thinking beyond open defecation free towards safely ... · pdf filemerp monitoring, evaluation...
TRANSCRIPT
i i
SOUTH ASIA REGIONAL LEARNING EVENT SYNTHESIS REPORT
8-11 NOVEMBER 2016 | KANDY, SRI LANKA
The CS WASH Fund is supported by the Australian Government and managed by Palladium International Pty Ltd.
Thinking beyond Open Defecation Free towards safely managed sanitation for all

Civil Society Water, Sanitation and Hygiene Fund
ii
Acknowledgements
Thanks to all the contributors to the CS WASH Fund
South Asia Regional Learning Event particularly: CSOs for their
preparation and participation, their project partners, and
numerous guest speakers and rapporteurs. Thank you to World
Vision Lanka as the hosting partner and the International Water
Management Institute (IWMI) for logistics support. Thank you
to the organising committee made up of representatives from
the Australian Red Cross, Habitat for Humanity, International
Rescue Committee, Plan International Australia, SNV, World
Vision Australia, the CS WASH Fund Monitoring, Evaluation and
Review Panel and Fund Management Facility.
The authors of this report are Mark Ellery, Paul Tyndale-Biscoe,
David van Eyck and Bronwyn Powell. This activity is supported
by the Australian Department of Foreign Affairs and Trade and
managed by Palladium International Pty Ltd.
Recommended citation:
Civil Society WASH Fund (2016) Thinking beyond Open
Defecation Free towards safely managed sanitation for all.
Synthesis Report of the South Asia Regional Learning Event.
Kandy, Sri Lanka, 8-11 November 2016
Cover: Toilets installed adjacent to barracks-style housing
for tea estate workers. These pour-flush latrines were built
as part of RIWASH-2 project with World Vision Lanka funded
by Australian Aid (then AusAID, now DFAT) completed in 2013.
Photo credit: CS WASH FMF / Dazzle Images
Partners:

iii
Contents
Acronyms and abbreviations iv
Executive summary 1
1 Chapter 1: Background 3
1.1 Purpose of this document 3 1.2 The Civil Society Water, Sanitation and Hygiene Fund 3 1.3 The CS WASH Fund in South Asia 4 1.4 Knowledge and Learning and the South Asia Regional Learning Event 4
2 Chapter 2: CSO projects, contexts and strategies 6
2.1 CSO project approaches 6 2.2 Project context and strategy mapping 9
3 Chapter 3: Status of sanitation in South Asia 11
4 Chapter 4: Moving from ODF to safely managed sanitation for all 15
5 Chapter 5: What is safely managed sanitation? 22
5.1 Managing faecal waste 23 5.2 Handwashing with soap 26 5.3 Menstrual Hygiene Management 28
6 Chapter 6: Ensuring equitable sanitation for all 29
6.1 Government roles and financing 29 6.2 Sanitation marketing 32 6.3 Disability inclusive WASH 33 6.4 Reaching women and girls and the underserved 33
7 Chapter 7: Priority SDG sanitation responses in South Asian countries 36
8 Chapter 8: Conclusion 39
Annex 1: References 40 Annex 2: Program 42 Annex 3: CSO projects 48 Annex 4: Latrine options 49
Partners:

iv
Acronyms & abbreviations
Civil Society Water, Sanitation and Hygiene Fund
ARC Australian Red Cross
BDRCS Bangladesh Red Crescent Society
CLTS Community Led Total Sanitation
CS WASH Civil Society Water, Sanitation and Hygiene
CBO Community Based Organisation
CSO Civil Society Organisation
DFAT Department of Foreign Affairs and Trade
EED Environmental Enteric Dysfunction
GDP Gross Domestic Product
GESI Gender Equality and Social Inclusion
GO Government Organisations
HfH Habitat for Humanity
iDE International Development Enterprises
IRC International Rescue Committee
JMP Joint Monitoring Programme
K&L Knowledge and Learning
LSHTM London School of Hygiene and Tropical Medicine
MDG Millennium Development Goal
MERP Monitoring, Evaluation and Review Panel
MFI Micro-Finance Institute
MHM Menstrual Hygiene Management
MOU Memorandum of Understanding
NGO Non-Government Organisation
NPCODA Northern Province Consortium of Organisations for Differently Abled
ODF Open Defecation Free
PATS Pakistan Approach to Total Sanitation
PHED Public Health Engineering Department
RLE Regional Learning Event
SanMark Sanitation Marketing
SDG Sustainable Development Goal
SNV Netherlands Development Organisation
UNICEF United Nations Children's Emergency Fund
WASH Water, Sanitation and Hygiene
WHO World Health Organization
WSP World Bank Water and Sanitation Program
WV World Vision

1 1
This challenge was the focus of the South Asia
Regional Learning Event (RLE) held in Kandy, Sri Lanka
by the Civil Society Water, Sanitation and Hygiene
Fund (CS WASH Fund, ‘the Fund’) from 8-11 November
2016. The event was part of the Fund-wide Knowledge
and Learning; a component of the Fund that fosters
evidence-based WASH knowledge and innovations
within, between and beyond projects and the Fund.
It consisted of four days of facilitated interactive
learning, key content delivery, peer-to-peer learning
and a field trip.
The South Asian region achieved significant
improvements in sanitation coverage within the
Millennium Development Goal (MDG) period. Near total
Open Defecation Free (ODF) status was achieved in
Bangladesh and Sri Lanka; with Bangladesh, Nepal and
Pakistan achieving more than 30% reduction in open
defecation between 1990 and 2015. Moving beyond ODF and working towards the targets set by the Sustainable Development Goals (SDGs) increases the challenge to not only reach improved sanitation but to achieve safely managed sanitation for all.
Executive Summary
Child at a Sri Lankan tea estate washing her hands. Photo credit: CS WASH FMF / Dazzle Images

Civil Society Water, Sanitation and Hygiene Fund
2
This report is a synthesis of the presentations
and discussions of the event whose 98 participants
included Civil Society Organisations (CSOs) in the
Fund, government partners and WASH sector
stakeholders. In South Asia the CS WASH Fund
supports Australian Red Cross (ARC), Habitat for
Humanity (HfH), International Rescue Committee
(IRC), Plan International Australia, Netherlands
Development Organisation (SNV) and World Vision
Lanka and Australia (WV) undertaking eight projects
in Bangladesh, Bhutan, Nepal, Pakistan and Sri Lanka.
These projects include direct support for up to 425,000
poor and vulnerable people to access basic sanitation
for improved health.
Meeting the new targets set by the SDGs, particularly
target 6.2, requires addressing the challenges
which sit beyond the ODF ‘finish line’: to not only
‘declare’ ODF, but to verify and maintain it, and move
households and communities to improved sanitation
with safely managed faecal waste treatment and
disposal. Different countries face different challenges
in climbing up the sanitation ladder. Participants
explored the application of the SDGs to their context
identifying a diversity of priority issues depending on
the country. In Bangladesh, for example, the emptying
of faecal sludge from direct pit latrines is a major issue
while in Sri Lanka the failure to contain the faecal
effluent released from septic tanks is the primary
public health risk associated with faecal
waste management.
‘Safe sanitation’ requires a holistic approach to
WASH including hygiene, especially hygienic
sanitation, handwashing with soap and Menstrual
Hygiene Management. CSOs are working to break the
silence surrounding Menstrual Hygiene Management:
this is critical in Nepal and Bangladesh if the needs
of women and girls are to be properly understood
and met. In Bhutan, SNV is trialling innovations in
behaviour change communication aiming to translate
handwashing knowledge into handwashing practice.
The SDG targets of ensuring that no-one is excluded
from safely managed sanitation services and
progressively eliminating all inequalities are areas
where CSOs make strong contributions to the sector.
For example, WV Lanka facilitated a field visit to
tea estates, exposing participants to the complex
realities of providing sanitation services for hard
to reach groups such as plantation workers where
the ownership of the land, assets and liabilities are
not clear. WV Lanka also contributed expertise on
strengthening disability inclusive WASH
in conjunction with their partner organisations that
work with people with disabilities.
The sanitation targets identified by the SDGs and
possible approaches to reach these were discussed
during the learning event. This was elaborated in a
workshop session designed to map the sanitation
service status, its institutional context within each
country, identify major bottlenecks and establish
priorities necessary to meet the rural sanitation SDG
target. The teams then worked to identify appropriate
social, legal and financial instruments to ensure safely
managed services for all that could be supported by
CSOs. Participants were also engaged in mapping their
project and the extent to which they can influence the
larger institutions of service delivery. In both cases, the
goal was to give participants the tools and reflective
space to engage with strengthening the enabling
environment within which their projects are situated.
3
CHAPTER 1
Background
1.1 Purpose of the document
This report provides a synthesis and summary of the
South Asia Regional Learning Event (South Asia RLE)
held in Kandy, Sri Lanka by the Civil Society Water,
Sanitation and Hygiene Fund from 8-11 November
2016. It seeks to capture the key content delivered by
topic experts and Civil Society Organisations (CSOs)
at the event, record important areas of discussion
by participants and direct practitioners to useful
resources. The intended audience is the CSOs within
the Fund, government partners and other WASH sector
stakeholders. This report may be read in conjunction
with the supporting resource materials available
online and linked in this document.
1.2 The Civil Society Water, Sanitation and Hygiene Fund
The CS WASH Fund is an Australian Aid initiative
funded by the Department of Foreign Affairs and
Trade (DFAT). The Fund resources 13 international
CSOs selected through a competitive grants program
to deliver 29 WASH projects over a four-year
implementation period in Southern Africa, South
Asia, East Asia and the Pacific. The ‘Theory of Change’
for the Fund is for CSO delivery teams to effectively
influence change agents, such as government, private
sector and local water authorities to scale-up and
sustain the improved delivery of water, sanitation
and hygiene services. A recently completed mid-
term review consisted of two parts: a review of
management arrangements by DFAT’s Office of
Development Effectiveness, and a review of projects’
progress by the Monitoring Evaluation and Review
Panel (MERP) in South Asia and globally.
Participants of the South Asia Regional Learning Event. Photo credit: CS WASH FMF / Dazzle Images
Civil Society Water, Sanitation and Hygiene Fund
4
1.3 The CS WASH Fund in South Asia
The CS WASH Fund is supporting five CSOs in
South Asia to undertake eight projects at a value of
approximately AUD 17 million expected to directly
support 425,000 poor and vulnerable people gain
access to basic sanitation for improved health in
the region. The five CSOs are Australian Red Cross
(ARC), Habitat for Humanity (HfH), International
Rescue Committee (IRC), Plan International Australia,
Netherlands Development Organisation (SNV) and
World Vision Australia (WV), managing projects in
Bangladesh, Bhutan, Nepal, Pakistan and Sri Lanka.
Further information on the CSO projects is in Annex 3.
1.4 Knowledge and Learning and the South Asia Regional Learning Event
The CS WASH Fund incorporates a Fund-wide
Knowledge and Learning (K&L) component which
fosters and shares good practice, evidence-based
WASH knowledge and innovations with Fund CSOs,
their partners and the global WASH sector to improve
projects and service delivery. Learning events are a key
opportunity for peer-to-peer learning across CSOs as
well as from sector specialists and researchers1.
Ninety-eight participants attended the South Asia RLE.
The objectives of the event were to:
• Improve the effectiveness and sustainability of
WASH projects within the Fund by facilitating
knowledge exchange and learning;
• Strengthen relationships between CSOs, local
government and other change agents to extend
specific areas for collaboration and sharing; and
1 Research by the Fund revealed that face-to-face learning is not only the preferred method of learning for CSO WASH professionals
but it is also the most effective means for improving WASH practice (CS WASH Fund/ISF-UTS 2016).
• Provide a forum to learn from and share with the
wider WASH sector, including CSOs that cannot
attend the event, and strengthen communities
of practice within the Fund.
The overarching topic was thinking beyond Open Defecation Free (ODF) towards the Sustainable Development Goals (SDGs) and safely managed sanitation for all (elaborated further in
Chapters 3 and 4). Specific objectives agreed by
CSOs were to:
• Improve the understanding of CSO approaches
to embedding and strengthening government/
change agent systems at multiple levels for
demand and supply-side sanitation and
monitoring, including supportive financing and
incentive schemes, and systems for monitoring
changes in access to sanitation;
• Explore approaches to ensure total sanitation
for all, particularly poor and disadvantaged
households, women and girls, people living with
disabilities and to increase sanitation access in
remote and challenging environments; and
• Improve understanding of effective integrated
hygiene behaviour change activities to ensure
maximum health benefits are achieved from
sanitation and water initiatives.
This topic is within the broader context of the overall
approach of the Fund, which is to tackle WASH
holistically, including a focus on crosscutting elements
such as hygiene, gender, environment, K&L, disaster
risk reduction and climate change.
The event deployed an Integrated Learning Platform
approach offering a series of sequential learning
opportunities. This format promotes continual

5
engagement, supports remote participation and
consolidates learning over time. This integrated learning
platform included:
• An e-discussion on the changing roles and
responsibilities in response to the different
challenges posed by the different steps in climbing
the sanitation ladder. This e-discussion focused on
the role of CSOs and others to assist communities
to move from the eradication of open defecation2
to improved sanitation for all.3 It explored total
sanitation including the management of faecal
sludge, drainage and solid waste services and
achieving improved health outcomes such as
regulation and enforcement of environmental
health sanitary standards.
• A webinar on the role of government in ensuring
versus providing safely managed sanitation, and
how CSOs can support government to perform
these two different roles. The webinar included an
introductory presentation distinguishing between
the roles played by government either through
short or long routes of accountability drawing on
the World Bank report, Making Services Work for
Poor People (2003). Plan International Pakistan and
SNV Bhutan presented case studies on their systems
strengthening work with government to eliminate
open defecation, promote the use of improved
sanitation for all and achieve total sanitation.
• The face-to-face Regional Learning Event which
commenced with an open day including WASH
sector stakeholders from Sri Lanka in addition to
Fund participants. This was followed by three days of
facilitated interactive learning, including key content
delivery, peer-to-peer learning and a field trip. A
guided learning tool enabled participants to capture
and reflect on their personal and team objectives
over the course of the event. A high representation
of people with disabilities was a feature of the event,
and their full participation was aided by guidelines
provided by CBM Australia on facilitating inclusive
meetings and events. The learning event was also
an opportunity for CSOs to utilise and develop their
skills with nine presentations given and five thematic
workshops led by CSOs.
2 Moving communities towards the eradication of open defecation involves triggering the behaviour change of individuals within communities to achieve
collective ODF status. 3 Sanitation for all includes proximate, sufficient, affordable and hygienic sanitation facilities for all including for children, women and girls, the poor and people
with disabilities.
Marcus Howard and Nilupuli Pethiyagoda participate in lighting the traditional Sri Lankan oil lamp – a ceremoney to mark the beginning of the learning event.
Photo credit: CS WASH FMF / Dazzle Images

