third annual meeting of the regional verification …participants of the third annual meeting of the...
TRANSCRIPT
18–21 March 2014Seoul, Republic of Korea
Meeting Report
Third Annual Meeting of theRegional Verification Commission
for Measles Elimination in the Western Pacific
Participants of the Third Annual Meeting of the Regional Verification Commission for Measles Elimination in the Western Pacific,
18–21 March 2014, Seoul, Republic of Korea

RS/2014/GE/04(KOR) English Only
REPORT
THIRD ANNUAL MEETING OF THE REGIONAL VERIFICATION COMMISSION
FOR MEASLES ELIMINATION IN THE WESTERN PACIFIC
Convened by:
WORLD HEALTH ORGANIZATION
REGIONAL OFFICE FOR THE WESTERN PACIFIC
Seoul, Republic of Korea
18–21 March 2014
Not for sale
Printed and distributed by:
World Health Organization
Regional Office for the Western Pacific
Manila, Philippines
May 2014

NOTE
The views expressed in this report are those of the participants of the Third Annual
Meeting of the Regional Verification Commission for Measles Elimination in the Western
Pacific, held from 18 to 21 March 2014 in Seoul, Republic of Korea, and do not necessarily
reflect the policies of the World Health Organization.
This report has been prepared by the World Health Organization Regional Office for the
Western Pacific for governments of Member States in the Region and for the participants of the
Third Annual Meeting of the Regional Verification Commission for Measles Elimination in the
Western Pacific held from 18 to 21 March 2014 in Seoul, Republic of Korea.
SUMMARY
The Third Annual Meeting of the Regional Verification Commission for Measles
Elimination in the Western Pacific was held in Seoul, Republic of Korea, from
18 to 21 March 2014.
The Regional Verification Commission (RVC) for Measles Elimination was established in
January 2012 in line with WHO Regional Committee for the Western Pacific resolution
WPR/RC61.R7 and the recommendation of the Technical Advisory Group on Immunization and
Vaccine-Preventable Diseases. The RVC held its inaugural meeting in April 2012 and its second
meeting in March 2013.
In September 2012, the Regional Committee passed a resolution urging Member States to
establish national verification committees (NVC) that would develop regular progress reports for
submission to the RVC (WPR/RC63.R5). The due date for the first submission from the 16
NVCs was 1 October 2013 for documenting progress towards measles elimination or requesting
verification of measles elimination.
The objectives of the third annual meeting were to review the first annual progress reports
of the NVCs to monitor progress towards and make recommendations for measles elimination, to
monitor progress towards control of rubella and congenital rubella syndrome, and to make a
determination for countries and areas for which their NVC has requested verification of measles
elimination.
First annual progress reports were submitted by 14 NVCs. The NVCs for Cambodia, the
Lao People's Democratic Republic and the Subregional Verification Committee for Pacific island
countries and areas did not submit progress reports in 2014. Among countries requesting
verification of measles elimination, Australia, Macao SAR (China), Mongolia and the
Republic of Korea were verified as having achieved measles virus elimination for a period of at
least 36 months since the last known endemic case.
RVC members made country- or area-specific recommendations to each of the NVCs, as
well as to WHO Regional Office for the Western Pacific and the Measles & Rubella Initiative
(M&RI).
The meeting concluded with an award ceremony held to acknowledge the achievement of
verification of measles elimination by the Republic of Korea, the host country for the meeting, at
which a congratulatory video message from Dr Shin Young-soo, WHO Regional Director for the
Western Pacific, was shown. A certificate from the RVC and an endorsement letter from
Dr Shin were also presented to the representative of the Republic of Korea.

LIST OF ACRONYMS
CPHL Central Public Health Laboratory
CRS congenital rubella syndrome
EPI Expanded Programme on Immunization
IgG Immunoglobulin G
IgM Immunoglobulin M
MCV measles-containing vaccine
MCV1 first dose of measles-containing vaccine
MCV2 second dose of measles-containing vaccine
MMR1 first dose of measles-mumps-rubella vaccine
MMR2 second dose of measles-mumps-rubella vaccine
M&RI Measles and Rubella Initiative
NIID National Institute of Infectious Diseases
NIP National Immunization Programme
NIR national immunization register
NVC national verification commission
PHLS Public Health Laboratory Services
RCV Rubella-containing vaccine
RVC Regional Verification Commission for the Western Pacific
SIA supplementary immunization activity
UNF United Nations Foundation
UNICEF United Nations Children's Fund
CDC United States Centers for Disease Control and Prevention
PAHO Pan American Health Organization
WHO World Health Organization

CONTENTS
Page SUMMARY �
LIST OF ACRONYMS�
1. INTRODUCTION.................................................................................................................... 1�
1.1� Objectives ..................................................................................................................... 1�
1.2� Organization ................................................................................................................. 1�
1.3� Opening session ............................................................................................................ 1�
2. PROCEEDINGS ...................................................................................................................... 2�
2.1� Background ................................................................................................................... 2�
2.2� Global and regional progress on measles elimination and rubella control ................... 2�
3. FINDINGS ............................................................................................................................... 2�
3.1� NVC reports .................................................................................................................. 2�
3.1.1��� Australia ................................................................................................................ 3�
3.1.2��� Brunei Darussalam ................................................................................................ 4�
3.1.3��� China ..................................................................................................................... 4�
3.1.4��� Hong Kong SAR (China) ...................................................................................... 5�
3.1.5��� Japan ...................................................................................................................... 6�
3.1.6��� Macao SAR (China) .............................................................................................. 7�
3.1.7��� Malaysia ................................................................................................................ 8�
3.1.8��� Mongolia ............................................................................................................... 8�
3.1.9��� New Zealand ......................................................................................................... 9�
3.1.10 Papua New Guinea .............................................................................................. 10�
3.1.11 Philippines ........................................................................................................... 11�
3.1.12 Republic of Korea ............................................................................................... 11�
3.1.13 Singapore............................................................................................................. 12�
3.1.14 Viet Nam ............................................................................................................. 13�
4. CONCLUSIONS AND RECOMMENDATIONS ................................................................. 14�
4.1� General recommendations to all NVCs ...................................................................... 14�
4.1.1��� Recommendations to the NVC of Australia ........................................................ 14�
4.1.2��� Recommendations to the NVC of Brunei Darussalam ........................................ 15�
4.1.3��� Recommendations to the NVC of China ............................................................. 16�
4.1.4��� Recommendations to the NVC of Hong Kong SAR (China) .............................. 16�
4.1.5��� Recommendations to the NVC of Japan ............................................................. 17�
4.1.6��� Recommendations to the NVC of Macao SAR (China) ...................................... 17�
4.1.7��� Recommendations to the NVC of Malaysia ........................................................ 18�
4.1.8��� Recommendations to the NVC of Mongolia ....................................................... 18�
4.1.9��� Recommendations to the NVC of New Zealand ................................................. 18�
4.1.10� Recommendations to the NVC of Papua New Guinea ........................................ 19�
4.1.11� Recommendations to the NVC of the Philippines............................................... 19�
4.1.12� Recommendations to the NVC of the Republic of Korea ................................... 20�
4.1.13� Recommendations to the NVC of Singapore ...................................................... 20�
4.1.14 Recommendations to the NVC of Viet Nam ....................................................... 20�
4.2� Recommendations to WHO and M&RI partners ........................................................ 21�
4.3� Partner comments ....................................................................................................... 21�
4.4� Closing session ........................................................................................................... 22�
4.5� Award ceremony for the Government of the Republic of Korea ................................ 22�

ANNEXES
ANNEX 1 - TIMETABLE
ANNEX 2 - LIST OF PARTICIPANTS
ANNEX 3 - RVC PRESENTATION
ANNEX 4 - AWARD CEREMONY PHOTO
Keywords:
1. Measles – prevention and control
2. Rubella – prevention and control
3. Vaccination

1. INTRODUCTION
The Third Annual Meeting of the Regional Verification Commission (RVC) for Measles
Elimination in the Western Pacific was held in Seoul, Republic of Korea, from
18 to 21 March 2014.
1.1 Objectives
The objectives of the meeting were:
(1) to review the first annual progress reports of the National Verification
Commission (NVC) to monitor progress towards and make recommendations for
measles elimination;
(2) to monitor progress towards control of rubella and congenital rubella
syndrome; and
(3) to make a determination for countries and areas for which their NVC has
requested verification of measles elimination.
1.2 Organization
The participants of the meeting included the 14 members of the RVC and six WHO staff
members from the WHO Regional Office for the Western Pacific. In addition, representatives
and partners from the Measles and Rubella Initiative (M&RI) including the American Red Cross,
United Nations Foundation (UNF), United Nations Children's Fund (UNICEF) East Asia and
Pacific Regional Office, and the United States Centers for Disease Control and Prevention (US
CDC) attended the meeting. The agenda and timetable for the meeting are provided in Annex 1
and the list of participants in Annex 2.
1.3 Opening session
The meeting was called to order by Dr Sergey Diorditsa, the Responsible Officer for the
meeting. Dr Mark Jacobs, Director of the Division of Combating Communicable Diseases
delivered the opening remarks on behalf of Dr Shin Young-soo, WHO Regional Director for the
Western Pacific. Dr Shin noted that this meeting had historical significance because it was the
first opportunity for countries and areas to be verified as having achieved measles elimination.
He reviewed the resolutions of Regional Committee meetings that had established the
mechanisms to form national verification committees, which would then submit annual progress
reports to the Regional Verification Commission. He acknowledged the efforts made by
Member States to achieve measles elimination and thanked the members of the RVC for their
dedication and service to the Commission.
After participants introduced themselves, Dr Jacobs nominated the office bearers as
follows:
(1) Chair: Professor David Durrheim
(2) Vice Chair: Dr Hiroshi Yoshikura
(3) Rapporteur: Dr Rose Capeding

