this 32 year old man presented with 2 weeks of visual loss ... pupil •pupils less than 2 mm in...
TRANSCRIPT

This 32 year old man presented with 2 weeks of visual loss OS. He first noted central blur 15 days ago, which has persisted, along with mild aching OS with extreme eye movement. Over the last day the central blur has improved, in that he can now see vague shapes. He denies other neurologic symptoms now or in the past. Medications: none. Past medical history: migraine, asthma, depression. Allergies: milk and wheat Family history: He has a brother well, no kids, glaucoma in father’s family. Social history: He does not smoke, drinks once or twice a month. Examination: Acuity without correction at far is 20/15 od and count fingers os. Pseudo-isochromatic plates are 14/14 od and 0/14 os. There is large RAPD os. Confrontation fields show full fields od, central depression os. Funduscopy (dilated os) shows normal optic discs ou, normal macula os, no central serous retinopathy. Pupils are 3 mm ou in light and 5 mm ou in dark. Palpebral fissures are symmetric. Ductions are full. Fixation is steady. Pursuit and VOR cancellation are intact. Saccades are rapid and accurate, no INO. There is no nystagmus. The rest of the neurological examination is normal.




VA Distant
6/60
6/30
6/20
6/15
6/12
6/9
6/7.5
6/6
6/5
6/4
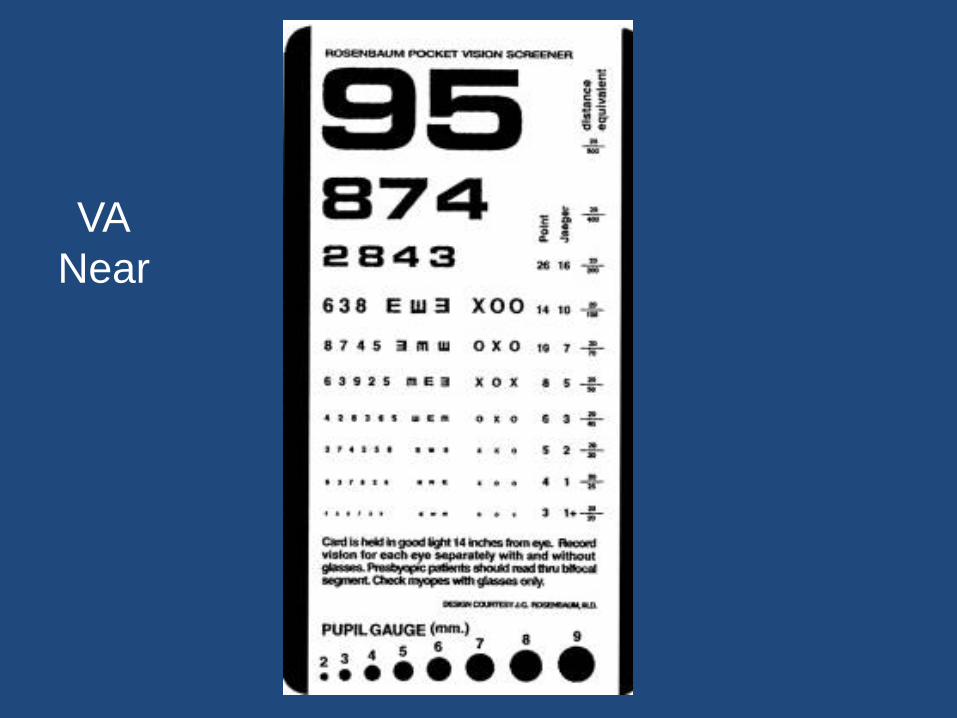
VA
Near

Visual Acuity
• Snellen’s near and distant
• For vision < 6/60
– 1,2,3,4,5 /60
– CF, HM,LP, NLP


– OD (Latin oculus dexter) for the right eye.
– OS (Latin oculus sinister) for the left eye.
– OU (Latin oculi uterque) for both eyes.

– cc (Latin cum correctore) with correctors.
– sc: (Latin sine correctore) without correctors
– D (distant) for the evaluation done at 20 feet (or 6 meters).
– N (near) for the evaluation done at 15.7 inches (or 40 cm).
– PH for pinhole correction – myopia and astigmatism

• Distant visual acuity of 20/60 and 20/25 with pinhole in the right eye will be: DscOD 20/60 PH 20/25
• Distant visual acuity of count fingers and 20/50 with pinhole in the left eye will be: DscOS CF PH 20/50

• Near visual acuity of 20/25 with pinhole remaining at 20/25 in both eyes with spectacles will be:
NccOU 20/25 PH 20/25

