Fallot, complete left heart remodeling in
hypoplastic left heart syndrome, and right ventricular patch in
Ebstein anomaly. To date, no commercially available patch can
completely restore native structure and function after
implantation.
Naturally derived cardiac patches
A number of strategies involve the use of naturally derived
materials as a scaffold for a cardiac tissue engineering
construct. The major advantage of naturally derived materials
is that they are composed of molecules found in vivo and will
degrade into natural metabolic products. Also cellular response
can be favorable compared to other synthetic materials in that
adhesion molecules which enhance bioactivity are already
present within the natural material. In CHDs, many surgical
procedures have used autologous pericardium as patch material
[59]. The advantages to this technique are that the material is
immediately available, nonimmunogenic, and free of cost.
Pericardium has mechanical properties that are inferior to
native cardiac tissue and therefore in order to enhance the
mechanical properties, some surgical procedures involve
glutaraldehyde fixation of the material. With this method,
aldehyde groups will crosslink at the amine groups on the
lysine and hydroxylysine residues of pericardium collagen.
Pericardium is typically crosslinked for 15 to 30 minutes,
where the duration of crosslinking can affect the resulting
mechanical properties [60]. Glutaraldehyde is a toxic solution
and therefore adequate washing of the patch material is needed
prior to implantation [61]. Other crosslinking agents, such as
genipin [62] and acyl azide [63], have been tested as well. One
of the main drawbacks in the use of autologous pericardium as a
patch material is the inability of the material to expand or grow
in pediatric patients. Also, crosslinking procedures will lyse
any native cells, as well as create a chemically different
material resulting in possible calcification and fibrous
encapsulation [64].
The use of decellularized matrix as a scaffold is appealing
because the construct was originally functional tissue.
Depending on the decellularization process, key ECM
molecules can be preserved and therefore may help in
promoting new tissue remodeling. Currently there are three
decellularized patches approved for cardiovascular patch
applications; a pulmonary artery patch material
(MatrACELLTM , Virginia Beach, VA), a pericardial patch
(CryoPatch®, CryoLife Inc, Kennesaw, GA), and a
decellularized porcine intestinal submucosa (CorMatrix®,
Alpharetta, GA) [65]. CorMatrix® however is approved only
for use on artery, valve and pericardial tissue repair. Some
disadvantages associated with decellularized matrices are
immunogenicity, risk of disease transmission, and donor
availability [66]. Recent studies by Rajabi-Zeleti et al. [67]
attempt to renew the use of pericardium-derived patches using
an alternative approach to glutaraldehyde fixation. Their group
used decellularized pericardium that was enzymatically
digested and then reformed into pericardium gels. They
showed that after one month of subcutaneous implantation in
rats, the pericardium gel based scaffold had low immunological
response, enhanced angiogenesis, and cardiomyocyte
differentiation compared to control collagen and plain
decellularized pericardium. Crapo et al. [68] show that a small
intestinal submucosa (SIS) based gel seeded with neonatal rat
cardiac cells created tissue closer to physiological function
compared to that of cells seeded on Matrigel. Function was
measured in terms of contraction rate and normalized troponin
T expression, both higher in the SIS gel group. This difference
is attributed to the differing components of each gel. While
both gels contain a variety of different ECM components, the
main difference is that the SIS based gel contains high
concentrations of collagen type I and III, similar to that of
myocardium. At a minimum this study proves that myocardial
cell attachment and resulting function is complex and must be
considered carefully when choosing biomaterials for cardiac
tissue engineering.
Since native cardiac tissue extracellular matrix is
predominately composed of collagen, many studies aim to
manipulate collagen based scaffolds using growth factors
and/or altering properties such as alignment and microstructure
[69]. Collagen has good cellular attachment and proliferation
[70]. The main drawbacks to collagen based scaffolds in tissue
engineering applications are inferior mechanical and
degradation properties. A major requirement for cardiac tissue
engineering is the ability to withstand contractile forces of a
beating heart. Also as a patch material, collagen patches can be
difficult to suture due to their mechanical weakness. However,
since collagen is still the main component of cardiac ECM,
there is relevance to its use as a scaffold. Miyagi et al [71]
produced a collagen based patch that contained covalently
immobilized vascular endothelial growth factor (VEGF). This
patch was implanted into the right ventricular walls of rat hearts
for up to 28 days, showing improved neotissue formation in
terms of cell recruitment, proliferation, and blood vessel
density when compared to scaffolds without VEGF. A higher
density of VEGF immobilization was also shown to have a
greater resulting blood vessel density compared to lower VEGF
concentrations. In another study, Serpooshan et al. [72] used
compressed collagen type I as scaffolds for myocardial
infarction repair. While this is not a congenital disorder, this
patch may have applications for remodeling hearts with
tetralogy of Fallot. Their results after four weeks of
implantation exhibited limited fibrosis, diminished dilation of
the left ventricle, as well as neo-angiogenesis within the patch
when compared to the control.
Because decellularized matrices and purely collagen based
scaffolds both have disadvantages in creating a fully
functioning cardiac patch, other naturally derived polymers
such as alginate, chitosan, and silk fibroin continue to have
research interest [73]. Each of these polymers is extracted
from living organisms and has shown to have applications for
tissue engineering. Studies have shown that alginate, a natural
polymer found in cell walls of seaweed [74], combined with
RGD peptide can be formed into scaffolds for cardiac tissue
engineering. The RGD is important in cellular attachment to
the scaffold, and is immobilized by carbodiimide chemistry.
Shachar et al. [75] show the maintenance of key cardiac
markers, α-actinin, N-cadherin, and connexin-43, suggesting
that alginate-RGD immobilized scaffolds alleviate the need for
the addition of ECM proteins or Matrigel into scaffolds.
Chitosan is also a promising natural polymer investigated as a

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
6
component for cardiac patch tissue engineering. It is a linear
polysaccharide derived from chitin, which is found in shellfish
exoskeletons. Alone, chitosan has been successfully applied to
the wound healing market as a clotting agent accelerating
hemostasis [76]. In tissue engineering, when chitosan is
combined with collagen, the resulting material has mechanical
properties superior than collagen alone. Kathuria et al. [77]
developed and characterized an elastic chitosan-gelatin cryogel
that could be used for potential tissue engineering applications.
This material was able to withstand cyclic deformations up to
40% without significant deformation with a Young’s modulus
ranging from 36-39 kPa.
Silk fibroin is investigated in a number of tissue engineering
applications because it is mechanically strong, noncytotoxic,
presents low immunogenicity, and is biodegradable. An
investigation into silk fibroin from A. mylitta silk worms shows
better cardiomyocyte attachment and functional beating after
seeding for up to 20 days [78]. These results are superior than
similar scaffolds using silk fibroin derived from mulberry B.
mori silk worms. This is proposed to be a result of A. mylitta
having RGD domains. Chi et al, [79] investigated a
chitosan-hyaluronan/silk fibroin cardiac patch implanted into
the left ventricles of rats. This patch was developed creating an
aqueous silk fibroin/chitosan/hyaluronan solution in a 10:1:1
ratio, and then spray-dried into patch form. Their implanted
patch showed reduced dilation of left ventricular diameter (4.27
0.29mm), increased wall thickness (1.5 0.13mm), and
improved left ventricular fractional shortening (42.8 2.4%).
Synthetic based cardiac patches
The use of synthetic polymers in surgical correction of CHDs
is limited to bioinert materials which can often illicit an
inflammatory response and fibrosis. The appeal of synthetic
polymers stem from their tunable mechanical, structural and
degradation properties. Fabrication of synthetic polymer based
scaffolds is very diverse and can involve techniques such as UV
polymerization [80], electrospinning [81], or laser sintering
[82], to name a few. Polymers such as polyethylene
terephthalate and expanded polytetrafluoroethlene (ePTFE)
have been used as cardiac patch materials in areas of lower
cyclic mechanical stress such as the septal wall. However both
polymers are not biodegradable and present issues in terms of
tissue ingrowth and remodeling. Ideally, corrections for CHDs
will only require one surgical procedure. In the case of cardiac
patches, this requires a delicate balance of new tissue ingrowth
aligned with scaffold degradation. Therefore much research
has focused on using biodegradable synthetic polymers such as
poly(lactic-co-glycolic acid) (PLGA), poly(plycerol sebacate)
(PGS), polyurethanes (PU), and polycaprolactone (PCL) as
scaffolds for cardiac tissue applications. The main issue when
using synthetic polymers as a scaffold material is inferior
cellular adhesion compared to that of natural polymers.
Therefore some strategies involve coating synthetic polymers
with other naturally derived materials, as discussed later in the
chapter.
Dacron® (polyethylene terephthalate) grafts are sometimes
used as septal defect patch material. Dacron® is a strong,
stable polymer that exhibits minimal degradation in vivo. Once
implanted, Dacron® elicits an inflammatory reaction and
subsequent fibrosis occurs. This is a structural solution for
defective cardiac tissue as applied to septal repairs, but the
material remains inert [83]. Another synthetic polymer,
ePTFE, is also currently used in repairing CHDs. The patch
materials developed from ePTFE are arranged spatially to have
pores ranging from 20-30 μm, which has shown to inhibit
cellular ingrowth [84]. Also, ePTFE does not induce as much
of a fibrous reaction as Dacron®, and therefore can be used as a
patch in areas of blood flow, such as a right ventricular outflow
reconstruction [85]. Both of these patch materials are far from
an ideal engineered cardiac tissue. Since they are not
remodeled and incorporated into existing tissue and elicit an
inflammatory response [86], they result in deficient mechanical
properties as well as hemodynamic changes. These polymers
will not degrade after implantation and will not promote
complete tissue remodeling. This is important in pediatric
patients that will continue to grow and therefore an inert patch
will likely require subsequent surgical operations.
Creating a synthetic material that is biocompatible and is
able to grow and remodel with a patient is no simple task.
Therefore bioresorbable polymer research into a viable patch
for CHDs has much attention. Like natural polymers, synthetic
bioresorbable polymers will be degraded over time in vivo
resulting from hydrolysis or enzymatic cleavage. The ideal
construct will provide mechanical support long enough for
native or seeded cells to produce and remodel ECM as well as
promote angiogenesis. In CHD patients, this allows for
continued growth without the need for additional surgical
interventions. Poly(lactic-co-glycolic acid) (PLGA) is a
biodegradable polymer that is used in many applications in
tissue engineering from drug delivery to hard and soft tissue.
The appeal of PLGA stems from the naturally metabolized
degradation products of lactic and glycolic acid. Zhou et al.
[55] showed that a PLGA scaffold wrapped with omentum
significantly improved ventricular remodeling and cardiac
function.
PGS has been studied frequently in the field of soft tissue
engineering. PGS is an appealing polymer that is able to
sustain and recover from deformation with minimal loss of
elasticity. Therefore the viscoelastic properties of PGS are
suggested to fit a mechanically dynamic environment such as
the heart. Chen et al. [87] developed a cardiac patch using
preconditioned PGS scaffolds in combination with human
embryonic stem cell-derived cardiomyocytes. The PGS
scaffolds were preconditioned for 6 days in media and
cardiomyocytes were seeded and shown to attach without the
need for a gelatin coating. The conditioned PGS scaffold was
able to sustain beating cardiomyocytes in vitro for longer than 3
months. Recently, Rai et al. [88] created a biomimetic PGS
scaffold attempting to chemically modify the surface of the
material in order to enhance cardiomyocyte attachment. This
was done by a process involving alkaline hydrolysis and
acidification to expose surface carboxyl chemical groups.
These groups could then be functionalized with peptides
YIGSR and GRGDSP in order to promote cellular attachment.
Their results showed that a ligand surface concentration of
10-15 mL/cm2 was sufficient to support attachment and growth
of both rat and human cardiac progenitor cells. The Karp lab
has expanded on the mechanical properties of PGS, creating

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
7
poly(plycerol sebacate urethane) (PGSU). This co-polymer
blend was shown to have tunable mechanics and the ability to
deliver localized biomolecules when tested as a cardiac patch
material [89].
Fujimoto et al. [84] developed a polyester urethane urea
(PEUU) cardiac patch and implanted them into rats with
infarcted left ventricular wall. Their results suggested that the
scaffold promoted ingrowth of smooth muscle bundles with
mature contractile phenotype. Also, 8 weeks after implantation
the PEUU patch was largely resorbed, suggesting cellular
migration and improved cardiac remodeling.
PCL is another synthetic polymer of interest when
considering cardiac patch development. PCL is a
biodegradable polymer and can be hydrolyzed at the ester
linkages forming nontoxic byproducts. Yeong, et al. [82]
fabricated a PCL scaffold using a computer-aided selective
laser sintering technique. This fabrication technique showed
proof of concept for a customizable scaffold design allowing
for uniform control of pore size and patterning. By controlling
the laser wattage and scanning speed, PCL particles were
sintered into a disc shaped scaffold composed of small
repeating square pyramid units. In this particular design, they
were able to obtain a compressive stiffness of 345 kPa. Further
optimization of scaffold design could lead to tensile strengths
closer to native myocardium, which is on the range of 3-15 kPa.
