tibial bone graft fiarvest - the podiatry institute · chapter 4 proximal tibial bone graft...
TRANSCRIPT

CHAPTER 4
PROXIMAL TIBIAL BONE GRAFT FIARVEST
Justin Fleming, DPM
INTRODUCTION
The need for cancellous bone grafting is quite apparent infoot and ankle reconstruction. Despite all of the expandingtechnology in the field of orthobiologics, no commerciallyavailable bone graft or bioengineered graft substitutes havebeen proven to be superior or equal to autoiogous bone.Potential donor sites for graft harvest include the iliac crest,
fibula, distal tibia, and calcaneus. These sites often yieldinadequate quantities and are associated with donor sitemorbidity such as pain and secondary fracture. The authorwill illustrate the previously described surgical technique ofbone graft harvest from the proximal tibial metaphysis andprovide the authors' experience with this technique.','
INDICAIIONS
The primary need for cancellous bone graft in foot andankle reconstruction is to augment arthrodesis in additionto filling bony voids. Autoiogous bone is the gold standardin bone grafting and "optimizes" the environmenr forhealing by providing both osteoconductive and osteogenic
properties. Although pladet gels, bone marrow aspirates,
and other technologies (BMP) have reduced the need
for autologous bone, their cost is substantial and nocomparison long term studies are currently available. Theauthor began to utilize this technique when hospitaladministration would no longer allow for the use oforthobiologics and implantable bone stimulation because
of their financial drawbacks. Specifically, the author findsthe most frequent procedures performed in conjunctionwith proximal tibial bone graft harvest are arthrodesis
procedures involving the ankle and subtalar joint in cases ofpost-traumatic arthritis. These injuries often leave large
avascular cystic changes in the talus and more commonlyin the distal tibia which require grafting (Figure 1). Inaddition, those cases of revisional fusions or high riskfusions (smokers, open fractures) and extended midfootfusions (i.e., neuroarthropathy) may benefit or requiresupplement grafting. Contraindications include those
patients with an open physis, total knee arthroplasqz, orprior anterior cruciate ligament reconstruction. Thegraft harwested in this region in not intended to be
structural in nature.
Figure 1A. Subtotal AVN of the distal tibia with cysticchange secondary to post-traunatic arthritis. Sagitralplane image through prior regiotr olt A\Nfollowing bone grafting and tibio-talo-calcaneala rth rodesis.
Figure 1B.
Figure 1C.

CHAPTER 4
PROXIMAL TIBIAL BONE GR\I'T FIARVEST
Justin Fleming, DPM
INTRODUCTION
The need for cancellous bone grafting is quite apparent infoot and ankle reconstruction. Despite all of the expandingtechnology in the field of orthobiologics, no commerciallyavailable bone graft or bioengineered graft substitutes have
been proven to be superior or equal to autologous bone.Potential donor sites for graft harvest include the iliac crest,
fibula, distal tibia, and calcaneus. These sites often yieldinadequate quantities and are associated with donor sitemorbidity such as pain and secondary fracrure. The authorwill illustrate the previously described surgical technique ofbone graft harvest from the proximal tibiai metaphysis andprovide the authors' experience with this technique.','
INDICAIIONS
The primary need for canceilous bone graft in foot andankle reconstruction is to augment arthrodesis in additionto filling bony voids. Autologous bone is the gold standardin bone grafting and "optimizes" the environment forhealing by providing both osteoconductive and osteogenic
properties. Although platlet gels, bone marrow aspirates,
and other technologies (BMP) have reduced the need
for autologous bone, their cost is substantial and nocomparison long term studies are currently available. Theauthor began to utilize this technique when hospitaladministration would no longer allow for the use ofonhobiologics and implantable bone stimulation because
of their financial drawbacks. Specifically, the author findsthe most frequent procedures performed in conjunctionwith proximal tibial bone graft harvest are arthrodesis
procedures involving the ankle and subtalar joint in cases ofpost-traumatic arthritis. These injuries often leave large
avascular cystic changes in the talus and more commonlyin the distal tibia which require grafting (Figure 1). Inaddition, those cases of revisional fusions or high riskfusions (smokers, open fractures) and extended midfootfusions (i.e., neuroarthropathy) may benefit or requiresupplement grafting. Contraindications include those
patients with an open physis, total knee arthroplasq., orprior anterior cruciate ligament reconstruction. Thegraft harvested in this region in not intended to be
structural in nature.
