thursday, may 10. and. msh6 • tumor suppressor genes involved in lynch syndrome • mismatch...
TRANSCRIPT


Thursday, May 10 7:30 a.m. - 7:55 a.m. Registration
7:55 a.m. - 8 a.m. Welcome by Daniel Knight, MD, FAAFP
8 a.m. - 9 a.m. MACRA Update: The Top 8 for 2018 by Amy Mullins, MD
9 a.m. - 10 a.m. Breast Cancer Update by Daniela Ochoa, MD
10 a.m. - 10:15 a.m. Break
10:15 a.m. - 11:15 a.m. Marijuana in the Field of Medicine: Rules, Roles and Rights of the PCP by Nate Smith, MD
11:15 a.m. - 12:15 p.m. Chronic Migraine: How Did We Get Here, and Where Do We Go From Here? by Dale Carter, MD
12:15 p.m. - 1 p.m. Lunch
1 p.m. - 2 p.m. Talking Dirty/Talking Turkey: Public Health and Tobacco by Gary Wheeler, MD
2 p.m. - 2:45 p.m. Smoke-Free for Baby and Me by Nicole Ward, MSN
2:45 p.m. - 3 p.m. Break
3 p.m. - 4 p.m. Incorporating Genetics into Gynecologic Cancer Care by Kristin Zorn, MD 4 p.m. - 5 p.m. Technology is Changing Healthcare by Charles Caldwell Jr., MD
Friday, May 11 7:30 a.m. - 8 a.m. Registration / Exhibits
8 a.m. - 9 a.m. Physician Involvement in Cancer Care Support Groups on Facebook by Jerad Gardner, MD
9 a.m. - 10 a.m. Practice Transformation Part 1: Project Management and the Business Model by Gary Bevill, MD, and Pete Atkinson, MHA
10 a.m. - 10:15 a.m. Break / Exhibits
10:15 a.m. - 11:15 a.m. Practice Transformation Part 2: Provider Engagement and Team-Based Care by Rachel Wallis, MPH 11:15 a.m. - 12:15 p.m. Opiate Prescribing and Use of the PDMP System by Jennifer Roberts, BS 12:15 p.m. - 1 p.m. Lunch / Exhibits
1 p.m. - 2 p.m. Case-Based Vaccine Update: Shingles, Pneumococcal and Adolescent by Robert Hopkins, MD 2 p.m. - 2:45 p.m. Practical Steps in Management of Fibromyalgia by Aaroop Haridas, MD 2:45 p.m. - 3 p.m. Break / Exhibits 3 p.m. - 4 p.m. ZZZ’s Without A Breeze: Sleep Apnea and OSA by Caris Fitzgerald, MD
4 p.m. - 5 p.m. When Counting Sheep Doesn’t Work: Insomnia and Sleep Medications by Caris Fitzgerald, MD
Saturday, May 12
7:30 a.m. - 8 a.m. Registration 8 a.m. - 8:30 a.m. Common Tendon Disorders of the Upper Extremity by Mark Tait, MD 8:30 a.m. - 9 a.m. Evaluation and Management of Numbness and Tingling in the Hands by John Bracey, MD 9 a.m. - 9:30 a.m. Common Causes of Shoulder Pain by Lawrence O’Malley, MD 9:30 a.m. - 9:45 a.m. Q&A for Upper Extremities 9:45 a.m. - 10 a.m. Break
10 a.m. - 10:30 a.m. PCP Ortho Review: Knee Pain Diagnosis and Treatment by Mike Cassat, MD 10:30 a.m. - 11 a.m. Ortho Review of Common Hip-Related Issues by Paul Edwards, MD 11 a.m. - 11:30 a.m. Evaluation of Foot and Ankle Pain by Chelsea Mathews, MD 11:30 a.m. - 11:45 a.m. Q&A for Lower Extremities 11:45 a.m. - 12:30 p.m. Lunch
12:30 p.m. - 1 p.m. Common Neck Issues by David Bumpass, MD 1 p.m. - 1:30 p.m. Evaluation and Management of Back Pain by David Bumpass, MD 1:30 p.m. - 1:45 p.m. Evaluation of Extremity Masses by Corey Montgomery, MD 1:45 p.m. - 2:15 p.m. Common Pediatric Musculoskeletal Disorders by Michael Israel, MD 2:15 p.m. - 2:30 p.m. Break Hands-On Workshop 2:30 p.m. - 3 p.m. Registration 3 p.m. - 5 p.m. Upper and Lower Extremities Joint Injection Workshop by John Bracey, MD, and Mike Cassat, MD

I
Medical Directors Marybeth Curtis, RN, BSN Nurse Educator Dept. of Family and Preventive Medicine UAMS College of Medicine Amanda Ferstl, PharmD Clinical Assistant Professor Ambulatory Care Pharmacist UAMS College of Pharmacy Diane Jarrett, EdD Assistant Professor Director of Education UAMS Dept. of Family and Preventive Medicine Shashank Kraleti, MD Assistant Professor Residency Program Director UAMS Dept. of Family and Preventive Medicine Kent D. McKelvey, MD Associate Professor, Family Medicine and Genetics Winthrop P. Rockefeller Chair in Clinical Genetics UAMS College of Medicine Bruce Schratz, MD Adjunct Faculty UAMS Dept. of Family and Preventive Medicine Stephen Sorsby, MD Assistant Professor UAMS Dept. of Family and Preventive Medicine
Course Director Alysia Dubriske, M.Ed., CHES Director of Community Health and Education UAMS Dept. of Family and Preventive Medicine
Exhibitors Aledade Allergan Pharmaceuticals Arkansas Foundation for Medical Care Arkansas Immunization Action Coalition Arkansas Prostate Cancer Foundation Arkansas Trauma Rehabilitation Program Boehringer-Ingelheim The Bridgeway Complete Provider Resource Correct Care Solutions Esperanza Hope Clinic Incyte NexMed Solutions UAMS Alumni Association UAMS AR Saves UAMS Adult Sickle Cell Clinical Program UAMS Outpatient Dietitian Services UAMS Physician Relations
Special Thanks:
Arkansas Dept. of Health’s Tobacco Prevention and Cessation Program Arkansas Blue Cross Blue Shield

II
Table of Contents
Speaker Title Section
Amy Mullins, MD MACRA Update: The Top 8 for 2018 1
Daniela Ochoa, MD Breast Cancer Update 2
Nate Smith, MD Marijuana in the Field of Medicine: Rules, Roles and Rights of the PCP
3
Dale Carter, MD Chronic Migraine: How Did We Get Here and Where Do We Go From Here?
4
Gary Wheeler, MD Talking Dirty/Talking Turkey: Public Health & Tobacco 5
Nicole Ward, MSN Smoke-Free for Baby and Me 6
Kristin Zorn, MD Incorporating Genetics into Gynecologic Cancer Care 7
Charles Caldwell Jr., MD Technology is Changing Healthcare 8
Jerad Gardner, MD Physician Involvement in Cancer Care Support Groups on Facebook
9
Gary Bevill, MD Pete Atkinson, MHA
Practice Transformation Part 1: Project Management and the Business Model
10
Rachel Wallis, MPH Practice Transformation Part 2: Provider Engagement and Team-Based Care
11
Jennifer Roberts, MS Opiate Prescribing and Use of the PDMP System 12
Robert Hopkins, MD Case-Based Vaccine Update: Shingles, Pneumococcal and Adolescent
13
Aaroop Haridas, MD Practical Steps in Management of Fibromyalgia 14

III
Caris Fitzgerald, MD ZZZ’s Without A Breeze: Sleep Apnea and OSA 15
Caris Fitzgerald, MD When Counting Sheep Doesn’t Work: Insomnia and Sleep Medications
16
Mark Tait, MD Common Tendon Disorders of the Upper Extremity 17
John Bracey, MD Evaluation and Management of Numbness and Tingling in the Hands
18
Lawrence O’Malley, MD Common Causes of Shoulder Pain 19
Mike Cassat, MD PCP Ortho Review: Knee Pain Diagnosis and Treatment 20
Paul Edwards, MD Ortho Review of Common Hip-Related Issues 21
Chelsea Mathews, MD Evaluation of Foot and Ankle Pain 22
David Bumpass, MD Common Neck Issues 23
David Bumpass, MD Evaluation and Management of Back Pain 24
Corey Montgomery, MD Evaluation of Extremity Masses 25
Michael Israel, MD Common Pediatric Musculoskeletal Disorders 26

IV
Our pledge to healthy conferences
UAMS Family Medicine Resolution to Host Healthy Conferences
Whereas the Dietary Guidelines for Americans 2015 state that Americans consume too much sodium, added sugars, refined grains and solid fats and not enough fruits, vegetables and whole grains; and
Whereas the Physical Activity Guidelines for Americans 2008 state that Americans should get 150 minutes of moderate to vigorous physical activity each week; and Whereas studies show a strong relationship between the physical and social environments of the workplace and the health behaviors of employees; and Whereas nearly half of many people’s waking hours are spent at work, and many of those hours are spent in meetings and conferences; and
Whereas the foods and beverages available at meetings and conferences are often high in fat, added sugars and sodium and contain few fruits, vegetables and whole grains; and
Whereas meetings and conferences generally involve too much time sitting and provide little opportunity for physical activity; and
Whereas the Department of Family and Preventive Medicine has the ability to model healthy eating and help to change social norms around meeting practices; and
Whereas it is consistent with the goals of the Department of Family and Preventive Medicine to support people’s ability to eat well while at work events; therefore be it
Resolved that the UAMS Department of Family and Preventive Medicine's conferences will adhere to healthy meeting guidelines; and we will practice the guidelines set forth by the National Alliance for Nutrition and Activity.
Food and Beverage Choices: Beverages are available including water, coffee and unsweetened tea. Meals and snacks will offer fresh fruits and vegetables and lean proteins.
Activity Breaks: We encourage you to stand between speakers to stretch and to move during the breaks. You are in a safe location to take a walk around the block during breaks. Take advantage of the fresh air by using the balconies.
Tobacco Free: The UAMS campus is tobacco-free. We ask that you refrain from all forms of tobacco and electronic cigarette devices even within your car while on campus.
Sustainability: Please use the recycling bins provided for plastic and aluminum.

V
Course Announcements
Parking validation: Please be sure to have your parking validated at the registration desk.
Please participate in electronic and paper CME evaluations. Evaluation is a creditable portion of CME/CE activities and is required by all accrediting bodies. Using electronic evaluations saves provides better reports to help shape future programming. Your opinion matters to us! So click and share.
Please wear nametags—we want to get to know you!
Please help us keep the auditorium clean by removing your trash at each break. Please do not leave valuables unattended.
Please silence all cell phones, pagers, and other devices.
In order to receive CME/CE credit, all participants MUST complete and return the appropriate Continuing Medical Education evaluation and statement of attendance. UAMS is a smoke-free facility It is the policy of UAMS to promote the health, well-being and safety of visitors, employees and students while on the UAMS campus. Smoking and the use of tobacco products by employees, students and visitors are prohibited within all UAMS-owned or leased facilities and UAMS adjacent grounds, including parking lots and ramps.

VI
UAMS Disclosure Policy
It is the policy of the University of Arkansas for Medical Sciences (UAMS) Office of Continuing Education to ensure balance, independence, objectivity and scientific rigor in all sponsored or jointly sponsored educational activities. All individuals who are in a position to control the content of the educational activity (course/activity directors, planning committee members, staff, teachers or authors of CME) must disclose all relevant financial relationships they have with any commercial interest(s) as well as the nature of the relationship. Financial relationships of the individual’s spouse or partner must also be disclosed if the nature of the relationship could influence the objectivity of the individual in a position to control the content of the CME. The ACCME describes relevant financial relationships as those in any amount occurring within the past 12 months that create a conflict of interest. Individuals who refuse to disclose will be disqualified from participation in the development, management, presentation or evaluation of the CME activity. The following planning committee members, moderators and speakers for the 40th Annual Family Medicine Intensive Review Course have no financial relationships with commercial interests. Alysia Dubriske, MEd, CHES Marybeth Curtis, RN, BSN Amanda Ferstl, PharmD Diane Jarrett, EdD Shashank Kraleti, MD Bruce Schratz, MD Stephen Sorsby, MD The Accreditation compliance reviews Courtney Bryant & Cathy Buzbee have no relevant financial relationships with commercial interest to disclose.
Pete Atkinson, MHA Gary Bevill, MD John Bracey, MD David Bumpass, MD Charles Caldwell Jr. MD Mike Cassat, MD Dale Carter, MD Caris Fitzgerald, MD Jerad Gardner, MD Aaroop Haridas, MD Robert Hopkins, MD Michael Israel, MD
Chelsea Mathews, MD Corey Montgomery, MD Amy Mullins, MD Lawrence O’Malley, MD Nate Smith, MD Daniela Ochoa, MD Jennifer Roberts, BS Mark Tait, MD Rachel Wallis, MPH Nicole Ward, MSN Gary Wheeler, MD Kristin Zorn, MD
The following speakers have financial relationships with commercial interests which have been resolved:
1) Paul Edwards, MD – Patent holder, DJO Surgical

VII
Accreditations
In support of improving patient care, University of Arkansas for Medical Sciences is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team.
AMA Designation Statement The University of Arkansas for Medical Sciences designates this live activity for a maximum of 23 AMA
PRA Category 1 AMA PRA Category 1 Credits™, Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The University of Arkansas for Medical Sciences College of Pharmacy is accredited by the
Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
These educational activities have been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Pharmacy Education (ACPE) through the co-sponsorship of the University of Arkansas for Medical Sciences College of Pharmacy and the University of Arkansas for Medical Sciences Department of Family & Preventive Medicine. These activities will provide pharmacists up to 23 contact hours or 2.30 CEUs.
American Nurses Credentialing Center (ANCC)
The University of Arkansas for Medical sciences designates this live activity for a maximum of 23 ANCC contact hours. Nursing contact hours will be awarded for successful completion of program components based upon documented attendance and completion of evaluation materials.
National Commission for Health Education Credentialing, Inc.
The National Commission for Health Education Credentialing, Inc. has reviewed and approved for up to
15.5 entry-level CECH. Provider number: 100173. Program number: 31116.
Academy of Nutrition & Dietetics
The Commission on Dietetic Registration, the credentialing agency for the Academy of Nutrition &
Dietetics has approved this activity for up to 21 CPEUs hours. Activity #140521.
Physical Therapy
The Arkansas State Board of Physical Therapy has approved this activity for 21 total contact hours.
Respiratory Therapy The Arkansas State Medical Board has approved this activity for up to 11 CEU’s for respiratory therapist by the Respiratory Care Examining Committee. Program #ASMB RT04172018.
Thursday, May 10, 2018: 4 CEU’s 1. MACRA Update: 1 ceu 2. Marijuana in the Field of Medicine: 1 ceu 3. Public Health and Tobacco: 1 ceu 4. Technology is Changing Healthcare: 1 ceu
Friday, May 11, 2018: 7 CEU’s 1. Cancer Care Support Groups on FB: 1 ceu 2. Practice Transformation 1: 1 ceu 3. Practice Transformation 2: 1 ceu 4. Opiate Prescribing: 1 ceu 5. Case-Based Vaccine Update: 1 ceu 6. ZZZ’s Without Breeze: 1 ceu 7. Insomnia and Sleep Meds: 1 ceu

1
MACRA Update: The Top 8 for 2018
Amy Mullins, MD
Medical Director for Quality Improvement American Academy of Family Physicians
Table of Contents

MACRA Update:The Top 8 For 2018
Amy Mullins, MD, CPE, FAAFP
MACRAM makingA allC cliniciansR reallyA angry
Medicare Accessand CHIP
ReauthorizationAct

What Does MACRA Do?
3
• Consolidates quality programs
Merit-Based Incentive Payment System (MIPS)
• Potential for bonus payment for participation
Advanced Alternative Payment Models (AAPM)
MIPS Performance Categories
4
Quality Cost ImprovementActivities
AdvancingCare
Information(ACI)

Weighting Progression
2017 2018 2019
Quality 60% 50% 50-30%
Cost 0% 10% 10-30%
Advancing Care Information 25% 25% 25%
Improvement Activities 15% 15% 15%
Advanced APMs Perks
• Not subject to MIPS
• 5% bonus 2019 2024
• Higher fee schedule update to 0.75% from 2026onward
6
2017 Primary Care Advanced APMs• Shared Savings Program (Tracks 2 & 3)• Next Generation ACO Model• Comprehensive Primary Care Plus (CPC+)• Vermont Medicare ACO Initiative (as part of the
Vermont All Payer ACO Model)
*2018 AAPMs announce as approved
7
8

Question #1
• How will you participate in QPP in performanceyear 2018?
• A. MIPS• B. AAPM• C. I’m Exempt• D. Don’t Know
9
Update #1:Low volume Threshold

Low volume Threshold• 2017: 100 Medicare Part B beneficiaries, or received
$30,000 or less in Medicare Part B payments• 2018: 200 Medicare Part B beneficiaries, or
received $90,000 or less in Medicare Part B payments(excludes Part B Drugs)
Low Volume Threshold

Low volume ThresholdThe Centers for Medicare and
Medicaid Services (CMS) has
published a CMS Look-Up Tool for
clinicians to verify their MIPS-
eligibility status by entering their
National Provider Identifier (NPI)
number
qpp.cms.gov
Update #2:Virtual Groups

VirtualGroups
Virtual Group
10 or fewer
Geographyor Specialty
WrittenAgreement
One Year
“All orNothing”
CombinedScore
applied toNPI
Virtual Groups
Those who fall below the
low-volume threshold can
participate in virtual groups,
but will not receive a
payment adjustment
(either positive or negative)

Update #3:Cost
Cost
• 2017: Cost 0% of the MIPSfinal score
• 2018: Cost accounts for 10%MIPS final score
• 2019 2021: Cost willaccount for 10 30% for theMIPS final score
Quality2017: 60%2018: 50%
2019 21: 5030%Cost
2017: 0%2018: 10%
2019 21: 1030%

Update #4:Performance Period
Performance Period• 2017 Pick Your Pace• 2018 – Quality/Cost (Full Year) | ACI/ IA (90 Days)
Quality/Cost Performance Period Feedback Available 2019
Data Submission Deadline
3/31/2019
Payment Adjustment 1/1/2020
ACI/IA Performance Period

Update #5:Improvement Activities (IA) andPCMH
Question
• Are you a recognized/certified PCMH?• A Yes• B No

IA and PCMH• 2017: One member of the TIN could have PCMH
“recognition” for 100% IA credit• 2018: 50% of TIN practice sites need PCMH
“recognition” for the TIN to receive full IA credit
IA and PCMH• Recognized/Certified still
defined as: NCQA,
AAAHC, TJC, URAC, and
Accrediting bodies that
have certified 500 or more
practices
• IA still account for 15% of
MIPS final score

Update #6:Bonus Points
Small Practice Bonus Points
• Small practices: 15 or fewer• Five points added to MIPS Final Score• Must submit data in at least one MIPS
category

Complex Patient Bonus Points
+ x =_______
Complex Patient Bonus Points
+ x =______
= .20

Update #7Performance Threshold
Performance Threshold
Performance Threshold in 2017: 3
Performance Threshold in 2018: 15
Exceptional Performance: 70
New provision: The Secretary may set the PerformanceThreshold for program years 2019, 2020 and 2021 (it willgradually increase)

Update #8Employed Physicians and Residents

Employed Physicians andResidents
• MIPS scores followyou
• MIPS scores arepublicly available
• Consider a practices’MIPS score as youevaluate employmentcontracts
*More information in the FPM Employed Physician Supplement
Resources Available• aafp.org/MACRAReady• qpp.cms.gov• FPM• TCPI: aafp.org/tcpi• QPP Service Center: 866 288 8292

MIPS Playbook• Step by Step guide• 2017 MIPS Playbook
available• 2018 MIPS Playbook
Coming Soon
Questions?Amy Mullins, MD, CPE, FAAFP

2
Breast Cancer Update
Daniela Ochoa, MD
Assistant Professor Department of Surgery – Breast Oncology
UAMS
Table of contents

Breast Care UpdateA Breast Surgeon
Perspective
Daniela A. Ochoa, M.D., F.A.C.S.Breast Surgical Oncology
UAMS
Update on Current Recommendations for the Treatment of Breast Disease for the Primary Care
Physician
No Disclosures

Objectives• Initial Evaluation of Patient with Breast Complaint• When to Refer• Screening Recommendations
• Mammograms
• MRI• Risk Factors• Genetics
Initial Evaluation• Thorough Hx including Risk Factors
• Prior Biopsies• H/o Atypia• Family History – 1st Degree Relatives, Pre Menopausal Breast Cancers
• PE• Bilateral Breasts and LN Basins• Abd Exam
• Diagnostic Imaging• MMG/US
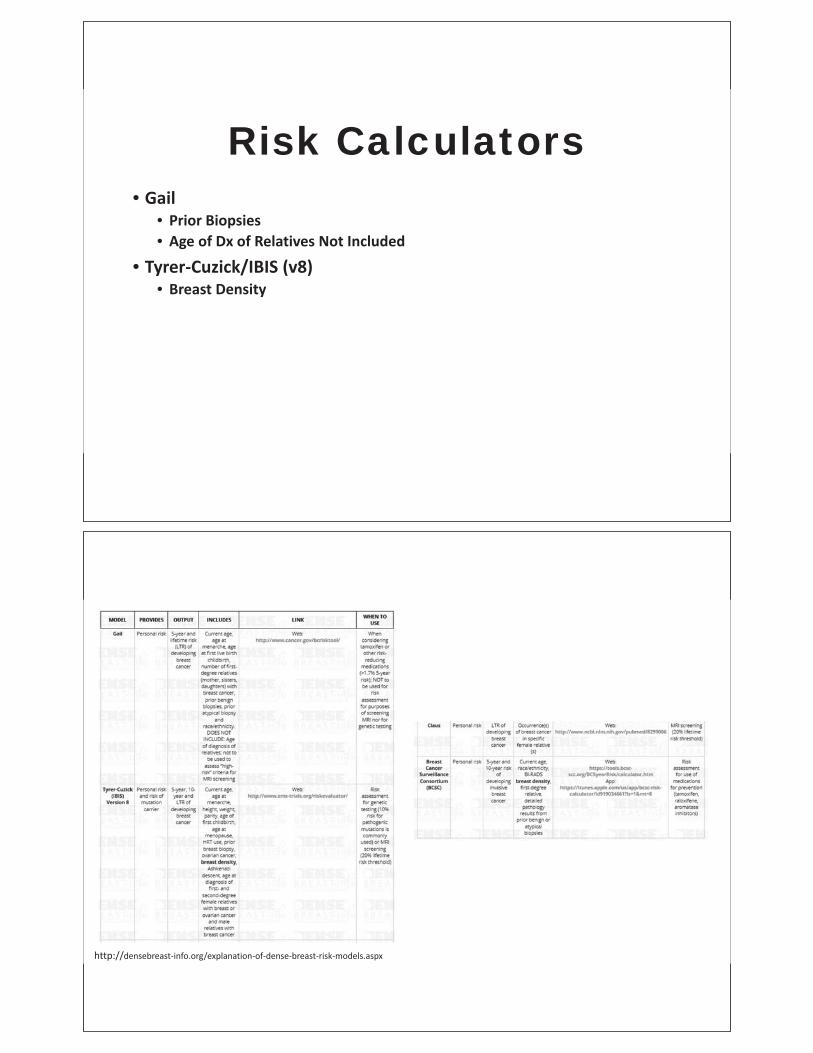
Risk Calculators• Gail
• Prior Biopsies• Age of Dx of Relatives Not Included
• Tyrer Cuzick/IBIS (v8)• Breast Density
http://densebreast info.org/explanation of dense breast risk models.aspx

http://www.ems trials.org/riskevaluator/
Amy Degnim, MD. ASBrS 2016

Refer• Abnormal Imaging or Pathology
• Birads 4 & 5 in Need of Bx, Atypia• Percutaneous Biopsy is Standard of Care
• Discordant Findings• Mass on Exam with No Imaging Correlate• Benign Pathology with Highly Suspicious Imaging (Birads 5)
• High Risk Stratification and Screening• Atypia, Family History
• Questionable Findings or Need for AdditionalEducation/Reassurance
Refer• Confusing Entities
• Inflammatory Breast Ca• Punch Biopsy
• Mastitis/Abscess• Pain, Induration• Ultrasound• Aspiration vs I&D• Biopsy
• Paget’s Dz• Biopsy
• Pregnancy, Young Pt• Can Get Breast Cancer Too!
• Beware of Delay in Diagnosis

Screening• ACR – American College of Radiology• ASBrS – American Society of Breast Surgeons• ACS – American Cancer Society• USPSTF – US Preventive Services Task Force• UAMS
Breast Cancer Risk: Age as a Risk Factor
By age 20 1 out of 2,532By age 30 1 out of 242 0.41%By age 40 1 out of 67 1.5%By age 50 1 out of 36 2.8%By age 60 1 out of 29 3.4%By age 70 1 out of 32 3.1%Lifetime risk 1 out of 9 11.1%
ref: Cancer Council
Which patientsare at higher risk
NOW?

https://www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf
https://www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf
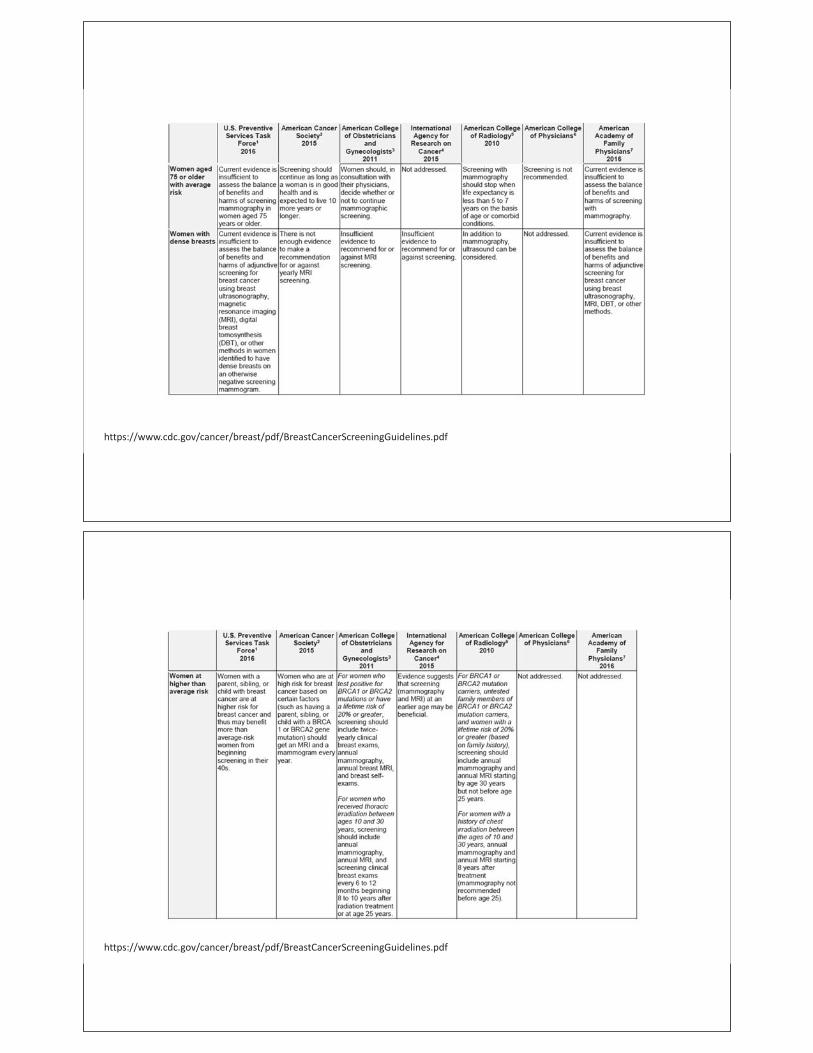
https://www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf
https://www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf

https://www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf
https://www.breastsurgeons.org/new_layout/about/statements/PDF_Statements/Screening_Mammography.pdf

Mammograms• When Can I Stop?
• American Cancer Society• Screening Should Continue as Long as a Woman is in Good Health and is Expected to Live 10 More Years
or Longer• USPSTF
• The Current Evidence is Insufficient to Assess the Benefits and Harms of Screening Mammography inWomen 75 years and Older
• ASBrS• 3 Observational Studies Showing Benefit Provided the Women Do Not have Severe Co Morbidities• 2 Studies Found a Survival Benefit for Screening Women with Mild Co Morbidities and No Benefit for
Women with Severe Co Morbidities• Another Study Did Show Cancers were Detected at an Earlier Stage• Mammographic Screening in an Older Compared to a Younger Population Would be Expected to Have a
Lower Rate of False Positives and Unnecessary Biopsies but Higher Risk for Over Diagnosis• Over Treatment May be More of a Problem in Women with Competing Co Morbidities Leading Experts
to Recommend Mammographic Screening in Women with at Least a 5 year Life Expectancyhttps://www.cancer.org/healthy/find cancer early/cancer screening guidelines/american cancer society guidelines for the early detection of cancer.htmlhttps://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/breast cancer screeningBadgwell BD, Giordano SH, Duan ZZ, et al., Mammography before diagnosis among women age 80 years and older with breast cancer. J Clin Oncol. 2008;26:2482 2488.Schonberg MA, Breslau ES, McCarthy EP. Targeting of mammography screening according to life expectancy in women aged 75 and older. J Am Geriatr Soc. 2013;61:388 395.Houssami N., Irwig L, Simpson JM, McKessar M, Blome S, Noakes J. Sydney Breast Imaging Accuracy Study: Comparative sensitivity and specificity of mammography and sonography inyoung women with symptoms. AJR Am J Roentgenol. 2003;180:935 940.

MRI• High Risk >20%
• Atypia, Fam Hx
• Brain and Bone Contrast Accumulation?• Gadoterate meglumine (Dotarem) Option
• Genetic Mutations• Cancer?
Kanda et al. High signal intensity in the dentate nucleaus and globus pallidus on unenhanced T1 weighted MR images: relationship with increasing cumulative dose of a gadoliniumcontrast material. Radiology 2014.Kanda et al. Gadolinium Deposition after Contrast enhanced MR Imaging. Radiology 2015.McDonald et al. Intracranial Gadolinium Deposition after Contrast enhanced MR imaging. Radiology 2015.Kanda et al. Brain gadolinium deposition after administration of gadolinium based contrast agents. Jpn J Radiol 2016.Olchowy, C. et al. The presence of the gadolinium based contrast agent depositions in the brain and symptoms of gadolinium neurotoxicity – A systematic review. PLOS One. Feb 2017.

MRI• ASBrS Recommendations – Consensus Statement 2017
• Not Routine in Newly Dx of Breast Ca• Occult Dz in Paget’s or Ax LN Mets• Extent of Dz (Multi focal or Multi centric Dz Concerns in ILC, Extremely Dense Breast
Tissue, Discrepancies bet PE and MMG/US)• Neoadj Syst Tx Response Assessment• Further Eval of Indeterminate Findings• Eval of Suspected Implant Rupture (Silicone)• High Risk Screening (Gene+, Chest XRT, >20%)• Not Rec’d
• VUS• H/o Breast Ca• Breast Pain• Inflammatory Changes
• Inconclusive• Nipple D/c• High Risk Lesions
https://www.breastsurgeons.org/new_layout/about/statements/index.php
Risk Factors for Breast Cancer

Risk Factors for Breast Cancer
Risk Factors for Breast Cancer

Bland, Kirby I., MD; Copeland, Edward M., MD; Klimberg, V. Suzanne, MD, PhD; Gradishar, William J., MD. The Breast: ComprehensiveManagement of Benign and Malignant Diseases, Fifth Edition. 2018
Bland, Kirby I., MD; Copeland, Edward M., MD; Klimberg, V. Suzanne, MD, PhD; Gradishar, William J., MD. The Breast: ComprehensiveManagement of Benign and Malignant Diseases, Fifth Edition. 2018

Bland, Kirby I., MD; Copeland, Edward M., MD; Klimberg, V. Suzanne, MD, PhD; Gradishar, William J., MD. The Breast: ComprehensiveManagement of Benign and Malignant Diseases, Fifth Edition. 2018
Risk Factors for Breast Cancer
• Most Women Don’t Have Any• Dietary Risks
• Alcohol• Lack of Fruits and Vegetables• Lack of Fiber• Obesity

Genetics• Panel Testing
• Insurance May Only Cover One Test• Caution When Using It!
• Counseling• VUS – Variant of Uncertain Significance• Negative Result Does Not Eliminate Possibility of Genetic Predisposition
All Cancer Arises From Gene Mutations
Germline Mutations Somatic Mutations
Somatic mutation (e.g., breast)
Mutationin egg or
sperm
All cells affected in offspring
Parent Child
Present in Egg or SpermAre Heritable Cause Cancer Family Syndromes5-10% of Cancer
Occur in Non-germline Tissues Are Non-heritableSporadic Cancer90-95% of Cancer
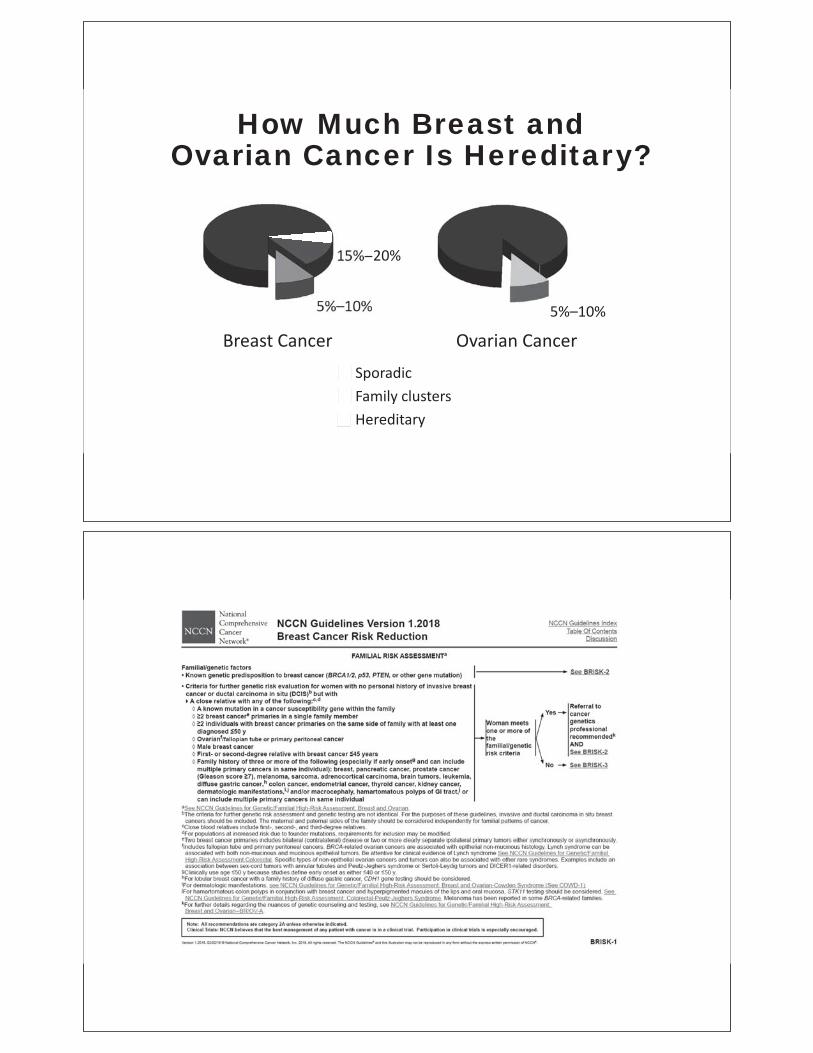
Ovarian CancerBreast Cancer
5%–10% 5%–10%
15% 20%
SporadicFamily clustersHereditary
How Much Breast and Ovarian Cancer Is Hereditary?

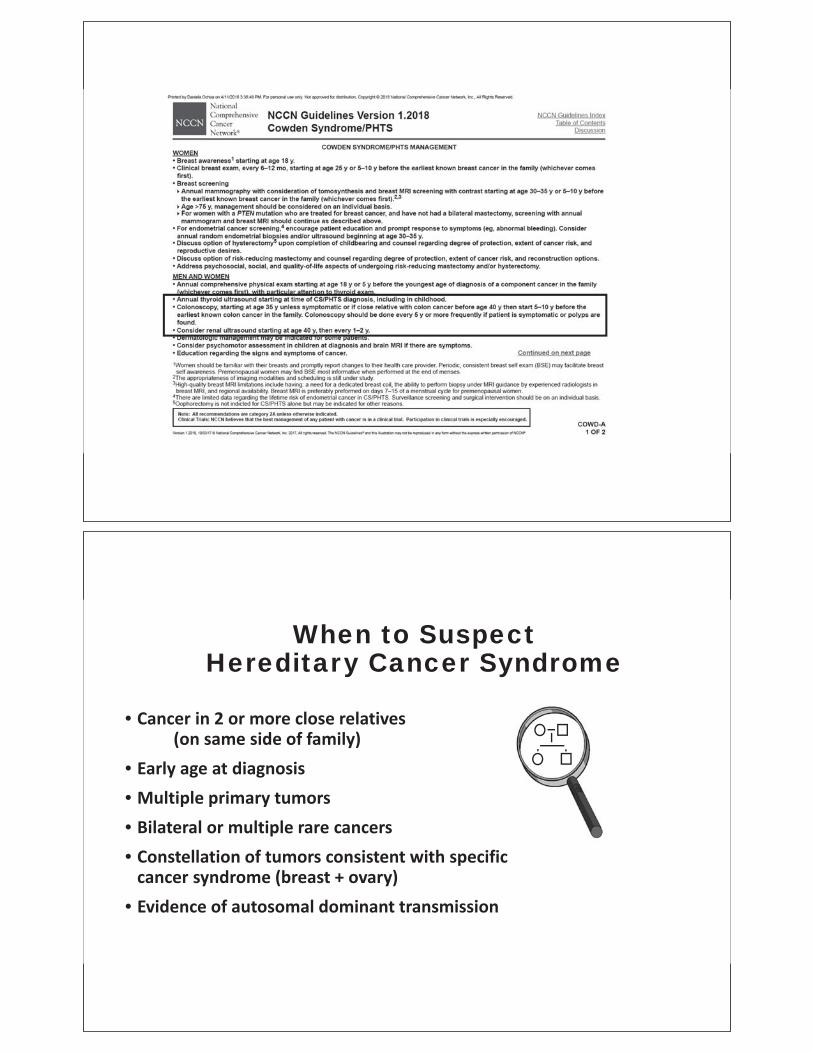
When to Suspect Hereditary Cancer Syndrome
• Cancer in 2 or more close relatives(on same side of family)
• Early age at diagnosis• Multiple primary tumors• Bilateral or multiple rare cancers• Constellation of tumors consistent with specific
cancer syndrome (breast + ovary)• Evidence of autosomal dominant transmission

BBreast Cancer Develops Before it’sDetected
How To Prepare• Same Day Biopsy
• Usually Able to Accommodate, but…• OSH Images• Stereotactic Needs• Anticoagulation
• Surgery Scheduling• Timeline, Not Day of Consultation Appt
• Breast Cancer Care• Neoadjuvant Systemic Treatment• BCT vs Mastectomy• LNs• Radiation• Endocrine• Reconstructive Options


3
Marijuana in the Field of Medicine: Rules, Roles and Rights of the PCP
Nate Smith, MD
Director and State Health Officer Arkansas Department of Health
Table of contents

ARKANSAS DEPARTMENT OF HEALTH
ARKANSAS DEPARTMENT OF HEALTH
Marijuana Rules, Roles, andPractice
Nathaniel Smith, MD, MPHDirector & State Health Officer
Arkansas Department of Health
ARKANSAS DEPARTMENT OF HEALTH
Objectives
• Review key provisions of Amendment 98, the Arkansas Medical Marijuana Act of 2016, as they pertain to Arkansas physicians
• Discuss the roles and responsibilities of Arkansas physicians regarding physician certification of qualifying conditions for patients desiring registration for use of medical marijuana
• Review some of the major risks and side effects of marijuana use
ARKANSAS DEPARTMENT OF HEALTH
Arkansas Medical Marijuana Act
• In November 2016 Arkansas voters approved medical marijuana through the passage of a constitutional amendment, known as Amendment 98, the Arkansas Medical Marijuana Act of 2016.
• The law allows qualifying patients to purchase and use medical marijuana from a licensed dispensary if certain criteria are met.
• One of the requirements is a physician certification of qualifying conditions.
ARKANSAS DEPARTMENT OF HEALTH
Case 1
A 25-year-old man presents to clinic requesting an Arkansas Department of Health (ADH) Medical Marijuana Physician Written Certification (physician certification) in order to obtain a Medical Marijuana Registration Card.
• He is a new patient to your practice.
• He does not appear to be physically disabled.
• He reports a history of chronic low back pain, which he says is much relieved by the use of recreational marijuana.