Civil Society Water, Sanitation and Hygiene Fund
6
CHAPTER 2
CSO projects, contexts and strategies
This chapter sets the context of the CSO projects and approaches implemented in South Asia, which include attention to water, sanitation and hygiene and various crosscutting issues, with a particularly strong emphasis on sanitation. This chapter also summarises each project context and the strategy mapping process.
2.1 CSO project approaches
The approaches taken by Fund CSOs in South Asia vary
depending on their context, organisational philosophy
and guidelines. Some approaches are described
below, along with selected highlights from project
posters and ‘bringing the field to the room’ sessions
at the South Asia RLE.
Anowara Begum smiling with her husband in front of her latrine bought with a CBO loan. Photo credit: Habitat for Humanity Bangladesh
7
Habitat for Humanity is working at a community level
in three Districts of Bangladesh. While official figures
suggest high latrine coverage, household access to
hygienic toilets is low. HfH is strengthening community
organisations to provide affordable credit to poor
households to upgrade their toilets.
Plan International Pakistan’s approach is
to strengthen the Punjab Provincial Government’s
capacity to implement the Government’s own Pakistan
Approach to Total Sanitation (PATS 2011). The project
is training community mobilisers and community
development officers from the Public Health
Engineering Department (PHED), and women health
workers from the Health Department Union Council
Secretaries at the district and village level. A focus of
the project is the establishment and support of formal
government-led WASH Core Groups at District level
that will develop WASH road maps to achieve ODF
certification.
The International Rescue Committee is working
in three districts of Khyber Pakhtunkhwa Province in
Pakistan to develop and implement environmental
health plans in 120 villages. The aim is to achieve ODF
through participatory village planning processes that
proactively involve both women and men in setting
environmental health priorities such as water supply
schemes, drainage and pavement, handwashing
facilities and solid waste management.
Thanujiya and Thamilperiyan, both affected by a nerve condition leaving them unable to walk or balance, are pictured in front of their completed disability
inclusive toilet. Photo credit: World Vision Lanka

Civil Society Water, Sanitation and Hygiene Fund
8
Civil Society Water, Sanitation and Hygiene Fund
IRC team members explain their project to South Asian colleagues during the
poster marketplace session. Photo credit: CS WASH FMF / Dazzle Images
Building on past successes the Australian Red Cross/Bangladesh Red Crescent Society project
in Bangladesh enables vulnerable individuals and
communities in targeted areas to address their WASH
related needs as part of a broader resilience focused
program that includes other components such as
shelter, livelihoods, education and disaster risk
reduction. WASH activities include hygiene promotion,
water-testing training, and sanitation marketing
activities leading to latrine construction, water supply
provision and water resources management. The
project is working with key government departments,
community radio, public schools, madrasahs, student
and community leaders and commercial and finance
service providers.
SNV’s Sustainable Sanitation and Hygiene for All
(SSH4A) projects in Bhutan and Nepal accelerate
progress in sanitation and hygiene by strengthening
professional and organisational capacity of local
governments, private sector and stakeholders to
develop a sustainable service delivery model at scale.
They integrate sanitation demand creation, supply
chain development, behaviour change communication
and governance. In Bhutan, the programme provides
technical support to the lead government agency
nationally and at a district level to further the
development and scaling up of the national Rural
Sanitation and Hygiene Programme based on the
SSH4A approach. In Nepal, the project builds on the
successes of the first phase of the CS WASH Fund by
deepening and expanding activities in the Mid-Western
Region with a focus on strengthening post ODF
support mechanisms and sustainability. The project is
also responding to the Government’s priority districts
in the Terai by adapting the approach to this new
context.
World Vision is working in rural areas in the Northern
Province of Sri Lanka where up to 96% of households
in the targeted villages are collecting water from
unprotected wells. WV is supporting national and local
government, and Community Based Organisations
(CBOs) to implement water supply projects in
communities and schools, and to provide financial
support to the most vulnerable members of the
community to construct latrines. Improved dialogue
between communities and government is achieved
through the project’s ‘Citizen Voice in Action’ initiative.
The project has a strong focus on vulnerable groups
and directly involves disabled persons organisations in
the design and implementation of project activities.

Figure 1: Engagement strategy spectrum
STRENGTHENING THE SECTOR /
GOVERNMENT / PRIVATE SECTOR
SUPPORTING THE SECTOR /
GOVERNMENT / PRIVATE SECTOR
COLLABORATING WITH SECTOR /GOVERNMENT
IMPLEMENTING THROUGH A
PARTNER
IMPLEMENTINGDIRECTLY
9
The strategy mapping tool requires teams to rate their
project deliverables according to the same spectrum and
component structure. The tool also allows mapping of
the kind of actor (or change agent) that comprises the
primary focus of the project deliverables (government,
private sector, community or a combination), which in
turn allows the project’s strategy to be mapped by these
classes of change agents.
A project context and strategy mapping session at
the event enabled project teams and their participating
change agents to reflect on their projects and the
context in which they are implemented. Using an
Excel-based tool, project teams first mapped the WASH
context in which their projects operate, and then
mapped their project strategies. The tool generates
two spider-graph ‘maps’ which can be overlain and
compared for relative alignment (see Figure 2). This
activity has been run at each of the Fund’s RLEs.
The mapping processes are based on a strategy
spectrum consisting of five stages (see Figure 1) and
incorporates engagement with government, community
and the private sector. The context mapping uses a
Likert scale that allows the country or regional context
to be placed on a spectrum from fully enabled to not
enabled in terms of delivery of WASH services, and
is done by component (WASH infrastructure; WASH
behaviour change; gender and social inclusion;
environment, climate change and disaster risk
reduction; policy and governance).
2.2 Project context and strategy mapping
Central Province Chief Minister, the Hon Sarath Ekanayake, welcomes participants.
Photo credit: CS WASH FMF / Dazzle Images

Civil Society Water, Sanitation and Hygiene Fund
10
The large number of RLE participants
from Sri Lanka meant that the context and
strategies for WV’s project were mapped
by three different groups (see Figure 2).
Interestingly the three maps generated
were not the same. While all three groups
mapped the infrastructure component
similarly, the other components diverged
for both the context and the project’s
strategic approach to the components.
While the three groups were mapping the
same project, they were all looking at it
from a slightly different perspective: one
group was predominately project staff, the
second predominately government change
agents and the third were staff from Plan
Sri Lanka (who were participating in
the event but are not part of the Fund).
This variation highlights the importance
of a collaborative approach to project
design and the need to ensure that all
stakeholders are involved in analysing
needs and defining the most appropriate
project approach. It also highlights the
subjectivity of mapping results and
its usefulness in triggering discussion,
particularly where views on strategies
and contexts diverge.
The session stimulated robust discussion
within project teams and their counterpart
change agents, which teams found useful.
Project teams were encouraged to take
the tools back to their project offices
and conduct the exercise with the whole
project team in a less time-constrained
environment.
Infrastructure
Behaviour ChangePolicy and Governance
Environment, Climate Change and DRR Gender and Social Inclusion
Infrastructure
Behaviour ChangePolicy and Governance
Environment, Climate Change and DRR Gender and Social Inclusion
Infrastructure
Behaviour ChangePolicy and Governance
Environment, Climate Change and DRR Gender and Social Inclusion
Country Context Map
Project Strategy Map
Figure 2: Three graphs produced for Sri Lanka showing variable results from differnent groups.

Newly constructed toilet. Photo credit: CS WASH FMF / Dazzle Images
11 11
CHAPTER 3
Status of sanitation in South Asia
South Asia has secured significant
improvements in sanitation over the
Millennium Development Goal (MDG)
period. While only the Maldives, Sri
Lanka and Pakistan achieved the MDG
target of halving those without access
to improved sanitation, all countries
saw improvements in the percentage
of their population with access to
sanitation over the MDG period
(see Figure 3).
Figure 3: Sanitation progress during the MDG period in South Asian countries (JMP, 2015)
34%
61% Bangladesh
19%
50% Bhutan
4%
46% Nepal
24%
64% Pakistan 71%
95% Sri Lanka
17%
40% India
21%
32% Afghanistan
68%
98% Maldives
0%
20%
40%
60%
80%
100%
120%
1990 1995 2000 2005 2010 2015
Popu
latio
n us
ing
impr
oved
sani
tatio
n (%
)
Sanitation MDG Progress JMP 2015
34%
1% Bangladesh 11% 2% Bhutan
88%
32% Nepal
49%
13% Pakistan 13%
0% Sri Lanka
75%
44% India
34%
13% Afganistan23%
0% Maldives
0%
20%
40%
60%
80%
100%
1990 1995 2000 2005 2010 2015
Popu
latio
n de
feca
ting
in th
e op
en (%
)
Year
Open Defecation Reduction
0
200
400
600
800
1,000
1990 2015 1990 2015
Mill
ions
of p
eopl
e
# People without Sanitation Facilities in SAR JMP 2015
-161 million
+29.6 million
Maldives Afghanistan Bhutan Sri Lanka
Nepal Bangladesh Pakistan India
Without any latrine (open defecation) Without improved latrine

Civil Society Water, Sanitation and Hygiene Fund
12
34%
61% Bangladesh
19%
50% Bhutan
4%
46% Nepal
24%
64% Pakistan 71%
95% Sri Lanka
17%
40% India
21%
32% Afghanistan
68%
98% Maldives
0%
20%
40%
60%
80%
100%
120%
1990 1995 2000 2005 2010 2015
Popu
latio
n us
ing
impr
oved
sani
tatio
n (%
)
Sanitation MDG Progress JMP 2015
34%
1% Bangladesh 11% 2% Bhutan
88%
32% Nepal
49%
13% Pakistan 13%
0% Sri Lanka
75%
44% India
34%
13% Afganistan23%
0% Maldives
0%
20%
40%
60%
80%
100%
1990 1995 2000 2005 2010 2015 Po
pula
tion
defe
catin
g in
the
open
(%)
Year
Open Defecation Reduction
0
200
400
600
800
1,000
1990 2015 1990 2015
Mill
ions
of p
eopl
e
# People without Sanitation Facilities in SAR JMP 2015
-161 million
+29.6 million
Maldives Afghanistan Bhutan Sri Lanka
Nepal Bangladesh Pakistan India
Without any latrine (open defecation) Without improved latrine
Globally, South Asia has made the most
significant improvements in reducing
open defecation with Bangladesh,
Nepal and Pakistan having all reduced
open defecation by more than 30
percentage points since 1990 (WHO
and UNICEF, 2015). During this time,
the Community Led Total Sanitation
(CLTS) approach of triggering ODF
communities was developed in South
Asia (Kar and Chambers, 2008).
Figure 4: Reduction in open defecation in South Asia over the MDG period (JMP, 2015)
The progress of South Asia in reducing
open defecation has exceeded the
increase in access to improved
sanitation: while the number of people
defecating in the open in South Asia
declined by 161 million over the MDG
period, the number of people without
improved latrines actually increased by
29.6 million (see Figure 5). This is due to
the access to improved latrines failing
to keep up with population growth
(i.e. while fewer people are defecating
in the open, an increased number still
use unimproved latrines).
Figure 5: Progress of sanitation versus open defecation in South Asia over the MDG period (JMP, 2015)
34%
61% Bangladesh
19%
50% Bhutan
4%
46% Nepal
24%
64% Pakistan 71%
95% Sri Lanka
17%
40% India
21%
32% Afghanistan
68%
98% Maldives
0%
20%
40%
60%
80%
100%
120%
1990 1995 2000 2005 2010 2015
Popu
latio
n us
ing
impr
oved
sani
tatio
n (%
)
Sanitation MDG Progress JMP 2015
34%
1% Bangladesh 11% 2% Bhutan
88%
32% Nepal
49%
13% Pakistan 13%
0% Sri Lanka
75%
44% India
34%
13% Afganistan23%
0% Maldives
0%
20%
40%
60%
80%
100%
1990 1995 2000 2005 2010 2015
Popu
latio
n de
feca
ting
in th
e op
en (%
)
Year
Open Defecation Reduction
0
200
400
600
800
1,000
1990 2015 1990 2015
Mill
ions
of p
eopl
e
# People without Sanitation Facilities in SAR JMP 2015
-161 million
+29.6 million
Maldives Afghanistan Bhutan Sri Lanka
Nepal Bangladesh Pakistan India
Without any latrine (open defecation) Without improved latrine

