three new cases of spondylocarpotarsal synostosis syndrome: clinical and radiographic studies
TRANSCRIPT
Three New Cases of Spondylocarpotarsal SynostosisSyndrome: Clinical and Radiographic Studies
Katia-Edni F.A. Coelho,1,2,4* Ester S. Ramos,1 Temis M. Felix,1,3 Lucia Martelli,1João M. de Pina-Neto,1 and Norio Niikawa4
1Departamento de Genetica, Faculdade de Medicina de Ribeirao Preto, Universidade de Sao Paulo,Ribeirao Preto, Brazil
2Setor de Patologia-Genetica, Hospital Sarah-Salvador, Salvador-Bahia, Brazil3Unidade de Genetica Medica do Hospital de Clinicas de Porto Alegre, Porto Alegre, Brazil4Department of Human Genetics, Nagasaki University School of Medicine, Nagasaki, Japan
Spondylocarpotarsal synostosis syndrome(SSS) or congenital synspondylism is a re-cently delineated clinical entity. At least 15patients have been reported. We present 3new patients, 2 of whom were sibs born tofirst-cousin parents. All of our patients hadmultiple synostoses involving cervical, tho-racic and/or lumbar vertebral bodies andcarpal/tarsal bones, scoliosis/lordosis, andshort stature. Sensorineural deafness wasfound in 2 of the 3 patients. Analysis of clini-cal manifestations suggests clinical vari-ability and genetic heterogeneity in SSS. Ofa total of 18 SSS patients, 10 were five pairsof sibs from five families, with first-cousinconsanguinity of parents in 3, indicatingthat at least one type of SS is an autosomal-recessive disorder. Am. J. Med. Genet. 77:12–15, 1998. © 1998 Wiley-Liss, Inc.
KEY WORDS: spondylocarpotarsal synos-tosis syndrome; vertebralanomalies; carpal and tarsalsynostosis; short stature;hearing loss
INTRODUCTION
Simultaneous occurrence of carpal and vertebralsynostosis is relatively rare. Spondylocarpotarsal syn-ostosis syndrome (SSS), first described by Langer andMoe [1975], also called congenital synspondilism[Wiles et al., 1992], is one such occurrence. SSS is char-acterized by carpal and tarsal synostoses, symmetricalblock-vertebrae, scoliosis or lordosis due to a failure of
normal spinal segmentation, and short stature withshort trunk. Sensorineural or mixed hearing loss is oneof the variable manifestations. At least 15 SSS patientsfrom 10 families are known [Jones et al., 1973; Langerand Moe, 1975; Akbarnia and Moe, 1978; Ventruto andCatani, 1986; Hunter et al., 1992; Wiles et al., 1992;Langer et al., 1994]. The cause of the disorder is un-known, although autosomal-recessive inheritance hasbeen suggested. This paper deals with 3 new patientsfrom two families. Their clinical, roentgenographic,and audiological findings are described, together with apossible inheritance mode.
CLINICAL REPORTSPatient 1
I.L.T. (Fig. 1a, III-2), a Brazilian girl, was first seenby us at age 2 years because of her short stature (Fig.2a). The infant was born at term by cesarean section,with a birth weight of 2,700 g and length of 46 cm, to a37-year-old, gravida 3, para 2, ab 1 mother and ahealthy father. The parents are not consanguineous.Physical examinations of the patient at age 5 yearsshowed that her height was 91.5 cm (<3rd centile), in-ner canthal distance 30 mm (50–75th centile), outercanthal distance 85 mm (75–97th centile), OFC 49.5
*Correspondence to: Dr. Katia-Edni F. Albuquerque Coelho,Setor de Patologia-Genetica, Hospital Sarah-Salvador, Av. Tan-credo Neves 2.782 STIEP, Salvador-Bahia, CEP 41.820/900,Brazil.