Illiterate Charts
• Tumbling E
• Lea Picture charts
• Landolt C

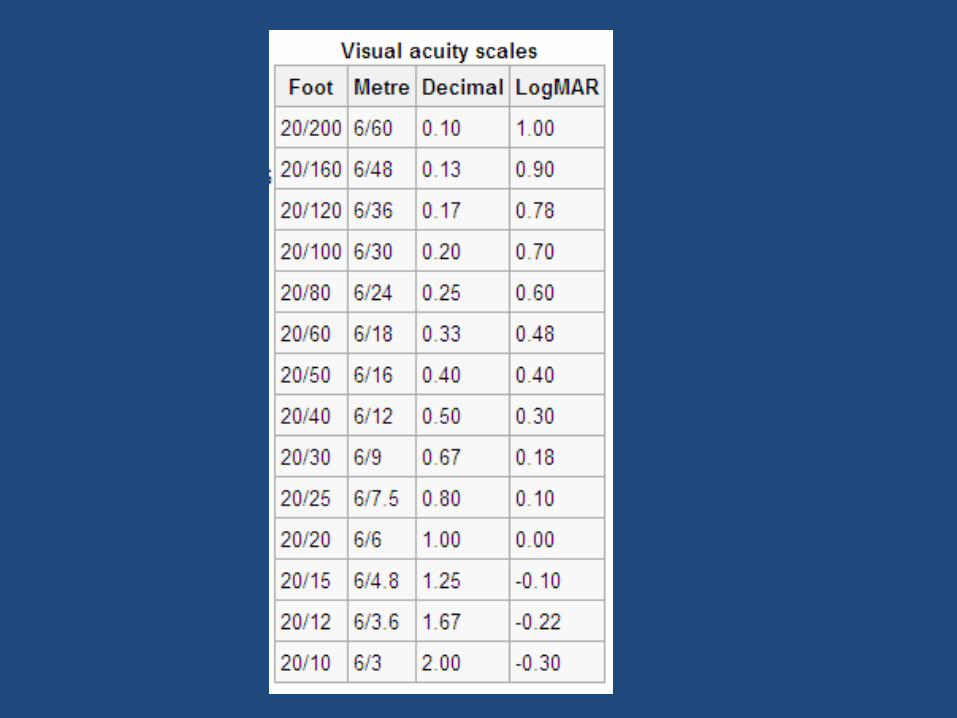
LogMAR Chart

LogMAR
• Logarithm of the mean angle of resolution
• Done at a distance of 4m
• The 6/6 line of Snellen equates to 0 on LogMAR
• At 6/6 the letter E has a resolution of 5 degrees with each line of 1 degree
• Log 1 = 0

• 5 letters on each line
• Each letter not seen contributes 0.02 points
• Poorer the VA, the larger the score
• At 6/6 the LogMAR is 0
• If patient can see 4 only, LogMAR is 0.02
• If patient sees one letter only, LogMAR is 0.08
• If patient sees none on the 6/6 line, LogMAR is 0.1 which is the score of the line above
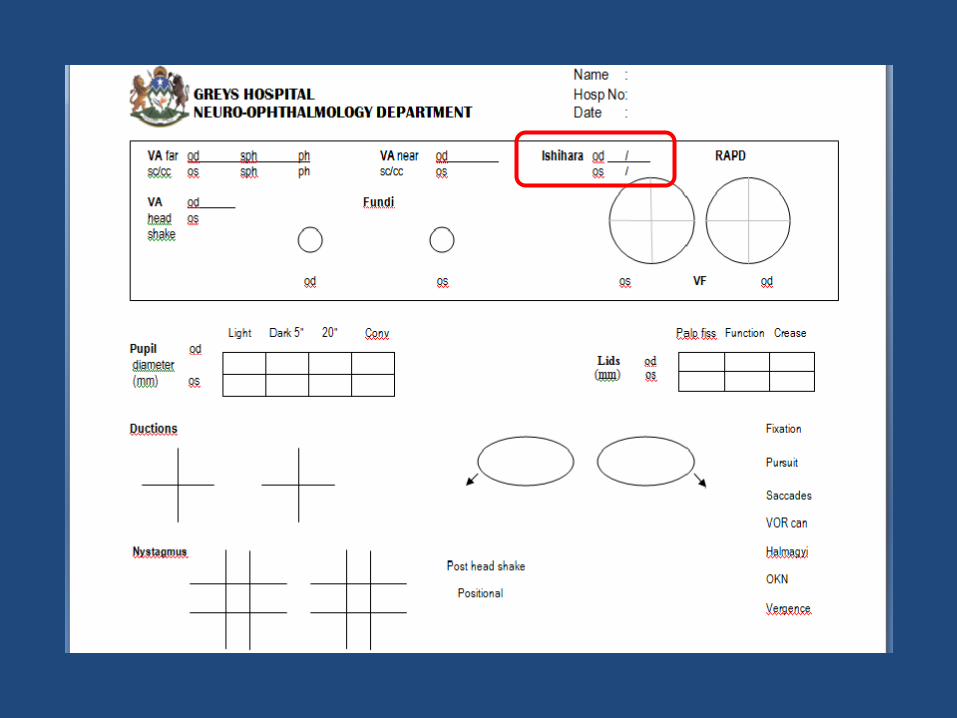

