thyroid dysfunction dr. mohammed ibrahim youssef (1)(1)
TRANSCRIPT

MCQ
1. 28 years old women with gravies disease in the 18th
week of pregnancy on carbimazole referred for
medication adjustment .
What of the following set of laboratory result is within the
recommended targets for this patient?
Total t3
70:220ng/dl
Freet4
(0.8;1.8ng/dl
Tsh
(0.5;5)
4002.10.05A
3501.80.1B
3301.51.5C
2801.32.5D
2101.03.5E

2. A 24 years old woman in the first trimester of pregnancy
present with heat intolerance , palpitation and failure to
achieve expected weight gain. she has no prior history of
thyroid disease and takes only prenatal vitamins. on
examination , her pulse is 112beat /min. she has no proptosis or
periorbital soft tissue changes her thyroid is slightly enlarged , and
she has resting hand tremors . free t4 is 25.7(normal 10.3-23.2
pmol/l)and serum TSH is 0.05 MIU/l Which one of the following
laboratory stuties is the most useful in determining the etiology of
this patient’s thyrotoxicosis?
A. TSH receptor antibody testing
B. Thyroid perioxidase antibodies.
C. Serum HCG level.
D. Free t3:freet4 ratio
E. RAIU usin I131
23/04/1436 2
video

Dr. Mohammed Ibrahim Youssef
Family Medicine Specialist
Albassam Diabetic Center .KSH

Objective:
Give an overview on updated clinical practice guidelines
(Published august.2012) for the management of thyroid dysfunction during pregnancy and postpartum .
Will be reviewed august 2015.
23/04/1436 4

Objective:
What are the normal physiological changes during
pregnancy?
How can we make interpretation of TFT in the context of
these changes?
hypothyroidism, or hyperthyroidism, how managed what's
our target?
Thyroid autoimmunity ! is it risky ?
Thyroid nodules & caner , how to manage?
Screening of thyroid dysfunctions ! with or against?

Thyroid problems during pregnancy.
1. Hypothyroidism.
2. Hyperthyroidism.
3. Gestational transient hyperthyroidism.
4. Autoimmune thyroid disease.
5. Thyroid nodules and cancer.
6. Iodine nutrition during pregnancy.
7. Postpartum thyroiditis.
8. Screening for thyroid dysfunction during pregnancy.
23/04/1436 6

Introduction..why guidelines.?
Pregnancy may affect the course of thyroid
Disorders, and conversely, thyroid diseases may affect
both the pregnant woman and the developing fetus.
Pregnant women may be under the care of multiple
health care professionals, including obstetricians,
nurse midwives, family practitioners, endocrinologists,
and/or internists, making the development of
guidelines more imporatant.
23/04/1436 7

Estrogen
TBGx2
TT4
TT3
HCG=TSH
TSH
TT3&TT4
FT4&FT3
Thyroid physiology
23/04/1436 8

