thrombophilia: practice aspects ibrahim alhijji, mb.bch., frcp head of clinical hematology ncccr hmc...
TRANSCRIPT

Thrombophilia: Practice Aspects
Ibrahim Alhijji, MB.BCh., FRCPHead of Clinical Hematology
NCCCRHMC
Feb. 2015

Contents
• Introduction• Heritable Thrmbophilia• Effect on management• Summary

Contents
• Introduction• Heritable Thrmbophilia• Effect on management• Summary

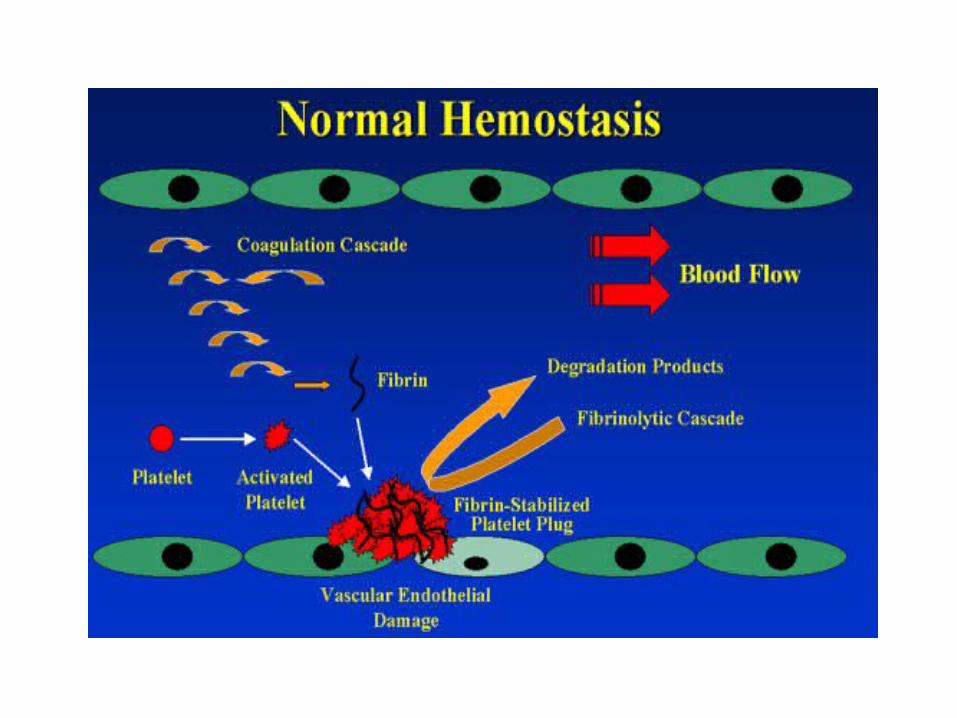
Normal Hemostasis
• Vessel wall– Endothelium
• Platelets• Coagulation factors• Fibrinolytic system• Natural anticoagulants

TF
VIIa
TF-expressing cell
TF
VIIa
Activated platelet
platelet
X
Va
Xa
prothrombin
thrombin
VIII/vWF VIIIa
V
XI XIa
Va
prothrombinthrombin
X
Xa
Va
IX
IXa
IXa
VIIIa
IXXIa
Hoffman M et al. Blood Coagul Fibrinolysis. 1998; 9(suppl 1): S61-S65.