It is important for a patch to exhibit stiffness similar to native
tissue as very elastic materials could form aneurysms and less
elastic materials could present with high local stress areas [90].
Natural/synthetic hybrid based patches
In order to take advantage of the cellular attachment and
signaling capabilities of natural polymers while maintaining a
way to control and optimize mechanical properties, researchers
have investigated a number of materials combining both natural
and synthetic materials. Pok et al. [90, 91] developed a
multilayered scaffold composed of PCL, chitosan and gelatin.
This scaffold was self-assembled with the stronger PCL core
sandwiched between emulsified solutions of gelatin/chitosan
(Figure 1). By controlling the average molecular weight of the
PCL core, the ultimate tensile strength of the scaffold could be
controlled in the range of 2-4 MPa. When combined with the
gelatin/chitosan, the compressive modulus of the scaffold was
close to native cardiac tissue (~15 kPa). This provided for a
biocompatible cardiac patch that when seeded with neonatal rat
ventricular myocytes resulted in spontaneous beating in a 50
vol.% gelatin:50 vol.% chitosan blend. Aside from layering
different polymers, the blending of both natural and synthetic
polymers without any chemical linkages show potential in the
development of viable cardiac scaffolds. Kharaziha et al. [92]
developed a scaffold composed of electrospun PGS and gelatin
nanofibers, showing that a 33 wt.% PGS formulation induced
optimal synchronous contractions of seeded cardiomyocytes.
Recent studies by Martins et al. [93] combine chitosan and
carbon nanofibers to create scaffolds that can enhance the
electrical properties of a patch material as well, showing a
tissue where conductivity is necessary to transmit signals for
beating. Being able to optimize the properties of both natural
and synthetic materials suggests a more adaptive and
structurally sound scaffold compared to a homogenous
construct.
Figure 1: Composite hydrogel patch with a multilayered
structure. The scaffold is made of a self-assembled PCL core
placed between gelatin–chitosan hydrogel layers. (A)
Macroscopic structure after disk formation. (B) Scanning
electron micrograph depicting a cross-section of the scaffold.
Reproduced from [90] with permission.
Injectable cardiac gels
Another highly researched area is the use of injectable
biomaterials for the treatment of myocardial defects. The idea
is that an amorphous matrix composed of critical tissue forming
components (cells, ECM proteins, small molecules) can be
injected directly to the site of deficiency, aiming to preserve
and promote cardiac tissue remodeling [94]. This strategy is
very appealing to myocardial infarction cases where the rapid
degradation of cardiac tissue is unrepairable. While CHDs do
not include myocardial infarction, a number of diseases
(coarctation of the aorta, anomalous origin of the left coronary
artery arising from the pulmonary artery, etc) [95] run the risk
of creating necrotic regions of cardiac tissue due to poor
perfusion or inadequate oxygen saturation of the systemic
blood [96]. As with myocardial infarction, the lack of
oxygenated blood due to CHD can manifest itself immediately
after birth and upon closure of the ductus arteriosus. Aside
from maintaining a PDA by administration of prostaglandin E1,
the use of an injectable cardiac matrix in CHD patients could at
a minimum help to preserve cardiac tissue until other corrective
action can be considered.
Similar to the cardiac patch studies, the variety of
biomaterials used for injectable gels can be both natural and
synthetic. Injectable gels are typically based on natural
materials such as fibrin, collagen, alginate, but there are some
gels which incorporate synthetic polymers either as hydrogel
copolymers or encapsulation vessels [97, 98]. Upon injection
into physiological temperatures (37oC), the gelling of the
components can occur very rapidly, within seconds in most
cases. The other key component of injectable materials are
living cells aimed to assist in regenerating damaged tissue by
paracrine delivery of different signaling molecules such as
growth factors, cytokines, hormones, etc. The key advantages
to an injectable strategy are: 1) they are minimally invasive and
easy to administer through injection, 2) amorphous structure
allows for high contourability allowing the gel to fill various
defect shapes and sizes and 3) therapeutic agents are easily
incorporated and delivered to the defect site.
Fibrin glue has been studied as an injectable material for
myocardium repair. Fibrin glue is currently FDA approved as a

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
8
hemostasis sealant for use during surgical operations [99].
When applied as an endoventricular heart patch, Christman et
al. [100] showed that the use of a fibrin glue increased cell
transport and survival of skeletal myoblasts, decreased the size
of infarcted left ventricle, and increased blow flow to the area
of myocardial ischemia compared to controls. Other studies
focused on the delivery of growth factors with the goal of
enhancing native cardiac cells to survive and proliferate. The
Christman group also developed an injectable material
composed of decellularized heart matrix [101], which was
shown to have endothelial and smooth muscle cell migration as
well as arteriole formation after 11 days. Ruvinov et al. [102]
show that an alginate based gel can be used to sequentially
deliver insulin-like growth factor (IGF-1) and hepatocyte
growth factor (HGF) aimed to induce myocardial regeneration.
The alginate gel sufficiently prevented proteolysis of the two
proteins and when injected into a rat acute myocardial
infarction model, infarct expansion was attenuated and
increased angiogenesis throughout affected area was observed
after 4 weeks. A combination of growth factors and stem cells
as a regenerative therapy is popular as well. This concept will
not only deliver signaling molecules to native cardiac cells, but
provide additional cells that may differentiate and aid in the
remodeling process. Wang et al. [97] developed an injectable
hydrogel composed of collagen type I, chondroitin sulfate, and
a thermosensitive copolymer (Figure 2). This hydrogel was
shown in vitro to be capable of releasing IGF-1 over a 2 week
period in order to enhance the survival and growth of
encapsulated mesenchymal stromal cells (MSC). The
differentiation potential of the MSCs was maintained within the
hydrogel, but the addition of IGF-1 was shown to significantly
accelerate MSC growth. The Davies group conducted studies
into the effects of injectable gels on cardiac tissue remodeling,
showing that injection of PEG based gels following infarction
could aid in the immediate healing and remodeling [103]. They
also showed a temporal remodeling relationship, where the
same gels were injected one week post-infarction had slower
degradation rates compared to gels injected immediately
post-infarction [104].
The major disadvantage of injectable biomaterials for the
repair of infarcted cardiac tissue is that they lack sufficient
stiffness compared to the tissue in chronic diseased states.
Where healthy adult myocardium has a modulus of
approximately 50 kPa , diseased states can range from 200-300
kPa [105]. Ifkovits et. al. elucidated the effects of stiffness on
ovine infarct models using injectable methacrylated hyaluronic
acid hydrogels with varying moduli. The study shows that a
higher modulus (~43 kPa) gel applied post-infarction resulted
in less infarct expansion and reduced left ventricular dilation
compared to a lower modulus (8 kPa) [106]. While these
injectable gels nearly match the modulus of healthy adult
myocardium, the stiffness may not be sufficient to support
chronic diseased myocardium. However, injectable
biomaterials may have potential in pediatric cases where years
of cardiac remodeling have not altered the mechanical
properties of the myocardium.
Figure 2: An injectable, flexible, thermally responsive
hydrogel composite for cardiovascular tissue engineering
applications. The material is comprised of type I collagen,
chondroitin sulfate, and a thermosensitive copolymer based on
N-isopropylacrylamide. (a) The composite is liquid at 4°C. (b)
Hydrogel forms upon temperature increase to 37°C. (c) The
material is injectable through a 26-gauge needle at 4°C. (d)
Hydrogel strip at 37°C before stretching. (e) Hydrogel strip at
37°C after stretching. Reproduced from [97] with permission.
4. HEART VALVE TISSUE ENGINEERING IN CONGENITAL HEART
DISEASE
The direction of blood flow through the heart is regulated by
the heart valves (aortic, pulmonary, mitral and tricuspid valve).
All four heart valves can be affected by a congenital defect.
Problems include stenosis and regurgitation, and both cases
impede physiological blood flow. Ebstein’s anomaly is
characterized by an abnormal structure of the tricuspid valve
and regurgitation. Another type of congenital heart defect is a
bicuspid aortic valve where two cusps are present instead of
three. This defect does not usually involve severe
complications in the pediatric population and surgical
correction, if deemed necessary, is performed well into
adulthood [107]. Anomalies of the pulmonary valve are the
most common among the four valves and are often manifested
in conjunction with other congenital heart defects [108]. Also,
in certain lesions, the pulmonary valve may be underdeveloped
and a reconstruction of the right ventricular outflow tract
(RVOT) is a beneficial option. A valved conduit is used to
connect the right ventricle to the pulmonary artery [109].
When replacing a failing heart valve, a surgeon generally
has the following options: A mechanical valve, or a
bioprosthetic valve which can be either a homograft or a
xenograft. The use of a mechanical valve is associated with
increased risk for thrombosis and patients will need lifelong
anticoagulant medication. Anticoagulants can prove dangerous
for children due to possible hemorrhaging which is a threat in
this physically active patient population. Therefore,
bioprosthetic valves are usually preferred for surgical
correction in pediatric patients. Human donor heart valves are
commonly cryopreserved until implantation, [110] but a main
drawback is immunogenicity [111]. Decellularization
techniques have been more recently proposed to reduce this
effect in homografts [112]. As with all homografts, availability

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
9
is a common limiting factor. In the pediatric population, this
proves even more problematic as a valve of the right size needs
to be found and transplanted for each child. Xenograft valves
are typically bovine or porcine tissues crosslinked with
glutaraldehyde. While xenografts are more readily available
than homografts, the concern about immunogenicity remains
[113, 114]. Bioprosthetic valves, both human and
animal-derived, oftentimes suffer from early degeneration
which can be detrimental to young patients, necessitating
replacement operations. One of the mechanisms of
bioprosthetic heart valve degeneration that can lead to failure is
linked to calcification. The phenomenon of bioprosthetic heart
valve calcification has been reviewed elsewhere [115].
As an alternative to tissue crosslinking, decellularization
has been introduced in order to preserve the original tissue
matrix to a certain extent while reducing cellular antigens.
Commercially available decellularized heart valve porcine
xenografts (e.g. Synergraft®, Matrix P®) and homografts
(CryoValve SG®) exist that are suitable for use in a pediatric
congenital heart disease population. However, failure resulting
in death or need for graft replacement has been reported for
porcine decellularized heart valves due to a possible immune
response and limited cell migration from the host causing poor
recellularization [116-118].
Another option for the surgical management of aortic valve
disease in children is the Ross procedure. During this
procedure, the aortic valve is replaced by the patient’s own
pulmonary valve. Since an autograft is placed in the aortic
position, the commonly associated problems with mechanical,
homo-or xenograft valves are eliminated, but it generates the
need for a suitable replacement for the pulmonary valve [119].
The autologously implanted aortic valve has been shown to
grow and function satisfactorily in young children [120].
For all types of currently available options, excluding the
new aortic valve after the Ross procedure, as the child grows,
reoperation will be necessary to provide a new valve that
matches their size. Additionally, the prosthetic tissues have
limited intrinsic potential for repair. General risk factors for
prosthetic heart valve complications in children have been
identified, which include age and type of defect [110, 121].
Therefore, the field of tissue engineering has been faced with
much anticipation for a solution that can eliminate some of the
current limitations in heart valve replacement for children.
Heart valves are unique tissues considering their
architecture and the biomechanical environment in which they
operate. Even though all four valves show a similar pattern in
cell phenotypes and extracellular matrix components, they have
structural and morphological variances. These differences in
structure allow valves to optimally serve their function, for
example the high pressure setting of the aortic valve presents
different mechanical loading compared to the lower-pressure
pulmonary circulation. Moreover, heterogeneity and anisotropy
is pronounced within regions of each valve [122-124].
Therefore, a profound understanding of the properties of each
valve is important in order to create tissue engineered analogs.
The field of heart valve tissue engineering is largely benefitting
from research performed in the biomechanics, mechanobiology
and cell biology of heart valves [125-128].
Approaches involving naturally derived matrices
Building upon the existing surgical practice of bioprosthetic
valves, heart valves have been decellularized and reseeded with
cells following a tissue engineering paradigm. The goal of this
effort is to combine the advantageous properties of a native
matrix with the regenerative and remodeling potential of living,
autologous cells. The first clinical case of this kind was
described in 2002. A cryopreserved pulmonary homograft was
decellularized and reseeded with endothelial cells from the
patient's forearm vein. One year after implantation, the patient
was in good clinical condition with appropriate valve function
[129]. The same group reported the results of clinical studies
performed over ten years. Eleven adult patients, some of them
with congenital heart disease, underwent the Ross procedure
and a tissue engineered heart valve (TEHV) was placed in the
pulmonary position. The TEHV was fabricated as above. At the
ten-year follow-up, the survival rate was 100% and there were
no signs of valve regurgitation, calcification or morphologic
degradation. These results were encouraging, however more
long-term studies are needed to evaluate the longevity of these
valves, especially in a younger patient population [130]. A
clinical report involving the placement of decellularized and
reseeded pulmonary valves in two pediatric tetralogy of Fallot
patients was reported in 2006. Autologous endothelial
progenitor cells were harvested from peripheral blood and
seeded on valve homografts. Both children were doing well
clinically at the 3.5 year follow-up. The valves showed
sufficient mobility, no degeneration or stenosis, and
importantly, they were shown to grow with the children [131].