- 2 -
2. PROCEEDINGS
2.1 Background
Professor David Durrheim, Acting Chair of the RVC reviewed the meeting objectives and
the expected outcomes of the meeting.
(1) Meeting objectives:
• to review the first annual progress reports of the NVCs to monitor progress
towards and make recommendations for measles elimination;
• to monitor progress towards control of rubella and congenital rubella syndrome;
and
• to make a determination for countries and areas for which their NVC has
requested verification of measles elimination.
(2) Expected outcomes:
• a determination about whether the countries and areas requesting verification
were successful in providing adequate documentation showing that endemic
measles virus transmission was interrupted for a period of at least 36 months since
the time of the last known endemic case, in the presence of verification standard
surveillance and genotyping evidence that supports the interruption of endemic
measles virus transmission;
• review of the first annual progress reports submitted by NVCs to monitor progress
towards measles elimination and control of rubella and congenital rubella
syndrome;
• recommendations to national verification committees about specific strategies that
should be considered to achieve or sustain measles elimination.
2.2 Global and regional progress on measles elimination and rubella control
An update on global and regional progress towards measles elimination and rubella control
was presented by Dr William Schluter. The presentation outlined global and regional targets and
then briefly summarized the progress towards these targets against the five lines of evidence that
are used for regional verification. A copy of the presentation is attached in Annex 3.
3. FINDINGS
3.1 NVC reports
Following these introductory comments, the progress towards or achievement of
elimination was reviewed country by country. For the 2014 RVC meeting, 14 countries and
areas submitted documentation for verification or progress towards measles elimination. The
- 3 -
NVCs for Cambodia, and the Lao People's Democratic Republic as well as the Subregional
Verification Committee for Pacific island countries and areas did not submit progress reports in
2014.
3.1.1 Australia
Epidemiology
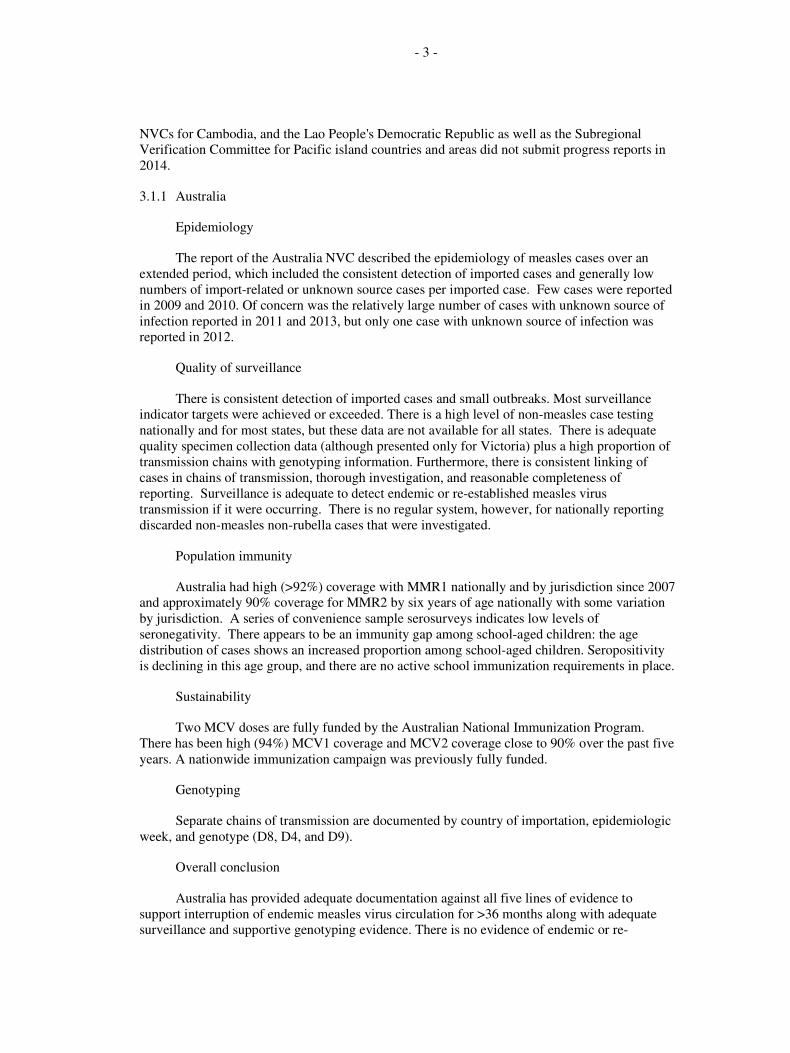
The report of the Australia NVC described the epidemiology of measles cases over an
extended period, which included the consistent detection of imported cases and generally low
numbers of import-related or unknown source cases per imported case. Few cases were reported
in 2009 and 2010. Of concern was the relatively large number of cases with unknown source of
infection reported in 2011 and 2013, but only one case with unknown source of infection was
reported in 2012.
Quality of surveillance
There is consistent detection of imported cases and small outbreaks. Most surveillance
indicator targets were achieved or exceeded. There is a high level of non-measles case testing
nationally and for most states, but these data are not available for all states. There is adequate
quality specimen collection data (although presented only for Victoria) plus a high proportion of
transmission chains with genotyping information. Furthermore, there is consistent linking of
cases in chains of transmission, thorough investigation, and reasonable completeness of
reporting. Surveillance is adequate to detect endemic or re-established measles virus
transmission if it were occurring. There is no regular system, however, for nationally reporting
discarded non-measles non-rubella cases that were investigated.
Population immunity
Australia had high (>92%) coverage with MMR1 nationally and by jurisdiction since 2007
and approximately 90% coverage for MMR2 by six years of age nationally with some variation
by jurisdiction. A series of convenience sample serosurveys indicates low levels of
seronegativity. There appears to be an immunity gap among school-aged children: the age
distribution of cases shows an increased proportion among school-aged children. Seropositivity
is declining in this age group, and there are no active school immunization requirements in place.
Sustainability
Two MCV doses are fully funded by the Australian National Immunization Program.
There has been high (94%) MCV1 coverage and MCV2 coverage close to 90% over the past five
years. A nationwide immunization campaign was previously fully funded.
Genotyping
Separate chains of transmission are documented by country of importation, epidemiologic
week, and genotype (D8, D4, and D9).
Overall conclusion
Australia has provided adequate documentation against all five lines of evidence to
support interruption of endemic measles virus circulation for >36 months along with adequate
surveillance and supportive genotyping evidence. There is no evidence of endemic or re-

- 4 -
established measles virus circulation. However, there is a concerning immunity gap which should
be addressed and updates provided in subsequent reports.
3.1.2 Brunei Darussalam
Epidemiology
Zero to four cases of measles have been reported annually from 2008 to 2013. The highest
number of cases (four) occurred in 2011 and three of the four cases reported that year were
classified as imported cases.
Quality of surveillance
From 2008 to 2013, Brunei Darussalam had a national discarded case rate of 1.4 to 2.6 per
100 000 population. The proportion of cases with adequate investigation has been >80% since
2007 and the proportion with adequate specimen collection has been >80% since 2010. All
laboratory results have been available within seven days since 2011.
Population immunity
From 2009 to 2012, administrative coverage with two doses of MMR has been >90%. A
2011 serosurvey conducted among children in primary 4 reported 79% positivity for measles-
specific IgG antibodies.
Sustainability
Two doses of MMR are provided at no cost to all children who are citizens or permanent
residents of Brunei Darussalam. Brunei Darussalam has both measles and rubella/CRS
elimination goals.
Genotyping
No genotyping data is available, but Brunei Darussalam has a plan to request genotyping
support from the Regional Reference Laboratory.
Overall conclusion
Brunei Darussalam has likely already achieved measles elimination, but additional
information is needed including detailed geographic distribution of cases, summary table of cases
classified by source of infection, genotyping evidence, and a measles preparedness plan for
outbreak response.
3.1.3 China
Epidemiology
Measles incidence has decreased significantly since implementation of the measles
elimination strategy in China, resulting in a historic low incidence rate in 2012. However, a
resurgence of measles cases occurred in 2013 related to the considerable size of birth cohorts.

- 5 -
Quality of surveillance
Most surveillance performance indicators are met with the exception of the sensitivity
indicator and certain aspects of laboratory surveillance (such as proportion of outbreaks with
viral specimen collected). The national measles laboratory and all provincial labs have passed
WHO accreditation annually. In addition, 98% of all measles suspected cases were tested for
measles-specific IgM by ELISA in 2012.
Population immunity
Administrative coverage for MCV1 and MCV2 were >95% from 2006–2012. A national
immunization coverage survey conducted in 2011 showed 99.5% coverage for MCV1 and 93.4%
for MCV2. No serosurveillance data were available.
Sustainability of NIP
There is a high level of commitment from the Government of China to provide financial,
technical, policy-related support for measles elimination in China. The national leading group
for measles elimination is chaired by a high-level political leader. In addition, an independent
NVC has been established.
Genotyping
The national measles laboratory is responsible for genotyping and analysing molecular
epidemiological data.
Overall conclusion
There is marked heterogeneity among the provinces with regard to measles incidence and
progress towards elimination. While some provinces may be close to elimination, others have
ongoing transmission. There are improved surveillance performance indicators and a stated
commitment by the Government to achieve measles elimination.
3.1.4 Hong Kong SAR (China)
Epidemiology
The incidence rate has been low and almost all cases (n=124 during the period from 2008–
2012) were sporadic with only six brief outbreaks with two cases each.
Quality of surveillance
Indicator targets for discarded non-measles reporting rate at the national level were
achieved in 2011 and 2012. Adequate investigations were conducted for 98% and 92% of
suspected cases in those years, respectively. Public Health Laboratory Services (PHLS) serves as
a WHO-accredited Regional Reference Laboratory.
Population immunity
High vaccination coverage was achieved with two doses of MCV. The second dose is
delivered at school. There has been >98% administrative coverage for MCV 1 and MCV 2 since
2006. Annual convenience seroprevalence studies show >95% immunity in all age groups
except adolescents 15–19 years of age in 2008.

- 6 -
Sustainability
The Government of Hong Kong SAR (China) is committed to measles elimination. An
NVC has been established.
Genotyping
Measles virus with genotype H1 are likely to be detected until China achieves elimination.
It is difficult to interpret whether the H1 strains detected in Hong Kong are endemic or imported,
but it is important to carefully identify their source and characterize chains of transmission.
Overall conclusion
Due to high coverage and sensitive surveillance, Hong Kong SAR (China) may have
already achieved elimination and should consider submitting documentation for verification after
the NVC makes their determination that elimination has been achieved.
3.1.5 Japan
Epidemiology
From 2009 through the first half of 2013, <1000 confirmed cases were reported annually
(range 228 in 2012 to 741 in 2009). Cases have not been classified with regard to source of
infection.
Quality of surveillance
There is no mechanism to identify discarded non-measles cases that were investigated. A
large proportion of the cases are clinically diagnosed. The measles and rubella laboratory at
NIID is WHO-accredited and serves as a Global Specialized Laboratory.
Population immunity
High vaccination coverage was achieved with two doses of MCV in 2012. Administrative
coverage estimates for earlier years were not presented. Japan conducted a successful mass
vaccination campaign targeting two school-age cohorts in each of five years between 2008 and
2012 to address a well-characterized immunity gap.
Sustainability
An infectious diseases control law (including measles) has been in place since 2008.
Funding for measles elimination efforts are provided through Japan's national and local
governments.
Genotyping
Numerous genotypes including B3, D4, D5, D8, D9, G3 and H1 have been detected since
2008.
Overall conclusion
Japan has nearly achieved or already achieved measles elimination. Measles cases with
genotype D5 (the formerly endemic strain) have not been detected since May 2010. However to

- 7 -
be sure that measles virus has not been re-established following multiple importations, more
detailed information is needed that categorizes source of cases, and describes the detailed
epidemiology of clinically diagnosed cases and laboratory-confirmed cases that have not been
genotyped. There is a need to confirm or discard clinically diagnosed cases by laboratory
investigation.
3.1.6 Macao SAR (China)
Epidemiology
There were only six outbreaks and a total of eight cases in Macao SAR (China) between
2006 and 2012. Of these, six were imported cases and two were import-related cases. Four
cases were <1 year of age, and five cases between 8 months and 14 years of age were all
unvaccinated. All cases from 2006–2013 were residents in Macao, had laboratory confirmation,
and a known source of infection. There were no clinically compatible cases.
Quality of surveillance
All surveillance performance indicators exceeded WHO standards: non-measles non-
rubella discarded rate was >2/100 000 between 2006 and 2013. All cases were laboratory
confirmed. All cases had adequate investigations, including adequate specimen collection, and
timely processing and availability of results.
Population immunity
Macao SAR (China) has had a two-dose schedule with MMR since 1990 and a three-dose
schedule (9M, 15M, 4–6 yrs) from 1994 to 2003. The current schedule, implemented since 2013,
has two doses of MMR at 12 and 18 months. Nursery and school entry checks, including
immigrant children, are performed and updated annually. Between 2007 and 2012,
administrative coverage for MCV1 was estimated at 95–98% and MCV2 at 93–96%.
Immunizations provided in the private sector are included in the government health information
system. Seroprevalence testing was conducted since 2003 and demonstrated <5% seronegativity
among children ≥2 years.
Sustainability
There is adequate funding allocated for sustaining the national immunization programme
as well as measures to improve the knowledge of health care workers. Regulation of nursery and
school entry checking, which includes migrant children, has been implemented since 2008. Risk
assessments are conducted regularly showing continued risk due to migration and population
movement of people between Macao SAR (China) and neighbouring countries. In addition,
outbreak response plans are in place, which are regularly reviewed.
Genotyping
There were no endemic cases during the period covered by the report. All cases were
either imported or import-related as supported by genotyping evidence.
Overall conclusion
Macao SAR (China) has provided documentation that supports interruption of endemic
measles virus transmission for >36 months in the presence of sensitive surveillance and
supportive genotyping data.

- 8 -
3.1.7 Malaysia
Epidemiology
There was decreased transmission of measles from 2008 to 2010, however, large outbreaks
occurred in 2011 and 2012.
Quality of surveillance
Annually, the rate of discarded non-measles cases was >2/100 000 from 2009 to 2013.
The proportion of suspected cases with adequate investigation was >80% in 2009 and
2011–2013. Adequate specimen collection was completed for >80% of cases in each of the last
five years except 2011.
Population immunity
Malaysia introduced MCV2 in 2002. Reported coverage with MCV1 has been >95%
since 2009 and for MCV2, >95% since 2008. No serosurveys have been conducted. SIA
coverage was missing from the report.
Sustainability
Funding for the national immunization programme is secure. An initial risk assessment
has been completed.
Genotyping
D8 and D9 genotypes continue to circulate.
Overall conclusion
Malaysia has endemic transmission of measles virus. Major difficulties include mobile
populations at the borders of Sabah and Sarawak. Vaccine refusal is not common, but vaccine
refusers are influential.
3.1.8 Mongolia
Epidemiology
Mongolia experienced measles epidemics every three to four years until 1988, but reported
only 82 measles cases between 2006 and 2012; 71 were laboratory confirmed and 11 were
clinically confirmed. Detailed information is provided on each outbreak that ranged from two to
nine cases. No measles cases have been confirmed since 2011.
Quality of surveillance
The national discarded non-measles rate is >2/100 000, but subnationally <80% of districts
are meeting this level of sensitivity. The proportion of cases with adequate investigation has
gradually improved from 22% in 2008 to 64% in 2012. Adequate specimen collection has been
>80% since 2008.