Bleeding or Thrombosis
• Any alterations in hemostatic mechanism may lead to either bleeding or thrombosis

Incidence
• VTE is affecting 1-2 in 1000/year• Leads to chronic post-thrombotic syndrome
(20%) and chronic thrombo-embolic pulmonary hypertension (10%)
• 3rd most common cardiovascular disease after MI and CVA
ACCP (Bates et al 2012, Kearon et al 2012) NICE (2012)

Causes of death in Europe
• 543,454 due to VTE
• Exceeds combined deaths due to: AIDS 5,860 BC 86,831 PC 63,636 Transport Accidents 53,599
T & H 2007 Circulation 1996

Contents
• Introduction• Heritable Thrmbophilia• Effect on management• Summary

Virchow’s Triad
• Pathogenesis of a ThrombusEndothelial injuryAbnormal blood flowHypercoagulability
• Primary (genetic)• Secondary (acquired)

Thrombophilias
• A heterogeneous group of conditions that predispose individuals to VTE

Acquired
• Age: largest gradient of risk• Malignancy: prevalence ranges from 3-18%• Surgery: – Orthopedic surgery:30 - 50%– Abdominal surgery: 30%– With anticoagulants: 18%
• Major trauma: 50-60%• Immobilization

Acquired
• Oral contraceptives: 4 X increase in risk• Hormonal replacement therapy: 2-4 X
increase• Pregnancy and post-partum: 10 X increase• Antiphospholipid antibodies: 10 X increase

Heritable Thrombophilia
1965 AT mutation identified [Egeberg et al]
1967 Dysfunctional fibrinogen [Egeberg et al]
1981 Protein C [Griffin et al]
1984 Protein S [Comp et al]]
1993/4 APCr/FV L [Dalhback/Bertina et al]
1996 Prothrombin mutation [Poort et al]

Heritable Thrombophilia
• FVL and Prothrombin gene mutation are the most common genetic abnormalities occurring in patients with VTE (Seligsohn et al’ NEJM 2001)
• One or more of these abnormalities occur in about 50% of patients with first VTE (Christiansen et al, JAMA 2005)

Thrombophilia Prevalence
Risk factor Subjects with thrombosis (%)
General population (%)
Relative Risk of Thrombosis
Antithrombin 1 0.2 25-50
Protein C 3 0.3 10-15
Protein S 2-3 0.2 11
Factor V LeidenHetero
20-50 3-15 3-8/80 Homo
Prothrombin 3' UTR mutation
Hetero
6 2 3

Multi-Casual Model
• The thrombotic event is the result of gene- gene interaction and/or gene-environment interaction.
Variable RR Annual Incidence%Normal 1 0.008Hyperhomocysteinemia 2.5 0.02Prothrombin G20210A 2.8 0.02Oral contraceptives 4 0.03Factor Leiden heterozygote 7 0.06OCT and Factor Leiden 35 0.3Factor Leiden homozygote 80 0.5-1

Thrombophilia screening: first-line tests
Coagulation screen APTT, PT, TT
Antithrombin activity Chromogenic assay
Protein C Chromogenic assay
Protein S Immunoreactive (free ± total)
Modified APC/SR Predilution in FV-deficient plasma
Factor V Leiden PCR
Prothrombin G20210A PCR
APC/SR, activated Protein C sensitivity ratio; APTT, activated partial thromboplastin time; prothrombin time;TT, thrombin time

Lab Evaluation
• Risks, benefits and limitations should be discussed• Patient should be consented• It may has uncertain predictive value of
recurrence (anxiety)• Negative test does not exclude an increased risk
of VTE (false reassurance)• Repeat testing for identification of abnormality is
indicated• Interpretation is difficult

Lab Evaluation
• Timing:– Acute thrombotic event, chronic inflammatory
conditions, pregnancy, liver disease, DIC, OCP or anticoagulant therapy will affect the results of functional assays
– 14 days after the discontinuation of oral anticoagulation therapy

Who Should we Test? (NICE & BJH-2010)
• Do not offer testing to patients who have had provoked VTE
• Do not offer thrombophilia testing to patients during acute VTE or who are continuing anticoagulation treatment

Who Should we Test? (NICE & BJH-2010)
• Consider testing in patients (selected) who have had unprovoked VTE, less than 40 yrs and who have a first degree relative who has had VTE if it is planned to stop anticoagulation treatment
• Children with purpura fulminans• Skin necrosis due to warfarin