Ishihara colour plates
• Given as a score
• Denominator is either 13,14,15,17
• Useful for initial evaluation and follow up


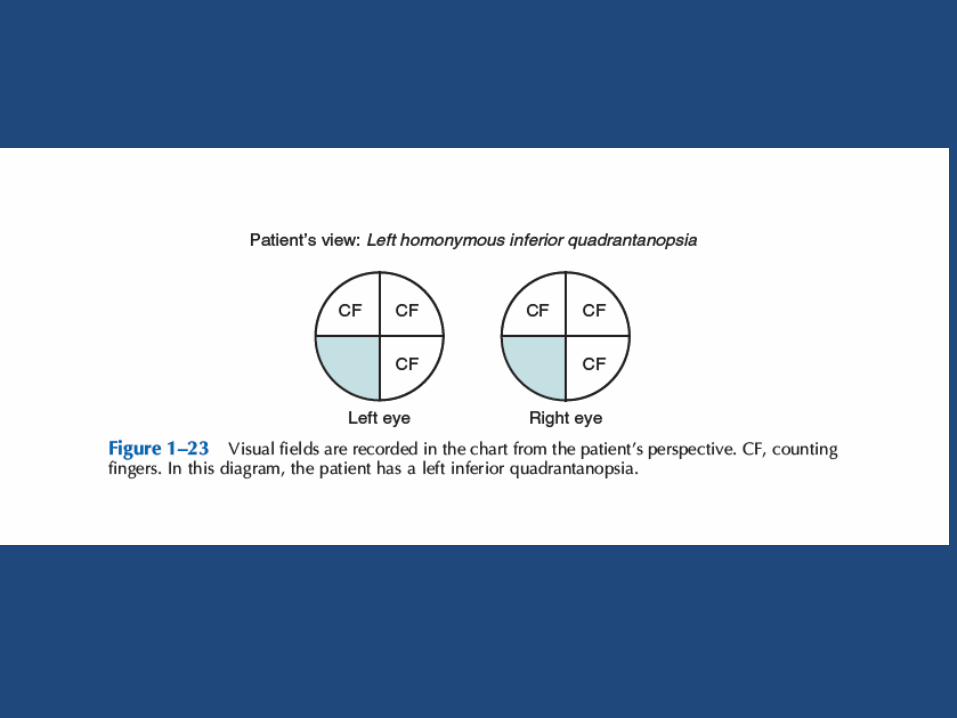
Visual Field testing by
Confrontation

Statokinetic Dissociation (Riddoch’s Phenomenon)
• Preservation of perception of motion in an otherwise blind hemifield
• Activation of extrastriate areas (V5)
• Residual island of function in the striate cortex
• Lateral summation of moving images
• Good prognostic sign in patients with homonymous hemianopia from an occipital CVA
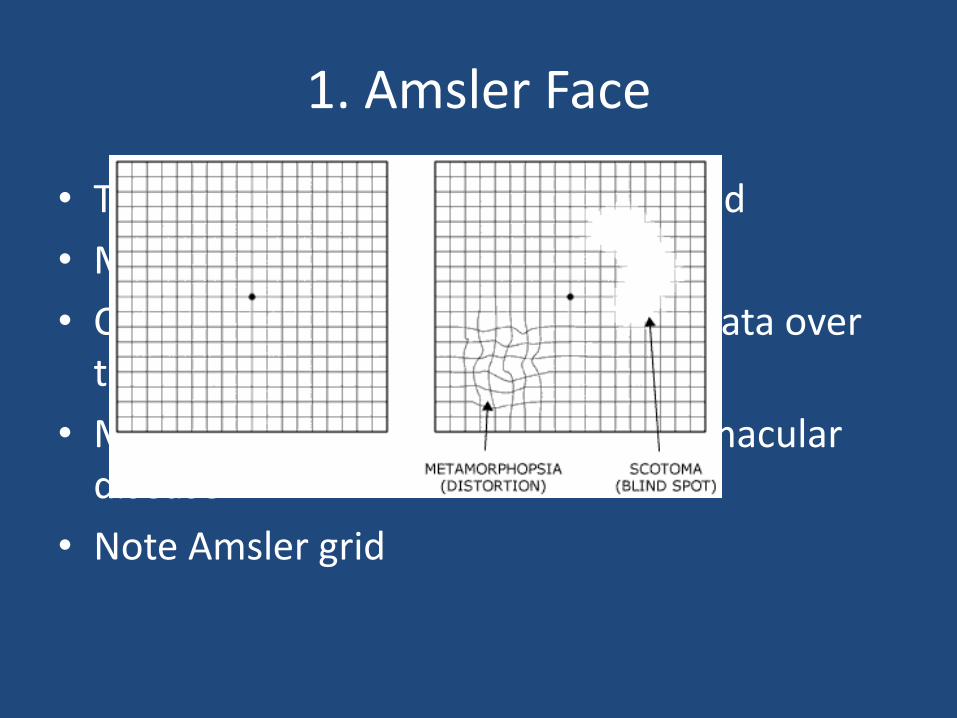
1. Amsler Face
• Tests central 10 degrees of visual field
• Macular region is tested
• Comment on loss of parts or scotomata over the different parts
• Metamorphopsia of parts suggests macular disease
• Note Amsler grid

