thomas repas do facp cde uw hospital and clinics department of medicine section of endocrinology,...
Post on 22-Dec-2015
217 views
TRANSCRIPT

Thomas Repas DO FACP CDEThomas Repas DO FACP CDEUW Hospital and Clinics Department of Medicine UW Hospital and Clinics Department of Medicine
Section of Endocrinology, Diabetes & Metabolism Section of Endocrinology, Diabetes & Metabolism
H4/568 CSC (5148), 600 Highland Avenue, Madison, WI 53792 H4/568 CSC (5148), 600 Highland Avenue, Madison, WI 53792
Thursday November 17, 2005Thursday November 17, 2005
Celiac Sprue: Review of a Celiac Sprue: Review of a Multisystem DiseaseMultisystem Disease

Common Misconceptions
• “Celiac is rare”• “Celiac is only a disease of children and young
adults”• “Celiac only occurs in patients of European
descent” • “All celiac patients have gastrointestinal
symptoms”• “Serologic testing is unreliable”• “What does it matter if they have celiac or not?”

• History/Background
• Prevalence
• Pathophysiology
• Clinical Manifestations
• Associated Disorders
• Diagnosis
• Management
ObjectivesObjectives
History of Celiac History of Celiac DiseaseDisease

History of Celiac
• Cereal grains were first domesticated from wild grasses in the Fertile Crescent about 10,000 years ago
Simopoulos AP (ed): Evolutionary Aspects of Nutrition and Health. Diet, Exercise, Genetics and Chronic Disease.World Rev Nutr Diet. Basel, Karger, 1999, vol 84, pp 19–73

History of Celiac
• Aretaeus from Cappadochia (now Turkey) in the 2nd century AD described a chronic malabsorptive condition
• He named this disorder "koiliakos” which is Greek for "suffering in the bowels.”
Booth, CC. History of celiac disease. BMJ 1989; 298:527.
History of Celiac
• The second classical description was in 1888 in a report entitled "On the Coeliac Affection“ by Samuel Gee
S. Gee: “On the coeliac affection” Saint Bartholomew’s Hospital Reports, London, 1888, 24: 17-20
"to regulate the food is the main part of treatment ... "to regulate the food is the main part of treatment ... The allowance of farinaceous foods must be small ... The allowance of farinaceous foods must be small ...
but if the patient can be cured at all, it must be by but if the patient can be cured at all, it must be by means of diet."means of diet."

History of Celiac
• During World War II, celiac children improved during the food shortages when bread was unavailable.
• After the war, symptoms reoccurred when bread and cereals were reintroduced.
• Dutch pediatrician Willem K Dicke recognized and confirmed this association between cereal grains and malabsorption.
Dicke, WK. Simple dietary treatment for the syndrome of GheeHerter. Ned Tijdschr Geneeskd 1941; 85:1715.DICKE, WK, WEIJERS, HA, VAN DE, KAMER JH. Coeliac disease. II. The presence in wheat of a factor having a deleterious effect in cases of coeliac disease. Acta Paediatr 1953; 42:34.

History of Celiac
• The celiac lesion in the proximal small intestine was first described by Paulley in 1954.
• It was learned that celiac disease and adult non-tropical sprue share many of the same features
• These classic findings are:– mucosal inflammation– crypt hyperplasia– villous atrophy
PAULLEY, JW. Observation on the aetiology of idiopathic steatorrhoea; jejunal and lymph-node biopsies. Br Med J 1954; 4900:1318RUBIN, CE, BRANDBORG, LL, PHELPS, PC, TAYLOR, HC Jr. Studies of celiac disease. I. The apparent identical and specific nature of the duodenal and proximal jejunal lesion in celiac disease and idiopathic sprue. Gastroenterology 1960; 38:28

Prevalence of Celiac Prevalence of Celiac DiseaseDisease

Prevalence of Celiac DiseasePrevalence of Celiac Disease
• Historically, celiac was thought to be an uncommon disease
• In the 1950s the prevalence of celiac disease among Europeans was thought to range between 1:4000 and 1:8000.
• However, this diagnosis was based upon a presentation with classic symptoms of malabsorption

Prevalence of Celiac DiseasePrevalence of Celiac Disease
• Celiac occurs primarily in whites of northern European ancestry
• However, it has been reported in many other groups:– It has been reported in Indians, Arabs, Hispanics,
Israeli Jews, Sudanese, and people of Cantonese extraction
– Punjabis and Gujaratis from India who lived in England developed celiac 2.7 times as often as Europeans when on a gluten-rich diet
Sher, KS, Fraser, RC, Wicks, AC, et al. High risk of coeliac disease in Punjabis. Epidemiological study in the South Asian and European populations
of Leicestershire. Digestion 1993; 54:178.

Prevalence of Celiac DiseasePrevalence of Celiac Disease
• In the 1970’s, celiac was recognized that celiac to be much more common than preciously thought.

Prevalence of Celiac DiseasePrevalence of Celiac Disease
• In one study, 17,201 Italian school children (aged 6 to 15 years) were recruited from several regions of Italy and represented 69 percent of the eligible population.– Screening was performed with anti-gliadin and anti-
endomysial antibodies– Diagnosis was confirmed with small intestines
mucosal biopsy
Catassi, C, Fabiani, E, Ratsch, IM, et al. The coeliac iceberg in Italy. A multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Acta Paediatr Suppl 1996; 412:29

In this study– The prevalence of biopsy proven celiac
was 1:184– The ratio of undiagnosed to diagnosed
celiac disease was a remarkable 7:1– Most children had minor but significant
nonspecific symptoms
Prevalence of Celiac DiseasePrevalence of Celiac Disease
Catassi, C, Fabiani, E, Ratsch, IM, et al. The coeliac iceberg in Italy. A multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Acta Paediatr Suppl 1996; 412:29
Prevalence of Celiac DiseasePrevalence of Celiac Disease
• Many studies have also shown high prevalence
– 1:152 in the Belfast MONICA project evaluating 1,823 participants 1
– 1:256 was noted in a screening study of 1866 Swedish blood donors 2
– 1:99 in a study of 3654 Finnish students 3 – 1:96 in a study of 3188 Italian school children 4
1. Johnston, SD, Watson, RG, McMillan, SA, et al. Preliminary results from follow-up of a large-scale population survey of antibodies to gliadin, reticulin and endomysium. Acta Paediatr Suppl 1996; 412:61.2. Grodzinsky, E. Screening for coeliac disease in apparently healthy blood donors. Acta Paediatr Suppl 1996; 412:36.3. Maki, M, Mustalahti, K, Kokkonen, J, Kulmala, P. Prevalence of Celiac disease among children in Finland. N Engl J Med 2003; 348:2517.4. Tommasini, A, Not, T, Kiren, V, et al. Mass screening for coeliac disease using antihuman transglutaminase antibody assay. Arch Dis Child 2004; 89:512