Figure 1A. Subtotal AVN of the distal tibia wjth cystic
change secondarv to post-traumatic arthriris. Sagittalplane image through prior region of AVNfollowing bone grafting and tibio-talo-calcanealarthrodesis.
Figure 1B.
F-igrLre 1C.
t2 CHAPTER 4
SURGICAL TECHNIQUE
Prior to surgery, a complete radiographic analysis of theproximal tibia and knee should be obtained in addition tothe studies appropriate for the index procedure. Pre-
existing clinical or radiographic abnormalities in the regionofharvest should be evaluated by an orthopedic surgeon oranother source of bone should be identified.
The proximal tibia can usually be accessed with thepatient in any position (supine, prone, lateral decubitus,etc.) and the procedure can be carried out with or with-out tourniquet control. If tourniquet time is not available,
retraction of the soft tissues generally provides adequate
hemostasis much like dissection on the plantar foot.If the patient is obese and the typical subcutaneous
landmarks are not readily palpable, fluoroscopy may be
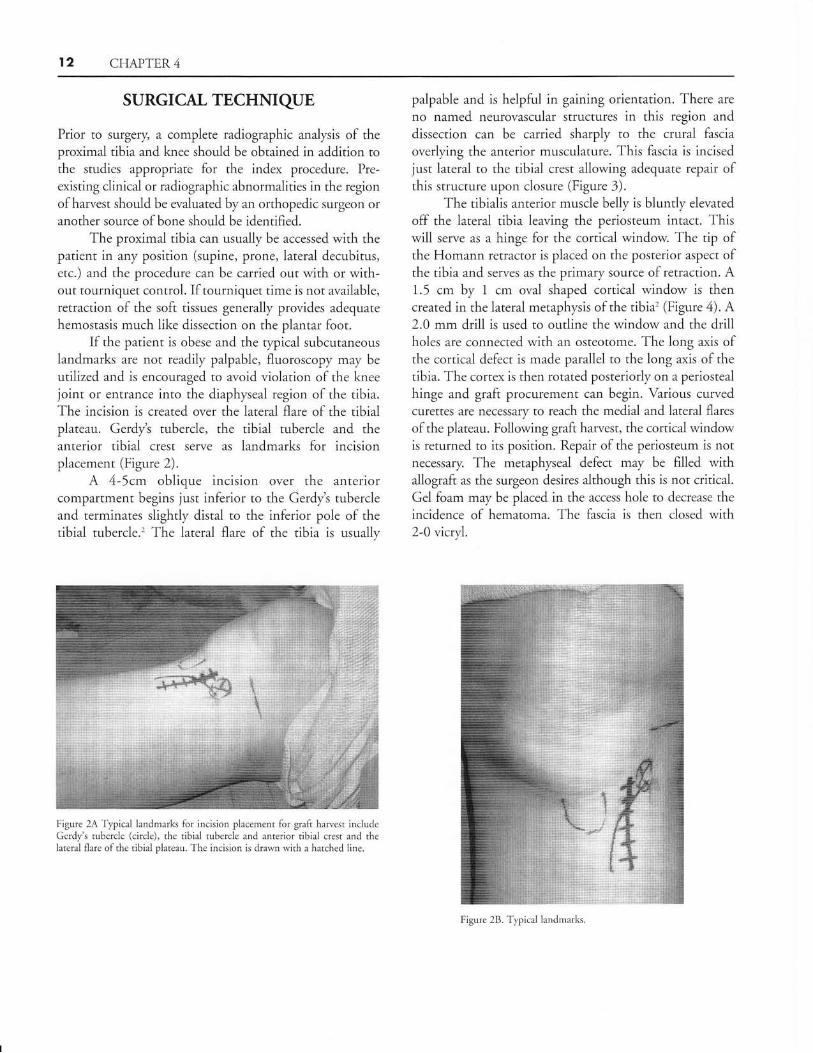
utilized and is encouraged to avoid violation of the kneejoint or entrance into the diaphyseal region of the tibia.The incision is created over the lateral flare of the tibialplateau. Gerdyt tubercle, the tibial tubercle and theanterior tibial crest serve as landmarks for incisionplacement (Figure 2).