Contents
• Introduction• Heritable Thrmbophilia• Effect on management• Summary

Treatment
• Initial management of acute thrombosis is the same for patients with and without inherited thrombophilia– Anticoagulation with warfarin for 3-6 months– There is no evidence that heritable thrombophilia
should influence the intensity of therapy (Schulman & Tengborn, TH 1992; Kearon et al, Blood 2008)

Recurrent VTE
• The risk for recurrent VTE after major factor related VTE is 1-3% patient per year
• Slightly higher for minor factor related VTE• For unprovoked VTE the risk is 5-15% per year,
up to 30-35% after 5 years (Iorio et al, AIM 2010; Douketis et al, AIM 2010; Eichinger et al, Circulation 2010; Prandoni et al, Hematologica 2007)

Cambridge Venous Thrombo-embolism Study (CVTE) (2003)
• Two year Prospective Study:– 570 patients– Recurrence rate was 11%• Lowest incidence after surgery related VTE (0%)• Highest incidence with un-precipitated VTE
(19.4%)

Cambridge Venous Thrombo-embolism Study (CVTE) (2003)– 85% of patients were tested for heritable
thrombophilic defects→ recurrence rates were not related to presence or absence of heritable thrombophilia.
– CONCLUSION: Thrombophilia testing had no predictive value for reoccurrence
Baglin et al. The Lancet 2003.

Leiden Thrombophilia study (LETS) JAMA 2005
• Prospective follow up study of LETS pts– 447 patients followed for a mean of 7.3 years– Incidence rate of recurrence was highest during the first two
years: annual rate of 3.2%; cumulative recurrence of 12.4% at 5 years• Risk of recurrence was 2.7 x higher in men than women (95% CI
, 1.8-4.2)• Higher risk of recurrence with idiopathic initial VTE• Lower risk of recurrence with provoked initial VTE• OCT use during follow up had a higher recurrence rate (28 per
1000 pt-yrs vs 12.9 per 1000 pt-yrs)

Leiden Thrombophilia study (LETS) JAMA 2005
• Conclusion:– Clinical factors (male sex, use of OCT’s, idiopathic
initial VTE) have a more significant role in risk of reoccurrence than lab abnormalities
(Christiansen et al, JAMA 2005)

Thrombophilia and Recurrent VTE
• Retrospective analysis showed detection of natural anticoagulants deficiency in selected patients predicted a risk of recurrence of 6.2% compared to 2.2% in patients with FVL or Prothrombin gene mutation (Lijfering et al, Blood 2009)
• In general the risk of recurrence is uncertain and it is low if first event was provoked (Cohn et al, CDSR 2009)

Guidelines ACCP 2008
• The presence of hereditary thrombophilia has not been used as major factor to guide duration of anticoagulation for VTE because evidence from prospective studies suggests that these factors are not major determinants of the risk of recurrence

Predicting Disease Recurrence- DASH(Tosetto, JTH 2012)
• 1818 with unprovoked VTE treated with warfarin for 3 months analyzed and followed up for 5 years

Predicting Disease Recurrence- DASH(Tosetto, JTH 2012)
Multivariate Score
D-dimer-abnormal 2
Age-less than 50 1
Sex-man 1
Hormonal associated VTE
-2

Predicting Disease Recurrence-DASH (Tosetto, JTH 2012)
• May be useful to decide whether therapy should be continued indefinitely (if score more than 1) or stopped after 3 months (if score 1 or less)
• Independent validation is required in separate population

D-dimer to guide the duration of therapy (DULCIS, Blood 2014)
• Multicentre prospective study• 1010 patients with unprovoked VTE• 2 years follow up

D-dimer to guide the duration of therapy (DULCIS, Blood 2014)

D-dimer to guide the duration of therapy (DULCIS, Blood 2014)
• D-dimer can be considered as an independent factor of VTE recurrence
• Serial measurement is suitable in clinical practice

D-dimer
• Potential need for gender specific and age specific D-dimer cut points (Legnani et al, IEM 2011)
• Additional research is needed