• The prevalence of celiac in the US is similar to Europe
• One large multi-center US study of 13145 subjects consisted of the following:– 4508 first-degree relatives of patients with celiac
disease– 1275 second-degree relatives– 3236 symptomatic patients– 4126 not-at-risk individuals
Prevalence of Celiac DiseasePrevalence of Celiac Disease
Fasano, A, Berti, I, Gerarduzzi, T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch Intern Med 2003; 163:286

Prevalence of Celiac DiseasePrevalence of Celiac Disease
• In this study, the prevalence of celiac disease was as follows:– 1:22 in first-degree relatives– 1:39 in second-degree relatives – 1:56 in symptomatic patients– 1:133 in the not-at-risk groups
Fasano, A, Berti, I, Gerarduzzi, T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch Intern Med 2003; 163:286

PathophysiologyPathophysiology of Celiac Disease of Celiac Disease

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• Celiac disease as an immune disorder that is triggered by an environmental agent (the gliadin component of gluten) in genetically predisposed individuals
Kagnoff, MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components. Gastroenterol Clin North Am 1992; 21:405.Schuppan, D. Current concepts of celiac disease pathogenesis. Gastroenterology 2000; 119:234.

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
Grain protein exists in four general storage forms which are categorized by their solubility characteristics:
• Prolamins (soluble in ethanol)• Glutenins (partially soluble in dilute acid or alkali
solutions)• Globulins (soluble in 10 percent NaCl)• Minor albumins (soluble in water)
Glutens specifically are the prolamins and the glutenins
Bernardin, JE, Saunders, RH, Kasarda, DD. Absence of carbohydrate in coeliac toxic A-gliadin. Cereal Chem 1976; 53:612.Freedman, AR, Galfre, G, Gal, E, et al. Western immunoblotting of cereal proteins with monoclonal antibodies to wheat gliadin to investigate coeliac disease. Int Arch Allergy Appl Immunol 1988; 85:346.Troncone, R, Auricchio, S, De Vincenzi, M, et al. An analysis of cereals that react with serum antibodies in patients with coeliac disease. J Pediatr Gastroenterol Nutr 1987; 6:346.Vader, LW, Stepniak, DT, Bunnik, EM, et al. Characterization of cereal toxicity for celiac disease patients based on protein homology in grains. Gastroenterology 2003; 125:1105

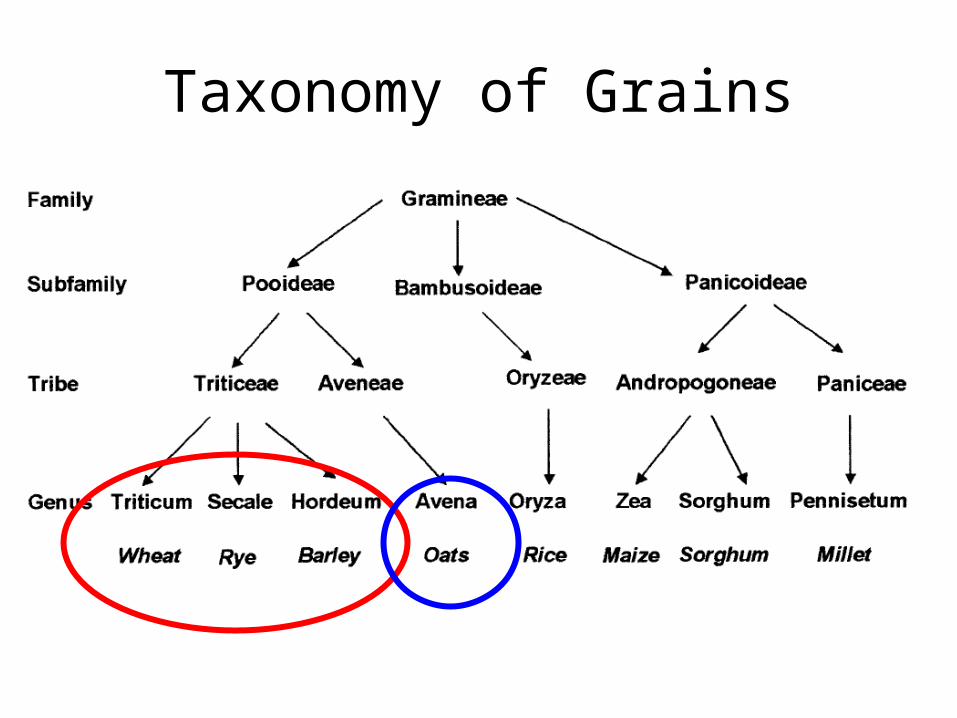
Taxonomy of Grains
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18
Gliadins Secalins Hordeins Avenins Zeins

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• The pathophysiology of gliadin toxicity in celiac patients is poorly understood
• One hypothesis is that similarities between gliadin proteins and certain enteral pathogens may result in the immunologic response to antigens in gluten.
Kagnoff, MF, Paterson, NY, Kumar, PJ, et al. Evidence for the role of a human intestinal adenovirus in the pathogenesis of coeliac disease. Gut 1987; 28:995
PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• Kagnoff et al suggested that the alpha fraction of gliadin demonstrated an amino acid region that was homologous to the 54KDa E1b protein coat of adenovirus 12
• The authors postulated that exposure to this virus in a susceptible person may be potentially be involved in the pathogenesis of celiac disease
Kagnoff, MF, Paterson, NY, Kumar, PJ, et al. Evidence for the role of a human intestinal adenovirus in the pathogenesis of coeliac disease. Gut 1987; 28:995
PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• Other studies, however, have failed to show an association with the presence of celiac sprue and serum antibody titers to the adenovirus 12 protein
Nilsen, EM, Lundin, KE, Krajci, P, et al. Gluten specific, HLA-DQ restricted T cells from coeliac mucosa produce cytokines with Th1 or Th0 profile dominated by interferon gamma. Gut 1995; 37:766

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• The current hypotheses:– Gliadin-sensitive T cells in genetically
predisposed individuals recognize gluten-derived peptide epitopes and develop an inflammatory response which produces mucosal damage
Nilsen, EM, Lundin, KE, Krajci, P, et al. Gluten specific, HLA-DQ restricted T cells from coeliac mucosa produce cytokines with Th1 or Th0 profile dominated by interferon gamma. Gut 1995; 37:766

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• Genetic factors play an important role- there is significantly increased risk of celiac among family members
• A close association with the HLA-DQ2 and/or DQ8 gene locus has been recognized
• HLA-DQ2 is found in 98 percent of celiac patients from Northern Europe.
• However, ~25% of “normal” individuals in this population will also demonstrate HLA-DQ2
Kagnoff, MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components. Gastroenterol Clin North Am 1992; 21:4Schuppan, D. Current concepts of celiac disease pathogenesis. Gastroenterology 2000; 119:234.Petronzelli, F, Bonamico, M, Ferrante, P, et al. Genetic contribution of the HLA region to the familial clustering of coeliac disease. Ann Hum Genet 1997; 61:307Houlston, RS, Ford, D. Genetics of coeliac disease. QJM 1996; 89:737.Houlston, RS, Tomlinson, IP, Ford, D, et al. Linkage analysis of candidate regions for coeliac disease genes. Hum Mol Genet 1997; 6:1335