A 4-5cm oblique incision over the anteriorcompartment begins just inferior to the Gerdyt tubercleand terminates slightly distal to the inferior pole of thetibial tubercle.' The lateral flare of the tibia is usually
Figure 2A'fypical landmarks for incision placement fbr graft hanest includeGerdy's tubercle (circle), thc tibial tubercle and anterior tibial crest and thelateral flare ofthe tibial plateau. The incision is drawn with a hatched line.
palpable and is helpful in gaining orientation. There are
no named neurovascular structures in this region and
dissection can be carried sharply to the crural fascia
overlying the anterior musculature. This fascia is incisedjust lateral to the tibial crest allowing adequate repair ofthis structure upon closure (Figure 3).
The tibialis anterior muscle belly is bluntly elevated
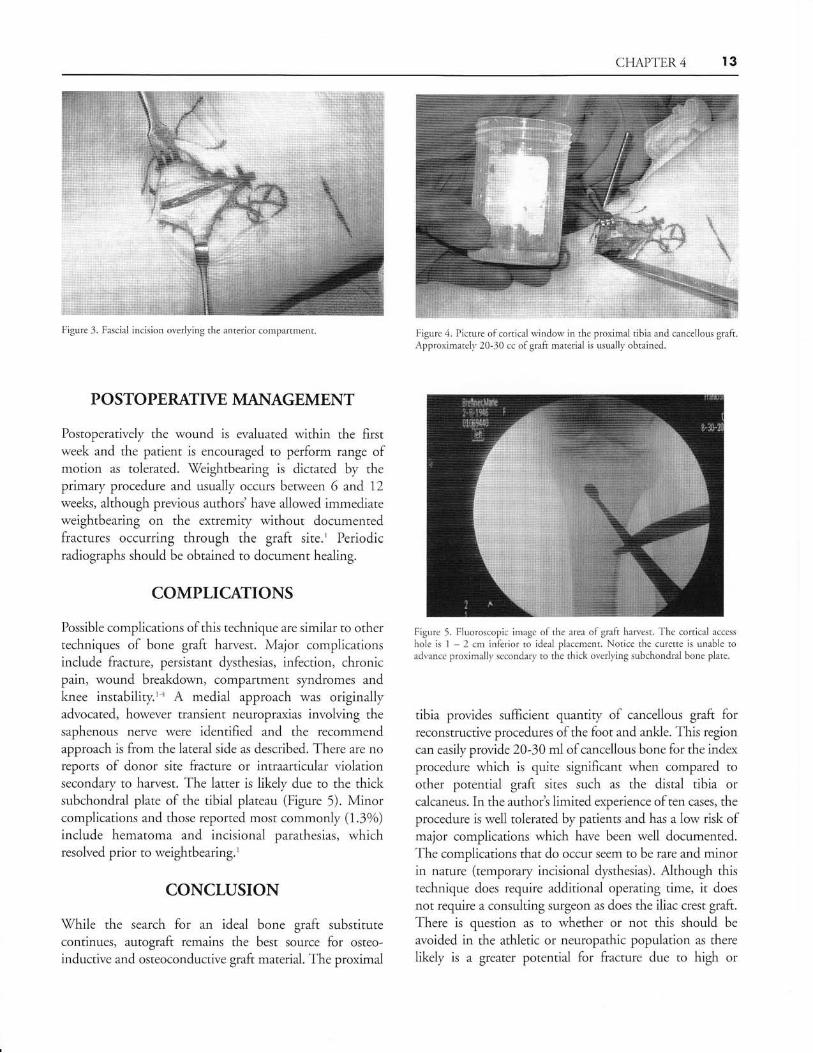
off the lateral tibia leaving the periosteum intact. Thiswill serve as a hinge for the cortical window. The tip ofthe Homann retractor is placed on the posterior aspect ofthe tibia and serves as the primary source of retraction. A1.5 cm by 1 cm oval shaped cortical window is thencreated in the lateral metaphysis of the tibia'(Figure 4). A2.0 mm drill is used to outline the window and the drillholes are connected with an osteotome. The long axis ofthe cortical defect is made paraliel to the long a-xis of the
tibia. The cortex is then rotated posteriorly on a periostealhinge and graft procurement can begin. Various curvedcurettes are necessary to reach the medial and lateral flares
of the plateau. Following graft harvest, the cortical windowis returned to its position. Repair of the periosteum is notnecessary. The metaphyseal defect may be filled withallograft as the surgeon desires although this is not critical.
