thr on ddh crowe iv technique and long term outcome m. kerboull
TRANSCRIPT

THR ON DDH CROWE IV
Technique and long term outcome
M. KERBOULL

• Luxation intermédiaire ou postérieure
• Class IV of Crowe
• Type C or D of Eftekhar
• Total dislocation of Hartofilakidis or Harris
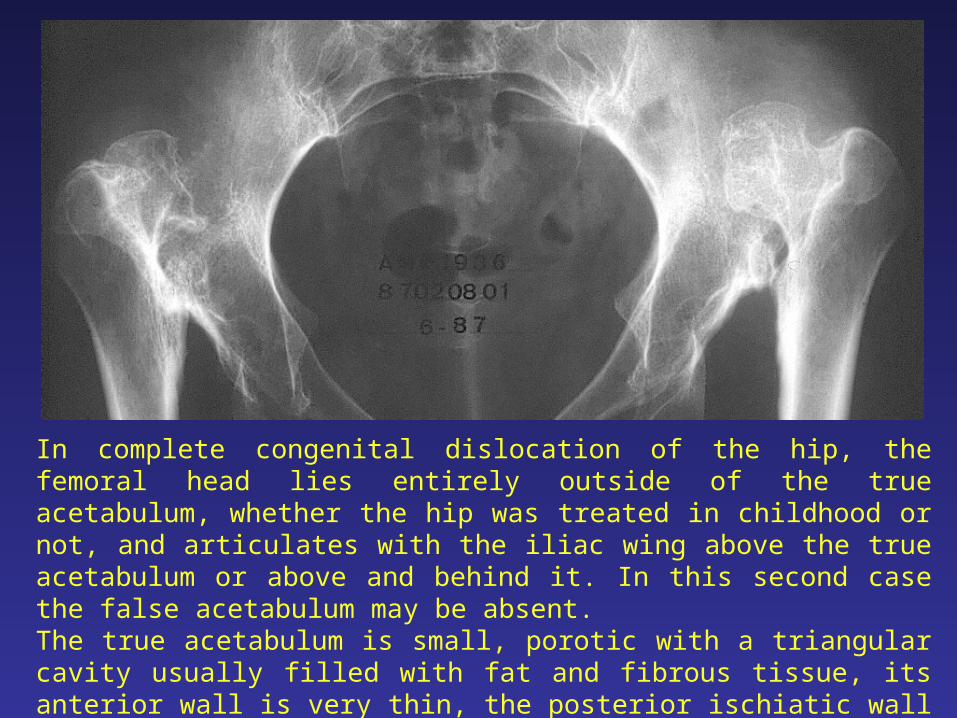
In complete congenital dislocation of the hip, the femoral head lies entirely outside of the true acetabulum, whether the hip was treated in childhood or not, and articulates with the iliac wing above the true acetabulum or above and behind it. In this second case the false acetabulum may be absent.The true acetabulum is small, porotic with a triangular cavity usually filled with fat and fibrous tissue, its anterior wall is very thin, the posterior ischiatic wall thick. The femur is also dysplastic with a narrow medullary canal, a small head, an anteverted neck, but its length is normal.

This distorted anatomy may be worsened by previous operations, especially by diaphyseal valgus osteotomy.

There are also many secondary anatomical abnormalities. The capsule is elongated, extending from the rim of the true acetabulum to the femoral head and sometimes surrounding it.
Because of the high and posterior riding head, the course of nerves and arteries is altered, but they are not actually shortened. When the hip was never operated, the muscles are not substantially contracted. Some, such as external rotators, are even elongated, but their courses are also altered.

The abnormal location of the hip and the frequent asymmetry of the dislocation result in several anatomical and physiological changes: leg length discrepancy, pelvic tilt, structural changes in the lumbo-sacral spine, malalignment of the ipsi lateral knee.