Current Model for Pathogenesis of Current Model for Pathogenesis of Celiac DiseaseCeliac Disease
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18

PathophysiologyPathophysiologyof Celiac Diseaseof Celiac Disease
• HLA class II molecules are expressed on the surface of antigen-presenting cells
• They can bind to and subsequently present “foreign” peptides to populations of CD4 T cells that recognize the DQ2- or DQ8-peptide complex
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18

Role of Tissue Transglutaminase
• Tissue transglutaminase can deamidate glutamine, converting glutamine to negatively charged glutamic acid
• This renders these peptides better binders to the disease relevant DQ2 or DQ8 molecules
• Once bound to DQ2 or DQ8, the DQ-“gluten” peptide complexes activate DQ2 or DQ8 restricted T cells
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18
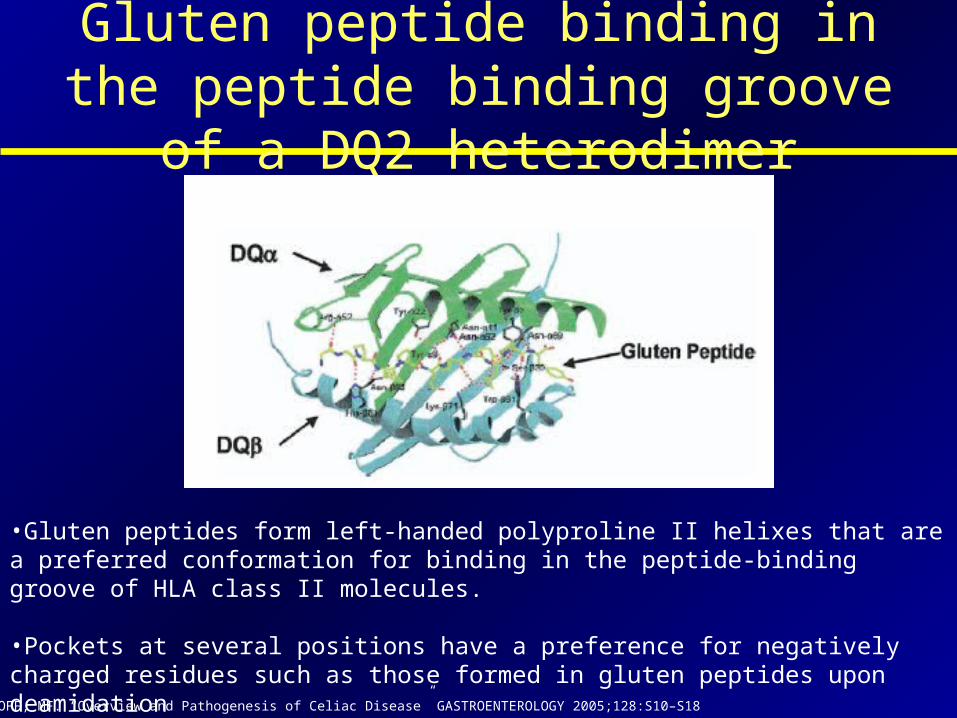
Gluten peptide binding in the peptide binding groove of a DQ2 heterodimer
•Gluten peptides form left-handed polyproline II helixes that are a preferred conformation for binding in the peptide-binding groove of HLA class II molecules.
•Pockets at several positions have a preference for negatively charged residues such as those formed in gluten peptides upon deamidation
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18

Activation of DQ-restricted T cells
in Celiac Disease
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18

Celiac Disease: Clinical Celiac Disease: Clinical ManifestationsManifestations

Celiac Disease: Clinical Celiac Disease: Clinical Manifestations in ChildrenManifestations in Children
The classical presentation is in children after weaning and introduction of cereals into the diet:
• Failure to thrive • Apathy• Pallor• Anorexia• Muscle wasting with generalized hypotonia • Abdominal bloating and distention• Soft, bulky, clay-colored, offensive stools

Celiac Disease: Clinical Celiac Disease: Clinical ManifestationsManifestations
• As our understanding of celiac improved and serologic testing has become available, subclinical forms of the disease have been recognized

Celiac Disease: Clinical Celiac Disease: Clinical Manifestations in ChildrenManifestations in Children
Catassi, C, et al Acta Paediatr 1996; 412(suppl):29.
Symptoms and signs at presentation Overall prevalence (%)
Iron deficiency with anemia 29
Iron deficiency without anemia 27
Recurrent Abdominal Pain 24
Mood Changes 17
Recurrent Aphthous Stomatitis 11
Poor appetite 10
Recurrent diarrhea 9
Short stature 7
Abdominal distension 5
Constipation 2
Pubertal delay 2
Hypoalbuminemia 2

Celiac Disease: Clinical Celiac Disease: Clinical Manifestations in AdultsManifestations in Adults
In a study of 1138 people with biopsy–proven celiac disease:
• Majority of individuals were diagnosed in their 4th to 6th decades.
• Women predominated (2.9:1)- the female predominance was less marked in the elderly.
• Diarrhea was the main presenting symptom occurring in 85%.
• 36% had a previous diagnosis of irritable bowel syndrome.
• Symptoms were present a mean of 11 years before diagnosis.
Green PHR, et al. Characteristics of adult celiac disease in the USA: results of a national survey. Am J Gastroenterol 2001;96:126–131.
Celiac Disease: Clinical Celiac Disease: Clinical Manifestations in AdultsManifestations in Adults
In a population-based study from Minnesota, Murray et al noted a 10-fold increase in the incidence of celiac disease from 1950 to 2001.
• The clinical severity of the disease decreased, with fewer people with diarrhea and weight loss at presentation.
• Only 54% had diarrhea at diagnosis, 34% abdominal pain and 30% bloating.
• Obesity was present in 27%.
Murray JA, et al. Trends in the incidence and clinical features of celiac disease in a North American community, 1950-2001. Clin Gastroenterol Hepatol 2003;1:19–27.