ARKANSAS DEPARTMENT OF HEALTH
Medical Marijuana Registration Card
• A valid registry identification card issued by the Arkansas Department of Health authorizes a qualifying patient to purchase and use medical marijuana from a licensed dispensary.
• There are a number of limitations on that use, especially in public settings.
• For example, smoking marijuana is prohibited:
– anywhere where tobacco smoking is not allowed,
– in the presence of children (under age 14), pregnant
women, or inside a motorized vehicle
ARKANSAS DEPARTMENT OF HEALTH
SAMPLE Registry ID card

ARKANSAS DEPARTMENT OF HEALTH
Physician Certification
• Physicians are not required to complete and sign the certification for a patient.
• If a physician chooses to complete and sign a physician certification form, he is certifying that:
– he has completed an in-person patient assessment,
– is licensed to practice medicine in Arkansas,
– has a current DEA number,
– the patient has one of the qualifying conditions
ARKANSAS DEPARTMENT OF HEALTH
Qualifying Conditions• Cancer
• Glaucoma
• HIV/AIDS
• Hepatitis C
• Amyotrophic lateral sclerosis
• Tourette’s syndrome
• Crohn’s disease
• Ulcerative colitis
• Post-traumatic stress disorder
• Severe arthritis
• Fibromyalgia
• Alzheimer’s disease
• Cachexia or wasting syndrome
• Peripheral neuropathy
• Intractable pain, which is pain
that has not responded to
ordinary medications,
treatment or surgical measures
for more than 6 months
• Severe nausea
• Seizures, including without
limitation those characteristic
of epilepsy
• Severe and persistent muscle
spasms, including without
limitation those characteristic
of multiple sclerosis

ARKANSAS DEPARTMENT OF HEALTH
ARKANSAS DEPARTMENT OF HEALTH
AR Medical Marijuana – April 2018
Patients/caregivers
• Applications: 5000
• Approved: 4800
• Denied: 0
• Pending: 200
Top 4 conditions
• Intractable pain: 2623
• Severe arthritis: 1378
• PTSD: 891
• Peripheral Neuropathy: 830

ARKANSAS DEPARTMENT OF HEALTH
Arkansas Department of Health
Medical Marijuana Physician Written Certification
I hold a valid, unrestricted, existing license to practice as a medical physician or osteopathic physician inArkansas.It is my professional opinion, after having completed an in person assessment of the patient’s medicalhistory and current medical condition in the course of a physician patient relationship, the patient has aqualifying medical condition identified below.
ARKANSAS DEPARTMENT OF HEALTH
ARKANSAS DEPARTMENT OF HEALTH
ARKANSAS DEPARTMENT OF HEALTH
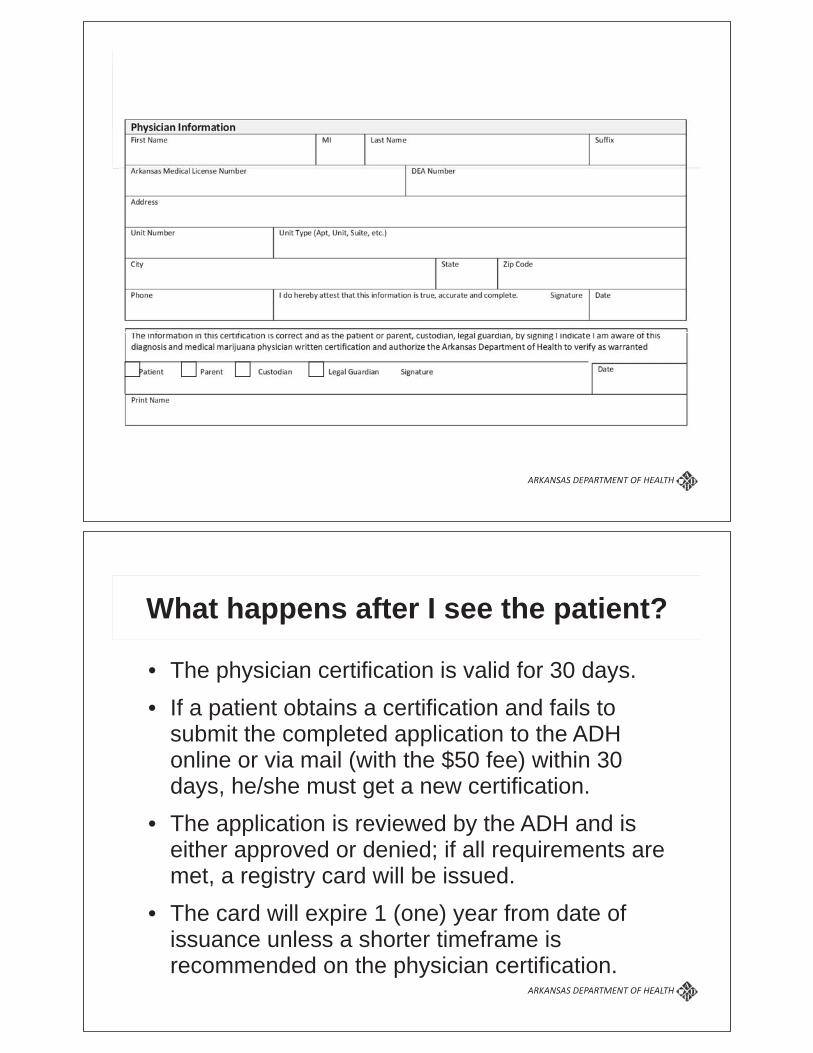
What happens after I see the patient?
• The physician certification is valid for 30 days.
• If a patient obtains a certification and fails to submit the completed application to the ADH online or via mail (with the $50 fee) within 30 days, he/she must get a new certification.
• The application is reviewed by the ADH and is either approved or denied; if all requirements are met, a registry card will be issued.
• The card will expire 1 (one) year from date of issuance unless a shorter timeframe is recommended on the physician certification.

ARKANSAS DEPARTMENT OF HEALTH
Medical Records
• The physician certification form may be copied and placed in the patient’s medical record as part of the physician’s documentation.
• The patient encounter should be documented, including discussion of treatment alternatives; potential benefits, adverse effects, drug interactions; and special cautions (e.g., use of marijuana during pregnancy or breast-feeding).
• All aspects of this process are covered by HIPAA, but documents may be subject to discovery in litigation and accessible to the DEA.
ARKANSAS DEPARTMENT OF HEALTH
Legal Status
• The DEA still classifies marijuana as a Schedule I drug with no accepted medical use and a high potential for abuse.
• Because medical marijuana cannot be prescribed, usage history will not be placed in the PMP database.
• Patients with a qualifying medical condition and valid registry card should not be considered in violation of their pain contracts if they test positive for marijuana without additional evidence of substance misuse (UAMS policy).

ARKANSAS DEPARTMENT OF HEALTH
Ethical Responsibilities
• Physicians remain responsible for following the standard of care and informing patients of known risks and benefits (if any) of medical marijuana based on accepted scientific research.
• Patients who plan to use medical marijuana should be informed of alternative treatment options for their condition and any potential interactions with other medications the patient may be taking.
ARKANSAS DEPARTMENT OF HEALTH
Additional Clarifications
• The physician certification is not a prescription for medical marijuana.
• Written certifications cannot be provided via telemedicine.
• Written certifications should not be provided by emergency department or urgent care physicians since they typically do not have ongoing physician-patient relationships (UAMS policy).

ARKANSAS DEPARTMENT OF HEALTH
Case 2
A 57-year-old woman with a history of type 2 DM and HTN presents for her regular follow up appointment and asks your advice regarding medical marijuana for her 3-year-old grandson, who has a history of seizure disorder.
• She would like to know whether you think medical marijuana might help his seizures.
• She asks whether children can get medical marijuana under Arkansas law.
• She asks whether you could certify his condition.
ARKANSAS DEPARTMENT OF HEALTH
Marijuana and Pediatric Epilepsy
• Marijuana contains >80 different cannabinoids in varying concentrations and proportions.
• GW Pharmaceuticals has an application pending before the FDA for approval of Epidiolex, a purified cannabidiol (CBD) extract, for treatment of pediatric epilepsy.
• Unlike -9-tetrahydrocannabinol (THC), the main psychoactive cannabinoid in marijuana, CBD does not produce euphoria or intoxication.
ARKANSAS DEPARTMENT OF HEALTH
Medical Marijuana for Children
• Patients under the age of 18 must have consent of a parent or guardian to receive a written certification.
• The parent/guardian must be present when the written certification is completed and must also sign the document.
• Minors are required to have a parent/guardian as a designated caregiver.
• No one under 21 years of age is permitted to smoke marijuana for medical use.
ARKANSAS DEPARTMENT OF HEALTH
Case 3
A 63-year-old man presents for follow up with multiple medical problems, including cirrhosis due to chronic hepatitis C and alcohol use, COPD, severe arthritis, and chronic depression. He is a Vietnam veteran and also suffers from PTSD. He has difficulty with ambulation due to his arthritis and severe peripheral neuropathy in his feet, and he uses an electric wheelchair to get around.
• He asks you to certify him for medical marijuana.
• He also asks you to certify his nephew as his designated caregiver for medical marijuana.

ARKANSAS DEPARTMENT OF HEALTH
Potential Benefits
What are this patient’s qualifying medical conditions?• Hepatitis C
• Severe arthritis
• Post-traumatic stress disorder (PTSD)
• Peripheral neuropathy
• Intractable pain?
QUALIFYING CONDITION INDICATION
ARKANSAS DEPARTMENT OF HEALTH
Potential Harms
• Hepatitis C: Cannabis use is not associated with acute hepatotoxicity, but daily cannabis use worsens the progression of chronic viral hepatitis C infection.
• PTSD: There is recent evidence suggesting poorer outcomes in PTSD patients who use marijuana (J Clin Psychiatry. 2015;76(9):1174).
• Depression: Cannabis use or cannabis use disorder is associated with subsequent development of depression or bipolar disorder.

ARKANSAS DEPARTMENT OF HEALTH
Potential Concerns
• COPD: Cannabis smoking produces acute, transitory respiratory symptoms, but chronic cannabis use is not associated with impaired pulmonary function.
• EtOH use: Among adults with a history of alcohol use disorder, cannabis use is associated with increased likelihood of persistent alcohol use disorder. The sedating effect of marijuana decreases mental alertness, increases the risk of motor vehicle accidents, and has additive effects when combined with alcohol.
ARKANSAS DEPARTMENT OF HEALTH
Designated Caregivers
• A designated caregiver is a person who may purchase and transport medical marijuana from an Arkansas dispensary for a qualified patient who is either a minor or is physically disabled.
• Minors are required to have a parent/ guardian as a designated caregiver. Physically disabled patients may have one if they so choose.
• Designations of age or physical disability must be marked on the physician certification form.

ARKANSAS DEPARTMENT OF HEALTH
Qualifications for Designated Caregivers
• at least twenty-one (21) years of age,
• has not been convicted of an excluded felony offense,
• has agreed to assist a physically disabled qualifying patient with the medical use of marijuana,
• has registered with the Arkansas Department of Health (the physician does not certify caregivers)
ARKANSAS DEPARTMENT OF HEALTH
Case 4
A 44-year-old man recently moved to Arkansas from California and has a Medical Marijuana Identification Card from that state.
• He requests medical evaluation and physician certification to purchase medical marijuana in Arkansas.
• His main symptom at this time is episodes of nausea that occur almost every day but get better when he takes a hot shower.

ARKANSAS DEPARTMENT OF HEALTH
Visiting Patient
• A “visiting patient” is a patient with a qualifying medical condition who is not a resident of Arkansas or who has been a resident of Arkansas for less than 30 days and who is in actual possession of a registry identification card or its equivalent that is issued under the laws of another state.
• Dispensaries will require visiting patients to certify that they have been diagnosed by a physician to have one or more qualifying medical conditions.
ARKANSAS DEPARTMENT OF HEALTH
Cannabinoid Hyperemesis Syndrome
• At low doses, THC is a potent antiemetic.
• At high dose, there is a paradoxical effect.
• Colorado observed a 1.92-fold increase in prevalence of cyclic vomiting in local EDsafter legalization of marijuana. Acad Emerg Med. June 2015.

ARKANSAS DEPARTMENT OF HEALTH
Potential Risks to Discuss
• The variability of quality and concentration of marijuana;
• The risk of cannabis use disorder;
• Possible exacerbation of psychotic disorders;
• Adverse cognitive effects for children and young adults;
• The risk of falls and motor vehicle accidents;
• Use of marijuana during pregnancy or breastfeeding;
• The need to safeguard all marijuana and marijuana-infused products from children and pets or domestic animals
ARKANSAS DEPARTMENT OF HEALTH
Case 5
A 52-year-old woman with well-controlled hyperlipidemia mentions to you during a routine follow-up visit that she and her husband are in the process of opening a medical marijuana dispensary in the area.
• She asks if they could refer patients to you for physician certification and suggests you might consider giving their patients a little discount.
• She knows you are very busy but asks if you would consider sending your APRN to their dispensary once a week to do certifications.

ARKANSAS DEPARTMENT OF HEALTH
Certification Restrictions
• A written certification can be completed only by a physician with a valid, unrestricted Arkansas medical license and a current DEA registration.
• APRNs and PAs cannot complete a written certification.
• Unlicensed medical residents or licensed residents who do not have their own DEA registration cannot complete a written certification.
ARKANSAS DEPARTMENT OF HEALTH
Conflicts of Interest
• The Medical Marijuana Amendment prohibits physicians from paying or receiving payment from a dispensary or cultivation facility.
• Certifying physicians are prohibited from affiliating financially with a dispensary and/or giving or receiving discounts related to a dispensary if they are assessing patients.
• A physician may not perform assessments for certification on the premises of a dispensary.

ARKANSAS DEPARTMENT OF HEALTH
Case 6
A 33-year-old woman with stable ulcerative colitis presents for her annual wellness exam.
• She mentions that her GI specialist recently certified her for medical marijuana.
• Since her marijuana was certified by her physician, she assumes it will be okay to smoke it on her work breaks.
• She works as a receptionist for your group practice.
ARKANSAS DEPARTMENT OF HEALTH
Employee Legal Protections• For the purposes of medical care a qualifying
patient's authorized use of marijuana is considered the equivalent of the authorized use of any other medication and does not constitute the use of an illicit substance.
• An employer shall not discriminate against an applicant or employee in hiring, termination, or any term or condition of employment, or otherwise penalize an applicant or employee, based upon the applicant's or employee's past or present status as a qualifying patient or designated caregiver.
ARKANSAS DEPARTMENT OF HEALTH
Employer Legal Protections
• May establish and implement a substance abuse or drug-free workplace policy that may include a drug testing program that complies with state or federal law;
• Take action with respect to an applicant or employee under that policy based on the good faith belief that a qualifying patient:
– Possessed or engaged in the use of marijuana while on the
premises of the employer or during the hours of employment; or
– Was under the influence of marijuana while on the premises of
the employer or during the hours of employment, provided that a
positive test result for marijuana cannot provide the sole basis
for the employer's good faith belief
•
ARKANSAS DEPARTMENT OF HEALTH
Permitted Employer Actions
• Implementing, monitoring, or taking measures to assess, supervise, or control the job performance of an employee
• Reassigning an employee to a different position or job duties
• Placing an employee on paid or unpaid leave
• Suspending or terminating an employee
• Requiring an employee to successfully complete a substance abuse program before returning to work
• Refusing to hire an applicant

ARKANSAS DEPARTMENT OF HEALTH
Safety Sensitive Positions
• A “safety sensitive position” is any position (designated as such in writing by an employer) in which a person performing the position while under the influence of marijuana may constitute a threat to health or safety.
• A qualifying patient may be excluded from being employed in or performing a safety sensitive position based on the employer's good faith belief that the qualifying patient was engaged in the current use of marijuana.
ARKANSAS DEPARTMENT OF HEALTH
Criteria for Safety Sensitive Positions
• Carrying a firearm;
• Performing life-threatening procedures;
• Working with confidential information or documents pertaining to criminal investigations;
• Working with hazardous or flammable materials, controlled substances, food, or medicine;
• A lapse of attention could result in injury, illness, or death (e.g., operating, repairing, maintaining, or monitoring heavy equipment, machinery, aircraft, motorized watercraft, or motor vehicles)

Guidance for the Medical Marijuana Physician Certification Form
In November 2016 Arkansas voters approved medical marijuana through the passage of a constitutional amendment, known as Amendment 98, the Arkansas Medical Marijuana Act of 2016. The law allows qualifying patients to purchase and use medical marijuana from a licensed dispensary if certain criteria are met. One of the requirements is a physician certification of qualifying conditions. Am I required to complete a physician certification for a patient?
• No. Physicians are not required to complete and sign the certification for a patient. Am I mandated to sign this form?
• Yes. If a physician is willing to complete a physician certification form for a patient to use medical marijuana obtained from a licensed dispensary, a physician must sign the form.
What am I actually certifying on this form? • You are certifying that you have completed an in-person patient assessment. • That the patient DOES have one of the qualifying conditions. • That you are licensed to practice in Arkansas. • That you have a current DEA number.
Is there an approved form?
• Yes. There is an approved form from the Arkansas Department of Health ( ADH) • This form cannot be substituted with a letter or other type of certification • This form is available to print from the ADH website. You can make blank copies of the form.
Do I need any special training or certification to sign the form?
• Any medical doctor or doctor of osteopathy licensed to practice in Arkansas with a current DEA number is authorized to sign the form.
• There is no specific medical marijuana training required by law in order to complete the form. Completing the form:
• All portions of the form must be filled out completely. • Do not leave the form blank anywhere in the content areas. • Complete the patient demographic portion at the top of the form. Patient must be an Arkansas resident. • Identify if the patient is disabled or under the age of 18.
o This is necessary for determining their need for a certified caregiver who will be authorized by law to purchase and transport medical marijuana for the patient.
• Check the correct time frame box for the patient. It may be up to 12 months, or less depending on your determination for the patient.
• Fully fill out all physician information. Do not leave any portion blank. • The patient or patient’s guardian must also sign the form.
What are the qualifying conditions?
• The form has a complete list of the qualifying conditions. • No other conditions are approved at this time.(New conditions are added by rule change of the Arkansas Board of Health) • Mark the applicable condition(s) for the patient. • ADH will not accept applications that have additional write-in conditions.

Will these forms be verified?
• Yes, the agency may contact the physician to verify the signature. • Physician’s license & DEA number will be verified.
Do I keep a medical record of the visit? • Yes. You should keep a record of the visit. • The physician certification form may be copied and placed in the patient’s medical record as part of your documentation. • All aspects of this process are covered by HIPAA.
Am I allowed to complete a certification for a minor?
• Yes. You may complete a certification for a minor who has a qualifying condition. • The parent/guardian must be present and they must sign the form. • Remember to certify that the patient is under 18 on the form.
What is a designated caregiver?
• A designated caregiver is a person who may purchase and transport medical marijuana from an Arkansas dispensary, for a qualified patient who is either a minor or is physically disabled.
• Minors are required to have a parent/ guardian as a designated caregiver. Physically disabled patients may have one if they so choose.
• Designations of age or physical disability must be marked on the certification form. • Physicians do not have to see a caregiver unless the patient is a minor, and then they must review the form with the minor
patient’s parent/guardian. How does ADH get this certification?
• The applicant will send the certification to ADH as part of their application. They may do this via mail, or through ADH’s online application system.
When does this physician certification expire?
• The physician certification is valid for 30 days. • If a patient gets a certification and fails to submit it to ADH within 30 days, they must get a new certification. • A patient’s registration identification card is valid for one year from issuance. • If you as the physician wish for the patient’s registration identification card to be valid for less than one year, please note
that on the form in the area marked “issue registry card for”.
• What happens after I see the patient? • The patient must submit their completed application online or via mail. • The application is reviewed and it is either approved or denied. • If all requirements are met, a registry cared will be issued. • The card will expire based on the date recommended on the physician certification.
If you have further questions, you may call 501-682-4982, or email your questions to [email protected]. NOTE: Applications are being accepted; however registry ID cards will not be issued until one month prior to medical marijuana availability in Arkansas dispensaries.
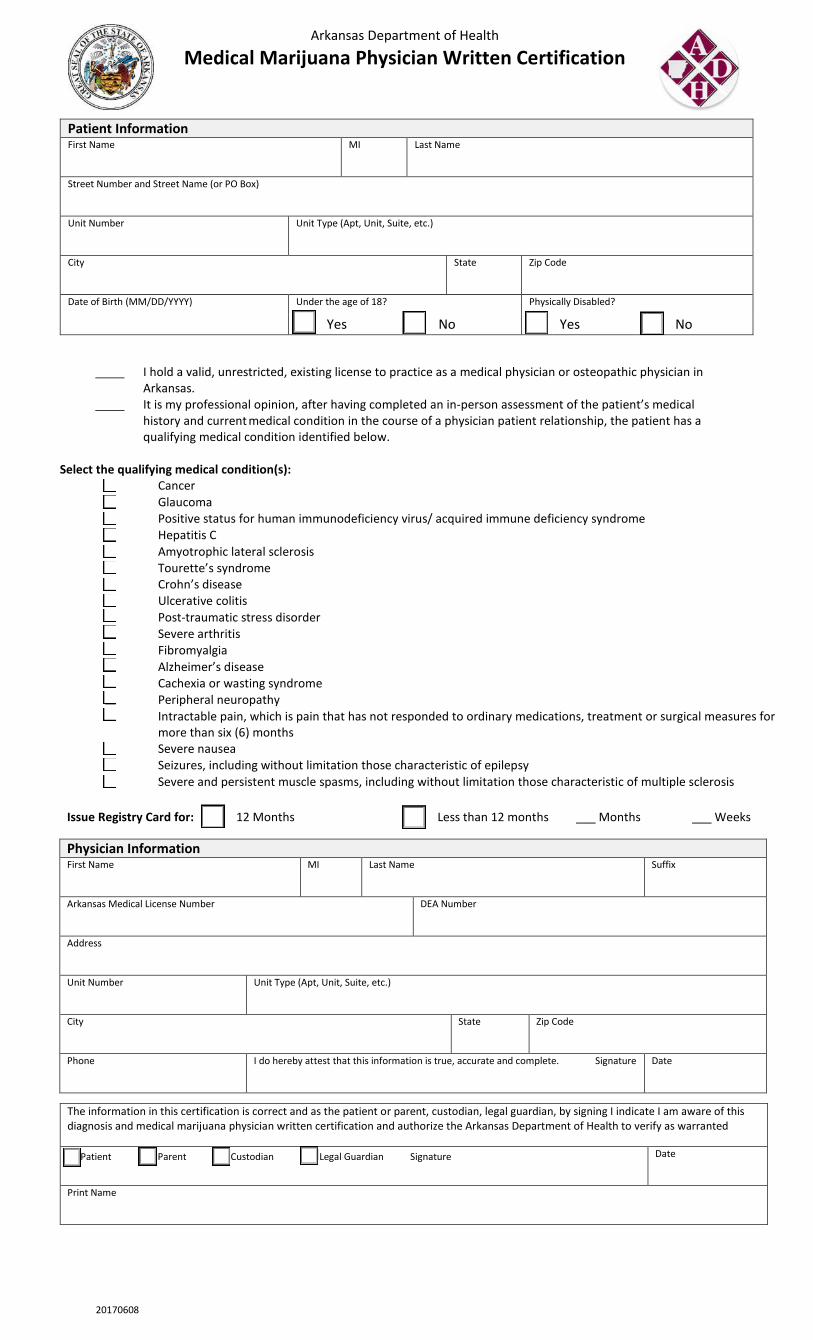
Arkansas Department of Health
Medical Marijuana Physician Written Certification
Patient Information First Name MI Last Name
Street Number and Street Name (or PO Box)
Unit Number Unit Type (Apt, Unit, Suite, etc.)
City State Zip Code
Date of Birth (MM/DD/YYYY) Under the age of 18? Physically Disabled?
Yes No Yes No
I hold a valid, unrestricted, existing license to practice as a medical physician or osteopathic physician in Arkansas.
It is my professional opinion, after having completed an in-person assessment of the patient’s medical history and current medical condition in the course of a physician patient relationship, the patient has a qualifying medical condition identified below.
Select the qualifying medical condition(s):
Cancer Glaucoma Positive status for human immunodeficiency virus/ acquired immune deficiency syndrome Hepatitis C Amyotrophic lateral sclerosis Tourette’s syndrome Crohn’s disease Ulcerative colitis Post-traumatic stress disorder Severe arthritis Fibromyalgia Alzheimer’s disease Cachexia or wasting syndrome Peripheral neuropathy Intractable pain, which is pain that has not responded to ordinary medications, treatment or surgical measures for
more than six (6) months Severe nausea Seizures, including without limitation those characteristic of epilepsy
Severe and persistent muscle spasms, including without limitation those characteristic of multiple sclerosis
Issue Registry Card for: 12 Months Less than 12 months ___ Months ___ Weeks Physician Information First Name MI Last Name Suffix
Arkansas Medical License Number DEA Number
Address
Unit Number Unit Type (Apt, Unit, Suite, etc.)
City State Zip Code
Phone I do hereby attest that this information is true, accurate and complete. Signature Date
The information in this certification is correct and as the patient or parent, custodian, legal guardian, by signing I indicate I am aware of this diagnosis and medical marijuana physician written certification and authorize the Arkansas Department of Health to verify as warranted
Patient Parent Custodian Legal Guardian Signature Date
Print Name
20170608

Copyright 2016 American Medical Association. All rights reserved.
Medical Board Expectations for PhysiciansRecommending Marijuana
Heightened public interest in marijuana and marijuana-infused products for medicinal and recreational pur-poses led the nation’s state medical and osteopathicboards recently to issue recommendations about mari-juana in patient care and a cautionary note advising ac-tively licensed physicians to abstain from using mari-juana while practicing medicine.1 This is the first time thatthe dispensing or use of products derived from theCannabis sativa plant have been highlighted in a policyrecommendation of the Federation of State MedicalBoards (FSMB), whose members include 70 state andterritorial medical licensing boards of the United States.We examine the dilemma of physicians caught be-tween increasingly permissive local statutes and pro-hibitive federal regulations and summarize 10 recom-mendations about marijuana for patient care from theagencies authorized by statute to protect the health andwelfare of the public through the licensure and disci-pline of physicians and other health care professionals.
Permissive State Laws, Restrictive Federal LawDuring the past 2 decades, attitudes and laws have be-come more tolerant toward marijuana, with the preva-lence of adults reportedly using the substance increas-ing from 4.1% in 2001 to 9.5% in 2013.2 Although thereis little evidence for the efficacy of marijuana in treatingcertain medical conditions, marijuana has been vari-ously suggested for alleviating some or all symptoms ofa range of debilitating medical conditions, including butnot limited to certain types of cancer, multiple sclero-sis, Alzheimer disease, posttraumatic stress disorder(PTSD), epilepsy, Crohn disease, and glaucoma.3
The “prescribing” of marijuana, however, remainsillegal under federal law, where it is classified as a Sched-ule I substance under the Controlled Substances Act of1970, meaning that the federal government considersmarijuana a substance with a high potential for depen-dency or addiction, with no accepted medical use intreatment. Therefore, under federal law, marijuana can-not be knowingly or intentionally distributed, dis-pensed, or possessed, and an individual who aids andabets another in violating federal law or engages in a con-spiracy to purchase, cultivate, or possess marijuana maybe punished to the same extent as the individual whocommits the crime.
With the increasing number of jurisdictions permit-ting the use of marijuana in patient care, the US Depart-ment of Justice updated its marijuana enforcementpolicy in 2013. It reiterated marijuana’s classification asan illegal substance under federal law but advised statesand local governments that authorize marijuana-related conduct to implement strong and effective regu-latory and enforcement systems to address any threat
those laws could pose to public safety, public health, andother interests. Should these state efforts be insuffi-cient, the policy warns, the federal government re-serves the right to challenge the regulatory structure andenforce actions against individuals, such as physicians,who may be violating federal law.
In 2015, FSMB Chair J. Daniel Gifford, MD, ap-pointed a work group to develop policy recommenda-tions for state medical boards regarding marijuana in pa-tient care. The work group was also tasked with thedevelopment of a position statement regarding the regu-lation of licensees who use marijuana, a charge that wasultimately transferred to the FSMB’s board of direc-tors, which includes representatives from more than adozen states and territories. Both the recommenda-tions for marijuana in patient care and the board’s state-ment about physician use of marijuana involved a sys-tematic review of more than 40 peer-reviewed articlesfrom the medical literature. Commentary and feed-back about draft language was received from state medi-cal board members and staff, including physicians andpublic members, as well as interested stakeholders suchas the American Society of Addiction Medicine, and in-cluded open testimony at a reference committee atFSMB’s annual meeting before unanimously adopted bystate medical boards on April 30, 2016. The 10 expec-tations of physicians relating to marijuana in patient careare summarized below.
Patient-Physician Relationship. Because thepatient-physician relationship is fundamental to the pro-vision of acceptable medical care, physicians mustdocument details of the patient encounter to reflectthat such a relationship was established and in place be-fore providing a recommendation, attestation, or au-thorization of marijuana for the patient. Consistent withprevailing standards of care, physicians should not rec-ommend, attest, or otherwise authorize marijuana forthemselves or a family member.
Patient Evaluation. A documented, in-person medi-cal evaluation and collection of relevant clinical historycommensurate with the presentation of the patient mustbe obtained before a decision is made to recommendmarijuana for medical use. At a minimum, the evalua-tion should include the patient’s history of present ill-ness, social history, past medical and surgical history, al-cohol and substance use history, family history (withemphasis on addiction or mental illness and psychoticdisorders), physical examination, documentation oftherapies with inadequate response, and a diagnosis re-quiring the marijuana recommendation.
Informed and Shared Decision Making. The physi-cian should discuss the risks and benefits of marijuanause with the patient, and patients should be advised of
VIEWPOINT
Humayun J. Chaudhry,DO, MSFederation of StateMedical Boards,Euless, Texas.
Arthur S. Hengerer,MDDepartment ofOtolaryngology–Headand Neck Surgery,University ofRochester, Rochester,New York.
Gregory B. Snyder, MDFederation of StateMedical Boards,Euless, Texas.
CorrespondingAuthor: Humayun J.Chaudhry, DO, MS,Federation ofState Medical Boards,400 Fuller Wiser Rd,Ste 300, Euless, TX76039 ([email protected]).
Opinion
jama.com (Reprinted) JAMA August 9, 2016 Volume 316, Number 6 577
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/ by a Public Health Information Access User on 11/10/2016

Copyright 2016 American Medical Association. All rights reserved.
the variability and lack of standardization of marijuana prepara-tions and the effect of marijuana. Patients should be reminded notto drive or operate heavy machinery while under the influence ofmarijuana. If the patient is a minor or without decision-making ca-pacity, the physician should ensure that the patient’s parent, guard-ian, or surrogate is involved in the treatment plan and consents tothe patient’s use of marijuana.
Treatment Agreement. The health care professional shoulddocument a written treatment plan that includes a review of othermeasures attempted to ease a patient’s symptoms that do not in-volve the recommendation of marijuana (Box), and a specific dura-tion for the authorization to obtain marijuana for a period no longerthan 12 months.
Qualifying Conditions. Recommending marijuana for certainmedical conditions is at the professional discretion of the physi-cian. The indication, appropriateness, and safety of the recommen-dation should be evaluated in accordance with current standards ofpractice and in compliance with state laws, rules, and regulations,which may specify conditions for which a patient may qualify.
Ongoing Monitoring. The physician should regularly assess thepatient’s response to the use of marijuana and overall health and levelof function. This assessment should include the efficacy of the treat-ment to the patient, the goals of the treatment, and the progress
of those goals. Where available, the physician recommending mari-juana should check the state’s prescription drug monitoring pro-gram, register with the appropriate oversight agency (such as a mari-juana registry, as exists in Colorado and Minnesota), and provide theregistry with information each time a recommendation, attesta-tion, authorization, or reauthorization is issued.
Consultation and Referral. A patient who has a known or sus-pected history of substance use disorder or a co-occurring mentalhealth disorder may require specialized assessment and treat-ment. The physician should seek a consultation with, or refer the pa-tient to, a pain management, psychiatric, addiction, or mental healthspecialist, as needed.
Medical Records. The physician should keep accurate and com-plete medical records. Information that should appear in the rec-ord includes the patient’s history; results of the physical examina-tion; patient evaluation; other treatments and prescribedmedications; authorization, attestation, or recommendation for mari-juana (including the date, expiration, and any additional informa-tion required by state statute); instructions to the patient (includ-ing discussions of the risk and benefits, adverse effects, and variableeffects); results of ongoing assessment and monitoring; and a copyof a signed treatment agreement (including instructions on safe-keeping and instructions on not sharing marijuana with others).
Physician Conflicts of Interest. A physician who recommendsmarijuana should not have a professional office located at a dispen-sary or cultivation center or receive financial compensation from,or hold a financial interest in, a dispensary or cultivation center. Thephysician should not be associated in any way with a dispensary orcultivation center.
Physician Use of Marijuana. State medical and osteopathicboards advise their licensees to abstain from the use of marijuanafor medical or recreational purposes while actively engaged in thepractice of medicine. Practicing medicine under the influence of mari-juana may constitute unprofessional conduct or incompetence.
ConclusionThe primary mission of state medical boards in the United States isto protect the public and ensure that only individuals who are quali-fied and fit to practice medicine do so.4 Although it is up to everystate medical board to incorporate all, some, or none of the lan-guage in these marijuana recommendations, unanimous adoptionof the recommendations by state board representatives at theFSMB’s annual meeting suggests they may influence local delibera-tions relating to the determination of professional conduct. Even ifthese recommendations are not adopted as a state statute, rule, orpolicy, they represent a reasonable effort to offer best practices forclinicians to follow when considering marijuana in patient care.
ARTICLE INFORMATION
Published Online: June 16, 2016.doi:10.1001/jama.2016.7741.
Conflict of Interest Disclosures: Dr Chaudhryreports being the president and chief executiveofficer of the Federation of State Medical Boards(FSMB). Dr Hengerer reports being the chair of theFSMB and chair of the New York Office ofProfessional Medical Conduct. Dr Snyder reportsbeing the chair-elect of the FSMB.
REFERENCES
1. Model Guidelines for the Recommendation ofMarijuana in Patient Care. FSMB House ofDelegates approves new policy guidelines for statemedical regulators. https://www.fsmb.org/Media/Default/PDF/FSMB/Advocacy/NR_New_FSMB_Position_Statements_May2016.pdf. Accessed May17, 2016.
2. Hasin DS, Saha TD, Kerridge BT, et al. Prevalenceof marijuana use disorders in the United States
between 2001-2002 and 2012-2013. JAMAPsychiatry. 2015;72(12):1235-1242.
3. Hill KP. Medical marijuana for treatment ofchronic pain and other medical and psychiatricproblems. JAMA. 2015;313(24):2474-2483.
4. Chaudhry HJ, Gifford JD, Hengerer AS. Ensuringcompetency and professionalism through statemedical licensing. JAMA. 2015;313(18):1791-1792.
Box. Recommended Review of Attempted Measures WithoutMarijuana Use to Ease the Symptoms Caused by a DebilitatingMedical Condition
1. Advice about other options for managing the condition.
2. Determination that the patient may benefit fromthe recommendation of marijuana.
3. Advice about the potential risks of the medical use of marijuanato include
• The variability of quality and concentration of marijuana;• The risk of cannabis use disorder;• Adverse events, exacerbation of psychotic disorder, adverse
cognitive effects for children and young adults, and other risks,including falls or fractures;
• Use of marijuana during pregnancy or breastfeeding;• The need to safeguard all marijuana and marijuana-infused
products from children and pets or domestic animals; and• The need to notify the patient that the marijuana is for
the patient’s use only and the marijuana should not be donatedor otherwise supplied to another individual.
4. Additional diagnostic evaluations or other planned treatments.
5. A specific duration for the marijuana authorization for a periodno longer than 12 months.
6. A specific ongoing treatment plan as medically appropriate.
Opinion Viewpoint
578 JAMA August 9, 2016 Volume 316, Number 6 (Reprinted) jama.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://jamanetwork.com/ by a Public Health Information Access User on 11/10/2016

4
Chronic Migraine: How Did We Get Here and Where Do We Go From Here?
Dale Carter, MD
Assistant Professor Department of Neurology
UAMS
Table of Contents

Chronic Migraine
How Did We Get HereAnd Where Do We Go From Here?
Updated Facts About Migraine in the US
• Data compiled from 3 major sources:• National Health Interview Survey• National Hospital Ambulatory Medical Care Survey• National Ambulatory Medical Care Survey
Encompassed multiple years of dataCaptured data from govt employed staff (not VA),
hospital clinics, ERs, independent clinics, group homes• and dormitories
Results – Gender and Age Prevalences
• Gender Differences:• Overall prevalence was 15.3%• Prevalence in females was 20.7% vs males 9.7%
• Age Differences:• Prevalence in 18-44 year olds 17.9%• Prevalence in 45-64 year olds 15.9%• Prevalence in 65-74 year olds 7.3%• Prevalence in 75 years and older 5.1%
•

Migraine and Insurance, Income, Jobs
• Income: less than 33,000/yr – 19.9% prevalence• less than 11,670/yr (poverty rate) – 21.7% prevalence
Insurance: Medicaid – 26% prevalence/yr• Medicare and Medicaid/over 65yrs old – 16.4% prevalence• Private Insurance – 15.1% prevalence• Unemployed/used to work – 21.4% prevalence• Unemployed/never worked – 16.6% prevalence• Part time worker – 15.6% prevalence• Full time worker – 13.7% prevalence
What About Chronic Migraine?• Definition by ICHD3 beta: occurrence of 15 or more headaches• per month for more than 3 months with 8 having features of• migraine headache
• Prevalence in the US: 1.3-2% • 2.5% of migraine sufferers progress to chronic migraine each year
• This is a fluid condition that may also improve with appropriate treatment, avoidance of triggers, stress management, proper diet

Risk Factors for Chronic Migraine
• Increasing frequency/severity of migraines• Analgesic overuse• Inadequate treatment of headache attacks• Depression• Stressful life events• Snoring• Obesity
Increased frequency of headaches
• Patients with 6-9 headache days/mo have increased risk of CM• Patients with 10-14 days/mo have even higher risk (considered• high frequency migraines)
• The presence of allodynia (increased skin sensitivity• to pain in headache areas and beyond) i.e. “it hurts to touch• my head or brush my hair” is an independent predictor of chronic • migraine