These approaches have shown promising clinical value, but
certain limitations are still present. The decellularized matrix is
a homograft, and the donor scarcity problem remains. The cell
harvesting, often done in an invasive manner, as well as the
isolation and expansion procedures, impose an additional step
which is time-and effort-consuming. Adequate quality control
systems must be in place. Finally, there are questions about the
fate of the seeded cells and their role in the regenerative
process. Work by Roh et al. [132] has shed some light on the
last question and will be discussed in the next chapter.
Therefore, some researchers have focused on the in situ
recellularization from the host. This approach falls under the
classical tissue engineering paradigm, which involves
scaffolds, cells and stimuli, and where cell seeding happens in
vivo. Commercially available, decellularized and not re-seeded
matrices have not always been very successful clinically, and
even devastating in some cases, as previously mentioned
[116-118]. Factors that will stimulate and improve the active in
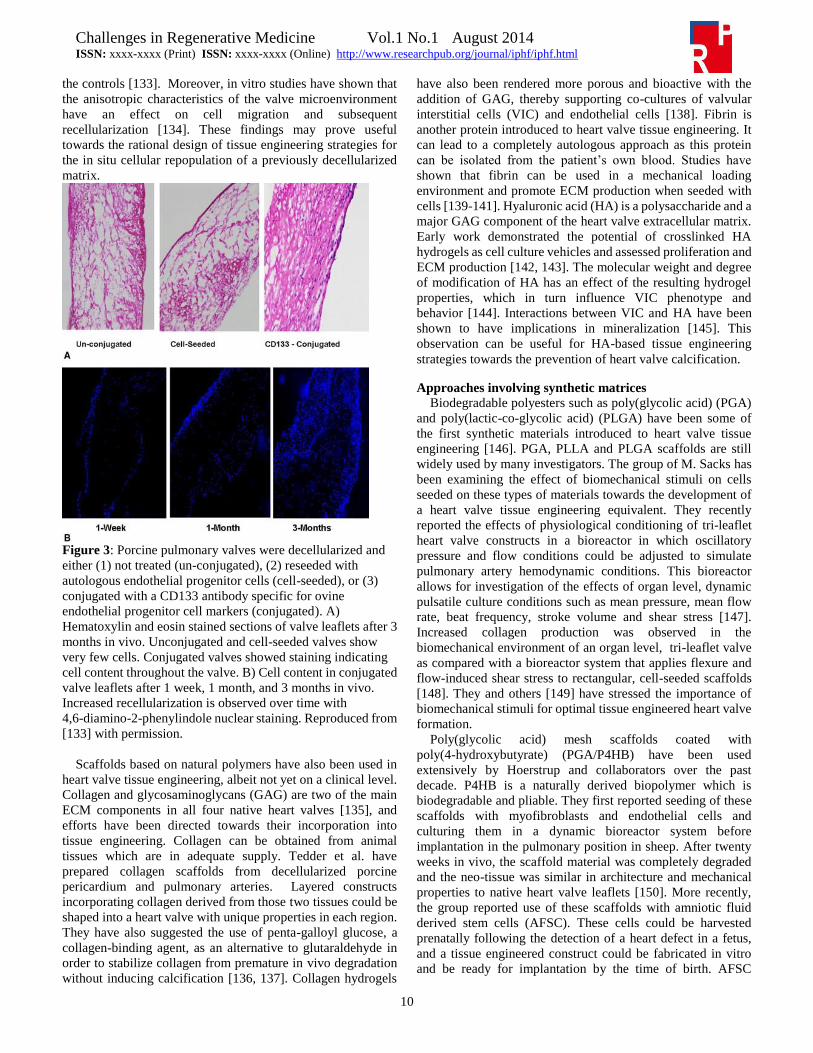
vivo recellularization are currently being investigated. Jordan et
al. decellularized porcine pulmonary valves and conjugated
them with an antibody that recognized ovine endothelial
progenitor cell (EPC) markers. The valves were implanted in
sheep in the pulmonary position. At three months
post-implantation, histological characterization showed
significantly higher cell numbers in the antibody-conjugated
valves compared to unconjugated, unseeded matrices or valves
seeded with EPCs that served as controls. On the latter type, the
initially seeded cells seemed to have disappeared within the
first month (Figure 3). The mechanical properties of the
conjugated valves were also found to be superior compared to
Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
10
the controls [133]. Moreover, in vitro studies have shown that
the anisotropic characteristics of the valve microenvironment
have an effect on cell migration and subsequent
recellularization [134]. These findings may prove useful
towards the rational design of tissue engineering strategies for
the in situ cellular repopulation of a previously decellularized
matrix.
Figure 3: Porcine pulmonary valves were decellularized and
either (1) not treated (un-conjugated), (2) reseeded with
autologous endothelial progenitor cells (cell-seeded), or (3)
conjugated with a CD133 antibody specific for ovine
endothelial progenitor cell markers (conjugated). A)
Hematoxylin and eosin stained sections of valve leaflets after 3
months in vivo. Unconjugated and cell-seeded valves show
very few cells. Conjugated valves showed staining indicating
cell content throughout the valve. B) Cell content in conjugated
valve leaflets after 1 week, 1 month, and 3 months in vivo.
Increased recellularization is observed over time with
4,6-diamino-2-phenylindole nuclear staining. Reproduced from
[133] with permission.
Scaffolds based on natural polymers have also been used in
heart valve tissue engineering, albeit not yet on a clinical level.
Collagen and glycosaminoglycans (GAG) are two of the main
ECM components in all four native heart valves [135], and
efforts have been directed towards their incorporation into
tissue engineering. Collagen can be obtained from animal
tissues which are in adequate supply. Tedder et al. have
prepared collagen scaffolds from decellularized porcine
pericardium and pulmonary arteries. Layered constructs
incorporating collagen derived from those two tissues could be
shaped into a heart valve with unique properties in each region.
They have also suggested the use of penta-galloyl glucose, a
collagen-binding agent, as an alternative to glutaraldehyde in
order to stabilize collagen from premature in vivo degradation
without inducing calcification [136, 137]. Collagen hydrogels
have also been rendered more porous and bioactive with the
addition of GAG, thereby supporting co-cultures of valvular
interstitial cells (VIC) and endothelial cells [138]. Fibrin is
another protein introduced to heart valve tissue engineering. It
can lead to a completely autologous approach as this protein
can be isolated from the patient’s own blood. Studies have
shown that fibrin can be used in a mechanical loading
environment and promote ECM production when seeded with
cells [139-141]. Hyaluronic acid (HA) is a polysaccharide and a
major GAG component of the heart valve extracellular matrix.
Early work demonstrated the potential of crosslinked HA
hydrogels as cell culture vehicles and assessed proliferation and
ECM production [142, 143]. The molecular weight and degree
of modification of HA has an effect of the resulting hydrogel
properties, which in turn influence VIC phenotype and
behavior [144]. Interactions between VIC and HA have been
shown to have implications in mineralization [145]. This
observation can be useful for HA-based tissue engineering
strategies towards the prevention of heart valve calcification.
Approaches involving synthetic matrices
Biodegradable polyesters such as poly(glycolic acid) (PGA)
and poly(lactic-co-glycolic acid) (PLGA) have been some of
the first synthetic materials introduced to heart valve tissue
engineering [146]. PGA, PLLA and PLGA scaffolds are still
widely used by many investigators. The group of M. Sacks has
been examining the effect of biomechanical stimuli on cells
seeded on these types of materials towards the development of
a heart valve tissue engineering equivalent. They recently
reported the effects of physiological conditioning of tri-leaflet
heart valve constructs in a bioreactor in which oscillatory
pressure and flow conditions could be adjusted to simulate
pulmonary artery hemodynamic conditions. This bioreactor
allows for investigation of the effects of organ level, dynamic
pulsatile culture conditions such as mean pressure, mean flow
rate, beat frequency, stroke volume and shear stress [147].
Increased collagen production was observed in the
biomechanical environment of an organ level, tri-leaflet valve
as compared with a bioreactor system that applies flexure and
flow-induced shear stress to rectangular, cell-seeded scaffolds
[148]. They and others [149] have stressed the importance of
biomechanical stimuli for optimal tissue engineered heart valve
formation.
Poly(glycolic acid) mesh scaffolds coated with
poly(4-hydroxybutyrate) (PGA/P4HB) have been used
extensively by Hoerstrup and collaborators over the past
decade. P4HB is a naturally derived biopolymer which is
biodegradable and pliable. They first reported seeding of these
scaffolds with myofibroblasts and endothelial cells and
culturing them in a dynamic bioreactor system before
implantation in the pulmonary position in sheep. After twenty
weeks in vivo, the scaffold material was completely degraded
and the neo-tissue was similar in architecture and mechanical
properties to native heart valve leaflets [150]. More recently,
the group reported use of these scaffolds with amniotic fluid
derived stem cells (AFSC). These cells could be harvested
prenatally following the detection of a heart defect in a fetus,
and a tissue engineered construct could be fabricated in vitro
and be ready for implantation by the time of birth. AFSC

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
11
showed growth and differentiation potential when cultured in a
bioreactor system. The mechanical properties of the resulting
valves did not reach physiological values, but sufficient
opening and closing of the valves was observed [151]. Seeded
scaffolds were implanted in sheep fetuses in the pulmonary
position via a minimally invasive transapical technique (Figure
4). This work served as a first proof of concept for a single-step,
fetal cardiac interventional procedure with potential
implications in congenital heart disease [152]. Another
approach presented by the same group involved the
decellularization of a PGA/P4HB scaffold that was previously
seeded with human myofibroblasts and cultured dynamically in
a bioreactor. These decellularized tissue engineered heart
valves showed significantly higher recellularization in vivo in a
non-human primate model as compared to decellularized native
homograft valves, which served as controls. The authors
suggest that this in situ tissue engineering approach might
facilitate the creation of “off the shelf” non-immunogenic heart
valve analogs [153].
Figure 4: Amniotic fluid stem cell-based heart valves. (a)
Matrices were fabricated from PGA and placed within
self-expandable stents. Asterisk indicates the three valve
leaflets. (b) Matrices were coated with P4HB. Demonstrated
here is the micro-CT image with arrows indicating the
PGA-P4HB-composite matrix. (c-d) Amniotic fluid stem cells
were seeded onto the valves using fibrin as a carrier. Grating
interferometry showed homogeneous cell seeding throughout
the scaffold. Arrows indicate fibrin matrix. (e) Macroscopic
view of cell-seeded matrix. (f-h) The cell-seeded matrices were
crimped and placed inside the delivery system. (i) Planar
fluorescence reflectance imaging was performed to analyze cell
loss during crimping. Red signal indicates autofluorescence
and yellow is specific signal for CFSE-labeled cells. (j)
Confocal microscopy image of cell-seeded matrix.
CFSE-labeled cells appear green. Reproduced from [152] with
permission.
Other synthetic materials currently used in heart valve tissue
engineering include polycaprolactone [154], poly(glycerol
sebacate) [155] or combinations thereof [156]. Polyurethanes
have been also attractive because of their largely tunable
properties [157, 158]. Poly (ethylene glycol) (PEG) hydrogels
have been used as three-dimensional matrices for valvular
interstitial cell encapsulation. Studies have led to a better
understanding of the cells’ mechanobiology while suggesting
that PEG-based hydrogels can be tailored to provide an
instructive environment for the development of more mature
tissues [159, 160]. Hydrogels also allow for the fabrication of
layered constructs which can mimic the architecture and
mechanical function of each region of the native valve.
Tri-layered PEG hydrogels with two stiff outer layers and a soft
inner layer as proposed by the researchers have potential of
creating a multilaminate environment for cell encapsulation
[161]. In another biomimetic approach, PEG-PLLA hybrid
scaffolds were electrospun and each region was functionalized
with biomolecules present in the extracellular matrix of native
heart valves [162]. In summary, promising results have been
obtained with synthetic matrices, however a better
understanding of their in vivo behavior, especially with regard
to cell infiltration and biomechanical performance, is necessary
before clinical translation.