NUMEROUS VARIETIES
OF DDH CROWE IV

Unilateral dislocation with contro lateral hip normal or dysplasticShortening = leg length discrepancyPelvis horizontal Lumbar spine vertical

Bilateral symmetrical dislocationRelatively rareNo leg length discrepancyPelvis horizontalLumbar spine vertical

Asymmetric bilateral dislocationMuch more frequentLeg length discrepancyPelvic tiltLateral bend of the lumbar spineCompensating for pelvic tilt

Pelvic tilt increased by the femoralabduction osteotomy
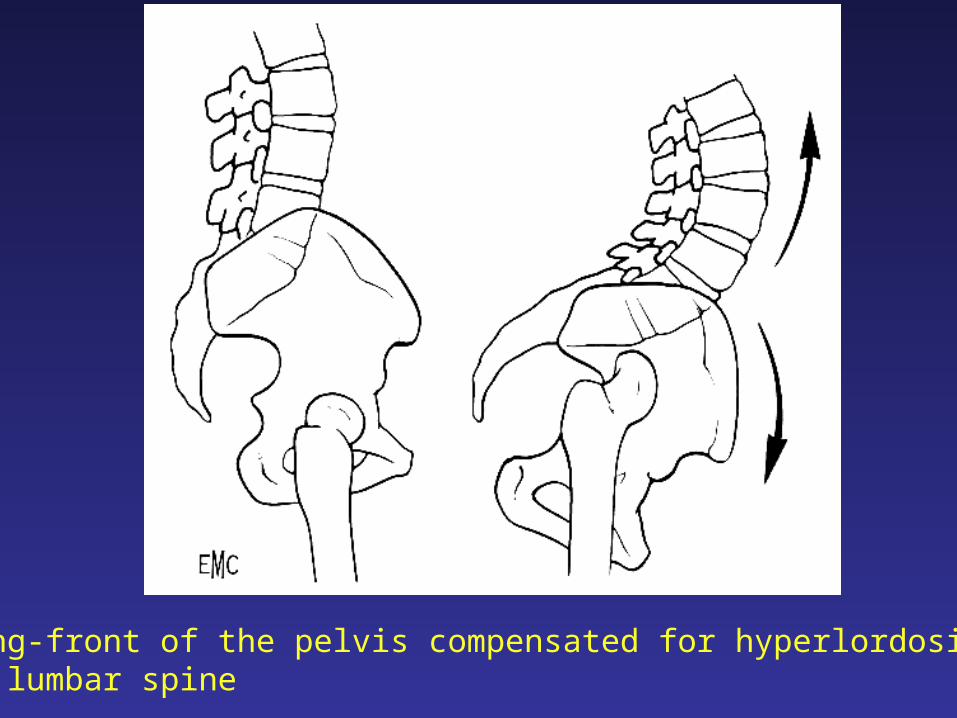
Swing-front of the pelvis compensated for hyperlordosis of the lumbar spine

Frontal asymmetry of the pelvis in unilateral or bilateralasymmetrical dislocations

Lateral bend of the lumbar spine with arthrosis

Anatomic genu valgum increased by sequelae of ostechondritis or femoral proximal angulation

3 GOALS
THA in this field aims at:
• Providing the patient with 1 or 2 pain free, mobile and stable hips
• Equalizing the leg length
• Relieving the low back pain and knee pain through improving of the static body balance
SURGICAL TECHNIQUE

SURGICAL TECHNIQUE
OPERATIVE PLANNING
• Measure of the leg shortening
• Choice of the prosthetic components
• Implantation seats of the components
• Possible necessity of an alignment osteotomy

Measure of leg shortening due to hip dislocation
1) On a radiograph of the lower part of a body without magnification taking on a single film pelvis and lower limbs on a standing position.
2) On AP x-rays of the hip taking into account magnification coefficient
R = H x 0,85
A = h x 0,85
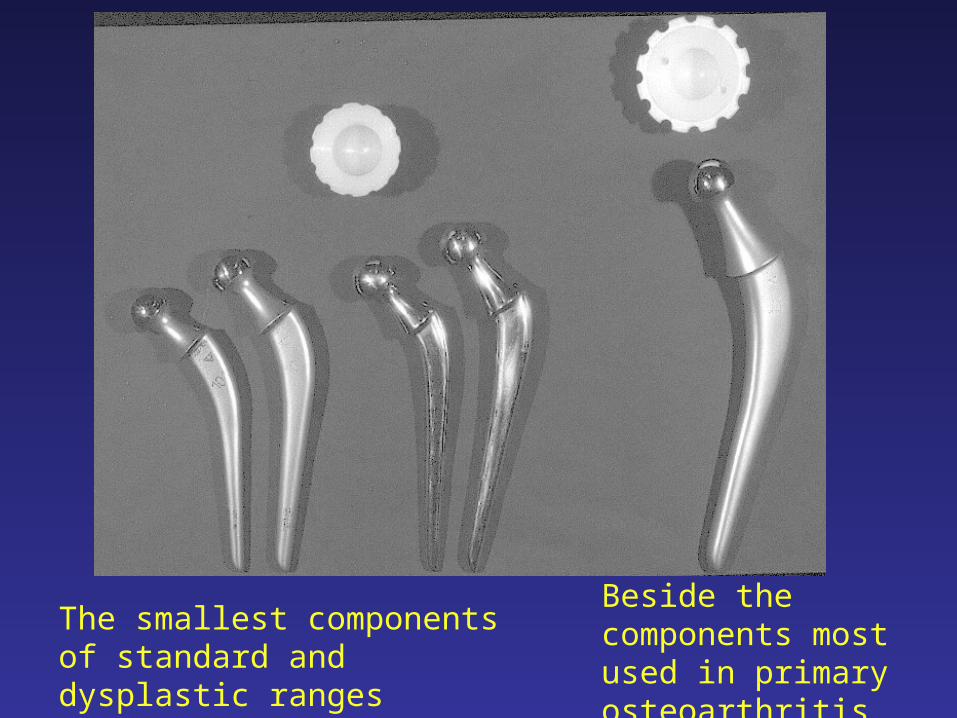
The smallest components of standard and dysplastic ranges
Beside the components most used in primary osteoarthritis