Inadequate Treatment of Migraines
• Many patients still have not tried triptans or wait too long to treat
Many patients that would meet the criteria for frequent migraineor chronic migraine have not tried a preventative medication
Many patients don’t understand the concept of analgesic overuseheadache (the use of any and all analgesics more than 2 days/wk)
Analgesic Medication Overuse
• Occurs when patients take any kind of analgesic (nsaids, aspirin,Tylenol, triptans, opiates, barbiturates, otc’s like Excedrin,BC Powders and related compounds 10-15 days/month dependingon the particular medication
• Headaches frequently improve when analgesic overuse stops

Depression/Stressful Life Events
• Mood disorders often are seen as comorbid disorders with• chronic migraine• Common conditions include depression and anxiety• Patel et al (2004) noted overall prevalence for major depression was
23.9% in migraineurs vs 10.3% for a control group• Scher et al found that recent stressful life events history is an• independent risk factor for chronic daily headache
Snoring
• Snoring was found to be an independent risk factor for chronic migraine by Scher et al in a group of chronic daily headache patients
• Whether due to sleep apnea or other sleep related disorders restless sleep with frequent awakening will increase the likelihood of migraine attacks

Obesity
• Obesity is a pro-inflammatory and pro-thrombotic state• It has been found to be an independent risk factor for chronic• migraine• In a study by Burg, Bigal and Lipton 30,215 people were inter-• viewed by phone to explore the relationship of obesity and• migraine• BMI was directly proportional to the number of migraines
experienced per month
Obesity, Continued
• In migraineurs of nl weight, 4.4% had 10-15d/month of migraine• “ “ who were overweight, 5.8% “ “ “
“ “ who were obese, 13.6% “ “ ”• “ who were morbidly obese, 20.7% “ “ “
• In a different study by Sher et al, in patients with a BMI>30, there• was a 5X greater risk of developing chronic daily headache• In overweight patients (BMI of 25-29), the risk was 3X greater

Adipocytes and Inflammation
• Adipocytes release Interleukin-6 and Tumor Necrosis Factor-alpha• In obese patients, indicators of inflammation are seen in blood• testing, including elevations in Interleukin-6, Tumor Necrosis• Factor-alpha, leukocytosis, elevated CGRP (especially in obese• females) and elevated CRP
How Her Headaches Became Chronic

Pathophysiology of Chronic Migraine
• A threshold disorder of neurons • When the threshold drops, there is increased susceptibility to• physiologic and environmental stimuli that can trigger a • migraine attack• Once trigeminal neurons are stimulated, CGRP and other pain-• inducing chemicals are released in the blood vessels of the • meninges, dura and extracranial vessels• These chemicals cause inflammation and vasodilation of the• aforementioned blood vesses, which results in the throbbing headache
Causes of Neural Activation
1. cortical spreading depression
2. dysfunction of the descending inhibitorypathways – periaqueductal gray, locus ceruleus, raphe
nucleus

Long-term changes in Chronic Migraine
Central Sensitization of the trigeminovascular system• First order sensitization – peripheral trigeminal nerve activation
causes• vasodilation and the pounding head pain• Second order “ - the neurons in the trigeminal nucleus caudalis• become activated causing more diffuse pain (i.e. “my hair hurts • when I brush it”)• Third order “ - the thalamic neurons are activated, causing • distant body areas to hurt (i.e. extremities, half of body, etc.)
Long-term Changes, Continued
1. Central Sensitization is a risk factor for chronic migraine
2. Structural changes over time• 1. iron deposition in the red nucleus, substantia nigra and PAG• 2. white matter infarct-like lesions, mainly in migraineurs with • aura in mid-life/cerebellar lesions in women only
3. Changes in Brain Metabolism• 1. Hyperexcitability• 2. Change in glutamate transmission

Changes in Brain Metabolism Continued
• Hyperexcitability –Aurora et al used transcranial magnetic • stimulation on migraineurs (CM, EM and controls) to• suppress perceptual accuracy• CM patients showed the least brain suppression by the magnetic• stimulation, with EM patients and controls more affected• This suggests hyperexcitability in the brain that is not suppressed• by magnetic stimulation
Long-term Changes, Continued
• Dr. Aurora did PET scanning of a subset of 10 of the above• chronic migraineurs and noted:• 1. increased metabolism in the pons and right temporal cortex• 2. decreased metabolism in medial frontal, parietal and
somato-• sensory cortices and bilateral caudate nuclei

Long-term Changes in Glutamate Levels
• Alterations in Glutamate Transmission
• Prescott et al used magnetic resonance spectroscopy to compare• interictal brain chemistry in 10 migraineurs and 8 controls
• Results revealed an increase in the N-acetyl-aspartyl-glutamate to• glutamine ratio in the insula and cingulate cortex of migraineurs
Where Do We Go From Here? - Treatment
Medications:for acute rescue – avoid opiates, barbituratesfor prevention – to reduce neuronal excitability and therebyreduce migraine frequency and severity
Non Medicinal options

Non-Medicinal Treatment Options
• Address analgesic rebound• Limit caffeine (i.e. no more than 16oz/d)• Hydrate well• Avoid processed foods/tyramine containing foods/better nutrition• Start a calendar to look for triggers (i.e. menses, lack of sleep,• stressful events, the wrong type of food, etc.)• Regulated and adequate sleep time• Predictable eating times
Non-medicinal Options, Continued
• Stress Management/Biofeedback and Relaxation Therapy• Cognitive Behavioral Therapy• Yoga (especially Hatha Yoga)/Tai Chi• Physical therapy to help with poor posture/poor work-related• ergonomics• Accupuncture

Medications - Preventatives
• In 2012 the American Headache Society and American Association • of Neurology established guidelines for prevention of episodic• migraine• This included 3 tiers of medications:• Level A – established as effective• Level B – probably effective• Level C- possibly effective
Level A Medications – should be offered
• Divalproex (Depakote) 400-1000mg/d (avoid in young women• due to risk of neural tube defects in pregnancy/weight issues• Topiramate (Topamax) 25-200mg/d (reconside if patient has had• kidney stones or won’t hydrate adequately• Metoprolol (Lopressor) – 47.5-200mg/d (not in asthmatics, athletes• or diabetics not well-controlled• Timolol 10-15mg bid “• Propranolol 120-140mg/d “• Petasites (butterbur) 50-75mg bid (avoid if ragweed allergies)

Level B – consider for prophylaxis
• Amitriptyline (Elavil, etc.) – 25-150mg/d (avoid in obese patients)• Atenolol 100mg/d (another beta blocker)• Magnesium (tri magnesium dictirate) – 600mg/d (reduce dose if
diarrhea/cramping)• Feverfew – 50-300mg bid (don’t combine with asa or nsaids)• Naproxen – 500-1100mg/d (try only for short periods to avoid ulcers,
increased cardiac risk)• Naproxen sodium – 550 bid “• Venlafaxine 150mg extended release/day
Level B Continued
• Fenoprofen 200-600mg tid (limit use for above reasons)• Ketoprofen 50mg tid “• Riboflavin 400mg/d • Histamine 1-10mg subcutaneously twice a week

Level C consider for prophylaxis
• Candesartan 16mg/d• Carbamazepine 600mg/d (frequent side effects)• Clonidine 0.75-0.15mg/d; patch formulations also studied (sedating)• Guanfacine 0.5-1mg/d• Lisinopril 10-20mg/d• Nebivolol 5mg/d• Pindolol 10mg/d
Level C Continued
• Flurbiprofen 200mg/d (cardiac risk)• Mefenamic acid 500mg tid “• Coenzyme Q10 100mg tid• Cyproheptadine 4mg/d (weight gain!)

Acute Treatment of Severe Migraine
Triptans (avoid in cardiac patients, hemiplegic migraine, stroke patients)
Medrol dosepack for a refractory migraineKetorolac IV/IM injections (avoid in patients with ulcers, on
daily steroids, or with nsaid allergies/sensitivities)DHE (dihydroergotamine) in IV/IM formulationDepacon IVInapsine or Lidocaine infusion with cardiac monitoringIV steroids
What Else?
• Botulinum toxin – FDA approved for chronic migraine• External brain stimulation – i.e. Cefaly, vagal nerve
stimulator,• magnetic brain stimulator for migraine with aura• Greater occipital nerve blocks (
Headache,2010;50(6):1041-1044)

“Coming To A Theater Near You”…..
• CGRP Antibody Blockers • Expensive! • Most available only as IM or IV infusion form (one is oral)• Excellent for patients with cardiac risk factors• Excellent for chronic migraine and some are also indicated
for• treatment of chronic cluster headache
In Summary……
• Migraine is a neurovascular disorder with an altered threshold• There are specific risk factors associated with the evolution of• chronic migraine, some of which can be modified:• obesity, depression/stressful life events, analgesic overuse,• inadequate acute treatment, snoring• Chronic Migraine should be treated with a preventative and an• appropriate rescue medication• Non-medicinal modalities also help to reduce headache frequency

5
Talking Dirty/Talking Turkey: Public Health and Tobacco
Gary Wheeler, MD
Chief Medical Director Arkansas Department of Health
Table of Contents

TALKING DIRTY, TALKING TURKEY: PUBLIC HEALTH AND TOBACCOJ. Gary Wheeler, MDChief Medical Officer, Arkansas Dept. of HealthMay 10, 2018
OBJECTIVES
• 1. Identify targets for intervention based on surveillance of tobacco use
• A. youth surveillance• B. literature on youth initiation• C. mechanisms of cessation by adults
• 2. Understand social communication strategies to optimally counter market the tobacco industry
• A. Cold Turkey quitting• B. Branding youth as tobacco free

CURRENT (2015) YOUTH CIGARETTEUSE
• Defined as using cigarettes on one or more of the past 30 days. • United States National Survey 2015: 10.8% The difference between
Arkansas and the U.S. is statistically significant.
• Arkansas 2015: 15.7% • Median of 37 Participating States: 10.8% • Range of Participating States: 4.8% to 18.8% • Only West Virginia and Kentucky were higher than Arkansas.
Percentage of High School Students Who Currently Smoked Cigarettes,* Arkansas YRBS 1995-2015†
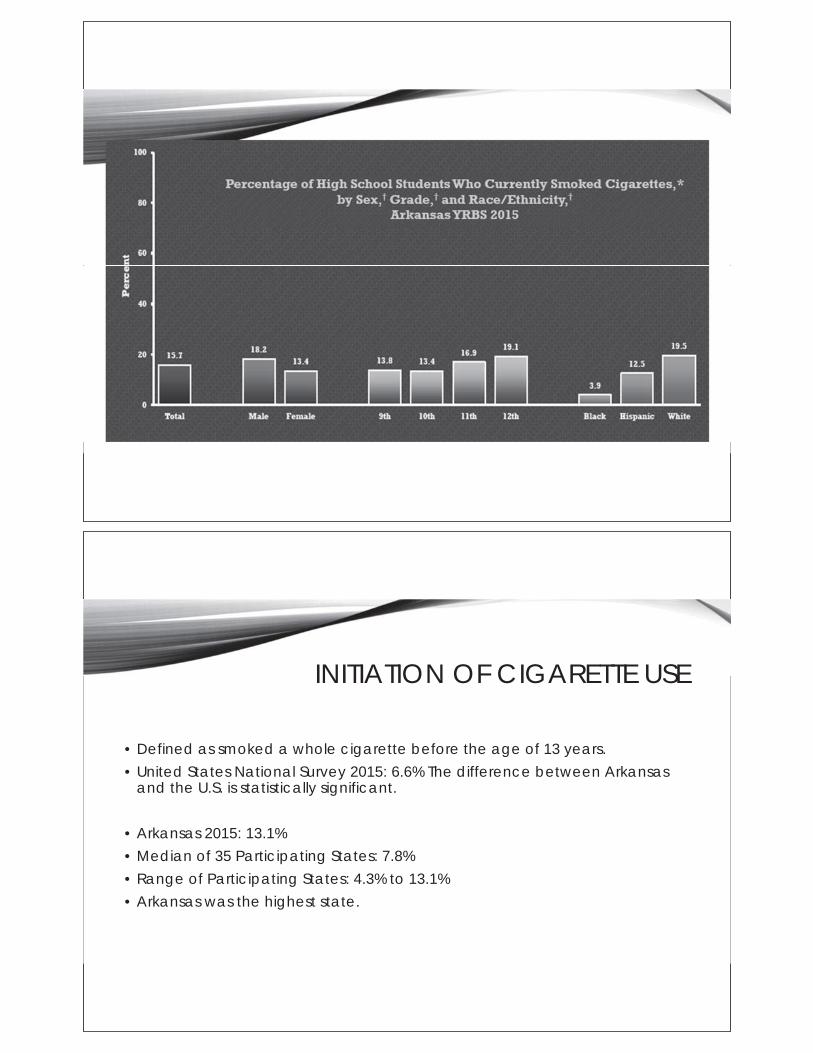
INITIATION OF CIGARETTE USE
• Defined as smoked a whole cigarette before the age of 13 years. • United States National Survey 2015: 6.6% The difference between Arkansas
and the U.S. is statistically significant.
• Arkansas 2015: 13.1% • Median of 35 Participating States: 7.8% • Range of Participating States: 4.3% to 13.1% • Arkansas was the highest state.

CURRENT FREQUENT CIGARETTE USE
• Defined as using cigarettes on 20 or more of the past 30 days. • United States National Survey 2015: 3.4% The difference between Arkansas and the
U.S. was not statistically significant.
• Arkansas 2015: 6.1% • Median of 37 Participating States: 3.6% • Range of Participating States: 1.5% to 7.4% • West Virginia was higher than Arkansas.
• Youth Risk Behavior Survey (YRBS) 16
SMOKELESS TOBACCO USE
• Defined as using chewing tobacco, snuff, or dip on one or more of the past 30 days.
• United States National Survey 2015: 7.3% The difference between Arkansas and the U.S. is statistically significant.
• Arkansas 2015: 10.6% • Median of 34 Participating States: 8.6% • Range of Participating States: 3.0% to 13.4% • Nine states were higher than Arkansas.

CURRENT CIGAR USE
• Defined as using cigars, cigarillos, or little cigars on one or more of the past 30 days.
• United States National Survey 2015: 10.3% The difference between Arkansas and the U.S. is statistically significant.
• Arkansas 2015: 14.2% • Median of 33 Participating States: 10.4% • Range of Participating States: 6.8% to 16.5% • Only Mississippi was higher than Arkansas.
CURRENT ELECTRONIC VAPOR PRODUCTS USE
• Defined as e-cigarette, e-cigar, e-pipe, vape pipes, vaping pens, e-hookahs, and/or hookah pens use at least 1 day in the past 30 days.
• United States National Survey 2015: 24.1% The difference between Arkansas and the U.S. was not statistically significant.
• Arkansas 2015: 26.4% • Median of 35 Participating States: 23.5% • Range of Participating States: 15.3% to 31.2% • Six states were higher than Arkansas.

JUULS

YOUTH INITIATION
• Addiction potential• Social environment • Marketing
NDIT STUDY (CANADA)
Predictors: Individual• Young age• Single parent family• Stress• Impulsivity• Low self-esteem• Poor school performance• Susceptibility to advertising• Addictiveness• Alcohol use• Use of other tobacco
Predictors: Contextual• Smoking by parents• Smoking by sibs• Smoking by friends• Smoking by school staff• Attending a smoking tolerant school

NDIT STUDY (CANADA)
• Other findings• 17% of novice smokers were tobacco dependent• Dependence could develop in 4mths• Slower metabolizers (CYP2A6) of nicotine had
higher rates of dependence• Ability to quit was positively affected by package
warnings, male sex, team sports, increased age
INITIATION OF E-CIGARETTES
• Middle and high school students, 2013-14• Surveyed 340 ever users in Fall 2013• If still using in Spring of 2014, examined predictors defined in Fall for
continued use:• YOUNGER, USE TRADITIONAL CIGARETTES• LOW COST• USE ANYWHERE• INTENT TO QUIT TRADITIONAL CIGARETTES
• Bold KW et al. Pediatrics 2016:138:e20160895

ROLE OF ADULTS
• 50 state review-Molly Miller, Bob DeLongchamp• Relative benefits of adult smoking rate, poverty, college education, per-cent
African-American and Hispanic, cigarette tax rate, smoke free laws, literacy, state funding for tobacco
• Adult smoking rate (BRFSS) had greatest impact on rates of youth smoking (YRBS, use in last 30 days)
• Clean indoor air laws also important
ROLE OF MARKETING
†Promotional expenditures and “others” included point of sale, promotionalallowances, sampling distribution, specialty item distribution, public entertainment, direct mail, endorsements/testimonials, Internet, coupons, retail value addedCokkinides V et al CA Cancer J Clin 2009: 59:352-365.

ROLE OF MARKETING
• E-cigarettes advertising:• 2010 5.6 million• 2014 115.3 million

INTERVENTIONS THAT WORK
• Normalization• Clean air regulations• Advertising Regulation (around schools, POS)
• Price• elasticity• No taxes (e-cigs)• Cheaper products (smokeless, e-cigs)
• Access• Voluntary-TARGET, CVS (2013)• Legal-e.g e-cigs (ENDS) Act of Arkansas, Act of US (2015)
CLEAN AIR REGULATIONS AND YOUTH SMOKING
• …implementing smoking bans through policies, regulations, and laws, as well as other coordinated efforts that establish smokefree social norms (USDHHS 2000; Task Force on Community Preventive Services [TFCPS] 2005; NIH [National Institutes of Health] State-of-the-Science Panel 2006; Bonnie et al. 2007; Centers for Disease Control and Prevention [CDC] 2007; National Cancer Institute [NCI] 2008).
• Chapter 6, 2012 Surgeon General’s report

CLEAN AIR NORMALIZATION
• Although there is a prevalent belief that providing effective warnings to youths requires approaches different from those used for adults, broad educational efforts that reach all age groups have been shown to be more effective in influencing youth behavior than efforts targeted specifically at them.
• WHO, http://www.who.int/tobacco/control/populations/youth/en/index1.html
ADVERTISING BANS
• Limited bans are not associated with drops in smoking; comprehensive bans are (substitution effect)
• Family Smoking Prevention and Tobacco Control Act of 2009. Bans flavorings in cigarettes (not cigars or ENDs and not menthol)
• Bans on use of menthol and flavorings are proposed particularly for cigars, little cigars, hookah, and ENDs.
• POS, outdoor, storefront (First amendment issues)

PRICE/ELASTICITY
• 17 low and middle income countries (S. Africa, Egypt, Russia, Mexico, Peru, India, China, etc) Ten per cent increase in price would reduce consumption by 7.4-10.9%
• Kostova, Tobacco Control 2011;20:419e424.
• RJ Reynolds: If prices were 10% higher, 12-17 incidence [youth smoking] would be 11.9% lower
• R.J. Reynolds Executive D. S. Burrows, “Estimated Change In Industry Trend Following Federal Excise Tax Increase,” September 20, 1982, Bates No. 501988846/8849
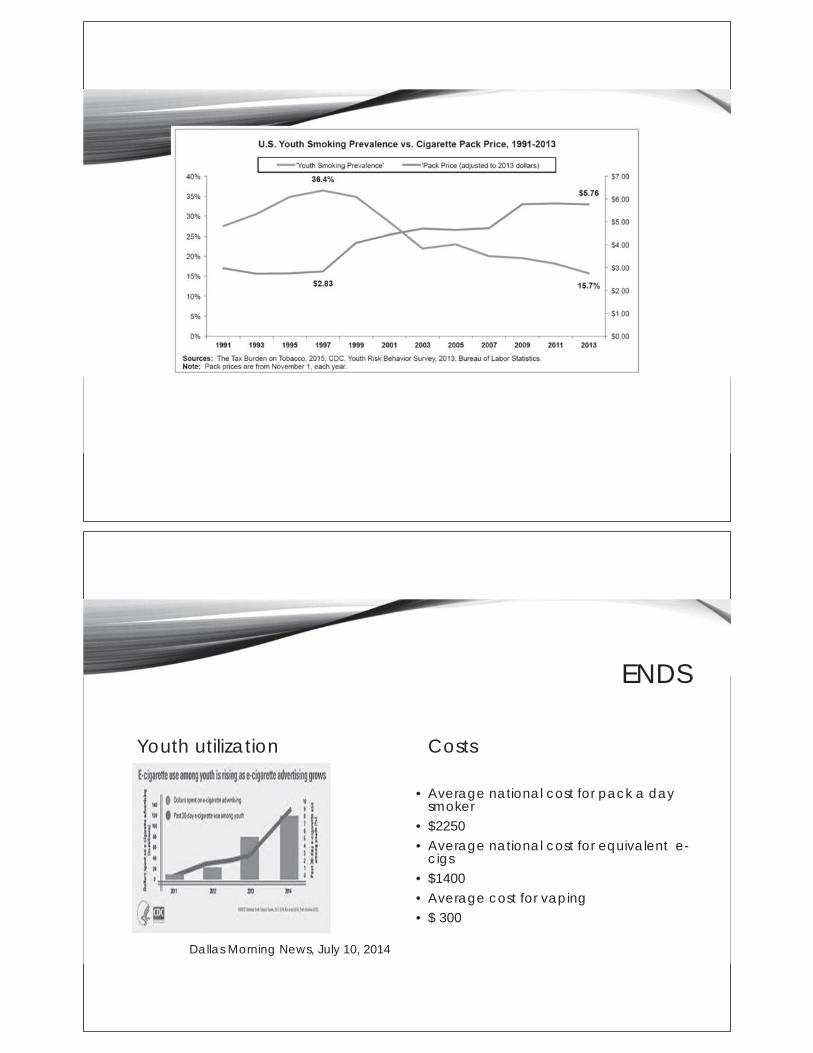
ENDS
Youth utilization Costs
• Average national cost for pack a day smoker
• $2250• Average national cost for equivalent e-
cigs• $1400• Average cost for vaping• $ 300
Dallas Morning News, July 10, 2014

SOCIAL MARKETING
RESCUE: SOCIAL BRANDING
• Profile youth• Identify population using social media• “Value identify” the population• Capture the population with brand• Utilize values to imprint behavior


DOWN AND DIRTY ACTIVITIES
• Sponsor rural events• Rodeo, mudding, ATV events, county fairs
• Branded gear• Targeted digital advertising on Facebook, Youtube
• Luke Bryan, Bass Pro, and Carhartt• Social media campaigns
• Aligned to values—personal freedom, love of country and family• Traditional media
DOWN AND DIRTY EXAMPLES
• https://www.facebook.com/DownandDirtyAR/videos/360334144420132/
• The Hunt
• https://www.facebook.com/DownandDirtyAR/videos/394242694362610/
• My Hometown
CESSATION

HOW ADULTS QUIT IN ARKANSAS
OPTIONS FOR QUITTING
• Quitlines• NRT, Chantix• Brief Tobacco Interventions• Counselling• Hypnosis and other alternatives• E-cigs, ENDS• Cold Turkey

MATH
• Per cent of smokers who use Quitline successfully3,000 /560,000= 0.53%
Per cent of smokers who try to quit in a year560,000 x 47%= 263,000
Who might quit cold turkey?2/3 x 263,000 or ~175,000 chances to help someone quit
ADULT TOBACCO SURVEY RESULTS
• 1) Unassisted quitters (cold turkey) are the largest group of successful quitters • 2) Successful CT quitters were younger, unmarried, healthier, refractory to e-
cigarettes, and possibly less addicted to nicotine.• 3) Further mining the cultural features of this group may allow development
of counter marketing that will lead unassisted quitters to cessation. In addition, confirming that certain methods of unassisted quitting (e.g. sudden vs gradual nicotine reduction) may become part of messaging that may make it more impactful.
•

DEVELOPING NEW STRATEGIES FOR QUITTING: COLD TURKEY
• Reviewed the literature to capture features of quitters to use to develop messaging
• Sum above with survey results• Draft messages• Conduct focus groups to test messages and to gain additional insights• Counter-marketing creation in cooperation with CJRW

I am a proud quitter. If I can do it, you can too.
I take it one day at a time. Working on our family farm
helps. The kids love the open space, and I love the hard
work
and the fresh air.

6
Smoke-Free for Baby and Me
Nicole Ward, MSN
Clinical Assistant Professor UAMS
Table of Contents
Smoke Free for Baby and Me
NICOLE WARD, MNSC, APRN, WHNP-BC, TTS
UAMS COLLEGE OF NURSING
Objectives
Describe risks associated with tobacco use during pregnancyDescribe risks associated with passive smoke exposure Identify challenges and benefits to smoking cessation during pregnancyIdentify ACOG recommendations for smoking cessation during pregnancyExplore risk differences between nicotine exposure and combustion exposureReview pharmacologic recommendations Discuss emerging tobacco products – e-cigarettes, juul, iQOS

Smoking during and after pregnancy
0
10
20
30
40
50
60
U.S. ArkansasPP Arkansas
2015 PRAMSModifiable risk factor
contributing to:
Low Birth Weight
Preterm Labor
Preterm Birth
Spontaneous Abortion
Birth Defects
SIDS
Infant and Child illnesses
Passive Exposure
Half of women who quit will relapse after delivery.
Exposure to SHS increases SIDS and respiratory illnesses.
Gap in knowledge creates an opportunity to promote quitting!

Benefits of Quitting
Increased O2 to baby within 1 day
Lower risk of infant respiratory illness and childhood asthma
Lower risk of premature labor and birth
Lower risk of low birth weight
Higher chances of hospital discharge with mom
Psychosocial benefits of being a non-smoker
Barriers to Quitting
0
10
20
30
40
50
60
70
80
Percentage of women who reported these as barriers to smokingcessation

ACOG Recommended 5 A’s Brief Intervention
Ask – Screen at Each Visit
Advise – Give a strong message to quit
Assess – Ask about readiness to quit
Assist – Help those who are ready
Arrange – Follow up for quitters
Smoking Myths
It will hurt the baby to completely stop smoking
The chemicals in nicotine replacement will hurt the baby
Saliva from nicotine gum goes straight to the baby
E-cigarettes are safe

Pharmacotherapy
Reserved for heavier smokers - >10 cigs/day
Unsuccessful attempts with counseling
Use the lowest dose for the shortest time, titrate accordingly
Postpone until 2nd trimester if possible
Pharmacotherapy
Use in combination with counseling for best resultsGum, lozenges, patches, inhaler, nasal sprayWill reduce cravings, will NOT address habitUsed under close supervision – make sure they actually stop smokingDiscuss the risks and benefits with the patientNo compelling evidence of harm, but no compelling evidence of safetyLimited evidence of efficacyACOG does not recommend buproprion or vareniclineduring pregnancy or breastfeeding

E-cigarettes
Contain nicotine
Eliminate Combustion
Substantial evidence of lower toxicity in adult use
Evidence of lower short term harms in adult use
Long term effects are unknown
No studies on perinatal outcomes
Include with tobacco screening
ACOG does not recommend them for pregnant women

7
Incorporating Genetics into Gynecologic Cancer Care
Kristin Zorn, MD
Associate Professor Department of Obstetrics and Gynecology
UAMS
Table of Contents

Incorporating genetics into gynecologic oncology:a change in the standard of care
Kristin Zorn, MDDivision Director, Gynecologic Oncology
Director, Hereditary Gynecologic Cancer ClinicActing Director, Adult Cancer Genetics
University of Arkansas for Medical Sciences
VERBAL DISCLOSURE
• I have no conflicts of interest to disclose.

Objectives
• Define the role of hereditary causes of ovariancancer
• Define the role of hereditary causes ofendometrial cancer
• Review impact of genetics on standard of carefor ovarian and endometrial cancer
Ovarian, fallopian tube, andperitoneal cancer
Peritoneum

Ovarian cancer overview
20172017
63yearsMedian age
at diagnosis Despite optimal upfront surgery and
adjuvant chemotherapy, 80% of
patients with advanced ovarian cancer
will relapse
Ovarian cancer is the leading cause of death from gynecologic cancers in the United States
Nearly two-thirds of women
with ovarian cancer are
diagnosed
at an advanced stage
22,440 Estimated new cases Estimated deaths14,080
CDC. https://www.cdc.gov/cancer/ovarian/basic_info/index.htmSEER. http://seer.cancer.gov/statfacts/html/ovary.htmlMcAlpine et al. Mod Pathol 2012Slide courtesy of K. Moore
Ovarian cancer treatment summary
• We have identified a standard of care that impacts ovarian cancer survival:
- aggressive initial debulking when possible
- chemotherapy with taxane and platinum
(neoadjuvant and/or adjuvant)
- intraperitoneal route when possible
• 75-80% of women with ovarian cancer will relapse despite our best efforts
NOVEL TREATMENTS ARE NEEDED

Majority of OC patients do not getguideline compliant care
• Current standard of caredebulking surgery6 cycles of chemotherapy including taxaneand platinum (neoadjuvant and/or adjuvant)
• Only 36% of American OC patients receive this SOC
Bristow et al. J Am Coll Surg 2015
High volume specialized careimproves OC outcomes
• Being treated by a gynecologic oncologist improvesoverall survival
• Being treated by a high volume hospital and ahigh volume physician improves overall survival
Engelen et al. Cancer 2006Bristow et al. Gynecol Oncol 2014Bristow et al. J Am Coll Surg 2015

Milestones in OC chemotherapy(frontline treatment)
REGIMEN CHANGE OS IMPROVEMENT
Addition of platinumGOG 47 1986
6 months
Addition of paclitaxelGOG 111 1996
14 months
Intraperitoneal routeGOG 172 2006
17 months
FDA approved drugs for ovarian cancer
• Cyclophosphamide 1959• Thiotepa 1959• Melphalan 1964• Doxorubicin 1974• Cisplatin 1978• Altretamine 1990
• Liposomal doxorubicin 1995• Carboplatin 1989• Paclitaxel 1992• Topotecan 1996• Gemcitabine 2006• Bevacizumab 11/14/14• Olaparib 12/19/14• Rucaparib 12/19/16• Niraparib 3/27/17

Germline mutations and cancer riskSporadic cancer: 2 acquired mutations
Hereditary cancer: 1 inherited and 1 acquired mutation
2 working copies 1 working copy1 mutation
2 mutations tumor develops
1 working copy1 mutation
2 mutations tumor develops
Autosomal dominant inheritance
-Parent of either sex has a
50-50 chance of passing a
mutation to a child of
either sex
-Paternal family history
shouldn’t be ignored even
when we’re discussing
breast and ovarian cancer
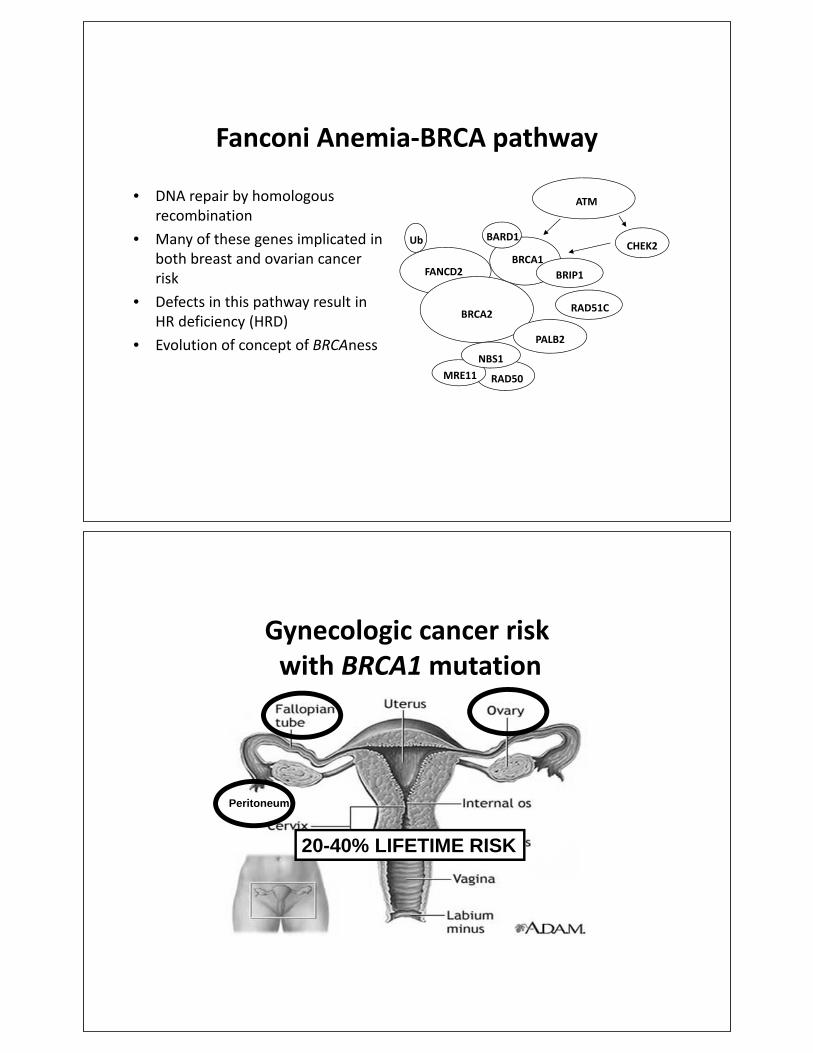
Fanconi Anemia BRCA pathway
• DNA repair by homologousrecombination
• Many of these genes implicated inboth breast and ovarian cancerrisk
• Defects in this pathway result inHR deficiency (HRD)
• Evolution of concept of BRCAness
FANCD2
Ub
RAD50MRE11
BRCA1
BRCA2
NBS1
ATM
BRIP1
PALB2
CHEK2BARD1
RAD51C
Gynecologic cancer riskwith BRCA1 mutation
Peritoneum
20-40% LIFETIME RISK

Gynecologic cancer riskwith BRCA2 mutation
Peritoneum
11-22% LIFETIME RISK
Germline mutations in ovarian cancer
• Massively parallel sequencing• Unselected by age or history• 24% of 360 subjects carried
mutation in 1 of 21 tumorsuppressor genes
• >30% had no family history• >35% were 60 at diagnosis• Mutations most common in but
not limited to grade 3 serouscancer
Walsh et al. Proc Natl Acad Sci 2011

Hereditary susceptibilityto ovarian cancer
Hereditary(~24%)
Sporadic
BRCA1(~45%)
BRCA2(~27%)
Courtesy of Elizabeth Swisher, MD
Lynch(<1%)
Other single genes(~27%)
NCCN guidelines for germline testing
• Personal history of epithelial ovarian, fallopian tube,or primary peritoneal cancer suffices to recommendgenetic counseling and testing
• Not dependent on family history• Not dependent on ethnicity (i.e. Ashkenazi descent)• Not dependent on tumor pathology (i.e. serous
histology)
Version 1.2011 onward, www.nccn.org
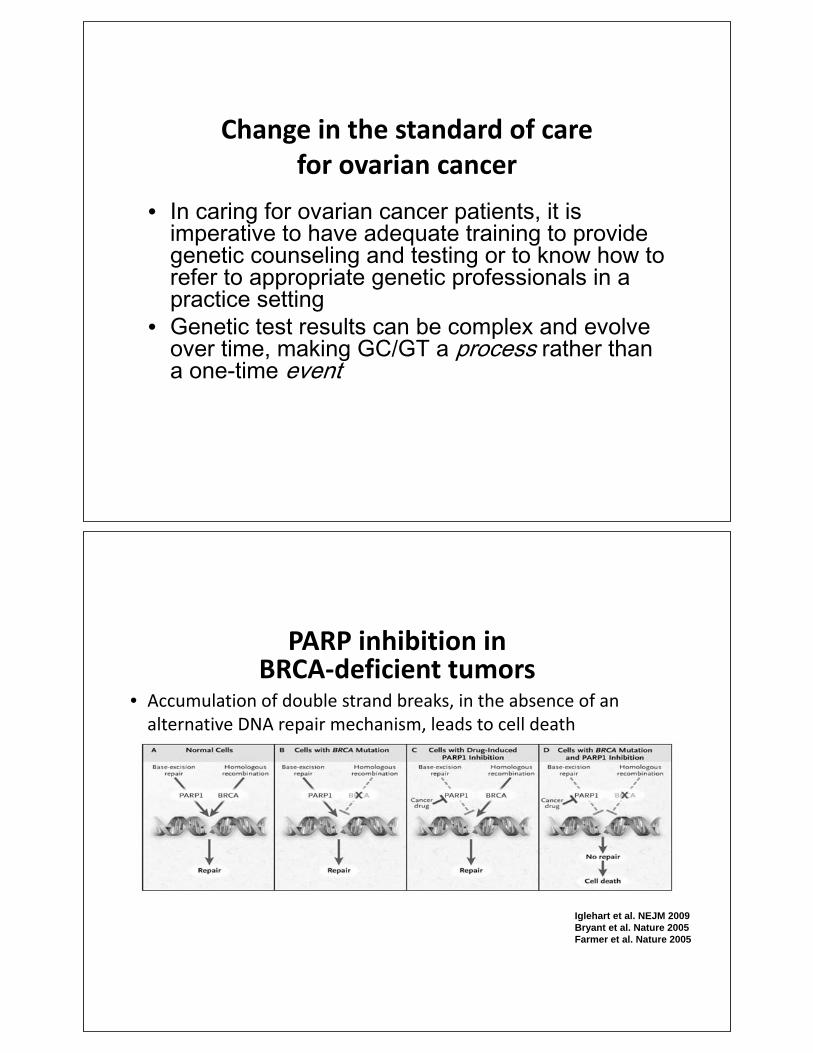
Change in the standard of carefor ovarian cancer
•
•
PARP inhibition inBRCA deficient tumors
• Accumulation of double strand breaks, in the absence of analternative DNA repair mechanism, leads to cell death
Iglehart et al. NEJM 2009Bryant et al. Nature 2005 Farmer et al. Nature 2005

Types of genetic events
• Germline variation in the lineage of germ cells that can betransmitted to offspring
• Somatic alterations in DNA that occur after conception in anytype of cell except germ cells; can be passed through celldivision to progeny of mutated cell but not to offspring
• Epigenetic heritable changes in gene expression that do notinvolve underlying DNA sequence; change in phenotypewithout change in genotype
HRD assays• Several somatic assays in development to quantify genomic instability• Components include loss of heterozygosity, telomeric allelic imbalance,
and large scale state transitions• Retrospective analysis shows that composite HRD score predicts
progression free and overall survival in serous OC patients treated withplatinum
• Evaluation ongoing in prospective trials with potential to direct treatmenttowards platinum therapy (breast cancer) and/or PARPi in sporadic tumors
Swisher et al. EORTC 2014Haluska et al. EORTC 2014McNeish et al. ASCO 2015
Wilcoxen et al. ASCO 2015Mills et al. SGO 2016

GOG 218: Presence of HRD increases PFS and OS
MutationCategory
Hazard Ratio (95% CI)
P-Value
BRCA2 0.36 (0.25 – 0.53) <0.0001
BRCA1 0.74 (0.59 – 0.94) 0.01
Other HR 0.67 (0.49 – 0.90) 0.007
Norquist et al. SGO 2016
MutationCategory
Hazard Ratio (95% CI)
P-Value
BRCA2 0.52 (0.40 – 0.67) <0.0001
BRCA1 0.80 (0.67 – 0.97) 0.02
Other HR 0.73 (0.57 – 0.94) 0.01
Progression-free survival
Overall survival
FDA approval of olaparib monotherapy• Accelerated approval granted to olaparib Dec. 2014 based on objective
response rate and duration of response• Indication granted for treatment of recurrent OC patients with deleterious
or suspected deleterious germline BRCA mutations– 3 lines of prior chemotherapy– Myriad’s germline test approved as companion diagnostic
• In Europe, maintenance therapy approved for platinum sensitive,recurrent OC patients with germline or somatic BRCA mutations
• 400 mg twice daily by mouth (capsule 16 total)