13
The reduction of the number of people defecating in the
open within a given area of a country can be represented
as a decrease in the density of open defecators. This
decrease in open defecation density (i.e. the number
of people open defecating within a particular area)
has a surprisingly high correlation with the average
height for children4 under the age of five (Spears, 2013).
The Demographic and Health Survey data for South
Asian countries shows that as the number of people
defecating in the open declines (i.e. the size of the bubble
decreases), the density of open defecation declines (i.e.
the bubbles move to the left) and the average height of
children increases (i.e. the bubbles move upwards) (see
Figure 6). This high correlation is particularly surprising
because of the difficulty that researchers have faced more
broadly in establishing a significant correlation between
access to improved sanitation and acute undernutrition
(i.e. abnormally low weight-for-age), let alone chronic
undernutrition (i.e. abnormally low height-for-age).
-2.4
-2.2
-2
-1.8
-1.6
-1.4
-1.2
-1
-0.8
1.2 1.4 1.6 1.8 2.0 2.2 2.4
Child
hei
ght f
or a
ge
Open defecation per square km
Bangladesh DHS Pakistan DHS Nepal DHS Sri Lanka DHS India DHS Maldives DHS
Open Defecation Density vs Stunting vs # Open Defecators
Bangladesh 1996-97
Bangladesh 1999-2000
Bangladesh 2004
2005-06
Nepal 2006
Nepal 2001
Nepal 2011
Pakistan 1990-91
Bangladesh 2007
Bangladesh 2014Sri Lanka1987
Maldives 2009
1998-99
Bangladesh 2011
Pakistan 2012-13
India
4 Child <5 height-for-age >2 SD below the normal representing chronic undernutrition or stunting
13
Source: ICF International, 2015. The DHS Program STATcompiler. Funded by USAID.
Figure 6: Correlation of open defecation density and chronic undernutrition of infants in South Asia. The graph shows open defecation density versus stunting (child height for age) versus number of open defecators using Demographic and Health Survey (DHS) data.
Civil Society Water, Sanitation and Hygiene Fund
14
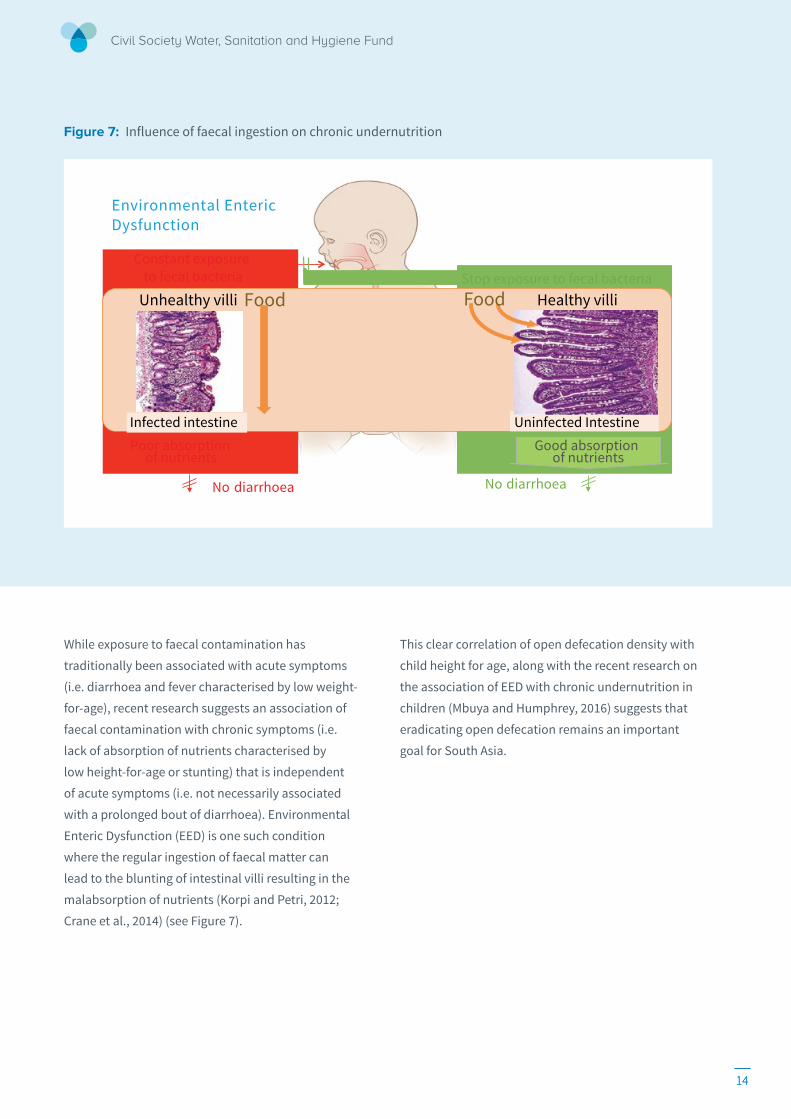
Figure 7: Influence of faecal ingestion on chronic undernutrition
Uninfected Intestine
Constant exposure to fecal bacteria
Food Healthy villi Food Unhealthy villi Stop exposure to fecal bacteria
No diarrhoea
No diarrhoea
Environmental Enteric Dysfunction
Significance of Faecal Ingestion on Undernutrition
Good absorption of nutrients
Infected intestine
Poor absorption of nutrients
While exposure to faecal contamination has
traditionally been associated with acute symptoms
(i.e. diarrhoea and fever characterised by low weight-
for-age), recent research suggests an association of
faecal contamination with chronic symptoms (i.e.
lack of absorption of nutrients characterised by
low height-for-age or stunting) that is independent
of acute symptoms (i.e. not necessarily associated
with a prolonged bout of diarrhoea). Environmental
Enteric Dysfunction (EED) is one such condition
where the regular ingestion of faecal matter can
lead to the blunting of intestinal villi resulting in the
malabsorption of nutrients (Korpi and Petri, 2012;
Crane et al., 2014) (see Figure 7).
This clear correlation of open defecation density with
child height for age, along with the recent research on
the association of EED with chronic undernutrition in
children (Mbuya and Humphrey, 2016) suggests that
eradicating open defecation remains an important
goal for South Asia.
14

15
District ODF ceremony in Jumla District. Photo credit: SNV Nepal
CHAPTER 4
Moving from ODF to safely managed sanitation for all
While some countries in South Asia
still have a significant problem with
open defecation, the challenge is
shifting to the quality of sanitary
containment. The scale, scope and
resources required to move beyond the
eradication of open defecation varies
significantly across the CS WASH Fund
countries in the South Asia Region (see
Figure 8). Countries with a higher Gross
Domestic Product (GDP) per capita
and smaller population have a greater
capacity to bear the financial costs
associated with higher quality sanitary
containment (WSP, 2013).5
Figure 8: Sanitation and economic status of CS WASH Fund countries in South Asia
Bangladesh 62,560,290
Bhutan 388,000
Nepal 15,358,140
Pakistan 67,731,840
Sri Lanka 1,080,600
0%
20%
40%
60%
80%
100%
0 1000 2000 3000 4000
% A
cces
s to
Impr
oved
San
itatio
n
GDP per capita (current US$)
# People without Improved Latrines JMP 2015
Improved facilities Shared facilities Other unimproved Open defecation
5 www.wsp.org/content/economic-impacts-sanitation
Source: World Bank Data Bank, WHO and UNICEF (2015) Drinking Water Supply and Sanitation Joint Monitoring Programme (JMP)

Civil Society Water, Sanitation and Hygiene Fund
16
Figure 5: Rural sanitation coverage in the South-East Asia at 2015 (WHO/UNICEF 2015)
TARGET 6.2
Language In proposed targets Normative interpretation
By 2030, achieve
access Implies facilities close to home that can be easily reached and used when needed
to adequate Implies a system which hygienically separates excreta from human contact as well as safe reuse/treatment of excreta in situ, or safe transport and treatment off-site
and equitable Implies progressive reduction and elimination of inequalities among population subgroups
sanitation The provision of facilities and services for safe management and disposal of human urine and faeces
and hygiene The conditions and practices that help maintain health and prevent spread of disease including handwashing, menstrual hygiene management and food hygiene
for all Suitable for use by men, women, girls and boys of all ages including people living with disabilities
and end open defecation
Excreta of adults or children are: deposited (directly or after being covered by a layer of earth) in the bush, a field, a beach, or other open area; discharged directly into a drainage channel, river, sea, or other water body; or are wrapped in temporary material and discarded
paying special attention to the needs of women and girls
Implies reducing the burden of water collection and enabling women and girls to manage sanitation and hygiene needs with dignity. Special attention should be given to the needs of women and girls in ‘high use’ settings such as schools and workplaces, and ‘high risk’ settings such as health care facilities and detention centres
and those in vulnerable situations
Implies attention to specific WASH needs found in ‘special cases’ including refugee camps, detention centres, mass gatherings and pilgrimages
Figure 9: SDG Target 6.2 definition.
The framing of the SDG for sanitation (Target 6.2)
helps to put the challenges of moving beyond ODF in
South Asia within a broader context. The specific SDG
sanitation targets and their interpretation are included
in Figure 9, and how these vary to the MDGs described
visually in Figure 10.
‘By 2030, achieve access to adequate and equitable sanitation and hygiene for all and end open defecation, paying special attention to the needs of women and girls and those in vulnerable situations.’ (UN Water, 2016)

17
Figure 10: Key shifts from the MDG to SDG definitions of sanitation access showing the move from MDG definitions (improved, shared, unimproved, OD) to SDG definitions (safely managed, basic, shared, unimproved, OD).
Sustainable Development Goals (SDGs)
Open defecation
Other unimproved
Basic
Safely managed
Shared
Millennium Development Goals (MDGs)
Eradicate all open defecation
Faecal sludge & menstrual hygiene management, handwashing & hygiene
Open defecation
Other unimproved
Shared
Improved
No targets for open defecation
Improved facilities are not necessarily safe
Shared facilities are not necessarily unsafe
Halving those
without access is
biased against
the hard to reach
(i.e. poor, disabled)
Target the universal access to sanitation
and the progressive elimination
of all inequalities
Add a ‘safely
managed’ category
Specifically, the SDGs have prioritised the eradication
of open defecation, where the MDGs did not have any
target for open defecation. In addition, the shift in the
SDGs towards universal access reflects the learning
that halving the numbers of those without access can
leave the poorest and most vulnerable behind. The
SDGs have therefore also prioritised the progressive
elimination of inequalities in all population sub-groups
and prioritised the needs of women and girls. A safely
managed category has also been introduced to ensure
that faecal waste from improved latrines is safely
emptied, transported, treated, disposed of and/or
re-used. Hygiene has also given priority to maintaining
health and stopping the spread of disease through
handwashing, food hygiene and menstrual hygiene
management practices
(WHO & UNICEF, 2015).
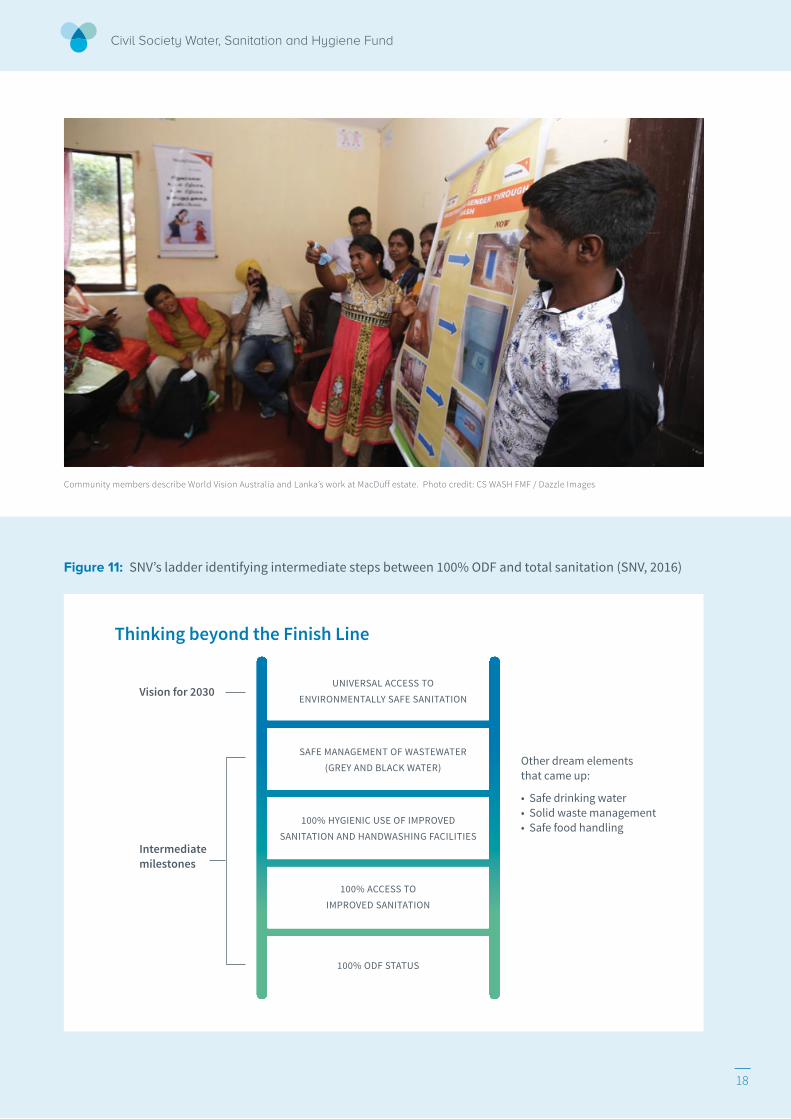
Moving beyond the eradication of open defecation
towards safely managed sanitation has been
conceptualised with a ladder progressing from lower-
cost sanitation options with lower health benefits to
higher-cost options with higher health benefits (see
Figure 11). SNV’s work in Nepal addresses the post-
ODF challenge of sustaining ODF on the sanitation
ladder, and they have prepared post ODF sustainability
tools and processes to assist with this (Regmi, 2016).
There has been a strong ODF movement in Nepal and
building on the momentum from this, there is growing
recognition of the need to avoid complacency by
targeting higher sanitary standards. To this end the
government and partners have drafted total sanitation
guidelines that also recognise the need to secure the
existing gains through processes designed to verify
and sustain ODF behaviours.
Civil Society Water, Sanitation and Hygiene Fund
18
Thinking beyond the Finish Line
Figure 11: SNV’s ladder identifying intermediate steps between 100% ODF and total sanitation (SNV, 2016)
100% ODF STATUS
100% ACCESS TO IMPROVED SANITATION
100% HYGIENIC USE OF IMPROVED SANITATION AND HANDWASHING FACILITIES
SAFE MANAGEMENT OF WASTEWATER (GREY AND BLACK WATER)
UNIVERSAL ACCESS TO ENVIRONMENTALLY SAFE SANITATION
Vision for 2030
Intermediate milestones
Other dream elementsthat came up:
• Safe drinking water• Solid waste management• Safe food handling
Community members describe World Vision Australia and Lanka’s work at MacDuff estate. Photo credit: CS WASH FMF / Dazzle Images