23/04/1436 9
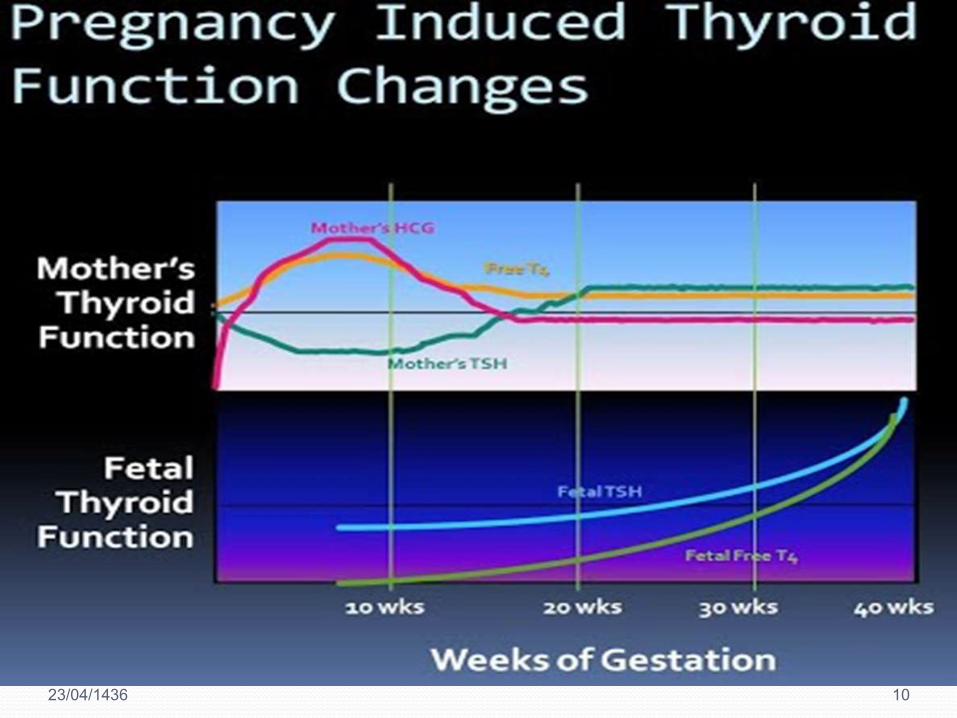
Increase in serum thyroxine-binding globulin (TBG) concentrations .
Estrogen effect.
2 fold increase.
Total t4 and t3 rise during the first half of pregnancy, plateauing at
approximately 20 weeks of gestation
Stimulation of the thyrotropin (TSH) receptor by human chorionic
gonadotropin (HCG).
Homology between the beta-subunit of HCG &TSH.
HCG &TSH are glycoprotein hormones.
Peak at 10 to 12 weeks gestation
Total (T4 and T3 )concentrations increase.
Free t4 and t3 increase slightly, usually within the normal range.
TSH reduced
Thyroid physiology
23/04/1436 10

Hypothyroidism
1. Hypothyroidism: maternal and
fetal aspects
23/04/1436 11

Hypothyroidism
Overt hypothyroidism occurs in 0.3–0.5% .
Subclinical hypothyroidism 2–3%.
Thyroid autoantibodies are found in 5–15% of women during childbearing age.
23/04/1436 12

23/04/1436 13

Hypothyroidism
Hypothyroid women have an increased prevalence of infertility, abortion,anemia, gestational hypertension, placental abruption,and postpartum hemorrhage .
Adverse fetal &neonatal outcomes including premature birth, low birth weight, and neonatal respiratory distress
Low IQ
23/04/1436 14

Trimester-specific reference ranges
23/04/1436 15
Hypothyroidism

FREE T4 INDEX
TOTAL T4 ASSAY
X (1.5)
FREE T4 ASSAY
0.3 to 3
3rd
trimester
0.2 to 3.0
2nd
trimester
0.1 to 2.5
1st
trimester
TSH Reference
range
MIU/L
23/04/1436 16
King Saud Hospital
23/04/1436 17
If hypothyroidism diagnosed before pregnancy, adjust of
the preconception thyroxine dose to reach TSH target ≤ 2.5 MIU/Liter.
thyroxine dose usually needs to be increased (30:50)% mostly during first trimester. (C)
Hypothyroidism

If hypothyroidism diagnosed during pregnancy, thyroid
function tests should be normalized as rapidly as possible.
maintain the target TSH ≤ 2.5 MIU/liter in the first
trimester (or 3MIU/liter in second and third trimesters) .
Thyroid function tests should be remeasured within 30–40
d and then every 4–6 wk
23/04/1436 18
Hypothyroidism

Euthyroid women with thyroid autoimmunity (TPO ab &thyroglobulin ab) are at risk of developing hypothyroidism and should be monitored for elevation of TSH every 4–6 wk.
After delivery, most hypothyroid women need to
Decrease the T4 dosage to the prepregnancy dose.
23/04/1436 19
Hypothyroidism

T4 replacement is recommended to women with SCH
(high TSH + normal free t4) regardless thyroid
peroxidase antibody status.(either positive or
negative).
(Normal TSH +Low FT4) treat or not??
23/04/1436 20
controversial and requires further study.
partial replacement therapy may be initiated with continued monitoring
Hypothyroidism

FridayThurs.WednesdayTuesdayMondaySundaySaturday
50+5050+505050505050
TSH ≤(2.5)
Thyroxine dose30%:50%
7 tab to 9 tabWeekly
Hypothyroidism
23/04/1436 21
Monitor frequently
Return back to prepregnancy dose
Anti TPO+ve