5. BLOOD VESSEL TISSUE ENGINEERING IN CONGENITAL HEART
DISEASE
It is important to differentiate how disorders involving the
blood vessels which may benefit from tissue engineering
present in children as compared to adults. Whereas heart
disease affecting children is mostly congenital, many forms of
acquired heart disease in adults stem from atherosclerosis,
which is caused by the buildup of fatty plaque inside the
arteries. This results in narrowing of the arteries leading to a
reduction in tissue perfusion. Coronary artery disease is a
common and serious manifestation. Bypass surgery is one of
the possible treatments for coronary artery disease, in which a
vascular graft is required.
Congenital heart defects involving blood vessels include
coronary artery anomalies [163], coarctation (narrowing) of the
aorta [164], interrupted aortic arch [165], and pulmonary artery
stenosis [166]. However, there are certain cases of complex
congenital heart disease, in which the blood flow to and from
the heart needs to be rearranged. This rearrangement allows for
proper oxygenation of the blood and improvement of
hemodynamic properties. In a structurally normal, biventricular
heart, the systemic and pulmonary circulations are each
supported by a ventricle and the circulations are in series. One
particular congenital defect is a heart with only one functional
ventricle. In patients born with a single ventricular chamber, the
two circulations are in parallel and patients only survive
because the systemic and pulmonary venous bloods mix [167].
A palliative surgical procedure that has been applied for
treatment of children born with a functional single ventricle is
the Fontan operation and its variations. The various
Fontan-type procedures involve diverting the systemic venous
blood to the pulmonary arteries, bypassing the right heart [168,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
12
169]. These surgeries are performed in stages and grafts are
required for the vascular reconstruction.
Solutions used by pediatric cardiothoracic surgeons include
synthetic and biological grafts. Synthetic polymer grafts such
as polyethylene terephthalate (Dacron®) and the currently
more prevalent expanded polytetrafluoroethylene (ePTFE,
Gore-Tex®) have been associated with increased risk for
thrombus formation, stenosis, foreign body reaction, and
calcification [170]. Due to the increased risk of thrombosis,
life-long use of anticoagulants is essential. Biological grafts
include auto-and homografts, which have a lower tendency for
thromboembolic events, but may show early degeneration due
to increased calcification [171, 172]. Additionally, their supply
is not always guaranteed. Vascular grafts presently employed
for Fontan-type operations and their limitations are
summarized in a review article by Patterson et al [173]. For
pediatric surgery, a vascular graft typically has smaller
diameters than those needed for similar procedures in adults,
and most importantly, it needs the ability to grow with the
patient and have high life expectancy. One exception where
growth is not required is the case of vascular grafts used in
temporary shunt systems as for example the modified
Blalock-Taussig shunt. This shunt connects the systemic to the
pulmonary artery and provides short-term palliation in complex
cyanotic cases until further corrective or palliative surgery can
be performed [174].
General considerations for blood vessel tissue engineering
Progress in the field of blood vessel tissue engineering has
brought some initial successes, and important basic research
has improved our understanding of the physiological
remodeling process. Some recent review articles [175-177]
summarize the advances in the general area of blood vessel
tissue engineering. As with other tissue engineering paradigms,
approaches include the use of cells with and without scaffolds,
which can be either decellularized native matrix, or a
natural/synthetic material. Some of the remaining challenges to
be resolved before tissue engineered blood vessels can be
translated into clinical practice have been in highlighted in
articles by L’Heureux et al. [178] and Udelsman et al. [179].
In the case of cell-seeded matrices, the cell source must be
easily accessible and cells should be readily expandable in
sufficient numbers in order not to slow down the
transplantation process. Additionally, a reproducible cell
seeding technique is important [180, 181]. Endothelial cells
play an important role in the function of blood vessels. They
serve as the interface between the blood and the vessel wall,
and among other functions, increase thromboresistance. The
presence of endothelial cells in tissue engineered blood vessels
has been shown to impart patency and prevent the formation of
thrombi [182]. Early studies by Campbell et al. [183] utilized a
silastic tube placed in the peritoneal cavity of rats and rabbits
which was covered in granulation tissue after two weeks in
vivo. This tissue was removed from the silastic tube, which
served as the inflammatory agent, and inverted. A layered
structure with myofibroblasts and collagen was observed.
Mesothelial cells, or migrated endothelial cells, which stained
positive for von Willebrand factor, formed the innermost layer.
The tube made of tissue was implanted in experimental animals
and served as a patent vascular graft over a period of four
months. In recent years, the quest for the elucidation of the
mechanism of endothelialization in vivo along with the
questions on graft stenosis as observed in early clinical trials
[184] have led to the intense investigation of the molecular and
cellular processes that govern the in vivo remodeling of tissue
engineered blood vessels. It was demonstrated that scaffolds
seeded with bone marrow mononuclear cells elicited an
inflammatory response in vivo, which attracted host
monocytes. The graft matured into a living blood vessel
repopulated with endothelial and smooth muscle cells over six
months. Interestingly, the initially seeded bone marrow
mononuclear cells were not detectable a few days after
implantation [132]. Further studies confirmed the adjacent
blood vessel wall as the source of the endothelial and smooth
muscle cells that were found in the tissue engineered blood
vessel graft [185]. Moreover, macrophage infiltration was
shown to be involved in the formation of stenosis in a murine
model [186]. These studies proved the importance of the
inflammation process in the in vivo remodeling of tissue
engineered blood vessels, and have initiated a discussion on the
role of seeded cells in the various tissue engineering models.
Blood vessel tissue engineering in congenital heart disease:
First clinically relevant attempts
Besides the need for small diameter (<6mm) vascular grafts
for coronary artery bypass surgeries in adults, for which no
ideal and readily available substitute exists, tissue engineering
has been also recognized as a potential solution for pediatric
vascular grafts. One of the first reported studies geared
specifically towards congenital heart defects was the work on
tissue engineered pulmonary artery autografts in 1998. Shinoka
et al [187] performed an in vivo study in sheep replacing a 2-cm
segment of their pulmonary arteries with tissue engineered
grafts. Tubular scaffolds were made of biodegradable
polyglactin/ polyglycolic acid mesh. The cellular source was
autologous artery or vein. Cells were separated and the
endothelial cell-rich fraction was seeded in the lumen, whereas
the endothelial-deficient fraction was seeded on the periphery
of the scaffold. After implantation, the sheep were monitored
by echocardiography and angiocardiography, and samples were
harvested in intervals up to six months. No scaffold material
was detectable after 11 weeks. Seeded scaffolds were patent
and did not show macroscopic signs of calcification, but
evidence of ECM remodeling and diameter increase was
observed.
The first successful clinical application of a tissue
engineered vascular graft was reported in 2001 in Japan. A
four-year old girl with single ventricle physiology received a
construct made of a PLLA/PCL copolymer reinforced with
PGA fibers and seeded with autologous peripheral vein cells.
The cells were previously expanded over a period of eight
weeks. The patient had previously undergone the Fontan
procedure and a 2-cm segment of her pulmonary artery was
occluded and needed replacement. The tissue engineered graft
had been cultured in vitro for ten days prior to implantation, and
measured 10 mm in diameter, 20 mm in length and 1 mm in
thickness. The polymer was designed to degrade within eight
weeks in vivo. No complications were reported immediately

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
13
after the surgery, and seven months post-operatively, the
patient was doing well [188]. Soon after, the same group
initiated a clinical trial in Japan involving a biodegradable
scaffold composed of PGA and PLLA or PCL formed into a
tubular graft. Autologous bone marrow-derived mononuclear
cells were obtained and seeded onto the scaffolds. The recipient
cohort comprised of twenty-five patients with single ventricle
physiology with an age range from 1 to 24 years. After the
surgery, patients were treated with anticoagulants for three to
six months and were monitored by angiography,
echocardiography and computed tomography. No adverse
reactions were reported immediately postoperatively. At a
late-term follow up (mean of 5.8 years after implantation) no
evidence of graft rupture, aneurysm, or ectopic calcification
was observed (Figure 5). No graft related mortality was
reported, however one patient died 6 months post implantation
of congestive heart failure, and three more within four years.
The later-term deaths were related to other cardiovascular
anomalies. Graft stenosis was observed in 24% of the patients.
This study as the first of its kind demonstrated the feasibility
and relevance of tissue engineered vascular grafts in congenital
heart surgery. It also raised questions about the in vivo
mechanisms of vessel remodeling and the causes of graft
stenosis [184].
Figure 5: Results from the first human trial involving tissue
engineered blood vessels in congenital heart disease. A tissue
engineered vascular graft was fabricated by seeding
mononuclear cells on a biodegradable scaffold and evaluated in
pediatric patients with single ventricle physiology. Image
depicts a computed tomography (CT) scan one year after the
tissue engineered vascular graft was implanted. The arrows
indicate the extracardiac graft. No signs of aneurysm formation
and graft rupture were observed, and the graft remained patent.
Reproduced from [184] with permission.
Further advances in blood vessel tissue engineering for
congenital heart disease
Hoerstrup et al. [189] demonstrated the fabrication of
pulmonary artery conduits using human umbilical cord cells
seeded on synthetic biodegradable PGA/P4HB scaffolds and
cultured in a bioreactor. Morphologic characterization of the
tissue engineered pulmonary artery showed ECM formation
and myofibroblast viability, and the construct’s mechanical
properties were comparable to human tissue. The authors
proposed umbilical cord cells as a new and easily available cell
source for tissue engineering with potential applications in
congenital heart disease. These cells could be harvested at birth
and cultured in vitro with promising growth potential. More
recently, the same authors evaluated amniotic-fluid derived
stem cells which is another attractive cell source for congenital
applications. They were able to construct in vitro small-and
large-diameter vascular grafts as a first pre-clinical attempt
[153].
Another approach suggested the use of a decellularized
allogeneic matrix as a scaffold for pulmonary artery tissue
engineering [190]. Ovine pulmonary arteries were
decellularized and seeded with autologous endothelial cells
obtained from carotid arteries, and subsequently implanted in
sheep. Unseeded, decellularized arteries served as controls.
After six months, no calcification or thrombus formation was
observed in any of the explanted blood vessels. All vessels
showed an increase in diameter; however the unseeded blood
vessels showed a disproportionate increase in diameter
resulting in aneurysm formation. This study served as a proof
of concept for the in vitro re-endothelialization of
decellularized pulmonary arteries as an alternative to
biodegradable synthetic scaffolds, and their short-term
performance in vivo.
The field of congenital heart disease may benefit from the
overall developments in the field of blood vessel tissue
engineering. Some challenges that remain are the translation
into high-pressure areas such as for congenital defects of the
aorta, as early studies by Shinoka and colleagues have been in
low-pressure systems. Compliance properties of the neo-vessel
should match those of the native vessels as the child grows.
Finally, more information on long-term outcomes is warranted.
The first clinical trial in the United States specifically geared
towards pediatric heart defects was initiated in 2009 with Dr.
Christopher Breuer as the principal investigator (A Pilot Study
Investigating the Clinical Use of Tissue Engineered Vascular
Grafts in Congenital Heart Surgery) [191]. Results of the study
had not been published at the time of writing this manuscript.
6. CONCLUSIONS
Current surgical management options for the treatment of
congenital heart disease have some limitations, and outcomes
could be potentially improved by employment of tissue
engineering strategies. Significant progress has been made in
the tissue engineering of cardiac patches, heart valves and
blood vessels, with valuable implications for their applicability
in congenital heart disease. Clinical studies with tissue
engineered heart valves and blood vessels have generated
excitement and paved the way for further research. However, a
clear appreciation of the in vivo processes is warranted for the

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
14
successful clinical translation of tissue engineering strategies.
Current research is broadening our knowledge about the in vivo
molecular mechanisms that govern cell behavior as well as
material-host interaction. Pediatric cardiac tissue engineering
shares most of the challenges that the general field is facing,
and some unique ones. A thorough understanding of the
patients and their needs is important so that appropriate
strategies can be designed. Ideally, a graft that grows with the
patients and one that is durable over their entire life span is
desired. In order to achieve this goal, more long term studies
need to be implemented. Appropriate animal models that can
parallel children’s growth and can demonstrate the long term
behavior of tissue engineered implants are necessary. Many of
the current studies are performed on adult animals, which may
not prove sufficient indicators for pediatric cardiac tissue
engineering. Scaffold materials might provoke varying
inflammatory responses and exhibit different degradation
profiles in younger versus adult bodies. The benefits of
including autologous cells in the tissue engineering paradigm
for children must be evaluated. Often, time is an extremely
critical factor and cell expansion can be time-consuming,
unless potent cells can be harvested prenatally in a safe manner
and be ready for use by the child’s birth. Lastly, the potential of
tissue engineering stems from its multidisciplinary nature.