Spectrum of Celiac DiseaseSpectrum of Celiac Disease
Few if any GI symptomsFew if any GI symptoms Marked GI symptomsMarked GI symptoms
FatigueFatigueDepression, irritabilityDepression, irritabilityMenstrual irregularityMenstrual irregularity
WeaknessWeaknessInfertilityInfertility
Growth DisturbanceGrowth DisturbanceNeurologic ComplaintsNeurologic Complaints
DiarrheaDiarrheaBulky, Pale, Foul stoolsBulky, Pale, Foul stools
Abdominal Distension, BloatingAbdominal Distension, BloatingAbdominal cramps Abdominal cramps
Weight lossWeight lossLoss of or increased appetiteLoss of or increased appetite
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18

Classification of Celiac DiseaseClassification of Celiac Disease
• Classical celiac disease• Celiac disease with atypical
symptoms• Silent celiac disease• Latent celiac disease
NATIONAL INSTITUTES OF HEALTH, CONSENSUS DEVELOPMENT CONFERENCE STATEMENT: Celiac Disease.June 28–30, 2004

Celiac Disease: Celiac Disease: Associated DisordersAssociated Disorders

Celiac Disease: Associated Celiac Disease: Associated DisordersDisorders
• Dermatitis Herpetiformis• Iron deficiency anemia• Osteoporosis, Osteomalacia and Vitamin D
deficiency• Malignancies• Type 1 diabetes• Other autoimmune endocrine disorders• Neuropsychologic Features • Others (Downs syndrome, IgA deficiency,
rheumatologic disorders)
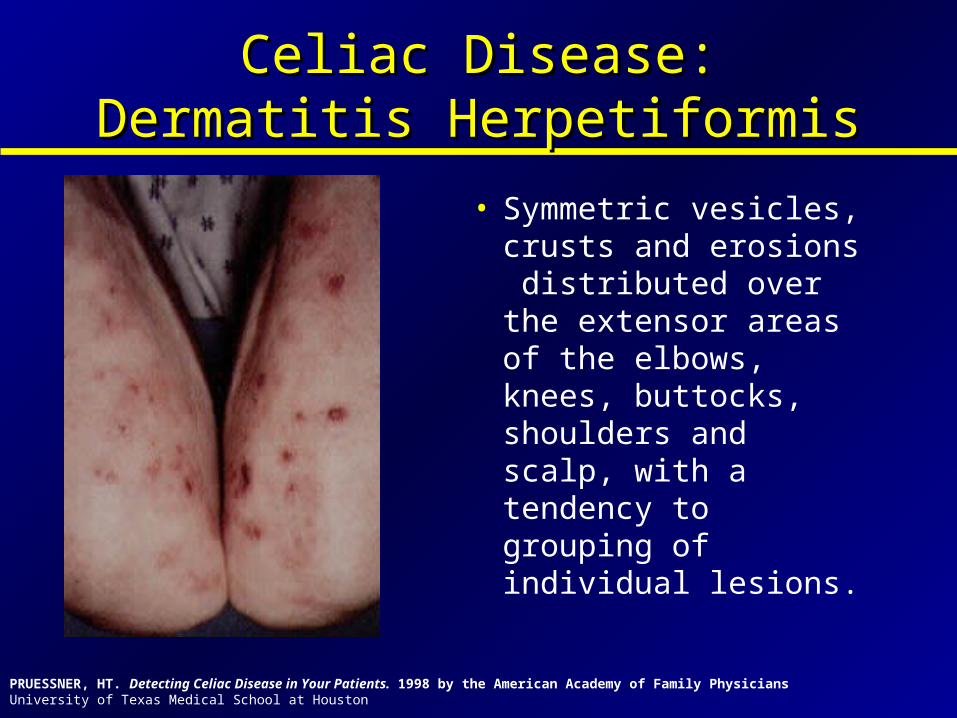
Celiac Disease: Dermatitis Celiac Disease: Dermatitis HerpetiformisHerpetiformis
• Symmetric vesicles, crusts and erosions distributed over the extensor areas of the elbows, knees, buttocks, shoulders and scalp, with a tendency to grouping of individual lesions.
PRUESSNER, HT. Detecting Celiac Disease in Your Patients. 1998 by the American Academy of Family Physicians University of Texas Medical School at Houston

Celiac Disease: Dermatitis Celiac Disease: Dermatitis HerpetiformisHerpetiformis
• It has been reported that up to 10 percent of individuals with celiac will also have dermatitis herpetiformis
American Gastroenterological Association, Ciclitra, PJ, Gastroenterology 2001; 120: 1526.Guidetti, CS, et al. Duration of gluten exposure in adult coeliac disease does not correlate with the risk for autoimmune disorders,Gut 2001;49:502–505
Celiac Disease: Other Skin Celiac Disease: Other Skin DisordersDisorders
• Acquired icthyosis• Cutaneous amyloid• Cutaneous vasculitis• Eczema• Epidermal necrolysis• Nodular prurigo• Pityriasis rubra pilara• Pustular dermatitis
American Gastroenterological Association, Ciclitra, PJ, Gastroenterology 2001; 120: 1526.

Celiac Disease: Iron Deficiency Celiac Disease: Iron Deficiency AnemiaAnemia
• In a study of 227 patients with biopsy–proven celiac disease- iron-deficiency anemia was the mode of presentation in 8%1
• In a Mayo Clinic study, celiac disease was identified as the cause of iron deficiency in 15% of those undergoing endoscopic assessment for iron deficiency.2
• In a prospective study of adults, mean age in their 50s, Karnum et al found 2.8% to have celiac disease.3
1. Lo W, Sano K, Lebwohl B, Diamond B, Green PH. Changing presentation of adult celiac disease. Dig Dis Sci 2003;48:395–398. 2. Oxentenko AS, et al. The insensitivity of endoscopic markers in celiac disease. Am J Gastroenterol 2002;97:933–938.3. Karnam US, et al. Prevalence of occult celiac disease in patients with iron-deficiency anemia: a prospective study. South Med J 2004;97:30–34.

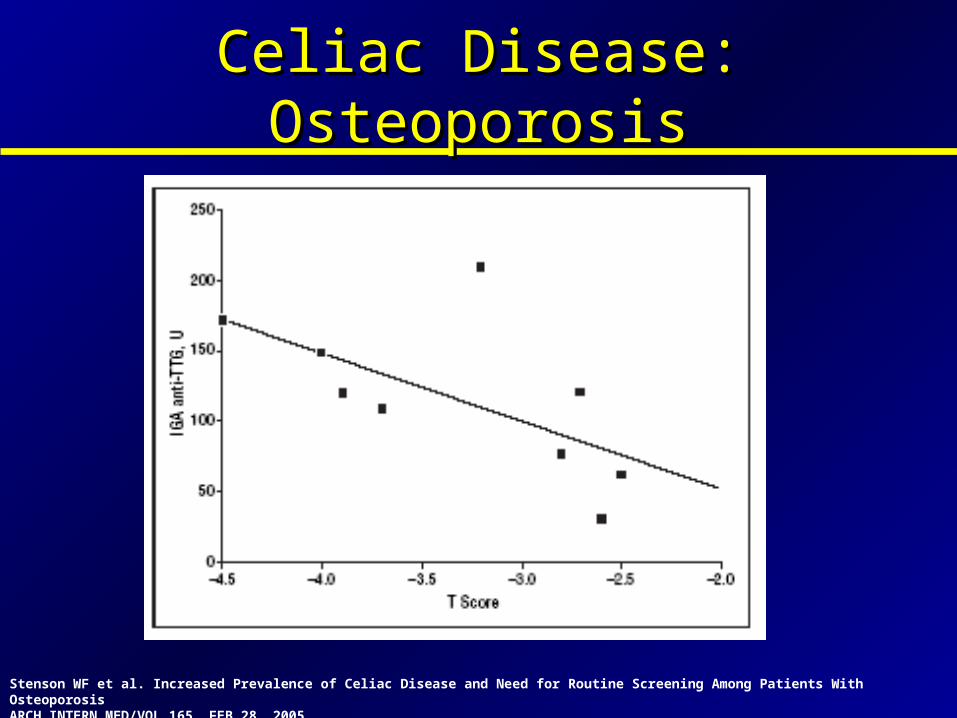
• 840 individuals were evaluated by serologic screening for celiac disease at the Washington University Bone Clinic – 266 with osteoporosis – 574 without osteoporosis
• Individuals with positive serologic test were offered endoscopic intestinal biopsy
• The prevalence of biopsy-proven celiac disease was – 3.4% in individuals with osteoporosis – 0.2% in individuals without osteoporosis
Celiac Disease: OsteoporosisCeliac Disease: Osteoporosis
Stenson WF et al. Increased Prevalence of Celiac Disease and Need for Routine Screening Among Patients With OsteoporosisARCH INTERN MED/VOL 165, FEB 28, 2005
Celiac Disease: OsteoporosisCeliac Disease: Osteoporosis
Stenson WF et al. Increased Prevalence of Celiac Disease and Need for Routine Screening Among Patients With OsteoporosisARCH INTERN MED/VOL 165, FEB 28, 2005