2. Hyperthyroidism
23/04/1436 22

HCG mediated hyperthyroidism
Hyperthyroidism
Gestational transient
thyrotoxicosis
Gestational trophoblastic
disease
Hyperemesis gravidarum
Graves disease
23/04/1436 23
prevalence of hyperthyroidism ranges from 0.1 to 0.4%.
Graves’ disease accounting for 85% of cases.
Graves’ disease may fluctuate during pregnancy, with exacerbation during the first trimester(high levels of HCG) and improvement by late gestation.
The presence of a goiter, especially with bruit or thrill, may point to true graves’ disease.
2. Hyperthyroidism….
23/04/1436 24

: ;
.
Maternal hyperthyroidism:Medically indicated preterm delivery, intrauterine growth restriction and low birth weight, preeclampsia,
Congestive heart failure, and fetal death.
Iatrogenic fetal hypothyroidism.
Central congenital hypothyroidism.
Fetal hyperthyroidism: intrauterine growth restriction,
Fetal tachycardia,
Fetal goiter,
Advanced bone age,
Fetal hydrops,
Preterm delivery, and
Fetal death
23/04/1436 25
2. Hyperthyroidism….

Recommendations.
Normal physiology Gestational
thyrotoxicosis
Overt hyperthyroidism
Must be distinguished from both normal physiology of pregnancy and gestational thyrotoxicosis.
Differentiation is supported by the presence of clinical evidence of autoimmune thyroid disease (typical goiter, and presence of thyrotropin receptor antibody (TRAb).
TPO-Ab may be present in either case. (B)
TSH in healthy pregnant women during the first trimester may be as low as 0.03 to 0.1 mU/L
Significant hyperthyroidism(gravies disease) in the first trimester will have a serum TSH <0.01 mU/L) associated with elevated free T4 and/or free T3 (or total T4 and/or total T3) measurement.
23/04/1436 26

freeT4 at the upper limit
(12 _ 22)pmol/l
Recommendations.
23/04/1436 27
For hyperthyroidism due to graves’ disease or thyroid nodules,
ATD therapy should be either:
Initiated (new diagnosis) or
Adjusted (for those with a prior history) to:
Maintain the maternal thyroid hormone levels for
free T4 at the upper limit of the non pregnant reference range. (B)

Recommendations.
PTU is the first line during the first trimester.
PTU may be associated with severe liver toxicity.
Liver toxicity may appear abruptly with PTU.
Monitor liver function in pregnant women on PTU every 3–4 wk .(C)
MMI (carbimazol)in 2nd and 3rd trimester.
MMI may be associated with specific congenital abnormalities . (B)
agranulocytosis
23/04/1436 28

PTU
Recommendations.
Choanal atresiaAplasia cutis
Hepatotoxicity
23/04/1436 29

Subtotal thyroidectomy may be indicated optimally
during the Second trimester if: severe adverse reaction to ATD therapy;
persistently high doses of ATD are required (over 30 mg/d of MMI or 450 mg/d of PTU)
patient is nonadherent to ATD therapy and has uncontrolled
hyperthyroidism. (c)
Recommendations.
23/04/1436 30
Radioactive iodine should not be given to a woman who is or may be pregnant. (A)
No data for or against termination of pregnancy after RAI exposure. (I)
Recommendations.
23/04/1436 31
No evidence that treatment of subclinical hyperthyroidism improves pregnancy outcome. It could potentially adversely affect fetal outcome. (C).
Subc l in ica l hyperthyroid ism

23/04/1436 32
Gravies disease
HCG mediated
TSH
FT4
FT3
TT3
SIGNS
TRAB
B.blockers
High normal ft4
Side effects SUBCLINICAL
HYPERTHYROIDISM
RAI
SURGERY SECOND
TRIMESTEER
ATD
BB

Hyperthyroidism
(Fetal aspects)
23/04/1436 33

Fetal (TSH) appears during the 10th to 12th week of gestation.
Fetal thyroid secretion increases gradually after 18th to 20th week.
Maternal thyroid hormones can cross the placenta??
TSH-receptor antibodies can cross the placenta and cause cause either fetal hyperthyroidism or hypothyroidism
Hyperthyroidism (Fetal aspects).
23/04/1436 34

Fetal& neonatal hyperthyroidism occurs in (1:5)% of neonates born to women with graves disease.
All fetuses of women with graves' disease should be monitored for fetal thyrotoxicosis .
Hyperthyroidism (Fetal aspects).
23/04/1436 35
HOW ?

