thoracentesis. etiology of pleural effusions the most common causes(adult): 1. congestive heart...
TRANSCRIPT

Thoracentesis

ETIOLOGY OF PLEURAL EFFUSIONS
The most common causes(adult):
1.Congestive heart failure (CHF)2.Pneumonia3.Malignancy4.Pulmonary embolism (PE)5.Viral disease
The most common causes(children):
1.Pneumonia, followed by congenital heart disease
2.Malignancy3.Renal disease4.Trauma

ETIOLOGY
Transudates :
Increase in intravascular hydrostatic pressureDecrease intravascular oncotic pressure
Most common cause CHF ( hydrostatic pressure)
Cirrhosis Decreased plasma oncotic pressure

Less common causes:Nephrotic syndromePeritoneal dialysisPericardial diseaseCentral venous obstructionMyxedemaAcute atelectasisBone marrow transplantationUrinothorax

Exudates:
Pleural inflammationIncreased pleural membrane permeabilityLymphatic obstruction
More than 90% Malignancy, Pneumonia, PTE

Less common causes:Trauma Drug inducedEsophageal perforation ChylothoraxPancreatitis AsbestosisIntraabdominal abscess Meig’s
syndromeAbdominal surgery RadiotherapyCollagen vascular disease CABGOHS

DIAGNOSIS
Three most common symptoms:
chest pain(dull ache), cough, dyspnea
Tactile fremitusDullness in percussionAbsent breath sounds, depending on the size
of the effusion
UltraSound

Radiologic Diagnosis
Chest x-ray:Usually visible on an upright(PA): 200-250 mlLateral radiograph: 50-75 ml
The earliest recognized sign: blunting of the lateral costophrenic angle
Larger free-flowing effusions: meniscus

Radiologic Diagnosis
The true height of an effusion corresponds to the highest portion of the meniscus.
The presence of a pneumothorax or abscess may alter the appearance of the meniscus to more of a straightline (air-fluid level).
Subpulmonic effusion:hemidiaphragm is elevated and the dome peaks more laterally

Radiologic Diagnosis(subpulmonic)

Radiologic Diagnosis(Meniscus)

Radiologic Diagnosis(D-shape)

Radiologic Diagnosis

Radiologic Diagnosis(CT-scan)
CT is more sensitive
CT can be used to assess pleural thickening, irregularities, and masses that are suggestive of malignancy and other diseases that result in exudative effusions.

Radiologic Diagnosis(CT-scan)

Radiologic Diagnosis(CT-scan)

Radiologic Diagnosis(Ultrasound)
US is superior to chest radiographs in diagnosing effusions.
Can detect effusions as small as 5 mL.
US is a useful bedside tool when performing thoracentesis.

Radiologic Diagnosis

INDICATIONS
Diagnostic: 50 to 100 mLMost new effusions that measure greater
than 10 mm on a decubitus radiograph/CT/US require diagnostic thoracentesis
Therapeutic:Help relieve the dyspnea associated with a
large pleural effusion

CONTRAINDICATIONS
No absolute contraindications
Under real-time US guidance, thoracentesis is safe despite abnormal coagulation parameters.
Avoid skin puncture through a site of cellulitis or herpes zoster

PROCEDURE(Equipment)
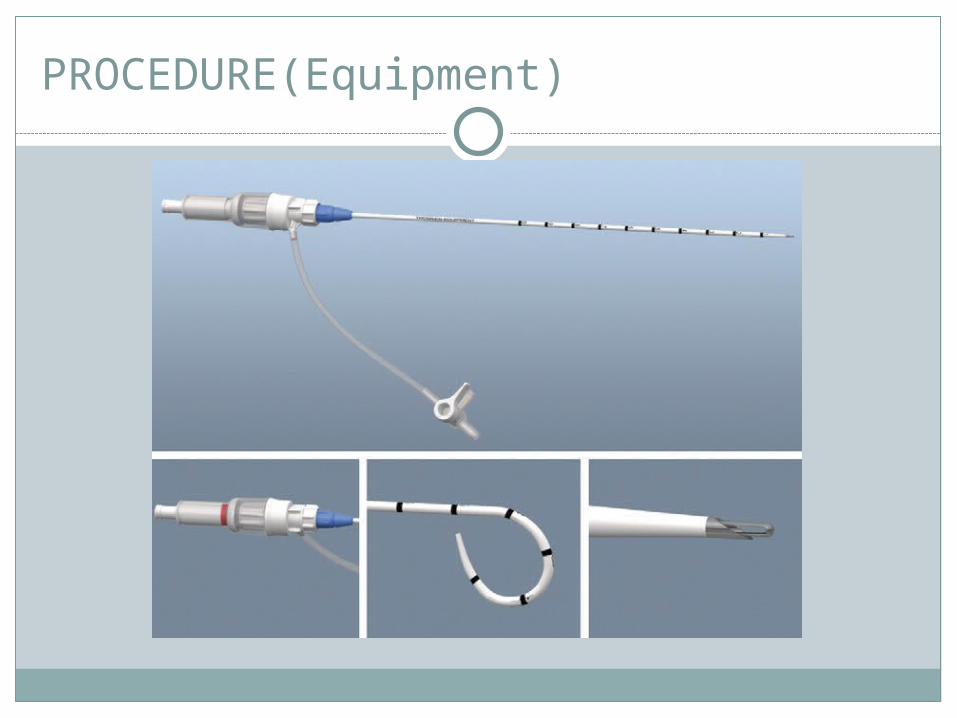
PROCEDURE(Equipment)