- 9 -
Population immunity
Mongolia started a single dose of MCV in 1973 and added MCV2 in 1989. The current
schedule that includes two doses of MMR at nine months and two years of age was adopted in
2009. Administrative coverage with both doses has been >95% every year since 2006.
Sustainability
Immunization services are regulated by law and provided at all levels of the health system.
Genotyping
H1 was detected in 2001, 2008 and 2009. D6 was detected in 2006.
Overall conclusion
Mongolia has documented the interruption of endemic measles virus transmission for a
period of at least 36 months in the presence of sensitive surveillance and supportive genotyping
evidence.
3.1.9 New Zealand
Epidemiology
Since 1997, two significant outbreaks have occurred, in 2009 and 2011. The latter
persisted with ongoing measles virus transmission for a period of 13 months.
Quality of surveillance
Nationally, the rate of discarded non-measles cases has been >2/100 000 from 2011 to
2013. At subnational level, the target was achieved by >90% of second-level administrative
units in 2011 and 2012, but only 56% in 2013. Laboratory support is provided by 5 ISO15189
standard laboratories. The national measles and rubella laboratory is WHO-accredited.
Population immunity
New Zealand provides two doses of MMR at 12–15 months and at 4 years of age. Greater
than 92% coverage for MCV1 was achieved for all birth cohorts since 2006. Coverage for
MCV2 is estimated at 89% for birth cohorts born in 2006 and 2007 at four years of age.
Insufficient population immunity is documented particularly among Maori and
socioeconomically deprived groups.
Sustainability
Two doses of MMR are available at no cost to any New Zealand resident born since 1969.
The national immunization register (NIR) assists with tracing children who are not fully
vaccinated.
Genotyping
Genotypes B3, D4, D8 and D9 have been detected in recent years.

- 10 -
Overall conclusion
New Zealand has likely achieved elimination of re-established transmission since June
2012.
3.1.10 Papua New Guinea
Epidemiology
A large measles outbreak occurred in 2002 and 2003. However, from 2005 no measles
cases were detected until October 2013 when four cases were laboratory confirmed, originating
from Vanimo Green, West Sepik, which is a community close to the Indonesia border.
Quality of surveillance
Case-based surveillance was started in 2008. While epidemiological surveillance
indicators have not reached the required target, it appears that surveillance sensitivity was
sufficient to detect rubella cases as well as dengue and chikungunya outbreaks in 2011/2012 and
the measles outbreak in 2013. The laboratory obtained WHO accreditation in 2011/2012 and has
sufficient capacity to conduct laboratory diagnosis if specimens are received.
Population immunity
Administrative coverage shows an increase of national MCV at 9 months from 54% in
2008 to 67% in 2012, while surveys showed improvement from 78% in 2004 to 86% in 2007–
2009. Biannual SIA from 2008 also showed increasing coverage from 86% in 2008/2009 to 88%
in 2012. The introduction of a second dose of MCV with rubella was discussed in the report and
planned for 2015.
Sustainability
The government funds 81% of the costs for routine immunization vaccines and is
committed to sustaining routine immunization and strengthening primary health care to improve
service delivery. A national expanded programme on immunization (EPI) review was conducted
in 2013. Districts with low vaccine coverage were identified.
Genotyping
Historical information about endemic strains prior to 2005 is not available. Recent
outbreaks in 2013 and 2014 involved D9 and B3 genotypes.
Overall conclusion
Given the extremely challenging environment in Papua New Guinea, the NVC has
identified areas in need of strengthening. It is encouraging that the NVC has made
recommendations and action plans for 2013–2014 and is holding meetings twice yearly to
monitor the progress of action plans. However, low measles incidence despite low vaccine
coverage may possibly reflect underreporting of measles cases. With the government
commitment to a sustainable immunization programme and strengthening of primary health care
services, vaccine coverage and case detection should improve further.

- 11 -
3.1.11 Philippines
Epidemiology
Large measles outbreaks occurred in 1997, 2003, 2010–2011, and 2013–2014 prior to
scheduled supplementary immunization campaigns in 2004, 2011, and 2014. More than 3000
cases were reported in both 2010 and 2011.
Quality of surveillance
National reporting of non-measles discarded cases has ranged from 2.1 to 4.3/100 000
population. The proportion of suspected cases with adequate investigation ranged from 14.5% to
88.6%.
Population immunity
Single antigen measles vaccine is provided as MCV1 at nine months of age with
administrative coverage estimated at 79% to 88% from 2008 to 2012. MMR is used for MCV2
and was introduced in 2010 with coverage estimated at 10% to 38% per year from 2010–2012.
Nationwide SIAs were conducted in 1998, 2004, 2007 and 2011.
Sustainability
The Philippines plans to strengthen routine immunization coverage through the "Reaching
Every Purok" strategy and by conducting a follow up MR SIA in September 2014.
Genotyping
Genotyping has shown different endemic dominant strains in different years: G3 in 2008–
2010; D9 in 2009–2012; and B3 in 2013–2014.
Overall conclusion
The Philippines has endemic measles virus transmission and in 2013 had the highest
incidence of any country or area in the Region. Epidemiological and laboratory surveillance
have improved in recent years. Suboptimal immunization coverage is a major challenge to
measles elimination.
3.1.12 Republic of Korea
Epidemiology
The Republic of Korea declared elimination of measles in 2006 but then experienced small
outbreaks in 2007, 2010, 2011 and 2013. The annual number of cases between 2008 and 2013
varied from 2 to 118 (average = 49). There is no evidence of re-establishment of endemic
transmission lasting 12 months. In 2011–2013, nine unknown source cases, nine imported cases
and 145 import-related cases occurred. All 163 cases were laboratory confirmed.
Quality of surveillance
The discarded non-measles reporting indicator rates at national and provincial level have
not been reached (0.8/100 000 was the highest in 2013). The Republic of Korea has
implemented an active surveillance program in the five large laboratory services (with

- 12 -
3500–4000 measles tests per annum, immunity screening excluded and conducting 97% of all
tests in the country). This has provided a steady rate >7/100 000 since 2009 and between 75%
and 88% of prefectures meet the target using this system.
There has been adequate investigation of 73%, 84% and 89% of suspected cases in 2011,
2012 and 2013, respectively. All outbreaks had serological confirmation and virology specimens
submitted. The quality of laboratory surveillance discussed in the report was based on the data
from the 17 public laboratories.
Population immunity
Nationwide telephone coverage surveys (by card check) found MMR1 coverage >95% and
>99% in 2011 and 2012. A nationwide survey of MMR2 coverage in 2012 by card found >97%
coverage.
Sustainability
There is a long-term commitment to measles elimination. An NVC has been established.
There is a legal basis for immunization (Infectious Diseases Prevention Act and School Health
Law). A previous large-scale mass campaign was funded by the Government and two doses of
measles-containing vaccine are provided free of charge to any child in the Republic of Korea.
Genotyping
H1 was the endemic genotype historically in the Republic of Korea. There have been no
H1 isolations since July 2010. Epidemiologically distinct D9 and B3 importations have resulted
in sporadic cases and outbreaks since 2011.
Overall conclusions
At the time of their report, the Republic of Korea meets the elimination criteria:
documentation of the interruption of endemic measles virus transmission for a period of at least
36 months from the last known endemic case; in the presence of verification standard
surveillance and genotyping evidence that supports the interruption of endemic transmission.
3.1.13 Singapore
Epidemiology
The most recent resurgence began in 2010 with 49 reported cases (compared to 13 in
2009) and 148 reported cases in 2011. This was largely attributed to single sporadic cases in
infants and young children less than five years of age. Most were unvaccinated. The timing of
both doses was changed so that MMR is given at 12 months and at 15–18 months of age. In
2012, 38 cases were confirmed by laboratory.
Quality of surveillance
Achievement against standard indicators is not included in the report. The National
Measles Laboratory is WHO-accredited.

- 13 -
Population immunity
MCV1 coverage by birth cohort has been >95% since 2008. The National Immunization
Registry is used to follow up children that are not fully vaccinated. Immunization status is
checked at school entry. Seroprevalence of measles-specific antibodies among persons aged
18–74 years of age increased from 89.1% in 1998 to 96.7% in 2005.
Sustainability
Resources appear available to sustain routine and supplemental immunization.
Genotyping
Numerous genotypes have been identified including B3, D4, D8, D9, G3 and H1. More
detailed data on lineages are required to confirm interruption of transmission.
Overall conclusion
Singapore may have already achieved elimination and may consider submitting
verification documentation after the NVC has independently determined that the elimination
criteria have been met.
3.1.14 Viet Nam
Epidemiology
Measles outbreaks occurred in 2006, 2008–2009, 2010, 2011, and 2013.
Quality of surveillance
Case-based surveillance started in 2002. Performance on meeting standard indicators
decreased in 2012 relative to previous years.
Population immunity
MCV1 coverage was reported as >95% from 2008 to 2012; while MCV2 was reported as
>95% from 2005 to 2010, but 90% in 2011 and only 83% in 2012. SIA coverage in 2010 was
reported as >95%. School entry immunization checks are in place.
Sustainability
An NVC has been established. The EPI programme is a high priority and vaccines are
provided at no cost for all children.
Genotyping
The genotype previously identified in Viet Nam is H1, but in 2014, D8 strain was also
identified in the southern part of the country.
Overall conclusion
Viet Nam may have interrupted transmission of measles following the 2010 campaign, but
has experienced multiple importations with current ongoing transmission.

- 14 -
4. CONCLUSIONS AND RECOMMENDATIONS
4.1 General recommendations to all NVCs
The RVC wishes to acknowledge the excellent reports received from the NVCs and to
thank the NVCs and their secretariats for their work in preparing such high-quality, thorough
reports.
Although some countries indicated that they had developed the following documentation,
the RVC urges that copies of these documents be submitted with future reports:
(1) NVC plan;
(2) Measles risk assessment; and
(3) Measles outbreak response plan.
A standardized tool for measles risk assessment is currently being developed at the global
level. The draft risk assessment tool will be shared with countries and areas once available. For
countries and areas that have not yet completed a measles risk assessment, the draft global tool
should be considered for adaptation and use.
During the 2013 Technical Advisory Group (TAG) meeting a recommendation was made
to establish a rubella elimination goal with the date for elimination to be determined. As the
Region continues with efforts to control rubella and congenital rubella syndrome (CRS) and
moves toward rubella elimination, the RVC encourages NVCs to include in future reports more
detail on progress towards rubella and CRS control and elimination. This information may
follow the same general format as that proposed for measles, namely:
(1) A detailed description of the epidemiology of rubella since the introduction of
rubella vaccine in the national immunization programme;
(2) Quality of epidemiological and laboratory surveillance systems for rubella;
(3) Population immunity presented as a birth cohort analysis with the addition of
evidence related to any underserved or marginalized populations;
(4) Sustainability of the rubella/CRS control efforts; and
(5) Genotyping data.
4.1.1 Recommendations to the NVC of Australia
• Please provide analysis of population immunity by birth year based on historical
immunization coverage and serosurveys in future reports.
• Consider establishing a system of regularly reporting discarded non-measles cases
to national level from all states.
- 15 -
To avoid re-establishment of endemic measles transmission:
• A targeted strategy to address the immunity gaps demonstrated by multiple data
sources among school-aged children (particularly in New South Wales) appears
essential to maintain adequate population based immunity:
– Encourage collaboration between education and health sectors to identify
schools at high risk;
– Consider referral of school-aged children who present as unvaccinated during
school entry immunization checks; and
– Consider SIAs in schools in high-risk areas or with a larger proportion of high-
risk children.
• In lower-performing states for MCV2 coverage (such as Western Australia and
Northern Territory), document the improvement in vaccination coverage predicted
by scheduling MCV2 from 4 years to 18 months and providing income-tested
payments to families.
• Characterize vulnerable community groups more fully (e.g. ethnicity) with lower
MCV coverage so that they can be more effectively targeted by social
mobilization and culturally-appropriate immunization strategies.
• Assure mechanisms to prevent nosocomial transmission of measles given
increasing cases among infants <1 year of age.
4.1.2 Recommendations to the NVC of Brunei Darussalam
• Brunei Darussalam may have already achieved measles elimination. When the
NVC has independently concluded that measles elimination has been achieved,
the RVC would welcome a report which outlines its achievement against the five
lines of evidence described in the Guidelines for Verification of Measles
Elimination in the Western Pacific Region. Please note that measles incidence
was an interim indicator and is not a necessary indicator for elimination,
particularly in relatively small populations. It is essential that all cases be
classified by source of infection (imported, import-related, endemic, or unknown).
• The RVC encourages Brunei Darussalam to continue with efforts to strengthen the
quality of laboratory and virological surveillance for measles and rubella
including:
– seeking WHO accreditation of the national measles and rubella laboratory;
– finalizing arrangements to obtain genotyping data through the Regional Reference
Laboratory; and
– clarifying appropriate testing to screen for rubella immunity among women during
antenatal care visits.
• Vaccination coverage should be monitored and risk assessments conducted to
ensure no pockets of susceptible populations exist for re-establishing measles