Celiac Disease: Osteoporosis Celiac Disease: Osteoporosis
Treatment of thepatients with celiac disease with a gluten-free diet for 1 year resultedin improvement in T scores.
Stenson WF et al. Increased Prevalence of Celiac Disease and Need for Routine Screening Among Patients With OsteoporosisARCH INTERN MED/VOL 165, FEB 28, 2005
P=0.02

Nuti, R et al. Prevalence of undiagnosed coeliac syndrome in osteoporotic women. Journal of Internal Medicine 2001; 250: 361±366
Celiac Disease: Vitamin D Celiac Disease: Vitamin D DeficiencyDeficiency
• 255 women with osteoporosis
• 53 women tested positive for tTG ab
• Prevalence of serological disease 9.4%

Nuti, R et al. Prevalence of undiagnosed coeliac syndrome in osteoporotic women. Journal of Internal Medicine 2001; 250: 361±366
Celiac Disease: Vitamin D Celiac Disease: Vitamin D DeficiencyDeficiency
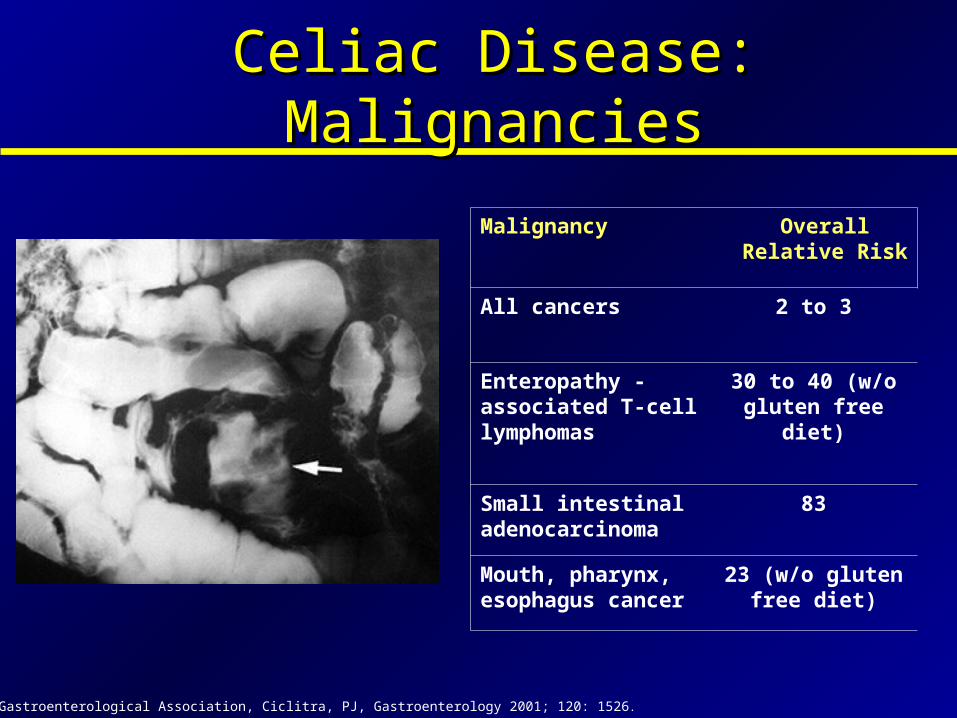
Malignancy Overall Relative Risk
All cancers 2 to 3
Enteropathy -associated T-cell lymphomas
30 to 40 (w/o gluten free
diet)
Small intestinal adenocarcinoma
83
Mouth, pharynx, esophagus cancer
23 (w/o gluten free diet)
Celiac Disease: MalignanciesCeliac Disease: Malignancies
American Gastroenterological Association, Ciclitra, PJ, Gastroenterology 2001; 120: 1526.

Celiac Disease: Type 1 DiabetesCeliac Disease: Type 1 Diabetes
• An association between CD and type 1 diabetes mellitus (T1DM) has been recognized for decades
• Several studies in children and adults, have shown that there is a 1.5% to 7% prevalence of CD in type 1 diabetes
• A community-based study of type 1 diabetics of all ages in Olmsted County, MN, revealed that 6.5% had celiac disease.
Talal AH, et al . Celiac disease in an adult population with insulin-dependent diabetes mellitus: use of endomysial antibody testing. Am J Gastroenterol 1997;92:1280.Fraser-Reynolds KA, et al. Use of immunoglobulin A-antiendomysial antibody to screen for celiac disease in North American children with type 1 diabetes. Diabetes Care 1985;1009:21.Koletzko S, et al . Prevalence of coeliac disease in diabetic children and adolescents: a multicentre study. Eur J Pediatr 1998;148:113.Sigurs N, et al . Prevalence of coeliac disease in diabetic children and adolescents in Sweden. Acta Paediatrica 1993;82:748.Collin P, et al. High frequency of coeliac disease in adult patients with type-I diabetes. Scand J Gastroenterol 1989;24:81.

Celiac Disease: Type 1 DiabetesCeliac Disease: Type 1 Diabetes
• Untreated celiac disease may increase risk of developing type 1 diabetes– Autoantibodies directed against islet cells are frequently
present in untreated CD but disappear with the gluten-free diet
– Patients in whom CD was identified and treated in early childhood had a lower rate of developing diabetes than children in whom CD was diagnosed later in childhood or as adults
Ventura AMG, Greco L. Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. SIGEP Study Group for Autoimmune Disorders in Celiac Disease. Gastroenterology 1999;117:297.
Ventura A, Neri E, Ughi C, Leopaldi A, Citta A, Not T. Glutendependent diabetes-related and thyroid-related autoantibodies in patients with celiac disease. J Pediatr 2000;137:263.