2. Counting Fingers
• Test each quadrant for each eye
• Adding the fingers is also useful

3. Hand Comparison
• Detects subtle altitudinal or hemifield defects
• Both hands may be seen but one may be vague or appears as a shadow

4. Peripheral field
• Tests 30-60 degrees of field
• Useful for detecting constriction
• Use red target for subtle central field defect – optic neuropathy
• Use blue target in periphery for constricted defects from papilloedema


The dials of the ophthalmoscope.
• In the front there is a switch for white light, green light and cobalt blue
• The green light (or red free filter) is particularly good for looking for drusen or for nerve fibre defects
• Cobalt blue is also used for RNFL
• The smaller light is good for small, undilated pupils, but the larger light provides better illumination.
The dials of the ophthalmoscope.
• bulls-eye” with a cross hatch is used for measurements or to identify where the patient is looking
• narrow slit beam is useful to view a lesion in the retina--if the beam is not distorted, the lesion is flat, if the lesion is elevated the beam is raised toward the observer.

The dials of the ophthalmoscope.
• The “wheel” has lenses with different dioptres of power.
• Dioptre is unit of optical power of a lens
• Equal to 1/focal length
• 3 dioptre lens brings parallel rays of light to focus at 1/3 metre

The dials of the ophthalmoscope.
• The red numbers are negative power (for near-sighted individuals, long eyes, and myopia)
• black or green numbers are positive power (for far-sighted individuals, short eyes, and hyperopia).


Technique
• check if ophthalmoscope is in good working condition
• inform the pt that you are going to flash bright light in his eyes to have a look at the back of his eyes and during examination u will come very near to his face
Technique
• DIM LIGHT examination of right eye - ophthalmoscope held in right hand and look through with your right eye vice versa is for left eye
Technique
• --hold instrument to eye with index finger on the lens dial --approach from shallow angel (15--20 degree) --approach on the same level as equator --note and comment on red reflex --note and comment on anterior surface of eye --come near and focus on retina --identify optic disc and comment on colour, cup, size and margins --follow blood vessels in 4 quadrants --seek to identify the macula and fovea

Technique
• The lens normally magnifies the back of the eye. When the lens has been surgically removed, this magnifying effect is lost. You can then see a much larger expanse of fundus.
•

Identify any lesions. Note their size shape colour and distribution. As you search the retina, move your head and ophthalmoscope as one unit. Next, ask the patient to look directly at the light OR, direct your light beam laterally. This will bring the macula into view.
• If you can’t find the optic disc, find any vessel and follow it centrally to the disc.
• Now, from the optic disc, follow the vessels peripherally in all four directions. Note size and character of vessels and arteriovenous crossings.

Normal Disc appearance is driven by the shape of the globe, the size of the scleral canal, and what is left behind in development.
Normal disc
• The disc is the slightly oval, pink structure
• The lamina cribrosa is a connective tissue “sieve” consisting of a fibrocollagenous weave of holes that “bundles” the million axons as they cross into the retrobulbar optic nerve
• The physiologic cup size varies from less that 0.1 to 0.9 of the total disc diameter. The usual cup to disc ratio is about 0.3.


The surface layer is the nerve fibre layer from all over the retina Its appearance is like fine horsehairs

- divides into superior and inferior branches. It further
branches to supply 4 quadrants of the retina.
The Central Retinal Artery

Cilioretinal Artery is present in 32% of eyes Looks like a hook Blood supply to the central retina

• Look for spontaneous venous pulsations
• Absent in 20% of eyes
• Look at normal variations of the fundus
– Colour. Blondes have light coloured fundus
– Blacks – Heavy pigmentation of fundus
– With age, more pigmentation is found


Normal Pupil
• The normal pupil is 2 mm to 6 mm in diameter.
• In ordinary ambient light the pupils are usually 3 mm to 4 mm in diameter.
Normal Pupil
• The pupils are small and poorly reactive at birth and in early infancy, becoming normal size around ages 7 to 8.
• They are normally larger in adolescents and young adults, about 4 mm in diameter and perfectly round.
• In middle age, they are typically 3.5 mm in diameter and regular, and in old age 3 mm or less and often slightly irregular.