Great progress can be achieved if research projects can bring
together basic scientists, engineers, and pediatric clinician
specialists, to work in a concerted effort. Once these challenges
are overcome, there is great opportunity for tissue engineering
to provide a solution to the large number of children affected by
congenital heart disease.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Wilson Lam for
consultation on the congenital heart defects. Grant support
through NSF (CAREER to J.G.J.) and AHA (Beginning Grant
in Aid to J.G.J.) is gratefully acknowledged.
References
[1] Hoffman JIE, Kaplan S, The incidence of congenital
heart disease, Journal of the American College of
Cardiology, 2002; 39(12): 1890-1900,
[2] Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle
WT, Correa A, Prevalence of congenital heart defects
in metropolitan Atlanta, 1998-2005, The Journal of
Pediatrics, 2008; 153(6): 807-813,
[3] Yang Q, Chen H, Correa A, Devine O, Mathews TJ,
Honein MA, Racial differences in infant mortality
attributable to birth defects in the United States,
1989–2002, Birth Defects Research Part A: Clinical
and Molecular Teratology, 2006; 76(10): 706-713,
[4] Gilboa SM, Salemi JL, Nembhard WN, Fixler DE,
Correa A, Mortality Resulting From Congenital Heart
Disease Among Children and Adults in the United
States, 1999 to 2006Clinical Perspective, Circulation,
2010; 122(22): 2254-2263,
[5] Øyen N, Poulsen G, Boyd HA, Wohlfahrt J, Jensen
PK, Melbye M, Recurrence of congenital heart defects
in families, Circulation, 2009; 120(4): 295-301,
[6] Hartman RJ, Rasmussen SA, Botto LD,
Riehle-Colarusso T, Martin CL, Cragan JD, Shin M,
Correa A, The contribution of chromosomal
abnormalities to congenital heart defects: a
population-based study, Pediatric cardiology, 2011;
32(8): 1147-1157,
[7] Bruneau BG, The developmental genetics of
congenital heart disease, Nature, 2008; 451(7181):
943-948,
[8] Miller A, Riehle-Colarusso T, Alverson C, Frías JL,
Correa A, Congenital heart defects and major
structural noncardiac anomalies, Atlanta, Georgia,
1968 to 2005, The Journal of Pediatrics, 2011;
159(1): 70-78. e2,
[9] Russo CA, Elixhauser A, Hospitalizations for birth
defects, 2004, 2007;
[10] El-Hamamsy I, Eryigit Z, Stevens L-M, Sarang Z,
George R, Clark L, Melina G, Takkenberg JJ, Yacoub
MH, Long-term outcomes after autograft versus
homograft aortic root replacement in adults with aortic
valve disease: a randomised controlled trial, The
Lancet, 2010; 376(9740): 524-531,
[11] Brown JW, Ruzmetov M, Eltayeb O, Rodefeld MD,
Turrentine MW, Performance of SynerGraft
decellularized pulmonary homograft in patients
undergoing a Ross procedure, The Annals of Thoracic
Surgery, 2011; 91(2): 416-423,
[12] Langer R, Vacanti JP, Tissue engineering, Science,
1993; 260(5110): 920+,
[13] Giannoudis PV, Einhorn TA, Marsh D, Fracture
healing: the diamond concept, Injury, 2007; 38(S3-S6,
[14] Pinto NM, Keenan HT, Minich LL, Puchalski MD,
Heywood M, Botto LD, Barriers to prenatal detection
of congenital heart disease: a population-based study,
Ultrasound in Obstetrics & Gynecology, 2012; 40(4):
418-425,
[15] Burdi AR, Huelke DF, Snyder RG, Lowrey GH,
Infants and children in the adult world of automobile
safety design: pediatric and anatomical considerations
for design of child restraints, J Biomech, 1969; 2(3):
267-80,
[16] Adkins B, T-cell function in newborn mice and
humans, Immunol Today, 1999; 20(7): 330-5,
[17] Diaz-Jauanen E, Strickland RG, Williams RC, Studies
of human lymphocytes in the newborn and the aged,
Am J Med, 1975; 58(5): 620-8,
[18] Hicks MJ, Jones JF, Minnich LL, Weigle KA, Thies
AC, Layton JM, Age-related changes in T- and
B-lymphocyte subpopulations in the peripheral blood,
Arch Pathol Lab Med, 1983; 107(10): 518-23,
[19] Manji RA, Zhu LF, Nijjar NK, Rayner DC, Korbutt
GS, Churchill TA, Rajotte RV, Koshal A, Ross DB,
Glutaraldehyde-fixed bioprosthetic heart valve
conduits calcify and fail from xenograft rejection,
Circulation, 2006; 114(4): 318-27,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
15
[20] Ross DN, Evolution of the homograft valve, Ann
Thorac Surg, 1995; 59(3): 565-7,
[21] Wong ML, Griffiths LG, Immunogenicity in
xenogeneic scaffold generation: Antigen removal vs.
decellularization, Acta Biomater, 2014;
[22] Hopkins RA, Lofland GK, Congenital, reconstructive
and regenerative cardiac surgery, Progress in
Pediatric Cardiology, 2013; 35(2): 87-90,
[23] Dolbec K, Mick NW, Congenital Heart Disease,
Emergency Medicine Clinics of North America, 2011;
29(4): 811-827,
[24] Talwar S, Keshri VK, Choudhary SK, Gupta SK,
Ramakrishnan S, Saxena A, Kothari SS, Juneja R,
Kumar G, Airan B, Unidirectional valved patch
closure of ventricular septal defects with severe
pulmonary arterial hypertension: Hemodynamic
outcomes, The Journal of Thoracic and
Cardiovascular Surgery, 0):
[25] Caimmi PP, Grossini E, Kapetanakis EI, Boido R,
Coppo C, Scappellato F, Vacca G, Teodori G, Double
Patch Repair Through a Single Ventriculotomy for
Ischemic Ventricular Septal Defects, The Annals of
Thoracic Surgery, 2010; 89(5): 1679-1681,
[26] Gruenstein DH, Bass JL, Transcatheter device closure
of congenital ventricular septal defects, Progress in
Pediatric Cardiology, 2012; 33(2): 131-141,
[27] Zhang B, Wu S, Liang J, Zhang G, Jiang G, Zhou M,
Li X, Unidirectional Monovalve Homologous Aortic
Patch for Repair of Ventricular Septal Defect With
Pulmonary Hypertension, The Annals of Thoracic
Surgery, 2007; 83(6): 2176-2181,
[28] Castleberry CD, Gudausky TM, Berger S, Tweddell
JS, Pelech AN, Stenting of the right ventricular
outflow tract in the high-risk infant with cyanotic
teratology of Fallot, Pediatr Cardiol, 2014; 35(3):
423-30,
[29] Shuhaiber JH, Robinson B, Gauvreau K, Breitbart R,
Mayer JE, del Nido PJ, Pigula F, Outcome after repair
of atrioventricular septal defect with tetralogy of
Fallot, The Journal of Thoracic and Cardiovascular
Surgery, 2012; 143(2): 338-343,
[30] Ong J, Brizard CP, d'Udekem Y, Weintraub R,
Robertson T, Cheung M, Konstantinov IE, Repair of
Atrioventricular Septal Defect Associated With
Tetralogy of Fallot or Double-Outlet Right Ventricle:
30 Years of Experience, The Annals of Thoracic
Surgery, 2012; 94(1): 172-178,
[31] Patel NH, Madan TH, Panchal AM, Thakkar BM,
Percutaneous closure of patent ductus arteriosus via
internal jugular vein in patient with interrupted
inferior vena cava, Annals of pediatric cardiology,
2009; 2(2): 162,
[32] Moore JW, George L, Kirkpatrick SE, Mathewson
JW, Spicer RL, Uzark K, Rothman A, Cambier PA,
Slack MC, Kirby WC, Percutaneous closure of the
small patent ductus arteriosus using occluding spring
coils, Journal of the American College of Cardiology,
1994; 23(3): 759-765,
[33] Fischer G, Masura J, Kramer HH, Gavora P,
Transcatheter occlusion of secundum atrial septal
defects with the self-centering Amplatzer Septal
Occluder, Progress in Pediatric Cardiology, 1999;
9(2): 119-124,
[34] Urena M, Rodés-Cabau J, Freixa X, Saw J, Webb JG,
Freeman M, Horlick E, Osten M, Chan A, Marquis
J-F, Champagne J, Ibrahim R, Percutaneous Left
Atrial Appendage Closure With the AMPLATZER
Cardiac Plug Device in Patients With Nonvalvular
Atrial Fibrillation and Contraindications to
Anticoagulation Therapy, Journal of the American
College of Cardiology, 2013; 62(2): 96-102,
[35] Aksüt M, Boyacıoğlu K, Kayalar N, Double-Layer
Pericardial Patch for Atrial Septal Defect Closure,
Heart, Lung and Circulation, 0):
[36] Ugaki S, Khoo NS, Ross DB, Rebeyka IM, Adatia I,
Modified Single-Patch Compared With Two-Patch
Repair of Complete Atrioventricular Septal Defect,
The Annals of Thoracic Surgery, 0):
[37] Stoica S, Carpenter E, Campbell D, Mitchell M, da
Cruz E, Ivy D, Lacour-Gayet F, Morbidity of the
arterial switch operation, Ann Thorac Surg, 2012;
93(6): 1977-83,
[38] Calabro R, Limongelli G, Complete atrioventricular
canal, Orphanet J Rare Dis, 2006; 1(8,
[39] Bakhtiary F, Takacs J, Cho M-Y, Razek V, Dähnert I,
Doenst T, Walther T, Borger MA, Mohr FW, Kostelka
M, Long-Term Results After Repair of Complete
Atrioventricular Septal Defect With Two-patch
Technique, The Annals of Thoracic Surgery, 2010;
89(4): 1239-1243,
[40] Siddiqui J, Brizard CP, Galati JC, Iyengar AJ,
Hutchinson D, Konstantinov IE, Wheaton GR,
Ramsay JM, d'Udekem Y, Surgical valvotomy and
repair for neonatal and infant congenital aortic
stenosis achieves better results than interventional
catheterization, J Am Coll Cardiol, 2013; 62(22):
2134-40,
[41] McLean KM, Lorts A, Pearl JM, Current treatments
for congenital aortic stenosis, Curr Opin Cardiol,
2006; 21(3): 200-4,
[42] Dearani JA, Said SM, Burkhart HM, Pike RB,
O'Leary PW, Cetta F, Strategies for tricuspid re-repair
in Ebstein malformation using the cone technique,
Ann Thorac Surg, 2013; 96(1): 202-8: discussion
208-10,
[43] Roberts PA, Boudjemline Y, Cheatham JP, Eicken A,
Ewert P, McElhinney DB, Hill SL, Berger F, Khan D,
Schranz D, Hess J, Ezekowitz MD, Celermajer D,
Zahn E, Percutaneous tricuspid valve replacement in
congenital and acquired heart disease, J Am Coll
Cardiol, 2011; 58(2): 117-22,
[44] Said SM, Dearani JA, Burkhart HM, Connolly HM,
Eidem B, Stensrud PE, Schaff HV, Management of
tricuspid regurgitation in congenital heart disease: is
survival better with valve repair?, J Thorac
Cardiovasc Surg, 2014; 147(1): 412-7,
Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
16
[45] Thompson LD, McElhinney DB, Reddy VM,
Petrossian E, Silverman NH, Hanley FL, Neonatal
repair of truncus arteriosus: continuing improvement
in outcomes, The Annals of Thoracic Surgery, 2001;
72(2): 391-395,
[46] Celermajer D, Greaves K, Survivors of coarctation
repair: fixed but not cured, Heart, 2002; 88(2):
113-114,
[47] Suarez de Lezo J, Pan M, Romero M, Medina A,
Segura J, Pavlovic D, Martinez C, Tejero I, Perez
Navero J, Torres F, et al., Balloon-expandable stent
repair of severe coarctation of aorta, Am Heart J,
1995; 129(5): 1002-8,
[48] Brown JW, Ruzmetov M, Okada Y, Vijay P, Rodefeld
MD, Turrentine MW, Outcomes in patients with
interrupted aortic arch and associated anomalies: a
20-year experience, Eur J Cardiothorac Surg, 2006;
29(5): 666-73; discussion 673-4,
[49] Sano S, Ishino K, Kawada M, Arai S, Kasahara S,
Asai T, Masuda Z-i, Takeuchi M, Ohtsuki S-i, Right
ventricle–pulmonary artery shunt in first-stage
palliation of hypoplastic left heart syndrome, The
Journal of Thoracic and Cardiovascular Surgery,
2003; 126(2): 504-509,
[50] Alsoufi B, Cai S, Van Arsdell GS, Williams WG,
Caldarone CA, Coles JG, Outcomes after surgical
treatment of children with partial anomalous
pulmonary venous connection, Ann Thorac Surg,
2007; 84(6): 2020-6; discussion 2020-6,
[51] Seale AN, Uemura H, Webber SA, Partridge J,
Roughton M, Ho SY, McCarthy KP, Jones S,
Shaughnessy L, Sunnegardh J, Total Anomalous
Pulmonary Venous ConnectionClinical Perspective
Morphology and Outcome From an International
Population-Based Study, Circulation, 2010; 122(25):
2718-2726,
[52] Balasubramanian S, Marshall AC, Gauvreau K, Peng
LF, Nugent AW, Lock JE, McElhinney DB,
Outcomes after stent implantation for the treatment of
congenital and postoperative pulmonary vein stenosis
in children, Circ Cardiovasc Interv, 2012; 5(1):
109-17,
[53] Lardhi AA, Anomalous origin of left coronary artery
from pulmonary artery: A rare cause of myocardial
infarction in children, Journal of Family and
Community Medicine, 2010; 17(3): 113,
[54] Jin Y, Wang A, Wang Y, Wang Y, Wang W, Hou X,
Natural history of prenatal ventricular septal defects
and their association with foetal echocardiographic
features, Cardiol Young, 2012; 22(3): 323-6,
[55] Zhou Q, Zhou J-Y, Zheng Z, Zhang H, Hu S-S, A
novel vascularized patch enhances cell survival and
modifies ventricular remodeling in a rat myocardial
infarction model, The Journal of Thoracic and
Cardiovascular Surgery, 2010; 140(6): 1388-1396.e3,
[56] Iyer RK, Chiu LLY, Reis LA, Radisic M, Engineered
cardiac tissues, Current Opinion in Biotechnology,
2011; 22(5): 706-714,
[57] Tandon V, Zhang B, Radisic M, Murthy SK,
Generation of tissue constructs for cardiovascular
regenerative medicine: From cell procurement to
scaffold design, Biotechnology Advances, 2013;
31(5): 722-735,
[58] Vasquez AF, Lasala JM, Atrial Septal Defect Closure,
Cardiology Clinics, 2013; 31(3): 385-400,
[59] Jonas RA, Dinardo JA, Comprehensive surgical
management of congenital heart disease. 2004: CRC
Press.