19 19
The notion of a sanitation ladder implies a shift in the
types of approaches deployed to move up the ladder. For
instance, the sanitation ladder developed by the World
Bank proposed that collective mobilisation approaches
such as CLTS were more effective in moving households
away from open defecation, while sanitation marketing
approaches were more effective in assisting households
to move up the sanitation ladder (WSP, 2012). SNV
described how they have been ‘thinking beyond the
finish line’ and engaging stakeholders in creating a
vision towards the SDG goals of universal access to safely
managed sanitation and seeing ODF as one of a series of
milestones. This approach requires ongoing engagement
in addressing the challenges that householders face
on the demand side in making informed choices when
purchasing latrines as well as addressing the supply side
challenges of providing appropriate technology options.
It also requires understanding the ‘last mile’ (i.e. what
is required to meet SDG Target 6.2), local leadership
and the public finance available to adequately
resource required activities. The sanitation ladder
developed by SNV (see Figure 12) proposes that the
shift from milestones related to improved sanitation to
safely managed systems will need to be accompanied
by a change in roles and responsibilities, including
regulation of compliance.
Figure 12: Sanitation ladder proposed by SNV to ensure health outcomes (SNV, 2016). Different milestones require different roles and responsibilities.
Open Defecation Free (ODF)
Total Sanitation
Healthy Village
Use of Improved Sanitation by All
- CLTS - Steering multi-stakeholder
coordination - Technical guidance - Informed Choice
- Supply Chain facilitation - Pro-poor strategies - Strategy for disabilities
- Solid waste management - Much stronger BCC - Drainage solutions
- Better sta�ed inspection
- Environmental standards and guidance
Thinking Beyond the Finish Line
Thinking beyond the Finish Line

Civil Society Water, Sanitation and Hygiene Fund
20 20
The generic representation of a
sanitation ladder and the changes in
approaches that the major steps imply
does not, however, give any sense of the
relative size of the different steps of the
ladder. To understand the relative scale
of the steps in the sanitation ladder,
and thus the scale of the challenge to
be addressed, a rural sanitation ladder
was developed using Joint Monitoring
Programme (JMP) data. By inverting
the MDG monitoring data for 2015 and
splitting the sanitation status into
sanitation ladder steps it was possible
to visualize the relative size of the steps
necessary to move up the sanitation
ladder in the five relevant countries
(see Figure 13).
Although this seems to suggest that
some countries in the region, such
as Sri Lanka, have almost completely
addressed the challenge of sanitary
containment, it is not true that
improved facilities are always operated
and maintained in a safe manner.
For this reason, the sanitation SDGs
have introduced an additional safely
managed target beyond the improved
sanitation target.
As communities move up the sanitation
ladder (see Figure 14), there is a greater
need for private sector involvement
(e.g. to supply improved latrines) as
well as public service provision (e.g.
handwashing and menstrual hygiene
management facilities in healthcare
centres and schools). There is a need
for public regulation of compliance to
sanitary codes, infrastructure standards,
sanitary behaviour, and clarity of
institutional roles and separation
at all steps of the ladder.
Figure 13: The three tables above show the three steps in developing a sanitation ladder in CS WASH Fund countries in South Asia based on JMP (WHO and UNICEF 2015) data.
Source: WHO and UNICEF (2015) Drinking Water Supply and Sanitation Joint Monitoring Programme (JMP)
32
4
18
46
0
20
40
60
80
100
2015
Cove
rage
(%)
Open defecation Other unimproved Shared facilities Improved facilities
10
28
61
2015
20
28
50
2015
13
14
9
64
2015
1 4
95
2015
Rural sanitation status upside down Nepal Bangladesh Bhutan Pakistan Sri-Lanka
46
18
4
32
0
20
40
60
80
100
2015
Cove
rage
(%
)
Improved facilities Shared facilities Other unimproved Open defecation
61
28
10 1
2015
50
28
20
2
2015
64
9
14
13
2015
95
4 1
2015
Rural sanitation status Nepal Bangladesh Bhutan Pakistan Sri-Lanka
32
4
18
46
0
20
40
60
80
100
Cove
rage
(%)
Open defecation Other unimproved Shared facilities Improved facilities
1 10
28
61
2
20
28
50
0 1 4
95
13
14
9
64
Rural sanitation status as a ladder Nepal Bangladesh Bhutan Sri-Lanka Pakistan
2 1
28

21 21
Mr Najeeb Aslam inspects a water meter at a tea plantation estate. Photo credit: CS WASH FMF / Dazzle Images
Basic
Safely managed
Health Benefits
Cost
s
Supply Chains - Appropriate technologies - Access to finance - Poor/disable inclusive - Gender equitable
Public Services - Fecal e�luent &
sludge management - Handwashing
facilities & hygiene behaviour
- Menstrual hygiene management
Public Regulation - Sanitary behaviour - Sanitary codes - Environmental standards - Quality tradespeople - Institutional separation
CLTS - Coordination - Behaviour Change - Informed Choice
Unimproved
Shared
Open Defecation
Adapted from: SNV (2016), Thinking Beyond the Finish Line: Sustainable Sanitation Services for All; Asia Regional Learning Event
Changing roles in response to the SDG sanitation ladder
Figure 14: Changing responses to the differing challenges presented by the SDG sanitation ladder. This illus-trates how with increasing complexity (increasing costs and health benefits) there is increasing private and public sector involvement.

Civil Society Water, Sanitation and Hygiene Fund
22
CHAPTER 5
What is safely managed sanitation?
To measure the achievement of SDG Target 6.2 an additional indicator of ‘safely managed sanitation’ has been added to the MDG monitoring of access to improved sanitation. The SDG 6.2 definition of ‘safely managed sanitation’ includes the safe management of faecal waste and the washing of hands with soap. This requires that all faecal waste is safely contained, transported and treated and that all of the risks of faecal exposure are managed in a safe manner.
Improving faecal waste management contributes to
other SDG6 targets, including reducing volumes of
untreated wastewater to improve water quality (6.3),
contributing to water-related ecosystem health (6.6)
and working towards Integrated Water Resources
Management by placing WASH in the broader water
cycle (6.5). Recognising these broader contributions
of safely managing sanitation, this section identifies
the challenges in achieving safely managed sanitation
as well as handwashing with soap and menstrual
hygiene management (MHM).
To measure the achievement of SDG Target 6.2 an
additional indicator of ‘safely managed sanitation’
has been added to the MDG monitoring of access to
improved sanitation. The SDG 6.2 definition of ‘safely
managed sanitation’ includes the safe management
of faecal waste and the washing of hands with soap.
This requires that all faecal waste is safely contained,
transported and treated and that all of the risks of
faecal exposure are managed in a safe manner.
Improving faecal waste management contributes to
other SDG6 targets, including reducing volumes of
untreated wastewater to improve water quality (6.3),
contributing to water-related ecosystem health (6.6)
and working towards Integrated Water Resources
Management by placing WASH in the broader water
cycle (6.5). Recognising these broader contributions
of safely managing sanitation, this section identifies
the challenges in achieving safely managed sanitation
as well as handwashing with soap and menstrual
hygiene management (MHM).
These young Bangladeshi masons have been trained to make concrete
latrine rings with support from Bangladesh Red Crescent Society/Australian
Red Cross. Photo credit: Bangladesh Red Crescent Society
22

23 23
5.1 Managing faecal waste
The inclusion of the faecal waste management
within the safely managed sanitation SDG requires
that sanitation facilities are not only safe but that
the disposal of the faecal sludge and effluent is also
safe. This not only requires the hygienic containment,
emptying, transport, treatment, disposal and re-use of
faecal sludge but it also demands greater understanding
of the faecal digestion process in order to know the
environmental and health risks associated with
different faecal containment options.
The use of anaerobic and aerobic digestion processes
in wastewater treatment plants have been extensively
studied and their application refined over time, however
the study of the anaerobic and aerobic digestion
processes within pit latrines and septic tanks has
been the subject of less attention. While there are well
defined parameters for what constitutes improved
latrines, safely managed sanitation requires assessing
the whole sanitation service chain and is yet to be
globally defined.6
The digestion of faecal sludge and effluent generally
comprises of both anaerobic (without air) and aerobic
(with air) processes. As anaerobic and aerobic bacteria
cannot co-exist in the same space and the transition
between these processes is vitally important to the
stability of faecal digestion.
Anaerobic digestion processes are more efficient
than aerobic processes in reducing the Biological
Oxygen Demand7 of faecal sludge and effluent (i.e. the
solid content including nitrogen and phosphorous).
Anaerobic digestion is efficient in reducing the
environmental loading of faecal sludge in addition to
reducing solids that hamper the aerobic digestion of
faecal effluent. Anaerobic processes are not as efficient
as aerobic processes in reducing pathogens that have
already survived the anaerobic processes within the
gut of humans and animals. Anaerobic chambers
only require a vent pipe if they aren’t connected to an
aerobic system allowing the gas pressure to build up to
a point where the latrine won’t flush.
Aerobic digestion processes are more efficient than
anaerobic processes in reducing the pathogen content
of faecal sludge and effluent (i.e. bacteria, viruses,
parasitic protozoa and helminths). Aerobic digestion
processes are most effective when solids have been
removed from faecal effluent, or when liquids have
been removed from faecal sludge. For this reason,
aerobic processes are most effective in reducing the
pathogens in clear faecal effluent or dry faecal sludge.
Safely managed faecal waste (as defined in the SDGs)
will generally require faecal sludge and effluent to be
exposed to both anaerobic and aerobic processes.
The exposure of faecal sludge and effluent to anaerobic
processes for reducing environmental health risks, and
aerobic processes for reducing public health risks, can
assist practitioners in understanding the point at which
sanitation can be considered to be ‘safely managed’.
The perceived safety of the faecal waste management
options based on the exposure to aerobic and
anaerobic processes to major sanitation technology
options in South Asia has been summarised in Figure
15 and further detailed in Annex 4.
During the South Asia RLE, country teams identified
the need to ensure that the contents of septic tanks
are subject to some form of aerobic process as a
major issue. In the short term the absence of leach
pits results in the release of faecal effluent with high
pathogen levels and in the long term this can lead to
a loss of retention time in septic tanks if they are not
pumped out periodically. This can result in both faecal
effluent and sludge being discharged directly into the
environment from septic tanks without any treatment.
6 The WHO Sanitation Safety Planning Toolkit (2015) provides guidelines on how to assess risk and manage sanitation waste treatment (WHO 2015). 7 Biological Oxygen Demand (BOD) is a measure of the amount of oxygen used by microorganisms to degrade organic matter over time (expressed in mg/L). A high
BOD can be caused by high levels of organic pollution or high nitrate levels.

Civil Society Water, Sanitation and Hygiene Fund
24 24
Given this risk, twin pit latrines may be a superior
option for the safe management of sanitation as
compared to septic tanks, particularly in rural areas
where equipment for safely emptying and treating
faecal sludge is difficult to access. Switching between
twin pit latrines can safely treat faecal sludge and
effluent to a point where pit contents are safe to
handle. Sealed septic tanks or pits will continue to be
more viable for high faecal loads (i.e. schools) or in high
water table areas.
In Bangladesh and other countries where direct
pit or single offset pit latrines are the common
rural sanitation solution, the handling of the faecal
sludge was identified as major area of risk. The safe
management of faecal sludge by sweepers8 and their
role in promoting the upgrade to technologies that
enable the safe management of faecal sludge was
also discussed. The experience of Welthungerhilfe
in developing desludging enterprises in small urban
centres in Zimbabwe was presented to illustrate the
issues in developing viable sludge enterprises. This
included the testing of the Technology Applicability
Framework (Potter et al., 2015) to assess the viability
of a proposed faecal sludge management approach
on six dimensions of sustainability (i.e. technological,
economic, social, environmental, institutional/legal,
skills/know how) from three different perspectives
(i.e. user/buyer, producer/provider, regulator/investor/
facilitator). The experience in the application of the
Technology Applicability Framework established that
this is a useful tool to guide discussion between users,
operators, authorities and regulators on the planning of
faecal sludge management operations.
The use of three rings can significantly reduce the costs of a septic tank for high loads
Aerobic Anaerobic
Septic Pits
Handle faecal sludge with care
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Fecal sludge is safe if dry
Water kills aerobic bacteria = unsafe
Anaerobic
Aerobic
Effluent Sludge
O�set Pit
Remove faecal sludge with care
Live pit is anaerobic so pathogen content is high
Sludge
Aerobic
Anaerobic
Twin O�set Pit
Faecal sludge is safe if le� for 1 year
Switched pit will shi� from anaerobic to aerobic
Anaerobic
Sludge
Direct Pit
Hard to empty faecal sludge
Superstructure makes it di�icult to empty
Aerobic Effluent
Rural Faecal Sludge Ladder Fecal sludge & faecal e�luent are most e�iciently digested by anaerobic + aerobic processes
Anaerobic digestion: is more e�icient in reducing solids (incl.nitrogen & phosphorous) Environmental Health Aerobic digestion: is more e�icient in reducing pathogens (i.e. fecal bacteria & viruses) Public Health
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank & Leach Pit
Handle faecal sludge with care • A septic tank without a leach pit will discharge both
fecal e�luent & sludge to drains • Septic tanks lose the retention time to treat
e�luent if they are not routinely pumped out
Effluent
Aerobic processes are e�ective when; - solids have been removed from liquids - liquids have been removed from solids
Anaerobic chambers only require a vent pipe if they aren’t linked to an aerobic process and if the latrine doesn’t flush
Incr
ease
d sa
fety
Increasing cost
Incr
ease
d sa
fety
Figure 15: Exposure to aerobic and anaerobic processes associated with different faecal waste management options
8 Sweepers are one of the lowest Hindu caste communities historically employed in the disposal of the solid and liquid waste.