- 16 -
transmission. This is especially important to consider in communities of foreign
workers and their families.
• Consider mechanisms to ensure awareness among clinicians and public health
staff of the clinical presentation of measles and appropriate case confirmation,
reporting and response.
4.1.3 Recommendations to the NVC of China
• Maintain high vaccination coverage for each birth cohort.
• Given that infants have the largest immunity gap, detailed analysis of infant
susceptibility would be informative. Consider including in future reports an
analysis of population immunity by birth year (and by month among those <2
years) based on historical immunization coverage and serosurveys.
• Given that most recent cases were <1 year of age and before the timing of the first
recommended dose, consider an earlier supplemental MCV dose for infants in
areas of high transmission.
• The RVC supports the recommendations of the National and International
Consultation, including assuring strategies to prevent nosocomial transmission
amongst infants <1 year of age.
• A follow-up consultation may be considered as a mechanism to monitor progress
towards implementation of the consultation recommendations and to evaluate their
effectiveness to interrupt endemic measles virus transmission.
• Additional information on outbreak response plans, including outbreak
investigation, classification of chains of transmission, and outbreak response
immunization activities, should be provided.
• Vulnerable community groups (e.g. migrant and inner city populations) should be
carefully characterized to permit more effective implementation of social
mobilization and immunization strategies.
• Noting the heterogeneity among the provinces (in surveillance quality, routine and
supplemental coverage, and progress towards elimination) the RVC encourages
the NVC to receive detailed provincial verification reports against the five lines of
evidence. Lessons learnt from high-performing provinces could be shared with
other provinces. This may require establishment of strong provincial verification
committees.
• The submission of brief province-specific summaries would be informative to the
RVC.
4.1.4 Recommendations to the NVC of Hong Kong SAR (China)
• Hong Kong SAR may have already achieved measles elimination. When the NVC
has independently concluded that measles elimination has been achieved, the RVC
would welcome a report which outlines its achievement against the five lines of

- 17 -
evidence in the Guidelines for Verification of Measles Elimination in the Western
Pacific Region. Please note that measles incidence was an interim indicator and is
not a necessary indicator for elimination, particularly in relatively small
populations. It is essential that all cases be classified by source of infection
(imported, import-related, endemic, or unknown).
• Detailed epidemiological analysis of all cases is required to confirm there is no
ongoing transmission and this should be provided in future reports.
• High vaccination coverage should be sustained and the NVC action plan fully
implemented (in particular to fully investigate all suspected measles cases, with
laboratory confirmation and specimens collected for genotyping for >80% of all
chains of transmission).
• The National Measles Outbreak Response Plan should be submitted.
4.1.5 Recommendations to the NVC of Japan
• The sensitivity of surveillance should be maintained by encouraging the reporting
of cases with clinical features consistent with measles.
• However, at least 80% of reported suspected cases should be adequately
investigated with collection of core variables and appropriate laboratory testing,
preferably serum (or oral fluid) specimen for measles-specific IgM testing, and
reported to the national level.
• Clinically-diagnosed measles cases that are fully investigated and not laboratory or
epi-linked confirmed should be reported as discarded cases.
• Investigations should include a mechanism to identify chains of transmission of
measles virus by place and time.
• >80% of measles chains of transmission should be genotyped with all sequences
reported to the global database, WPRO, and the national programme of Japan
through the NIID.
• All confirmed cases should be classified as to source of infection (imported,
import-related, endemic, or unknown).
• Vaccination coverage monitoring and risk assessment at the prefecture and
municipality level would ensure no pockets of susceptible population exist for re-
establishing measles transmission.
4.1.6 Recommendations to the NVC of Macao SAR (China)
• Maintain homogenous and high vaccination coverage across the entire population.
• Maintain high levels of surveillance sensitivity and quality.
• Given that most cases were <1 year of age and before the timing of the first
recommended dose, consider advising an earlier supplemental MCV dose to
infants travelling to endemic areas.
- 18 -
4.1.7 Recommendations to the NVC of Malaysia
• In settings with endemic transmission of measles virus, the RVC supports the 2012
TAG recommendation that the second dose of measles vaccine should preferably
be administered in the second year of life.
• School entry requirements for evidence of two doses of measles vaccination would
provide an opportunity for checking that all children at school entry were fully
vaccinated.
• A detailed risk assessment that includes unofficial migrants and districts with low
routine immunization coverage, with implementation of mitigation strategies, is
recommended.
• The RVC notes the gains achieved through focal SIAs. Consideration should be
given to conducting a national/larger-scale wide age range SIA to address
immunity gaps.
4.1.8 Recommendations to the NVC of Mongolia
• Maintain the high level of government awareness, commitment and financial
support to the national measles elimination initiative through: (i) developing a
measles elimination maintenance plan; and (ii) documenting ongoing achievement
of elimination.
• Clarify the methods for determining the numerator and denominator (i.e. target
population) for calculating immunization coverage in the next NVC report.
• Monitor and review reported vaccination coverage and conduct risk assessment at
subnational level to ensure no pockets of susceptible population exist for re-
establishing measles transmission.
• Pursue plans with the Ministry of Education to establish a national system for
checking vaccination history at the time of school entry.
• Ensure the sensitivity of surveillance, including case investigation at subnational
level.
• Actively conduct genotyping of all confirmed cases (to confirm genotype of >80%
of chains of transmission).
4.1.9 Recommendations to the NVC of New Zealand
• New Zealand has clearly demonstrated immunity gaps among adolescents and
young adults. The RVC looks forward to learning how these immunity gaps will
be addressed as they pose an ongoing risk of re-established transmission.
• Plans to address immunity gaps should particularly focus on defined risk groups
including low-coverage districts and Pacific peoples who have experienced a
higher disease burden during recent outbreaks.
- 19 -
• There is a need to reconcile current classification criteria of source of infection with
the WHO recommended classification and provide data accordingly.
• The NVC plan should be provided.
4.1.10 Recommendations to the NVC of Papua New Guinea
• Continue implementing the Reaching Every Child strategy to achieve and record
high routine immunization coverage at local levels as recommended by the
International EPI Review.
• The RVC encourages measles elimination activities to be used as an opportunity to
strengthen routine primary health care services including routine immunization.
• The RVC notes and supports the NVC recommendations of conducting risk
assessments and establishing an outbreak response preparedness plan.
• Consider mechanisms to ensure awareness among clinicians and public health staff
of the clinical presentation of measles and appropriate case confirmation,
reporting and response.
• Maintain and further improve the laboratory performance of the national measles
laboratory (Central Public Health Laboratory). Genotyping could be performed in
collaboration with WHO Regional Reference Laboratories.
• Strengthen accountability at each level for improving routine vaccination coverage
throughout the country.
4.1.11 Recommendations to the NVC of the Philippines
• To progress towards elimination, it is essential that >95% coverage be achieved in
all communities during the planned 2014 MR SIA.
• The RVC notes with concern the low coverage for MCV2 and encourages the
Philippines to continue with the Reaching Every Purok strategy to achieve and
record high routine immunization coverage with two doses of MCV at local level.
• Accountability should be strengthened at each level for improving routine
vaccination coverage throughout the country.
• Further improvements of epidemiologic surveillance are recommended, including
active case investigation.
• Genotyping should be actively pursued for more of the confirmed cases.

- 20 -
4.1.12 Recommendations to the NVC of the Republic of Korea
• Monitor vaccination coverage and conduct risk assessment at the third
administrative level to ensure no pockets of susceptible population exist for re-
establishing measles transmission.
• Prepare and submit the NVC's annual plan of action and a national plan on
preparedness and response to measles outbreaks in the next annual NVC report to
RVC.
• More actively conduct genotyping (to confirm genotype of >80% of chains of
transmission).
• Consider conducting an investigation to determine the apparent higher-than-
expected vaccination failure rate in the Incheon outbreak.
• Continue to conduct thorough outbreak investigations and provide descriptions of
all outbreaks in subsequent annual reports.
• Actively conduct case investigations to identify the sources of infection.
4.1.13 Recommendations to the NVC of Singapore
• Ensure harmonization of data in the NVC report and that submitted to WHO,
especially genotyping data, by including laboratory data from all laboratories
conducting measles and rubella testing.
• More detailed genotype lineage data are needed to differentiate between re-
established transmission and multiple imported strains.
• Genotype as many cases as possible.
• Conduct and provide detailed epidemiological analysis including chains of
transmission, source of infection (imported, import-related, endemic or unknown)
and residence status (resident or visitor).
• The RVC encourages submission of detailed outbreak investigation reports.
• Conduct and provide birth-cohort analysis by year to reflect population immunity.
• Prepare and submit the NVC's annual plan in future reports to the RVC.
4.1.14 Recommendations to the NVC of Viet Nam
• Consider mechanisms to ensure awareness among clinicians and public health staff
of the clinical presentation of measles and appropriate case confirmation,
reporting and response.
• Recognizing the challenges of reaching children in mountainous and remote areas,
special efforts should be made to ensure high routine immunization coverage
among these hard-to-reach populations.