Preoperative planning with component seats

This femoral angulation will need an alignment osteotomy

OPERATIVE TECHNIQUE MAIN POINTS
• Lateral transtrochanteric approach• Complete excision of the capsule, scar fibrous tissue,
osteophytes, shelf.• Neither muscle nor tendon section• Acetabular reconstruction in anatomic position• Femoral component implantation at the level of the
lesser trochanter to avoid any difficulties due to excessive anteversion
• Reduction on a limb in adduction, the hip slightly flexed, knee flexed at 90°, by direct thrust on the neck

Bilateral dislocation
Bilateral THR with reconstruction of the acetabuli augmented by autograft in anatomic position.Insertion of a femoral component at the lesser trochanter level.

MAIN STEPS
OF THE OPERATION

Lateral decubitus position
Lateral transtrochanteric approach
Excision of the superior and lateral capsule

Section of the neck
Dissection and excision of the inferior and medial capsule

Deepening and widening of the true acetubulum at the expenses of ischiatic wall
Augmentation of the deficient acetabulum with a structural autograft secured with 2 screws

Cementation of the acetabular component

A diaphyseal femoral angulation may complicate the operation

The alignment osteotomy is doneat the top of the femoral angulation.Pure alignment osteotomy.
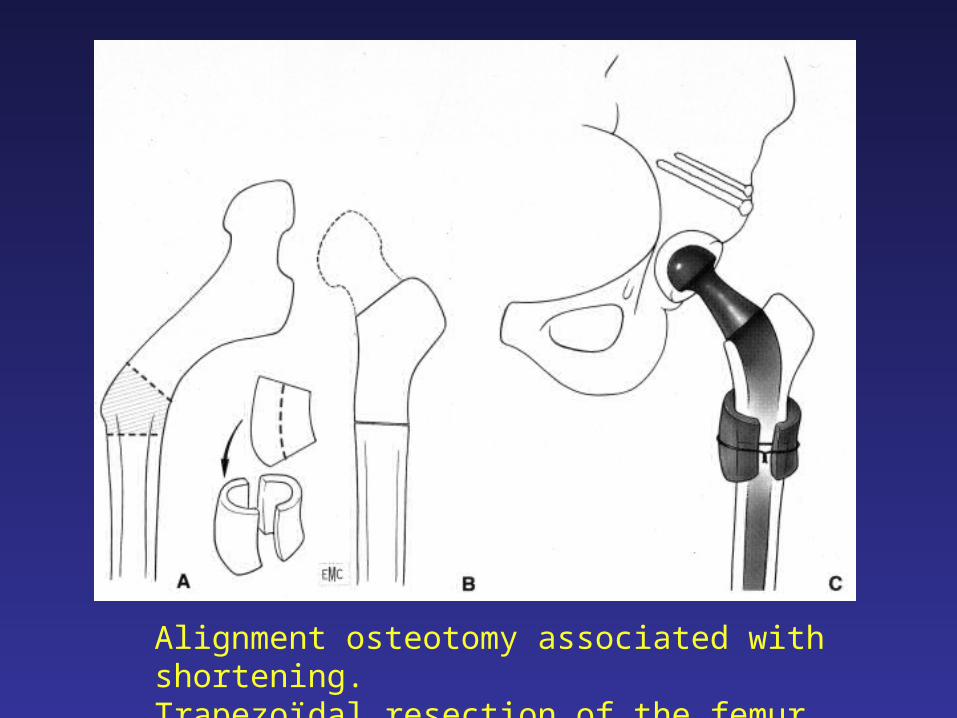
Alignment osteotomy associated with shortening.Trapezoïdal resection of the femur