• In one study of 83 patients with autoimmune thyroid disease found a frequency of celiac disease of 4.8 percent
• An epidemiologic study of 335 patients diagnosed with celiac disease between 1980 and 1990 determined that 5.4 percent of the patients with celiac disease also had autoimmune thyroid disease
Celiac Disease: Autoimmune Celiac Disease: Autoimmune Thyroid DiseaseThyroid Disease
Collin P, Reunala T, Pukkala E, Laippala P, Keyrilainen O, Pasternack A. Coeliac disease--associated disorders and survival. Gut 1994;35:1215-8. Collin P, Salmi J, Hallstrom O, Reunala T, Pasternack A. Autoimmune thyroid disorders and coeliac disease. Eur J Endocrinol 1994;130:137-40

Celiac Disease: Other Autoimmune Celiac Disease: Other Autoimmune Endocrine Disorders Endocrine Disorders
Guidetti, CS, et al. Duration of gluten exposure in adult coeliac disease does not correlate with the risk for autoimmune disorders,Gut 2001;49:502–505
In study of 605 controls and 422 patients (aged 16–84 years): 30% of adult patients with CD had at least one AI disease with
an overall 2–3-fold higher frequency than controls.

Celiac Disease: Celiac Disease: Neuropsychologic Features Neuropsychologic Features
• Depression- 10.6%• Epilepsy- 3.5%• Migraine headaches- 3.2%• Anxiety- 2.6%• Suicidal tendency- 2.1%• Carpal tunnel- 1.8%• Myopathy- 1.5%
Holmes, JKT, Acta Paediatr 1996; 412 (Suppl): 68

Celiac Disease: Celiac Disease: Neuropsychologic Features Neuropsychologic Features
• Computed tomographic scan showing occipital calcification in a patient with celiac disease and epilepsy
PRUESSNER, HT. Detecting Celiac Disease in Your Patients. 1998 by the American Academy of Family Physicians University of Texas Medical School at Houston

Celiac Disease: Celiac Disease: Neuropsychologic FeaturesNeuropsychologic Features
• A review of 39 published articles on patients with celiac disease, cerebral calcifications and epilepsy concluded that the exact pathogenic process was unknown
Cuvellier JC, Vallee L, Nuyts JP. Celiac disease, cerebral calcifications and epilepsy syndrome. Arch Pediatr 1996;3:1013-9

Diagnosis of Celiac Diagnosis of Celiac DiseaseDisease

Diagnosis of Celiac DiseaseDiagnosis of Celiac Disease
• Clinical Findings
• Small Intestines Mucosal Biopsy
• Gluten Re-challenge
• Serologic testing
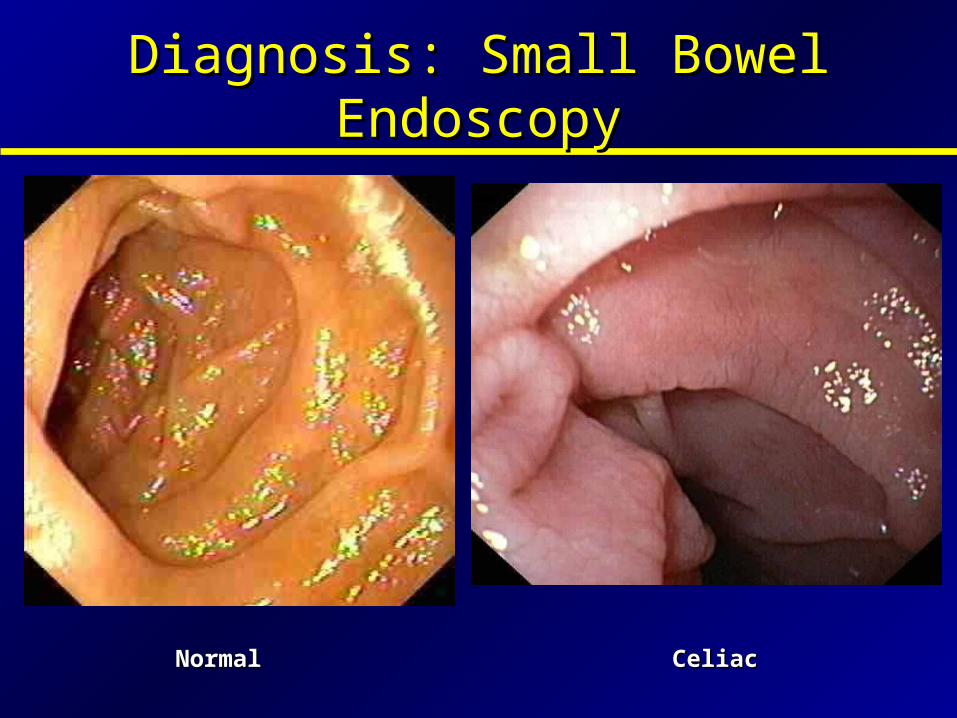
Diagnosis: Small Bowel Diagnosis: Small Bowel EndoscopyEndoscopy
NormalNormal CeliacCeliac

Diagnosis: Small Bowel Diagnosis: Small Bowel EndoscopyEndoscopy

Histologic Findings of Celiac Histologic Findings of Celiac
Normal Jejunum
Virginia Commonwealth Univ, Richmond, Virginia Celiac Disease (Gluten-Induced Enteropathy) 65000-45800-F2923
Celiac

Histologic Findings of CeliacHistologic Findings of Celiac
Normal Flattened Villi in Celiac

Histologic Findings of CeliacHistologic Findings of Celiac
• The lamina propria shows a marked increase in the number of plasma cells and lymphocytes and transepithelial migration of lymphocytes across the surface epithelium (arrow) is common.
Virginia Commonwealth Univ, Richmond, Virginia Celiac Disease (Gluten-Induced Enteropathy) 65000-45800-F2923

Intestinal Lesions of Celiac Disease
Marsh, MN, Gastroenterology 1992; 102:330.

Histologic Findings of CeliacHistologic Findings of Celiac
Virginia Commonwealth Univ, Richmond, Virginia Celiac Disease (Gluten-Induced Enteropathy) 65000-45800-F2923

Other Causes of Villous AtrophyOther Causes of Villous Atrophy
• Bacterial Overgrowth• Crohn’s disease• Cow’s milk protein intolerance (children)• Eosinophilic gastroenteritis• Giardiasis• Lymphoma• Peptic duodenitis• Post gastroenteritis• Tropical sprue• Zollinger Ellison syndrome
American Gastroenterological Association, Ciclitra, PJ, Gastroenterology 2001; 120: 1526.