- 21 -
• The RVC noted with concern the recent declines in routine immunization coverage
and recommends a detailed evaluation of root causes followed by implementation
of necessary activities.
• Continue to progress the recent strengthening of the surveillance system by fully
investigating suspected measles and rubella cases with collection of appropriate
laboratory specimens including genotyping.
• The RVC draws the attention of the NVC to the recent Strategic Advisory Group of
Experts on Immunization (SAGE) recommendation that following wide age range
catch-up campaigns, countries introducing rubella-containing vaccines (RCV) for
the first time should provide MR or MMR in routine immunization as the first
dose of MCV.
4.2 Recommendations to WHO and M&RI partners
• The RVC encourages WHO and M&RI partners to facilitate international cross-
border and cross-regional collaboration to enhance surveillance, improve routine
and supplemental immunization, and strengthen outbreak response and
information sharing.
• Technical and financial support should be prioritized by WHO and M&RI partners
to the endemic and outbreak-affected countries in the Region.
• Provide guidance to NVCs for submitting to the next RVC meeting risk
assessments and outbreak response plans including for countries and areas
previously verified.
• Provide support to NVCs to standardize the report content, especially for
epidemiological and virological surveillance data including genotyping. Best
practices from previous reports should be considered for dissemination with
country-specific permission.
• Provide support for countries and areas that have not yet submitted reports
(Cambodia, Lao People's Democratic Republic, and the Pacific Islands).
4.3 Partner comments
Partner comments were presented by Andrea Gay on behalf of all five partners of the
Measles & Rubella Initiative:
The M&RI started in 2001 as "the Measles Initiative" with five partner organizations: the
American Red Cross, UNICEF, the United Nations Foundation (UNF), the U.S. Centers for
Disease Control and Prevention (CDC), and the World Health Organization. The M&RI
recognized the work that had been done in this Region, not only by the countries putting these
reports together but by the RVC members who read and evaluated the reports. Ms Gay
acknowledged the importance of this first opportunity for any countries or areas outside of the
Americas to be verified as having achieved measles elimination. She noted that the verification
of Australia, Macao SAR (China), Mongolia, and the Republic of Korea had global implications
that reach beyond the Region and will help motivate and mobilize other regions and countries.
The lessons learnt from the process, the Guidelines, the materials, and planning will be useful to
other regions as they begin their verification process. Lessons from Hong Kong SAR (China),
- 22 -
Macao SAR (China) and Singapore provide important information about the need for very high
coverage with excellent surveillance systems in densely populated urban areas to prevent re-
establishing transmission from multiple importations. China can also serve as an example to
large countries. Lastly, she noted that Tim Wirth, the former Director of UNF once said, “Our
main responsibility is to make sure people want to come back.” She expressed appreciation to
Professor Durrheim, Acting Chair of the RVC and noted that he had achieved this. She
expressed appreciation to the WHO Regional Office for the Western Pacific secretariat for their
support to the meeting.
4.4 Closing session
Closing comments on behalf of the Regional Director for the Western Pacific were shared
by Dr Mark Jacobs. The Regional Director recognized the important role of the M&RI partners
in measles elimination as collaborators in this regional effort. Dr Shin thanked the members of
the RVC for their tremendous efforts in reviewing the NVC reports that were submitted this year.
RVC members were originally appointed to a two-year term of service from approximately
February 2012 to March 2014. Therefore, RVC members were asked to indicate by email to the
Secretariat their willingness to continue serving on the Commission. Finally, he closed by noting
that the verification of the four countries and areas may serve to encourage others in the Region,
noting in particular that the verification of Mongolia highlights an important achievement among
low- and middle-income countries.
4.5 Award ceremony for the Government of the Republic of Korea
Following the close of the meeting, an award ceremony was held to acknowledge the
achievement of the verification of measles elimination by the host country of the meeting, the
Republic of Korea. At the ceremony, the Acting Chair of the RVC, Professor David Durrheim
provided an overview of the verification process and a description of what it means to be verified
as having achieved measles elimination. Next, Dr Mark Jacobs provided the background and
progress towards measles elimination. This was followed by a congratulatory message from the
Dr Shin Young-soo. A certificate of verification of measles elimination from the RVC signed by
Professor Durrheim and a letter of endorsement signed by Dr Shin were presented to
Dr Yang Byungguk, Director for the Korea Centers for Disease Control and Prevention.

THIRD ANNUAL MEETING OF THE REGIONAL VERIFICATION COMMISSION FOR MEASLES ELIMINATION
IN THE WESTERN PACIFIC
ANNEX 1
14 March 2014
English only Seoul, Republic of Korea, 18–21 March 2014
TIMETABLE
Time Tuesday, 18 March 2014 Time Wednesday, 19 March 2014 Time Thursday, 20 March 2014 Time Friday, 21 March 2014
08:00–08:30
08:30–09:00
REGISTRATION
Opening Session
• Opening remarks
• Self-introduction
• Administrative announcements
08:30–09:00
09:00–10:00
9. Review recommendations from
Day 1
10. Report from Macao (China)
08:30–09:00
09:00–09:30
09:30–10:00
20. Review recommendations from
Day 2
21. Report from Singapore
22. Draft recommendations to
Singapore
08:30–9:00
09:00–09:30
09:30–10:00
31. Review recommendations from
Day 3
32. Report from Papua New Guinea
33. Draft recommendations to
Papua New Guinea
09:00–09:45 GROUP PHOTO AND COFFEE
BREAK
10:00–10:30 COFFEE BREAK 10:00–10:30 COFFEE BREAK 10:00–10:30 COFFEE BREAK
09:45–10:00
10:00–11:00
11:00–12:00
1. Meeting objectives
2. Global and regional progress on
measles elimination and rubella
control
3. Report from the Republic of Korea
10:30–11:00
11:00–12:00
11. Draft recommendations to
Macao (China)
12. Report from Mongolia
10:30–11:30
11:30–12:00
23. Report from China
24. Draft recommendations to
China
10:30–11:30
11:30–12:00
34. Review all recommendations
Closing session:
• Comments by M&R Initiative
o American Red Cross
o UN Foundation
o UNICEF
o US CDC
• WHO Closing remarks
12:00–13:00 LUNCH BREAK 12:00–13:00 LUNCH BREAK 12:00–13:00 LUNCH BREAK 12:00–13:00 LUNCH BREAK
13:00–13:30
13:30–14:30
14:30–15:00
4. Draft recommendations to the
Republic of Korea
5. Report from Australia
6. Draft recommendations to Australia
13:00–13:30
13:30–14:00
14:00–14:30
14:30–15:00
13. Draft recommendations to
Mongolia
14. Report from Brunei Darussalam
15. Draft recommendations to
Brunei Darussalam
16. Report from Hong Kong (China)
13:00–13:45
13:45–14:15
14:15–15:00
25. Report from Malaysia
26. Draft recommendations to
Malaysia
27. Report from the Philippines
14:00–15:00 Presentation to the Government of
the Republic of Korea
15:00–15:30 COFFEE BREAK 15:00–15:30 COFFEE BREAK 15:00–15:30 COFFEE BREAK
15:30–16:30
16:30–17:00
18:00–19:30
7. Report from Japan
8. Draft recommendations to Japan
Regional Director's Reception
15:30–16:00
16:00–16:30
16:30–17:00
17. Draft recommendations to
Hong Kong (China)
18. Report from New Zealand
19. Draft recommendations to
New Zealand
15:30–16:00
16:00–16:30
16:30–17:00
28. Draft recommendations to the
Philippines
29. Report from Viet Nam
30. Draft recommendations to
Viet Nam
15:00–16:30 Reception hosted by the Korea
Centers for Disease Control and
Prevention (KCDC)
ANNEX 2
LIST OF REGIONAL VERIFICATION COMMISSION MEMBERS
OBSERVERS/REPRESENTATIVES AND SECRETARIAT
1. REGIONAL VERIFICATION COMMISSION MEMBERS
Dr Maria Rosario Capeding, Head, Department of Microbiology, Research Institute for Tropical Medicine, Filinvest Corporate City, Alabang, Muntinlupa City 1781, Philippines Mobile No. (63) 9178509788. Tel. No. (632) 7724916. Fax No. (632) 7724916 E-mail : [email protected]
Professor David Durrheim, Professor of Public Health Medicine, University of Newcastle District, Locked Bag 10, Wallsend, New South Wales 2287, Australia. Tel. No. (612) 49246395. Fax No. (612) 49246215. E-mail : [email protected].; [email protected]
Dr Kee Tai Goh, Senior Consultant, Ministry of Health, College of Medicine Building, 16 College Road, Singapore 169854, Republic of Singapore. Tel. No. (65) 63258450. Fax No. (65) 62241677 E-mail : [email protected]
Dr Dukhyoung Lee, Director, National Cancer Control Institute, 323 Ilsan-ro, Goyang-si, Gyeonggi-do 410-769, Republic of Korea. Tel. No.: (8231) 9202003. Fax No.: (8231) 9202909. E-mail : [email protected]; [email protected]
Dr Wilina Wei Ling Lim, Honorary Consultant, Department of Health, Hong Kong Government 9F Public Health Laboratory Centre, 382 Nam Cheong Street, Shek Kip Mei, Kowloon Hong Kong. Tel No. :(882) 94994006. Fax No.: (852) 23195989. E-mail : [email protected]
Dr Pagbajabyn Nymadawa, President and Leader, Molecular Epidemiology Team, Mongolian Academy of Medical Sciences, P.O. Box 596, Central Post, Ulaanbaatar 15160 Mongolia. Tel no. : (976) 99112306. Fax no.: (976) 11450267. E-mail : [email protected]
Dr Mark James Papania, Medical Epidemiologist, Centers for Disease Control and Prevention, 1600 Clifton Rd., Atlanta, Georgia 30249, United States of America. Tel. No.: (770) 265 6483. Fax No. : (404) 6398761. E-mail : [email protected]; [email protected]
Dr Phan Trong Lan, Director, Pasteur Institute, Hanoi, Viet Nam. Tel. No.: (844) 0913002797. Fax No.: (848) 8231419 E- mail: [email protected]
Dr Bounpheng Philavong, Director, Centre for HIV/AIDS and STI, Ministry of Health, Km3 Thadeua Road, Vientiane, Lao People's Democratic Republic. Tel. No. (856) 20 23671175. Fax No. (856) 21 315500. E-mail : [email protected]
Dr Paul Rota, Lead Scientist, Measles Team, Measles, Mumps, Rubella and Herpesvirus Laboratory Branch, Division of Viral Diseases, Centers for Disease Control and Prevention, Mailstop C-22, 1600 Clifton Road, Atlanta, Georgia 30333, United States of America. Tel. No.: (404) 6394181. Fax No.: (404) 6394187. E-mail : [email protected]
Dr Soo Thian Lian, Senior Consultant Paediatrician and Head, Paediatric Department, Sabah Women and Children's Hospital, Kota Kinabalu 88996. Tel. No.: (6088) 522600. Fax No.: (6088) 437185. E-mail : [email protected]
Annex 2
Dr John David Vince, Ex-officio Member, National Verification Committee, Director, Taurama Postgraduate and Research Centre, Deputy Dean, School of Medicine and Health Sciences University of Papua New Guinea, Box 5623 Boroko, Papua New Guinea. Tel No.: (675) 73260185. E-mail : [email protected]
Dr Xu Aiqiang, Deputy Director, Shandong Center for Diseases Prevention and Control 16992 Jingshi Road, Jinan, Shandong Province 250014, China. Tel. No.: (86) 531 82679606 Fax No.: (86) 531 82679620. E-mail : [email protected]
Dr Hiroshi Yoshikura, Adviser, Department of Food Safety, Ministry of Health Labour and Welfare, Japanese Government, 1-2-2 Kasumigaseki Chiyoda-ku, Tokyo 100 8916, Japan. Tel. No.: (813) 35952326. Fax No.: (813) 35037965. E-mail : [email protected]
2. REPRESENTATIVES AND OBSERVERS
AMERICAN
RED CROSS
Dr Myrna Charles, Senior Technical Advisor, International Services, American Red Cross, 2025 E Street, NW, 3rd Floor, Washington DC 20006, United States of America. Tel. No.: +1 (202) 303 5243. Fax No.: +1 (202) 303 0052. E-mail : [email protected]
UNICEF Ms Karen Mah, Communicaitons Specialist, Measles and Rubella Initiative, UNICEF, 3 United Nations Plaza, New York, New York 10017, United States of America. Tel. No.: +1 (917) 265 4603. E-mail : [email protected]
Dr Wang Xiaojun, Immunization Specialist, UNICEF East Asia and Pacific Regiona Office, 19 Phra Atit Road, Chanasongkram, Phra Nakorn, Bangkok, 10200, Thailand. Tel. No.: (+662) 3569468. Fax No.: (662) 2803563. E-mail : [email protected]
UNITED
NATIONS
FOUNDATION
Ms Anrea Gay, Executive Director, Children's Health, United Nations Foundation, 1750 Pennyslvania Avenue NW, Suite 300, Washington D.C. 20006 United States of America. Tel. No.: (202) 8879040. Fax No.: (202) 8879021. E-mail : [email protected]
UNITED
STATES
CENTERS FOR
DISEASE
CONTROL AND
PREVENTION
Dr Eugene Lam, Medical Officer, Global Immunization Division, Center for Global Health, Center for Disease Control and Prevention, 1600 Clifton Road, NE Mailstop A-04, Atlanta, Georgia 30333, United States of America. Tel. No.: +1 (404) 7184294. Fax No.: +1 (404) 2350011. E-mail : [email protected]

Annex 2
3. SECRETARIAT
Dr Mark Jacobs, Director, Combating Communicable Diseases, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel. No. : (632) 5289701. Fax No.: (632) 5211036. E-mail : [email protected]
Dr Sergey Diorditsa, Team Leader, Expanded Programme on Immunization, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel. No.: (632) 5289745. Fax No.: (632) 5211036. E-mail : [email protected]
Dr Youngmee Jee, Scientist and Regional Laboratory Coordinator, Expanded Programme on Immunization, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel. No.: (632) 52889744. Fax No. (632) 5211036. E-mail : [email protected]
Dr Jorge Mendoza-Aldana, Technical Officer (Vaccine Safety and Management), Expanded Programme on Immunization, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel. No.: (632) 5289751. Fax No.: (632) 5211036. E-mail : [email protected]
Dr William Schluter, Medical Officer, Expanded Programme on Immunization, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel No.: (632) 5289748. Fax No.: (632) 5211036. E-mail : [email protected]
Dr Yoshihiro Takashima, Medical Officer, Expanded Programme on Immunization, World Health Organization Regional Office for the Western Pacific, United Nations Avenue, 1000 Manila, Philippines. Tel. No.: (632) 5289746. Fax No.: (632) 5211036. E-mail : [email protected]