[60] Jang WS, Kim YJ, Kim SH, Effects on tensile strength
and elasticity after treatment with glutaraldehyde,
solvent, decellularization and detoxification in fresh
bovine pericardium, The Korean Journal of Thoracic
and Cardiovascular Surgery, 2010; 43(1): 1-10,
[61] Gendler E, Gendler S, Nimni M, Toxic reactions
evoked by glutaraldehyde‐fixed pericardium and
cardiac valve tissue bioprosthesis, Journal of
biomedical materials research, 1984; 18(7): 727-736,
[62] Sung HW, Chang Y, Chiu CT, Chen CN, Liang HC,
Crosslinking characteristics and mechanical
properties of a bovine pericardium fixed with a
naturally occurring crosslinking agent, Journal of
biomedical materials research, 1999; 47(2): 116-126,
[63] Petite H, Rault I, Huc A, Menasche P, Herbage D, Use
of the acyl azide method for cross-linking
collagen-rich tissues such as pericardium, Journal of
biomedical materials research, 1990; 24(2): 179-187,
[64] Grabenwöger M, Sider J, Fitzal F, Zelenka C,
Windberger U, Grimm M, Moritz A, Böck P, Wolner
E, Impact of glutaraldehyde on calcification of
pericardial bioprosthetic heart valve material, The
Annals of Thoracic Surgery, 1996; 62(3): 772-777,
[65] Lofland GK, O'Brien Jr JE, Gandy KL, Dennis PA,
Marshall JA, Mastbergen RK, Hopkins RA, Initial
Pediatric Cardiac Experience With Decellularized
Allograft Patches, The Annals of Thoracic Surgery,
2012; 93(3): 968-971,
[66] Hawkins JA, Hillman ND, Lambert LM, Jones J, Di
Russo GB, Profaizer T, Fuller TC, Minich LL,
Williams RV, Shaddy RE, Immunogenicity of
decellularized cryopreserved allografts in pediatric
cardiac surgery: comparison with standard
cryopreserved allografts, The Journal of Thoracic and
Cardiovascular Surgery, 2003; 126(1): 247-252,
[67] Rajabi-Zeleti S, Jalili-Firoozinezhad S, Azarnia M,
Khayyatan F, Vahdat S, Nikeghbalian S,
Khademhosseini A, Baharvand H, Aghdami N, The
behavior of cardiac progenitor cells on macroporous
pericardium-derived scaffolds, Biomaterials, 2014;
35(3): 970-982,
[68] Crapo PM, Wang Y, Small intestinal submucosa gel
as a potential scaffolding material for cardiac tissue
engineering, Acta Biomaterialia, 2010; 6(6):
2091-2096,
[69] Griffith LG, Naughton G, Tissue engineering--current
challenges and expanding opportunities, Science,
2002; 295(5557): 1009-1014,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
17
[70] Prabhakaran MP, Venugopal J, Kai D, Ramakrishna
S, Biomimetic material strategies for cardiac tissue
engineering, Materials Science and Engineering: C,
2011; 31(3): 503-513,
[71] Miyagi Y, Chiu LLY, Cimini M, Weisel RD, Radisic
M, Li R-K, Biodegradable collagen patch with
covalently immobilized VEGF for myocardial repair,
Biomaterials, 2011; 32(5): 1280-1290,
[72] Serpooshan V, Zhao M, Metzler SA, Wei K, Shah PB,
Wang A, Mahmoudi M, Malkovskiy AV, Rajadas J,
Butte MJ, Bernstein D, Ruiz-Lozano P, The effect of
bioengineered acellular collagen patch on cardiac
remodeling and ventricular function post myocardial
infarction, Biomaterials, 2013; 34(36): 9048-9055,
[73] Hubbell JA, Biomaterials in tissue engineering,
Nature Biotechnology, 1995; 13(6): 565-576,
[74] Sapir Y, Kryukov O, Cohen S, Integration of multiple
cell-matrix interactions into alginate scaffolds for
promoting cardiac tissue regeneration, Biomaterials,
2011; 32(7): 1838-1847,
[75] Shachar M, Tsur-Gang O, Dvir T, Leor J, Cohen S,
The effect of immobilized RGD peptide in alginate
scaffolds on cardiac tissue engineering, Acta
Biomaterialia, 2011; 7(1): 152-162,
[76] Rao SB, Sharma CP, Use of chitosan as a biomaterial:
studies on its safety and hemostatic potential, Journal
of biomedical materials research, 1997; 34(1): 21-28,
[77] Kathuria N, Tripathi A, Kar KK, Kumar A, Synthesis
and characterization of elastic and macroporous
chitosan–gelatin cryogels for tissue engineering, Acta
Biomaterialia, 2009; 5(1): 406-418,
[78] Patra C, Talukdar S, Novoyatleva T, Velagala SR,
Mühlfeld C, Kundu B, Kundu SC, Engel FB, Silk
protein fibroin from Antheraea mylitta for cardiac
tissue engineering, Biomaterials, 2012; 33(9):
2673-2680,
[79] Chi N-H, Yang M-C, Chung T-W, Chou N-K, Wang
S-S, Cardiac repair using chitosan-hyaluronan/silk
fibroin patches in a rat heart model with myocardial
infarction, Carbohydrate Polymers, 2013; 92(1):
591-597,
[80] Alves P, Cardoso R, Correia TR, Antunes BP, Correia
IJ, Ferreira P, Surface modification of polyurethane
films by plasma and ultraviolet light to improve
haemocompatibility for artificial heart valves,
Colloids and Surfaces B: Biointerfaces, 2014; 113(0):
25-32,
[81] Orlova Y, Magome N, Liu L, Chen Y, Agladze K,
Electrospun nanofibers as a tool for architecture
control in engineered cardiac tissue, Biomaterials,
2011; 32(24): 5615-5624,
[82] Yeong WY, Sudarmadji N, Yu HY, Chua CK, Leong
KF, Venkatraman SS, Boey YCF, Tan LP, Porous
polycaprolactone scaffold for cardiac tissue
engineering fabricated by selective laser sintering,
Acta Biomaterialia, 2010; 6(6): 2028-2034,
[83] Serraf A, Lacour-Gayet F, Bruniaux J, Ouaknine R,
Losay J, Petit J, Binet J-P, Planche C, Surgical
management of isolated multiple ventricular septal
defects. Logical approach in 130 cases, The Journal of
Thoracic and Cardiovascular Surgery, 1992; 103(3):
437,
[84] Fujimoto KL, Guan J, Oshima H, Sakai T, Wagner
WR, In Vivo Evaluation of a Porous, Elastic,
Biodegradable Patch for Reconstructive Cardiac
Procedures, The Annals of Thoracic Surgery, 2007;
83(2): 648-654,
[85] Miyazaki T, Yamagishi M, Nakashima A, Fukae K,
Nakano T, Yaku H, Kado H, Expanded
polytetrafluoroethylene valved conduit and patch with
bulging sinuses in right ventricular outflow tract
reconstruction, The Journal of Thoracic and
Cardiovascular Surgery, 2007; 134(2): 327-332,
[86] Swartbol P, Truedsson L, Norgren L, The
inflammatory response and its consequence for the
clinical outcome following aortic aneurysm repair,
European Journal of Vascular and Endovascular
Surgery, 2001; 21(5): 393-400,
[87] Chen Q-Z, Ishii H, Thouas GA, Lyon AR, Wright JS,
Blaker JJ, Chrzanowski W, Boccaccini AR, Ali NN,
Knowles JC, Harding SE, An elastomeric patch
derived from poly(glycerol sebacate) for delivery of
embryonic stem cells to the heart, Biomaterials, 2010;
31(14): 3885-3893,
[88] Rai R, Tallawi M, Barbani N, Frati C, Madeddu D,
Cavalli S, Graiani G, Quaini F, Roether JA, Schubert
DW, Rosellini E, Boccaccini AR, Biomimetic
poly(glycerol sebacate) (PGS) membranes for cardiac
patch application, Materials Science and Engineering:
C, 2013; 33(7): 3677-3687,
[89] Pereira MJN, Ouyang B, Sundback CA, Lang N,
Friehs I, Mureli S, Pomerantseva I, McFadden J,
Mochel MC, Mwizerwa O, A highly tunable
biocompatible and multifunctional biodegradable
elastomer, Advanced Materials, 2013; 25(8):
1209-1215,
[90] Pok S, Myers JD, Madihally SV, Jacot JG, A
multilayered scaffold of a chitosan and gelatin
hydrogel supported by a PCL core for cardiac tissue
engineering, Acta Biomaterialia, 2013; 9(3):
5630-5642,
[91] Pok S, Benavides OM, Hallal PA, Jacot J, Use of
myocardial matrix in a chitosan-based full thickness
heart patch, Tissue engineering, 2014; ja):
[92] Kharaziha M, Nikkhah M, Shin S-R, Annabi N,
Masoumi N, Gaharwar AK, Camci-Unal G,
Khademhosseini A, PGS:Gelatin nanofibrous
scaffolds with tunable mechanical and structural
properties for engineering cardiac tissues,
Biomaterials, 2013; 34(27): 6355-6366,
[93] Martins AM, Eng G, Caridade SG, Mano JF, Reis RL,
Vunjak-Novakovic G, Electrically conductive
chitosan/carbon scaffolds for cardiac tissue
engineering, Biomacromolecules, 2014;
[94] Bidarra SJ, Barrias CC, Granja PL, Injectable alginate
hydrogels for cell delivery in tissue engineering, Acta
Biomaterialia, 0):

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
18
[95] Basso C, Frescura C, Corrado D, Muriago M,
Angelini A, Daliento L, Thiene G, Congenital heart
disease and sudden death in the young, Human
Pathology, 1995; 26(10): 1065-1072,
[96] Franciosi RA, Blanc WA, Myocardial infarcts in
infants and children. I. A necropsy study in congenital
heart disease, The Journal of Pediatrics, 1968; 73(3):
309-319,
[97] Wang F, Li Z, Khan M, Tamama K, Kuppusamy P,
Wagner WR, Sen CK, Guan J, Injectable, rapid gelling
and highly flexible hydrogel composites as growth
factor and cell carriers, Acta Biomaterialia, 2010;
6(6): 1978-1991,
[98] Huang C-C, Wei H-J, Yeh Y-C, Wang J-J, Lin W-W,
Lee T-Y, Hwang S-M, Choi S-W, Xia Y, Chang Y,
Sung H-W, Injectable PLGA porous beads
cellularized by hAFSCs for cellular cardiomyoplasty,
Biomaterials, 2012; 33(16): 4069-4077,
[99] Spotnitz WD, Fibrin sealant: past, present, and future:
a brief review, World journal of surgery, 2010; 34(4):
632-634,
[100] Christman KL, Vardanian AJ, Fang Q, Sievers RE,
Fok HH, Lee RJ, Injectable Fibrin Scaffold Improves
Cell Transplant Survival, Reduces Infarct Expansion,
and Induces Neovasculature Formation in Ischemic
Myocardium, Journal of the American College of
Cardiology, 2004; 44(3): 654-660,
[101] Singelyn JM, DeQuach JA, Seif-Naraghi SB,
Littlefield RB, Schup-Magoffin PJ, Christman KL,
Naturally derived myocardial matrix as an injectable
scaffold for cardiac tissue engineering, Biomaterials,
2009; 30(29): 5409-5416,
[102] Ruvinov E, Leor J, Cohen S, The promotion of
myocardial repair by the sequential delivery of IGF-1
and HGF from an injectable alginate biomaterial in a
model of acute myocardial infarction, Biomaterials,
2011; 32(2): 565-578,
[103] Dobner S, Bezuidenhout D, Govender P, Zilla P,
Davies N, A synthetic non-degradable polyethylene
glycol hydrogel retards adverse post-infarct left
ventricular remodeling, Journal of Cardiac Failure,
2009; 15(7): 629-636,
[104] Kadner K, Dobner S, Franz T, Bezuidenhout D, Sirry