Diagnosis of Celiac: Gluten Rechallenge
• Gluten Rechallenge- improvement in symptoms and histology with gluten avoidance with a documented return of these features upon gluten reintroduction.
• May be performed by consuming 10 g of gluten per day (an amount contained in four slices of regular bread) for four to six weeks.
• One hazard of rechallenge is development of fulminant diarrhea, with dehydration, acidosis, and other metabolic disturbances ("gliadin shock").
KRAINICK, HG, DEBATIN, F, GAUTIER, E, et al. [Additional research on the injurious effect of wheat flour in celiac disease.I. Acute gliadin reaction (gliadin shock).]. Helv Paediatr Acta 1958; 13:432

• Per the European Society of Paediatric Gastroenterology and Nutrition guidelines: gluten rechallenge is not required in patients with improvement in symptoms, histology, and a decline in the antibody titers.
• Gluten rechallenge is also considered to be unnecessary by the 2004 consensus statement issued by the National Institutes of Health.
Diagnosis of Celiac: Gluten Rechallenge
National Institutes of Health Consensus Development Conference Statement. Celiac Disease 2004. Available at http://consensus.nih.gov. Walker-Smith, JA, Guandalini, S, Schmitz, J, et al. Revised criteria for diagnosis of coeliac disease. Arch Dis Child 1990; 65:909.
Diagnosis of Celiac: Serologic Diagnosis of Celiac: Serologic TestingTesting
• Some of the serologic tests used to diagnose celiac:– IgA and IgG antigliadin antibodies– IgA endomysial antibodies– IgA and IgG tissue transglutaminase
antibodies– Anti reticulin antibodies (no longer used)

• IgA and IgG antigliadin antibody tests are considered less accurate, less sensitive and less specific than other serologic tests.
• Frequent false positive results (15 to 20 %) often leads to unnecessary endoscopy with biopsy
• Therefore, antigliadin antibody is no longer recommended for initial diagnostic evaluation or screening
National Institutes of Health Consensus Development Conference Statement. Celiac Disease 2004. Available at http://consensus.nih.gov. Walker-Smith, JA, Guandalini, S, Schmitz, J, et al. Revised criteria for diagnosis of coeliac disease. Arch Dis Child 1990; 65:909.
Diagnosis of Celiac: Diagnosis of Celiac: Antigliadin AntibodiesAntigliadin Antibodies

• Endomysial antibodies bind to connective tissue surrounding smooth muscle cells
• IgA endomysial antibodies bind to the endomysium, producing a characteristic staining pattern, which is visualized by indirect immunofluorescence.
• IgA endomysial antibody testing is moderately sensitive and highly specific for untreated celiac disease
Diagnosis of Celiac: Diagnosis of Celiac: IgA Endomysial Antibodies Antibodies
National Institutes of Health Consensus Development Conference Statement. Celiac Disease 2004. Available at http://consensus.nih.gov. Walker-Smith, JA, Guandalini, S, Schmitz, J, et al. Revised criteria for diagnosis of coeliac disease. Arch Dis Child 1990; 65:909.

• The antigen against which antiendomysial antibodies are directed is a tissue transglutaminase (tTG)
• IgA anti-tTG antibodies testing by ELISA are considered easier to perform and less costly than the immunofluorescence assay used to detect IgA endomysial antibodies.
• Anti-tTG antibodies are both highly sensitive and specific
Diagnosis of Celiac: Diagnosis of Celiac: Anti-tissue Transglutaminase Antibodies
National Institutes of Health Consensus Development Conference Statement. Celiac Disease 2004. Available at http://consensus.nih.gov. Walker-Smith, JA, Guandalini, S, Schmitz, J, et al. Revised criteria for diagnosis of coeliac disease. Arch Dis Child 1990; 65:909.

Diagnosis of Celiac: Serologic TestingDiagnosis of Celiac: Serologic Testing
•IgA antigliadin antibodies•Sensitivity 80 to 90 %•Specificity 85 to 95 %
•IgA endomysial antibodies•Sensitivity 85 to 98 %•Specificity 97 to 100 %
•IgA tissue transglutaminase antibodies•Sensitivity 90 to 98 %•Specificity 95 to 97 %
Kelly, CP. Coeliac disease: Non-invasive tests to screen for gluten sensitive enteropathy and to monitor response to dietary therapy. Dublin University, Trinity College, Dublin 1995. Kelly, CP, Feighery, CF, Gallagher, RB, et al. Mucosal and systemic IgA anti-gliadin antibody in celiac disease. Contrasting patterns of response in serum, saliva, and intestinal secretions. Dig Dis Sci 1991; 36:743.

• IgA deficiency is more common in celiac disease (2 to 5 percent) than in the general population (<0.5 percent).
• IgA EMA and IgA tTG will be falsely negative in patients with IgA deficiency.
• Thus, total serum IgA should be also measured in addition to IgA EMA or IgA tTG
• If total IgA levels are abnormally low, consider IgG-based assay
Diagnosis of Celiac: IgADiagnosis of Celiac: IgA
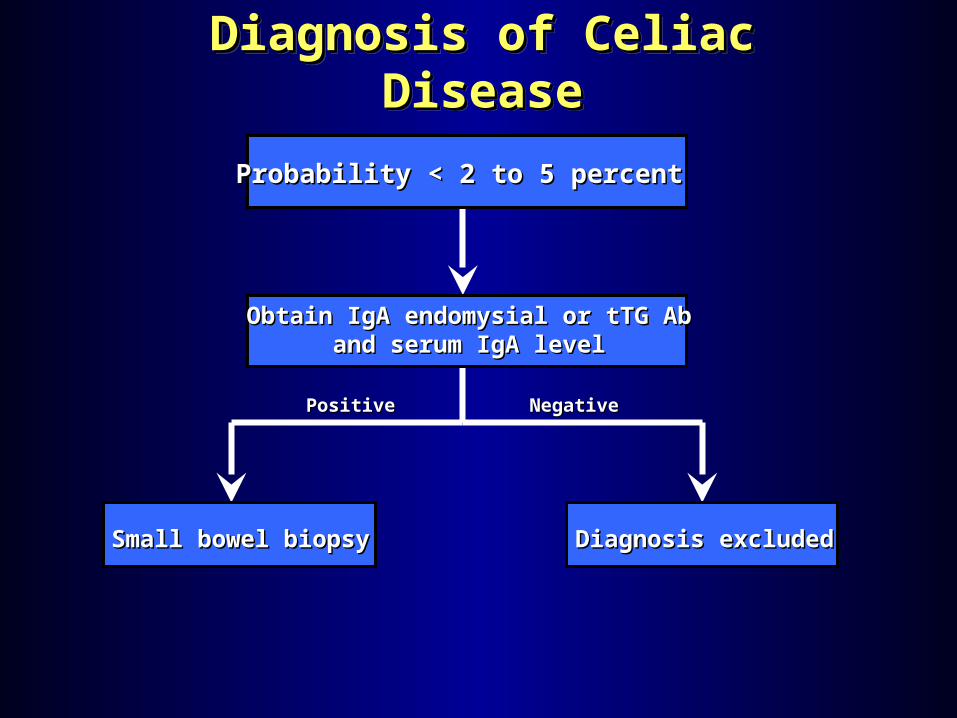
Diagnosis of Celiac DiseaseDiagnosis of Celiac DiseaseDiagnosis of Celiac DiseaseDiagnosis of Celiac Disease
PositivePositive NegativeNegative
Probability < 2 to 5 percentProbability < 2 to 5 percent
Obtain IgA endomysial or tTG AbObtain IgA endomysial or tTG Aband serum IgA leveland serum IgA level
Small bowel biopsySmall bowel biopsy Diagnosis excludedDiagnosis excluded