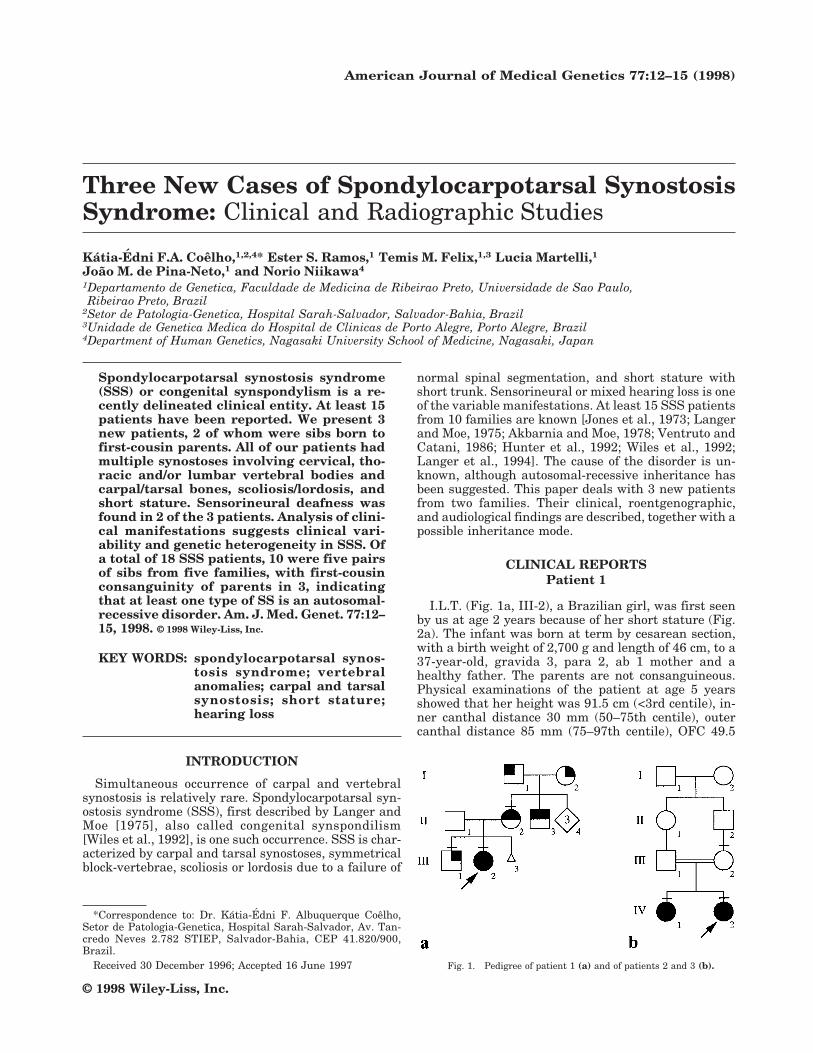
Received 30 December 1996; Accepted 16 June 1997 Fig. 1. Pedigree of patient 1 (a) and of patients 2 and 3 (b).
American Journal of Medical Genetics 77:12–15 (1998)
© 1998 Wiley-Liss, Inc.

cm, and arm span 86 cm. She had a short neck withlimited movements, kyphoscoliosis with vertebralprominence in the cervical and thoracic regions, mildarticular limitation at the elbow joints, bilateralbrachydactyly, clinodactyly of the fifth finger, andsmall hands and feet with a gap between the halluxand the second toe. Psychomotor development was nor-mal. A systolic murmur was heard. Roentgenographyof the spinal column showed fusion of spinous pro-cesses between C2 and C3 with a reduced space be-tween C2/C3, thoracic scoliosis convex to the right, andfusions of vertebral bodies from T6–T8 which showedmultiple symmetrical block-appearing vertebrae in thethoracic spine (Fig. 3a). Hand films demonstrated fu-sion of the capitate and hamate, and hypoplasia ofmiddle phalanges (Fig. 4a). Her carpal bone age at 4years was retarded, corresponding to 2 years. Electro-cardiogram and echocardiogram were normal. Laryn-gological and audiometric examinations demonstratedbilateral moderate sensorineural deafness.
The mother (Fig. 1a, II-2) was short (140 cm) and hadbilateral brachydactyly and a suprarenal enlargement.Radiography showed that the spine, hands, and feetwere all normal except for generalized short digits. Au-diometry was normal as well. The father’s height wasnormal. An 8-year-old brother (Fig. 1a, III-1) had shortstature (110 cm, <3rd centile), but was otherwise nor-mal on physical examination. Several maternal rela-tives were short and had brachydactyly. A brother (Fig.1a, II-3) of the mother was short (150 cm) and hadbrachydactyly. The father of the patient (Fig. 1a, II-1)was 170 cm tall and had normal skeletal bones, and hismother (or patient’s grandmother) was 150 cm tall.
Patient 2
A.A.G. (Fig. 1b, IV-2), a Brazilian girl, was born tofirst-cousin parents at term with a birth weight of2,890 g and length of 48 cm. Psychomotor developmentwas normal. Physical examinations at age 9 6/12 yearsshowed a height of 109.5 cm (<3rd centile), lower seg-ment 57 cm, arm span 113.5 cm, OFC 51.5 cm (2–50thcentile), inner canthal distance 30 mm (75th centile),and outer canthal distance 89 mm (50–70th centile).Other findings included malocclusion and enamel hy-poplasia of teeth, short and wide trunk (Fig. 2b), tho-racic/lumbar scoliosis convex to the left, lumbar lordo-sis, and bilateral clinodactyly of the fifth fingers. Skel-etal radiography showed a decreased interdisc spacebetween C4/C5 with a fusion of spinous processes, ver-tebral fusion from T6–T11, scoliosis and lordosis, spinabifida at L4/L5 and L1/L2 (Fig. 3b), and fusions of thecapitate/hamate and lunate/triquetrum (Fig. 4b). Car-pal bone age was 8 9/12 years (chronological age, 9 4/12years). Echocardiogram, audiogram, and ear-polytomogram were all normal.