Miotic pupil
• Pupils less than 2 mm in diameter are miotic.
• Common causes of acquired miosis include old age, hyperopia, alcohol abuse, and drug effects.

Miotic pupil
• Neurologically significant causes of miosis include
– neurosyphilis,
– diabetes,
– levodopa therapy
– Horner's syndrome.

Miotic pupil
• Acute, severe brainstem lesions, such as pontine hematoma, may cause bilaterally tiny, “pinpoint” pupils that still react.
• Due to bilateral sympathetic pathway lesions
• Normal reaction is confirmed using magnifying lenses

Mydriatic Pupil
• Pupils more than 6 mm in diameter are dilated.
• Common causes of bilateral mydriasis include anxiety, fear, pain, myopia, and drug effects—especially anticholinergics.
• Large pupils were once considered a sign of youth and beauty, and the anticholinergic belladonna (Ital. “fair lady”) alkaloids were named for their ability to produce this effect.

Mydriatic Pupil
• Persons with light irises have larger pupils than those with dark irises.
• Only severe, bilateral lesions of the retina or anterior visual pathways, enough to cause near blindness, will affect the resting pupil size.

Mydriatic Pupil
• Neurologically significant bilateral mydriasis occurs in
– midbrain lesions
– comatose patients following cardiac arrest
– cerebral anoxia
Light reflexes
• Direct and consensual reflexes
• Measure pupil sizes in light and darkness
• Look for dilatation lag in Horner’s syndrome by measuring pupil size at 5 and 20 seconds in darkness


• Swinging flashlight test
– Bright hand light in a darkened room
– Patient should fix on a distant object
– Light should cross from one eye to the other fairly rapidly and remain 3 to 5 seconds on each eye to allow pupillary stabilization

Relative afferent Pupillary Defect (Marcus Gunn Pupil)
• Amount of light transmitted from one eye is less than the other eye. During swinging flashlight, the fol may be noted from normal eye to defective eye
1+ Initial constriction. Greater escape to larger intermediate size
2+ No change in pupil size initially. Followed by dilatation of pupil
3+ Immediate dilation of pupil, instead of normal initial constriction
4+ Immediate dilation of pupil, NPL VA




Lid Anatomy
• Eyelid opening and closing is mediated through 3 muscle groups
– Levator palpebrae: elevator of upper eyelid
– Muller’s muscles: LL known as inferior tarsal muscle
– Orbicularis oculi: closure of upper and lower lids

Lid Anatomy
• Innervation of 3 muscle groups
– Levator palpebrae: Sup division of 3rd cranial nerve
– Muller’s muscles: 3rd order neuron of oculosympathetic pathway
– Orbicularis oculi: 7th cranial nerve

Lid Physiology
• The normal upper eyelid in primary position crosses the iris between the limbus (junction of the iris and sclera) and the pupil, usually 1 mm to 2 mm below the limbus;
• The lower lid touches or crosses slightly above the limbus.
• Normally there is no sclera showing above the iris.
Lid Physiology
• The palpebral fissures are normally 9 mm to 12 mm from upper to lower lid margin.
• Measurement can also be made from the lid margin to the corneal light reflex. The upper lid margin is normally 3 mm to 4 mm above the light reflex.

Lid Physiology
• Levator function can be assessed by measuring the upper lid excursion from full downgaze to full upgaze just to the point where the frontalis begins to contract.
• This excursion is typically 10 mm to 12 mm.
• Upper lid excursion of 4 mm or less indicates poor levator function
• 8 mm or more indicates good function.

Disorders
• Abnormalities of eyelid opening
• Abnormalities of eyelid closure

Aponeurotic Ptosis
• Aponeurotic
– Ptosis is consistent in all positions of gaze
– Good levator function (>10mm)
– Raised skin crease
– Thinned upper lid may be almost transparent

Aging may cause levator dehiscence disinsertion (LDD)—with stretching,
thinning, or detachment of the aponeurosis.
Normally, with the eyelids gently closed, the upper lid margin lies 5 mm to 7 mm
below the upper lid fold (the skin fold at the upper part
of the lid).
An increase in this distance suggests LDD (Figure 14.16). The lid excursion is
normal, usually 9 mm or more.
Lid Dehiscence Disinsertion