Probability > 2 to 5 percentProbability > 2 to 5 percent
IgA endomysial or tTG Ab + IgAIgA endomysial or tTG Ab + IgAAND Small bowel biopsyAND Small bowel biopsy
•Family historyFamily history•Unexplained iron deficiency anemiaUnexplained iron deficiency anemia•Steatorrhea or other GI symptomsSteatorrhea or other GI symptoms•Failure to thriveFailure to thrive•Type 1 diabetes mellitus or other Type 1 diabetes mellitus or other associated disordersassociated disorders•Other symptomsOther symptoms{
Both Both positivepositive
Histology -Histology -
Serology +Serology +
Histology +Histology +
Serology -Serology -
Both Both negativenegative
Review and/or Review and/or repeat biopsyrepeat biopsy
Diagnosis Diagnosis excludedexcluded
Rule out Rule out other other
causes of causes of villous villous atrophyatrophy
-- ++++TREATTREAT
--

Management of Celiac Management of Celiac DiseaseDisease

Management of Celiac DiseaseManagement of Celiac Disease
• Gluten avoidance is the mainstay of treatment• Prior to the introduction of a strict gluten-free
diet, prognosis was very poor• Mortality was 12 percent in one retrospective
study of 544 children
Hardwick, C. Prognosis in coeliac disease. Arch Dis Child 1939; 14:279

Management of Celiac DiseaseManagement of Celiac Disease
In general, the following advice can be given to all patients:
• Foods containing wheat, rye, and barley should be avoided.
• Soybean or tapioca flours, rice, corn, buckwheat, and potatoes are safe.
• Read labels on prepared foods and condiments carefully (many stabilizers or emulsifiers contain gluten)
• Dairy products may need to be avoided initially- many patients have secondary lactose intolerance.

Foods That May Contain Gluten
• Bouillon Cubes• Canned soups• Catsup• Cheese spreads• Chips and dips mixes• Hot chocolate mixes
or cocoa• Ice cream• Luncheon meats• Meat sauces (soy,
Worcestershire, etc)
• Mustard• Non-dairy creamer• Peanut butter• Processed canned
meats and poultry• Salad dressing• Soup mixes• Tomato sauces• Wieners and other
sausages products• Yogurt with fruit
Trier, JS. Celiac Sprue and refractory sprue. In: Sleisenger and Fordtran’s Gastrointestinal and Liver Disease, 6th Ed, Feldman, M,Scharscmidt, BF, Sleisenger, MH (Eds), Saunders, Philadelphia 1998. p. 1568

What about oats?
•Whether oats may be included in a gluten free diet is controversial
• Some studies suggest that oats can be tolerated without disease recurrence
Taxonomy of Grains
KAGNOFF, MF. “Overview and Pathogenesis of Celiac Disease” GASTROENTEROLOGY 2005;128:S10–S18
Gliadins Secalins Hordeins Avenins Zeins

• In one study, 52 adults with celiac disease in remission and 40 with newly diagnosed celiac disease were randomly assigned to a gluten-free diet without oats, or a gluten-free diet with a total daily consumption of 50 to 70 g of oats.
• At the end of one year, no significant difference were observed in the nutritional status, symptoms, or laboratory or histologic measures between the two groups
What about oats?
Janatuinen, EK, Pikkarainen, PH, Kemppainen, TA, et al. A comparison of diets with and without oats in adults with celiac disease. N Engl J Med 1995; 333:1033
• Another controlled trial involved 39 adults who were randomly assigned to either a gluten-free diet with 50 g of oat-containing products daily or to a gluten-free diet without oats for one year.
• Quality of life scores were similar between the groups, and there were no significant differences in the villous structure of small bowel biopsies.
• However, patients consuming oats had significantly more gastrointestinal symptoms (including diarrhea and constipation) and had a significantly higher density of intraepithelial lymphocytes
What about oats?
Peraaho, M, Kaukinen, K, Mustalahti, K, et al. Effect of an oats-containing gluten-free diet on symptoms and quality of life in coeliac disease. A randomized study. Scand J Gastroenterol 2004; 39:27

• Limit oat consumption to 50 to 60 g/day (approximately 2 oz) in patients with mild disease or whose disease is in remission after a stringent gluten-free diet.
• Patients should be followed carefully for clinical or serologic evidence of disease recurrence after reintroducing oats.
• Patients with severe disease should avoid oats altogether
What about oats?
Lundin, KE, Nilsen, EM, Scott, HG, et al. Oats induced villous atrophy in coeliac disease. Gut 2003; 52:1649.Thompson, T. Gluten contamination of commercial oat products in the United States. N Engl J Med 2004; 351:2021. Hoffenberg, EJ, Haas, J, Drescher, A, et al. A trial of oats in children with newly diagnosed celiac disease. J Pediatr 2000; 137:361

Monitoring Adherence by Serologic Testing
•Monitoring response to gluten free diet by measuring levels of antibodies is controversial•Variations in test results between assays may be substantial and make interpretation difficult or impossible. •It is unknown if monitoring antibodies improves outcomes or is cost effective
NATIONAL INSTITUTES OF HEALTH, CONSENSUS DEVELOPMENT CONFERENCE STATEMENT: Celiac Disease.June 28–30, 2004

Management of Celiac DiseaseManagement of Celiac Disease
Serum IgA antigliadin titers at diagnosis and after 12 – 16 months of dietary therapySerum IgA antigliadin titers at diagnosis and after 12 – 16 months of dietary therapy
N=20N=10
• A pretreatment antibody level should be determined at the time of diagnosis.
• Serologic testing is of no use if antibody levels are not elevated prior to therapy.
• Exclusion of gluten from the diet results in a gradual decline in serum IgA antigliadin and IgA tTG levels.
• A normal baseline value is typically reached within three to six months.
• If the levels do not fall as anticipated, the patient may be continuing to ingest gluten either intentionally or inadvertently
Monitoring Adherence by Serologic Testing
Kelly, CP. Coeliac disease: Non-invasive tests to screen for gluten sensitive enteropathy and to monitor response to dietary therapy. Dublin University, Trinity College, Dublin 1995.
Summary: Management of Celiac Summary: Management of Celiac DiseaseDisease
• Consultation with a skilled dietitian • Education about the disease • Lifelong adherence to a gluten-free diet • Identification and treatment of nutritional
deficiencies • Access to an advocacy group • Continuous long-term follow-up by a
multidisciplinary team
NATIONAL INSTITUTES OF HEALTH, CONSENSUS DEVELOPMENT CONFERENCE STATEMENT: Celiac Disease.June 28–30, 2004
A recent NIH statement recommended the following strategy when managing individuals with celiac disease:

Questions?Questions?Questions?Questions?