25 25
Participants engaging in discussion during the field trip at the South Asia RLE. Photo credit: CS WASH FMF / Dazzle Images
Pour flush latrine. Photo credit: SNV Nepal
Civil Society Water, Sanitation and Hygiene Fund
26 26
The classification of safely managed sanitation
identified within the SDGs includes the provision of
handwashing facilities close to a latrine. The provision
of handwashing facilities in rural areas requires the
provision of sustainable access to soap or detergent,
water and drainage. The failure to secure access to
either water or soap or drainage fails to offer a safe
handwashing option for households.
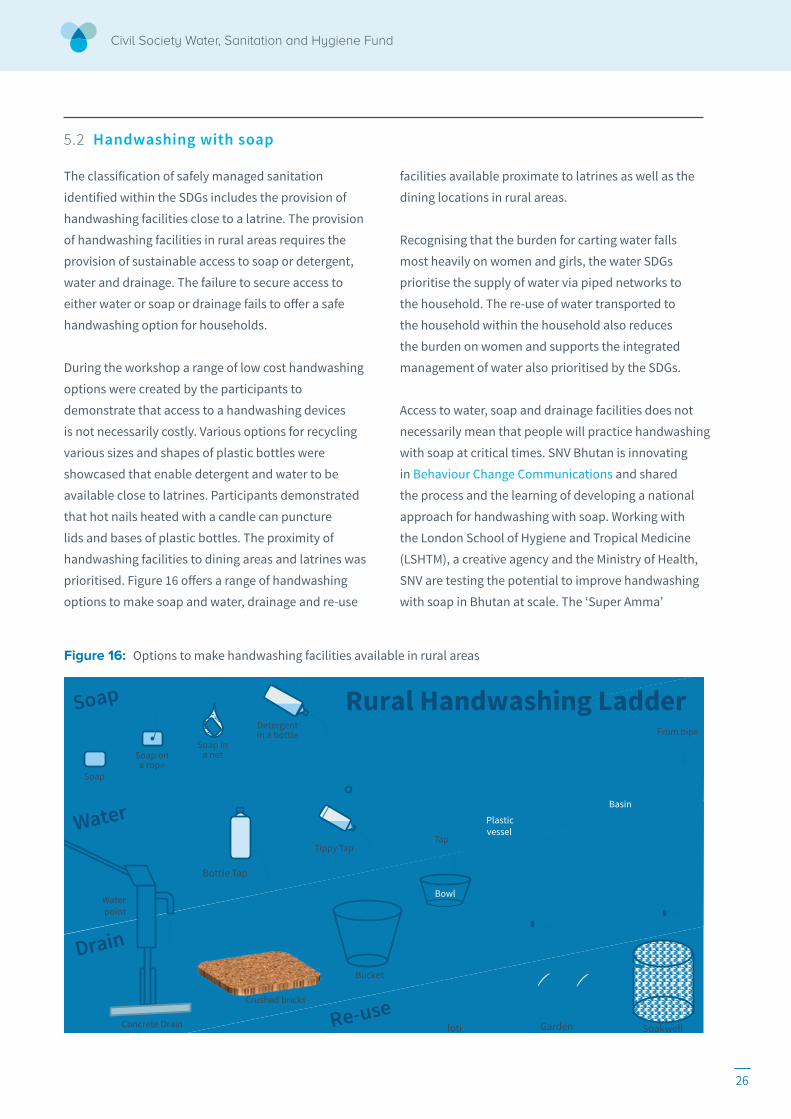
During the workshop a range of low cost handwashing
options were created by the participants to
demonstrate that access to a handwashing devices
is not necessarily costly. Various options for recycling
various sizes and shapes of plastic bottles were
showcased that enable detergent and water to be
available close to latrines. Participants demonstrated
that hot nails heated with a candle can puncture
lids and bases of plastic bottles. The proximity of
handwashing facilities to dining areas and latrines was
prioritised. Figure 16 offers a range of handwashing
options to make soap and water, drainage and re-use
facilities available proximate to latrines as well as the
dining locations in rural areas.
Recognising that the burden for carting water falls
most heavily on women and girls, the water SDGs
prioritise the supply of water via piped networks to
the household. The re-use of water transported to
the household within the household also reduces
the burden on women and supports the integrated
management of water also prioritised by the SDGs.
Access to water, soap and drainage facilities does not
necessarily mean that people will practice handwashing
with soap at critical times. SNV Bhutan is innovating
in Behaviour Change Communications and shared
the process and the learning of developing a national
approach for handwashing with soap. Working with
the London School of Hygiene and Tropical Medicine
(LSHTM), a creative agency and the Ministry of Health,
SNV are testing the potential to improve handwashing
with soap in Bhutan at scale. The ‘Super Amma’
Figure 16: Options to make handwashing facilities available in rural areas
5.2 Handwashing with soap
Drain
Soap
Soap on a rope
Soap in a net
Detergent in a bottle
Bottle Tap
Tippy Tap
Soap
Water
Concrete Drain
Water point
Crushed bricks
Bucket
Tap
Bowl
Plastic vessel
Rural Handwashing Ladder From pipe
Basin
Garden Soakwell loti Re-use
27 27
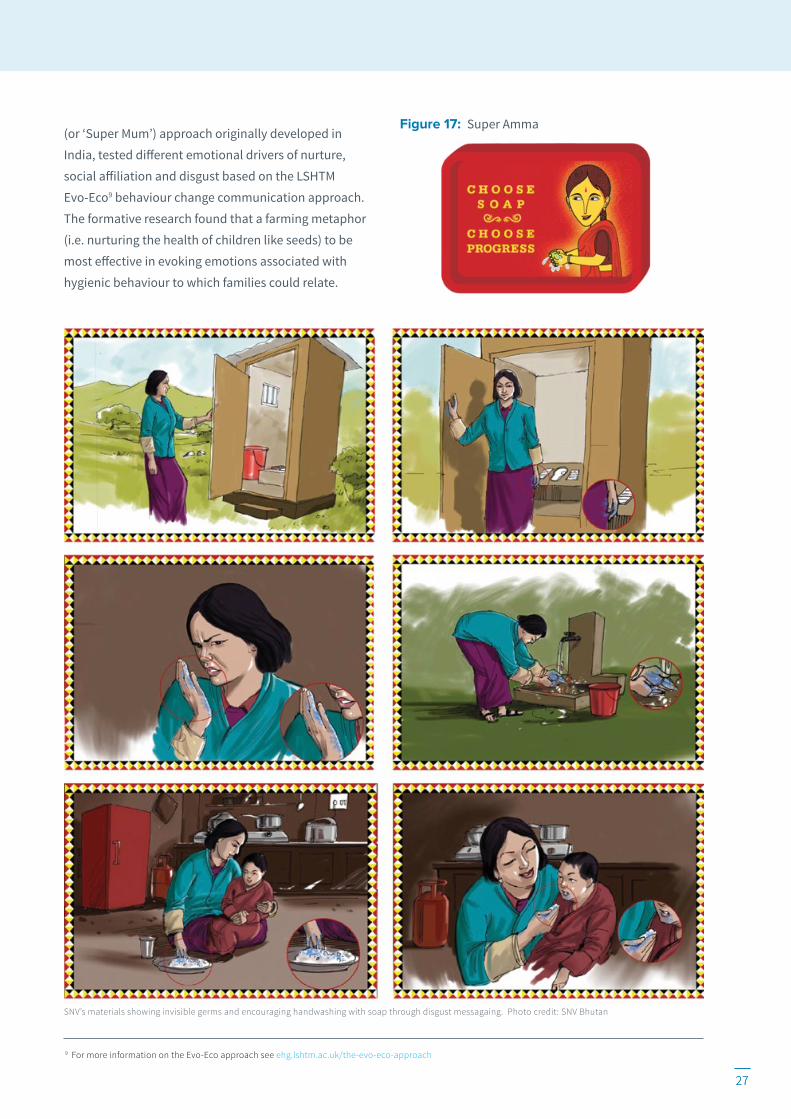
(or ‘Super Mum’) approach originally developed in
India, tested different emotional drivers of nurture,
social affiliation and disgust based on the LSHTM
Evo-Eco9 behaviour change communication approach.
The formative research found that a farming metaphor
(i.e. nurturing the health of children like seeds) to be
most effective in evoking emotions associated with
hygienic behaviour to which families could relate.
Figure 17: Super Amma
9 For more information on the Evo-Eco approach see ehg.lshtm.ac.uk/the-evo-eco-approach
SNV’s materials showing invisible germs and encouraging handwashing with soap through disgust messagaing. Photo credit: SNV Bhutan

Civil Society Water, Sanitation and Hygiene Fund
28
MHM impacts on women and girls’ health, right to
work, education and ability to engage in society.
The explicit mention in SDG Target 6.2 of the need for
access to sanitation for women and girls to manage
sanitation and hygiene needs with dignity implies,
amongst other things, the safe management of
menstrual hygiene. This requires sanitation facilities
to have the provisions that potentially enable:
• changing (i.e. space for changing menstrual
products within the latrine facility)
• washing (i.e. water and soap for changing
and washing oneself and the cleaning of
menstrual rags)
• drying (i.e. a place for drying of menstrual rags)
• storage (i.e. a place for keeping spare emergency
menstrual products)
• disposal (i.e. a means for disposing of used
menstrual products)
SNV’s work in MHM has highlighted the catalytic role
played by various communication strategies aimed
at ‘breaking the silence,’ which often surrounds this
taboo issue. SNV’s work on integrating MHM within
ongoing country programmes in Asia as part of SSH4A
and five countries in Africa as part of the Girls in
Control projects has aimed to strengthen demand
(through behaviour change communication) and
supply (through supply chain interventions) as well as
working to advocate for and to improve governance
and enabling environments for MHM. SNV found that
underdeveloped supply chains were challenged to
meet consumer preferences for menstrual products in
rural areas and impacted by subsidy practices. Linking
various actors from health, education, WASH, women
and economic empowerment at the district and
national level to bring different activities to bear on
menstrual hygiene matters was considered essential
to breaking the silence.
5.3 Menstrual Hygiene Management
Learning event participants reflected similar
experiences to those of SNV, identifying a range of
issues for girls both ‘in’ and ‘out’ of school, and women
in workplaces. Participants identified particular action
points that included advocacy for a government
budget line for MHM (i.e. specific budget allocations
for improving menstrual hygiene), advocacy against
white secondary school girl’s uniforms and advocacy
for waste bins in toilet facilities to prevent blockages
associated with flushing menstrual pads down toilets.
The strong taboos around menstruation lead to
inadequate menstrual hygiene facilities. Additionally,
the re-use of unclean or damp rags is a significant
health issue for adolescent girls and women in
Bangladesh. HfH Bangladesh is working on MHM in
schools, and has activated School Hygiene Groups
(teachers and selected students) as change agents
responsible for delivering hygiene messaging in
schools. The provision of facilities for changing and
disposing of menstrual hygiene products within
adolescent female facilities is complemented by
increased hygiene awareness.

29
CHAPTER 6
Ensuring equitable sanitation for all
In moving beyond ODF to safely managed sanitation,
it is important to ascertain what systems need to be
retained, upgraded or changed. One important lesson
from the success in eradicating open defecation is that
an area that is ODF provides a pure public good (i.e. it
is both non-rival and non-excludable). It is non-rival
because one person enjoying an ODF area does not
reduce the availability for anyone else to enjoy. It is
non-excludable because it is not possible to include
some while excluding others from the benefits of an
ODF area. The provision of public goods are the raison
d’être of government.
Almost all of the other aspects of sanitation are private
goods (i.e. they are rival and excludable). Latrines
and sewers, masons and pit emptiers are rival and
excludable. Rival, because one person using a toilet or
a sewer, a mason or a pit emptier means that there is
less for others to use. Excludable because one can be
excluded access while others use that good. Private
goods are most efficiently dealt with by market forces,
irrespective of whether the front-end provider is public
or private.
6.1 Government roles and financing
Sanitation entrepreneur in Punjab Pakistan. Photo credit: Plan Pakistan
Civil Society Water, Sanitation and Hygiene Fund
30
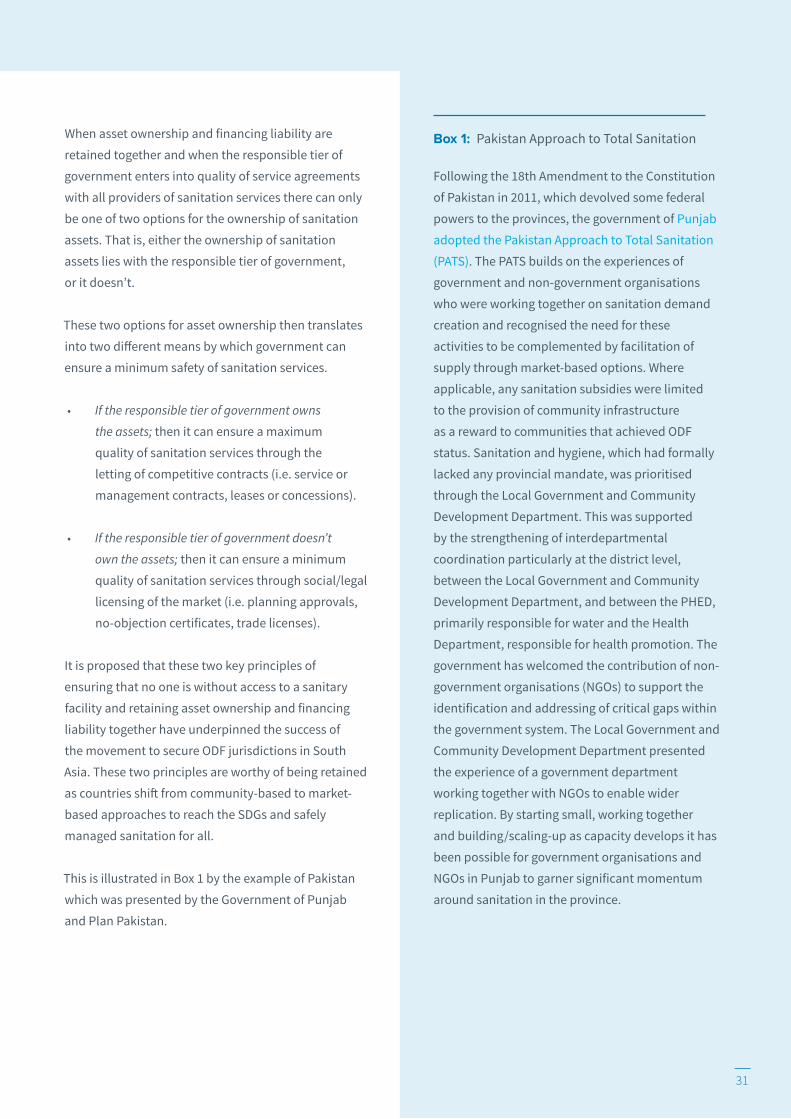
This delineation of public versus private goods through
CLTS supports the understanding that a primary role of
government is to ensure that no one (including future
generations) is excluded from a safe sanitation service.
This is separate from and above the role of providers
(public and private, community and household) that
deliver services to the underserved. This distinction is
particularly important for government as it typically
plays both roles (see Figure 18).
In the same way that local governments have
established certified ODF jurisdictions by deploying
social instruments preventing citizens from practising
open defecation, local governments can also deploy
legal instruments to ensure that the sanitary facilities
in all households, public buildings and utilities are
safely managed. This is most efficiently pursued
by government entering into quality of service
agreements with all of the providers of sanitation
services (i.e. public and/or private, community and/or
household providers) within their jurisdiction.
Another lesson from the CLTS approach to eradicating
open defecation is the notion that household latrines
should not be subsidised (Kar and Paster, 2005). While
there are instances where subsidies for sanitation can
be effective, the risk of creating perverse incentives
suggests that such subsidies need to be approached
with caution. Although a ‘no subsidy’ mantra
promoted by CLTS is oversimplified it was effective in
maintaining an important principle of retaining asset
ownership and financing liability together.
Provision of an ‘open defecation free’ jurisdiction
Non-Rival + Non-excludable
Public Good Government
Provision of latrines,
masons, sewers & emptiers
Rival + Excludable
Private Good
Market Forces
Public and Private Sanitation Goods Separate the primary role of government of ensuring that no-one is excluded from a minimum sanitation service above all of the agents (including government agents) that provide services to the underserved
Figure 18: CLTS untangling of public and private goods
Mr Najeeb Aslam from the Government of Punjab, Pakistan, is welcomed with a wreath in Central Province, Sri Lanka. Photo credit: CS WASH FMF / Dazzle Images
31
When asset ownership and financing liability are
retained together and when the responsible tier of
government enters into quality of service agreements
with all providers of sanitation services there can only
be one of two options for the ownership of sanitation
assets. That is, either the ownership of sanitation
assets lies with the responsible tier of government,
or it doesn’t.
These two options for asset ownership then translates
into two different means by which government can
ensure a minimum safety of sanitation services.
• If the responsible tier of government owns
the assets; then it can ensure a maximum
quality of sanitation services through the
letting of competitive contracts (i.e. service or
management contracts, leases or concessions).
• If the responsible tier of government doesn’t
own the assets; then it can ensure a minimum
quality of sanitation services through social/legal
licensing of the market (i.e. planning approvals,
no-objection certificates, trade licenses).
It is proposed that these two key principles of
ensuring that no one is without access to a sanitary
facility and retaining asset ownership and financing
liability together have underpinned the success of
the movement to secure ODF jurisdictions in South
Asia. These two principles are worthy of being retained
as countries shift from community-based to market-
based approaches to reach the SDGs and safely
managed sanitation for all.
This is illustrated in Box 1 by the example of Pakistan
which was presented by the Government of Punjab
and Plan Pakistan.
Following the 18th Amendment to the Constitution
of Pakistan in 2011, which devolved some federal
powers to the provinces, the government of Punjab
adopted the Pakistan Approach to Total Sanitation
(PATS). The PATS builds on the experiences of
government and non-government organisations
who were working together on sanitation demand
creation and recognised the need for these
activities to be complemented by facilitation of
supply through market-based options. Where
applicable, any sanitation subsidies were limited
to the provision of community infrastructure
as a reward to communities that achieved ODF
status. Sanitation and hygiene, which had formally
lacked any provincial mandate, was prioritised
through the Local Government and Community
Development Department. This was supported
by the strengthening of interdepartmental
coordination particularly at the district level,
between the Local Government and Community
Development Department, and between the PHED,
primarily responsible for water and the Health
Department, responsible for health promotion. The
government has welcomed the contribution of non-
government organisations (NGOs) to support the
identification and addressing of critical gaps within
the government system. The Local Government and
Community Development Department presented
the experience of a government department
working together with NGOs to enable wider
replication. By starting small, working together
and building/scaling-up as capacity develops it has
been possible for government organisations and
NGOs in Punjab to garner significant momentum
around sanitation in the province.
Box 1: Pakistan Approach to Total Sanitation
31