1
Third Annual Meeting of the Regional
Verification Commission for Measles
Elimination in the Western Pacific
Global and Regional Progress on
Measles Elimination and Rubella
Control
1
18-21 March 2014
Sheraton D Cube City Hotel
Seoul, Republic of Korea
Measles and Rubella Targets
Global targets by 2015:
Measles mortality reduction of 95% vs. 2000
Measles reported incidence <5 cases per million
Measles vaccination coverage
national level: 90%
every district: 80%
Regional targets:
Measles Elimination goals:
2000 AMRO
2012 WPRO
2015 EURO, EMRO
2020 AFRO, SEARO
Rubella Elimination goals:
2010 – AMRO, 2015 – EURO
GVAP goal:
2020 Measles and rubella elimination in 5 WHO regions
2
Reported measles cases by WHO
Region, 2000-2012
0
100
200
300
400
500
600
700
800
900
Re
po
rte
d n
um
be
r o
f ca
ses
10
00
s
Year
WPR
SEAR
EUR
EMR
AMR
AFR
0.1
1.0
10.0
100.0
1,000.0
Me
asl
es
inci
de
nce
pe
r m
illi
on
po
pu
lati
on
(lo
g s
cale
)
GOAL
AFR
EMR
EUR
SEAR
WPR
AMR
GLOBAL
needed
2015 Goal
Projected 10-
yr trend
Trend to
reach
goal
77% Reduction in Global Measles Incidence per Million Population, 2000-2012
4
ANNEX 3RVC Presentation

2
!
! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! !
!
! !
! ! !
! ! !
! ! !
! !
! ! ! !
! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! !
! ! ! !
! ! !
! !
! ! ! ! ! !
! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! !
! !
! ! !
! ! ! !
! ! ! ! !
! ! ! !
! ! ! !
! ! ! !
! ! ! ! !
! ! ! !
! ! !
! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! !
!
! !
! ! !
!
!
! ! ! !
! ! ! !
! !
! ! !
! ! !
! ! !
! !
! ! !
! ! ! !
! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! !
!
! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! !
! ! ! !
! ! ! ! !
! ! ! ! !
! !
! ! !
! ! ! !
! ! ! !
! !
! ! !
! ! ! !
! ! ! !
! ! ! !
! ! !
! !
! !
!
! ! !
! ! !
! ! !
! ! !
! !
! ! !
! ! !
! !
!
! !
! !
!
! ! !
! ! ! ! !
! ! ! !
! !
! !
! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! !
! ! !
! ! ! ! ! !
! ! ! ! ! ! ! !
! ! ! ! ! !
!
! ! ! !
! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! !
! ! ! !
! ! ! !
! !
! ! ! !
! ! ! ! !
! ! ! ! !
! ! !
! !
! ! !
! !
!
! !
! !
! ! !
! ! ! !
! ! ! !
!
!
!
! ! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! ! ! ! ! !
! ! ! ! ! ! ! !
! ! !
! !
!
! ! !
! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! !
! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! !
! ! ! !
! !
! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! !
! ! !
! ! !
! !
!
! !
!
! ! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! !
! !
! !
! ! ! !
! ! ! ! ! !
! ! ! ! ! !
! ! ! !
! ! !
! !
! ! !
! ! ! !
! ! ! !
!
! !
! ! !
! ! ! ! !
! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! !
! ! !
! !
!
! !
! ! ! ! !
! ! ! ! !
! ! ! ! ! ! !
! ! ! ! ! ! ! !
! ! ! ! !
! ! ! ! !
! ! ! ! ! ! !
! ! ! !
! !
! !
! !
Reported Measles Incidence Rate*,
Feb 2013 to Jan 2014 (12M period)
*Rate per 1'000'000 population
Data source: surveillance DEF file
Data in HQ as of 10 March 2014
The boundaries and names shown and the designations used on this map do not imply the
expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement. ©WHO 2014. All
rights reserved.
<1 (83 countries or 43%)
≥1 - <5 (35 countries or 18%)
≥5 - <10 (12 countries or 6%)
≥10 - <50 (38 countries or 20%)
≥50 (14 countries or 7%)
No data reported
to WHO HQ
(12 countries or 6%)
Not applicable
0.7 1.4 2.3 3.2 4.15.2 6.3
7.6 8.910.1 11.3 12.5 13.8
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Est
ima
ted
me
asl
es
de
ath
s (m
illi
on
s)Year
Estimated measles deaths in absence of vaccination
(numbers give the cumulative number of deaths prevented in millions)
95% CI of estimated measles deaths with vaccination
Estimated measles deaths with vaccinationDeaths averted by measles vaccination
Global estimated measles mortality and measles
deaths averted, 2000 - 2012
78% reduction from 2000 to 2012
Measles Surveillance System Sensitivity
Feb 2013 to Jan 2014 (12M period)
reporting rate of discarded cases* per 100'000 population**
Target: at least 2 discarded cases
per 100'000 population by country
in last 12 month period.
*discarded cases are suspected
measles cases which have been investigated
and discarded as non-measles cases using
laboratory testing and/or epidemiological-
linkage.
** World population prospects, 2012 revision.
Data source: surveillance DEF file
Data in HQ as of 10 March 2014
The boundaries and names shown and the designations used on this map do not imply the
expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement. ©WHO 2014. All
rights reserved.
≥2 (60 countries or 31%)
>1 - <2 (23 countries or 12%)
≤1 (48 countries or 25%)
No case based
surveillance or
No or insufficient data reported
(63 countries or 32%)
Not applicable
16
1920
37
42
4847
54
63
68
73
69 6970
7273 73
7172 72
73 7372
74
7776
81 81
8384 84 84 84
86
88
90
0
10
20
30
40
50
60
70
80
90
100
MC
V1
Co
ve
rag
e*
(%)
Global AFR SEAR EMR AMR EUR WPR
Global coverage has levelled off at 84%1st Dose measles vaccine coverage by WHO region, 1980-2012
8
Source: WHO/UNICEF coverage estimates 2012 revision. July 2013; Immunization Vaccines and Biologicals, (IVB), World Health Organization.
194 WHO Member States. Date of slide: 17 July 2013
Annex 3

3
Weak Immunization Systems
• 21 million infants
missed MCV1 in 2012
• 2/3 live in
– India
– Nigeria
– Ethiopia
– Indonesia
– Pakistan
– DRC
21 million infants not immunized (MCV1), 2012
India, 6.37
Nigeria, 3.76
Ethiopia, 1.00Indonesia, 0.92
Pakistan, 0.73Democratic Republic
of the Congo, 0.68
Philippines, 0.35
United States of
America, 0.34
Afghanistan, 0.31
Iraq, 0.31
Rest of the world,
6.38
0 2,400 4,8001,200 Kilometers
Measles 2nd dose introductions planned in 9 more
countries during 2013-14
10
Not available
Not applicable
No (39 member states or 20%)
Introduced or planned 2013-2014 (9 member states or 5%)
Introduced prior to 2013 (146 member states or 75%)
2013: Kenya, Rwanda, Sao Tome e Principe,
Zambia
2014: Burkina Faso, Nepal, Senegal, Sierra
Leone, Tanzania
Data in HQ as of 15 October 2013
Measles campaigns in 32 countries in 2012
11
Vitamin A – 18
De-worming – 11
Bed nets – 1
OPV – 18
Other interventions -8 Not Applicable
Not Available
Measles (10)
Measles and OPV (15)
Measles and Rubella (7)
• 112 million children reached• 81% (26 of 32) SIAs integrated 1
or more other interventions
Not applicable
Distribution of measles genotypes
from Jan to Dec 2013
Data source: MeaNS Database
Updated on 03 February 2014
The boundaries and names shown and the designations used on this map do not imply the
expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement. ©WHO 2014. All
rights reserved.
Annex 3

4
In the Western Pacific Region
13
• 2003: Measles elimination to be used to strengthen
routine immunization
• 2005: By 2012, the Region should aim to eliminate
measles;
• 2010: Reaffirms the 2012 measles elimination goal and
calls to accelerate control of rubella; and to develop
regional verification mechanism;
• 2012: Reaffirms the commitment to eliminate measles
and accelerate rubella control; NVCs should develop and
submit regular reports to the RVC
Regional Measles and Rubella Goals
• Measles
– The TAG urges countries to make intensified efforts to
accelerate progress towards achieving and sustaining
measles elimination.
• Rubella
– The TAG recommends establishing a regional goal of
eliminating rubella, with a target date to be determined
Technical Advisory Group on Immunization
Recommendations, June 2013
Line of Evidence 1: Measles Epidemiology
Measles Cases by Month and Year, Region, 2008–2013
Data as of 20 February 2014Source: National measles and rubella monthly report
0
5 000
10 000
15 000
20 000
25 000
30 000
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2008 2009 2010 2011 2012 2013
Number of measles cases
China Japan Philippines Viet Nam Others
Annex 3
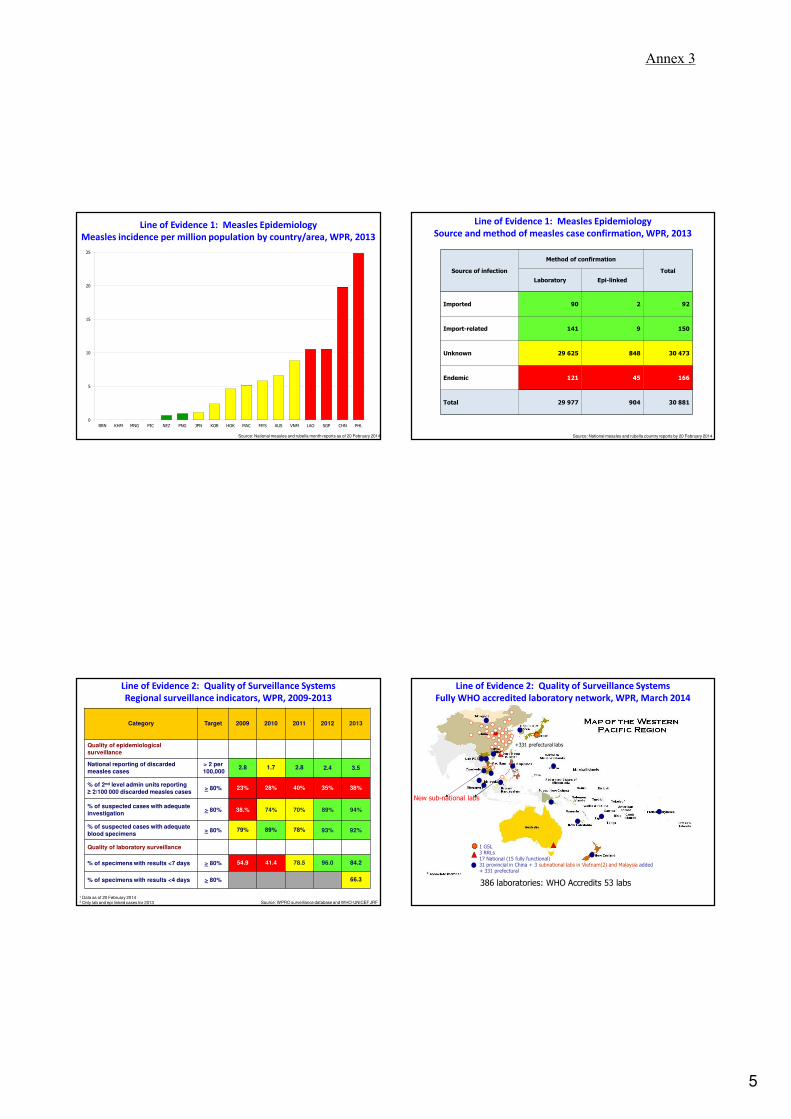
5
Line of Evidence 1: Measles Epidemiology
Measles incidence per million population by country/area, WPR, 2013
Source: National measles and rubella month reports as of 20 February 2014
0
5
10
15
20
25
BRN KHM MNG PIC NEZ PNG JPN KOR HOK MAC MYS AUS VNM LAO SGP CHN PHL
Source: National measles and rubella country reports by 20 February 2014
Source of infection
Method of confirmation
Total
Laboratory Epi-linked
Imported 90 2 92
Import-related 141 9 150
Unknown 29 625 848 30 473
Endemic 121 45 166
Total 29 977 904 30 881
Line of Evidence 1: Measles Epidemiology
Source and method of measles case confirmation, WPR, 2013
Source: WPRO surveillance database and WHO-UNICEF JRF
¹ Data as of 20 February 2014
2
Only lab and epi linked cases for 2013
Category Target 2009 2010 2011 2012 2013
Quality of epidemiological
surveillance
National reporting of discarded
measles cases
> 2 per
100,0002.8 1.7 2.8 2.4 3.5
% of 2nd level admin units reporting
≥ 2/100 000 discarded measles cases> 80% 23% 28% 40% 35% 38%
% of suspected cases with adequate
investigation> 80% 38.% 74% 70% 89% 94%
% of suspected cases with adequate
blood specimens > 80% 79% 89% 78% 93% 92%
Quality of laboratory surveillance
% of specimens with results <7 days > 80% 54.9 41.4 78.5 96.0 84.2
% of specimens with results <4 days > 80% 66.3
Line of Evidence 2: Quality of Surveillance Systems
Regional surveillance indicators, WPR, 2009-2013
+331 prefectural labs
1 GSL3 RRLs17 National (15 fully functional)31 provincial in China + 3 subnational labs in Vietnam(2) and Malaysia added + 331 prefectural
386 laboratories: WHO Accredits 53 labs
New sub-national labs
Line of Evidence 2: Quality of Surveillance Systems
Fully WHO accredited laboratory network, WPR, March 2014
Annex 3