FDA approval of rucaparib monotherapy
• Accelerated approval granted to rucaparib Dec. 2016 based on objectiveresponse rate and duration of response
• Priority Review, Breakthrough Therapy and Orphan Drug designationsgranted for this application
• Indication granted for treatment of recurrent OC patients with deleteriousgermline or somatic BRCA mutations– 2 lines of prior chemotherapy– Foundation Medicine next generation sequencing approved as
companion diagnostic (somatic testing)• 600 mg twice daily by mouth (4 total)
FDA approval of niraparib monotherapy
• Approval granted to niraparib Mar. 2017 based on improved progressionfree survival compared to placebo
• Fast Track, Priority Review, Breakthrough Therapy and Orphan Drugdesignations granted for this application
• No requirement for BRCA testing because both those with and withoutgermline BRCA mutations had significant benefit
• 300 mg once daily by mouth (3 total)

Updated FDA approval of olaparib• Regular approval granted to olaparib Aug. 2017 based on improved
progression free survival• Indication granted for maintenance treatment of recurrent OC patients
with complete or partial response to platinum based therapy regardless ofBRCA mutation status
• Olaparib tablets also approved for both indications (replacing capsules)• Tablet dose is 300 mg (2 150 mg tablets) twice daily by mouth; 100 mg
tablet also available for dose reductions• Capsules and tablets CANNOT be substituted mg to mg because of
bioavailability differences
Veliparib
• GOG 3005: first clinical trial incorporating a PARPiinto frontline therapy for ovarian cancer completedaccrual this spring
• Combination therapy with taxane and platinum aswell as monotherapy for maintenance

Event Olaparib Placebo Niraparib Placebo
G1 4 G3/4 G1 4 G3/4 G1 4 G3/4 G1 4 G3/4
Nausea 68.4% 2.2% 35.2% 0% 73.6% 3% 35.2% 1.1%
Vomiting 31.6% 2.2% 14.1% 0.8% 34.3% 1.9% 16.2% 0.6%
Fatigue 48.5% 6.6% 37.5% 3.1% 59.4% 8.2% 41.3% 0.6%
Anemia 16.9% 5.1% 4.7% 0.8% 50.1% 25.3% 6.7% 0%
Thrombocytopenia
NR NR 61.3% 33.8% 5.6% 0.6%
Neutropenia NR NR 30.2% 19.6% 6.1% 1.7%
Ledermann et al. NEJM 2012Mirza et al. NEJM 2016
• Patients on placebo have adverse events; they are not without symptoms
• AEs are manageable with low rates of discontinuation
PARPi toxicity
GI toxicities are common with all PARPi(% of pts)
Toxicities Grade of toxicity Olaparib 1 Rucaparib2 Niraparib3
Nausea All Grades 64 77 73.6
Grade 3 and 4 3 5 3.0
Constipation All 20.65 40 39.8
Grades 3 and 4 0 2 0.5
Vomiting All 43 46 34.3
Grades 3 and 4 4 4 1.9
Decreased appetite All 22 39 25.3
Grades 3 and 4 1 3 0.3
Abdominal pain All 43 32 22.6
Grades 3 and 4 8 3 1.1
Diarrhea All 31 34 19.1
Grades 3 and 4 1 2 0.3
Dyspepsia All 25 104 11.4
Grades 3 and 4 0 <1% 0
Dysgeusia All 215 39 10.1
Grades 3 and 4 0 0.3 0
1FDA package insert2FDA package insert3NOVA NEJM 20164Swisher Lancet Onc 20165Ledermann Lancet Onc 2014

Hematologic toxicities are common with all PARPi(% of pts)
Toxicities Grade of Tox Olaparib1 Rucaparib2 Niraparib3
Decrease in
hemoglobin
All Grades 90 67 50.1
Grade 3 and 4 15 23 25.3
Decrease in
platelets
All 30 39 61.3
Grades 3 and 4 3 6 33.8
Decrease in
neutrophil count
All 25 35 30.2
Grades 3 and 4 7 10 19.6
1FDA package insert2FDA package insert3NOVA NEJM 2016
Fatigue is common with all PARPi(% of pts)
Toxicities Grade of Tox Olaparib 1 Rucaparib2 Niraparib3
Fatigue All Grades 66 77 59.4%
Grade 3 and 4 8 11 8.2%
Insomnia All NR 12% 24.3%
Grades 3 and 4 NR 0 0.3%
Headaches All Grades 255 174 25.9
Grades 3 and 4 0 04 0.3
1FDA package insert2FDA package insert3NOVA NEJM 20164Swisher Lancet Onc 20165Ledermann Lancet Onc 2014

MDS/AML risk
• Myelodysplastic syndrome and acute myeloidleukemia are potentially fatal complications
• Rare: 0.5 2% in trials to date• Can be seen months to years after starting therapy• Role of PARPi vs chemotherapy difficult to discern
Resistance to PARP inhibitorsthrough multiple mechanisms
Bouwman et al. Clin Cancer Res 2014

Immunotherapy• Pembrolizumab (PD 1 receptor antibody) granted accelerated
approval by FDA in May 2017 for patients with metastatic orunresectable solid tumors with microsatellite instability (MSIH) or mismatch repair deficient (abnormal IHC) based onresponse rate
• First FDA drug approval based on presence of a biomarkerrather than the primary site of the tumor
• Recommended dose 200mg IV every 3 weeks (flat dose)• Since 2014, all colorectal and endometrial cancer patients are
being screened at UAMS with MSI and IHC for Lynchsyndrome
Lynch syndrome
• First described by Henry Lynch in 1960s, running counter to prevailing theory that all cancer had viral or environmental origins
• Also known as hereditary non-polyposis colorectal cancer (HNPCC)

Question #1
What percentage of ovarian cancer is due to
hereditary causes?
A. 5%
B. 10%
C.20%
D.24%
Question #1
What percentage of ovarian cancer is due to
hereditary causes?
A. 5%
B. 10%
C.20%
D.24%

Lynch syndrome
• Accounts for 3-5% of colorectal and endometrial cancer cases in the US
• 1 million Americans are projected to have Lynch syndrome but only 5% are currently diagnosed
• Lynch syndrome is not a rare condition but rather an extremely underdiagnosed one!
lynchcancers.com
Dr. Henry Lynch
Estimated new US cancer cases
Siegel et al. CA Cancer J Clin 2017

Estimated new US cancer cases
Siegel et al. CA Cancer J Clin 2017
~9,840 patients with cancer related to Lynch syndrome
each year
Lynch syndrome related cancers
• Colorectal• Endometrial• Ovarian• Gastric• Pancreatic• Ureteral• Renal pelvis• Brain (usually glioblastoma)• Small intestinal• Sebaceous adenoma, carcinoma, & keratoacanthoma
Version 2.2017, www.nccn.org

MLH1, MSH2, PMS2 and MSH6
• Tumor suppressor genes involved in Lynch syndrome
• Mismatch repair pathway
• EPCAM can have germline deletions in last few exons that cause epigenetic silencing of MSH2
• Mutations associated with increased cancer susceptibility in adulthood
Ligtenberg et al. Nat Genet 2009
NCCN guidelines for colon cancer
• Universal mismatch repair (IHC) or microsatelliteinstability testing recommended in all patients witha personal history of colon or rectal cancer
• MMR or MSI testing should be performed only inCLIA approved laboratories
Version 2.2017, www.nccn.org

NCCN guidelines for endometrial cancer
• Tumor screening for mismatch repair deficiency isappropriate for all colorectal and endometrialcancers regardless of age at diagnosis
Version 2.2017, www.nccn.org
Universal screening for Lynch syndrome
• Screening of all colorectal and endometrial cancer patients for Lynch syndrome has been in place at UAMS since 2014

NCCN guidelines forLynch syndrome surveillance
• Colonoscopy at 20 25 or 2 5 years earlier than youngestcolon cancer (whichever is earliest) and repeat every 1 2years
• Aspirin may decrease risk of colon cancer but optimal doseand duration of therapy uncertain
• Consider upper GI endoscopy every 3 5 years starting at 3035
• Consider annual urine cytology starting at 30 35 (especiallywith MSH2m)
• No increased breast cancer screening above routinerecommendations
• Consider annual endometrial biopsy until hysterectomy• Consider hysterectomy and BSO after childbearing complete
Version 2.2017, www.nccn.org
Inherited cancer risk can be managed
• Prevention to keep cancer from developing– Lifestyle choices– Medications– Surgery
• Screening to find cancer early– Colonoscopy– Mammograms & breast MRI
• Treatment once cancer is found– Surgery– Chemotherapy– Targeted therapy like PARP inhibitors

Models for providing genetic counseling and testing
• Physician with appropriate training
• Allied professional with appropriate training– Genetic counselor
– Advanced practice nurse
• Remote provider– GC via testing company
– GC via telehealth
• One-on-one vs group appointments
Question #2
What percentage of endometrial cancer is due to
Lynch syndrome?
A. 1-2%
B. 3-5%
C.8-10%
D.18-20%

Question #2
What percentage of endometrial cancer is due to
hereditary causes?
A. 1-2%
B. 3-5%
C.8-10%
D.18-20%
Cancer genetics in Arkansas•
•
•
•

Community Review Board
•
Current grant
• Increase access to cancer GC/GT across AR through telehealth conferences between local providers and UAMS experts
• Goal 1: educate local providers about LS and its impact on cancer risk
• Goal 2: implement algorithm for screening CRC and EC patients through local providers
Arkansas Minority Health CommissionRed County Report 2015

We need your help!
• If you are a surgeon, pathologist, primary care provider or other practitioner who wants to increase access to cancer GC/GT for your patients, please sign up for telehealth conferences with us
• Anticipate conference about once a month for no more than an hour
Cancer genetics research501 526 6990 ext 8529
[email protected]@uams.edu
Gyn cancer genetics research team
Mindy Simonson, ScM, CGC
Joshua Acuna, MPH
Amanda Compadre, MS4
Collaborators:
Kent McKelvey, MD
Jill Kelsay, CGC
Matt Quick, MD
Jennifer Laudadio, MD
Jonathan Laryea, MD
Jason Mizell, MD
Conan Mustain, MD
Katy Gray, MD
Ledare Finley, CGC
Elizabeth Swisher, MD
Arkansas
Breast Cancer
Research Program

Summary
• The standard of care is evolving rapidly for ovarianand endometrial cancer for the first time in decades
• Genetic information is playing an increasingly criticalrole in directing therapy– PARP inhibitors are a new class of drug approved for the
first time in ovarian cancer– Mismatch repair deficiency is a tumor biomarker used to
determine eligibility for pembrolizumab regardless oftumor site
Summary
• Despite these advances, the cure rate for ovarian andadvanced endometrial cancer is not improving
• Prevention of gynecologic cancer throughidentification of high risk individuals is our currentchallenge

8
Technology is Changing Healthcare
Charles Caldwell Jr., MD
Cardiologist North Little Rock, Arkansas
Table of Contents

T E C H N O L O G Y I S C H A N G I N G
H E A L T H C A R E
C H A R L E S R . C A L D W E L L , M D
A R K A N S A S C A R D I O L O G Y
B A P T I S T H E A L T H H E A R T I N S T I T U T E
D I S C L O S U R E S
• Founder and Board Chairman: iHeartDoc, Inc.-
Housecall Telemedicine

M A X P L A N K
N O B E L P R I Z E W I N N E R I N P H Y S I C S , 1 9 1 8
“A new scientific truth does not win adoption by convincing
its opponents and making them see the light, but because
its opponents eventually die.
… and a new generation comes up that is familiar with it.”
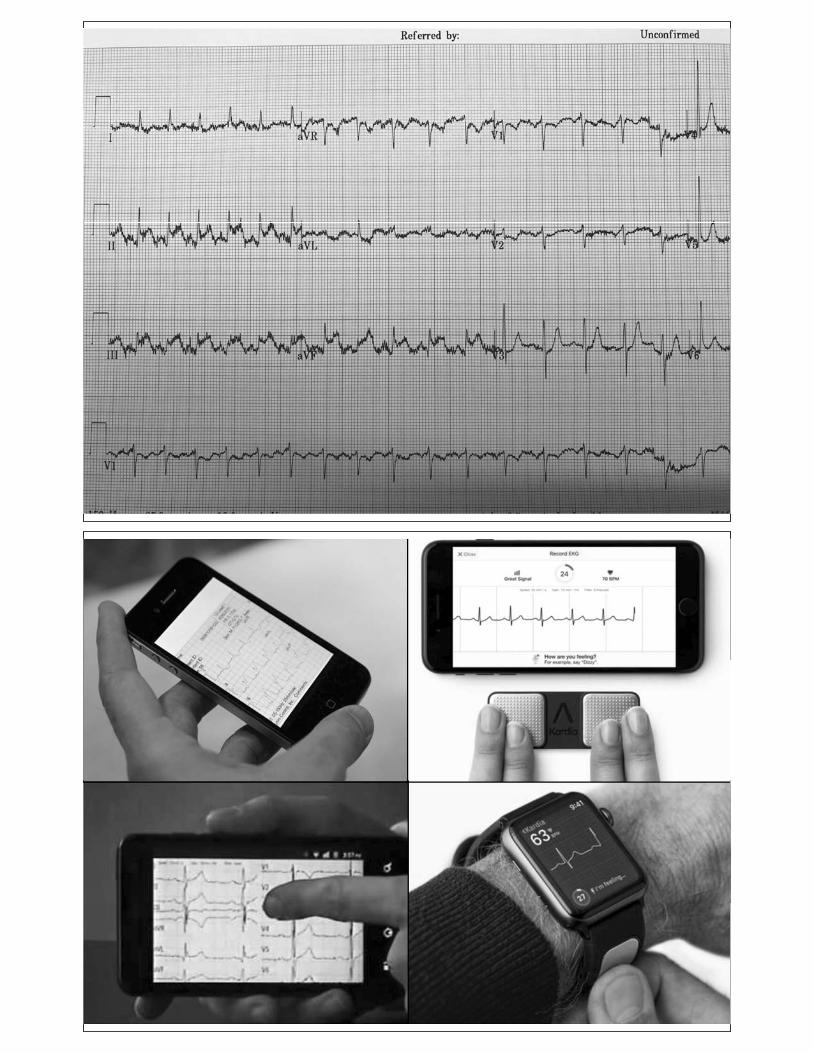

- J A C K W E L C H , F O R M E R C E O G E N E R A L E L E C T R I C
“When the rate of change inside an institution is
slower than the rate of change outside, the end is
in sight.”

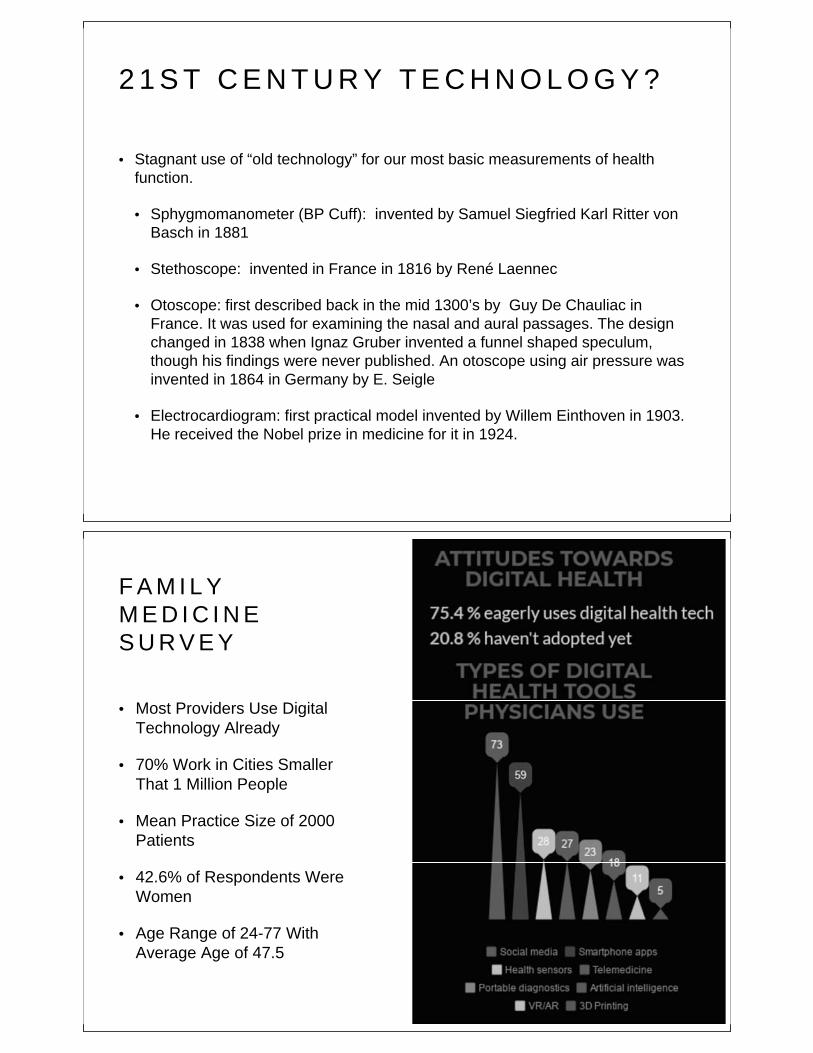
2 1 S T C E N T U R Y T E C H N O L O G Y ?
• Stagnant use of “old technology” for our most basic measurements of health
function.
• Sphygmomanometer (BP Cuff): invented by Samuel Siegfried Karl Ritter von
Basch in 1881
• Stethoscope: invented in France in 1816 by René Laennec
• Otoscope: first described back in the mid 1300’s by Guy De Chauliac in
France. It was used for examining the nasal and aural passages. The design
changed in 1838 when Ignaz Gruber invented a funnel shaped speculum,
though his findings were never published. An otoscope using air pressure was
invented in 1864 in Germany by E. Seigle
• Electrocardiogram: first practical model invented by Willem Einthoven in 1903.
He received the Nobel prize in medicine for it in 1924.
F A M I L Y
M E D I C I N E
S U R V E Y
• Most Providers Use Digital
Technology Already
• 70% Work in Cities Smaller
That 1 Million People
• Mean Practice Size of 2000
Patients
• 42.6% of Respondents Were
Women
• Age Range of 24-77 With
Average Age of 47.5

F A M I L Y
M E D I C I N E
S U R V E Y
• Portable Diagnostics,
Health Sensors and
Telemedicine Lead the
Way
• Less “Dr Google”, More
Curated Websites
• Skepticism of Very High
Tech
W H Y N O T N O W ?
F A M I L Y M E D I C I N E S U R V E Y

F A M I L Y
M E D I C I N E
S U R V E Y
• Patients Want It
• Access To Care
• Efficiency
• Quality
F A M I L Y
M E D I C I N E
S U R V E Y
• Misinterpretation of Data
• Cost
• “Dr Google”
• Hassle Factor

T H E F U T U R E O F M E D I C I N E
F A M I L Y M E D I C I N E S U R V E Y
T E C H N O L O G Y C H A N G I N G
H E A L T H C A R E : B E F O R E T H E V I S I T
• Computer Medical Assistants
• Medical Chatbots For Patients
• Administrative
• Drugs
• Questions
• Wearable Sensors and Devices Stream Data To Providers
• Doctor-Time As A Commodity
• A Team Approach to Care

D I S R U P T I V E T E C H N O L O G Y :
R E Q U I R E S A C H A N G E O F C U L T U R E
• Despite popular belief, disruptive technologies cannot bring change on
their own. Social media, artificial intelligence, robotics, 3D printing, virtual
or augmented reality and health sensors have no effect whatsoever
without a change in stakeholders’ attitude and the structure of the system.
• Redefine Participant Roles. “More Partner, Less Paternal”
• “Googling is a sign of an engaged patient!”
• Recognize That Patients Have More Health Data Than Ever Before
• Home Thermometer, Home Pregnancy Tests, Genetic Analysis, BP
Cuffs, HR monitors and EKGs, Glucometers, CPAP Analysis, Sleep
Analysis
D I S R U P T I V E T E C H N O L O G Y : I T ’ S N O T
T E C H N O L O G Y A L O N E
• Information alone doesn’t change behavior.
• Technology enables behavior change, but technology alone is not sufficient.
• Study of Health Fitness Trackers In Diabetics
• Regardless of physical activity levels of participants before the study began, activity
trackers alone or when combined with rewards designated for charity did not increase
activity levels.
• Nearly half of participants were no longer wearing their trackers by the six-month
assessment period.
• Technology cannot substitute willpower and action, cannot change people from passive
yes-men into proactive leaders if they don’t want to.
• Ancillary Behavioral Programs: Diabetes Prevention/Control, Weight Loss, CHF
Management, Smoking Cessation

V I N T O N C E R F - “ T H E F A T H E R O F T H E I N T E R N E T ”
“The internet is not merely a technology but a new
way of cooperating, sharing, and caring.”

D I S R U P T I V E T E C H N O L O G Y : D I G I T A L I N F O R M A T I O N -
C O L L E C T I O N , I N T E R P R E T A T I O N , O W N E R S H I P
• “Better informed in order to better perform.”
• The patient as collector of medical data
• Reliability
• Accuracy
• Security
• A collaborative approach to data interpretation. The end of medical
paternalism
• The patient owns his/her data, not the provider or the system.
C E N T E R F O R M E D I C A R E / M E D I C A I D
S E R V I C E S ( C M S )
• CPT 99091: Remote Patient Monitoring: Added 1/1/2018
• Collection and interpretation of physiologic data digitally stored and/or
transmitted by the patient and/or caregiver to the physician or other qualified
health care professional, requires minimum 30 minutes
• $58.68 in Arkansas
• Billed no more than every 30 days (Max $704.16 / year)
• Must be transmitted via secure mechanism. Not via unsecured email or text
• Must be seen in person within a year of the service
• Must obtain documented consent from the patient prior to the service.

R E M O T E P A T I E N T M O N I T O R I N G : C P T
9 9 0 9 1
• Patient is remotely managed. Does not have to be seen in person.
• Service can be combined with Chronic Care Management and Transitional Care
Codes
• Applies to:
• Hypertension BP readings
• CPAP management for sleep medicine
• Diabetes: Glucose readings
• EKG readings for rhythm management
• Weight management program
• CHF management
M A C R AM E D I C A R E A C C E S S A N D C H I P R E A U T H O R I Z A T I O N A C T O F
2 0 1 5
• Repealed the Sustainable Growth Rate (SGR) methodology
for determining updates to the Medicare physician fee
schedule.
• MACRA was designed to offer physicians a choice between
two payment pathways:
• A modified fee-for-service model (MIPS)
• New payment models that reduce costs of care and/or
support high-value services not typically covered under the
Medicare fee schedule (APMs)

M A C R AM E D I C A R E A C C E S S A N D C H I P R E A U T H O R I Z A T I O N A C T O F 2 0 1 5
• “MACRA clearly states that CMS’s initial goal was to
move 30% of Medicare reimbursement to value-based
compensation by the end of 2016, with a future goal of
50% by the end of 2018.”
• Changing from VOLUME to VALUE
Q U A L I T Y P A Y M E N T I N I T I A T I V E S
• Merit-based Incentive Payment System (MIPS)
• Traditional Part B Medical Payment Methodology
• Performance Based Payment Adjustment (up or down)
• Advanced Alternative Payment Models (AAPM):
• Shared Risk Based Payment Methodology
• Incentive Payment for Participating in Innovative Payment Models
• Patient Centered Medical Home (PCMH)
• Accountable Care Organizations (ACO): UAMS and Baptist Partnership in ACO
• Medicare Shared Savings Programs (MSSP)
• Comprehensive Primary Care Plus Program (PCP+)

Q U A L I T Y P A Y M E N T I N I T I A T I V E S : P A Y M E N T
C O M P R E H E N S I V E P R I M A R Y C A R E
P L U S ( C P C + )

C O M P R E H E N S I V E P R I M A R Y C A R E
P L U S ( C P C + )
• Access and Continuity
• 24/7 Access To Care
• Care Management
• Identify high-needs patients, provide targeted individual case management, and offer ED
and hospital visit follow-up care
• Comprehensiveness and Coordination
• Manage specialty care needs across the system; monitor patient admission, discharge, and
transfers from EDs and hospitals; identify appropriate specialists for referrals
• Patient and Caregiver Engagement
• Planned Care and Population Health
• Provider Reporting and Health IT Requirements
C O M P R E H E N S I V E P R I M A R Y C A R E
P L U S ( C P C + )

A R K A N S A S B L U E C R O S S B L U E S H I E L D
V A L U E - B A S E D C O M P E N S A T I O N I N I T I A T I V E ( V B C I )
• A 5 Year Plan
• “In the future, a successful business model will be
achieved not by providing a high volume of services,
but rather by meeting goals and expectations
regarding high-quality outcomes, patient-satisfaction
measures, and the elimination of services that are
preventable, redundant, or of low value to patients.”
A R K A N S A S B L U E C R O S S B L U E S H I E L D
V A L U E - B A S E D C O M P E N S A T I O N I N I T I A T I V E ( V B C I )
• Primary Care Value Pool
• Reduced Fee For Service
• Enhanced Fee for Patient-Centered Medical Homes, and meeting agreed-
upon population management measures and achieving high value scores
• Rewarded by increased per-member per-month care coordination fees.
• Speciality Value Pool
• “A specialist’s ratings will be shared with primary care physicians because
each PCP’s value rating will be impacted by the value rating of the referral
specialist selected.”
• Hospital Value Pool
F U T U R E T E C H N O L O G Y
3 D - P R I N T E D C A S T
F U T U R E T E C H N O L O G Y

M E D T R O N I C - A R T I F I C I A L
P A N C R E A S
F U T U R E T E C H N O L O G Y
T E L E M E D I C I N E
N O T S O F U T U R E T E C H N O L O G Y

P A T I E N T C O L L E C T E D D A T A
F U T U R E T E C H N O L O G Y
D A T A M O N I T O R I N G
F U T U R E T E C H N O L O G Y

C O R O N A R Y A T H E R O S C L E R O S I S
G E N E T I C S

C L O P I D O G R E L M E T A B O L I S M
P H A R M A C O G E N E T I C S
C L O P I D O G R E L M E T A B O L I S M
P H A R M A C O G E N E T I C S

A R T I F I C I A L I N T E L L I G E N C E
F U T U R E T E C H N O L O G Y
S U M M A R Y
• Medical Technology Continues To Change The Patient-Physician Relationship
• Recent Changes In Health Policy Like MACRA, Along With CMS And Private Insurance
Payment Policies, Are Changing Medical Practices From Volume To Value Based
• Physician Attitudes Toward Digital Healthcare Are Changing. A Change Of Culture Is
Beginning
• The Patient As The Source Of Medical Data
• 3D Scanning And Cast Printing
• Telemedicine As An Access To Care Portal And Data Analysis Platform
• Personalized Medicine And Pharmacogenetics
• Artificial Intelligence to Rapidly Analyze The Data, Literature, and Make
Recommendations

Q U E S T I O N S ?

9
Physician Involvement in Cancer Care Support Groups on Facebook
Jerad Gardner, MD
Associate Professor Department of Pathology and Dermatology
UAMS
Table of Contents

Physician Involvement in CancerPatient Support Groups on Facebook
Jerad M Gardner, M.D.
Associate Professor of Pathology & DermatologyUniversity of Arkansas for Medical Sciences
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
“I went for more than 30 years without meetinganother person [with angiosarcoma]. It's thisgroup, right here, these people, that are my
tribe.”Angiosarcoma patient
“It was bizarre and isolating to have never metanother person with my mom's diagnosis…I'mso, so glad we [found this group]. Witnessingsuch an extraordinary community…has given
me so much hope in the future...”Daughter of angiosarcoma patient


My role in the groups
Educate patients. Explain their disease.
Explain medical terminology & whatpathologists do
Help them navigate the cancer care system
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
This is how I volunteer

The teacher becomes the student
Savvy patients – THEY teach ME
View whole spectrum of a disease
Different approaches to clinical management
Strengths & weaknesses of status quoWhat we do well, what we could do better
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Cheerleader not Treating Physician
No doctor patient relationship
Real friendships have developed
I was interested in disease…now I am INVESTED
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

Research

DFSP Partnership
Videoconference meetings with DFSP patientpartners, UAMS researchers and a representativefrom Sarcoma Foundation of America
PATIENTS helped design & conduct survey… abouttheir own disease.
They are co authors on study with us!
$50,000 PCORI grant for patient centeredresearch
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
DFSP Partnership
213 DFSP patients from Facebook took the surveyin ONLY THREE WEEKS
Largest survey study of DFSP patients to date
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

Diagnosis delays
3.5 yearsMean time from first noticing lesion to visiting medicalprovider for evaluation
3.6 yearsinitial medical visit to correct diagnosis
7.1 yearsfirst noticing lesion to correct diagnosis
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
0
5
10
15
20
25
30
35
40
45
50
Cyst Lipoma Scar Unknown/Notstated
Others
Perc
ento
ftot
alre
spon
dent
s
PRE BIOPSY CLINICAL SUSPICION
[email protected] Media 101: www.bit.ly/1Aaxuiz

Facebook facilitates long termprospective research of rare diseases
I used to spend hundreds of hours on the phonetrying to track down clinical follow up forresearch projects
Patients move, phone numbers change, doctorsretire…
…but Facebook is forever!
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Crowdsourcing
Large group of rare disease patients can beincredibly useful
In 2015, I started providing url links to Facebookpatient support groups in my official pathologyreports for certain diseases including DFSP,desmoid fibromatosis, and angiosarcoma.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

Patients have pictures of their tumor

Do patients really WANT doctors to beinvolved in their groups?
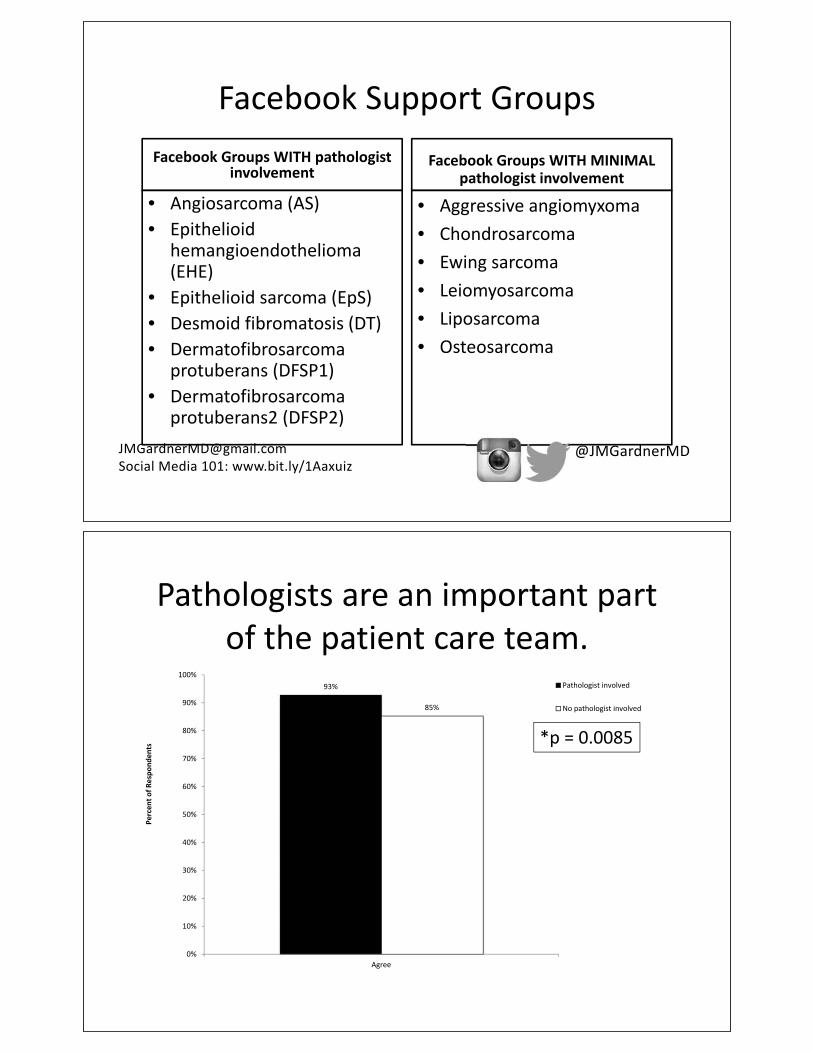
Facebook Support GroupsFacebook Groups WITH pathologist
involvement
• Angiosarcoma (AS)• Epithelioid
hemangioendothelioma(EHE)
• Epithelioid sarcoma (EpS)• Desmoid fibromatosis (DT)• Dermatofibrosarcoma
protuberans (DFSP1)• Dermatofibrosarcoma
protuberans2 (DFSP2)
Facebook Groups WITH MINIMALpathologist involvement
• Aggressive angiomyxoma• Chondrosarcoma• Ewing sarcoma• Leiomyosarcoma• Liposarcoma• Osteosarcoma
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Pathologists are an important partof the patient care team.
93%
85%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Agree
Perc
ento
fRes
pond
ents
Pathologist involved
No pathologist involved
*p = 0.0085

The pathologist’s posts helped meunderstand my disease.
90%
10%
0%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Agree Neutral Disagree
Perc
ento
fRes
pons
es
Pathologist involved
The pathologist on the Facebook supportgroup helped relieve some of my disease
related anxiety.
77%
22%
1%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Agree Neutral Disagree
Perc
ento
fRes
pons
es
Pathologist Involved

Overall, having a pathologistinvolved in this group is a good thing.
98%
1% 1%0%
20%
40%
60%
80%
100%
120%
Agree Neutral Disagree
Perc
ento
fRes
pons
es
Pathologist involved
@JMGardnerMD
77%
20%
Yes
No
Unsure
For groups without a pathologist, we asked:
Do you want a pathologist involved in yourFacebook Support group?