TSH-receptor antibodies(TRAB) should be measured by 22wk gestation in:
Current graves’ disease.
History of graves ’ disease treated with RAI or thyroidectomy before pregnancy.
Previous neonate with graves’ disease.
Previously elevated TRAb.
Negative TRAb have very low risk of fetal or neonatal thyroid dysfunction. (B)
Recommendations.
23/04/1436 36

TRAb or( thyroid-stimulating Ig) elevated at least (2-3) folds
Fetal thyroid dysfunction should be screened for during the fetal anatomy ultrasound (18th-22 nd wk)
And TFT
Fetal thyroid enlargement.
growth restriction. Hydrops.
Tachycardia.cardiac failure.
MMI or PTU should be givenwith frequent clinical, laboratory, and
ultrasound monitoring.Umbilical blood
sampling
23/04/1436 37

2.HCG mediated hyperthyroidism
Gestational transient
thyrotoxicosis
Hyperemesis gravidarum
Trophoblastic hyperthyroidism
Familial gestational hyperthyroidism
23/04/1436 38

Gestational transient hyperthyroidism
Limited to the first half of pregnancy,
Elevated serum free T4 .
Suppressed or undetectable serum TSH.
Absence of thyroid autoimmunity.
Typically associated with hyperemesis gravidarum.
Thyroid stimulation is due to HCG itself, or molecular variant proteins related to HCG.
Hydatidiform mole or choriocarcinoma with very high elevations of HCG may be associated with clinical hyperthyroidism.
23/04/1436 39

Diagnosis:
Thyroid function tests and TRAb should be measured in patients with hyperemesis gravidarum and clinical features of hyperthyroidism.
Suppressed TSH, and elevated free T4.
Treatment:
Do not require ATD treatment(A).it remit spontaneously.
In women who appear significantly thyrotoxic or who have high serum total T3 . Clinical judgment should be followed .
Beta blockers (metoprolol) may be helpful and used with obstetrical agreement. (B)
23/04/1436 40
Gestational transient hyperthyroidism

23/04/1436 41
4. Autoimmune thyroid disease

4. Autoimmune thyroid disease
TSH every month during the first half of pregnancy
andat least once during the last trimester
Positive association exists between thyroid antibodies (anti TPO)and pregnancy loss.
Universal screening for thyroid antibodies, and possible treatment, cannot be recommended at this time.(like ATA.)
However, monitoring for the development of hypothyroidism was recommended
SO TSH should be measured before pregnancy, as well as during the first and second trimesters of pregnancy.(C)…. How?
23/04/1436 42
some experts, including some UpToDate editors suggest levothyroxine (50 mcg daily) with carful monitoring :
euthyroid women with TPO ab+ve
in case of recurrent miscarriage.
((Uptodate Jun 19, 2014))
4. Autoimmune thyroid disease
and miscarriage
23/04/1436 43

23/04/1436 44
5. Thyroid nodules and cancer

Pregnancy may promote the onset of growth of a thyroid
nodule .
No clear evidence that pregnancy worsens the survival
from well-differentiated thyroid cancer .
Some evidence that thyroid cancers discovered during
pregnancy have a greater chance of recurrence.
Evaluation is the same.
23/04/1436 45
5. Thyroid nodules and cancer

5. Thyroid nodules and cancer
FNA cytology should be performed for
predominantly Solid thyroid nodules greater than 1 cm discovered In pregnancy.
Nodules 0.5 cm to 1 cm in size should be considered for FNA if they have a high-risk history or suspicious findings on ultrasound.
Complex nodules 1.5–2 cm or larger .
During late pregnancy, FNA can be delayed until after delivery.
Ultrasound guided FNA is better. B
23/04/1436 46
Suspicious findings on ultrasound.
All solid consistency.
Calcifications, especially tiny or microcalcifications.
Really dark appearing or hypoechoic.Irregular margins.
Suspicious neck lymph nodes.
23/04/1436 47

if malignant or highly suspicious to exhibit rapid growth nodule:
Surgery should be offered in the second trimester.
Papillary cancer without evidence of advanced disease
Can be delayed until the postpartum period for definitive surgery. (B)
5. Thyroid nodules and cancer
23/04/1436 48