Lid Dehiscence


Observation
• Ocular alignment
• Associated ptosis/ anisocoria
• Range of eye movements
• Abnormal eye movements
– Nystagmus
– Ocular Oscillations
Ductions
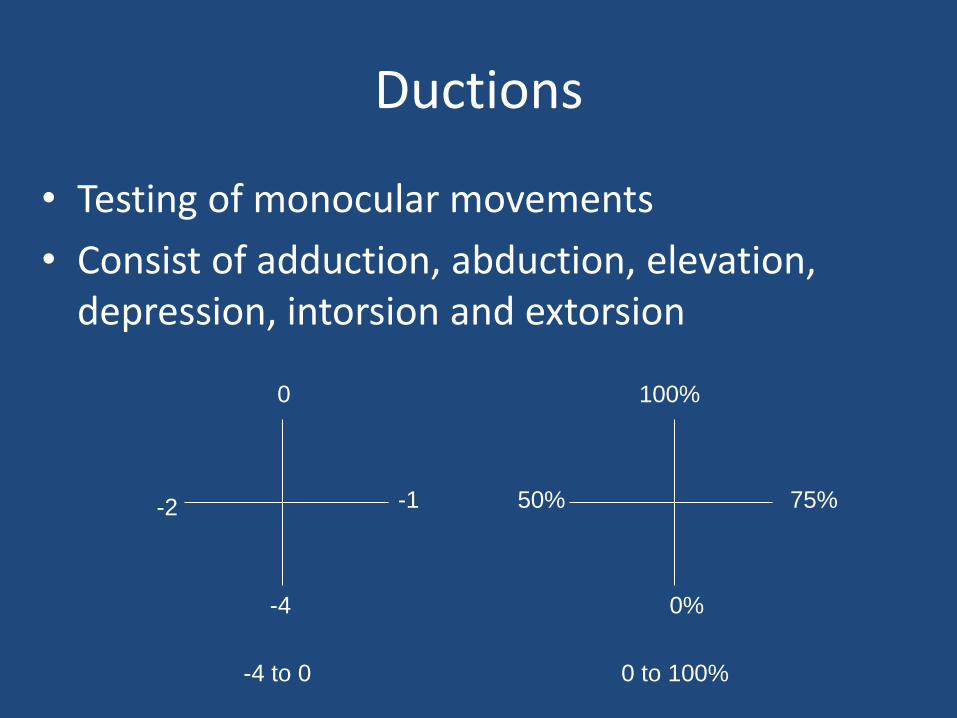
• Testing of monocular movements
• Consist of adduction, abduction, elevation, depression, intorsion and extorsion
0
-2 -1
-4
50%
100%
75%
0%
-4 to 0 0 to 100%

SR
LR
IR
IO
MR
SO
Cover test: outer most image is the false image

Ocular alignment
• Phoria – ortho/hetero – latent squint
• Tropia – manifest squint
• Eso/Exo – deviation along horizontal plane
• Hyper/Hypo – deviation along vertical plane
• XT = exotropia X’T = exophoria
• ES = esotropia E’S = esophoria
• HT = hypertropia H’T = hypotropia

Cover Tests
• Alternate cover test – detects misalignments with phorias and tropias
• Cover/Uncover test – differentiates between phorias and tropias.
– More useful for congenital strabismus where the fixating eye determines the squint

• Phorias and tropias are measured using prisms
• Prisms are graded in dioptres
• Alternate cover test is done with prisms adjusted in front of the deviated eye until no deviation is noted
• Base out prism for esodeviation
• Base in prism for exodeviation
• Base down prism for hyperdeviation
• Base up prism for hypodeviation