Do you want other doctors involved inthe Facebook support group?
69%
5%
26%
63%
6%
31%
0%
10%
20%
30%
40%
50%
60%
70%
80%
yes no unsure
Perc
ento
fRes
pons
esPathologist involved
No pathologist involved
Top Requested Specialties
Patient
Research
HolisticMedicine
PainManagement
Psychiatry
InternalMedicineEndocrine
Oncology
Surgery
Radiology

Most amazing of all
• 541 respondents in 3 weeks–403 respondents were patients–138 were family members, etc
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Long term vision
Every disease would have a support group
Every group would be partnered with team ofinterested doctors
Free. Powerful.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

How does this apply to Family Medicine?
Search Facebook for ANY disease of interest toyou or your patients
Tell your patients about these groups. Remindthem the groups are not official advice but maystill be helpful
Consider joining a group(s) to participate andvolunteer. Life changing experience for me.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD


Tips for avoiding dermatology pitfalls• Call your dermatopathologist when you need advice on what
type of biopsy to perform, do not understand the pathologyreport, or have any other questions.
• Take a picture of lesion/rash before biopsy. PLEASE.
• Shave and punch biopsies are BIOPSIES, not therapeuticexcisions. “Not extending to section edges” or “marginsnegative in plane of section examined” does NOT equal“entire lesion is excised.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

Tips for avoiding dermatology pitfalls• NEVER biopsy or excise skin lesion and then just throw it
in the trash. Never use LN2 on any lesion where thediagnosis is uncertain.
• It’s not “just a cyst” unless you have a biopsy to prove it.Numerous things can present as skin colored nodules,including rare cancers.
• If a rash or lesion is not improving with treatment, get abiopsy or dermatology consult. Don’t just keep givingsteroids for it.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Tips for avoiding dermatology pitfalls
• Do not ignore an obviously atypical pigmented lesionon your patient just because that wasn’t what theycame in for or because you don’t like to deal withskin lesions. Don’t figure someone else will look intoit. You notice it, it’s your responsibility to saysomething.
• Melanoma can closely mimic seborrheic keratosisand vice versa. Same with BCC.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

Tips for avoiding dermatology pitfalls
• Not all that is annular is tinea (dermatophytefungus).
• Not all rashes in groin/axilla are Candida.
• Cellulitis is not bilateral, but stasis dermatitis is.
• It’s probably NOT a spider bite. MRSA, yes. Skincancer, yes. Spider bite, very unlikely.
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD
Tips for avoiding dermatology pitfalls
A special request from my dermatologist friends:
please please please do NOT use Lotrisone(clotrimazole/betamethasone)
especially not in the groin!
[email protected] Media 101: www.bit.ly/1Aaxuiz
@JMGardnerMD

10
Practice Transformation Part 1: Project Management and the
Business Model
Gary Bevill, MD
SAMA Healthcare Services El Dorado, Arkansas
Pete Atkinson, MHA
SAMA Healthcare Services El Dorado, Arkansas
Table of Contents

Practice Transformation, Part 1: Project Management and the Business ModelUAMS IRC May 11, 2018
Session Objectives
• Identify strategies for fully operationalizing comprehensive primary care
• DDiscuss best practices in resource allocation for expanding the care team
• IIdentify three action items to discuss with your team
Confidential & Proprietary 2

3Confidential & Proprietary
Today’s Speakers
• Dr. Gary Bevill, Physician with SAMA Healthcare• Pete Atkinson, Administrator with SAMA Healthcare• Rachel Wallis, Executive Director with Aledade Arkansas
4Confidential & Proprietary
Aledade/SAMA Partnership
Good for Doctors
Good for Patients
Good for Society

SAMA Healthcare
Confidential & Proprietary 5
SAMA Healthcare Services
• El Dorado, AR• 21,000+ active patients• EMR
• Allscripts Professional EHR• Open extended hours and weekends• Technologically advanced• Same day appointments available• Full Service: Lab, X-Ray, CT, US,
Bone Density, Allergy Clinic, and Pharmacy on Site

History of SAMA
• Practicing Independently• South Arkansas Medical Associates• SAMA Healthcare Services
Evolution of Value Based Care
Confidential & Proprietary 8

9Confidential & Proprietary
Evolution of Value Based Care
• Electronic Medical Records• Meaningful Use/PQRS• Affordable Care Act• Comprehensive Primary Care Classic and Plus• State Patient Centered Medical Home Program
• Medicaid and private payer programs • Aledade Arkansas ACO• Advanced Payment Models• MIPS/MACRA
ogram
Let’s discuss the business side of value-based care.
Confidential & Proprietary 10

11Confidential & Proprietary
Let’s discuss the business side of value based care.
• How do you manage all of these programs? • How has value based care effected your day-to-day practice?• How have you restructured your team to be successful? • How have you allocated resources to drive outcomes?
12Confidential & Proprietary

13Confidential & Proprietary
Measuring Success
• Process Measures• Outcome Measures• Patient Experience Measures
SAMA’s Outcomes
• Change in physician practices• Change in APRN practices• Change in accessibility• Change in continuity of care

CPC+ ACUTE INPATIENT DISCHARGES
CPC+ AMBULATORY SENSITIVE CONDITION Discharges

CPC+ EXPENDITURES
CPC+ ER VISITS

ACO Measures
What advice do you have for other practices?
Confidential & Proprietary 20
Questions?
22Confidential & Proprietary
Contact Information
• Pete Atkinson, MHA [email protected]• Gary Bevill, MD [email protected]• Rachel Wallis, MPH [email protected]

11
Practice Transformation Part 2: Provider Engagement and Team-Based Care
Rachel Wallis, MPH
Executive Director Aledade, Inc.
Table of Contents
DRAFT:
Session Objectives
• Discuss best practices in provider engagement in team-based care
• Identify strategies for enhancing the care team
• Identify three action items to discuss with your team
Confidential &Proprietary 2

3Confidential &Proprietary
Today’s Speakers
• Dr.Gary Bevill,Physician with SAMA Healthcare• Pete Atkinson, Administrator with SAMA Healthcare• Rachel Wallis, Executive Director with Aledade Arkansas
4Confidential &Proprietary
Aledade/SAMA Partnership
Good forDoctors
Good forPatients
Good forSociety

SAMA Healthcare
Confidential &Proprietary 5
SAMA HEALTHCARE SERVICES• El Dorado, AR• 21,000+ active patients• EMR
• Allscripts Professional EHR• Open extended hours and
weekends• Technologically advanced• Same day appointments
available• Full Service: Lab, X-Ray, CT,
US, Bone Density, AllergyClinic, and Pharmacy onSite
BOARD OF DIRECTORS
Gary Bevill, MD
Matthew Callaway, MD
R. Eric Hatley, MD
HISTORY OF SAMA• Practicing
Independently• South Arkansas
Medical Associates
• SAMA HealthcareServicesestablished May 7, 1998

Interdisciplinary Teams &Physician Engagement
Confidential &Proprietary 9
10Confidential &Proprietary
Interdisciplinary Team Members
• What type of team members do you have on each care team?• How do they work together?
• Care ManagerWorkflow• Behaviorist Workflow
• How do physicians engage in this process?• How do patients react to this type of approach?
Board
Administrator
Business OfficeManager
HealthInformatics/Populati on Health
Physicians
Mid-LevelsNurseMan ager
Ancillary Manager
Nursing/ Phlebotomy
Lab/Radi ology
Business Office
SAMA HEALTHCARE SERVICESHIERARCHY
MANAGEMENT TEAM
Elaine Butler, RN
Jan Risinger
Terri Townley

PRACTICE IMPROVEMENT TEAMBoard
Pete, ADM
Nancy, Health
Informatics
Susan, Population
Health
Elaine, Nurse
Manager
Terri, Office Manager
Misc
SUSAN TAYLOR, RN - POPULATIONHEALTH
ACOAWVs
NANCY NEW, LPN - HEALTHINFORMATICS/IT
CLINICAL SUPPORT STAFF
Elaine Butler, RN Nurse Manager
Candy Cates, LPN
Lindsay Lee,LPN
Austin Collins, LPN

CLINICAL WORKFLOW PROCESSPre-visit Planning-
Identify Care Gaps
Insurance Verification
Patient Check-InCollect Copay
Vitals/CC/Hx/VerifyMeds/Room Patient
Execute CareGaps/Standing
Orders
Provider sees patient
Provider entersadditional orders/
referrals/eRxmedications
Follow-upAppointment
scheduled Additionalorders executed
Patient Check-Out
CC schedules referral& contacts patient
Referral coordinatorreceives specialist
note & closes referralloop
Provider notifiesnurse of results forpatient contact
TEAM STAFF NURSE(LPN)Patient Triage
Appointment Scheduling
Phone Calls, Web
Messages, Refills
Notification ofTest Results
Fulfillment of Provider Orders

CARE COORDINATOR (LPN)
Pre-Visit Planning—
Communicate Gaps in Care
PriorAuthorizations
Referral Coordination
CARE COORDINATORS
Amanda Dickson, LPN
Lorrie Rapp, LPN
Yolanda Moody, LPN

CARE MANAGER (LPN)
Episodic/Longitudinal Care Management
Coordinate Weekly Team Huddle
Structured Proactive Phone Calls
Hospital/ERDischargeFollow-Up
CARE MANAGERS
Beverly Smith, LPN
Karen Wooten, LPN
Lindsay Cranford, LPN
Teresa Sherman, LPN

BEHAVIORAL RESOURCES
Heather Story, LPC
Mark Clark,Psychologist
TEAM SAMA
Physician
APRN/PA
LPN LPN
CareManager
CareCoordinatorLPN

ORANGE TEAMDr. Gary Bevill
AmbrosiaMisenheimer,APRN
ChristinaNavarette, LPN
Anne MichelleColeman, LPN
Beverly Smith, CareManager
Lorrie Rapp, CareCoordinator
SophieBurgie, LPN
Teresa Sherman,CareManager
BLUE TEAM – LIFESTYLE MEDICINE
James Sheppard,MD
HannahRuiz, LPN

PEDIATRICS
Christy Buhrman,APRN
Kristi Rogers, LPN
PHLEBOTOMY
Janna Doss
Breana Downs
Kayla Forbes

LABORATORY
Jan Risinger, Ancillary Manager
Sheila Elmore, MT
Leslie Darden, MLT
Angela Shackleford, MLT
RADIOLOGY
Jan Risinger, Ancillary Manager
Shannon Kooms, RT(R)(CT)
Jenny Hoggard, RT(R)
Jessica Dawson, RT(R)
Lori Dodson, RT (R)
FRONT OFFICE (CHECK-IN)
Morgan Mitchell
Courtney Ray
Terri Kilby
BUSINESS OFFICE
Terri Townley, Manager
Emma Wood
Karen Miller
Sherron West
Brooke Rhoades
Melissa Smith
Katie Richard
ReferralCoordinator
ADMINISTRATION
Pete Atkinson, Administrator
Carlee Smith, AdministrativeAssistant
Donna Bevill, Accounting
Outcomes
Confidential &Proprietary 34

SAMA’S OUTCOMES
• Change in physician practices• Change in APRN practices• Change in accessibility• Change in continuity of care
CPC+ ACUTEINPATIENT
DISCHARGES

CPC+ AMBULATORY SENSITIVECONDITION DISCHARGES
CPC+EXPENDITURES

CPC+ ER VISITS
ACO MEASURES

-S-A-M--A-are \n\t \at ive
. -o'-''\H E A L T H C A R E -
s2017<::v<§'
Administration
c Business Office
Lab
Radiology
What advice do you havefor others?
Confidential &Proprietary 42

QUESTIONS?
44Confidential &Proprietary
Contact Information
• Pete Atkinson, MHA [email protected]• Gary Bevill,MD [email protected]• Rachel Wallis, MPH [email protected]

12
Opiate Prescribing and Use of the PDMP System
Jennifer Roberts, MS
Assistant Director Department of Pharmacy
UAMS
Table of Contents

13
Case-Based Vaccine Update: Shingles, Pneumococcal and Adolescent
Robert Hopkins, MD
Professor of Medicine and Pediatrics Department of Internal Medicine
UAMS
Table of Contents

Case-Based Vaccine Update:Shingles
PneumococcalAdolescent
Robert H. Hopkins, Jr., MD, MACP, FAAPProfessor of Internal Medicine and Pediatrics
UAMS College of Medicine
COI Disclosure
• I am employed by UAMS and currently serve as an appointed member of a number of local and national vaccine-related organizations. I have a science-based bias that vaccines are beneficial, underutilized, and should be more consistently used to protect us and our patients.
• I have no financial conflicts of interest.

Objectives
• Shingles vaccination• Why• Which• How
• Pneumococcal vaccination• Why• Which• How
• Adolescent immunization• Why• Which• How
ACIP 2018 Adult Schedule [Tip of iceberg: handholds are in footnotes!]
https://www.cdc.gov/vaccines/schedules/hcp/adult.html
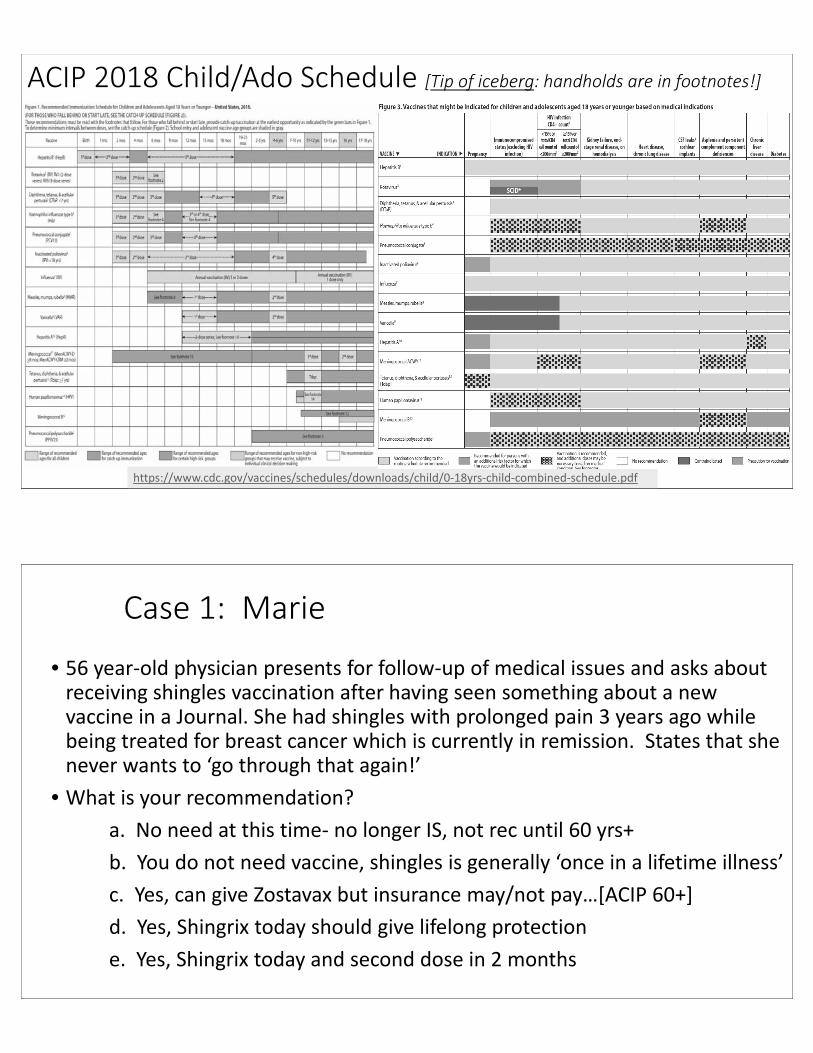
ACIP 2018 Child/Ado Schedule [Tip of iceberg: handholds are in footnotes!]
https://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-child-combined-schedule.pdf
Case 1: Marie
• 56 year-old physician presents for follow-up of medical issues and asks about receiving shingles vaccination after having seen something about a new vaccine in a Journal. She had shingles with prolonged pain 3 years ago while being treated for breast cancer which is currently in remission. States that she never wants to ‘go through that again!’
• What is your recommendation?a. No need at this time- no longer IS, not rec until 60 yrs+b. You do not need vaccine, shingles is generally ‘once in a lifetime illness’c. Yes, can give Zostavax but insurance may/not pay…[ACIP 60+]d. Yes, Shingrix today should give lifelong protectione. Yes, Shingrix today and second dose in 2 months

Shingles= Herpes Zoster
• Results from reactivation of varicella-zoster virus • ~ 99.5% of US adults aged > 40 years susceptible• >1 million cases in the United States every year• 20% of cases in people 50-59 y/o• >50% of cases occur in those aged >59 years• Frequency, severity increase with age
7
Oxman MN et al; Shingles Prevention Study Group. N Engl J Med. 2005;352(22):2271-2284; Wood MJ, Easterbrook P. Shingles, scourge of the elderly.
In: Sacks SL, Straub SE, eds. Clinical Management of Herpes Viruses. Amsterdam, The Netherlands: IOS Press; 1995:193-209; Jung BF et al.
Neurology. 2004;62(9):1545-1551; Levin MJ et al; Veterans Affairs Cooperative Studies Program Shingles Prevention Study Investigators. J Infect Dis.
2008;197(6):825-835.
Image
Graphic
Shingles• Risk: correl. w/ varicella-zoster virus-specific T-cell mediated immunity (VZV-CMI)
• NOT with Varicella-Zoster antibody presence, absence or levels…
• Major clinical factors: age, immune compromise [conditions (IC) or treatment]• Age and IC increase both rate and severity of zoster • Additional factors:
• Female sex• White race• Physical trauma in involved dermatome• Family history• IL-10 gene polymorphism
• PHN: Post-herpetic Neuralgia = Primary complication• Can occur before, during, and after rash • More frequent/severe w/ older age [> 90% of those >50 years experience pain (40% severe)]• Why? As age ^^, VZV-CMI at the time of HZ slower to amplify and stop spread of infection ->
greater damage to ganglion -> more persistent pain
8
Cohen JI. N Engl J Med. 2013;369(3):255-263. Johnson RW, Rice AS. N Engl J Med. 2014;371(16):1526-1533.
Drolet M et al. J Pain. 2010;11(11):1211-1221. Benbernou A et al. Eur J Pain..

Complications of Shingles
9Gnann JW Jr, Whitley RJ. N Engl J Med. 2002;347(5):340-346; Arvin AM. Clin Microbiol Rev. 1996;9(3):361-381;
Moriuchi H, Rodriguez W. Pediatr Infect Dis J. 2000;19(7):648-653.
TableImage
Shingles Vaccination
• ACIP Recommends RZV for all adults 50+ [Option: ZVL at age 60+ if not immune compromised]
• Two Vaccines:• ZVL: Zostavax- Live virus vaccine FDA licensed 50+, 1 dose SQ, ACIP recommended 60+
• 50-60% efficacy, lasts at least 5-6 years• RZV: Shingrix- Adjuvanted subunit vaccine. FDA licensed/ACIP recommended 50+
• 2 Doses IM: Initial and 2-6 months later• PREFERRED over Zostavax and recommended in those who had ZVL at least 2 months ago• 90+% efficacy• Aduvanted= More local reactions/pain at injection site but most in trials completed trial…
• Implementation:• Persons with prior ZVL: Recommend RZV (Shingrix), start at least 2 mo after• Shingles vaccine IS indicated in those with prior Shingles • Immune suppressed, 50+ years: Recommend RZV, 2 doses • There is modest data on RZV, ZVL in 80+ years population vs. 50-70 years of age.
https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/shingles.html
There is no evidence for a specific interval.
Shingles Vaccine: Systems-Based Practice 2018
• Shingles vaccination is “A” recommended by ACIP• PRIVATE INSURANCE: Covered with no copy
• Every patient for whom ACIP recommends it [ACA Requirement].• As long as you are an empaneled provider on patient’s plan…
• MEDICARE: Shingles vaccines NOT Covered under Part A/B • Covered by Medicare Part D [Drug benefit] with variable patient deductible• For most Medicare patients, best coverage/lowest cost by vaccination thru
Pharmacy.• MEDICAID: ZVL [Live Shingles vaccine] not covered by Arkansas
Medicaid. • I have not yet heard back on my inquiry about RZV
RH Looking forward: Shingles and Vaccination
• ZVL likely to fade from use in US with introduction of/recommendations for RZV
• Unless vaccine can be altered to improve efficacy… OR• Unless cost reduced or ‘special deals’ with insurers/health systems…
• Those immunized against varicella and without ‘wild type’ infection• Should not be at risk for Shingles or need vaccine…• Will likely affect immunization recommendations in future…
• We can expect to see Shingles become an uncommon disease in US in the next 20-30 years with ongoing childhood varicella vaccination and adult zoster vaccination (despite our aging population).

Case 2: Joseph
• 40 year old plumber to establish care after prior MD left the community. He smokes ½ PPD cigarettes, is overweight and has intermittent episodes of ‘bronchitis.’ He takes no Rx medications but does take Naproxen OTC 2-3 times a week for knee and back pain. He received influenza vaccine in the fall and Tdap in 2015.
• Which of the following Pneumococcal vaccines do you recommend for Joseph?a. Pneumococcal conjugate [PCV13] todayb. Pneumococcal conjugate [PCV13] today and Polysaccharide [PPSV23]
in 8 weeks c. Pneumococcal polysaccharide [PPSV23] todayd. Pneumococcal polysaccharide [PPSV23] today and Conjugate [PCV13]
in 8 weekse. Pneumococcal polysaccharide [PPSV23] today and Conjugate [PCV13]
in 1 year
Case 2b: Joseph [2 years later]
• Joseph has had a rough last 6 weeks… he was in MVA and had to have emergent abdominal exploration with splenectomy and ORIF of femur fracture. He is here for hospital DC followup. Unfortunately, DC Summary does not indicate any immunizations were given in the hospital. Your nurse has also pulled ADH WebIZ data which shows no vaccinations except for influenza since you last saw him and gave PPSV23 [2 years ago].
• Which of the following Pneumococcal vaccines do you recommend for Joseph?a. None today- he received PPSV23 in the past 2 years. Needs PCV13 in 3 years.b. Pneumococcal conjugate [PCV13] today and Polysaccharide [PPSV23] in 8 weeks c. Pneumococcal conjugate [PCV13] today and Polysaccharide [PPSV23] in 3 yearsd. Pneumococcal polysaccharide [PPSV23] today and Conjugate [PCV13] in 8 weekse. Pneumococcal polysaccharide [PPSV23] today and Conjugate [PCV13] in 1 year

Pneumococcal [GNB] Pathophysiology
15Henriques-Normark B, Tuomanen EI. Cold Spring Harb Perspect Med. 2013;3(7). pii: a010215; van der Pol T, Opal SM. Lancet. 2009;374(9700):1543-1556.
Airborne Droplets
COUGH
SNEEZE
Nasopharyngeal Colonization
Asymptomatic Colonization
Auto-Inoculation
OtitisMedia
Sinusitis
Meningitis
HematogenousSpread
Blood-Brain Barrier
Aspiration
Bacteremia/ Septicemia
Pneumonia
Childhood PCV and IPD: Adults
16Centers for Disease Control and Prevention. Surveillance and reporting. https://www.cdc.gov/pneumococcal/surveillance.html. Accessed April 21, 2017.
RH Message: Herd immunity works… Introduction of each pneumococcal vaccine has reduced IPD both in population vaccinated and in community as a whole…

Pneumococcal Immunization… Is Hard!!• Recommendations are complex
• 2 Vaccines: 13 and 23 serotypes• Doses: PCV13 only 1 adult dose; PPSV23 up to 3 adult doses • 3 Critical Intervals: 8 weeks, 12 months, 5 years• 3 Risk Groups: AVERAGE, INCREASED, HIGH• FDA and ACIP: NOT in (complete) agreement
• Evidence for PCV13 and PPSV23 is individual• No trial data published on combined strategy• Both vaccines reduce IPD
• CDC: “Vaccination rates are unacceptably low…”
17
Adult Pneumococcal Immunization
HIGHEST RiskImmune compromise [IC], ‘anatomic risk’, adults aged 65+ years
INCREASED RiskSmokers, chronic medical conditions –not immunocompromised
AVERAGE RiskYoung [< 65 years], NO chronic medical conditions
18
NO
NO
PCV + PPSV23
PPSV23 ONLY
NO PNEUMOCOCCAL VACCINE

1919
Pneumococcal ‘Boosters’
• Only adults who have a BMT or stem cell transplant [e.g. immune system reset]should receive >1 dose of PCV13 (special circumstance outside scope of this talk)
• PPSV23• Dose 1 before age 60 for Intermediate risk: No booster until/unless highest risk by condition or age• Dose 1 before age 60 for highest risk and risk continues:
• Booster [dose 2] in 5 years [If highest risk indication was cochlear implant or CSF leak, this is final dose]• Last booster [dose 3] after age 65 and at least 5 years after dose 2
• Dose 1 before age 60 for highest risk and risk resolved [Had cancer- treated, now remission, no Tx]: • Return to average risk- no further doses indicated until/unless highest risk
• PCV13 then PPSV23 at age 65+ [regardless of medical indication]: no further doses.

Specific Risk Populations• Diabetes:
• Intermediate risk for Pneumococcal disease [PPSV23] but also at risk for HBV• Hepatitis B vaccinati0n for all to age 60 and consider in those 60+= highly
underutilized• Renal Disease
• Stages 1-3: Intermediate risk for Pneumococcal disease= PPSV23• Stages 4-5, ESRD, Nephrotic Syndrome: Immune suppressed, highest risk= PCV13+
PPSV23• Also need Dialysis formulation [HD] Hepatitis B vaccination
• Splenectomy and Splenic Dysfunction [Hemoglobinopathy, etc.]• Highest risk for Pneumococcal disease= PCV13 + PPSV23• Also need Meningococcal and HiB vaccination [Encapsulated Gram Negative
Bacteria]• Cancer Patients
• Highest risk for Pneumococcal disease with active CA, CTX, XRT= PCV13 + PPSV23• Return to average risk if in remission and not on Immune Suppressing treatment• Hematologic Malignancy, Stem Cell TXP: Highest risk and pose special challenges…
RH Looking Forward: Pneumococcal Imm.
• CDC will release/publish data on effects of PCV/PPS combined adult strategy in the next 12-18 months
• This may lead to changes in current recommendations
• New invasive pneumococcal strains• We have already seen emergence of different Pneumococcal strains which are
not covered with current vaccines- leading to broader PCV combinations… • Note that different countries use different PCV combinations based on strains
causing most/most severe disease in their populations
• PPSV23 has been in regular use in US since 1977… will this tool be supplanted by newer and more powerful Pneumococcal vaccines?

Case 3: Armond
• 14 year old for HSE and pre-participation evaluation to participate in 7-on-7 this summer. He has been healthy other than occasional sprains/strains and a concussion/MTBI last baseball season from which he has recovered completely. School performance is good. He has no allergies, is on no meds. Your MA pulled WebIZ report: shows no immunizations since age 6 years but UTD at that time.
• Which of the following vaccinations is/are recommended for Armond?
a. HPV vaccinationb. Tdap vaccinationc. Meningococcal [MCV4] quadrivalentd. Meningococcal [MenB] type Be. [a, b, and c above]f. All of the above
Adolescent Immunization: ‘Segmenting for Success’
• 11-14 Years• Influenza AAA= All And Annual• HPV9 Only 2 doses required for series completion if given before age 15…• MCV4 Initial dose recommended at 11-12 years Required for 7th grade entry
Catchup dose OK to age 13-15 years• Tdap Recommended at 11-12 years Required for 7th grade entry
• 15-20 Years• Influenza AAA= All And Annual • HPV9 3 doses required if series started after 15th birthday.
Complete series for all girls to 26, boys to 21 [High Risk to 26]• MCV4 Booster dose recommended at 16 [catchup to age 18 years]
Dorm. residence, military barracks are high risk settings.• MenB Level B recommendation: Consider 2 dose series at 16-23 years for avg. risk
http://adecm.arkansas.gov/Attachments/LS-18-012--ADE_Immunization_Rules.pdfhttps://www.cdc.gov/vaccines/schedules/hcp/child-adolescent.html

Influenza -- Alll Annd Annnually !!!
• 1 dose for all who are >9 years of age. • 2 doses in kids 6 mo-9 yrs. first season immunized only
• Egg allergy is NOT a contraindication-Precaution in those with Anaphalaxis onlyCan use RIV in those at highest risk
• Multiple different vaccines: ACIP recommends Vaccinate! No missed opportunities!
Most patients= specific vaccine (as long as indicated) does not matter.Consider High Dose (hd) or Adjuvanted in Seniors (65+) if available, but do not wait! Evidence these are +/- better than standard.LAIV will be avail in 2018-19 for patients 2-49 yo who want a needle-free
vaccine option. [NOT recommended in patients with asthma.]
14http://www.cdc.gov/vaccines/recs/acip/downloads/mtg-slides-fe09/04-1-flu.pdf25
Image
Influenza vaccination: Egg allergy
• Egg allergy is NOT a contraindication to Influenza vaccination• Patients with hives caused by eggs may receive any flu vaccine in any setting• Patients with other reactions may also receive any flu vaccine but in a
medical setting under the supervision of a healthcare provider who can recognize and manage severe allergic reactions.
• Includes angioedema, respiratory distress, emesis, lightheadedness
• Only contraindication is previous severe allergic reaction to a flu vaccine• If you have it available, the Recombinant Influenza Vaccine [RIV= ‘Flublock’]
can be given to any of these individuals whom you consider at high risk.
https://www.cdc.gov/flu/protect/vaccine/egg-allergies.htm

Human Papilloma Virus (HPV)
• Large family of viruses (>120 types)• Most innocuous, including strain(s) which causes common skin warts• Vast majority clear spontaneously• Highest infection rate in teens-early 20’s. Nearly all in US have had HPV
infection…• > 40 types infect mucosal cells, genital/oral
• ~14 M inf/yr, 79 M infected people in the US at any time• Persistent infection with some high-risk (oncogenic) types leads to
cancer• HPV 16, 18 cause ~66% of cervical Ca (24,600) in women and most other HPV-
related Ca in men and women• Other HPV serotypes contribute to ~15% of cervical Ca (3,800)
• HPV 6, 11 cause genital warts
https://www.cdc.gov/hpv/hcp/need-to-know.pdf
HPV vaccine
• Since 2006, 56% decrease in new HPV infections in US (despite not great uptake)
• No significant decline in protection after 10+ years• No data on long-term outcomes
• Cancer screening [PAP] should continue as currently recommended
• This is a safe and effective vaccine millions and millions doses admin worldwide!
• Non-infectious virus-like particle + Aluminum colloid adjuvant, produced in yeast
• Currently only HPV9 available in USA [Strains: 6, 11, 16, 18, 31, 33, 45, 52, 58]
https://www.cdc.gov/hpv/hcp/need-to-know.pdf

HPV vaccination
• Can be given as early as age 9 years• Recommended for adolescents 11 - 12 y/o• Catch-up:
• Females 13-26• Males 13-21• Males 22-26 with risk factors including MSM, immune compromise
• < 15 y/o 2-dose schedule (0, 6-12 months)• > 15 y/o 3-dose schedule (0, 1-2, 6 months)• Immune compromised, HIV: Need 3 doses regardless of start
age
https://www.cdc.gov/hpv/hcp/need-to-know.pdf
We need to reformulate the debate about HPV vaccine…
• We have not learned enough from our past mistakes:• Mis-steps similar to universal HBV vaccine for adolescents in the
1990’s…Mandate ~~> ^^ resistance esp. for vaccines with perceived ‘moral
impact’• ‘STD prevention’– How dare you suggest my child would…
• Do NOT link HPV vaccine, ‘SEX’ in conversation• HPV vaccine is a CANCER PREVENTION VACCINE!
• Cervical cancer• Oropharyngeal cancers• Respiratory papillomatosis • Genital warts and pre-cancers• Anal cancers• Head/neck CA
https://www.cdc.gov/cancer/hpv/index.htm

Meningococcal Vaccine
Why:Protect against devastating invasive Meningococcal infections(Spread as depicted in Pneumococcal ‘Cartoon’ earlier in slide set)3 types:• MCV4: Quadrivalent meningococcal conjugate vaccine
(MenACWY) – Menactra® or Menveo®• MPSV4: Quadrivalent meningococcal polysaccharide vaccine• MenB: Serogroup B meningococcal vaccine
• 2-dose (Bexsero®, 0-1)• 3-dose (Trumenba®, 0-2-6) – may give 2 doses (0-6) in low-risk groups
https://www.cdc.gov/vaccines/vpd/mening/hcp/who-vaccinate-hcp.html
MCV4: ROUTINE 11-12 years, Booster at 16.RISK BASED
MenB: Level B Recommend at 16-18 (2 doses)RISK BASED
MPSV4: Teens= Use only if MCV4 not avail…
Meningococcal Vaccination – Risk-basedSustained Risk• HIV infection• Complement deficiency• Asplenia
• MenACWY x2 + q 5 yrs, and MenB
• MenACWY not to be given at the same time as PCV13
• Microbiology laboratory personnel
• MenACWY x1 + q 5 yrs, and MenB
Time-limited Risk• Defined outbreaks
• MenACWY (<56 y/o) or MPSV4 (>=56 y/o) or MenB
• Travelers to areas where meningococcal disease is hyperendemic (“meningitis belt” in Sub-Saharan Africa, Middle East)
• MenACWY (<56 y/o) or MPSV4 (>=56 y/o)
• Unvaccinated college students / Military recruits
• MenACWY x1 +/- MenB
https://www.cdc.gov/vaccines/vpd/mening/hcp/who-vaccinate-hcp.html

Td/Tdap—Focus on Pertussis
• Adolescents/Adults are reservoir for Bordetella pertussis• All are susceptible to ‘the 100 days cough’
• And potential complications [emesis, pneumonia, fractures, CNS bleeds, etc.]
• Herd immunity important to reduce illness across all ages, especially in crowded conditions• Most important, adults/adolescents are are primary source of infection for infants
• Infants have highest mortality
• Pertussis is highly communicable; cough/sneeze transmits via respiratory droplets • Persistent transmission for ≥6 weeks, with > 4 months of cough
• Effective antibiotics eliminate contagion but no proven effective symptom controllers…
• Incidence increasing since 1970s, likely >10x more than reported
33 CDC. Vaccines and Immunizations. http://www.cdc.gov/vaccines
Tdap Recommendations
• Tdap dose at 11-12 years of age ‘boosts’ immunity from childhood DTAP series• Single dose replaces 1 dose Td for all adults
• Except in pregnancy, only 1 Tdap recommended in adulthood• Optimal timing between 27 and 36 weeks gestation EACH pregnancy
• Maximize passive antibody transfer to fetus• No adverse outcomes seen with subsequent pregnancy administration• Immune response peaks 2 weeks after administration,
so consider giving to other family members BEFORE delivery
• Current recommendation for subsequent Td every 10 years
• Ongoing concern about effectiveness of current acellular pertussis vaccines • Reason for lower effectiveness is highly debated in ‘vaccinology circles’…
34
CDC. Vaccines and Immunizations. http://www.cdc.gov/vaccines
Sukumaran L et al.JAMA. 2015;314(15):1581-1587.

RH Looking Forward: Adolescent Immunization
• We have been using more and more combination vaccines and other tools to improve the effectiveness of vaccines- adjuvants, VLP’s, different production methodologies.
• I anticipate we will see broader development and use of combination vaccines in teens and children to improve immune protection and reduce need for multiple visits and complex vaccine schedules
• New more effective Pertussis vaccine? HPV vaccine with more types?• Vaccine development will be particularly critical in our worsening
crisis of antimicrobial resistance and in the face of potential pandemics…
The Yearly Toll of Vaccine-Preventable Diseases
36National Foundation for Infectious Diseases. Call to Action: Adult Vaccination Saves Lives.Bethesda, MD, 2012.

PostTest 1:
• Which of the following is NOT a major difference between the 2 Shingles vaccines [RZV= Shingrix and ZVL= Zostavax]?
a. Adjuvant b. Age at which vaccine is approved by FDA to be usedc. ACIP recommended age of administrationd. Contraindicated in immune suppressed patientse. Method of administration
PostTest 2
• Which of the following is most correct about evidence supporting the use of PCV13 and PPSV23 vaccines in adults?
a. PCV13 and PPSV23 have both been demonstrated to reduce all cause pneumonia in adults.
b. Evidence for benefits of PCV13 and PPSV23 is based on studies of each vaccine individually and not used together.
c. Epidemiologic studies have shown reduction in invasive pneumococcal disease with PCV13 but not with PPSV23.
d. Animal studies show synergy when Conjugate vaccine is given shortly after Polysaccharide but not the converse.

PostTest 3
• Which of the following is most correct about HPV vaccination?a. 3 doses of HPV vaccine are recommended for all children/
adolescents 9-21 years of ageb. 2 doses of HPV vaccine provide lasting immunity if given
before age 15 but 3 doses are required at age 15+c. 3 doses of HPV vaccine provide lasting immunity if given
before age 15 but only 2 doses are required at age 15+d. HPV vaccination is effective against all strains of virus in the
vaccine regardless of whether infection occurs before or after immunization.
Boston Medical and Surgical Journal 1910 Dec 22; 163(25):961
Let me please leave you with this thought from Sir William Osler, MD

Important Tools
https://adhimmreglive.arkansas.gov/webiznet/Login.aspx
https://www.stepsforward.org/modules/adult-vaccinations
https://www.standingorders.org/nurse-or-manager/

14
Practical Steps in Management of Fibromyalgia
Aaroop Haridas, MD
Assistant Professor Division of Rheumatology
UAMS
Table of Contents

Fibromyalgia/ Chronic Pain
Aaroop Haridas MD RhMSUSAssistant Professor
Division of Rheumatology UAMS
Disclosures
None

A 35-year-old woman with a past history of a car wreck 7 months ago, comes to the physician due to muscle and joint pains over her entire body for the past 6 months. The patient also experiences fatigue, mental slowness. Vital signs are within normal limits. On examination, she has tenderness to gentle palpation over the muscles of her neck, shoulders, and back. There is no synovitis. Laboratory results show normal electrolytes, complete blood count, erythrocyte sedimentation rate, and thyroid function.Which of the following is the best initial therapy to improve this patient's symptoms?A) Physical therapyB) Hydrocodone/acetaminophenC) NaproxenD) Low-dose prednisoneE) Methotrexate
A 40-year-old woman is evaluated during a follow-up visit for a 1-year history of medically unexplained symptoms. She reports shortness of breath, generalized pain, fatigue, arthralgia, nausea, headaches. She has been evaluated by multiple primary care and specialty physicians and has had more than 7 emergency department visits during this time; all studies have been normal. Trials of two different antidepressant medications were unsuccessful. Her quality of life has significantly declined over the past several years. Medical history is otherwise unremarkable. Medications are tramadol, albuterol and ibuprofen all taken as needed. The vitals and physical examination are normal.What is the most appropriate management of this patient1) Neuropsychological testing2) Physical therapy3) long acting benzodiazepine4) regular primary care visits

A 74-year-old man has a 2-month history of progressively worsening bilateral shoulder and hip pain. He currently has difficulty rising from a chair and reaching overhead because of the pain. He also reports fatigue, malaise, and stiffness lasting > 2 hrs. in his shoulders. He reports no other symptoms. He takes acetaminophen as needed for pain with little or no relief.On physical examination, the patient appears depressed. Temperature is 100.2 °F, blood pressure is 126/66 mm Hg, pulse rate is 72/min, and respiration rate is 18/min. BMI is 26. There is markedly limited range of motion of the shoulders and hips due to pain; strength cannot be adequately assessed. The remainder of the physical examination is normal.Laboratory studies- basic metabolic panel, complete blood count, liver chemistries, and thyroid-stimulating hormone level are normal. Which of the following is the most appropriate treatment?A Aspirin 81 mg/dB Ibuprofen 800 mg Q 8 hC Duloxetine 60 mg/dD Prednisone 15 mg/d
A 29-year-old woman is evaluated for increasing fatigue and diffuse pain of 6 months' duration. The pain becomes more severe for several days if she “overdoes it.” She reports chronically poor sleep and has difficulty concentrating at work. History is also significant for hypothyroidism, for which she takes levothyroxine. She takes ibuprofen as needed for the pain, which provides minimal benefit.On physical examination, vital signs are normal. BMI is 25. Tenderness to palpation of multiple muscle groups is noted. Muscle strength is normal. There is no joint swelling or rash. The remainder of the examination is normal.Laboratory studies, including complete blood count, chemistry panel, erythrocyte sedimentation rate, and thyroid-stimulating hormone, are normal.Which of the following is the most appropriate next step in management?
A Begin scheduled ibuprofenB Increase levothyroxineC Obtain an antinuclear antibody panelD Start an aerobic exercise program

ObjectivesDefine and diagnose the Fibromyalgia Syndrome.Discuss the various differentials and mimics of chronic widespread painDescribe various practical steps to manage Fibromyalgia in primary practice.
“Fibromyalgia” is the current term for chronic widespread musculoskeletal pain for which no alternative cause can be identified.Smith and Moldofsky in 1970 established the concept of fibromyalgia. The name change reflected the increasing evidence that there was no “-itis” (inflammation) in the connective tissues of individuals with this condition, but instead “-algia” (pain).The hallmark of this condition is diffuse hyperalgesia or allodynia.

Fibromyalgia
Chronic widespread pain associated with any one of the following
# Fatigue# Poor sleep# Cognitive problems

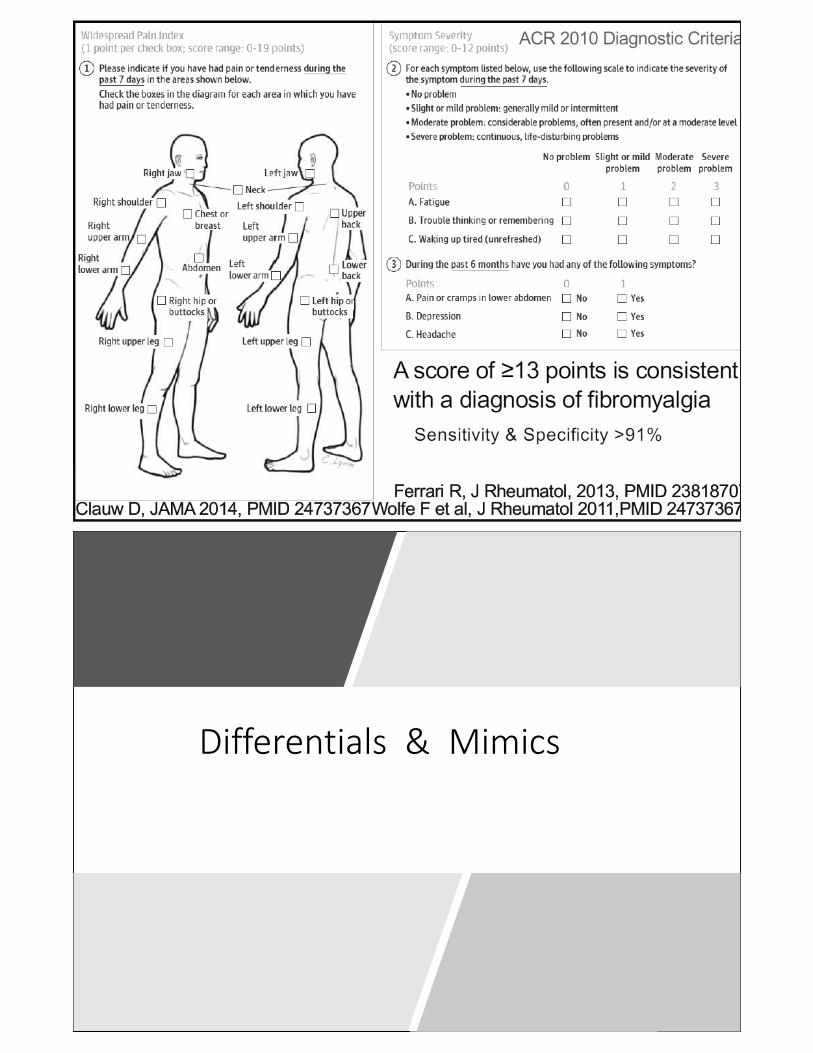
Differentials & Mimics

Differentials
Hypothyroidism, Steroid withdrawalVitamin D deficiencyUndiagnosed Sleep apnea, leading to worsening painChronic fatigue syndromeConversion disordersSomatoform disordersHepatitis C, HIVPolymyalgia Rheumatica Inflammatory disorders–inflammatory arthritis/ lupus/ myositisOsteoarthritis

Lab Testing in chronic widespread pain
CBC w/ diffComprehensive Metabolic PanelFasting GlucoseHepatitis B & CHIV RPRTSHB12, Folate levelsCK (useful, if objective evidence of muscle weakness present)Symptom directed work-up
What is missing in the above slide and why
No ANA testing- test only if suggestive features of SLEESR/CRP- does not point out a definite cause of underlying diseaseUric acid- not useful in the absence of a history of acute swollen jointRF- again not very useful in the absence of swollen joints.