Stair-step osteotomy to block fragments rotation for alignment of the femur with resection

Left femoral angulation aligned with osteotomy. The result 18 years PO

Inter trochanteric angulation.Implantation of the femoral component in the focus of angulation and remodelling of the proximal femur, by removing a triangular grey bone fragment, to give it a normal anatomy.

SOME EXAMPLES
WITH LONG TERM RESULTS
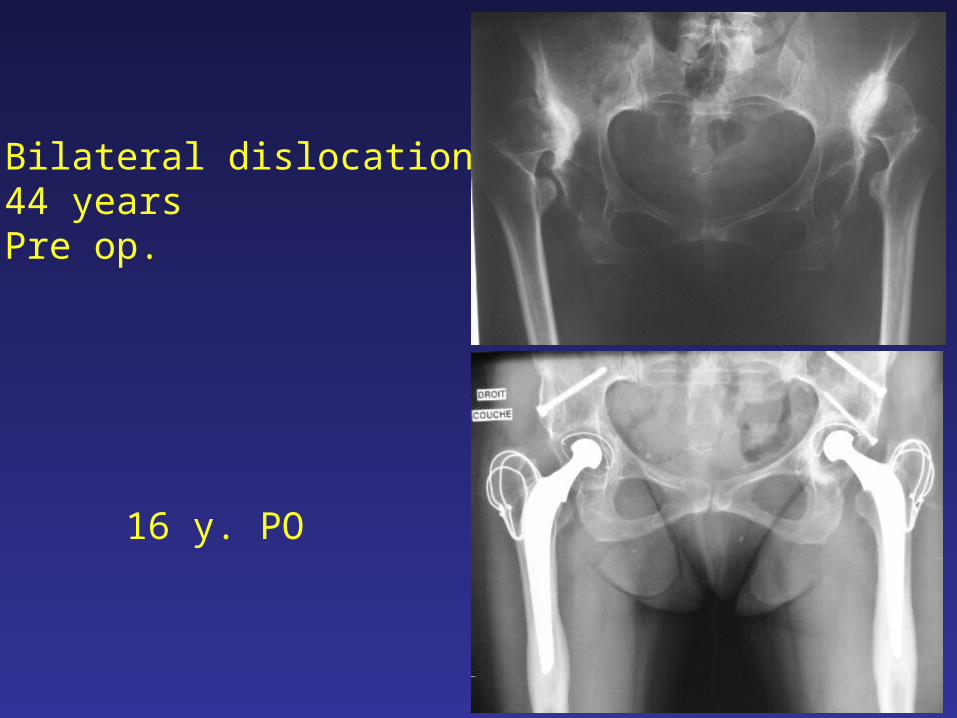
Bilateral dislocation44 yearsPre op.
16 y. PO
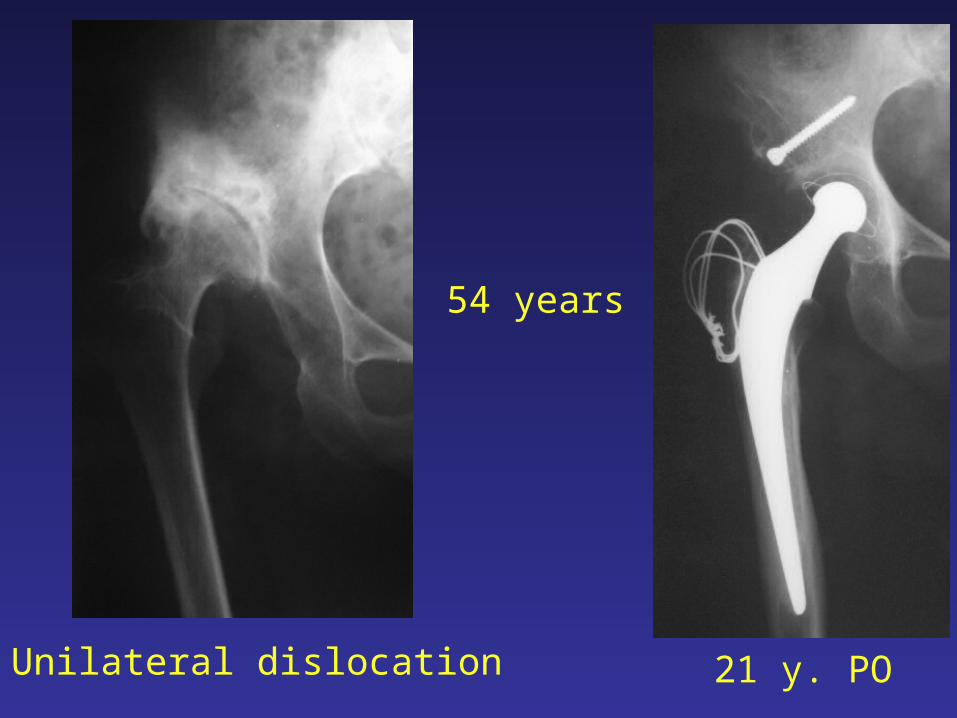
54 years
Unilateral dislocation 21 y. PO