6
Line of Evidence 3: Population Immunity
MCV1 and MCV2 coverage and reported cases, 1980-2012
21
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0
200
400
600
800
1000
1200
1400
1980 1981 1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Measles cases Rubella Cases
Source: WHO-UNICEF Joint Reporting Form (data for 2012)
Category 2009 2010 2011 2012 2013
High population immunity
% countries with MCV1 ≥90% 57% 66% 70% 76%
% countries with MCV1 ≥80% in all
dist46% 46% 41% 63%
Source: WPRO surveillance database and WHO-UNICEF JRF
¹ Data as of 20 February 2014
2
Only lab and epi linked cases for 2013
Line of Evidence 3: Population Immunity
Regional estimates of population measles immunity, WPR, 2009-2012
Line of Evidence 3: Population Immunity
MCV2 introduction into routine EPI in (region) 2014
Line of Evidence 3: Population Immunity
MCV2 introduction into routine EPI in (region) 2014
Only 4 countries or areas have not yet introduced
MCV2:
• Lao People’s Democratic Republic
• Papua New Guinea: 2013 GAVI application
• Solomon Islands
• Vanuatu
With MCV2
With no MCV2
Line of Evidence 3: Population Immunity
Measles Supplemental Immunization Campaigns, WPR, 2013-2015
24
Country Vaccine Target Age Dates Geographic Extent
Micronesia MR 9-59 m Jul 2013 Chuuk State
Vanuatu MR 9-59m Q2 2013 Nationwide
Cambodia MR 9m-15y Q4 2013 Nationwide
Micronesia MMR 12-59 m Jun 2014 Pohnpei State
Viet Nam MR 9m-15yQ3 2014 –
Q2 2015 Nationwide
Philippines MR 9-59 m Sept 2014 Nationwide
Lao PDR MR 9-59 m Nov 2014 Nationwide
Papua New Guinea MR 9m-15y 2015 Nationwide
Solomon MR 9m-15y 2015 Nationwide
Annex 3
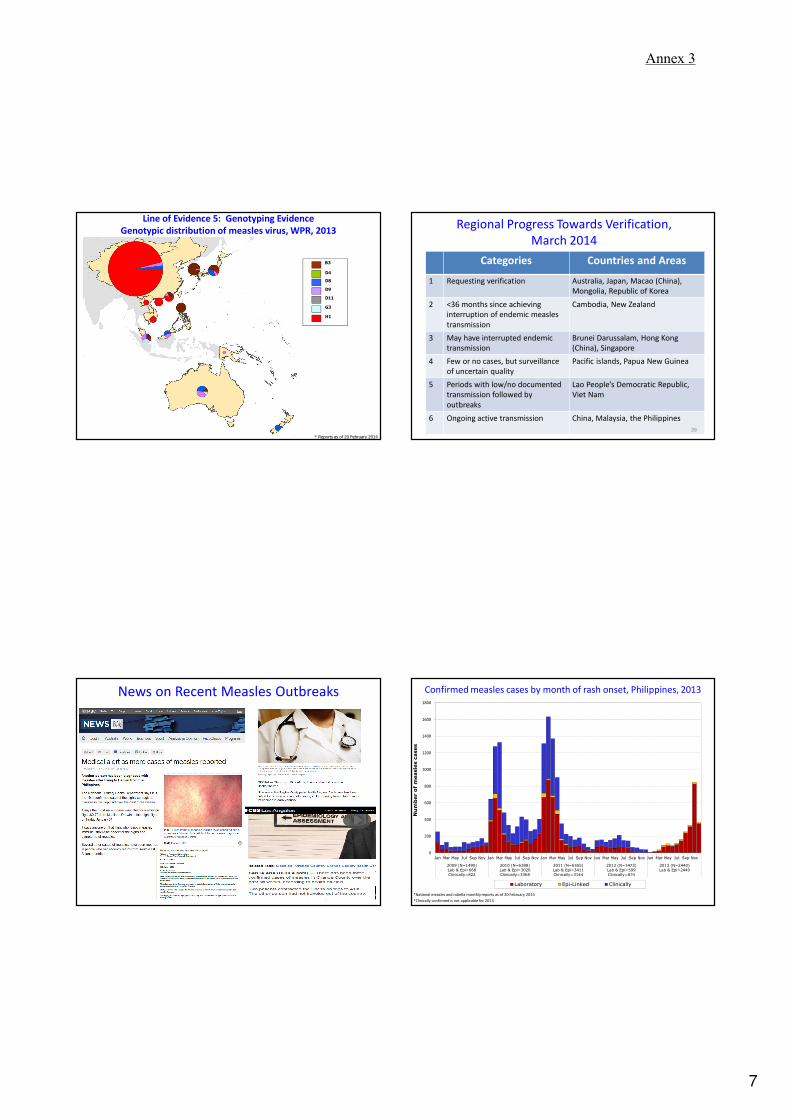
7
D4
D8
D9
D11
G3
H1
B3
* Reports as of 20 February 2014
Line of Evidence 5: Genotyping Evidence
Genotypic distribution of measles virus, WPR, 2013
Line of Evidence 5: Genotyping Evidence
Genotypic distribution of measles virus, WPR, 2013Regional Progress Towards Verification,
March 2014
Categories Countries and Areas
1 Requesting verification Australia, Japan, Macao (China),
Mongolia, Republic of Korea
2 <36 months since achieving
interruption of endemic measles
transmission
Cambodia, New Zealand
3 May have interrupted endemic
transmission
Brunei Darussalam, Hong Kong
(China), Singapore
4 Few or no cases, but surveillance
of uncertain quality
Pacific islands, Papua New Guinea
5 Periods with low/no documented
transmission followed by
outbreaks
Lao People’s Democratic Republic,
Viet Nam
6 Ongoing active transmission China, Malaysia, the Philippines
26
News on Recent Measles Outbreaks
27
Confirmed measles cases by month of rash onset, Philippines, 2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
200
400
600
800
1000
1200
1400
1600
1800
Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov
2009 (N=1490)
Lab & Epi=668
Clinically=822
2010 (N=6388)
Lab & Epi=3020
Clinically=3368
2011 (N=6555)
Lab & Epi=3411
Clinically=3144
2012 (N=1473)
Lab & Epi=599
Clinically=874
2013 (N=2440)
Lab & Epi=2440
Number of measles cases
Laboratory Epi-Linked Clinically
Annex 3

8
Laboratory and epi-linked confirmed measles cases by province,
Philippines, 2012 and 20131
1 dot = 1 case
20122013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
D9
genotype
B3
genotype
Laboratory and epi-linked confirmed measles cases by age group and
vaccination status, Philippines, 2013 (N=2440)
*National measles and rubella monthly reports as of 20 February 2014
0
100
200
300
400
500
600
700
800
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
0
100
200
300
400
500
600
700
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 ≥40
Measles cases
Age in years
0 dose 1 dose ≥2 doses Unknown
Laboratory and epi-linked confirmed measles cases by age in year and
vaccination status, Philippines, 2013 (N=2440)
*National measles and rubella monthly reports as of 20 February 2014
32
Emergency Outbreak Response Immunization Campaign
Philippines, Jan 22 to Feb 14, 2014
Annex 3
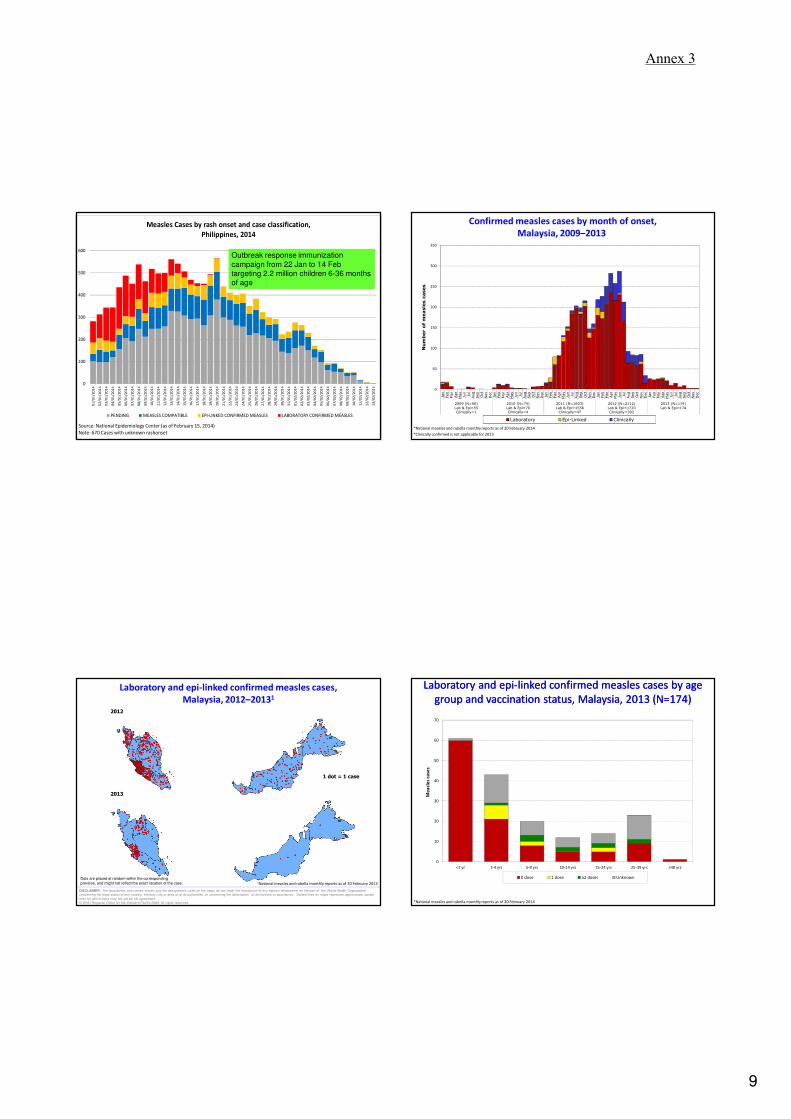
9
33
0
100
200
300
400
500
600
01
/01
/20
14
02
/01
/20
14
03
/01
/20
14
04
/01
/20
14
05
/01
/20
14
06
/01
/20
14
07
/01
/20
14
08
/01
/20
14
09
/01
/20
14
10
/01
/20
14
11
/01
/20
14
12
/01
/20
14
13
/01
/20
14
14
/01
/20
14
15
/01
/20
14
16
/01
/20
14
17
/01
/20
14
18
/01
/20
14
19
/01
/20
14
20
/01
/20
14
21
/01
/20
14
22
/01
/20
14
23
/01
/20
14
24
/01
/20
14
25
/01
/20
14
26
/01
/20
14
27
/01
/20
14
28
/01
/20
14
29
/01
/20
14
30
/01
/20
14
31
/01
/20
14
01
/02
/20
14
02
/02
/20
14
03
/02
/20
14
04
/02
/20
14
05
/02
/20
14
06
/02
/20
14
07
/02
/20
14
08
/02
/20
14
09
/02
/20
14
10
/02
/20
14
11
/02
/20
14
12
/02
/20
14
13
/02
/20
14
Measles Cases by rash onset and case classification,
Philippines, 2014
PENDING MEASLES COMPATIBLE EPI-LINKED CONFIRMED MEASLES LABORATORY CONFIRMED MEASLES
Source: National Epidemiology Center (as of February 15, 2014)
Note: 670 Cases with unknown rashonset
Outbreak response immunization
campaign from 22 Jan to 14 Feb
targeting 2.2 million children 6-36 months
of age
Confirmed measles cases by month of onset,
Malaysia, 2009–2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
50
100
150
200
250
300
350
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=56)
Lab & Epi=55Clinically=1
2010 (N=74)
Lab & Epi=70Clinically=4
2011 (N=1603)
Lab & Epi=1556Clinically=47
2012 (N=2112)
Lab & Epi=1720Clinically=392
2013 (N=174)
Lab & Epi=174
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases,
Malaysia, 2012–20131
1 dot = 1 case
2012
2013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Malaysia, 2013 (N=174)
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Malaysia, 2013 (N=174)
*National measles and rubella monthly reports as of 20 February 2014
0
10
20
30
40
50
60
70
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Annex 3