Patient 3
P.A.G. (Fig. 1b, IV-1), an older sister of patient 2, wasborn at term after a normal pregnancy. Birth weightwas 3,010 g and length 47 cm. Psychomotor develop-ment was normal. Physical examinations at age 105/12 years showed that her height was 120 cm (<3rdcentile), lower segment 62 cm, arm span 123 cm, andOFC 54.5 cm (50–98th centile). The following abnor-malities were observed: apparent hypertelorism with
Fig. 2. a: Patient 1 at age 5 years, showing short stature with shorttrunk and short neck. b: Patient 2 at 9 years (right) and patient 3 at 10years (left), exhibiting short stature.
Fig. 3. Spinal column of patients1 (a), 2 (b), and 3 (c).
Spondylocarpotarsal Synostosis 13

an inner canthal distance of 34 mm (75–97th centile),outer canthal distance of 95 mm (97th centile), incom-plete development of the scapha helices, irregular in-sertions and enamel hypoplasia of teeth, short andwide trunk (Fig. 2b), a systolic murmur, scoliosis thathad been surgically corrected, bilateral clinodactyly,and flat feet. X-ray examinations showed morphologicalterations of cervical vertebrae without fusion, tho-racic scoliosis convex to the right, fusions and spina
bifida of vertebrae T3–T11, a decreased interdisc spaceat L3–S1 (Fig. 3c), and a fusion of the capitate andhamate (Fig. 4c). Electrocardiogram documented sinustachycardia, a ventricular septal defect, and conductivedisturbance in the right bundle branch. Echocardiog-raphy demonstrated anterior mitral prolapse. Audio-gram showed bilateral sensorineural deafness in acutesounds.
The mother was 155 cm tall with normal radio-
TABLE I. Comparison of Clinical Manifestations in 15 Reported Cases With Those in Our 3 Patients
Manifestations
Joneset al.[1973]
Langerand Moe
[1975]
Ventrutoet al.[1986] Hunter
et al.[1992]
Wiles et al.[1992] Langer et al. [1994]
Ourpatients
No. ofpatients
(totalof 18)1 2 1 2 1 2 3 1 2 3 4 5 6 1 2 3
Sex M M F M M M M M F F F F F M F F F FNormal intelligence + + + + + + + + + + + + + + + + + + 18Thoracolumbar fusion + + + + + + + + + + + + + + + + + 17Carpal synostosis + + + + + + + + + + + + + + + + 16Short stature + + + + + + + + + + + + + + + + 16Short trunk + + + + + + + + + + + + + + 14Scoliosis + + + + + + + + + + + + + + + 14Lordosis + + + + + + + + + + + + + 13Cervical fusion + + + + + + + + + + 9Narrowed intervertebral space + + + + + + + + + 9Fusion of spinous process + + + + + + + + + 9Flatfoot + + + + + + + + + 9Deafness + + + + + + + 7Hypertelorism + + + + + + + 7Tarsal synostosis + + + + + + 6Kyphosis + + + + + + 6Clynodactyly of fifth finger + + + + + + 6Dysmorphic face + + + + + + 6Joint mobility limitation + + + + + 5Short neck/mobility limitation + + + + + 5Defective dentition/enamel + + + + + 5Delayed bone age + + + + 4Brachydactyly/short phalanx + + + + 4Ear anomaly + + + + 4Sacral anomaly + + + 3Gap between first and second toes + + + 3Congenital heart disease + + + 3Clubfoot + + 2Hyperextension of joint + + 2High/narrow palate/cleft
uvula/palate + + 2Inguinal hernia + + 2Renal anomaly + + 2Bowed humerus + 1Metatarsus aductus + 1Glenoid hypoplasia + 1
Fig. 4. Hand radiographs of pa-tients 1 (a), 2 (b), and 3 (c), showingfusion between capitate/hamate, and/or between lunate/triquetrum.
14 Coelho et al.

graphic findings of the skeleton. The father was notavailable for examination.