MS, Zilla P, Davies NH, The beneficial effects of
deferred delivery on the efficiency of hydrogel
therapy post myocardial infarction, Biomaterials,
2012; 33(7): 2060-2066,
[105] Chen Q-Z, Harding SE, Ali NN, Lyon AR, Boccaccini
AR, Biomaterials in cardiac tissue engineering: Ten
years of research survey, Materials Science and
Engineering: R: Reports, 2008; 59(1–6): 1-37,
[106] Ifkovits JL, Tous E, Minakawa M, Morita M, Robb
JD, Koomalsingh KJ, Gorman JH, Gorman RC,
Burdick JA, Injectable hydrogel properties influence
infarct expansion and extent of postinfarction left
ventricular remodeling in an ovine model,
Proceedings of the National Academy of Sciences,
2010; 107(25): 11507-11512,
[107] Hoffman JI, Kaplan S, Liberthson RR, Prevalence of
congenital heart disease, Am Heart J, 2004; 147(3):
425-39,
[108] Papadopoulos N, Esmaeili A, Zierer A, Bakhtiary F,
Ozaslan F, Moritz A, Secondary repair of incompetent
pulmonary valves, Ann Thorac Surg, 2009; 87(6):
1879-84,
[109] Stark J, The use of valved conduits in pediatric cardiac
surgery, Pediatr Cardiol, 1998; 19(4): 282-8,
[110] Boethig D, Thies WR, Hecker H, Breymann T, Mid
term course after pediatric right ventricular outflow
tract reconstruction: a comparison of homografts,
porcine xenografts and Contegras, Eur J Cardiothorac
Surg, 2005; 27(1): 58-66,
[111] Hawkins JA, Breinholt JP, Lambert LM, Fuller TC,
Profaizer T, McGough EC, Shaddy RE, Class I and
class II anti-HLA antibodies after implantation of
cryopreserved allograft material in pediatric patients,
J Thorac Cardiovasc Surg, 2000; 119(2): 324-30,
[112] da Costa FD, Dohmen PM, Duarte D, von Glenn C,
Lopes SV, Filho HH, da Costa MB, Konertz W,
Immunological and echocardiographic evaluation of
decellularized versus cryopreserved allografts during
the Ross operation, Eur J Cardiothorac Surg, 2005;
27(4): 572-8,
[113] Konakci KZ, Bohle B, Blumer R, Hoetzenecker W,
Roth G, Moser B, Boltz-Nitulescu G, Gorlitzer M,
Klepetko W, Wolner E, Ankersmit HJ, Alpha-Gal on
bioprostheses: xenograft immune response in cardiac
surgery, Eur J Clin Invest, 2005; 35(1): 17-23,
[114] Wilhelmi MH, Mertsching H, Wilhelmi M, Leyh R,
Haverich A, Role of inflammation in allogeneic and
xenogeneic heart valve degeneration:
immunohistochemical evaluation of inflammatory
endothelial cell activation, J Heart Valve Dis, 2003;
12(4): 520-6,
[115] Simionescu DT, Prevention of calcification in
bioprosthetic heart valves: challenges and
perspectives, Expert Opin Biol Ther, 2004; 4(12):
1971-85,
[116] Perri G, Polito A, Esposito C, Albanese SB,
Francalanci P, Pongiglione G, Carotti A, Early and
late failure of tissue-engineered pulmonary valve
conduits used for right ventricular outflow tract
reconstruction in patients with congenital heart
disease, Eur J Cardiothorac Surg, 2012; 41(6):
1320-5,
[117] Simon P, Kasimir MT, Seebacher G, Weigel G,
Ullrich R, Salzer-Muhar U, Rieder E, Wolner E, Early
failure of the tissue engineered porcine heart valve
SYNERGRAFT in pediatric patients, Eur J
Cardiothorac Surg, 2003; 23(6): 1002-6; discussion
1006,
[118] Voges I, Brasen JH, Entenmann A, Scheid M,
Scheewe J, Fischer G, Hart C, Andrade A, Pham HM,
Kramer HH, Rickers C, Adverse results of a
decellularized tissue-engineered pulmonary valve in
humans assessed with magnetic resonance imaging,
Eur J Cardiothorac Surg, 2013; 44(4): e272-9,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
19
[119] Laudito A, Brook MM, Suleman S, Bleiweis MS,
Thompson LD, Hanley FL, Reddy VM, The Ross
procedure in children and young adults: a word of
caution, J Thorac Cardiovasc Surg, 2001; 122(1):
147-53,
[120] Elkins RC, Thompson DM, Lane MM, Elkins CC,
Peyton MD, Ross operation: 16-year experience, J
Thorac Cardiovasc Surg, 2008; 136(3): 623-30, 630
e1-5,
[121] Caldarone CA, McCrindle BW, Van Arsdell GS,
Coles JG, Webb G, Freedom RM, Williams WG,
Independent factors associated with longevity of
prosthetic pulmonary valves and valved conduits, J
Thorac Cardiovasc Surg, 2000; 120(6): 1022-30;
discussion 1031,
[122] Aldous IG, Veres SP, Jahangir A, Lee JM, Differences
in collagen cross-linking between the four valves of
the bovine heart: a possible role in adaptation to
mechanical fatigue, Am J Physiol Heart Circ Physiol,
2009; 296(6): H1898-906,
[123] Grande-Allen KJ, Liao J, The heterogeneous
biomechanics and mechanobiology of the mitral
valve: implications for tissue engineering, Curr
Cardiol Rep, 2011; 13(2): 113-20,
[124] Sacks MS, Schoen FJ, Mayer JE, Bioengineering
challenges for heart valve tissue engineering, Annu
Rev Biomed Eng, 2009; 11(289-313,
[125] Aggarwal A, Ferrari G, Joyce E, Daniels MJ, Sainger
R, Gorman JH, 3rd, Gorman R, Sacks MS,
Architectural Trends in the Human Normal and
Bicuspid Aortic Valve Leaflet and Its Relevance to
Valve Disease, Ann Biomed Eng, 2014;
[126] Driessen NJ, Bouten CV, Baaijens FP, Improved
prediction of the collagen fiber architecture in the
aortic heart valve, J Biomech Eng, 2005; 127(2):
329-36,
[127] Schoen FJ, Evolving concepts of cardiac valve
dynamics: the continuum of development, functional
structure, pathobiology, and tissue engineering,
Circulation, 2008; 118(18): 1864-80,
[128] Tseng H, Grande-Allen KJ, Elastic fibers in the aortic
valve spongiosa: a fresh perspective on its structure
and role in overall tissue function, Acta Biomater,
2011; 7(5): 2101-8,
[129] Dohmen PM, Lembcke A, Hotz H, Kivelitz D,
Konertz WF, Ross operation with a tissue-engineered
heart valve, Ann Thorac Surg, 2002; 74(5): 1438-42,
[130] Dohmen PM, Lembcke A, Holinski S, Pruss A,
Konertz W, Ten years of clinical results with a
tissue-engineered pulmonary valve, Ann Thorac Surg,
2011; 92(4): 1308-14,
[131] Cebotari S, Lichtenberg A, Tudorache I, Hilfiker A,
Mertsching H, Leyh R, Breymann T, Kallenbach K,
Maniuc L, Batrinac A, Repin O, Maliga O, Ciubotaru
A, Haverich A, Clinical application of tissue
engineered human heart valves using autologous
progenitor cells, Circulation, 2006; 114(1 Suppl):
I132-7,
[132] Roh JD, Sawh-Martinez R, Brennan MP, Jay SM,
Devine L, Rao DA, Yi T, Mirensky TL, Nalbandian
A, Udelsman B, Hibino N, Shinoka T, Saltzman WM,
Snyder E, Kyriakides TR, Pober JS, Breuer CK,
Tissue-engineered vascular grafts transform into
mature blood vessels via an inflammation-mediated
process of vascular remodeling, Proc Natl Acad Sci U
S A, 2010; 107(10): 4669-74,
[133] Jordan JE, Williams JK, Lee SJ, Raghavan D, Atala A,
Yoo JJ, Bioengineered self-seeding heart valves, J
Thorac Cardiovasc Surg, 2012; 143(1): 201-8,
[134] Iop L, Renier V, Naso F, Piccoli M, Bonetti A,
Gandaglia A, Pozzobon M, Paolin A, Ortolani F,
Marchini M, Spina M, De Coppi P, Sartore S, Gerosa
G, The influence of heart valve leaflet matrix
characteristics on the interaction between human
mesenchymal stem cells and decellularized scaffolds,
Biomaterials, 2009; 30(25): 4104-16,
[135] Hinton RB, Yutzey KE, Heart valve structure and
function in development and disease, Annu Rev
Physiol, 2011; 73(29-46,
[136] Tedder ME, Liao J, Weed B, Stabler C, Zhang H,
Simionescu A, Simionescu DT, Stabilized collagen
scaffolds for heart valve tissue engineering, Tissue
Eng Part A, 2009; 15(6): 1257-68,
[137] Tedder ME, Simionescu A, Chen J, Liao J,
Simionescu DT, Assembly and testing of stem
cell-seeded layered collagen constructs for heart valve
tissue engineering, Tissue Eng Part A, 2011; 17(1-2):
25-36,
[138] Flanagan TC, Wilkins B, Black A, Jockenhoevel S,
Smith TJ, Pandit AS, A collagen-glycosaminoglycan
co-culture model for heart valve tissue engineering
applications, Biomaterials, 2006; 27(10): 2233-46,
[139] Alfonso AR, Rath S, Rafiee P, Hernandez-Espino M,
Din M, George F, Ramaswamy S, Glycosaminoglycan
entrapment by fibrin in engineered heart valve tissues,
Acta Biomater, 2013; 9(9): 8149-57,
[140] Flanagan TC, Cornelissen C, Koch S, Tschoeke B,
Sachweh JS, Schmitz-Rode T, Jockenhoevel S, The in
vitro development of autologous fibrin-based
tissue-engineered heart valves through optimised
dynamic conditioning, Biomaterials, 2007; 28(23):
3388-97,
[141] Syedain ZH, Meier LA, Reimer JM, Tranquillo RT,
Tubular heart valves from decellularized engineered
tissue, Ann Biomed Eng, 2013; 41(12): 2645-54,
[142] Masters KS, Shah DN, Leinwand LA, Anseth KS,
Crosslinked hyaluronan scaffolds as a biologically
active carrier for valvular interstitial cells,
Biomaterials, 2005; 26(15): 2517-25,
[143] Ramamurthi A, Vesely I, Evaluation of the
matrix-synthesis potential of crosslinked hyaluronan
gels for tissue engineering of aortic heart valves,
Biomaterials, 2005; 26(9): 999-1010,
[144] Duan B, Hockaday LA, Kapetanovic E, Kang KH,
Butcher JT, Stiffness and adhesivity control aortic
valve interstitial cell behavior within hyaluronic acid
based hydrogels, Acta Biomater, 2013; 9(8): 7640-50,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
20
[145] Rodriguez KJ, Piechura LM, Masters KS, Regulation
of valvular interstitial cell phenotype and function by
hyaluronic acid in 2-D and 3-D culture environments,
Matrix Biol, 2011; 30(1): 70-82,
[146] Shinoka T, Breuer CK, Tanel RE, Zund G, Miura T,
Ma PX, Langer R, Vacanti JP, Mayer JE, Jr., Tissue
engineering heart valves: valve leaflet replacement
study in a lamb model, Ann Thorac Surg, 1995; 60(6
Suppl): S513-6,
[147] Hildebrand DK, Wu ZJ, Mayer JE, Jr., Sacks MS,
Design and hydrodynamic evaluation of a novel
pulsatile bioreactor for biologically active heart
valves, Ann Biomed Eng, 2004; 32(8): 1039-49,
[148] Ramaswamy S, Gottlieb D, Engelmayr GC, Jr.,
Aikawa E, Schmidt DE, Gaitan-Leon DM, Sales VL,
Mayer JE, Jr., Sacks MS, The role of organ level
conditioning on the promotion of engineered heart
valve tissue development in-vitro using mesenchymal