10
Confirmed measles cases by month of rash onset, China, 2013
*Clinically confirmed is not applicable for 2013
Source: Measles Surveillance System (MSS)
Laboratory and epi-linked confirmed measles cases by province, China,
2012 and 20131
Note: Dots are placed at random within the county, and might not reflect the exact location of the case within the county.
2012 2013
Source: Measles Surveillance System (MSS)
Laboratory and epi-linked confirmed measles cases by age group and
vaccination status, China, 2013
Source: Measles Surveillance System (MSS)
Age distribution of measles cases, China, 2013
Age (months)
<1 year: 50%
1-4 years: 19%
5-19 years: 5%
≥20 years: 26%
Annex 3

11
Select Recommendations from National / International
Consultation on Measles, China, June 2013
• Provincial (or smaller) SIAs needed to fill
immunity gap
• Survey population coverage among young
children at national and subnational levels
• Develop stronger immunization practice
standards to reduce missed opportunities
• Reduce nosocomial transmission of
measles by reducing admissions, isolating
cases, and vaccinating health workers
Measles in Viet Nam, 2014
Confirmed measles cases by month of rash onset, Viet Nam, 2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov
2009 (N=5222)
Lab & Epi=4958
Clinically=264
2010 (N=1826)
Lab & Epi=847
Clinically=979
2011 (N=745)
Lab & Epi=103
Clinically=642
2012 (N=550)
Lab & Epi=5
Clinically=545
2013 (N=802)
Lab & Epi=802
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases by province, Viet Nam, 2012 and 20131
1
National measles and rubella monthly reports as of 20 February 2014
1 dot = 1 case
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
2012 2013
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
H1
genotype
D8
genotype
Annex 3

12
Laboratory and epi-linked confirmed measles cases by age group and
vaccination status, Viet Nam, 2013 (N=802)
*National measles and rubella monthly reports as of 20 February 2014
0
50
100
150
200
250
300
350
400
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Confirmed measles cases by month of rash onset, Lao PDR, 2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
10
20
30
40
50
60
70
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=72)
Lab & Epi=72
Clinically=0
2010 (N=153)
Lab & Epi=6
Clinically=147
2011 (N=113)
Lab & Epi=29
Clinically=84
2012 (N=36)
Lab & Epi=32
Clinically=4
2013 (N=68)
Lab & Epi=68
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases by province, Lao
PDR, 2012 and 20131
1National measles and rubella monthly reports as of 20 February 2014
1 dot = 1 case
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
2012 2013
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Laboratory and epi-linked confirmed measles cases by age group and
vaccination status, Lao PDR, 2013 (N=68)
*National measles and rubella monthly reports as of 20 February 2014
0
2
4
6
8
10
12
14
16
18
20
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Annex 3

13
Rubella-containing vaccine introduction in (region) 2013Rubella-containing vaccine introduction in (region) 2013
Only 4 countries and areas have not introduced
RCV in RI in 2013:
• Cambodia: 2013 MR SIA (9 mos to <15 years)
• Papua New Guinea: 2013 GAVI application
• Vanuatu: 2013 MR SIA (9 to 59 months)
• Viet Nam: 2014 MR SIA
With RCV
With no RCV
Summary
• In 2013, number of measles cases and incidence markedly
increased since 2012
– Large and ongoing outbreaks in China, Philippines and Viet Nam
• 99% of confirmed cases have unknown source of infection
• Epidemiological and laboratory surveillance performance are high
and improving
– Increased sensitivity needed at subnational levels
• Very high regional routine immunization coverage but significant
heterogeneity among countries/areas and districts
• All but three countries have introduced (or planned) routine MCV2
• Many countries still require periodic measles SIAs to increase
population immunity
• Multiple genotypic changes in the Region should be considered
when assessing virological data 50
Acknowledgements
• WHO/HQ (slides 2-12)
• Department of Health, Philippines (slide 33)
• China CDC (slide 40)
51 52
Annex 3

14
Confirmed measles cases by month of onset,
Singapore, 2009–2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
5
10
15
20
25
30
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=16)
Lab & Epi=16
Clinically=0
2010 (N=54)
Lab & Epi=54
Clinically=0
2011 (N=143)
Lab & Epi=143
Clinically=0
2012 (N=40)
Lab & Epi=37
Clinically=3
2013 (N=56)
Lab & Epi=56
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases,
Singapore, 2012–20131
1 dot = 1 case
2012
2013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Singapore, 2013 (N=56)
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Singapore, 2013 (N=56)
*National measles and rubella monthly reports as of 20 February 2014
0
5
10
15
20
25
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Confirmed measles cases by month of onset,
Hong Kong (China), 2009–2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
1
2
3
4
5
6
7
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=22)
Lab & Epi=9
Clinically=13
2010 (N=11)
Lab & Epi=4
Clinically=7
2011 (N=12)
Lab & Epi=7
Clinically=5
2012 (N=8)
Lab & Epi=5
Clinically=3
2013 (N=34)
Lab & Epi=34
Number of measles cases
Laboratory Epi-Linked Clinically
Annex 3

15
Laboratory and epi-linked confirmed measles cases,
Hong Kong (China), 2012–20131
1 dot = 1 case
2012
2013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Hong Kong (China), 2013 (N=34)
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Hong Kong (China), 2013 (N=34)
*National measles and rubella monthly reports as of 20 February 2014
0
2
4
6
8
10
12
14
16
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s0 dose 1 dose ≥2 doses Unknown
Confirmed measles cases by month of onset,
Papua New Guinea, 2009–2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
1
2
3
4
5
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=0)Lab & Epi=0
Clinically=0
2010 (N=0)Lab & Epi=0
Clinically=0
2011 (N=0)Lab & Epi=0
Clinically=0
2012 (N=0)Lab & Epi=0
Clinically=0
2013 (N=7)Lab & Epi=7
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases,
Papua New Guinea, 2012–20131
1 dot = 1 case
2012
2013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Annex 3
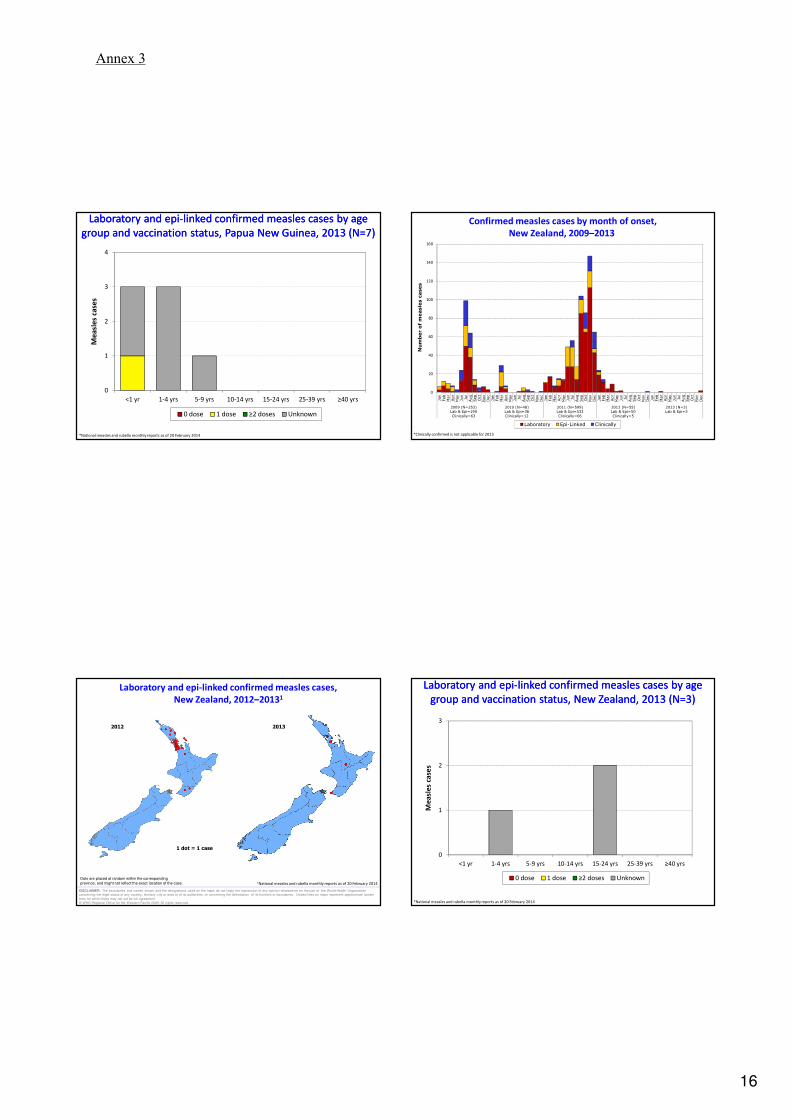
16
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Papua New Guinea, 2013 (N=7)
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, Papua New Guinea, 2013 (N=7)
*National measles and rubella monthly reports as of 20 February 2014
0
1
2
3
4
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Confirmed measles cases by month of onset,
New Zealand, 2009–2013
*National measles and rubella monthly reports as of 20 February 2014
*Clinically confirmed is not applicable for 2013
0
20
40
60
80
100
120
140
160
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
2009 (N=253)Lab & Epi=190
Clinically=63
2010 (N=48)Lab & Epi=36
Clinically=12
2011 (N=599)Lab & Epi=533
Clinically=66
2012 (N=55)Lab & Epi=50
Clinically=5
2013 (N=3)Lab & Epi=3
Number of measles cases
Laboratory Epi-Linked Clinically
Laboratory and epi-linked confirmed measles cases,
New Zealand, 2012–20131
1 dot = 1 case
2012 2013
1National measles and rubella monthly reports as of 20 February 2014
Dots are placed at random within the corresponding
province, and might not reflect the exact location of the case.
DISCLAIMER: The boundaries and names shown and the designations used on the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
© WHO Regional Office for the Western Pacific 2009. All rights reserved.
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, New Zealand, 2013 (N=3)
Laboratory and epi-linked confirmed measles cases by age
group and vaccination status, New Zealand, 2013 (N=3)
*National measles and rubella monthly reports as of 20 February 2014
0
1
2
3
<1 yr 1-4 yrs 5-9 yrs 10-14 yrs 15-24 yrs 25-39 yrs ≥40 yrs
Me
asl
es
case
s
0 dose 1 dose ≥2 doses Unknown
Annex 3

ANNEX 4
Award Ceremony Photo
Award ceremony in Seoul, Republic of Korea, 21 March 2014.

www.wpro.who.int