Give thyroxine to achieve suppressed but detectable TSH in pregnant women with
Treated thyroid cancer .
if surgical treatment delayed until postpartum.
keep free t4 or total t4 levels within the high normal range for pregnancy.(I)
RAI should not be given to women who are breastfeeding. (A)
Pregnancy should be avoided for 6 months to 1 year in women
received therapeutic RAI .(B)
5. Thyroid nodules and cancer.
23/04/1436 49
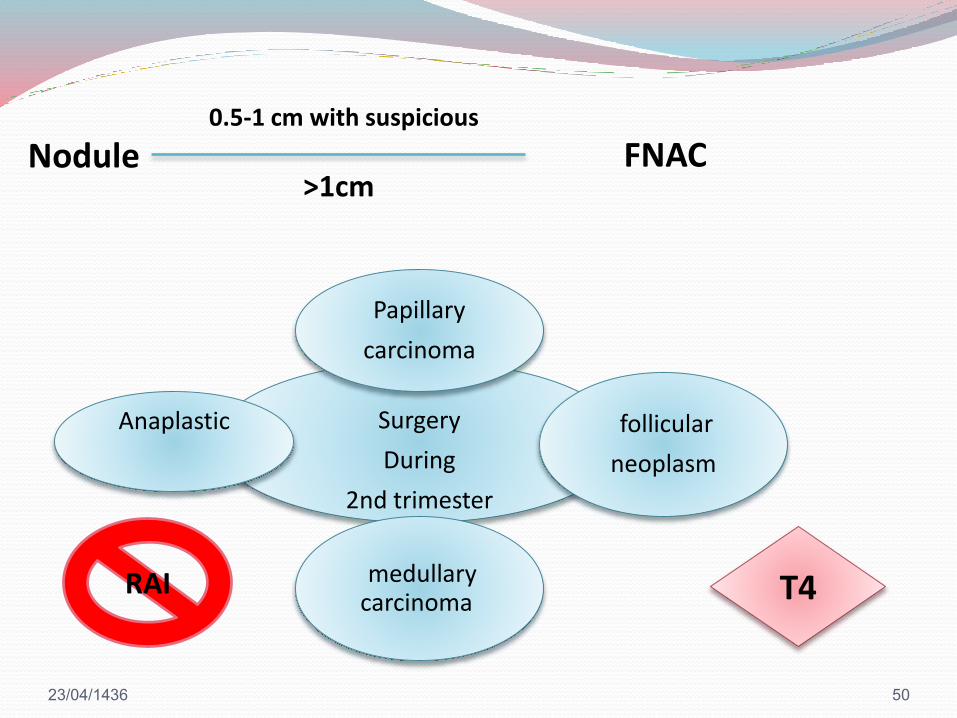
Surgery
During
2nd trimester
Papillary
carcinoma
follicular
neoplasm
medullary carcinoma
Anaplastic
RAI T4
Nodule0.5-1 cm with suspicious
>1cmFNAC
23/04/1436 50
23/04/1436 51
6.0. Iodine nutrition during
pregnancy

6.0. Iodine nutrition during pregnancy
Women in the childbearing age should have
an average iodine intake of 150 microgram/day.
As long as possible before and during pregnancy and breastfeeding, iodine intake should be increased their daily to 250 microgram on average. (A)
Breast milk provides 100 microgram iodine per day to the infant.
23/04/1436 52

During pregnancy and breastfeeding do not exceed twice the recommended daily dose ( 500 microgram iodine per day). (I)
Once-daily prenatal vitamins should contain 150–200 microgram iodine in the form of potassium iodide or iodate.
6.0. Iodine nutrition during pregnancy
23/04/1436 53

23/04/1436 54
7.0. Postpartum thyroiditis

PPT is the occurrence of
Hyperthyroidism. Or
Hypothyroidism. Or
Hyperthyroidism followed by hypothyroidism
During the first year postpartum in women without clinically evident thyroid disease ??Before pregnancy.
Caused by thyroid autoimmunity.
Exclusively in thyroid antibody positive.
7.0. Postpartum thyroiditis
23/04/1436 55