42 years
Unilateral dislocation 22 y. PO

48 years
Posterior dislocation5 y. PO 18 y. PO

19 y. PO 3 years after reoperation

41 years
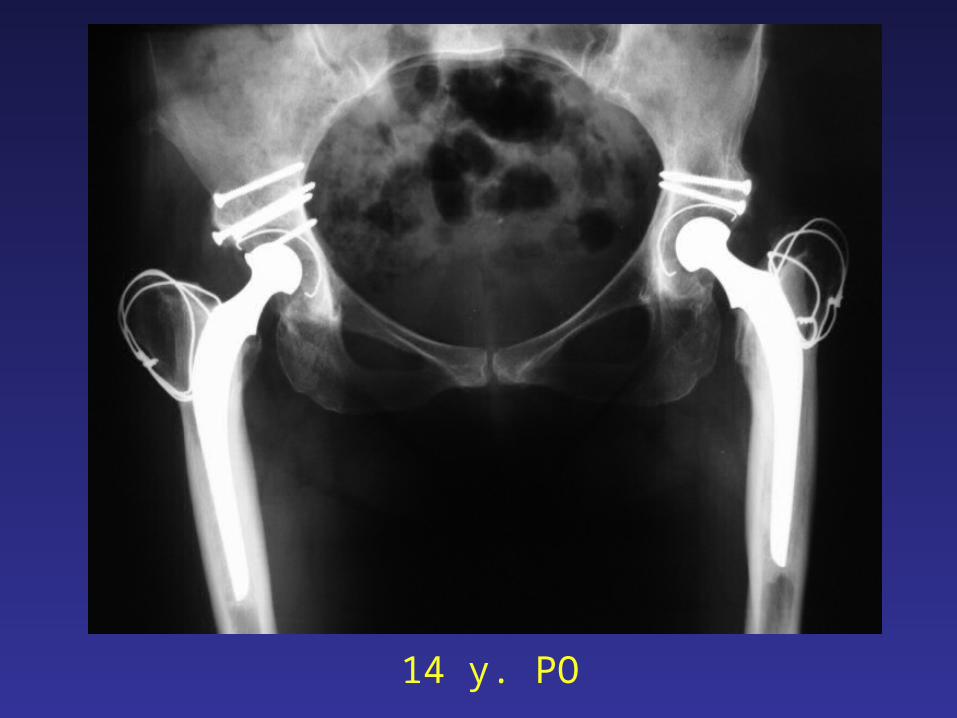
14 y. PO

16 y. PO

18 y. PO

RH: 3 years after reoperation LH: 21 y. PO

RH: 6 years after reoperationBreak of the screws
LH: 24 y. PO

RH: 1 year after second reoperation LH: 25 y. PO

On an one surgeon series of 535 THA on DDH with 352 on Crowe IV, operated on between 1969 and 2004, the first 118 on Crowe IV were many times studied and published in Journal of Arthroplasty.