Diagnostic labeling
Once a physician rules out other potential disorders, an important step in the management of Fibromyalgia is asserting the diagnosis.

Medications in FMS
The majority of clinical trials in FM have examined the use of antidepressants of one class or another. Tricyclic antidepressantsSerotonin reuptake inhibitors Atypical antidepressants- includes dual reuptake inhibitors

Medications in FMS
1. Amitriptyline, 10-30 mg at bedtime( TCA)2. Cyclobenzaprine, 10-30 mg at bedtime(TCA)3. Pregabalin, 300-450 mg/day (antiepileptic)4. Gabapentin, 1600-2400 mg/day (antiepileptic)5. Duloxetine, 60-120 mg/day(SNRI)6. Milnacipran, 100-200 mg/day(SNRI)7. Tramadol, 100-300 mg/day
Cannabinoids-There have been two randomized controlled trials examining the use of synthetic cannabinoids in FM (both using nabilone), and both studies concluded that the drug was efficacious (in one study for improvement of both pain and sleep, in the other study at a lower dose just for sleep improvement) Tizanidine (centrally acting 2-adrenergic agonist) approved by the FDA for the treatment of muscle spasticity associated with multiple sclerosis and stroke. Literature suggests that this agent is a useful adjunct in treating several chronic pain conditions, including chronic daily headaches and low back pain. Tramadol is a compound that has some opioid activity (weak μ agonist activity) combined with serotonin-norepinephrine reuptake inhibition. This compound does appear to be somewhat efficacious in the management of FM.
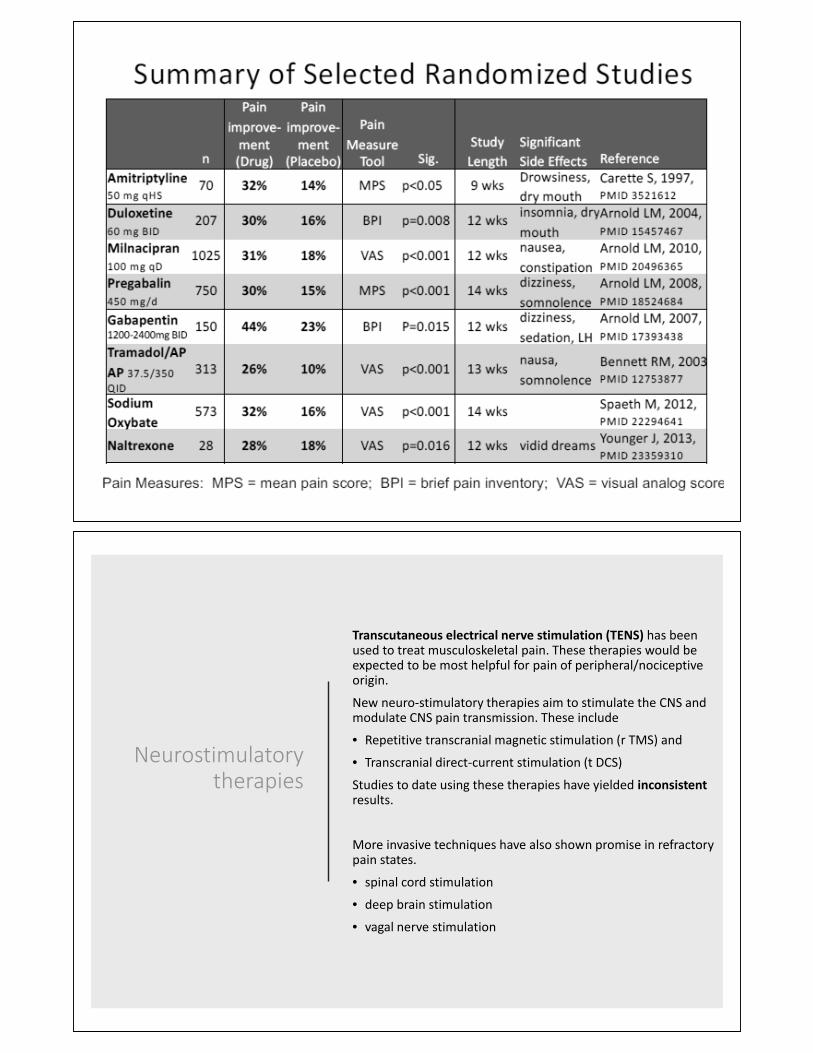
Neurostimulatory therapies
Transcutaneous electrical nerve stimulation (TENS) has been used to treat musculoskeletal pain. These therapies would be expected to be most helpful for pain of peripheral/nociceptive origin.
New neuro-stimulatory therapies aim to stimulate the CNS and modulate CNS pain transmission. These include
• Repetitive transcranial magnetic stimulation (r TMS) and
• Transcranial direct-current stimulation (t DCS)
Studies to date using these therapies have yielded inconsistentresults.
More invasive techniques have also shown promise in refractory pain states.
• spinal cord stimulation
• deep brain stimulation
• vagal nerve stimulation


Good Sleep

A self guide for patients- FFIBROGUIDE
https://fibroguide.med.umich.edu/

Interdisciplinary Pain Management
Summary
Fibromyalgia represents a condition of central sensitization to pain.Systemic disease should be excluded in patients with fibromyalgia.Making the diagnosis of fibromyalgia is important to limit unnecessary medical utilization.Fibromyalgia is manageable with a multidisciplinary approach.

END

15
ZZZ’s Without a Breeze: Sleep Apnea and OSA
Caris Fitzgerald, MD
Assistant Professor Department of Psychiatry and Sleep Medicine
UAMS
Table of Contents

ZZZs without a Breeze
Caris Talburt Fitzgerald, MDAssistant Professor of Psychiatry and Sleep Medicine
University of Arkansas for Medical Sciences
DISCLOSURES
None

Objectives
• Identify one easy screening tool for OSA
• List options for diagnosis of OSA
• Understand PAP machines and basic problem solving
• Identify and Discuss nonPAP OSA treatment options
Diagnosing Sleep Apnea
• AHI = (Apneas + Hyponeas) / Time
• PSG (Polysomnogram)• Good for ruling in or out sleep apnea
• Time is TST (total sleep time)
• Assessment of Supine and REM sleep
• HST or HSAT (Home Sleep Apnea Test)• Only good for ruling in sleep apnea
• Time is TIB (time in bed)

Definitions
• Hypopnea (exact definition matters!!!)• Decrease in the flow of air through the upper airway
for 10 seconds with a pathologic decrease in the oxygen saturation or abrupt arousal from sleep• AASM (3% Sa02 drop or arousal)
• Medicare (4% Sa02 drop)
• Apnea• Complete airflow obstruction through the upper airway
for 10 seconds, with continued ventilatory effort
Definitions
• AHI – (apnea-hypopnea index) number of apnea + hypopneas per hour of sleep
• RDI – includes events that don’t meet hypopnea definition, but result in arousal which causes increased respiratory effort (aka RERAs or Respiratory Effort Related Arousals) per hour• Greater than or equal to 5 is diagnostic of Sleep Apnea
Obstructive vs. Central Apnea
• Obstructive Sleep Apnea – airway is closing off while the body trying to move air
• Central Sleep Apnea – airway may be open, but the body is not pulling for air• usually due to opiates or heart failure, but also seen
with other neurological issues
• Can have a mixed picture especially with Opiates (very hard to get under control)• Take off Opiates
Cheyne-Stokes Respirations
• A pattern of breathing that oscillates between apnea and hyperpnea
• The body is trying to compensate for changing partial pressures of oxygen and carbon dioxide
• Seen in patients with stroke, CHF, brain tumor, traumatic brain injury (TBI), carbon monoxide poisoning,

Cheyne – Stokes Respirations
• www.egms.de/.../cto/2006-5/cto000034.f2.png
OSAIncidence, Signs, Symptoms
• 10-30% of patients without symptoms or risk factors
• Men > women overall (until Menopause)
• Higher BMI increases risk
• Family history increases risk
• Increasing age increases risk (also teeth matter)
• Comorbidites can be big clue!!! (snoring, htn, hld, DM, GERD/LPR,
insomnia, hypersomnia, fatigue, chronic pain, nightmares, nocturia, low testosterone or hypothyroid, morning HA)

Other OSASigns and symptoms
• Sometimes noticed when patient gets sedation
• Close call or accident due to sleepiness
• Memory problems/irritability/depression
• Insomnia/Hypersomnia
• Mixed Sleep Wake States (RBD, Parasomnia)
• Fighting between spouses about whether or not sleep occurred
• RLS type symptoms
STOP BANG
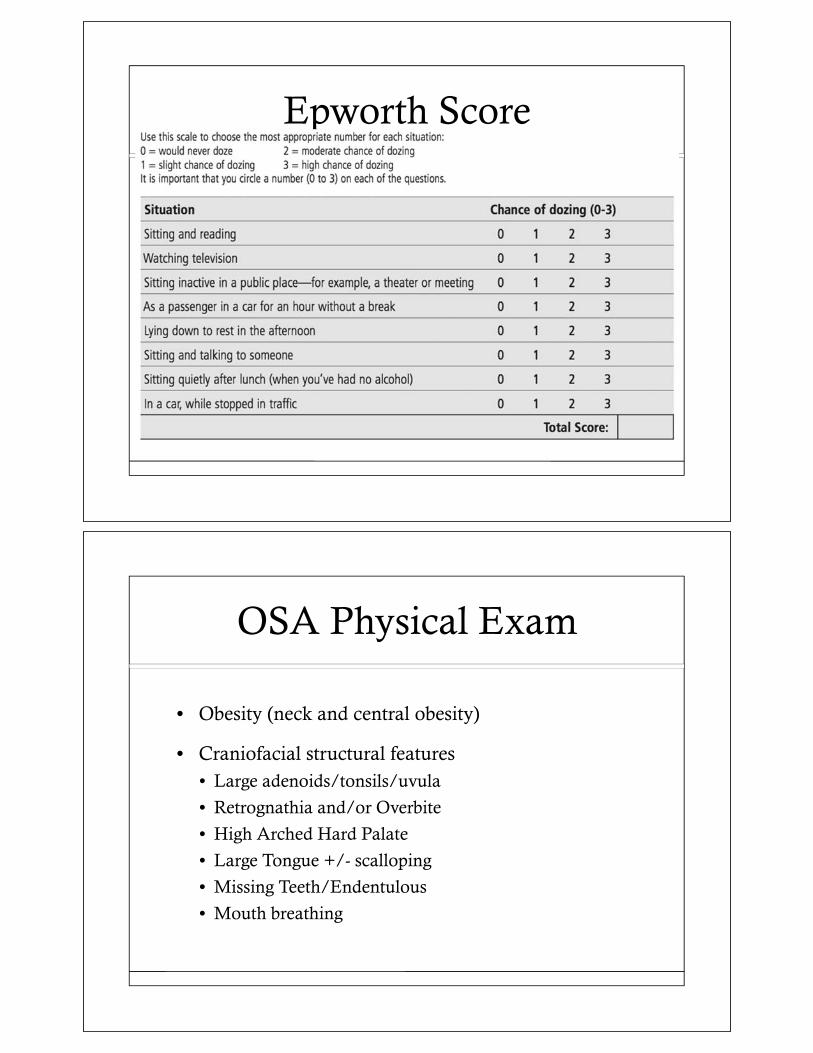
Epworth Score
OSA Physical Exam
• Obesity (neck and central obesity)
• Craniofacial structural features• Large adenoids/tonsils/uvula
• Retrognathia and/or Overbite
• High Arched Hard Palate
• Large Tongue +/- scalloping
• Missing Teeth/Endentulous
• Mouth breathing

Mallampati Score
Pt is not saying “Ahhh”
OSA Consequences
• Abnormal Physiology Results• Hypoxia/Hypercapnia and Reperfusion Injury
• Sympathetic Surges
• Increased Inflammation
• Thoracic Pressure Changes

OSA Long Term Complications
• Sudden Death (increased with EtOH, Opiates, Barbs, and Benzos)
• CHF, CVA, MI, Dementia
• Arrhythmias, especially Afib
• HTN, HLD, DM, Chronic Pain
• GERD/LPR
• Chronic Insomnia/Hypersomnia
• Depression/Irritablity
• Floppy Eyelid Syndrome
OSA Diagnosis
• Polysomnography (PSG)• “sleep study”

OSA Treatment CPAP or APAP
• Continuous Positive Airway Pressure• Delivers a fixed level of positive pressure to the upper
airway to act as a splint to prevent airway collapse, and therefore prevent apneas and hypopneas
• First line treatment for patients diagnosed with straightforward OSA (and have had a successful CPAP titration study)
• APAP used even more commonly these days
OSA Treatment BiPAP
• Bilevel Positive Airway Pressure• Inspiratory pressure is different than expiratory
pressure
• Helpful in very obese patients for true hypoventilation, and severe OSA not effectively treated with CPAP
• Sometimes is better tolerated than CPAP
• More advanced machine may incorporate a back up rate or deliver specific tidal volumes

OSA Management
• PSG
• If AHI >5 may result in PAP titration
• Sometimes can do a split night study –• If it’s so obvious in the first few hours that the patient
has OSA, CPAP titration can be done the same night
OSA Management
• After PAP titration, PAP is set up for home
• The patient has a meeting with the equipment supplier to find the appropriate mask, and is taught how to clean the mask, tubing and water chamber (for humidity)

OSA Mask options
• Nasal• Pillows
• Nonpillows
• Can use chin strap for mouth breathers• Overtime the mouth breather may or may not adjust to the
nasal mask
• Full face mask• Cover mouth and nose
PAP masks

PAP machines
OSA Treatment monitoring
• Should see the patient back in 4-6 weeks after setup to evaluate compliance and troubleshoot
• Detailed Download

OSA Troubleshooting
• Mouth Breathers give the most trouble• Everyone wants the smallest mask
• FFM• More surface area to seal
• Facial hair and lack of teeth can cause problems
• Poor mask fit technique can lead to air leaks
• Leaks Matter• Residual AHI (still have sleep apnea)
• Decreased Compliance
• Disrupted Sleep
• Dryness
OSA Treatment
• Avoid sedatives, narcotics, benzodiazepines and alcohol
• If the patient needs any procedures/surgery which require sedation, the patient should use their machine for 2wks prior and the MD should be notified to minimize the above meds
• Periodic Limb Movements of Sleep (PLMS) are often present, but resolve with use of effective PAP

OSA Treatment Alternatives
• PAP 90-95% effective
• Surgeries and Dental Devices• If you have mild OSA
• If you are a good candidate• Then you may see a 50% improvement in AHI 50% of the time
• WEIGHT LOSS!
• Sleep positioning for a small subset (tennis ball method)
• Medications do not work• It is a mechanical problem that requires a mechanical solution
Positional T-Shirt

OSA Surgical Options
• Bariatric Surgery
• Uvulopalatopharyngoplasty (UPPP) is being replaced• Removes tonsils, uvula, soft palate, adenoids, pharynx
• T&A
• Septoplasty with Turbinate Reduction
• Hypoglossal Stimulator
• Mandibular Advancement
• Tracheostomy – reserved for very severe cases; OHS (obesity hypoventilation) is usually also present
UP3
Image of Airway with UP3 performed

OSA Considerations
• Patient with little EDS are especially hesitant to use CPAP/APAP
• Even if a patient is aggressively trying to lose weight, it is important to treat in the meantime to prevent sequelae of complications (sustained HTN, etc.)• Also positive effects on leptin and grehlin
• DOT requires re-evaluation, and certification by Sleep MD that patient is compliant with PAP
OSA Considerations
• The Oxygen Delimma
• Desensitization• Wearing the machine while wide awake for 2hrs each
day back to back for 2wks• There is a significant adjustment period for some
patients
• OSA is more widely and publicly recognized now• Airports, etc.

OSA Conclusion
• THINK ABOUT SLEEP APNEA IN ALL PATIENTS!!!
SUMMARY
• HST is good for ruling in, not for ruling out OSA
• Surgery and dental devices success rates allow PAP to remain the gold standard, but have each have their place
• Settings matter and the enemy of PAP is leak and must be addressed if found in excess
• Detailed download and close follow up are needed for success

QUESTIONS
Caris Talburt Fitzgerald, MDAssistant Professor of Psychiatry and Sleep Medicine
University of Arkansas for Medical Sciences

16
When Counting Sheep Doesn’t Work: Insomnia and Sleep Medications
Caris Fitzgerald, MD
Assistant Professor Department of Psychiatry and Sleep Medicine
UAMS
Table of Contents

When Counting Sheep
Doesn’t Work
Caris Talburt Fitzgerald, MDAssistant Professor of Psychiatry and Sleep Medicine
University of Arkansas for Medical Sciences
DISCLOSURES
None

OBJECTIVES
• Identify best practices for the insomnia patient
• List meds and when to use them
• Understand Behavioral Treatments for Insomnia
TYPES INSOMNIA
• Acute Insomnia (Increased Arousal)• Any strong emotion (Happy, Sad, Worry, etc)• Acute substance abuse• Medication side effect
• Chronic Insomnia ( Decreased Sleep Drives plus or minus Increased Arousal)
• Maladaptive behaviors• OSA• Chronic substance abuse

ACUTE INSOMNIA
• Screen for sleep apnea before you handout a sedative!!!!• STOPBANG
• Insomnia/Hypersomnia is a natural and important response to trouble breathing during sleep. Do not use sedation in the setting of sleep apnea
• Otherwise acute insomnia of 1-3month duration is appropriate for a short time limited trial of medication
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonsits

PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos (GabaA)• NonBenzo Benzos aka “Z drugs” (GabaA)• Sedating Antidepressants (H1)• Antipsychotics (H1)• Melatonin Receptor Agonists (MT1and2)• Orexin Antagonist (OX1and2)
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines
• Lower Delirium Threshold/Impaired Cognition• Increased Daytime Sleepiness/Fatigue• Tolerance?
• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin (you produce plenty on your own!)
• May exacerbate phase advancement• Increased risk of depression
• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol (VERY DISRUPTIVE TO SLEEP)
• Metabolites greatly disrupt the latter half of sleep• Exacerbates reflux and primary sleep disorders
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos
• Lower Delirium Threshold/Impaired Cognition• Increased Daytime Sleepiness/Fatigue• Tolerance and Withdrawal (1-3mon w/ chronic use)• Fall/Hip Fx and Twice the risk of traffic accidents in Elderly
• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs
• Withdrawal Insomnia (1-2days)• Little to No Tolerance• Increased Parasomnias
• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists

BZRA PRESCRIBING GUIDELINES
• Use lowest dose possible
• Take while in bed with TV off
• Do NOT fight sleep
• Allow sufficient time for sleep
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants
• Trazodone (Priapism), Doxpein, Amitrip, Mirtazepine• Work mainly thru histamine• Daytime Sedation better at lower doses
• Antipsychotics• Melatonin Receptor Agonists• Orexin Antagonists

PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics
• Weight Gain, Hyperlipidemia, DM (Development of OSA)• Daytime Sedation• Increased Movement Disorders (Development of PLMD)• Black Box for Increased Risk of Mortality in the Elderly
• Melatonin Receptor Agonists• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists (Ramelteon)
• Does it work?• Avoid with Hepatic Impairment• Hyperprolactinemia
• Orexin Antagonists
PHARMACOLOGIC TREATMENT
• OTC• Antihistamines• Melatonin• Alcohol
• Rx• Benzos• NonBenzo Benozs• Sedating Antidepressants• Antipsychotics• Melatonin Receptor Agonists• Orexin Receptor Antagonists (Suvorexant)
• Does it work? Clinical expericences?
WHERE DOES THAT LEAVE US?
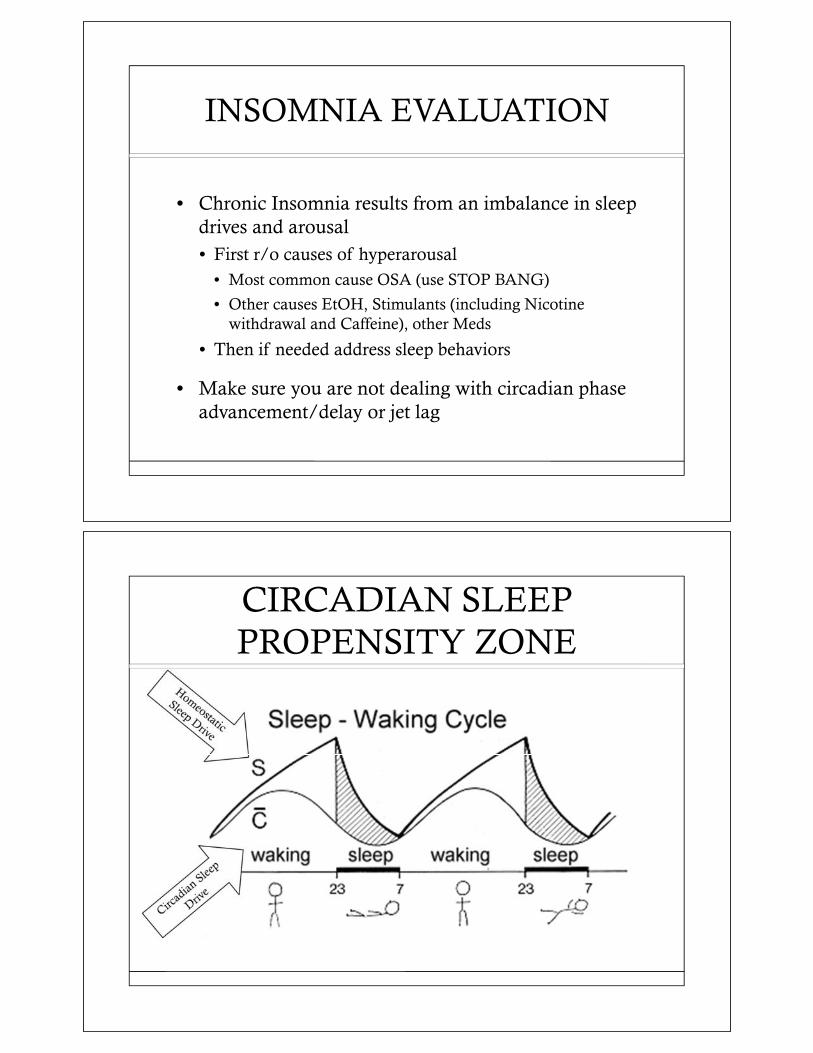
INSOMNIA EVALUATION
• Chronic Insomnia results from an imbalance in sleep drives and arousal• First r/o causes of hyperarousal
• Most common cause OSA (use STOP BANG)
• Other causes EtOH, Stimulants (including Nicotine withdrawal and Caffeine), other Meds
• Then if needed address sleep behaviors
• Make sure you are not dealing with circadian phase advancement/delay or jet lag
CIRCADIAN SLEEP PROPENSITY ZONE
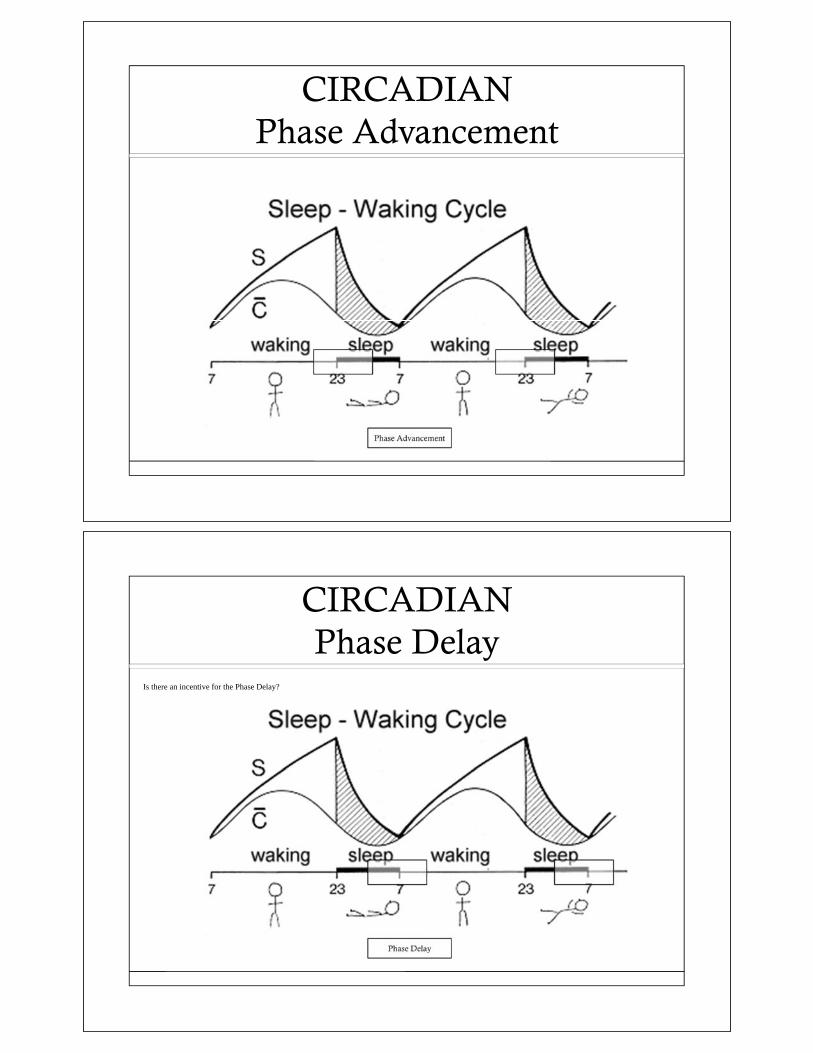
CIRCADIANPhase Advancement
CIRCADIANPhase Delay
Is there an incentive for the Phase Delay?

Circadian Sleep Disorders
Visual Sleep Diary

Actigraphy
Behavioral Treatments for Chronic Insomnia
• Sleep Handouts• Might as well throw them in the trash
• BBT-I (Brief Behavioral Treatment for Insomnia)
• CBT-I (Cognitive Behavioral Treatment for Insomnia)

EFFICACY OF CBT FOR INSOMNIA
EFFICACY OF CBT FOR INSOMNIA

Goal for Best Sleep
Goals for Best SleepAddress all at once!!!
HomeostaticSleeping InNappingLack of ExerciseCaffeine Intake
CircadianInconsistent Wake TimeBright Light Before BedExcess Time in Bed
OSA/UARSGERD/LPRSensory InputEmotionsMedsSubstancesExcess Time in Bed

Behavioral Therapy for Insomnia
You must take a multilevel approach!
COGNITIVE BEHAVIORAL THERAPY for INSOMNIA
• Dysfunctional Cognition• Worry over sleep loss• Rumination over
consequences• Unrealistic expectations• Misattributions/
amplifications
• Arousal• Emotional• Cognitive• Physiologic
• Consequences• Mood Disturbances• Fatigue• Performance impairments• Social discomfort
• Maladaptive Habits• Excessive time in bed• Irregular sleep schedule• Daytime napping• Sleep-incompatible
activities
Morin CM. Insomnia: Psychological Assessment and Management. New York, NY: Guilford; 1993

CBT-I Continued
• Sleep hygiene education• Specific behaviors will directly interfere with the ability
to sleep• The behaviors can be changed with education• NOT sufficient as a ‘stand alone’ treatment
• Sleep restriction therapy• Increased propensity to sleep by increasing homeostatic
sleep drive with partial sleep deprivation• Systematic reduction of time in bed to the amount of
total sleep time from sleep diaries• Increase time in bed by 15 minutes only when sleep
efficiency exceeds 90% after a certain time period
CBT-I Continued
• Stimulus control therapy• Assumes that there is a learned associated between
wakefulness and the bedroom• To break the cycle, the patient must not spend time
wide awake in the bedroom• Go to bed only when sleepy• Do not use the bedroom for sleep-incompatible
activities• Leave the bedroom if awake for more than 20 minutes• Return to bed only when sleepy• Do not nap during the day• Arise at the same time every morning

CBT-I Continued
• Relaxation training• Progressive muscle relaxation
• Guided Imagery
• Biofeedback
• Self-hypnosis
CBT-I Continued
• Cognitive restructuring
• Rational-Emotive therapy• “Men are not disturbed by things, but by the views
which they take of them”
• Specific techniques for rumination• Thought-stopping
• Meditation techniques
CBT-I Help Online
Pay for Help with http://www.myshuti.com/
Free Help at http://www.freecbti.com/sleepthoughts
SUMMARY
• Understand best practices for the insomnia patient• R/O OSA
• Use meds for acute insomnia
• If meds are not working gather more data and start the behavioral route
• Encourage patients to use meds wisely and do not sedate Sleep Apnea!!!
• Behavioral interventions can be very rewarding but require a comprehensive approach

QUESTIONS
Caris Talburt Fitzgerald, MDAssistant Professor of Psychiatry and Sleep Medicine
University of Arkansas for Medical Sciences

17
Common Tendon Disorders of the Upper Extremity
Mark Tait, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

18
Evaluation and Management of Numbness and Tingling in the Hands
John Bracey, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

Evaluation of Numbness and Tingling in theHand
John W. Bracey, MDMay 12, 2018
Who is this guy?• Orthopaedic trained hand
and nerve surgeon• Born and raised in
Arkansas• Hendrix College• UAMS: Med school,
Residency• OrthoCarolina: Fellowship• Clinical interest in
pathology/injuries to theperipheral nervous system

Outline
• Recall the anatomy of the upperextremity
• Identify the common causes ofnumbness and tingling in the upperextremity
• Describe the appropriate workup andinitiation of treatment for commoncauses of numbness in tingling in thehand
Upper extremity Anatomy• Peripheral nervous
system begins inthe cervical spineas the C5 – T1nerve roots
• Roots exit thespinal cord tocreate the brachialplexus andperipheral nervoussystem
C5C6C7C8T1

Sensory dermatomes
• Important to recognize thatsensory dermatomes canbe organized by peripheralnerves or nerve roots
Sensory dermatomes of the hand: PeripheralNerves
• Median nerve• Ulnar Nerve• Radial Nerve

Sensory dermatomes of the hand: Cervical Roots
• C6• C7• C8
Sensory dermatomes: Similarities and differences
• Overlap of C6/C7 withmedian nerve
• Overlap of C8 with ulnarnerve
• Median and ulnar nervesensation isolated to thehand
• Cervical root innervationextends much moreproximally to the neck

Carpal Tunnel Syndrome
• Common– 2.7% prevalence– 500,000 surgeries/year in USA
• $2 billion annual estimateimpact– Cranford et al. JAAOS 2007
What is the carpal tunnel?
• Passage way for themedian nerve and 9 flexortendons exiting theforearm and entering thehand
• The roof is the transversecarpal ligament
• Relatively tight space withinability to expand

What is CTS?• Median nerve compression at the
wrist– Chronic– Acute
• Compression occurs beneaththe transverse carpal ligament
• Impaired nerve microcirculationleads to symptoms– i.e. nerve ischemia
What cause CTS?• Increased tissue pressure carpal canal
– Static• Decreased space
– Distal radius malunion• Increased volume
– Hemorrhage– Infection– Mass
– Dynamic• Wrist position (2.5 – 30mmHg)• Fist

Risk factors for CTS
– Metabolic neuropathies• Diabetes• Hypothyroidism• Renal failure
– Fluid retention states• Pregnancy (20 45%)
– Female gender (3:1)– Obesity
Is work a risk factor?• Controversial• Many consider repetitive activities
with the hands to be a risk factor• Activities know to increase CT
pressure– Driving– Vigorous grasp– Operating heavy/vibrating
equipment• Computer use has not been show
to increase CT pressures– Stevens et al. Neurology 2001

Symptoms of CTS• Numbness in median
nerve distribution– Nocturnal– Often wakes patients
from sleep• Tingling• Pain
– Often described asburning or electric like
• Clumsiness• Weakness/muscle
atrophy– Thenar muscles
CTS Physical Exam• Tinel’s sign• Phalen’s test• Carpal tunnel
compression test• Sensation testing• Thenar strength
– Abductor pollicisbrevis
– Innervated byrecurrent medianbranch

Conservative management of CTS• Splinting
– Neutral wrist brace– Particularly helpful during sleep
• Stretching/Exercises• Ergonomic interventions• Steroid injection
• If patient fails initial attempts atconservative management considerobtaining a nerve study/EMG– Confirms diagnosis– Stratifies severity of the disease
When to refer to a hand surgeon?• Failed conservative
treatment• Significant
abnormalities onphysical exam– Widened 2 point
discrimination– Thenar atrophy and
APB weakness• Nerve study showing
moderate or severecarpal tunnel syndrome

Thank You

19
Common Causes of Shoulder Pain
Lawrence O’Malley, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

Common Causes of Shoulder Pain
Lawrence O’Malley, MD
Assistant Professor
Disclosures
None

Agenda
Common Shoulder Pathology
• Rotator cuff pathology
• Frozen shoulder
• Osteoarthritis of shoulder
• Shoulder instability
Treatment Options
Evaluation
Where are symptoms?
• Injury?
• What is specific location of pain?
• Duration?
• Weakness/Dysfunction?
• Does pain wake patient up at night?
• Numbness of arm/hand?
• Any treatment?

Differential Diagnosis
Shoulder Pain Rotator Cuff always!!
Cervical Pain, Radiculopathy
Arthritis (Glenohumeral, Acromioclavicular)
Adhesive Capsulitis/Frozen Shoulder
Calcific Tendinitis
Shoulder Instability
Rarer causes: Os Acromiale, Thoracic outlet syndrome, Brachial plexopathy/neuritis (Parsonage-Turner, etc.), Suprascapular Nerve Entrapment
Anatomy
Bony anatomy
• AC joint
• GH joint
• CC ligaments
• Labrum

Anatomy
4 muscles
connecting the
humerus with the
scapula
• Supplies stability and
balance to the
shoulder joint
• Proper rotator cuff
balance is essential
for raising arm and
rotation
Rotator Cuff Function
• Depresses humeral head
• Force couples
• Subscapularis and infraspinatus form the anterior and
posterior forces respectively to compress the humerus against
the glenoid.
• The deltoid forms the lateral force with lesser help from
supraspinatus

Clinical Presentation
• Lateral and/or anterior shoulder pain• Radiates distally towards deltoid insertion
• Anterior pain, biceps tendonitis
• Weakness, difficulty with outstretched activities or overhead lifting
• Night pain, cannot lie on that side
• Acute tear may have traumatic event
Physical Examination
• Inspection: atrophy, symmetry
• Palpation: AC, biceps, cuff tenderness
• Range of motion: active, passive (adhesive capsulitis)
• Strength: elevation, ER/IR power
• Provocative: impingement sign, Spurling’s test
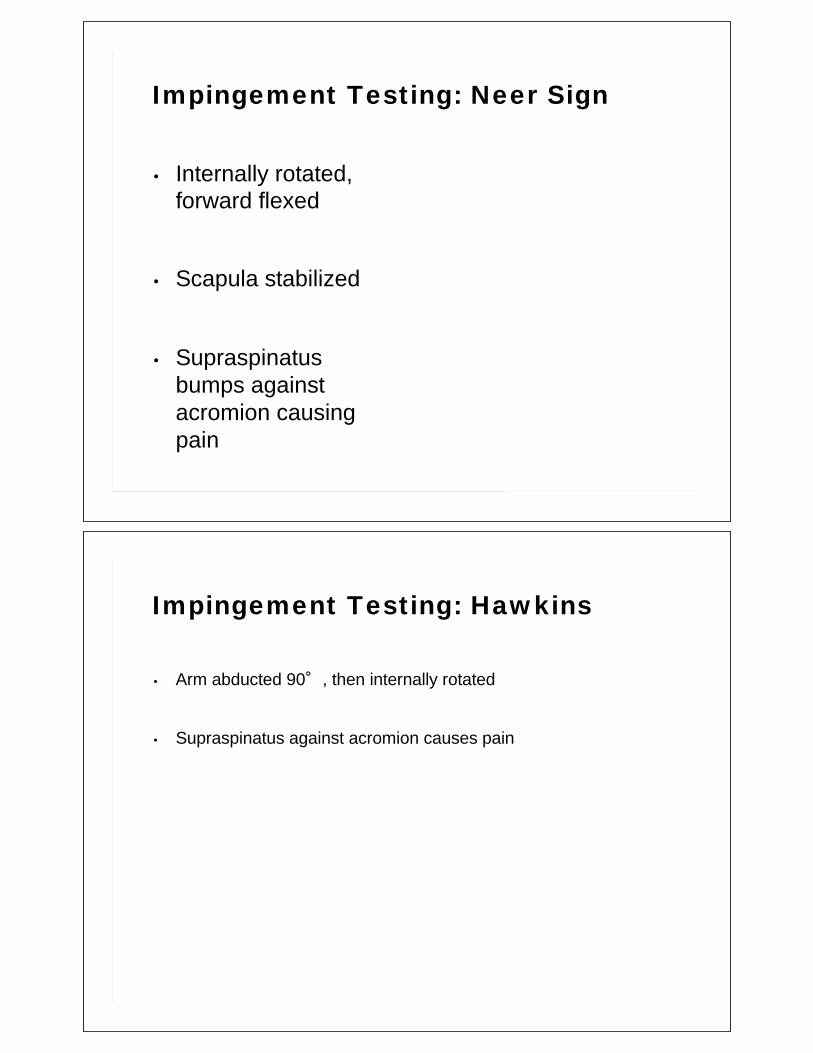
Impingement Testing: Neer Sign
• Internally rotated,
forward flexed
• Scapula stabilized
• Supraspinatus
bumps against
acromion causing
pain
Impingement Testing: Hawkins
• Arm abducted 90 , then internally rotated
• Supraspinatus against acromion causes pain

Rotator Cuff Strength Testing: Supraspinatus
Jobe's Test (Empty Can):• Arm Abducted in plane of
scapula
• Thumb down
• Elevation resisted
Rotator Cuff Strength: Infraspinatus
• Resisted ER with arm by
side
• Mostly Infraspinatus, some
teres minor

Rotator Cuff Strength: Teres MinorHornblower Test/Sign
Rotator Cuff Strength: Subscapularis
Lift off test:• Push hand away
from belt posteriorly
Bear Hug Test
Belly Press Test:• Push on belly, look
for elbow to dropbackwards

Biceps Clinical Tests
Speed’s test• FF 90, elbow 0, supinated forearm
• Resisted downward force
• Biceps or SLAP
Yergason’s test• Arm at side, elbow flexed 90
• Examiner resists supination
Acromioclavicular (AC) Tests
PalpationCross Body Adduction
• Flexion 90 , adduction

Scapular Winging
Wall Pushup
• Look for medial prominence
• Serratus Anterior
Imaging
X-RAYS ALWAYS FIRST!!!• Arthritis, fracture
• If arthritis, cuff repair not indicated, MR
may not be useful
• AP (calcific tendinitis, superior head
migration, impingement signs)
• True AP of glenohumeral Joint (Grashey),
eval for arthritis
• Scapular Y (acromial morphology)
• Axillary (os acromiale, subluxation/wear)