Civil Society Water, Sanitation and Hygiene Fund
32
In Bangladesh, less than one percent of the population
is now practicing open defecation but only 61%
of the population uses an improved facility. The
leading sanitation challenge for Bangladesh is thus
to improve the quality of latrine facilities. Moving
from a basic latrine to an improved latrine is most
efficiently supported by market instruments when the
requisite technologies and their compliance, finance
and affordability are readily available. In seeking to
address some of these bottlenecks in the markets for
sanitation in Bangladesh, HfH and the Bangladesh
Red Crescent Society (BDRCS, with iDE) showcased
their projects with sanitation markets to reach the
‘ultra-poor’ in Bangladesh. Where HfH have supported
financing via the introduction of a revolving fund
managed by CBOs, BDRCS and iDE have supported
a financing system via vouchers and access to
micro-finance institutions (MFIs).
Habitat for Humanity is supporting the training of
sanitation entrepreneurs on the supply of hygienic
latrine options and community WASH committees to
raise demand and enable access to finance for their
members through the establishment of a revolving
sanitation fund. On the other hand, iDE and BDRCS
have a project approach of providing vouchers
to ‘ultra-poor’ households to access a discount on
the sanitation options offered by various trained
sanitation entrepreneurs. As the vouchers can be
claimed from any sanitation entrepreneurs, the
onus remains on the entrepreneurs to market their
sanitation products. The next step of the project
is to seek to replace the vouchers with loans from
micro-finance institutions.
Plan International Pakistan is similarly supporting
market-side sanitation as Pakistan has transitioned
from a context of low demand to high demand
for sanitation. Plan’s experience highlighted the
importance of timing in the staging of support for
demand creation before extending support in the
supply of sanitation technologies and finance. In the
Pakistan context, a wide range of affordable sanitation
options and the diversification of local service
provision fostered greater viability in the provision
of sanitary products. In the future, Plan is seeking to
ensure the availability of comprehensive business
support to sanitation entrepreneurs (i.e. counselling,
market linkages, finance, banking and market
solutions).
6.2 Sanitation marketing
Demostrating handwashing methods in Kalikot District. Photo credit: SNV Nepal

33
6.3 Disability inclusive WASH
World Vision Lanka has partnered with The Northern
Province Consortium of Organisations for Differently
Abled (NPCODA) for the delivery of its WASH work
in Jaffna, Sri Lanka to strengthen disability inclusive
WASH. They highlighted the following barriers that
inhibit WASH access for the differently abled10 during
their presentation at the learning event:
• Physical: rough pathways, steps, narrow
doorways, insufficient room, no handle, facilities
too low or high, etc.
• Attitudinal: within communities (i.e. ‘they don’t
need to collect water – someone else will do it
for them’, ‘they shouldn’t collect water – they are
unclean’) and within implementing NGOs and
partners (i.e. ‘we don’t ‘do’ disability’ or ‘it is too
hard’).
• Communication: can’t find the toilet/water
point, can’t read/access hygiene promotion
materials, can’t participate in community
planning.
• Institutional and Policy barriers: lack of
funding for accessible/universal design, building
codes don’t consider universal accessibility, no
accessibility requirement in public places.
While there are now national regulations and Ministry
of Health guidelines for universal accessible latrines in
Sri Lanka, local governments and contractors were still
largely unaware of these requirements.
6.4 Reaching women and girls and the underserved
The impact of WASH on the lives of women and
girls is immense as women predominantly carry
the household burden for water-related tasks yet
are excluded from decision-making forums. Many
Fund projects already include a strong gender focus
including the South Asia projects as illustrated by the
IRC project in Pakistan.
In Khyber Pakhtunkhwa, Pakistan, the role of women
in decision-making is hampered by a conservative
religious culture, male dominance, a lack of education,
a lack of confidence and disagreement about the role
of women in society. In this situation where women
and men are unable to meet together, discussions
must take place separately for men and for women.
IRC undertook a study to ascertain the impact that
improved tools and approaches on women’s decision-
making had on securing their priorities in approved
local development plans. IRC’s work translating
gender-disaggregated environmental health needs
into village decision-making analysed gender
segregated planning to assess the extent to which
men’s and women’s priorities were included
in planning.
10 The UN Convention on the Rights of Persons with Disabilities defines: “Persons with disabilities include those who have long-term physical,
mental, intellectual, or sensory impairments which in interaction with various barriers may hinder their full and effective participation in
society on an equal basis with others.” (Article 1)

Civil Society Water, Sanitation and Hygiene Fund
34
The multiple challenges that such cultural norms raise
were discussed, where even the recruiting of female
staff to facilitate local planning processes is extremely
difficult. This requires the project to recruit paired
male and female activists (brother and sister, husband
and wife, etc.) to find women who are able to spend
time working with women’s groups (i.e. able to spend
time away from their family or able to gain permission
from their husband). By being respectful of local
customs and blending these with the project priorities,
IRC has been able to improve local government
planning processes sufficiently to improve the extent
to which they are able to incorporate the priorities of
women in a context where women are generally not
permitted to meet with men outside of their family.
World Vision Lanka is also working to improve the
lives of women workers and their families in the hard
to reach and underserved communities of tea workers
(see Box 2).11
Have you ever wondered who picked the tea leaves in your morning brew? The first thing to know about
your morning brew, especially if it is mixed with Sri
Lankan premium blend, is that it was picked by a
woman on high, steep muddy slopes on an isolated
tea estate many hours from a town. During the day she
works in the field with no access to a toilet, and at the
end of the day carries anywhere between 10-15kg of
leaves on her head back home, to a home that more
than likely also doesn’t have a toilet.
Participants of the South Asia RLE visited Sri Lankan
tea estates on a field trip hosted by WV Lanka. Until
recently many tea workers did not have the most
basic of services, including toilets and access to
water. In these elevated green mountainous areas of
the Central Province, the local people are Sri Lankan
and, after a long history of colonial intervention from
the Portuguese and Dutch, finally succumbed to the
British in 1815. The proud people refused to work as
labourers on the tea estates. With a booming demand
for tea and plants to be picked, the British brought
over Tamils as indentured labourers from India in the
early 1800s. Generations have now grown up, married,
raised families, and died, on the tea estates, which still
bear their colonial masters names such as MacDuff, St
Clair and Mayfield Estates.
Plantation workers rely on the tea estate companies
for their wages, housing and public services including
water and sanitation, schooling and healthcare.
While these workers have been reliant on plantation
companies ‘from the womb to the tomb’, their rights
have been gradually recognised over time. From 1988
they received Sri Lankan citizenship and recently
received an increase in their daily wage from Rs. 700 to
Rs. 1,000 per day. The government and tea plantation
companies have also started enabling the workers to
own the houses and land on which they live.
Sophia Cooke and Towfika Khatun from Habitat for Humanity.
Photo credit: CS WASH FMF / Dazzle Images
11 Note that the project activities described in Box 2 are not
CS WASH Fund projects.
Box 2: Toilets and jobs: tea workers in Sri Lanka
34

35
The low standard of sanitation and water facilities in the tea workers residences is in stark contrast to the generally high quality of water and sanitation services throughout Sri Lanka. WV Lanka has
worked with tea plantations in Nuwara Eliya District
to improve the WASH conditions of plantation
workers. This work was completed as part of the Rural
Integrated Water, Sanitation and Hygiene (RIWASH)
initiative supported by the Australia Government and
implemented by WV Lanka between 2010 and 2013.
The project provided WASH facilities to over 23,000
people – including 7,500 school children – spread over
a number estates, schools and rural villages. Visits to
the sites where WV Lanka has been working with tea
plantation owners and local governments to improve
the water and sanitation facilities for tea estate
workers included:
1. MacDuff estate where WV Lanka provided
subsidised household toilets attached to
each household, and connected to a central
treatment filtration system. This filtration
system discharged treated effluent to a wetland
downstream of the village.
2. Lindula estate where WV Lanka negotiated land
allocation from the estate to build integrated
housing for families with children. Through a
grant from WV Lanka and the support of the tea
estate, families enter an agreement to pay off
the financing gap through their salaries over a
period of ten years at which point they will own
their house and the land. Sanitation and water
is built into the house design with a pour-flush
toilet connected to a leach pit the location and
design of which were approved by the local
municipal government sanitary inspectors.
WV Lanka has started tackling the challenge of water, sanitation and housing rights for estate workers crucially opening the dialogue between estates, workers and local governments. While
Lanka is using advocacy and cost-sharing mechanisms
to leverage WASH service improvements for tea estate
workers, the scale of the challenge is well beyond
their resources. As the plantations are state owned,
but operated by companies, individual owners or
cooperatives, the responsibilities to safeguard the
rights of the workers are complicated. While the local
government act requires tea estates to meet water
and sanitation quality for workers, and while some tea
buyers require estates to meet environmental health
standards (including housing standards for workers),
the reality is that the water and sanitation rights of tea
estate workers have not been guaranteed. WV Lanka
is seeking to bring options to the table to highlight an
urgent need among this underserved group.
Left: Water tank – part of a community-managed water scheme. Right: Clarence Sutharsan, Program Manager, World Vision Lanka explains a centralised
community multi-chamber treatment to learning event participants at MacDuff Estate. Photo credit: CS WASH FMF / Dazzle Images
35

Civil Society Water, Sanitation and Hygiene Fund
36
CHAPTER 7
Priority SDG sanitation responses in South Asian countries
This chapter summarises the results of country-focused sanitation analyses and planning activities and presents the outcomes of group discussions, agreed priorities and issues and potential future actions. During the whole-day workshop at the South Asia RLE, country-based groups assessed their country’s sanitation context in light of SDG6 and considered what is needed to work towards safely managed sanitation.
Led by the Topic Expert Mark Ellery, teams utilised
a range of tools to identify the major sanitation
bottlenecks within their country contexts, identify
priority sanitation targets and develop scenarios for
how these could be addressed to meet the sanitation
SDGs. The country profiles described here have applied
the bottleneck analysis to estimate the size of the steps
of the safely managed component of the sanitation
ladder.12
Hand washing in Rolpa, Nepal – with plate drying rack, water bucket and waste collection pit present. Photo credit: SNV Nepal
12 A more detailed description of the analysis for the five CS WASH Fund countries are available online.