Men and HER DOO2
• Prospective cohort of patients with first unprovoked VTE
• All men are considered at high risk of recurrence

Men and HER DOO2
• For women >=2 factors (comprising lower extremity hyperpigmentation, edema, redness, D-dimer >=250 ng/ml [during therapy], obesity [body mass index >=30 kg/m2] and age over 65 years) identifies women at high risk for recurrent VTE
(Le Gal et al, TH 2010; Rodger et al, CMAJ 2008)

Residual Vein Occlusion
• Lack of a standard definition for RVO and the potential for operator variability in the interpretation of US findings
• Detected in at least 40% of patients at 3-6 months treatment
• Poor predictor of VTE recurrence
JTH 2011AJH 2011TH 2011EJVES 2010Blood 2014

Risk Factors of VTE Recurrence
1. Mode of initial presentation2. Patient’s gender3. D-dimers4. Age5. ? Thrombophilia
Baglin et al, 2003; Douketis et al, BMJ 2011; DULCIS, Blood 2014

Duration of Therapy
• Depends on the presence or absence of risk factors of VTE recurrence
• The benefit of continued therapy needs to be balanced against the risk of therapy related bleeding (Schulman et al, Chest 2008)
• Annual risk for therapy related bleeding is 1-3% with 0.3% associated with major hemorrhage (Schulman et al, Chest 2008)

Factors that increase the risk of VKA-related bleeding (Scientifica 2012)
Treatment related Patient related
First 3 months of therapy Advanced age (>75 years)
Actual INR values > 4.5 Frequent falls
Low quality of anticoagulation monitoring History of major bleeding
Uncontrolled hypertension
Renal or liver failure
Associated antiplatelet therapy
Drugs
Poor compliance
Absence of familial or social support
Recent surgery
Cancer

HAS-BLED score (Lip et al, JACC 2011)
Risk factors Score for each risk factor
Total score Major bleeding events (% patients) in relation to the total score
None / 0 0.9
Hypertension 1 1 3.4
Abnormal renal or liver function
1 each 2 4.1
Stroke 1 3 5.8
Bleeding history or predisposition
1 4 8.9
Labile INR 1 5 9.1
Age > 65 years 1 6 /
Drugs/alcohol concomitantly
1 each / /

HAS-BLED
• HAS-BLED score has been developed for patients with AF who are generally elderly (Pisters et al, Chest 2010)
• It needs to be studied in VTE patients

Guidelines ACCP 2012
• Recommend at least 3 months treatment for unprovoked DVT
• Suggest to evaluate for the risk-benefit ratio of extended therapy
Extended Therapy
• Periodic reassessment:1. Patient’s bleeding risk2. Patient’s values and preferences3. New research findings

Contents
• Introduction• Heritable Thrmbophilia• Effect on management• Summary
Summary
• Inherited thrombophilia can be found in up to 50% of VTE cases
• Only selected pts should be tested• Laboratory testing should be done at right
time and results should be interpreted with caution

Summary
• Initial management is not different from non inherited thrombophilia
• Risk of recurrence should be identified for unprovoked VTE
• Duration of therapy is determined largely by clinical factors and patients preferences

Suggested management Clinical condition ManagementSecondary* isolated distal DVT 6 weeks AC#
Unprovoked isolated distal DVT 3 months ACSecondary proximal DVT and/or PE 3–6 months ACUnprovoked first proximal DVT and/or PE 3–6 months AC, then stratify for
individual risk of recurrence
Life-threatening PE as index event Consider extended£ ACVTE associated to active cancer AC until cancer is no longer activeUnprovoked VTE associated with antiphospholipid syndrome or antithrombin deficiency
Extended AC
Unprovoked VTE associated with other major thrombophilic alteration (protein C or S deficiency, homozygous factor V Leiden or G20210A prothrombin mutation or double heterozygous)
Consider extended AC
Second unprovoked VTE Extended AC

Thank you