MATERIAL
• 89 PATIENTS (8 Men, 81 women) Average age 52 years (29-78)
• 119 HIGH DISLOCATIONS30 bilateral59 unilateral, with a contro lateral hip
- Crowe II and III (15)- dysplastic (23)- normal (21)

MATERIAL
• 118 THA Carried out between 1970 and 1986
10 Original Charnley (narrow stem)108 Charnley-Kerboull
CONTINUOUS SERIESONE SURGEON

MATERIAL
• 39 patients no previous operation• 59 previous operation (average 2,22)
- Attempt of closed reduction 27- Attempt of open reduction 11- Shelf operation 32- femoral osteotomy 23- Girdlestone 8- Arthrodesis 1- Arthroplasties (cup, acrylic …) 9
BUT IN NO INSTANCE WAS THE FEMORAL HEAD REPLACED INTO THE TRUE ACETABULUM

MATERIAL
• Pain in hip with stiffness and limitation in activity was the main indication for surgery
• For 11 patients (12.35 %) back or knee pain was the chief complaint
METHOD
PRE OPERATIVELY :• A thorough assessment of the patient was made, including
- the dislocated hip, the controlateral hip, knees and lumbo-sacral spine- noting : pelvic tilt, fixed deformities, lumbo-sacral residual
flexibility, leg shortening, true and apparent leg length discrepancy, knee malalignment and skeletal disorders due to previous operations.
• X-Rays :• Routinely and AP and lateral X-rays of the lumbar spine in a standing
position• AP radiograph of the lower part of the body, taking on a single film
pelvis and lower limbs in a standing position• Classical AP and lateral X-rays of pelvis, hips and upper part of the
femur• Clinically the hip was assessed according to the d’Aubigné six digit scale
evaluating pain, motion, stability and gait, global function and the average value of each criterion.
METHODPOSTOPERATIVELY
• The same clinical assessment of operated hip was made at each examination
• And on an AP X-rays of the pelvis were noted:- for the acetabular component - position of the socket relative to usual reference marks and lines, radiolucent lines, linear wear- for the femoral component were recorded - position, radiolucent lines, debonding and subsidence- osteolysis- heterotopic bone

METHOD
EVALUATION OF LOOSENING
Was made according to Harris and Johnston in
Definite, probable, possible

•A radiograph of the lower part of the body in a frontal view was taken to assess:- The result of the unilateral or bilateral hip replacement on: - Pelvic tilt - Leg lengthening - Residual leg length discrepancy• On AP and lateral radiograph of the lumbar spine was evaluated the correction of lordosis and lateral curve
1 YEAR POSTOPERATIVELY
COMPLICATIONS
• 1 intra operative femoral fracture (cerclage)• 1 peroneal nerve palsy (recovered in a few days)• 2 trochanteric non unions (united after revision)• 1 dislocation• 4 heterotopic ossifications
– 2 Brooker II– 1 Brooker III
- 1 Brooker IV• No infection
Both revised

FOLLOW UP
• At each examination 6 weeks, 3 months, 6 months, 1 year, every year until 5
years and then every 2 or 3 years
• Lost: 7 patients (9 hips)
2 between 1 and 10 years and 5 between 10 and 20 years
• Deceased: 41 patients (48 hips)
12 between 1 and 10 years and 29 between 10 and 27 years
• Still alive and regularly seen: 40 patients (61 hips)
Average follow up: 22 years (18 to 32)
• Average follow up of the whole series: 16.9 years
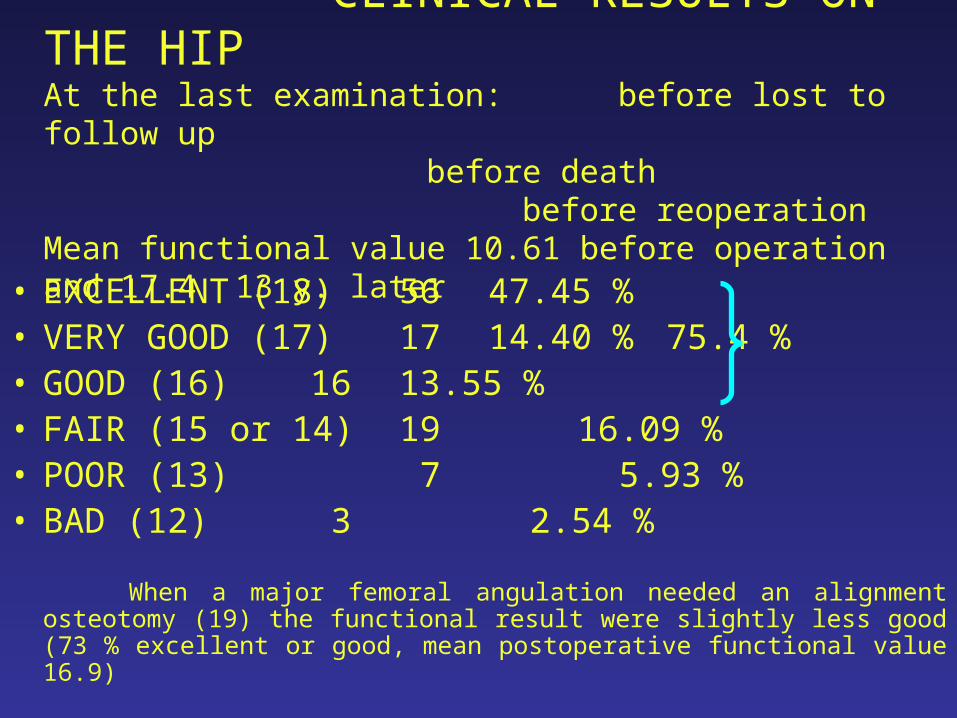
CLINICAL RESULTS ON THE HIPAt the last examination: before lost to follow up before death
before reoperationMean functional value 10.61 before operation and 17.4 13 y. later
• EXCELLENT (18)56 47.45 %• VERY GOOD (17) 17 14.40 % 75.4 %• GOOD (16) 16 13.55 %• FAIR (15 or 14) 19 16.09 %• POOR (13) 7 5.93 % • BAD (12) 3 2.54 %
When a major femoral angulation needed an alignment osteotomy (19) the functional result were slightly less good (73 % excellent or good, mean postoperative functional value 16.9)