37
For rural Bangladesh, addressing the risks of
faecal sludge management associated with the high
percentage of direct pit latrines, could be improved if
union parishads are supported to issue a quality mark
to sweepers and masons that have been trained in the
safe management of faecal sludge and the upgrading
of latrines from direct pit to offset pit. The upgrade
to an offset pit latrine offers the opportunity to
introduce the functionality for safe changing, washing
and drying (or disposing) of menstrual pads and the
washing of hands with soap in addition to the safe
emptying of faecal sludge from pits.
In rural Nepal, there is both a need and an opportunity
to fill the void left by the success of the movement
to eradicate open defecation. With a shift of targets
to secure total sanitation, it will be incumbent on
Village Development Committees (VDCs) to monitor
this achievement. This can be achieved through the
passage of by-laws requiring households to comply
with total sanitation standards. Given the high rates of
chronic undernutrition, VDCs could also pass by-laws
requiring the registration of births and monitoring
of growth of all children, thus measuring any
improvement to child stunting.
In rural Pakistan, where cultural patriarchy and
religious fundamentalism reduce the ability of
women to engage in planning processes, the greatest
bottleneck in reaching the sanitation SDG is most
likely going to be the access to hygienic menstrual
management facilities in rural areas. With the
assignment of the responsibility for sanitation service
provision to union (and village) councils, councils
could ensure the provision of facilities for women
through by-laws making it mandatory for households
to install latrines and bathing facilities. The provision
of facilities for women to dispose of sanitary napkins
should be an essential planning approval requirement
for all places of work and restaurants, all public
buildings and secondary schools attended by girls.
Raising the issue of MHM through local legislation
could also contribute to ‘breaking the silence’ through
Figure 19: Bangladesh rural SDG sanitation ladder
Figure 20: Nepal rural SDG sanitation ladder
Figure 21: Pakistan rural SDG sanitation ladder
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. soap for hands)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
21
18
106
10
2015
33
1 1
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
1 14
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
Pakistan
Other unimproved
Opendefecation
BasicfacilitiesShared
facilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
0 0 3
19
2015
16
16
Sri Lanka
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
37
713
8
22
2015
11
Nepal
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
431
32
26
2015
3
Bhutan
Bangladesh
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities0
20
40
60
80
100
Cove
rage
(%)
2 7
28
9
2015
8
16
31
1
25
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
1 2
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. soap for hands)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
21
18
106
10
2015
33
1 1
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
1 14
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
Pakistan
Other unimproved
Opendefecation
BasicfacilitiesShared
facilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
0 0 3
19
2015
16
16
Sri Lanka
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
37
713
8
22
2015
11
Nepal
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
431
32
26
2015
3
Bhutan
Bangladesh
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities0
20
40
60
80
100 Co
vera
ge (%
)
2 7
28
9
2015
8
16
31
1
25
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
1 2
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. soap for hands)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
21
18
106
10
2015
33
1 1
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
1 14
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
Pakistan
Other unimproved
Opendefecation
BasicfacilitiesShared
facilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
0 0 3
19
2015
16
16
Sri Lanka
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
37
713
8
22
2015
11
Nepal
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
431
32
26
2015
3
Bhutan
Bangladesh
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities0
20
40
60
80
100
Cove
rage
(%)
2 7
28
9
2015
8
16
31
1
25
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
1 2

Civil Society Water, Sanitation and Hygiene Fund
38
official channels that are potentially less subject to
cultural restrictions.
In rural Bhutan, where open defecation rates are
low and access to water and sanitation facilities are
relatively high, the prevalence of diarrhoea and the
incidence of stunting are still unacceptably high. In
addition to targets to secure 100% access to basic
sanitation facilities there is a growing recognition of
the need to improve hygiene behaviours to secure
health benefits for all. The responsibility of the
Gewog (elected rural village government) for ensuring
sanitation service provision could be strengthened
through the drafting of national model by-laws on
handwashing and hygiene. These by-laws could then
be amended by Gewogs according to their context
with the goal of making access to handwashing and
hygiene facilities a necessity for all households and
restaurants.
In rural Sri Lanka, to address the unsafe containment
of faecal effluent and sludge the central government
may update the building code to include leach pits
with septic tanks and draft model sanitation by-laws
for local governments to ensure that this code is
applied. This would involve the pradeshiya sabha
council (local authority) passing the sanitation by-law
and licensing the compliance of all sanitation facilities
(i.e. through planning approvals and No Objection
Certificates) and sanitation providers (i.e. trade
licenses against certificate of competence of masons,
plumbers and sweepers).
Figure 22: Bhutan rural SDG sanitation ladder
Figure 23: Sri Lanka rural SDG sanitation ladder
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. soap for hands)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
21
18
106
10
2015
33
1 1
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
1 14
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
Pakistan
Other unimproved
Opendefecation
BasicfacilitiesShared
facilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
0 0 3
19
2015
16
16
Sri Lanka
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
37
713
8
22
2015
11
Nepal
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
431
32
26
2015
3
Bhutan
Bangladesh
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities0
20
40
60
80
100
Cove
rage
(%)
2 7
28
9
2015
8
16
31
1
25
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
1 2
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. soap for hands)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
21
18
106
10
2015
33
1 1
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
1 14
Safe (wrt. fecal
sludge)Safe
(wrt. fecale�luent)
12
Pakistan
Other unimproved
Opendefecation
BasicfacilitiesShared
facilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
0
20
40
60
80
100
Cove
rage
(%)
0 0 3
19
2015
16
16
Sri Lanka
Other unimproved
Opendefecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
37
713
8
22
2015
11
Nepal
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities
Safe (wrt. mentrual
hygiene)
Safe (wrt. soap for hands)
0
20
40
60
80
100
Cove
rage
(%)
431
32
26
2015
3
Bhutan
Bangladesh
Other unimprovedOpen
defecation
Basicfacilities
Sharedfacilities0
20
40
60
80
100
Cove
rage
(%)
2 7
28
9
2015
8
16
31
1
25
Safe (wrt. mentrual
hygiene)
Safe (wrt. fecal
sludge)
Safe (wrt. fecale�luent)
1 2

39
CHAPTER 8
Conclusion
The South Asia RLE enabled participants to reach
a new level of understanding in regards to the key
topic of moving beyond ODF to the SDGs and safely
managed sanitation for all. CSOs with differing
approaches had the opportunity to discuss and
debate the pros and cons of these approaches, such
that all participants could reach a more informed
understanding. Participants also left with a renewed
appreciation of the differing contexts within South
Asia in regards to the current status of progress in
sanitation and the challenges associated with meeting
the SDG targets for sanitation. From the strategy
context mapping exercises, the participants gained a
greater understanding of the role that the CSO projects
are already playing in respect to the context of the
current status of the country in the sanitation sector.
Participants also left with a greater understanding of
the potential instruments that could be deployed by
governments to assist countries to move beyond ODF
and towards the SDGs and safely managed sanitation
for all.
The statement from one participant in the concluding
session of the workshop indicated that the primary
goal of the workshop of moving beyond ODF toward
ensure safely managed sanitation for all had aligned
with the Fund’s primary goal of strengthening the
institutions of service delivery. “In many instances, the
laws and regulations that can support us to deliver on
our own WASH interests and desired outcomes already
exist and there’s something about us understanding
what those are and working with them, rather than
thinking about they don’t exist.”
Understanding the country context and strengthening
the licensing instruments already assigned to local
government institutions is central to enabling
countries to move up the sanitation ladder to ensure
safely managed sanitation for all. After attending the
South Asia RLE, CSO staff and partners returned to their
projects equipped with a more in-depth understanding
of the challenge set by SDG Target 6.2, priority issues
for their country and actions on how to tackle these.
World Vision Lanka presenting on Plantation Sanitation Model . Photo credit: CS WASH FMF / Dazzle Images

Civil Society Water, Sanitation and Hygiene Fund
40
ANNEX 1
References
Crane, R.J. et al. (2014) Environmental enteric dysfunction: An overview, Community-based Management of Acute Malnutrition (CMAM) Forum. www.ncbi.nlm.nih.gov/pmc/articles/PMC4472379
Hanchett, S. et al. (2011) Long-Term Sustainability of Improved Sanitation in Rural Bangladesh, WSP World Bank. www.wsp.org/sites/wsp.org/files/publications/WSP-Sustainability-Sanitation-Bangladesh-Report.pdf
Kar, K. and Pasteur, K. (2005) Subsidy or self-respect? Community Led Total Sanitation – An update on recent developments, IDS Working Paper 257, Institute for Development Studies. www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/ wp257_0.pdf
Kar, K. and Chambers, R. (2008) Handbook on Community Led Total Sanitation (CLTS), Plan UK and the Institute for Development Studies at the University of Sussex. www.communityledtotalsanitation.org/page/clts-approach
Korpe, P.S. and Petri, W. A. Jr. (2012) Environmental enteropathy: critical implications of a poorly understood condition. Trends in Molecular Medicine June; 18(6): 328-36.
Mbuya, M. N. and Humphrey, J. H. (2016) Preventing environmental enteric dysfunction through improved water, sanitation and hygiene: an opportunity for stunting reduction in developing countries, Maternal Child Nutrition. www.ncbi.nlm.nih.gov/pubmed/26542185
Potter, A., Nothomb, C. and Tuffuor, B. (2015) Technology Applicability Framework (TAF) questions: mobile desludging units. IRC: The Hague, Netherlands. www.ircwash.org/resources/technology-applicability-framework-taf-questions-mobile-desludging-units
Regmi, A. (2016) Tools for embedding post-ODF sustainability: experiences from Nepal. In Bongartz, P., Vernon, N. and Fox, J. Sustainable Sanitation for All. Warwickshire: International Development Studies, CLTS Knowledge Hub. dx.doi.org/10.3362/9781780449272.000
SNV (2016) Thinking Beyond the Finish Line: Sustainable Sanitation Services for All; Asia Regional Learning Event. www.cswashfund.org/shared-resources/references/thinking-beyond-finish-line-sustainable-sanitation-services-all
Spears, D. (2013) How much international variation in child height can sanitation explain? Policy Research Working Paper 6351, World Bank. elibrary.worldbank.org/doi/abs/10.1596/1813-9450-6351
UN Water, The United Nations Inter-Agency Mechanism on all Freshwater related issues, including sanitation. www.unwater.org/sdgs/from-mdgs-to-sdgs/en
UN Water (2016) Integrated Monitoring Guide for SDG 6 Targets and global indicators. www.unwater.org

41
World Bank (2004) World Development Report 2004: Making Services Work for Poor People. World Bank. openknowledge.worldbank.org/handle/10986/5986
WHO (2015) Sanitation Safety Planning: Manual for safe use and disposal of wastewater, greywater and excreta. France: World Health Organization. www.who.int/water_sanitation_health/publications/ssp-manual/en
WHO and UNICEF (2015) WASH Post-2015, Proposed indicators for drinking water, sanitation and hygiene. www.wssinfo.org/fileadmin/user_upload/resources/JMP-WASH-Post-2015-Brochure.pdf
WHO and UNICEF (2015) Drinking Water Supply and Sanitation Joint Monitoring Programme (JMP). www.wssinfo.org
WSP (2012) What Does It Take to Scale Up Rural Sanitation, World Bank. www.wsp.org/sites/wsp.org/files/publications/WSP-What-does-it-take-to-scale-up-rural-sanitation.pdf
WSP (2013) Economics of Sanitation Initiative for South Asia, World Bank. www.wsp.org/content/south-asia-economic-impacts-sanitation

Civil Society Water, Sanitation and Hygiene Fund
42
ANNEX 2
South Asia Regional Learning Event Program 8 – 11 November 2016, Kandy, Sri Lanka
Thematic objectives of the event include to:
1. Improve the understanding of CSO approaches to embedding and strengthening government/change agent systems at multiple levels for demand and supply-side sanitation and monitoring, including supportive financing and incentive schemes, and systems for monitoring changes in access to sanitation;
2. Explore approaches to ensuring total sanitation for all, particularly poor and disadvantaged households, people living with disabilities and to increasing sanitation access in remote and challenging environments; and
3. Improve understanding of effective integrated hygiene behaviour change activities to ensure maximum health
benefits are achieved from sanitation and water initiatives.
Learning objectives of event include to:
1. Improve the effectiveness and sustainability of WASH projects within the Fund by facilitating knowledge exchange and learning;
2. Strengthen relationships between CSOs, local government and other change agents to extend specific areas for collaboration and sharing; and
3. Provide a forum to learn from and share with the wider WASH sector and strengthen communities of practice
within the Fund.
Theme: Thinking beyond Open Defecation Free (ODF) towards the SDGs and safely managed sanitation for all
DAY 1: Open DayTime Tuesday 8 November
8:00 – 9:00 Registration
9:00 – 9:10 Welcome and Lighting of the LampDavid van Eyck, National Facilitator and Master of Ceremonies
9:10 – 9:20 Welcome by World Vision Dr Dhanan Senathiraja, National Director, World Vision Lanka
9:20 – 9:30 Welcome to Central Province The Hon. Sarath Ekanayake, Chief Minister, Central Province, Sri Lanka
9:30 – 9.40 Australian Aid and WASH in Sri Lanka Charlotte Blundell, Counsellor, Development Cooperation, Sri Lanka and Maldives, DFAT, Australian High Commission, Sri Lanka
9:40 – 9:50 Official Opening Representative of The Hon. Rauf Hakeem, Minister for Water Supply and City Planning, Ministry of Water Supply and City Planning
9:50 – 10:10 Current status of sanitation and water in Sri Lanka Representative of Eng. G. A. Kumararathna, General Manager, National Water Supply and Drainage Board

43
DAY 1: ContinuedTime Tuesday 8 November
10:10 – 10:40 Break
10:40 – 10:50 Introduction to the learning event program and objectivesBronwyn Powell, Knowledge and Learning Manager (KALM), CS WASH Fund Management Facility
10:50 – 11:15 Keynote Presentation – Moving beyond ODF to safely managed sanitation for allMark Ellery, Topic Expert/Facilitator of South Asia Regional Learning Event
11:15 – 12:00 Presentations and panel discussion 1) Beyond the finish line and total sanitation – Gabrielle Halcrow, SNV Netherlands Development
Organisation2) Partnering with Disabled Peoples Organisations to strengthen disability inclusive WASH – Vellayan
Subramaniam (President of Northern Province Consortium of Organization for Differently Abled (NPCODA) and Jeyald Rasaratnam, Operations Manager, World Vision Lanka
3) Supporting market-side responses to demand generated by CLTS activities – Asim Muhammad Saleem, Plan Pakistan
12:00 – 1:00 Lunch
1:00 – 2:00 “Marketplace” of CS WASH Fund project posters in South Asia
2:00 – 2:05 CS WASH Fund video
2:05 – 2:20 Australian Aid support to WASH and the Civil Society WASH Fund Marcus Howard, Water, Sanitation and Hygiene Section, Australian Department of Foreign Affairs and Trade
2:20 – 2:35 Communities of Practice and innovation for CSOs and WASH sector learning Bronwyn Powell, KALM
2:35 – 2:50 CS WASH Fund progress and trends Dr Paul Crawford, Monitoring, Evaluation and Review Panel (MERP)
2:50 – 3:00 Question and answer session
3:00 – 3:30 Break
3:30 – 4:45 Thematic sharing sessions 1) Sanitation marketing and financing amongst poor communities in Bangladesh – Habitat for Humanity
Bangladesh and iDE 2) Decision-making at the village level and ensuring women’s voice in decision-making – lessons from
Khyber Pakhtunkhwa – IRC Pakistan3) Behaviour change communications and hygiene cost effectiveness – SNV BhutanThese are parallel sessions with brief presentations, group activities and discussion
4:45 – 5:00 Day 1 Wrap-up session
Briefing for field visit
5:15 – 6:30 Welcome function at Earl’s Regency
ANNEX 2 continued