Gel foam may be placed in the access hole to decrease the
incidence of hematoma. The fascia is then closed with2-0 vicryl.
Figure 28. Typical landmarks
CHAPTE,R 4 I3
F-igure 3. Fascial incision overlying the anterior compartment.
P O STO PERAITVE MANAGEMENT
Postoperatively the wound is evaluated lvithin the firstweek and the patient is encouraged to perform range ofmotion as tolerated. tWeightbearing is dictated by theprimary procedure and usually occurs between 6 and 72
weeks, although previous authors'have allowed immediateweightbearing on the extremiq/ without documentedfractures occurring through the graft site.' Periodicradiographs should be obtained to document healing.
COMPLICAIIONS
Possibie complications of this technique are similar to othertechniques of bone graft harvest. Major complicationsinclude fracture, persistant dysthesias, infection, chronicpain, wound breakdown, compartment syndromes andknee instability.'z A medial approach was originallyadvocated, however transient neuropraxias involving thesaphenous nerve were identified and the recommendapproach is from the lateral side as described. There are noreports of donor site fracture or intraarticular violationsecondary to harvest. The latter is likely due to the thicksubchondral plate of the tibial plateau (Figure 5). Minorcomplications and those reported most commonly (7.3o/o)
include hematoma and incisional parathesias, whichresolved prior to weightbearing.'
CONCLUSION
\X/hile the search for an ideal bone graft substitutecontinues, autograft remains the best source for osteo-
inductive and osteoconductive graft material. The proximal
FigrLre 4- Picture ofcortical windorv in the proximal tibia and cancellous graltApproxirnately 20-30 cc ofgraft material is usually obtained.
Figure 5. Fluoroscopic image ofthe area ofgralt haruest. The cortical access
hole is 1 2 cm inferior to ideal placernent. Notice the curette is unable toadvance proximallv sccondary to the thick overlying subchondral bone plate.
tibia provides sumcient quantity of cancellous graft forreconstructive procedures of the foot and ankle. This region
can easily provide 20-30 ml of cancellous bone for the index
procedure which is quite significant when compared toother potential graft sites such as the distal tibia orcalcaneus. In the authorb limited experience of ten cases, the
procedure is well tolerated by patients and has a low risk ofmajor complications which have been well documented.The complications that do occur seem to be rare and minorin nature (temporary incisional dysthesias). Although thistechnique does require additional operating time, it does
not require a consulting surgeon as does the iliac crest graft.
There is question as to whether or not this should be
avoided in the athletic or neuropathic population as there
likely is a greater potential for fracture due to high or

t4 CFIAPTER 4
unrecognized loads placed on the tibial plateau. Further
imaging studies need to be performed documenting the
neo-trabeculation which is thought to occur sometime after
graft harvest. Figure 6 shows a 9 month postoperative
CT scan demonstrating incomplete reestablishment oftrabecular patterns in the proximal tibial metaphysis. The
patient is asymptomatic and the clinical relevance of this
finding is uncertain. Long term studies investigating these
questions are necessary.
REFERENCES
1. O'Keefe RM Jr, fuemer BL, Butterfield SL. Hawesting of autogenous
cancellous bone graft lrom the proximal tibial netaphysis. J Orthop
Trauma.7991:5:469 74.2. Thorderson N, Early JS. Hanesting cancellous graft fi'otl the proximal
tbia l"oot Ankle Surg2004;3:206 9.
3. Alt V, Narvab A, Seligson D. Bone grafting from the proximal tibia.
J Trauma 1999;47:555 7.
4. Geideman WM, Brodsky J\X/, Earlv JS. Clinical results of harvcsting
autogenous cancellous graft lrom the ipsilateral proximal tibia for use
in foot and ankle surgery. Presented at: American Orthopaedic Foot
and Ankle Society 19th Annual Summer Meeting; Final Program
19:57r 2003.Figure 6. Postoperative CTincomplete reestablishment ofthe proximal tibial metaphysis
scan demonstratingtrabecular patterns in