Prism Bars

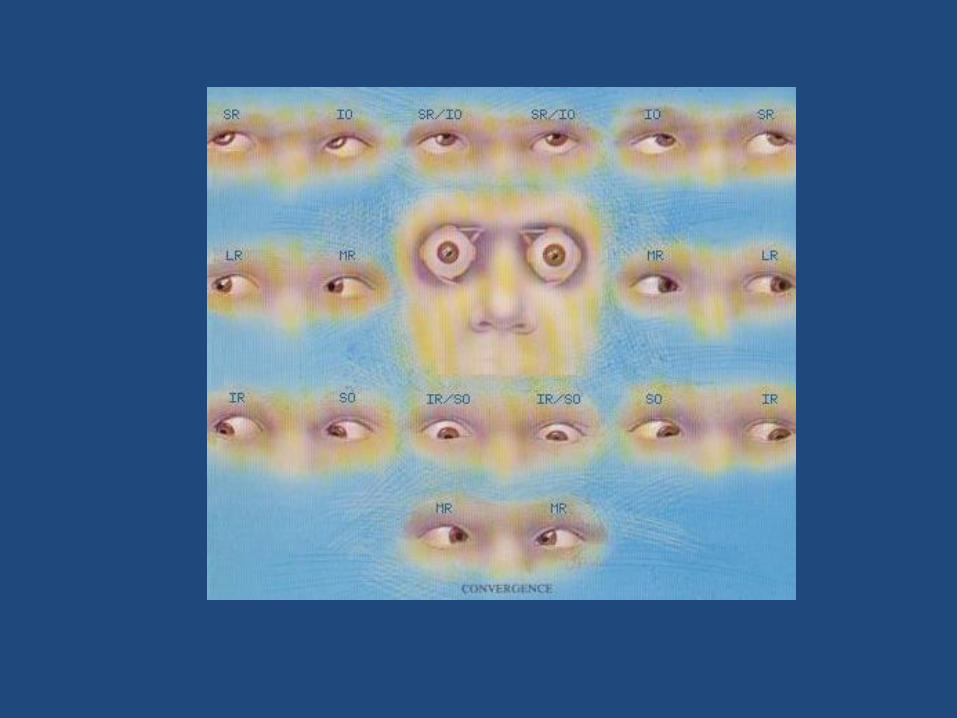
Versions
• Binocular, simultaneous , conjugate movements of eyes in 9 cardinal positions
• Primary position – Fixation tested
• On right gaze, left gaze, upgaze and downgaze – secondary positions tested
• Gaze up and right, gaze down and right, gaze up and left, gaze down and left – tertiary positions
• Head tilt – test cycloversion
Laws of Ocular Motility • Agonist – antagonist – pairs of muscles of the
same eye that move the eye in opposite directions eg Medial rectus and lateral rectus
• Synergists – muscles of the same eye that move the eye in the same direction – superior rectus and inferior oblique elevate the eye
• Yoke muscles – pairs of muscles, one in each eye that produce conjugate ocular movements eg Left SO and Right IR
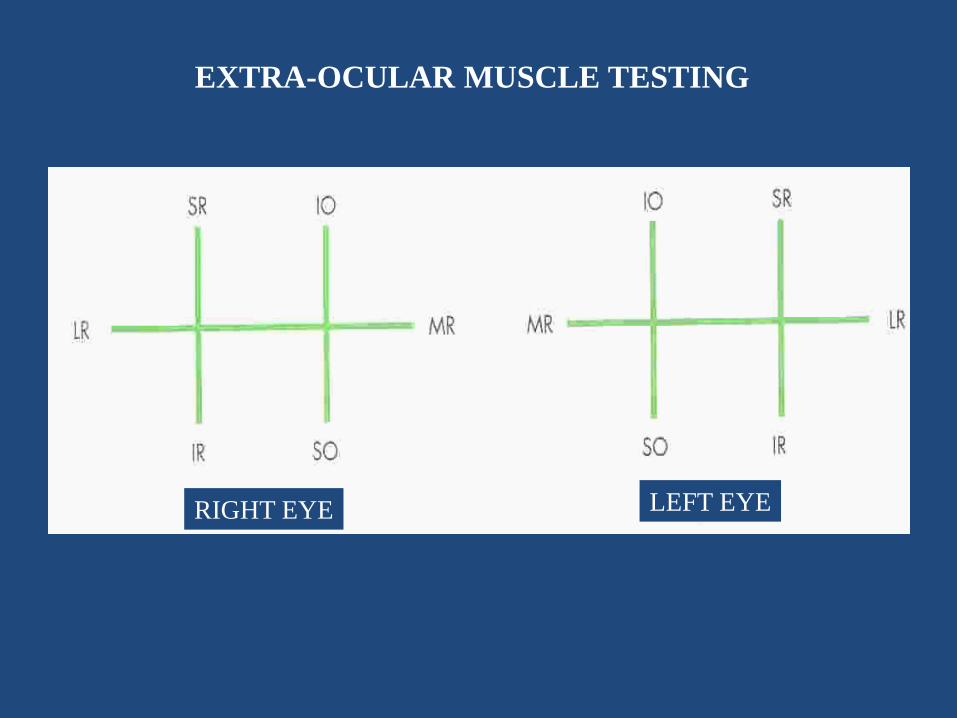
EXTRA-OCULAR MUSCLE TESTING
RIGHT EYE LEFT EYE