Prevalence:
In unselected populations is 7 %
Type 1 diabetes mellitus. 25%
The highest rates occur with
history of postpartum thyroiditis ( 42 %) and
positive antithyroid peroxidase antibodies (40 : 60)%
may occur after pregnancy loss (miscarriage, abortion, ectopic pregnancy), as well as after normal delivery.
23/04/1436 56
7.0. Postpartum thyroiditis
Insufficient data to recommend screening of all women for postpartum thyroiditis.(I)
Monitor TSH at 6–12 wk gestation and at 6 months postpartum for TPO ab + ve .(a)
Screening by TSH is recommended at 3 and 6 months postpartum in patients with
Type1 diabetes.
Chronic viral hepatitis. (B)
23/04/1436 57
7.0. Postpartum thyroiditis

PPT has Increased risk of developing permanent primary hypothyroidism in the 5- to 10-yr period after the episode of PPT.
Annual TSH level should be performed. (A)
23/04/1436 58
7.0. Postpartum thyroiditis

7.0. Postpartum thyroiditis: Treatment.
Asymptomatic hypothyroidismSymptomatic hypothyroidism
TSH less than 10 MIU/liter
Not planning for subsequent pregnancy
No intervention, but should be remonitored in 4–8 wk.
When a TSH above the reference range continues, women should be treated .
women With TSH above normal .
planning for pregnancy.
should be treated with levothyroxine.
Beta blockers. propranolol
23/04/1436 59
Symptomatic hyperthyroidism

Screening for thyroid dysfunction
during pregnancy
23/04/1436 60

Universal screening of healthy women for thyroid dysfunctionusing serum TSH before pregnancy is not recommended. (I)
Identify individuals at “high risk” for thyroid illness.
If high risk measure TSH .
IF >2.5 MIU/L repeat to confirm. Give low dose thyroxine to bring TSH below 2.5 mIU/liter.
Thyroxine can be discontinued if the woman does not become pregnant .
23/04/1436 61
8.0. Screening for thyroid dysfunction before&
during pregnancy

23/04/1436 62
High risk for thyroid illness:
Age over 30 years.
Family history or autoimmune thyroid disease or hypothyroidism
Goiter
Thyroid antibodies, primarily thyroid peroxidase antibodies
Symptoms or clinical signs suggestive of thyroid hypofunction
Type 1 DM or other autoimmune disorders
Infertility
History of miscarriage or preterm delivery
Prior head or neck irradiation or thyroid surgery
Women currently receiving levothyroxine replacement
Women living in a region with presumed iodine deficiency

Universal screening for anti-TPO antibodies either before or during pregnancy is not recommended.(C)
But if identified, screen for serum TSH abnormalities before pregnancy, as well as during the first and second trimesters of pregnancy (C)
23/04/1436 63
8.0. Screening for thyroid dysfunction
during pregnancy

for newly pregnant women. Two versions are presented:
Some members recommended screening of all pregnant women by the ninth week or at the time of their first visit. (C)
Others. Strongly support aggressive case finding to identify high-risk women.
23/04/1436 64
8.0. Screening for thyroid dysfunction
during pregnancy

23/04/1436 65

Summary
Consider the physiological changes during pregnancy.
Establish trimester specific ranges for TSH &free t4.
Maintain target TSH ≤ 2.5 during treatment of hypothyroidism
Maintain free T4 near upper limit during treatment of hyperthyroidism.
Do not give ATD in HCG mediated hyperthyroidism.
TRAB only with gravies disease.
PPT exclusively in anti TPO +ve.
Surgery for cancer thyroid optimally in 2nd trimester
Iodine requirement during pregnancy is 250 mcg.
23/04/1436 66

Abbreviations.
ATD, Antithyroid drug.
FNA, fine-needle aspiration.
GH, gestational hyperthyroidism.
HCG, human chorionic gonadotropin.
MMI, methimazole.
PPT, postpartum thyroiditis.
PTU, propylthiouracil.
TG, thyroglobulin.
TPO-Ab, thyroid peroxidase.
TRAb, TSH receptor antibodies.
RAI, radioactive iodine.
SCH, subclinical hypothyroidism.
23/04/1436 67

Referenes
Management of Thyroid Dysfunction during Pregnancy and Postpartum: An Endocrine Society Clinical Practice Guideline
Overview of thyroid disease in pregnancy last updated: Jun 19, 2014.
23/04/1436 68
23/04/1436 69