DISCUSSION
Diagnosis of SSS in our patients was made on thebasis of their clinical manifestations. The manifesta-tions common to the 3 patients included cervical andthoracic block-appearing vertebrae, scoliosis and/or lor-dosis, carpal and tarsal synostosis, clinodactyly of thefifth fingers, retarded bone age, and short stature, allfitting the cardinal manifestations of the syndrome(Table I). Other abnormalities, including limitation ofelbow joint movement in patient 1, hypertelorism andtooth anomalies in patients 2 and 3, and congenitalheart disease and hearing impairment in patients 1and 3, were less frequent among those in 15 previouslyreported SSS patients [Langer et al., 1994]. It is likelythat the short stature and brachydactyly seen in pa-tient 1 were not only attributable to SSS but also toanother condition in the maternal family, becausesome relatives also had these abnormalities (Fig. 1a).Forney et al. [1966] reported 3 patients in a family, whorepresented a similar combination of clinical manifes-tations, such as short stature, vertebral abnormality,hearing loss, and heart defects. However, the vertebrallesions in their patients were restricted to a cervicalregion and were much less severe than those in ourpatients. Moreover, a parent-child transmission with aprobable autosomal-dominant mode was observed inthe family of Forney et al. [1966]. Therefore, the disor-der of their family is likely different from that in ourcases. Both spondylocostal and/or spondylothoracicdysplasia [Ayme and Preus, 1986] and Klippel-Feilsyndrome [Guille et al., 1995] were ruled out, since ourpatients had no rib anomalies but had vertebral in-volvement extending to the thoracic/lumbar columnand carpal/tarsal synostoses.
Spondylocarpotarsal synostosis syndrome or congen-ital synspondilism is a recently delineated clinical en-tity [Wiles et al., 1992; Langer et al., 1994]. A total of 18patients with the disorder is known [Jones et al., 1973;Langer and Moe, 1975; Akbarnia and Moe, 1978; Ven-truto and Catani, 1986; Hunter et al., 1992; Wiles etal., 1992; present patients]. The main findings in thedisorder are 1) fusions of cervical, thoracic, or lumbarvertebral bodies with or without unilateral unseg-
mented bar, 2) carpal and/or tarsal synostosis, 3) shortstature, and 4) scoliosis and/or lordosis (Table I). Ver-tebral involvement, which is usually severe and maycause disproportionally short trunk/stature, is not as-sociated with any rib anomalies. Occasional manifes-tations include hearing impairment, limitation oflarge-joint movement, tooth anomalies, brachydactyly,and minor facial anomalies. Among them, hearing im-pairment tends to be overlooked, since it was found inour 2 patients by focused examinations. Thus, we rec-ommend audiological assessments of all patients withvertebral anomalies.
The cause of SSS remains unknown. Of a total of 18patients, 10 were five sib pairs from five families inwhich three couples of parents were first cousins. Thesex ratio of the 10 familial cases was even. The dataindicate that at least one type of SSS is an autosomal-recessive disorder.
REFERENCESAkbarnia BA, Moe JH (1978): Familial congenital scoliosis with unilateral
unsegmented bar. Case report of two siblings. J Bone Joint Surg [Am]60:259–261.
Ayme S, Preus M (1986): Spondylocostal/spondylothoracic dysostosis: Theclinical basis for prognosticating and genetic counseling. Am J MedGenet 24:599–606.
Forney WR, Robinson SJ, Pascoe DJ (1966): Congenital heart disease,deafness, and skeletal malformations: A new syndrome? J Pediatr 68:14–25.
Guille JT, Miller A, Bowen JR, Forlin E, Caro PA (1995): The naturalhistory of Klippel-Feil syndrome: Clinical, roentgenographic, and mag-netic resonance imaging findings at adulthood. J Pediatr Orthop 15:617–626.
Hunter A, Farrell S, MacLeod P, Gillies C (1992): Abnormal vertebralsegmentation and carpal bone fusions. Dysmorphol Clin Genet 6:93–98.
Jones KL, Guthrie RD, Smith DW (1973): Case report 8. Syndrome Iden-tification I(2):10–11.
Langer LO, Moe JH (1975): A recessive form of congenital scoliosis differ-ent from spondylothoracic dysplasia. BD:OAS 11(6):83–86.
Langer LO, Gorlin RJ, Donnai D, Hamel BCJ, Clericuzio C (1994): Spon-dylocarpotarsal synostosis syndrome (with or without unilateral un-segmented bar). Am J Med Genet 51:1–8.
Prata MF, Liberal MI, Gonçalves V, Maroteaux P, Magalhaes J (1984):Acrodysplasia (hands and feet) with scoliosis, by autosomal recessivetransmission. Ann Genet (Paris) 27:233–236.
Ventruto V, Catani L (1986): New syndrome: Progressive scoliosis by uni-lateral unsegmented fusion bar, foot deformity, joint laxity, congenitalinguinal herniae, peculiar face. Am J Med Genet 25:429–432.
Wiles CR, Taylor TFK, Sillence DO (1992): Congenital synspondylism. AmJ Med Genet 42:288–295.
Spondylocarpotarsal Synostosis 15