CLINICAL RESULTS
40 still alive, 61 hips followed up 18 to 32 y.
• Before reoperation
Ex. + VG + G 75.4 %
• After reoperation
Ex. + VG + G 95 %

RADIOLOGICAL RESULTSAT LONG TERM
Polyethylene wear• Not measurable: 58 hips (48 %)• Between 1 mm and 7 mm: 60 hips (52 %)
LooseningsFemoral: 1Acetabular (definite + probable): 22
2 before they get lost (elsewhere reoperated?) 17 (3 of them were recurrent and reoperated
on)
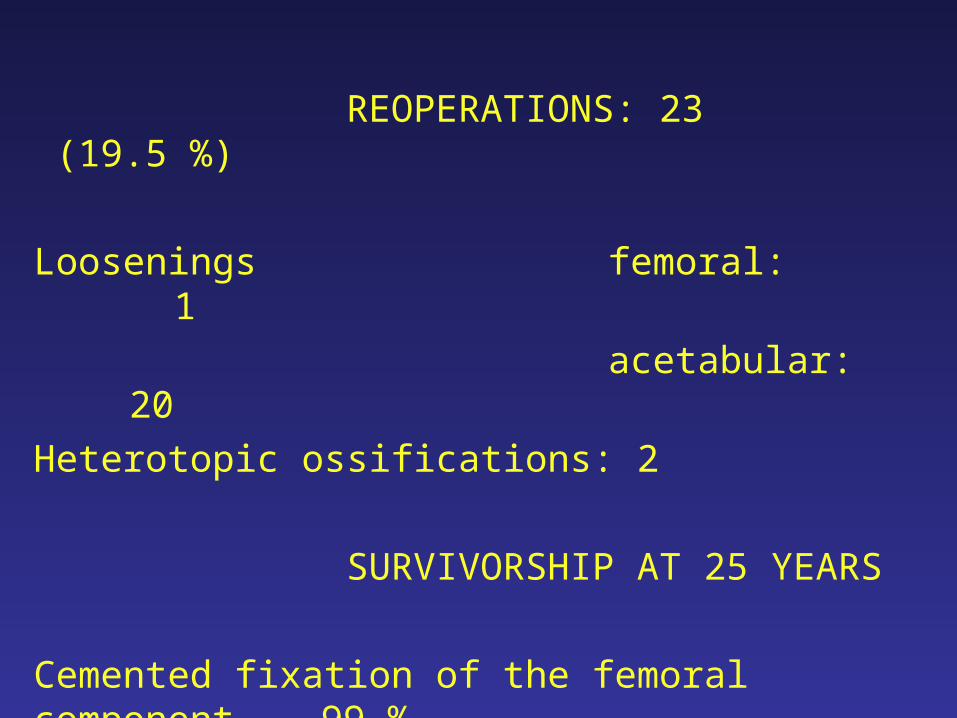
REOPERATIONS: 23 (19.5 %)
Loosenings femoral: 1
acetabular: 20
Heterotopic ossifications: 2
SURVIVORSHIP AT 25 YEARS
Cemented fixation of the femoral component 99 %
Cemented fixation of the acetabular component 79 %
Of the prosthesis 75 %