Laws of Ocular Motility
• Sherrington’s Law of reciprocal innervation
– Increased innervation to an agonist is accompanied by reciprocal decrease in innervation to an antagonist
• Hering’s Law of equal innervation
– During conjugate eye movement, equal and simultaneous innervation flows to the yoke muscles
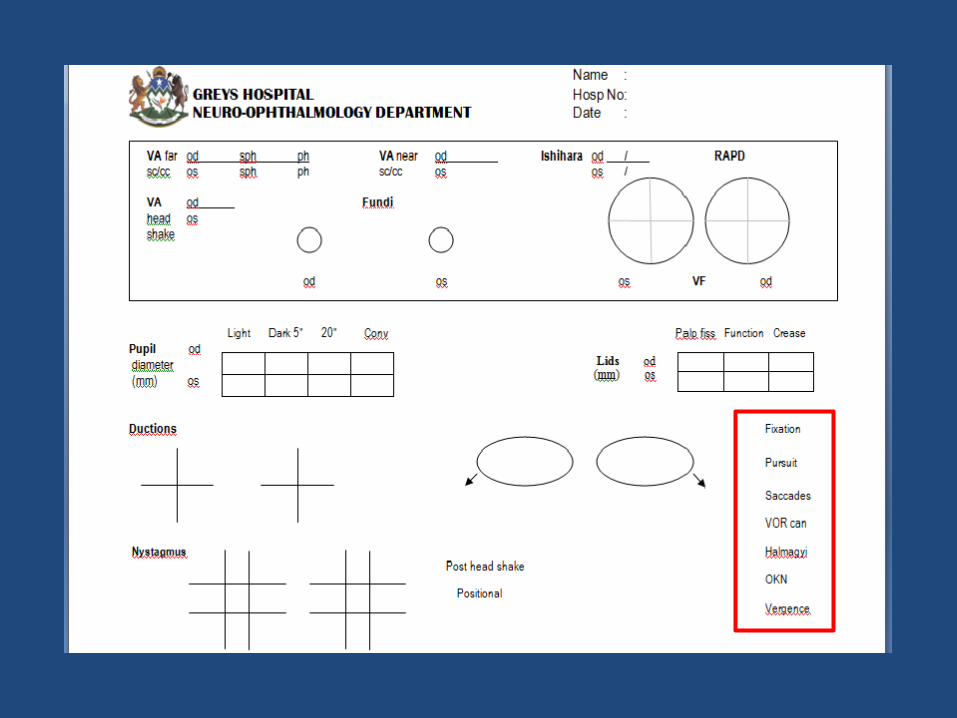

Supranuclear testing
• FIXATION – look for square wave jerks, saccadic oscillations
• SACCADES- between 2 targets. First horizontal then vertical. Tests initiation, speed, accuracy
Between a peripheral target and your nose – tests accuracy- hypo/hypermetric saccades. Reveals lateropulsion

• PURSUIT – patient follows a slow moving target. Look for saccadic pursuit
• VOR – head impulse test. Tests for peripheral vestibular dysfunction. Corrective saccades made when impaired
• VOR cancellation – Patient rotated on a chair while fixating on extended thumbs on outstretched arms. Look for jerky eye movements. Indicates cerebellar dysfunction

• OPTOKINETIC NYSTAGMUS – use an OKN drum or striped tie. Tests parietal lobe function and useful for functional vision loss
• VERGENCE – Test ability to follow a moving target towards the patients nose. Test fixation at distance then to target close to nose. Examine for convergence and pupillary constriction

Nystagmus
• Binocular or monocular?
• Binocular symmetric or dissociated?
• Conjugate or dysconjugate?
• Spontaneous in primary position?
• Gaze-evoked in eccentric position
• In all positions of gaze? Null point? Vary in different gaze positions?
• Fast and slow phase – Jerk nystagmus?
• Equal speed in both directions – Pendular nystagmus?

Moderate frequency Moderate amplitude Upbeat nystagmus
Low frequency High amplitude Right beating nystagmus
Low frequency Moderate amplitude Pendular nystagmus
High frequency Low amplitude Left beating nystagmus
Low frequency High amplitude Torsional nystagmus

Vestibular testing
• VA with head shaking at 1Hz should not lose > 1 line on Snellen in both horizontal and vertical directions
• Post head shaking nystagmus implies vestibular imbalance. Best done with Frenzel goggles
• Dix Hallpike test for positional nystagmus
• Halmagyi test – Head impulse test – tests VOR

This 32 year old man presented with 2 weeks of visual loss OS. He first noted central blur 15 days ago, which has persisted, along with mild aching OS with extreme eye movement. Over the last day the central blur has improved, in that he can now see vague shapes. He denies other neurologic symptoms now or in the past. Medications: none. Past medical history: migraine, asthma, depression. Allergies: milk and wheat Family history: He has a brother well, no kids, glaucoma in father’s family. Social history: He does not smoke, drinks once or twice a month. Examination: Acuity without correction at far is 20/15 od and count fingers os. Pseudo-isochromatic plates are 14/14 od and 0/14 os. There is large RAPD os. Confrontation fields show full fields od, central depression os. Fundoscopy (dilated os) shows normal optic discs ou, normal macula os, no central serous retinopathy. Pupils are 3 mm ou in light and 5 mm ou in dark. Palpebral fissures are symmetric. Ductions are full. Fixation is steady. Pursuit and VOR cancellation are intact. Saccades are rapid and accurate, no INO. There is no nystagmus. The rest of the neurological examination is normal.