stem cells, Biomaterials, 2010; 31(6): 1114-25,
[149] Mol A, Bouten CV, Zund G, Gunter CI, Visjager JF,
Turina MI, Baaijens FP, Hoerstrup SP, The relevance
of large strains in functional tissue engineering of
heart valves, Thorac Cardiovasc Surg, 2003; 51(2):
78-83,
[150] Hoerstrup SP, Sodian R, Daebritz S, Wang J, Bacha
EA, Martin DP, Moran AM, Guleserian KJ, Sperling
JS, Kaushal S, Vacanti JP, Schoen FJ, Mayer JE, Jr.,
Functional living trileaflet heart valves grown in vitro,
Circulation, 2000; 102(19 Suppl 3): III44-9,
[151] Schmidt D, Achermann J, Odermatt B, Breymann C,
Mol A, Genoni M, Zund G, Hoerstrup SP, Prenatally
fabricated autologous human living heart valves based
on amniotic fluid derived progenitor cells as single
cell source, Circulation, 2007; 116(11 Suppl): I64-70,
[152] Weber B, Emmert MY, Behr L, Schoenauer R,
Brokopp C, Drogemuller C, Modregger P,
Stampanoni M, Vats D, Rudin M, Burzle W, Farine
M, Mazza E, Frauenfelder T, Zannettino AC, Zund G,
Kretschmar O, Falk V, Hoerstrup SP, Prenatally
engineered autologous amniotic fluid stem cell-based
heart valves in the fetal circulation, Biomaterials,
2012; 33(16): 4031-43,
[153] Weber B, Kehl D, Bleul U, Behr L, Sammut S, Frese
L, Ksiazek A, Achermann J, Stranzinger G, Robert J,
Sanders B, Sidler M, Brokopp CE, Proulx ST,
Frauenfelder T, Schoenauer R, Emmert MY, Falk V,
Hoerstrup SP, In vitro fabrication of autologous living
tissue-engineered vascular grafts based on prenatally
harvested ovine amniotic fluid-derived stem cells, J
Tissue Eng Regen Med, 2013;
[154] Brugmans MM, Driessen-Mol A, Rubbens MP, Cox
MA, Baaijens FP, Poly-epsilon-caprolactone scaffold
and reduced in vitro cell culture: beneficial effect on
compaction and improved valvular tissue formation, J
Tissue Eng Regen Med, 2013;
[155] Masoumi N, Johnson KL, Howell MC, Engelmayr
GC, Jr., Valvular interstitial cell seeded poly(glycerol
sebacate) scaffolds: toward a biomimetic in vitro
model for heart valve tissue engineering, Acta
Biomater, 2013; 9(4): 5974-88,
[156] Masoumi N, Larson BL, Annabi N, Kharaziha M,
Zamanian B, Shapero KS, Cubberley AT, Camci-Unal
G, Manning KB, Mayer JE, Jr., Khademhosseini A,
Electrospun PGS:PCL Microfibers Align Human
Valvular Interstitial Cells and Provide Tunable
Scaffold Anisotropy, Adv Healthc Mater, 2014;
[157] Amoroso NJ, D'Amore A, Hong Y, Rivera CP, Sacks
MS, Wagner WR, Microstructural manipulation of
electrospun scaffolds for specific bending stiffness for
heart valve tissue engineering, Acta Biomater, 2012;
8(12): 4268-77,
[158] Thierfelder N, Koenig F, Bombien R, Fano C,
Reichart B, Wintermantel E, Schmitz C, Akra B, In
vitro comparison of novel polyurethane aortic valves
and homografts after seeding and conditioning,
ASAIO J, 2013; 59(3): 309-16,
[159] Benton JA, Fairbanks BD, Anseth KS,
Characterization of valvular interstitial cell function in
three dimensional matrix metalloproteinase
degradable PEG hydrogels, Biomaterials, 2009;
30(34): 6593-603,
[160] Wang H, Tibbitt MW, Langer SJ, Leinwand LA,
Anseth KS, Hydrogels preserve native phenotypes of
valvular fibroblasts through an elasticity-regulated
PI3K/AKT pathway, Proc Natl Acad Sci U S A, 2013;
110(48): 19336-41,
[161] Tseng H, Cuchiara ML, Durst CA, Cuchiara MP, Lin
CJ, West JL, Grande-Allen KJ, Fabrication and
mechanical evaluation of anatomically-inspired
quasilaminate hydrogel structures with layer-specific
formulations, Ann Biomed Eng, 2013; 41(2): 398-407,
[162] Hinderer S, Seifert J, Votteler M, Shen N,
Rheinlaender J, Schaffer TE, Schenke-Layland K,
Engineering of a bio-functionalized hybrid
off-the-shelf heart valve, Biomaterials, 2014; 35(7):
2130-9,
[163] Vida VL, Torregrossa G, De Franceschi M, Padalino
MA, Belli E, Berggren H, Cicek S, Ebels T, Fragata J,
Hoel TN, Horer J, Hraska V, Kostolny M, Lindberg H,
Mueller C, Pretre R, Rosser B, Rubay J, Schreiber C,
Speggiorin S, Tlaskal T, Stellin G, European
Congenital Heart Surgeons A, Pediatric coronary
artery revascularization: a European multicenter
study, Ann Thorac Surg, 2013; 96(3): 898-903,
[164] Seirafi PA, Warner KG, Geggel RL, Payne DD,
Cleveland RJ, Repair of coarctation of the aorta during
infancy minimizes the risk of late hypertension, Ann
Thorac Surg, 1998; 66(4): 1378-82,
[165] Messner G, Reul GJ, Flamm SD, Gregoric ID,
Opfermann UT, Interrupted aortic arch in an adult
single-stage extra-anatomic repair, Tex Heart Inst J,
2002; 29(2): 118-21,
[166] Wilson W, Osten M, Benson L, Horlick E, Evolving
trends in interventional cardiology: endovascular
options for congenital disease in adults, Can J
Cardiol, 2014; 30(1): 75-86,

Challenges in Regenerative Medicine Vol.1 No.1 August 2014
ISSN: xxxx-xxxx (Print) ISSN: xxxx-xxxx (Online) http://www.researchpub.org/journal/iphf/iphf.html
21
[167] Nayak s BP, The Fontan circulation, Continuing
Education in Anaesthesia, Critical Care & Pain,
2008; 8(1):
[168] Fontan F, Baudet E, Surgical repair of tricuspid
atresia, Thorax, 1971; 26(3): 240-8,
[169] Kreutzer G, Galindez E, Bono H, De Palma C, Laura
JP, An operation for the correction of tricuspid atresia,
J Thorac Cardiovasc Surg, 1973; 66(4): 613-21,
[170] Mehta RI, Mukherjee AK, Patterson TD, Fishbein
MC, Pathology of explanted polytetrafluoroethylene
vascular grafts, Cardiovasc Pathol, 2011; 20(4):
213-21,
[171] Cleveland DC, Williams WG, Razzouk AJ, Trusler
GA, Rebeyka IM, Duffy L, Kan Z, Coles JG, Freedom
RM, Failure of cryopreserved homograft valved
conduits in the pulmonary circulation, Circulation,
1992; 86(5 Suppl): II150-3,
[172] Shinoka T, Breuer C, Tissue-engineered blood vessels
in pediatric cardiac surgery, Yale J Biol Med, 2008;
81(4): 161-6,
[173] Patterson JT, Gilliland T, Maxfield MW, Church S,
Naito Y, Shinoka T, Breuer CK, Tissue-engineered
vascular grafts for use in the treatment of congenital
heart disease: from the bench to the clinic and back
again, Regen Med, 2012; 7(3): 409-19,
[174] Dirks V, Pretre R, Knirsch W, Valsangiacomo
Buechel ER, Seifert B, Schweiger M, Hubler M, Dave
H, Modified Blalock Taussig shunt: a not-so-simple
palliative procedure, Eur J Cardiothorac Surg, 2013;
44(6): 1096-102,
[175] Dahl SL, Blum JL, Niklason LE, Bioengineered
vascular grafts: can we make them off-the-shelf?,
Trends Cardiovasc Med, 2011; 21(3): 83-9,
[176] Li S, Sengupta D, Chien S, Vascular tissue
engineering: from in vitro to in situ, Wiley Interdiscip
Rev Syst Biol Med, 2013;
[177] Peck M, Gebhart D, Dusserre N, McAllister TN,
L'Heureux N, The evolution of vascular tissue
engineering and current state of the art, Cells Tissues
Organs, 2012; 195(1-2): 144-58,
[178] L'Heureux N, Dusserre N, Marini A, Garrido S, de la
Fuente L, McAllister T, Technology insight: the
evolution of tissue-engineered vascular grafts--from
research to clinical practice, Nat Clin Pract
Cardiovasc Med, 2007; 4(7): 389-95,
[179] Udelsman BV, Maxfield MW, Breuer CK, Tissue
engineering of blood vessels in cardiovascular
disease: moving towards clinical translation, Heart,
2013; 99(7): 454-60,
[180] Soletti L, Nieponice A, Guan J, Stankus JJ, Wagner
WR, Vorp DA, A seeding device for tissue engineered
tubular structures, Biomaterials, 2006; 27(28):
4863-70,
[181] Udelsman B, Hibino N, Villalona GA, McGillicuddy
E, Nieponice A, Sakamoto Y, Matsuda S, Vorp DA,
Shinoka T, Breuer CK, Development of an
operator-independent method for seeding
tissue-engineered vascular grafts, Tissue Eng Part C
Methods, 2011; 17(7): 731-6,
[182] Kaushal S, Amiel GE, Guleserian KJ, Shapira OM,
Perry T, Sutherland FW, Rabkin E, Moran AM,
Schoen FJ, Atala A, Soker S, Bischoff J, Mayer JE, Jr.,
Functional small-diameter neovessels created using
endothelial progenitor cells expanded ex vivo, Nat
Med, 2001; 7(9): 1035-40,
[183] Campbell JH, Efendy JL, Campbell GR, Novel
vascular graft grown within recipient's own peritoneal
cavity, Circ Res, 1999; 85(12): 1173-8,
[184] Hibino N, McGillicuddy E, Matsumura G, Ichihara Y,
Naito Y, Breuer C, Shinoka T, Late-term results of
tissue-engineered vascular grafts in humans, J Thorac
Cardiovasc Surg, 2010; 139(2): 431-6, 436 e1-2,
[185] Hibino N, Villalona G, Pietris N, Duncan DR,
Schoffner A, Roh JD, Yi T, Dobrucki LW, Mejias D,
Sawh-Martinez R, Harrington JK, Sinusas A, Krause
DS, Kyriakides T, Saltzman WM, Pober JS, Shin'oka
T, Breuer CK, Tissue-engineered vascular grafts form
neovessels that arise from regeneration of the adjacent
blood vessel, FASEB J, 2011; 25(8): 2731-9,
[186] Hibino N, Yi T, Duncan DR, Rathore A, Dean E,
Naito Y, Dardik A, Kyriakides T, Madri J, Pober JS,
Shinoka T, Breuer CK, A critical role for macrophages
in neovessel formation and the development of
stenosis in tissue-engineered vascular grafts, FASEB
J, 2011; 25(12): 4253-63,
[187] Shinoka T, Shum-Tim D, Ma PX, Tanel RE, Isogai N,
Langer R, Vacanti JP, Mayer JE, Jr., Creation of
viable pulmonary artery autografts through tissue
engineering, J Thorac Cardiovasc Surg, 1998; 115(3):
536-45; discussion 545-6,
[188] Shin'oka T, Imai Y, Ikada Y, Transplantation of a
tissue-engineered pulmonary artery, N Engl J Med,
2001; 344(7): 532-3,
[189] Hoerstrup SP, Kadner A, Breymann C, Maurus CF,
Guenter CI, Sodian R, Visjager JF, Zund G, Turina
MI, Living, autologous pulmonary artery conduits
tissue engineered from human umbilical cord cells,
Ann Thorac Surg, 2002; 74(1): 46-52; discussion 52,
[190] Leyh RG, Wilhelmi M, Rebe P, Ciboutari S, Haverich
A, Mertsching H, Tissue engineering of viable
pulmonary arteries for surgical correction of
congenital heart defects, Ann Thorac Surg, 2006;
81(4): 1466-70; discussion 1470-1,
[191] Clinicaltrials.gov. A Pilot Study Investigating the
Clinical Use of Tissue Engineered Vascular Grafts in
Congenital Heart Surgery. [cited 2014 04/10/2104].