X-rays
Xrays
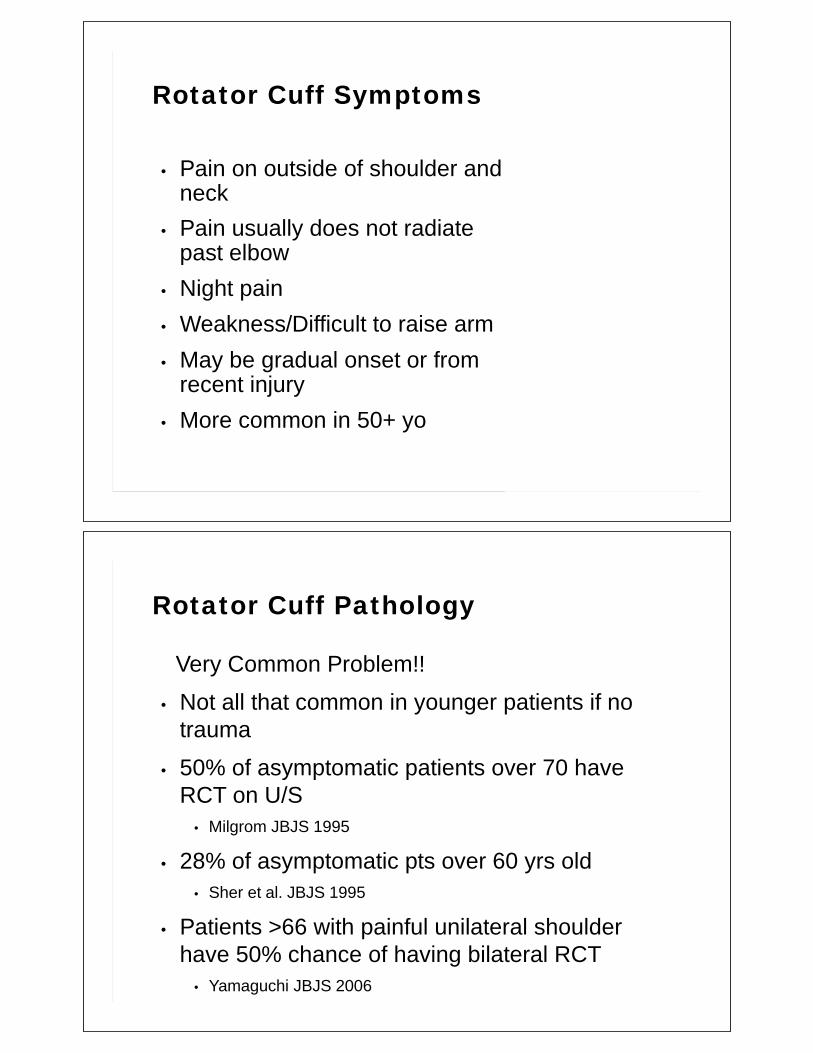
Rotator Cuff Symptoms
• Pain on outside of shoulder and neck
• Pain usually does not radiate past elbow
• Night pain
• Weakness/Difficult to raise arm
• May be gradual onset or from recent injury
• More common in 50+ yo
Rotator Cuff Pathology
Very Common Problem!!
• Not all that common in younger patients if no
trauma
• 50% of asymptomatic patients over 70 have
RCT on U/S
• Milgrom JBJS 1995
• 28% of asymptomatic pts over 60 yrs old
• Sher et al. JBJS 1995
• Patients >66 with painful unilateral shoulder
have 50% chance of having bilateral RCT
• Yamaguchi JBJS 2006

Spectrum of Rotator Cuff Problems
Rotator cuff Tendonitis
• Impingement
•Bursitis Rotator
cuff tears
• Partial thickness
• Bursal sided v Articular sided
• Full thickness
• Small v Large tears
Tendonitis
Rotator cuff tendonitis/biceps tendonitis
Overuse and inflammation
• Lateral or anterior(biceps) pain
• Mild swelling, morning tenderness, and
stiffness may also occur, but may improve with
use
• Usually a gradual onset
• Pain with rotator cuff strength testing
• Should not have weakness/disability

Tendonitis
Treatment
• Injections
• NSAIDS
• Physical Therapy• Home vs Formal
• Very important to restore normal motion
• Strengthening
• Literature
• Recent meta-analysis in therapy literature stated a home stretching and
strengthening program equal to injections and modalities• Abdulla et al. Manual Therapy 2015
Partial Thickness Rotator Cuff Tear
• Partial thickness tears
• Articular sided tears
• Throwers (internal impingment)
• Bursal sided tears
• Impingment of acromion
• Indications for surgery
• Bursal sided tears >3mm or 25% of tendon
• Articular sided tears >7mm of footprint or >50%
• Surgery
• Most likely will do an acromioplasty and repair cuff by making
full thickness tear or repairing in situ in articular surface tears

Partial Thickness Rotator Cuff Tear
Articular surface tear
Bursal sided tear
Rotator Cuff PathologyFull thickness rotator cuff tears
• Small (<1cm)
• Medium (1-3cm)
• Large (3cm)
• Massive (3cm+)

Rotator Cuff Pathology
Tears progress over time
• Asymptomatic tears progress 22% over 5 years
• Symptomatic tears progress 50% over 5 years
• Yamaguchi et al. JSES 2001
• Tears have fatty infiltration as they enlarge and
that fatty infiltration does not reverse after
repair
• Gerber et al. JBJS 2004
• Gladstone et al. AJSM 2007
Rotator Cuff Tear
• Non-op Treatment• Medications
• Injections
• ROM/Strengthening Therapy
• Operative Treatment• Arthroscopic/Mini-open
• Single v. Double row repair
• When to fix?• Failed non-op
• Traumatic full thickness tears
• Symptomatic partial thickness tears

Arthroscopic Rotator Cuff Repair
Rotator Cuff Tear
Healing
• Tendon healing is immature until 12 weeks from surgery
• Sonnabend DH et al. JBJS 2010
• Reformation of normal tendon bone connection takes 24 weeks after repair
• Koike Y et al. J Orthop Res 2005
• Smoking interferes with tendon healing• Galatz LM et al. JBJS 2006

Rotator Cuff Repair Outcome
• 26% Retear rate in all rotator cuff repairs
• 85% Clinical improvement all comers
• McElvany/Matsen AJSM 2014
• Younger patients 40-50yo have reliable good
results after rotator cuff repair
• Lin et al. Arthroscopy 2013
• MacKechnie et al. Arthroscopy 2014
• Younger patients healed better with rotator cuff
repair than older (>70)
• Moraiti Arthroscopy 2015
Rotator Cuff Tear
Rehab
• Passive ROM does not effect tendon mechanical properties after repair
• Peltz CD et al. JBJS 2009
• Recent studies show that early rehab improves motion but causes higher rates of recurrent tears in large tears
• Chang et al. AJSM 2015
• Rotator cuff strength recovery takes 6 weeks after tendon repair
• Trudel G et al. J Orthop Res 2009

Rotator Cuff Tear Rehab• Individualized to each patient
• Age
• Size of tear
• Tendon quality
• Repair quality
• Preoperative stiffness
• Larger tears• Less likely to get stiff long term
• Smaller tears• More likely to get stiff
• Start early PROM motion
Adhesive Capsulitis aka “FrozenShoulder”
Occurs when the capsule thickens or
decreases in size, restricting the joint
• Creates pain and stiffness in the
shoulder joint
• Limits ROM
• Insidious onset
• Most common in middle aged women
• Associated with diabetes and renal
disease

Adhesive Capsulitis
Stage one: The "freezing" stage may last from six weeks
to nine months the shoulder loses motion and pain
develops.
Stage two: The "frozen" stage is marked by a slow
improvement in pain, but the stiffness remains. Generally
lasts 4 to 9 months.
Stage three: The "thawing stage is when the shoulder
motion slowly returns toward normal and generally lasts 5
to 26 months.
Adhesive Capsulitis
• Exam – Limited in all range of motion• Especially in****ER***** and IR
• Very painful with ROM• Full strength of Rotator cuff• Make sure they do not have osteoarthritis on X-ray
• Abnormal Active and Passive PROM
• Normal xrays

Adhesive Capsulitis Rehab
• AAROM/PROM/AROM
• Gentle stretching
• Injection at the early stages of disease has
been shown to be very effective
• Frequent therapy
Adhesive Capsulitis Outcomes
• 90% of people get better with non-operative
treatment over a 2 year period
• 10% either need MUA + Capsular release
• Griggs et al. JBJS 2000
• Some studies have shown that MUA = to
Capsular release
• Patients continue to have good outcomes at 7
years post treatment
• Hugh JBJS 2012

Frozen Shoulder – Capsular Release
Osteoarthritis
• Pain all over the shoulder
• Pain with movement
• Loss of ROM
• May or may not have hx of
trauma in the past
• Rotator cuff intact
Non-Surgical Treatment
NSAIDs
• Meloxicam/ibuprofen/naproxen
• Steroid dose pack if cannot tolerate injection
• Creams(Voltaren)/patches
Injections
Non-Surgical Treatment
Therapy
• Try to restore ROM
• Strengthening of Rotator cuff
• Scapular positioning/posture

Total Shoulder Arthroplasty
• Replace glenoid with polyethylene
• Replace humeral head with hemishperical prosthesis and stem
into humeral canal
• Rotator cuff has to be competent
Total Shoulder Arthroplasty
Rehab
• Goal of therapy is to maintain and improve ROM and protect the
soft tissues
• Start early PROM
• Protect the subscap!
• Limit ER (max 30-40 degrees)
• 6-12 weeks
• Stretching/PROM
• AROM
• Isometric strengthing
• 12 weeks
• Formal rotator cuff strengthening
• Continue stretching if not to full ROM

Rotator Cuff Arthropathy
• Pain all over the shoulder
• Pain with movement
• Significant weakness of
rotator cuff (psedoparalysis)
• Migration of humeral head
superior
• Fatty infiltration exists in the
rotator cuff
• Loss of force couples at GH
joint
Rotator Cuff Arthropathy

Reverse Total Shoulder Arthroplasty
• Uses deltoid to power arm movement
• Prosthesis has the sphere fixated at the
glenoid/scapula and stem with polyethylene on the
humerus
Reverse Total Shoulder Rehab
• Patients are not as “stiff” as osteoarthritic
patients
• Will keep in sling for 6 weeks to let soft tissues
heal
• ROM will have limits due to constrained implant
• Limited ER and IR
• Good forward flexion can be optained
• Do not allow patient to push up from a chair
with arm

Shoulder Dislocation
• Fall onto outstretched arm
• Arm extendsà humeral head
dislocates anterior
• Anterior is by far the most common
direction of dislocation
• Posterior may happen in seizures
• Mostly in young active population
• May occur in older population after fall
• Can become recurrent problem
especially for younger patients
Labral Tears
• Acute dislocations
• Xrays to confirm shoulder reduced
• Sling for comfort
• Recommend referral to ortho
• Chronic instability
• Physical therapy
• Strengthen rotator cuff
• Failed PT
• Recommend referral

Dislocation Rehabilitation
• Immobilization?
• Initial immobilization for 1-2 weeks until patient is more
comfortable
• Rehab to restore ROM/Strength
• When to go back to play?
• Patient has to demonstrate the same strength as contralateral
side
• Full ROM
• No apprehension or recurrent instability
• Test patient in game like setting
• Use positional brace if possible (football)
SLAP Lesion
Superior labrum anterior to posterior tears
• Tears of the labrum or peel back of the biceps
anchor on the superior labrum
• Internal impingement – common in throwers
• Greater tuberosity impingement on the superior glenoid which
causes articular surface rotator cuff tears as well
• Posterior capsule/PIGHL gets tight as well
• Check passive ROM
SLAP Treatment
• Younger patients including throwers repair
SLAP lesion
• Be careful to not over constrain the biceps. It is meant to be
mobile in the throwers and overhead athletes
• Older patients biceps tenodesis is becoming
the preferred treatment
• Recent review showed that in patients over 40 biceps
tenodesis is preferred
• Erikkson AJSM 2015
Common things are very common
Impingement/bursitis• Positive Neer/ Hawkins
• Normal xrays
Rotator Cuff Tears• Weakness
• Normal Passive ROM
• Normal Xrays
Adhesive Capsulitis• Abnormal Active and Passive PROM
• Normal xrays
Osteoarthritis• Abnormal Active and Passive ROM
• Abnormal xrays


20
PCP Ortho Review: Knee Pain Diagnosis and Treatment
Mike Cassat, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

21
Ortho Review of Common Hip-Related Issues
Paul Edwards, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

University of Arkansas for Medical Sciences
Hip Pain Workup
Paul K. Edwards, MDHip & Knee Replacement
May 12, 2018
About Myself• Born & Raised: Fort Smith, AR
• Undergraduate: U of AR – Fayetteville
• Medical School: UAMS – Class 2005
• Residency: Univ. of South FL, Tampa, FL
• Fellowship: OrthoCarolina, Charlotte, NC
Adult Reconstruction – Hip & Knee Replacement

Hip Pain Outline
A. Epidemiology
B. History
C. Location
D. Clinical Exam
E. Imaging
F. Diagnosis
Treatment options
Epidemiology
Osteoarthritis
• Leading cause disability in US
• Affects 33% US adults
Post traumatic arthritis
• 12% of symptomatic OA

Epidemiology
Inflammatory Arthritis
• RA = 1.3 million
• JRA = 300,00
• SLE = 300,000
History
Two day history of mild hip pain
without injury.
Two months history of excruciating
hip pain with every step you take

History Location of Pain
1. Anterior Superficial Thigh
2. Anterior Deep Groin
3. “C-sign”
4. Lateral Greater Trochanter
5. Posterior
6. Unexplained Knee Pain
Location of Pain
– Radiate to the knee or below• Lumbar spine issues
– Lumbar spine pain w/u
– Localized• Meralgia Parasthetica
– Lateral Femoral Cut. Nerve– Rare (previous surgery)
• Anterior thigh pain or numbness - (superficial)

Location of Pain
• Anterior Deep Groin
• Osteoarthritis
• Avascular Necrosis
• Femoral Neck Fracture
• Stress Fracture – rarely seen on x-ray
• Septic Arthritis – SEVERE pain, + log roll
Location of Pain
• Anterior Deep Groin
• Point to the groin for hip
pain with ROM
• Always cautious to perform
hip replacement on anyone
that does not have groin
pain.

Location of Pain
• Anterior Deep Groin
• Osteoarthritis
• Avascular Necrosis
• Femoral Neck Fracture
• Stress Fracture
Location of Pain
Stress Femoral Neck Fracture

Location of Pain
“C-sign” Anterior / Lateral Groin
• Femoral - Acetabular
Impingement (FAI)
• Hip Labral Tears
Location of Pain
“C sign”
X-ray = wide joint space
Then MRI to assess for labral tear

Location of Pain
• Lateral
• Trochanteric Bursitis
– common
• Gluteus Tear – rare
without trauma
Location of Pain
• Lateral hip pain
– Trochanteric Bursitis pain can beexcruciating
– Rarely order MRI of hip
– If pain radiates below the knee –often LS issues and not Bursitis

Trochanteric Bursitis
• Non surgical
– Corticosteroid injection
• Use 21 gauge spinal needle
– NSAIDS
– PT, PT, PT
• ITB stretching is most
important
Location of Pain
• Posterior
• Lumbar Spine
• Sacroiliac Joint
• Piriformis Syndrome
• Gluteus Medius/Minimus Tear
• Hamstring origin avulsion / strain

Location of Pain
• Unexplained Knee Pain
• I examine every hip also with every knee exam.
• If stiffness / reduced ROM of the hip I will obtain
hip x-rays
Location of Pain
• Unexplained Knee Pain
• 1x per year – I take care of patient with persistent
knee pain after Total Knee Replacement
• Review x-rays before TKA – normal / minimal OA
• Hip x-rays – severe DJD / OA
• Solution = Total Hip Replacement

Hip Physical Exam
• Gait
• Leg length
• Hip ROM
• Provocative maneuvers and palpation
• Neurovascular exam
• Spine exam
Hip Physical Exam
• Gait
– Antalgic
– Abnormal
– Trendelenburg
– Use of walker, cane, assistive device?

Trendelenburg
Leg Length
EOS

Hip PROM
Special / Provocative
+ Pain = Intra-articular

FAI
“C - sign”
FAI

FAI
Hip Flexion Contracture

Lumbar Spine
Lumbar Spine
Straight Leg Raise

Hip Pain Imaging
Every hip pain patient gets x ray:
a) AP pelvis
b) Frog lateral
Hip Pain Imaging

Hip Pain Imaging
Normal AVN
AP
Hip Pain Imaging
Normal AVN
AP

Location of Pain
• Anterior Deep Groin
AVN – collapseOA
Hip Pain Imaging
Normal AVN – “Crescent Sign”
Frog Lateral

Hip Pain Imaging
Osteoarthritis AVN
Frog Lateral
Hip Pain Imaging
CT
• Not commonly ordered
• Femoral Neck Fracture
• AVN if unable to get
MRI
AVN
Femoral Neck Fx

Hip Pain ImagingT1 MRI without contrast
Hip Pain ImagingMRI
Labral Tear
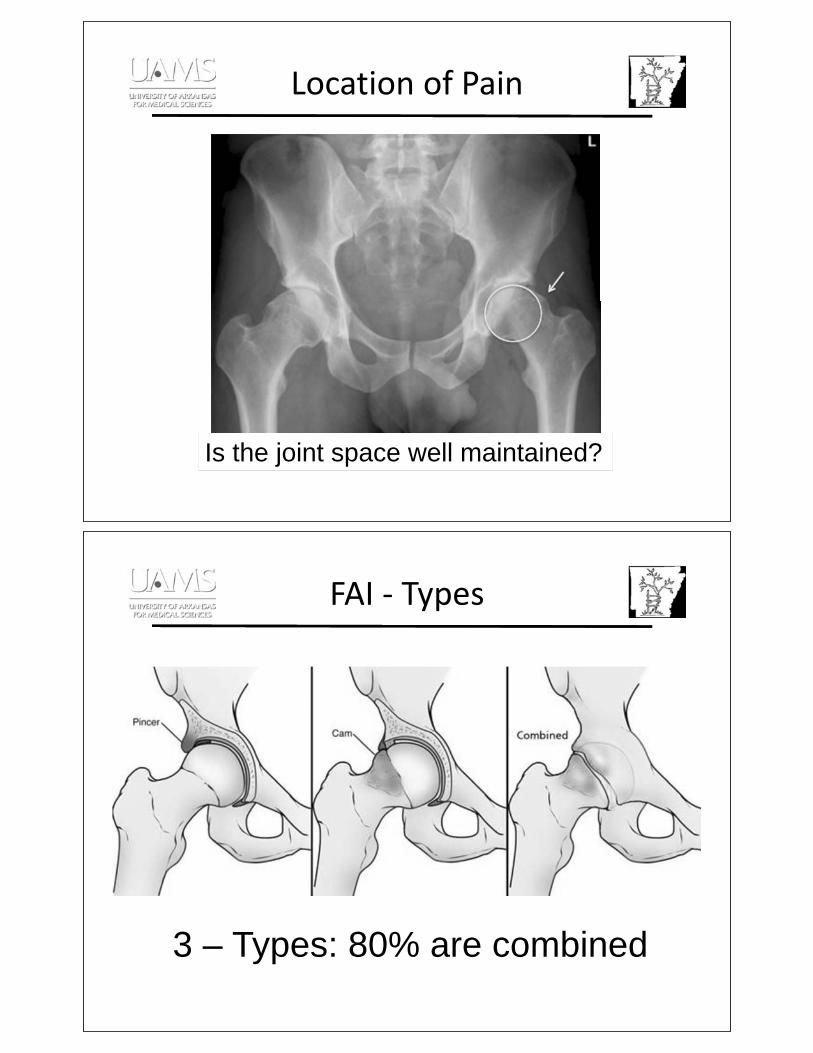
Location of Pain
Is the joint space well maintained?
FAI Types
3 – Types: 80% are combined

Location of Pain
FAI
Pincer – Type predominant
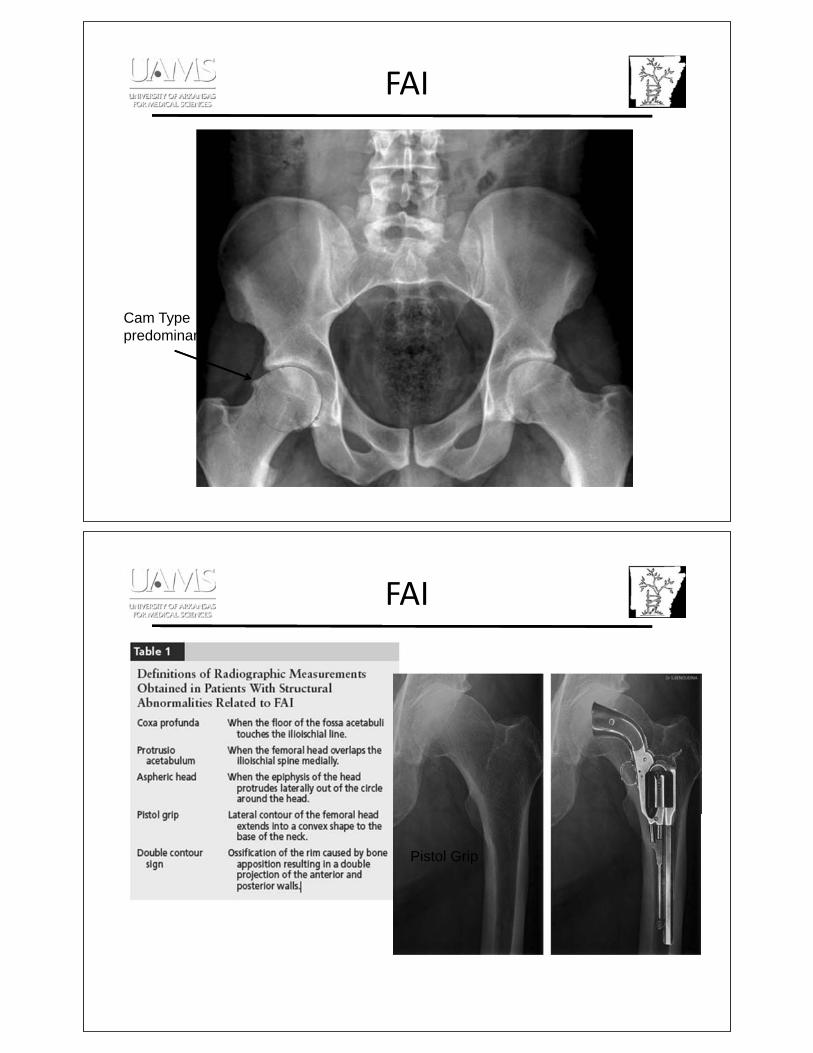
FAI
Cam Type
predominant
FAI
Coxa ProfundaProtrusio
Pistol Grip

FAI
Open surgical dislocation is gold standard80-90% successful results
Indicated unless:
• Tonnis 2
• 40 or older
FAI
Labral Tear

Hip Arthroscopy
• Not the gold standard
• Limited role in posterior FAI pathology
• Coxa profunda
• Protrusio
• Severe acetabular retroversion
• Obese patient
Caution when choosing Hip Scope as board answer
Satisfactory results can be obtained, and that the outcomes are comparable to those of the
open technique, although patient selection may play an important role in the outcomes
between these two groups.
FAI or OA?
Does not need MRI – patient needs Total Hip Replacement
65 yo with groin pain
MRI – bilateral labral tear
I need a hip scope
Diagnosis:OA

Dysplasia
• Locking, catching with groin pain
• Excessive femoral anteversion =
internal rotation gait
• Trendelenburg gait
• Anterior impingement sign
Dysplasia
Shentons Line

Dysplasia
CE Angle: < 25 degrees = dysplasia> 39 degrees = over coverage
Dysplasia THA
CROWE classification
% femoral head
superior migration
Avoid lengthening > 3.5 cm

AVN
60% Idiopathic
Insult / Injury:
1) bone death follows
2) reparative process
(creeping substitution)
3) reparative process
weakens subchondral
bone
4) collapse
AVN
Frog-Lateral x-ray
MRI is 98% sensitive and
98% specific.
Bone scan is 85% sensitive
and 80% specific with
accuracy 85%.

Hip Pain Imaging
• All patients with AVN – MRI of bilateral hip
• 80% incidence
T1 MRI
AVN
Non-arthroplasty
Arthroplasty

AVNNon-operative
1. Protected Weight Bearing – demonstrated failure rate of greater than
80% at a mean of 34 months and is not recommended as sole treatment.
2. Hyperbaric Oxygen, Extracorpeal shock – Not Recommended
3. Pharmacologic
i. Lipid lowering medications – potential?
ii. Bisphosphonates – potential?
Mont MA, Carbone JJ, Fairbank AC. Clin Orthop Relat Res 1996;324(324):169-178.
AVN
Arthroplasty – Gold Standard
• Total Hip Arthroplasty – High failure rates with cemented
implants, great success with uncemented acetabular and
femoral implants.
• Higher risks:
• Infection
• Dislocation
• Intraoperative bleeding
• Reoperation rate
Fye MA, Huo MH, Zatorski LE, Keggi KJ:J Arthroplasty 1998
Hungerford MW, Hungerford DS, Jones LC:Orthop Clin North Am 2009
Steinberg ME, Lai M, Garino JP, Ong A, Wong KL:Orthopedics 2008

Cases
OA #804452

OA #804452
OA #804452

Dysplasia #1005907
CROWE ?
Dysplasia #1005907
CROWE ?
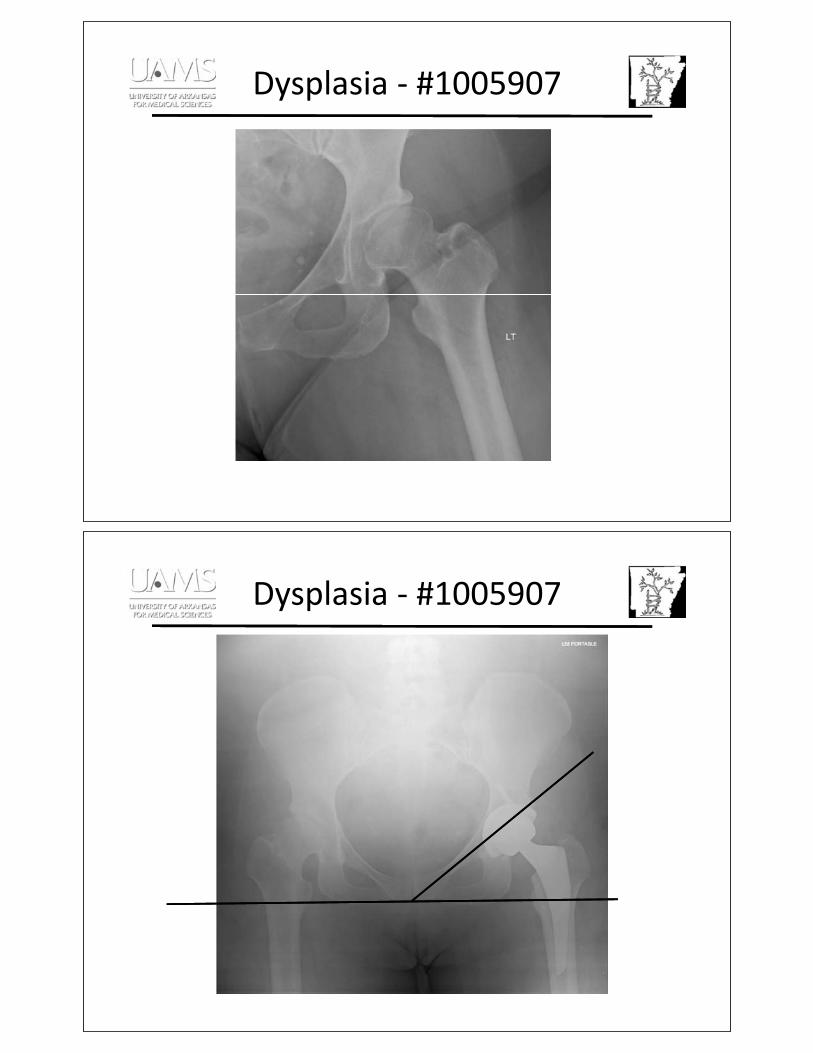
Dysplasia #1005907
Dysplasia #1005907
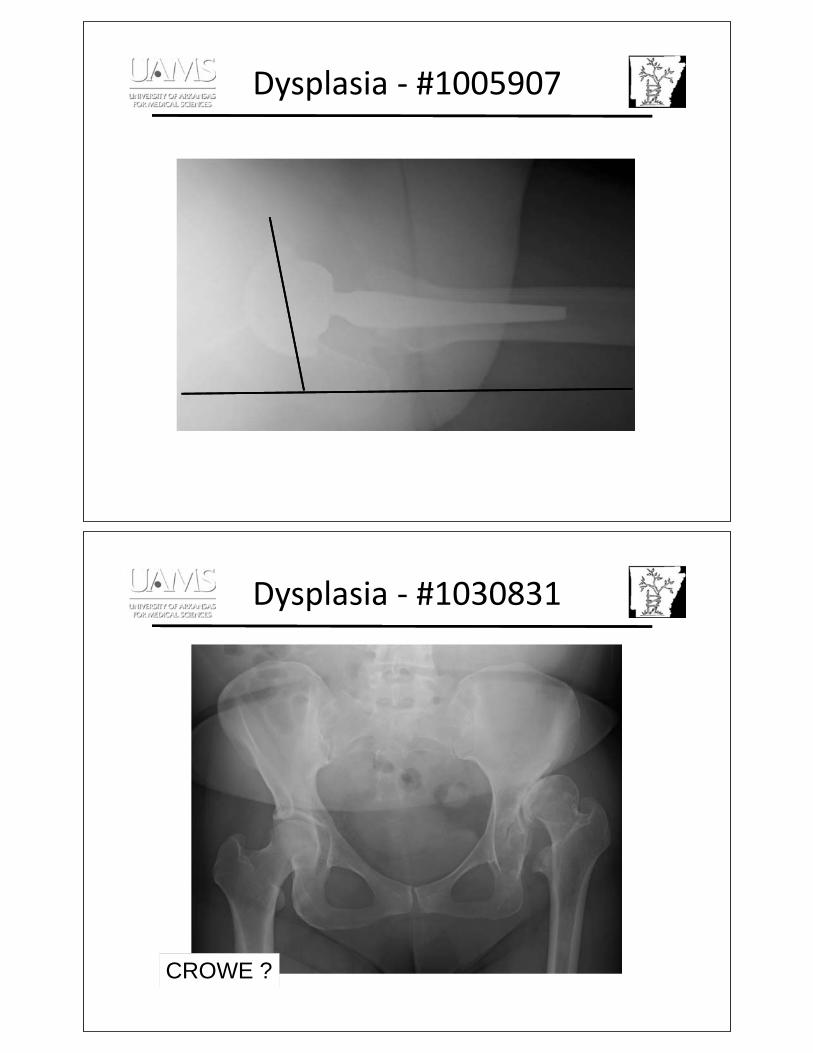
Dysplasia #1005907
Dysplasia #1030831
CROWE ?

Dysplasia #1030831
CROWE ?
Dysplasia #1030831
CROWE ?

Dysplasia #1030831
Dysplasia #1030831

AVN #1529558
AVNOA
AVN #1529558

AVN #1529558
AVN #1529558

AVN #3020955
AVN #3020955

AVN #3020955
AVN #3020955
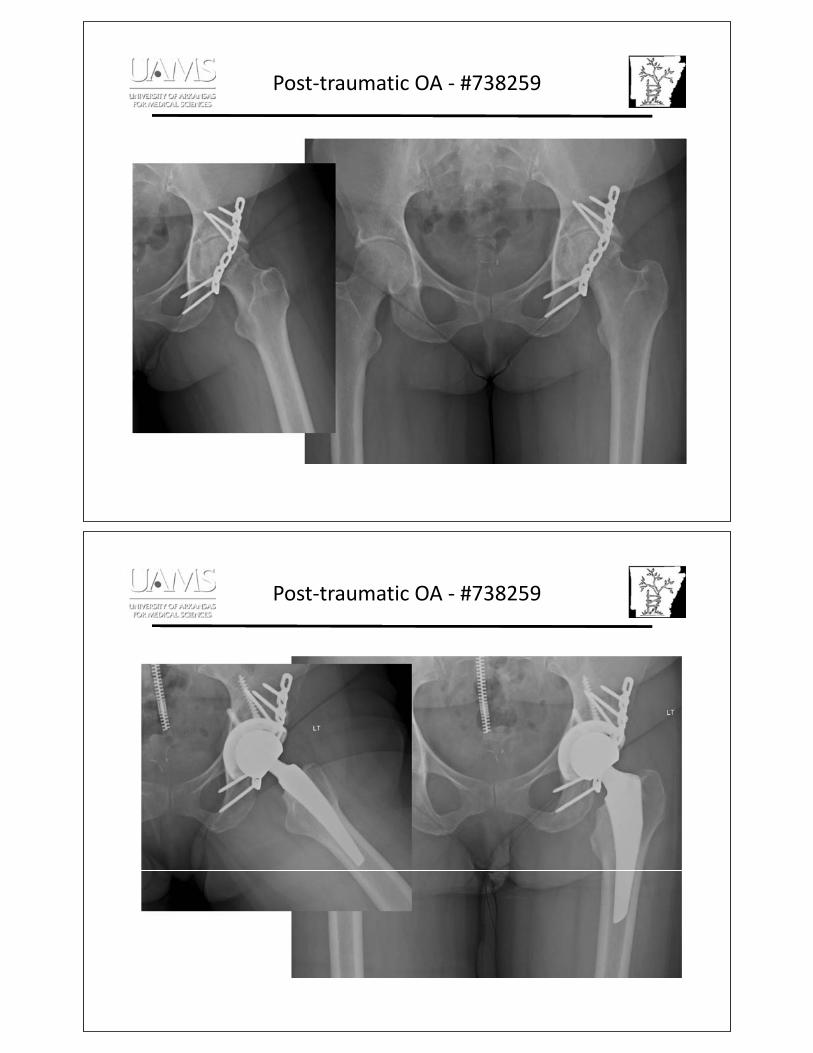
Post traumatic OA #738259
Post traumatic OA #738259

Post traumatic OA #3323787
Post traumatic OA #3323787

Conversion Arthroplasty #3336780
Conversion Arthroplasty #3336780

Conversion Arthroplasty #3336780
Conversion Arthroplasty #3336780

Conversion THA #704088
Conversion THA #704088

Conversion THA #704088
Cup Failure #3315446

Cup Failure #3315446
Cup Failure #3315446

Cup Failure #3315446
Cup Failure #3315446

Thank You
I am happy to answer any questions at anytime.
Clinic Tuesday – all day, Friday AM
Cell: 501-258-1115

22
Evaluation of Foot and Ankle Pain
Chelsea Mathews, MD
Resident Physician UAMS
Table of Contents

Foot and Ankle for the Primary Care
ProviderChelsea Mathews, MD
PGY-4, Orthopaedic SurgeryUniversity of Arkansas for Medical Sciences
No Disclosures

• Grew up in Greensboro, NC
• Family in Stuttgart, AR
• UAMS Residency
• Tiger fan
A little about me……
It is never wrong to immobilize (Boot) and refer!!!!
???

Overview• Anatomy
• History and Exam
• Diagnostic Modalities
•Common Conditions
My Goals For You:• Basic Anatomy of the Foot/Ankle
• Comfortable with Examination
• Diagnostic Tests (if any!) to Order
• Basic Treatment Algorithms for Common Conditions
• When in doubt, send it out!

Anatomy: The Bones
Anatomy: String and Things
“Outside” or LateralFoot/Ankle Anterior Talofibular Ligament
Peroneal Tendons
Achilles Tendon

Anatomy: Strings and Things
“Inside” or MedialFoot/Ankle
Posterior Tibial Tendon
Achilles Tendon
Anatomy: Blood Supply

Anatomy: Nerves
History and Examination: The Quick and Easy for Young/Active Patients
NORMAL EXAM!!!!

History and Examination: The basics
•Temporal
•Practical
•Objective
History: Timing
• How long has it hurt?• Injury/Inciting Event?
• When does it hurt?• Rest pain?• Activity Related?
• Has it gotten better or worse?
History: Practical
• Able to Bear Weight?• What makes it better/worse?• How have you been treating?
• Where does it hurt (Point with one finger)?
Examination: Motor Exam• Observe patient standing (shoes/socks off)
• Symmetry/asymmetry?
• Observe patient walking• Antalgic gait?
• Strength Testing• Toe/heel walk?• Basic Movements—Plantar Flexion etc.• Focused Exam

Examination: Sensory Exam
Focused Exam!
Diagnostic Modalities: When to Order and What to Order?
X-rays?
MRI?
CT Scan?
Ultrasound?

Diagnostic Modalities: X-rays
• Trauma• Ottawa Rules?
• Arthritis• Remote Trauma• Inflammatory
• Foreign Body• Metallic objects seen best
If uncomfortable/unable to read x-rays, refer
X-RAYS: What to Order?
• X-ray what hurts!
• 3-Views Foot (AP/Lat/Oblique)
• 3-Views Ankle (AP/Lateral/Mortise)
• Weight-bearing X-rays if possible

X-RAYS: What to Order?
• 3-Views Ankle (AP/Lat/Mortise)
• Weight-bearing X-rays if possible
X-RAYS: What to Order?
• 3-Views Foot (AP/Lat/Oblique)
• Weight-bearing X-rays if possible
APOblique
Lateral

Diagnostic Modalities: CT Scan
• Excellent Bony Detail
• Rarely indicated in Primary Care Setting
• Radiation
• If CT needed, refer to Ortho
Diagnostic Modalities: MRI
• Excellent for both Soft-Tissue and Bony/Cartilage Injury
• Compatibility with Imaging Systems???
• Rarely indicated in primary care setting (unless you own your own MRI)
• If MRI needed, refer to Ortho

Diagnostic Modalities: Ultrasound
• Soft-Tissue Evaluation
• No radiation
• Operator Dependent
• Evaluate for foreign body if X-rays negative
It is never wrong to immobilize (Boot) and refer!!!!
???

Common Conditions in The Ankle
Ankle Sprain
• History• Twisting Mechanism
• Inversion Most Common
• Lateral Ligaments
• Pain with weight bearing
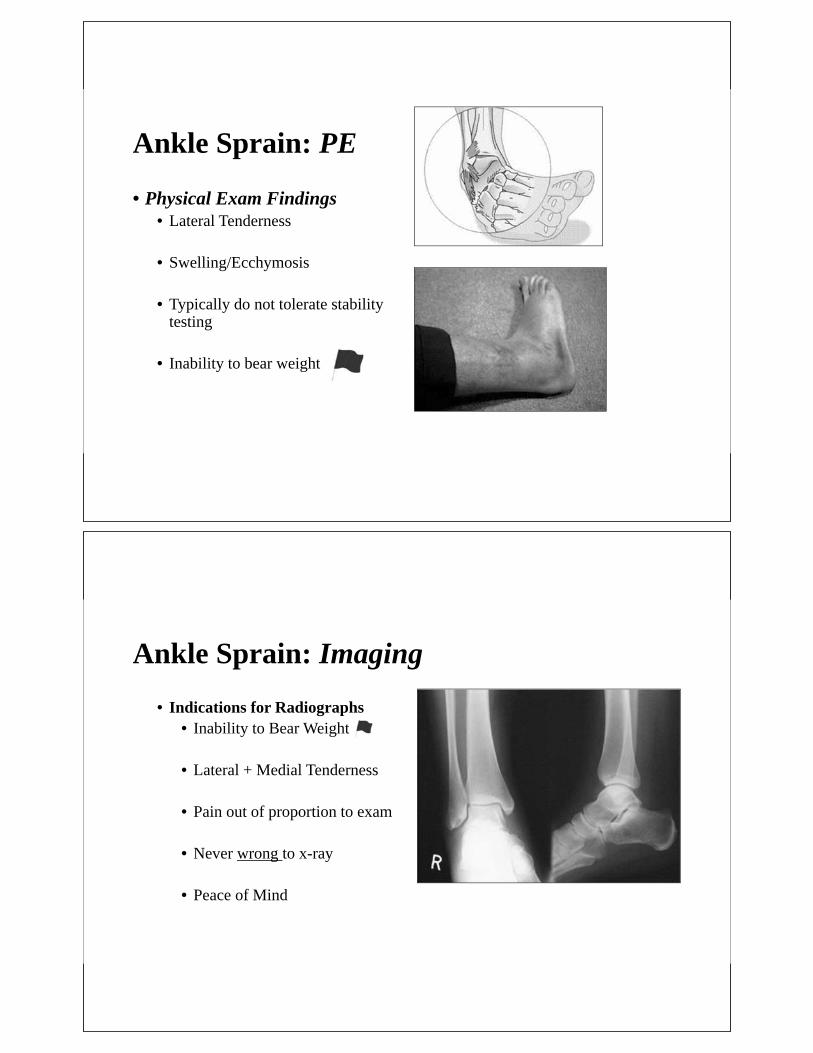
Ankle Sprain: PE
• Physical Exam Findings• Lateral Tenderness
• Swelling/Ecchymosis
• Typically do not tolerate stability testing
• Inability to bear weight
Ankle Sprain: Imaging
• Indications for Radiographs• Inability to Bear Weight
• Lateral + Medial Tenderness
• Pain out of proportion to exam
• Never wrong to x-ray
• Peace of Mind

Ankle Sprain: Treatment Algorithm
•Week 1-4•R.I.C.E!•Boot/Crutches if unable to WB•Lace-up Brace if able to WB•Weight bearing as tolerated
Ankle Sprain: Treatment Algorithm
•Week 4-8•Advance activities as tolerated•Start rehabilitation program (PT)•Lace-up Brace

Ankle Sprain: Treatment Algorithm
•Week 8-12•Continue activities as tolerated•Aggressive strengthening/rehabilitation program (PT)
•Brace/Taping?•Return to Sports?
15X
Ankle Sprain: When to Refer?
•If uncomfortable with managing…hopefully not after today
•No improvement after 4-6 week•Mechanical Symptoms•MRI?