Termination of the Procedure
Procedure on relief of dyspnea or when up to 1500 mL of fluid has been withdrawn.
Avoid significantly negative pleural pressure; symptomatic hypovolemia and reexpansion pulmonary edema.
Aspiration of air Suspicion for a complication

Insertion Site and Patient Position
Upright positioning is the desired
Insert the thoracentesis catheter one to two intercostal spaces below the highest level of effusion in midscapular or posterioraxillary line.
The lowest level recommended is the space between the eighth and the ninth ribs.
Below the eighth intercostal space, the risk for diaphragmatic or hepatic/splenic injury increases.

Insertion Site and Patient Position

Insertion Site and Patient Position
If the patient is too ill to sit upright, perform the procedure with the patient in the lateral decubitus.
The side of the effusion down, and the back at the edge of the bed.
Insert the needle at the posterior axillary line.
Insertion Site and Patient Position
Alternatively, position the patient supine with the head elevated as much as possible.
Use the midaxillary line as the point of needle insertion for this position.

Insertion Site and Patient Position












Postprocedure Radiograph
In many centers, chest radiographs are routinely obtained after thoracentesis to evaluate for procedure-related pneumothorax.
Obtain a chest radiograph in patients who require multiple needle passes, if air is aspirated, in those at risk for adhesions, or in those in whom any new symptoms (chest pain, dyspnea).

PLEURAL FLUID ANALYSIS
Perform an initial evaluation to determine whether the fluid is transudative or exudative and obtain other tests only if the fluid is an exudate.
Pleural fluid sent for cell count with differential should be transferred to an anticoagulant-containing tube.
Analyze the fluid within 4 hours.Samples are collected and refrigerated at 4°C.

PLEURAL FLUID ANALYSIS
Transfer samples for pleural fluid pH immediately to a blood gas syringe, place it on ice, and analyze it within 1 hour.

Distinguishing Transudate from Exudate:
Light’s Criteria:
Pleural fluid-serum protein ratio >0.5
Pleural fluid lactate dehydrogenase (LDH) level greater than two thirds the upper limit of the serum reference range
Pleural fluid-serum LDH ratio >0.6

Distinguishing Transudate from Exudate:
An exception to using Light’s criteria:
CHF treated with diuretics.
Pleural fluid or serum NT-proBNP level of 1500 pg/mL or higher indicates a diagnosis of CHF.

Distinguishing Transudate from Exudate:
All undiagnosed exudates, at a minimum pleural fluid should be sent for :
Cell count with differential GlucoseAdenosine deaminase (ADA)Cytologic evaluation

Distinguishing Exudates:
RBC count Grossly bloody or >100,000 cells/mm3: Trauma, malignancy, PTE, pneumonia
WBC count >10,000 cells/mm3: Parapneumonic effusion

Distinguishing Exudates:
Neutrophils >50%(Acute pleural process): infection, pulmonary infarct
Lymphocytes >50%(Chronic pleural process): malignancy, TB

Distinguishing Exudates:
Glucose <60 mg/dL:
Parapneumonic infectionMalignancyTBRA
Distinguishing Exudates:
ADA>40 IU/L TB (lymphoma, empyema)
Amylase>100 U/L Pancreatitis, esophageal rupture
Triglycerides>110 mg/dL Chylothorax
pH <7.2 Complicated parapneumonic (malignancy, TB, esophageal rupture,collagen
vascular disease)
Indications for Surgical Managementof Parapneumonic Effusions
1. Effusion >50% of the hemithorax2. Loculated effusion3. Pleural thickening seen on a computed
tomography scan4. Aspiration of frank pus5. Pleural fluid pH <7.26. Pleural fluid glucose <60 mg/dL7. Positive Gram stain or culture of pleural
fluid

COMPLICATIONS
PneumothoraxCoughInfectionReexpansion pulmonary edemaVasovagal