EQUALIZATION OF THE LEG LENGTH
• SHORTENING 4.84 cm (3 to 8 cm)
– Accurate correction 63
– Within 1 cm 42
• LENGTHENING 3.8 cm (2 to 7 cm)
• AVERAGE LEG LENGTH DISCREPANCY
– Preoperatively 2.60 cm
– Postoperatively 0.4 cm
2 patients needed a shortening of the long femur to get equality

RESULTS ON THE IPSI LATERAL KNEE
• On the 18 preoperative painful knees:
–10 were greatly improved
– 8 needed an operation
(4 osteotomies and 4 prostheses)
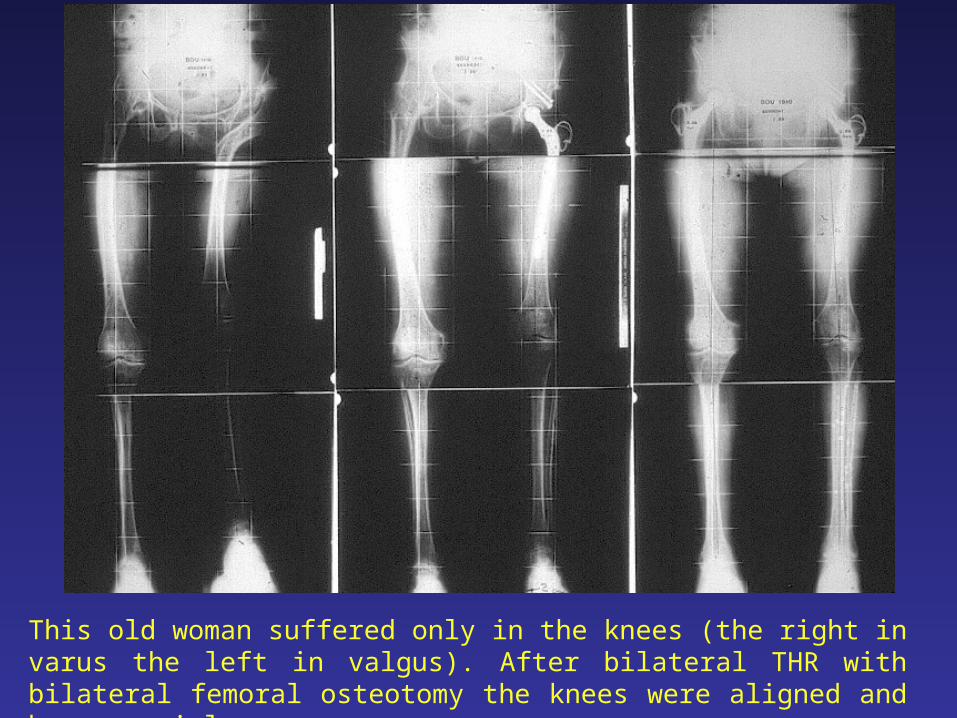
This old woman suffered only in the knees (the right in varus the left in valgus). After bilateral THR with bilateral femoral osteotomy the knees were aligned and became painless.
RESULTS ON THE LUMBAR SPINE
Reconstruction of the hip and equalization of the leg length have led to many improvements on pelvis and lumbo-sacral spine.
Lateral pelvic tilt was corrected in more than 50 %21 postoperative versus 47 before THRPelvic frontal asymmetry has often been corrected at least partiallyand also lordosis and lateral curve of the lumbar spine.
So low-back pain has been relieved in 40 patients but 2 required a laminectomy for lumbar canal stenosis
CONCLUSION
Total hip arthroplasty on high riding hips may be a wonderful operation, able to greatly improve not only the hip function, but also lumbo-sacral spine and knee thanks to a dramatic improvement of the static body balance. Yet, this operation, full of pitfalls, poses a wide spectrum of difficulties and represents a serious risk of complication.
A successful result depends on a complete preoperative assessment of the patient, a perfect carrying out of the surgical procedure with a suitable prosthesis and a reasonable selection of its indications.