It is never wrong to immobilize (Boot) and refer!!!!
???
Ankle Fractures (Briefly)
•History• Twisting Mechanism
• Fall
• MVA
• Diabetic

Ankle Fractures
• Exam• Bony palpation
• Skin exam
• Pulses
• Compartment Syndrome Rare
Ankle Fractures
•X-rays:• 3-View Ankle• Weightbearing if
patient will tolerate•Immobilize:
• Tall Boot• Splint• Crutches

Ankle Fractures: Not IF but When to Refer?
•Emergent• Deformity• High Energy• Skin integrity
•Non-emergent (7-10 days)• No deformity• Low energy
It is never wrong to immobilize (Boot) and refer!!!!
???

Ankle Arthritis
• History• No acute injury
• Post-traumatic• Multiple Sprains• Fracture
• Inflammatory• RA
• Primary…..much less common
Ankle Arthritis
• Imaging• 3-Views Ankle
• Weightbearing

Ankle Arthritis
• Treatment• Conservative
• Weight-loss• NSAIDS• OTC Bracing/Boot (Temp)• Rocker Sole Shoe• Rheumatology?• PT limited benefit
Ankle Arthritis
• Injection• 1:1 Depo/Marcaine• 25 Ga needle• Anteromedial easiest• U/S?• CPT 20605• No more than 4/year

Ankle Arthritis: When to Refer?
• Conservative Treatment Not Working
• Patient Unhappy
• Doctor Unhappy
Ankle Arthritis: How We Treat?
Arthrodesis/Fusion
JointReplacement

Common Conditions in The Heel
Achilles Insertional Tendinopathy• 3Fs (Female, Fat, >50)
• Concomitant symptoms from• Haglund’s deformity
• Retrocalcaneal bursitis• Morning pain, stiffness, progresses to constant• If bilateral, consider inflammatory arthropathy

Achilles Insertional Tendinopathy
• Exam• Palpable bump
• Skin Irritation
• Pain with plantarflexion/driving
• Better with elevated heel
Achilles Insertional Tendinopathy
• Imaging• Lateral view of heel
• MRI rarely indicated
Achilles Insertional Tendinopathy
• Treatment1. Immobilize (boot)
2. NSAIDs (oral/topical)
3. Shoe with elevated heel
4. Physical Therapy of limited efficacy
Achilles Insertional Tendinopathy
• Refer• Failed non-operative
management 3-6 months
• Patient not happy
• Doctor not happy
• Surgery with good results….but, long recovery process 4-6 months

Achilles Tendinopathy: Non-Insertional
• Peritendinitis• Diffuse swelling and tenderness along course of tendon
• Tendinosis• Pain and swelling with nodular area within tendon
• Peritendinitis with Tendinosis
Achilles Tendinopathy: Non-Insertional
• What you need to know• Difficult to differentiate clinically between the 2 conditions
• Treatment is the same• If pain above insertion site, x-rays of limited value

Achilles Tendinopathy: Non-Insertional
• Non-surgical management effective in 75% of patients
• Rest, NSAIDs, Eccentric Stretching, Boot Immobilization
• PRP, Stem Cell injection?
Achilles Tendinopathy: Non-Insertional
• When to Refer• High Performance Athletes
• No improvement 4-6 weeks conservative care• Patient Unhappy• Doctor Unhappy

Plantar Fasciitis• Plantar Heel Pain
• Very Common• Morning pain, pain with prolonged weightbearing
Plantar Fasciitis
• Anatomy/Path• Thick band of soft tissue,
inserts into plantar calcaneus, supports the arch
• Inflammatory• Traumatic• Etiology uncertain
Plantar Fasciitis
• Exam:• Tenderness to palpation over plantar-medial heel
• Motor/Sensory exam normal
• Usually unimpressive exam
• Tight calf muscle associated
Plantar Fasciitis
• Imaging:• Limited value
• Lateral View of Heel

Plantar Fasciitis
•But what about the heel spur, Doctor?
Plantar Fasciitis
The Good News…..• It doesn’t last forever
• There are several non-operative modalities to treat PF
• Surgery is rarely required
The Bad News…..• I don’t know how long it’s going
to last
• Different people respond differently to different modalities
• If all else fails, injection/surgery may help

Plantar FasciitisTreatment Protocol
1. Icing (frozen water bottle)2. NSAIDs, Oral/Topical3. Stretching Excersises (see handout)4. Gel Heel Cups (OTC)5. Night Splinting (if morning pain significant)
• Acute phase (0-6 months)
Plantar FasciitisTreatment Protocol
1. Icing (frozen water bottle)
2. NSAIDs, Oral/Topical
3. Stretching Excersises/PT
4. Gel Heel Cups (OTC)
5. Night Splinting (if morning pain significant)
6. Injections• 1:1 Depomedrol/0.5% Marcaine• PRP/Stem Cells?
• $$$
• Chronic phase (>6 months)

Plantar Fasciitis
• When to Refer?
When you just can’t take it any longer!!!
Plantar Fasciitis
Patients will eventually get better but it can be a long and painful process

Common Conditions of the Midfoot
5th Metatarsal Base Fractures
• Most common Metatarsal Fracture
• Mechanism varies• Most often twisting,
inversion-type• Commonly seen concurrently
with other Injuries:• Ankle Sprain• Ankle Fracture

5th Metatarsal Base Fractures
• Exam• Lateral foot pain
• Swelling• Ecchymosis• Point Tenderness
• Pain with eversion/WB• Peroneus Brevis• Plantar Fascia
5th Metatarsal Base Fractures
• Imaging• X-ray what hurts• 3-Views Foot• 3-Views Ankle

5th Metatarsal Base Fx: Zone 1• Classification
• Zone I• Most common• Hindfoot inversion
• Treatment• WBAT in boot• Heals ~6-8 weeks
Refer if Unsure
5th Metatarsal Base Fx: Zone II• Classification
• Zone II (Jones fracture)• Forefoot adduction• 4th/5th Intermetatarsal joint• Risk of nonunion
• Treatment• NWB in boot or cast 6-8
weeks• Competitive athlete
• Needs Surgery
Refer

5th Metatarsal Base Fx: Zone III• Classification
• Zone III• Stress fractures• Distal to 4th/5th Intermetatarsal
joint• Nonunion Risk
• Treatment• NWB in boot or cast 6-8
weeks• Competitive athlete
• Surgery
Refer
5th Metatarsal Base Fractures•Zone 1: Boot x 6 weeks
•Zones 2/3, Immobilize and Refer
Boot Refer Refer

Common Conditions of the Forefoot
Hallux Rigidus (1st MTP Arthritis)
• Degenerative joint disease of 1st MTP
• Idiopathic• Inflammatory
• Gout• Rheumatoid
Arthritis

Hallux Rigidus (1st MTP Arthritis)
• Exam• Pain with walking, sand,
uneven ground, flimsy shoes
• Skin Irritation• “Bump” over dorsal MTP
joint, tender• Decreased ROM
Hallux Rigidus: Imaging• 3-Views of Foot
• Lateral View shoes the “bump”• AP View shows the joint space narrowing
Lateral
A/P

Hallux Rigidus: Treatment
• Non-Operative Treatment• NSAIDs (Oral/Topical)
• Immobilization
• Shoe modifications• Morton’s Extension• Rigid-last Shoe• Large Toe Box
• Injection?
Refer When Conservative Treatment Unsuccessful

Morton’s Neuroma• Benign neuroma of
interdigital nerve• Intermetatarsal
ligament compression• 3rd webspace, most
common• 2nd webspace, next
most common
Morton’s Neuroma•Exam
• Burning, electricity, paresthesia, numbness in webspace to toes
• “Pebble in shoe”

Morton’s Neuroma•Exam
•Mulder’s sign
•TTP in webspace
Morton’s Neuroma: Imaging
• Clinical Diagnosis!!!!

Morton’s Neuroma•Treatment
• Metatarsal Pad• Carried at Most Pharmacies• Place proximal to area of
tenderness
Morton’s Neuroma•Treatment
• Injection• Diagnostic/Therapeutic• 1:1 Corticosteroid/Anesthetic• Nerve near Plantar Surface of
foot• No more than 2 injections total!
Refer When Conservative Treatment Unsuccessful

Take Home Points
• Most acute problems of the foot and ankle can be treated appropriately with immobilization
• Weightbearing x-rays show more pathology and should be obtained when possible
• Never hesitate to refer a patient on to an Orthopaedic Surgeon
501-258-0189

23
Common Neck Issues
David Bumpass, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

24
Evaluation and Management of Back Pain
David Bumpass, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

25
Evaluation of Extremity Masses
Corey Montgomery, MD
Associate Professor Department of Orthopedics
UAMS
Table of Contents

Corey Montgomery MD, MS
Associate Professor
Department of Orthopaedic Surgery
Division of Orthopaedic Oncology
University of Arkansas Medical Sciences
Arkansas Children’s Hospital
EVALUATION OF EXTREMITY MASSES
There are no financial relationships related to this discussion to disclose.
FINANCIAL DISCLOSURE

Be able to appropriately evaluate extremity masses.
Be able to recognize common extremity masses using physical exam and radiological findings.
Be able to recognize possible malignant tumors and know when to refer for appropriate treatment.
OBJECTIVES
Extremity masses primarily arise from two sources
Soft-tissueBenignMalignant
BoneBenignMalignant
The vast majority of extremity masses are benign.
Benign soft-tissue tumors/masses are 100 times more common than malignant.
INTRODUCTION

Misdiagnosis can be very problematicDelayed treatmentInappropriate treatment
WHY IS THIS TALK IMPORTANT??
History of IllnessAge
Malignancies more common patients >60 years old
DurationBenign conditions are more likely to have been around for longer durations of time
EEVALUATION

Medical HistoryGout Rheumatoid arthritis Diabetics
Skeletal muscle necrosis
Family HistoryFamily members with any findings similar to the patient
Neurofibromatosis & Multiple Hereditary Exostosis
Social HistoryType of job, hobbies, and pets
EVALUATION
Physical ExamInspection
Skin changesPalpation
MobilityFirmnessDeepPainful
Neurovascular examination
EEVALUATION

Laboratory TestUsually not beneficial unless
Infection
Rheumatoid ArthritisGout
EVALUATION
RadiographsBest for bone evaluationSoft-tissue masses
UltrasoundGood for evaluating ganglions
Non-invasive, cheap and fast
CT-scanVery good for evaluation of osseous masses
IIMAGING

ZONE OF TRANSITION
Geographic Permeative
BENIGN PERIOSTEAL REACTION
Smooth, solid

AGGRESSIVE PERIOSTEAL REACTION
Onion skin, Lamellated Spiculated, Hair-on-end, Sunburst
MRIGold standard for the evaluation of soft-tissue masses
PET-scanMinimal usefulness in the initial evaluation
Bone ScanUseful in evaluating for possible multiple bone lesions
Metastatic cancer to the bone
IMAGING

Benign Soft-tissue
LipomaHemangioma or vascular tumorsMyositis OssificansGanglionHematoma
SOFT-TISSUE LUMPS AND BUMPS
PresentationPresent for many years
Slow growthCan be found anywhereUsually painful
DiagnosisClinical
Usually compressibleImaging
TreatmentTreat if symptomatic
Beware of the atypical lipomatous tumor
LIPOMA

Presentation:Slow enlargementPainfulSize changes with activity
DiagnosisClinical
Skin markings sometimes
ImagingX-rays: PhelobilithsMRI: Serpentine pattern
TreatmentObservation if asymptomatic
VASCULAR TUMORS
Presentation Can be associated with traumaHard non-mobile massOccasionally painful
DiagnosisMature peripheral ossification on x-rays
TreatmentSymptomatic
Beware of similar appearing conditions
Parosteal osteosarcomaSoft-tissue sarcoma with calcifiations
MYOSITIS OSSIFICANS

PresentationFrequently appears around jointsCan change in size
DiagnosisClinical
Transilluminate with lightAspiration
ImagingU/SMRI
TreatmentObservationAspirationSurgical removal
GANGLION CYST (BIBLE CYST)
Common soft-tissue tumor found on along tendon sheathsSlow enlarging painless massVariant of PVNSTreatment
Marginal Excision
Local Recurrence
GIANT CELL TUMOR OF TENDON SHEATH

PresentationHistory of traumaAnticoagulation or clotting deficiency
DiagnosisClinical
Ecchymosis usually present
ImagingCan be deceiving
TreatmentObservation
Proceed with cautionRapidly enlarging hematomas Soft-tissue sarcomas can bleed from within
HEMATOMA
Soft-tissue sarcomas are malignant neoplasms that arise from mesenchymal tissue.
FatMuscle
SkeletalSmooth
Fibrous
PresentationDeep fascia>5cm Firm/FixedRapid Growth
MALIGNANT TUMORS

Wide Excision
Radiation
TREATMENT
The removal of a malignant mass thought to be benign without appropriate attention to preoperative imaging, pre-excision biopsy, or operative margins.
UNPLANNED EXCISIONS OF SOFT-TISSUE MASSES: DEFINITION
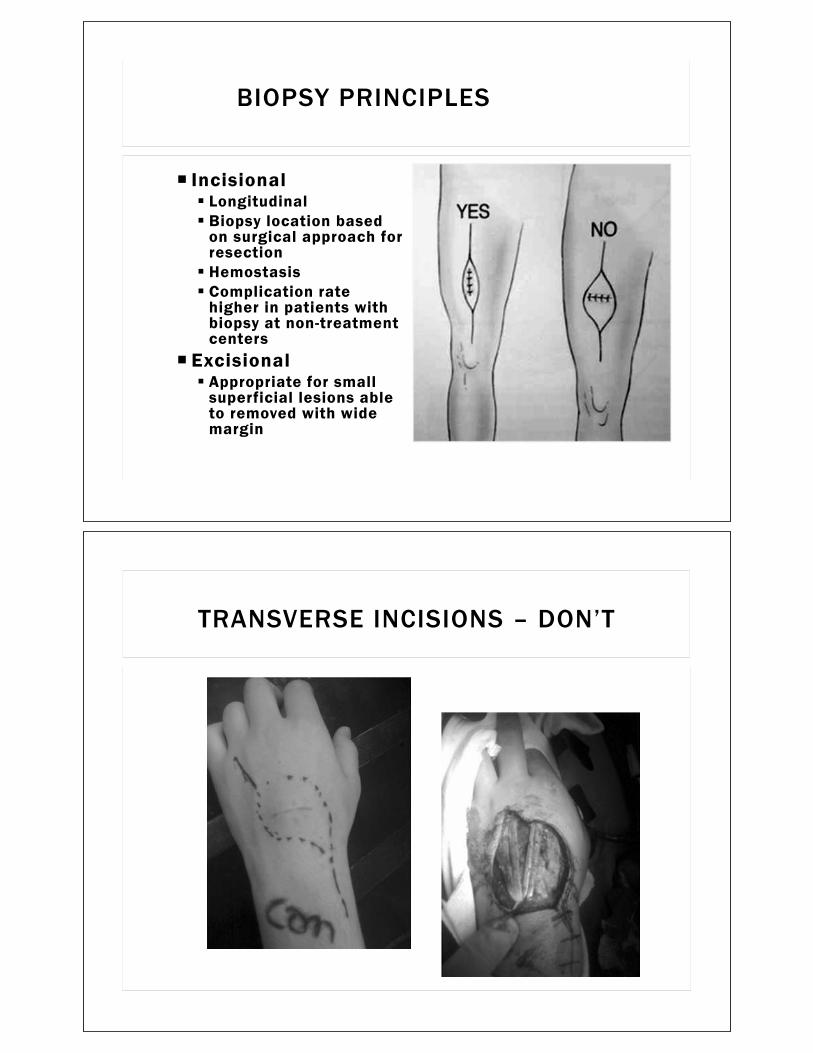
IncisionalLongitudinalBiopsy location based on surgical approach for resectionHemostasisComplication rate higher in patients with biopsy at non-treatment centers
ExcisionalAppropriate for small superficial lesions able to removed with wide margin
BIOPSY PRINCIPLES
TRANSVERSE INCISIONS – DON’T

Unplanned Excisions occur in up to 50% of all STS
Residual Disease – 24-91 %
Reconstructive Requirements – 30-82% skin graft or flap rate
Local Recurrence – 22-57% (2 to 6-fold )
Prognostic Implications Does not affect survival
Doubles the cost of care
UNPLANNED EXCISIONS - SEQUELAE
Benign
OsteochondromaUnicameral bone cystNon-ossfying fibroma
BONE LUMPS AND BUMPS

PresentationSolid non-painful massChildhoodMultiple lesions
Multiple Hereditary Exostoses
Diagnosis Plain filmCT-scanMRI
Cartilage cap thickness
TreatmentRemoval if symptomatic
OSTEOCHONDROMA
PresentationPainFractureIncidental
DiagnosisX-ray
Lucent lesionThinning of cortexFallen leaf –pathognomonic for simple bone cyst
TreatmentObservationOperative if symptomatic
UNICAMERAL BONE CYST

PresentationPainFractureIncidental
DiagnosisClinicalImaging
Soap-bubble appearance
TreatmentObservationSurgical removal if symptomatic
NON-OSSIFYING FIBROMA
Malignant
Bone sarcomasRare malignant tumors
Osteosarcoma
Ewing’s sarcoma
Metastatic Disease or Multiple Myeloma
Lung cancer
Breast cancer
MALIGNANT BONE MASSES

PresentationMore common in 2nd decade of lifePainRapidly enlarging mass
DiagnosisClinical
Destructive lytic lesion on imaging
TreatmentWide excisionChemotherapy and/or radiation
BONE SARCOMAS
PresentationOver the age 40PainFracture
DiagnosisHistoryImaging
Bone scanCT-chest, abd & pelvis
TreatmentChemotherapyStabilization of fracture
METASTATIC DISEASE

Delayed treatment
Inappropriate treatmentIncorrectly performed biopsy
Increased # of surgical procedures
Amputation
CONSEQUENCES OF INCORRECT DIAGNOSIS
The majority of extremity masse are benign
A through evaluation is required in every patient
Clues for Referral/ImagingPainful masses
Rapidly enlarging masses
Large and deep masses
CONCLUSIONS

QUESTIONS

26
Common Pediatric Musculoskeletal Disorders
Michael Israel, MD
Assistant Professor Department of Orthopedics
UAMS
Table of Contents

Common Pediatric Musculoskeletal Disorders
MICHAEL ISRAEL, MD, CAQSM
What are Overuse Injuries?
•AMSSM: “An injury that involves the muscle-tendon unit, bone, bursa, neurovascular structures, or the physis due to repetitive submaximal loading of the musculoskeletal system when rest is not adequate to allow for structural adaptation to take place”
•Apophyseal injuries and physeal injuries are unique to the pediatric population

Definitions
•Physis• Primary ossification center located at the ends of long bones• Responsible for longitudinal growth
•Apophysis• Secondary ossification center located where major tendons attach
to bone• Provide shape and contour to growing bone but add no length
•Apophysitis• Irritation of the musculotendinous attachment

Evaluation Concerns•Recent change in activity or training
•Insidious onset of pain that worsens with activity and improves with rest
•Point tenderness with or without swelling
•Pain with stretch of attached ligament/muscle-tendon unit
Common Physeal and Apophyseal Injuries

Little League Shoulder•Fatigue fracture of the proximal humeral physis
• Does not fuse until ages 14-20
•Typically high-performance male pitchers
•Rotatory torque stresses to the epiphyseal growth plate
•9-14 years old
•Pain
•Inability to perform
•Decreased ROM
•TTP at anterior proximal humerus
•Remember– physis is the weak link!
Little League Shoulder•Evaluation
• Detailed history• Pitch counts/innings thrown/teams played on• Routine shoulder examination• Comparison xrays
•Treatment• Relative rest for 4-6 weeks NO THROWING• Interval throwing program• PT Thrower’s 10 program

Little League Shoulder
Little League Elbow•Medial epicondyle apophysitis
•9-14 y/o overhead athletes• ~18-29% incidence of elbow pain in youth and HS baseball players
•Point tenderness over medial epicondyle
•Classically worsened by repetitive throwing
•Hypertrophy of medial epicondyle
•Flexion contracture
•Pain with valgus stress and milking maneuver

Little League Elbow•If apophysis not significantly displaced (<5mm)
• (Relative) rest 4 - 6 weeks• Isometric strengthening, stretching, resistive strengthening• Throwing mechanics evaluation• Gradual return to throwing after 6 - 12 weeks
• Interval Throwing Program • Follow pitch counts & types
•If apophysis significantly displaced (>5mm) surgery is warranted
Little League Elbow•X-rays may reveal widening of medial epicondyle apophysis and/or fragmentation of medial epiphysis
•85% of X-rays are normal

Sever’s Disease•Calcaneal apophysitis
• Repetitive heel impact and traction stress from the Achilles tendon
•Boys = girls
•Ages 8-13 most common
•Bilateral in 60% of cases
Sever’s•Heel pain worse with activity
•No swelling
•Point tender at posterior calcaneus
•Pain with medial-lateral compression
•Pain with calf stretch or contraction against resistance
•Tight heel cord, weak dorsiflexors, subtalar overpronation

Sever’s Risk Factors
•Repetitive explosive activities•Repetitive trauma
– Jumping, landing, cleats, etc.
•Recent increase in activities•Tight heel cord•Before/during rapid periods of growth•Beginning of new season
Sever’s- Treatment•Relative rest
•Heel cord stretching
•Heel cups
•Ice
•NSAIDs

Pelvic Apophysitis
•10-14 years old
•Insidious onset of hip pain or sudden sharp pain • Running, jumping, kicking sports
•Point tender
•Pain with stretch or contraction of involved muscle
•Widening of physis or avulsion of apophysis
Pelvic Apophysitis

Pelvic Apophysitis•Ischial tuberosity- 38%
• Hamstrings & Adductor
•ASIS- 32%• Sartorius
•AIIS- 18%• Rectus Femoris
•Lesser trochanter- 9%• Iliopsoas
•Iliac crest- 3%• ITB/Tensor Fascia Latae• Abdominal muscles
Ischial Tuberosity

AIIS Avulsion
Pelvic Apophysitis- Treatment•Relative rest until pain free (~4-6 weeks)
•WBAT without limping
•NSAIDs
•Ice
•Stretching & strengthening
•Progressive return to activities
•Rare need for surgery

Osgood-Schlatter
•Tibial tubercle apophysitis
•Occurs in 20% of young athletes• Most common pediatric overuse injury
•20% of OSD is bilateral
•Girls 8–13yo
•Boys 10-15yo
•Aggravated by running, jumping, or other explosive activities
•Occasionally aggravated by kneeling or direct trauma
Osgood-Schlatter•Evaluation:
• Point tender +/- swelling at tibial tubercle• Pain with quadriceps stretch or contraction, poor quad flexibility• Widened physis or fragmented tibial tubercle on radiographs• Tight quadriceps or hip flexors
•Treatment:• Relative rest• Quadriceps and hip flexor stretching• Ice• NSAIDs• Cho-Pat strap• Knee pads

Osgood-Schlatter
Sinding-Larsen-Johansson•Apophysitis at the inferior pole of the patella
•10-12 years old
•Most common in running/jumping athletes• Basketball, soccer, gymnastics
•“Adolescent Jumper’s Knee”

Sinding-Larsen-Johansson•Evaluation
• Tenderness at the inferior pole of the patella• Pain worsened with explosive activity• Tight quadriceps• Radiographs may reveal fragmentation of the inferior pole and/or
calcification at the proximal patella tendon
•Treatment• Relative rest• Quadriceps stretching• Ice• NSAIDs• Cho-Pat strap
Sinding-Larsen-Johansson

Spondylolysis•Stress fracture of the pars interarticularis
•Insidious back pain exacerbated by strenuous activity
•Occasional radiation to the buttocks
•Rising to an upright posture against resistance elicits pain
•Pain exacerbated by hyperextension & rotation bilateral, unilateral
•Hamstring tightness in 80% of patients
•Tenderness in lumbar spine to palpation
Spondylolysis

Spondylolysis Workup•Xray- AP, lateral, obliques
•Bone scan/SPECT CT
•MRI
Spondylolysis

Spondylolysis
Spondylolysis•Relative rest & activity modification
•Time (>3 months)• Retrospective analysis of 57 youth soccer players who took at least 3 months
off, with or without bracing had the most optimal results
•Physical therapy- Flexion-based core strengthening
•NSAIDs
•Bracing?• If still painful after the above
•Surgery- option if symptomatic 6-12 months after treatment
•High rates of nonunion for delayed treatment
•Progression to >20% spondylolistheses ~5%Increased if bilateral
FRACTURES
Introduction•Orthopedic problems are over 10% of all primary care visits
•1.6% of all visits to any physician are fracture related
•16% of all fracture care is handled by family physicians

Metatarsal / Phalanges•Keep
• Minimally/Non-displaced fractures• Short leg cast• NWB 4-8 weeks
•Refer• Lis Franc fracture or Jones Fracture• Displaced Metatarsal Shaft or intra-articular fractures• Multiple fractures• Short leg splint; NWB
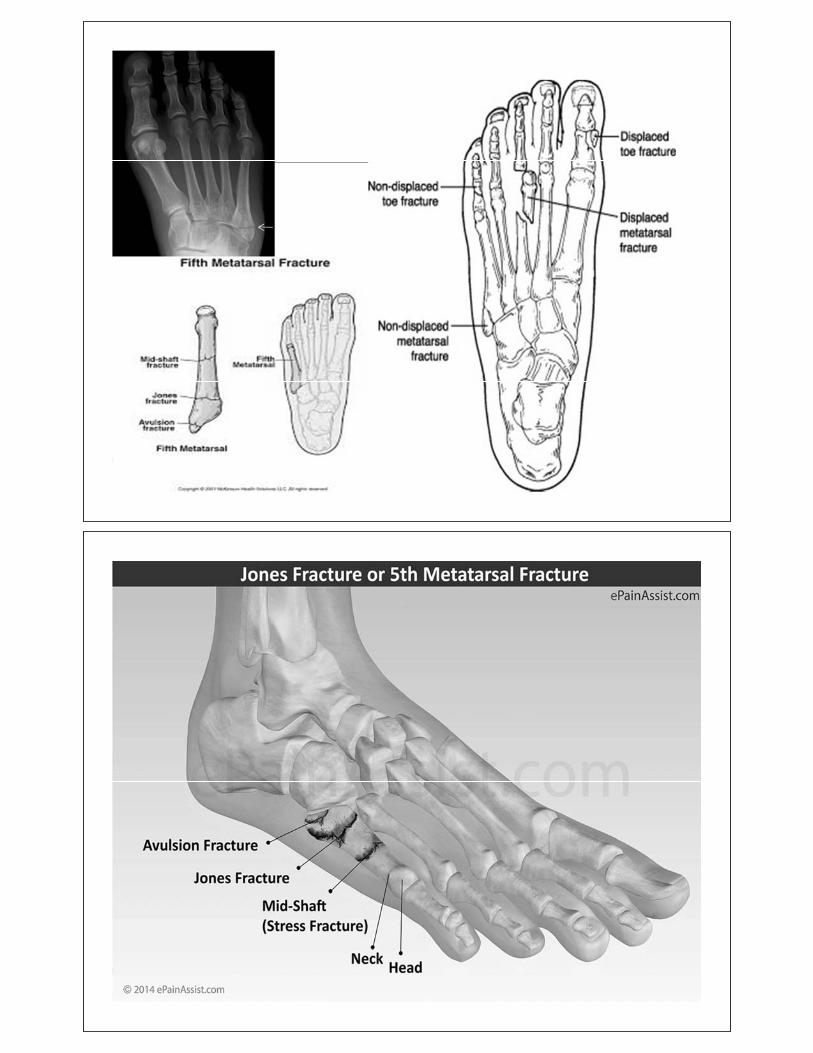

Ankle Fractures•Keep:
• Avulsion fractures and some Weber A type• Some Weber B fractures
• Need stress radiograph• Splint : posterior slab +/- stirrups x1 week• Cast: Short leg x2-6 weeks• NWB 2-8 weeks• AROM ~4 weeks• PT for ankle strengthening and proprioceptive training

Clavicle Fractures•Keep
• Shaft type with minimal displacement and shortening• Sling or Figure 8 for 4-6 weeks• ROM/Strengthening thereafter
•Refer• Comminution, shortening, distal/proximal type (2 cm)• Sling

Distal Radius•Most common orthopedic injury with a bimodal distribution
• Younger patients - high energy • Elderly patients – low energy fall
•Keep• Non-displaced extra-articular• Well reduced extra-articular with good bone quality in a well-molded
cast/splint
•
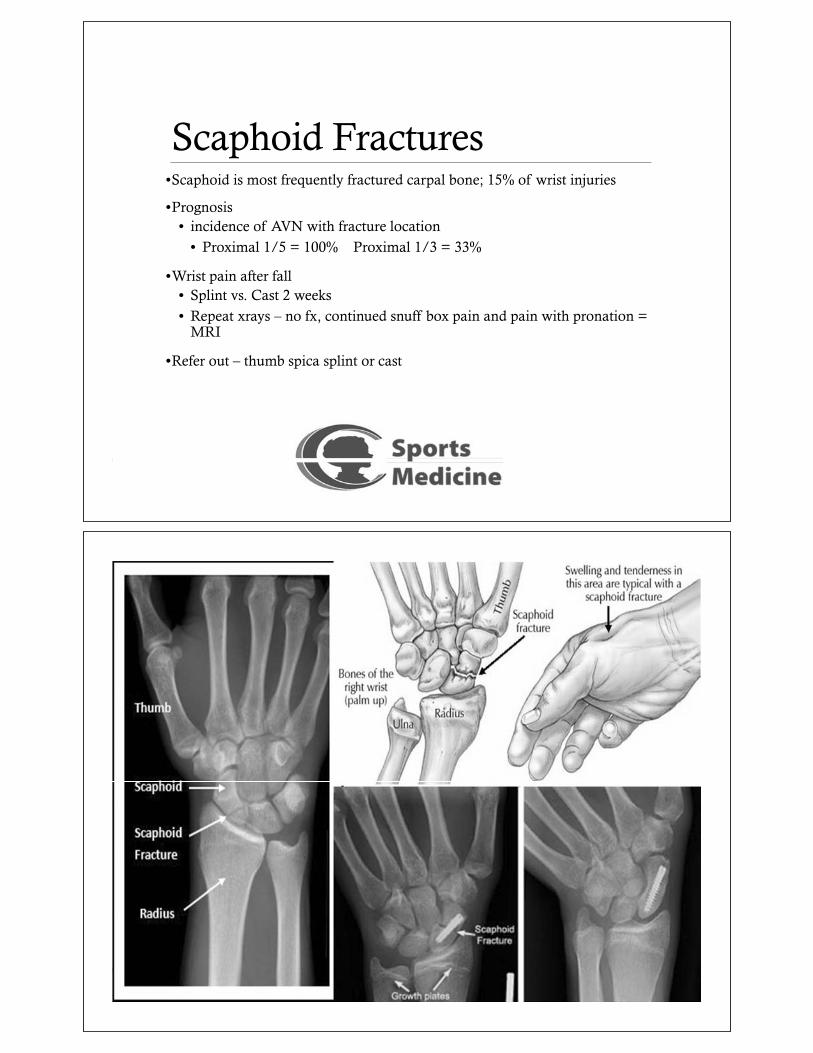
Scaphoid Fractures•Scaphoid is most frequently fractured carpal bone; 15% of wrist injuries
•Prognosis • incidence of AVN with fracture location
• Proximal 1/5 = 100% Proximal 1/3 = 33%
•Wrist pain after fall• Splint vs. Cast 2 weeks• Repeat xrays – no fx, continued snuff box pain and pain with pronation =
MRI
•Refer out – thumb spica splint or cast
Pediatric Considerations

Radiographic Evaluation of the Injured Child
•At least 2 orthogonal views
•Include joint above and below fracture
•Understand normal ossification patterns
•Comparison radiographs rarely needed, but can be useful in some situations
Fractures common only in skeletally immature
•Physeal injuries• “weak link” = physis,
especially toward end of growth
•Buckle or Torus Fracture
•Plastic Deformation
•Greenstick Fracture
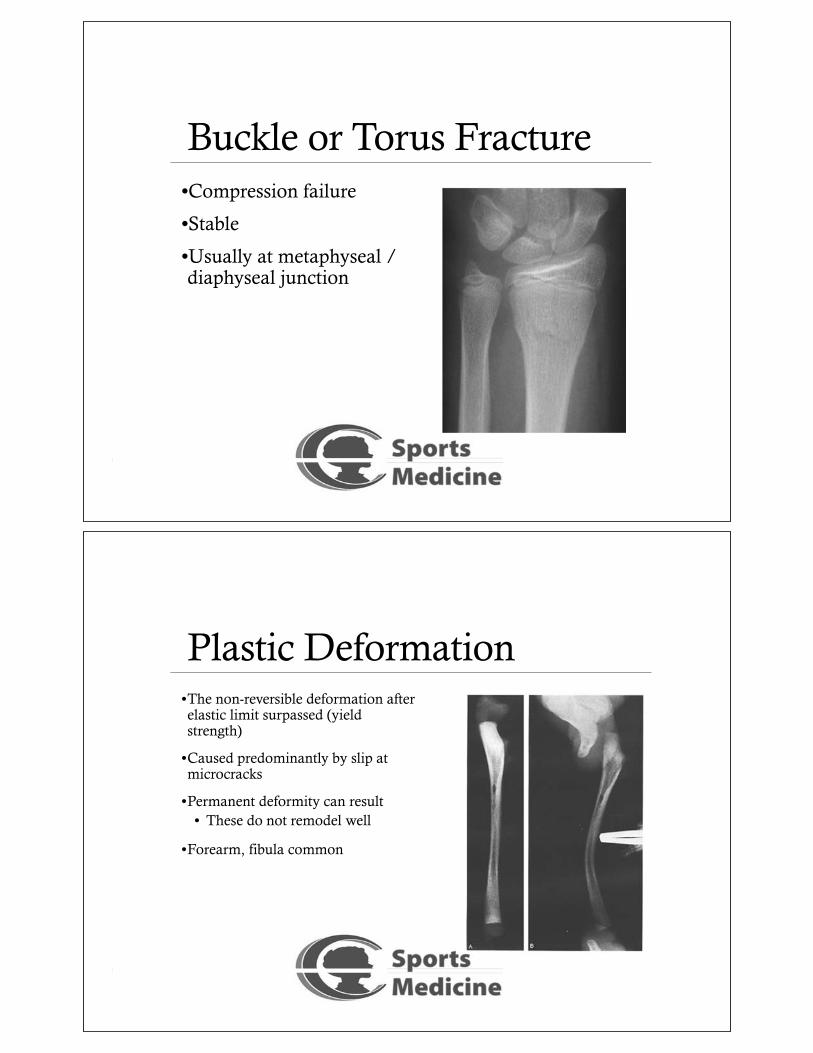
Buckle or Torus Fracture•Compression failure
•Stable
•Usually at metaphyseal / diaphyseal junction
Plastic Deformation•The non-reversible deformation after elastic limit surpassed (yield strength)
•Caused predominantly by slip at microcracks
•Permanent deformity can result• These do not remodel well
•Forearm, fibula common

Greenstick Fractures•Bending mechanism
•Failure on tension side
•Incomplete fracture, plastic deformation on compression side
•May need to complete fracture to realign
Salter - Harris Classification•Type I
• Through physis only
•Type II• Through physis & metaphysis
•Type III• Through physis & epiphysis
•Type IV• Through metaphysis, physis &
epiphysis
•Type V• Crush injury to entire physis

Salter Harris type I•Transverse through the entire physis, without metaphyseal fragment.
•Most common
•Closed reduction if displaced.
•Complications• Most heal uneventfully• Growth slowdown/arrest
Salter Harris type II•Extends partially along the physeal-metaphyseal interface, and then propagates into the metaphysis.
•Most common after 4 years
•Closed reduction.
•Complication: majority heal without significant consequences.

Salter Harris type III•Propagates transversely along the physeal-metaphyseal interface and cross the physis, epiphysis, ossification center and articular cartilage• unstable and intraarticular
•Open reduction may necessary with internal fixation
•Complication: Growth arrest angular deformity, osteoarthritis, non union
Salter Harris type IV•Intraarticular vertical splitting of all zones of the physis.
•Open reduction may necessary with internal fixation
•Complication: Growth arrest angular deformity, osteoarthritis, non union

Salter Harris type V• Crush injury to growth plate.
Salter Harris Classification General Treatment Principles
•Type I & Type II• Closed reduction &
immobilization• Exceptions
• Proximal femur• Distal femur

Salter Harris Classification General Treatment Principles
•Type III & IV• Intra-articular and physeal
step-off needs anatomic reduction
• ORIF, if necessary
Nurse Maid’s Elbow
•Peak 2-3 yo Girls> boys, L> R
•Sudden longitudinal traction on outstretched arm
•Annular ligament of Radius displaces into Radio-capitellar articulation (baby will not move arm)
•Adducted semiflexed in Prone position
•No significant tenderness to palpation
•Attempts to pronate/supinate PAIN

Slipped Capital Femoral Epiphysis• An abrupt or gradual displacement of the proximal femoral head on
the femoral neck.• Male/female 2:1; mean age 11.5 years in girls, 13 years in boys• Pts often tall, overweight• Cause unknown. Possible factors: growth spurts, hormonal factors, an
intrinsically defective growth plate, genetic predisposition, trauma• Hip motion painful & limited• Tx: stabilization of epiphysis w/ screw or cortical bone graft, followed
by crutch.• No tx: premature degenerative arthritis

Legg-Calve-Perthes
• Males, caucasion, 4-8 yo with hip/knee pain• Resolves 18 mo to 4 years. 50% resolve w/out tx• Tx: surgery, or more conservative bracing

Questions?