Civil Society Water, Sanitation and Hygiene Fund
44
ANNEX 2 continued
Time Wednesday 9 November
7:00 am Depart Earl’s Regency – Packed breakfast provided
7:00 – 9:30 Travel to Hatton
9:30 – 10:00 Morning tea
10:00- 11:00 • Security and child protection briefing by World Vision • Welcome by plantation management, Local Authority and Provincial Government representatives • Split into two groups for Gallery Walk
11.00 – 12.30 Group 1 – Mayfield Estate – Site 1 This project was completed two years ago and is now operating as a community managed scheme. It provides a good example of partnerships with community, private sector and government. Communities are ODF. Visitors will see sanitation projects and learn how WV works with partners and CBOs to achieve ODF.
Group 2 – Lindula EstateThis estate has new housing estates with integrated housing. This estate provides an example of different institutions have partnered (microfinance organisations, government, WV) to meet the basic needs of the community. Visitors will see the technical challenges of supplying services to and emptying septic tanks in hilly areas.
12.30 – 1:30 Lunch at Tea Estate Lunch at Lindula Estate Bungalow
1:30 – 4:00 Mayfield Estate – Site 2 • Visit a gravity-fed water project for
household water supply scheme and meet user groups.
• Inspect handwashing stations and household latrines
• Learn about Operation and Maintenance, user fees and how plantations support sustainability
MacDuff EstateThis is a privately owned estate that had been neglected and had no basic facilities for workers. With the RIWASH DFAT grant, a central sewerage system connecting all plantation workers houses to a central system was built. This was a pilot test and now provides a model for community-managed systems that will be rolled out to other areas. Improvements to the estate included electricity, sanitation and water connections. The communities have been ODF certified for 5 years.
4:00 – 4:30 Evening Tea at Hotel Asvika – Group 1 and 2 meet for debriefing
4:30 – 7:00 Travel back to Earl’s Regency
Group 1 – Mayfield Estate
Focus on sanitation advocacy, gravity flow water projects with private-public partnership, and the institutional
arrangements for CBOs for operation and maintenance (O&M) of infrastructure.
Group 2 – Lindula and MacDuff Estates
Lindula Estate – Focus on integrated housing projects that were part of a water and sanitation program with different stakeholder partnerships to meet the basic needs of plantation communities.
MacDuff Estate – This estate has been certified ODF for five years. The visit will focus on how the community is maintaining centralised sanitation infrastructure (sewerage).
DAY 2: Field Trip to tea plantation estates with World Vision Lanka

45
ANNEX 2 continued
DAY 3: Workshop: Beyond ODF towards safely managed sanitation for all
Time Thursday 10 November
9:00 – 9:30 Field trip debriefing
9:30 – 10:15 SESSION 1: Sanitation status and mapping bottlenecks by country
1) Introductory presentation to sanitation status in the South Asia Region – Mark Ellery
2) Activity In 5 country groups, CSOs and change agents will be issued with a PowerPoint presentation that contains a graph of the rural sanitation status in their country and a graph of the major rural sanitation bottlenecks in their country. The groups will be asked to annotate this PowerPoint to identify the dimensions (i.e. the scope, scale, type) of the bottlenecks in rural sanitation.
3) Post-ODF tools presentation – Anup Regmi, SNV Nepal
10:15 – 10:45 Break
10:45 – 12:30 SESSION 2: Sanitation ladder analysis
1) Presentations
• Introductory presentation on sanitation ladder in the South Asia Region – Mark Ellery
• Challenges and approaches to addressing water contamination – Nazmul Azam Khan and Biplob Kanti Mondal, Bangladesh Red Crescent Society
• Developing a mobile desludging business: lessons from Zimbabwe – Bronwyn Powell for Welthungerhilfe
2) Activity In 5 country groups, the CSOs and Change Agents will be issued with a PowerPoint presentation that contains a graph of the size of the steps in the rural sanitation ladder in their country. The 5 country groups will be asked to annotate this PowerPoint presentation to identify the priority interventions necessary to assist the different households to move up the different steps in the rural sanitation ladder.
12:30 – 1:30 Lunch
1:30 – 3:00 SESSION 3: Roles and responsibilities for sanitation
1) Presentations • Assigning roles and responsibilities for sanitation – Mark Ellery
2) Activity In 5 country groups, CSOs and change agents will be issued with a generic PowerPoint presentation on the vertical and horizontal assignment of roles and responsibilities for rural sanitation in their country. The 5 country groups, will be requested to identify the vertical and horizontal assignment of responsibilities to the different government agents associated with the 4 major sanitation steps necessary to achieve the SDGs (versus an assessment of their capacity).
3:00 – 3:30 Break
Civil Society Water, Sanitation and Hygiene Fund
46
Time Thursday 10 November
3:30 – 4:45 SESSION 4: CSO priorities to strengthen national sanitation institutions
1) Presentations
• Working with government at scale – wider replication of project approaches – Najeed Aslam, Director (Community Development and Training), Local Government and Community Development Department, Government of Punjab
• Menstrual Hygiene Management – Towfika Khatun, Habitat for Humanity
• Levers of change in sanitation – Mark Ellery
2) Activity In the 5 country groups, CSOs and change agents will identify the short, medium and long term priority actions for CSOs to support the government institutions in each country.
4:45 – 5:00 Day wrap-up
6:15 – 9:30 Conference Dinner
ANNEX 2 continued
DAY 3: Workshop continued

47
Time Friday 11 November
9:00 – 10:15 Thematic sharing sessions
1) Strengthening disability inclusive WASH – NPCODA and World Vision Lanka2) Learning for impact in WASH – CS WASH Fund K&L Component/ISF UTS3) Menstrual Hygiene Management – SNV
These are parallel sessions with brief presentations, group activities and discussion
10:15 – 10:45 Break
10:45 – 11:00 Context Mapping Exercise – Paul Tyndale-Biscoe and Paul Crawford (MERP)
• Activity to place your project on the strategy spectrum (direct delivery through to strengthening the enabling environment)
11:00 – 12:15 Context Mapping Exercise
• ‘Mapping the Context’ overview• Group work activity
12:15 – 1:15 Lunch
1:15 – 2:45 Strategy Mapping Exercise continued
• Introduction to the Strategy Spectrum• Strategy Mapping – Overview and the mapping process• Strategy mapping activity in project teams
2:45 – 3:15 Break
3:15 – 5:00 Workshop closing session
• Team action planning • Activities for synthesising and consolidating learning
ANNEX 2 continued
DAY 4
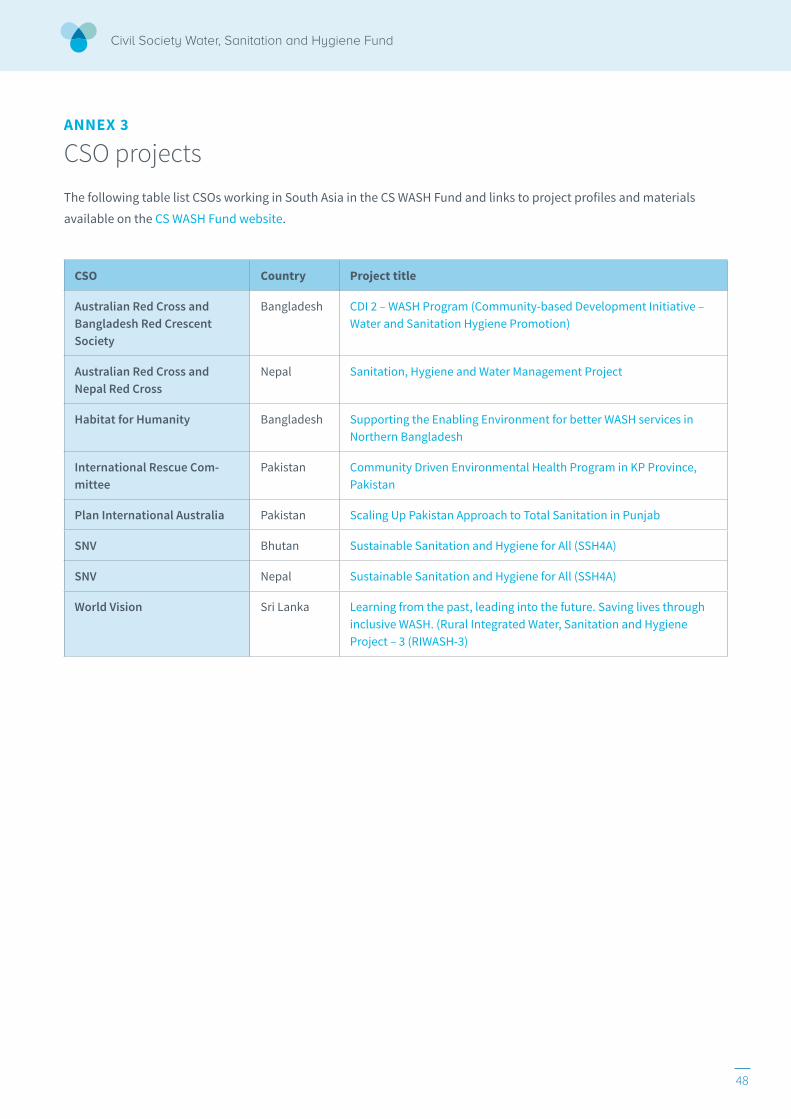
Civil Society Water, Sanitation and Hygiene Fund
48
ANNEX 3
CSO projects The following table list CSOs working in South Asia in the CS WASH Fund and links to project profiles and materials
available on the CS WASH Fund website.
CSO Country Project title
Australian Red Cross and Bangladesh Red Crescent Society
Bangladesh CDI 2 – WASH Program (Community-based Development Initiative – Water and Sanitation Hygiene Promotion)
Australian Red Cross and Nepal Red Cross
Nepal Sanitation, Hygiene and Water Management Project
Habitat for Humanity Bangladesh Supporting the Enabling Environment for better WASH services in Northern Bangladesh
International Rescue Com-mittee
Pakistan Community Driven Environmental Health Program in KP Province, Pakistan
Plan International Australia Pakistan Scaling Up Pakistan Approach to Total Sanitation in Punjab
SNV Bhutan Sustainable Sanitation and Hygiene for All (SSH4A)
SNV Nepal Sustainable Sanitation and Hygiene for All (SSH4A)
World Vision Sri Lanka Learning from the past, leading into the future. Saving lives through inclusive WASH. (Rural Integrated Water, Sanitation and Hygiene Project – 3 (RIWASH-3)

49
ANNEX 4
Latrine options Dry Pit Latrines: The digestion of fresh faecal matter
is primarily aerobic but anaerobic at greater depths
due to an increasing moisture content from urine
seeping to the bottom. In temperate climates most
bacteria will be destroyed within 3-4
months and faecal sludge can be safely
handled. Small amounts of carbon (i.e.
leaves) increase the pit temperature
and ash raises the pH to assist in
destroying pathogens. The introduction
of any water into the pit will kill the
aerobic bacteria making faecal sludge
unsafe.
Direct Pit Latrines: The digestion process within
the pit is primarily anaerobic. As the bottom of the
pit quickly becomes blocked with faecal sludge, the
effluent primarily leaches through the
walls of the pit where it is exposed
to an aerobic digestion process. In
addition to the risks associated with
broken water seals and/or platforms,
the faecal contents of the pit are
unsafe to handle in addition to being
difficult to access to empty.
Offset Pit Latrines: Similar to the direct pit latrine
the digestion process within the pit is anaerobic while
the effluent is subject to an aerobic digestion process.
In many cases, the absence of sufficient holes for the
effluent to leach through the sides of the pit means
that the pit fills up relatively
quickly with a mixture of faecal
effluent & sludge. This means
that the pit contents are generally
highly liquid and unsafe for
handling. It also means that when
the pits are emptied the contents
need to be buried.
Twin Offset Pit Latrines: The introduction of a twin
offset pit means that the ‘on-line’ pit will be anaerobic
while the ‘off-line’ pit will gradually become aerobic.
This means that the off-line pit
will become safe for handling
after a period of 1 year or
more. In those cases where pits
are slow to leach, it should be
possible to switch between the
two pits several times before
emptying.
Septic Tank & Leach Pit: Faecal sludge within a septic
tank is subject to anaerobic digestion, while the faecal
effluent is subject to aerobic digestion. The contents
of the septic tank need to be emptied about every
five years and are never safe to handle. A septic tank
without a leach pit doesn’t treat pathogens within
the faecal effluent
and as the faecal
sludge builds up
within the tank, the
retention time is
lost and the sludge
is discharged with
the effluent.
Septic Pits: The high cost of septic tanks, the poor
performance of leach drains (associated with high
density soils in South Asia that don’t leach) and
the risks associated with the handling of the septic
sludge has resulted in the development
of a lower cost option
comprised of septic pit.
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic
TwinO�set
Pit
Sludge Aerobic
Effluent
Aerobic
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic
TwinO�set
Pit
Sludge Aerobic
Effluent
Aerobic
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic
TwinO�set
Pit
Sludge Aerobic
Effluent
Aerobic
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic Twin
O�setPit
Sludge Aerobic
Effluent
Aerobic
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic
TwinO�set
Pit
Sludge Aerobic
Effluent
Aerobic
Aerobic
Anaerobic
Vent pipe
Urine
Dry Pit
Anaerobic
Aerobic Effluent
Sludge
O�set Pit
Anaerobic
Sludge
Direct Pit
Effluent
Scum
Sludge
Effluent
Anaerobic Aerobic
Septic Tank& Leach Pit
Anaerobic
Septic Pits
Anaerobic Scum
Effluent Effluent
Sludge Sludge
Aerobic
Effluent
Sludge
Aerobic
Anaerobic
TwinO�set
Pit
Sludge Aerobic
Effluent
Aerobic
Level 7, 307 Queen Street
Brisbane Qld 4000, Australia
+61 7 3025 8500