therapeutic hypothermia: where do we stand?wcm/@gra/documents/... · 5/29/2015 1 therapeutic...
TRANSCRIPT
5/29/2015
1
Therapeutic Hypothermia:
Where Do We Stand?
Melina Aguinaga-Meza, MD
Assistant Professor of Medicine
Gill Heart Institute
University of Kentucky
Disclosure Information
Melina Aguinaga-Meza, MD
“Therapeutic Hypothermia: Where Do We Stand?”
• FINANCIAL DISCLOSURE:
– No relevant financial relationship exists
• UNLABELED/UNAPPROVED USES DISCLOSURE:
– No relevant relationship exists

5/29/2015
2
The Clinical Problem
• Out-of-hospital cardiac arrest (OHCA) is a leading
cause of death among adults in the US
• Approx. 300,000 OHCA events occur each year in the
US
• Resuscitation is attempted in 100,000 of these arrests
• Less than 40 000 survive to hospital admission
MMWR / July 29, 2011 / Vol. 60 / No. 8

5/29/2015
3
• The effects of this syndrome are severe and pervasive
MMWR / July 29, 2011 / Vol. 60 / No. 8
Consequences From Cardiac Arrest
Brain injury Myocardial dysfunction
Systemic ischemia + reperfusion
responses
Disorder that caused the cardiac
arrest
Post-Cardiac Arrest
Syndrome
Survival and Neurological Outcomes
after OHCA
• Only one third of patients admitted to the hospital survive to
hospital discharge
• Approx. one out of ten people who experience OHCA survive
to hospital discharge
• Only 2 out of 3 of them have a good/moderate neurologic
recovery
MMWR / July 29, 2011 / Vol. 60 / No. 8: CARES

5/29/2015
4
“Chain of Survival”
• Actions needed to improve chances of survival from
out-of-hospital cardiac arrest
Circulation 2010; 122:S676-84
• Try to identify and treat the precipitating causes of
the arrest and prevent recurrent arrest.
• Identify and treat acute coronary syndromes (ACS)
• Optimize mechanical ventilation to minimize lung
injury
• Reduce the risk of multiorgan injury and support
organ function if required
• Control body temperature to optimize survival and
neurological recovery

5/29/2015
5
Historical Development
History
• 1803 “Russian Method of Resuscitation” consisted of
burying the victim of a cardiac arrest in snow hoping for
ROSC
Resuscitation 80 (2009) 1335

5/29/2015
6
History
• In 1930s-1940s, hypothermia in cancer patients
• In 1950s, induced TH was widely used during head/
spinal cord injuries and cardiac surgery
• In 1959, Benson et al., case series of 19 patient post
cardiac arrest
CHEST 2008; 133:1267–1274
Induced
Hypothermia
(30-32oC)
Normothermia
Survived 6 (50%) 1(14%)
Died 6 6
Total 12 7
History
• 1950 -1960s , Deep Hypothermia (<30°C)
– Cardiac irritability and ventricular fibrillation
– Infections
– Coagulopathy
• 1960 -1990s, the use of TH decreased
• 1990s, animal experiments
– Neurological outcome could be improved by
using mild to moderate hypothermia (31°C–35°C) rather
than deep hypothermia (<30°C)
– Fewer and less severe side effects
CHEST 2008; 133:1267–1274

5/29/2015
7
Pathophysiology and Effect
of Therapy
Ischemia-Reperfusion Brain Injury
• Cascade of destructive events and processes
• Begins in minutes and continues for hours/days
• Retriggered by new episodes of ischemia
Crit Care Med 2009; 37[Suppl.]:S186 –S202
All of these processes are temperature dependent

5/29/2015
8
Maintains Neuronal Integrity
• Inhibit the “Neuroexcitatory cascade”
(Ca++ influx, accumulation of glutamate, and release of glycine)
• Blocks Astroglial activation
Front Neuro 2011; 2:1-8
Crit Care Med 2009; 37[Suppl.]:S186 – S202
Avoids Apoptosis
Front Neuro 2011; 2:1-8
Crit Care Med 2009; 37[Suppl.]:S186 – S202

5/29/2015
9
Decreases Brain Metabolism and
Oxidative Stress
Front Neuro 2011; 2:1-8
Crit Care Med 2009; 37[Suppl.]:S186 – S202
• Decrease in Cerebral Metabolism, oxygen consumption and glucose
• Lowers lactate levels from anaerobic metabolism decreasing cellular acidosis
• Blocks release of free radicals
• Decreases the concentrations of thromboxane A2
Other Mechanisms of Action
• Decreases Inflammation:
– Decreases inflammatory cytokines, leukotrienes,
and inflammatory cells function (macrophages)
• Decreases cytotoxic edema
• Reduces disruption of the blood–brain barrier
• Decreases the damage of the endothelial vasculature
• Suppresses epileptogenic electrical activity
Front Neuro 2011; 2:1-8
Crit Care Med 2009; 37[Suppl.]:S186 – S202

5/29/2015
10
Clinical Evidence
Fever

5/29/2015
11
Hypothermia-40%
Hyperthermia-26%
Fever � Worse survival
Stroke. 2002;33:1759-1762
• Japan, 1980-1990
• Fever � Worse neurological outcomes
• Hyperthermia is an early indicator of brain damage
after resuscitation
Intensive Care Med (1991) 17:419-420

5/29/2015
12
• Austria, observational, prospective, 1992-1995
• Witness cardiac arrest with ROSC
• Fever � Unfavorable neurologic recovery
Arch Intern Med 2001;161:2007
• Fever is a common complication in patients
with various types of neurological injury
• Fever is independently associated with an
increased risk of adverse outcome

5/29/2015
13
Therapeutic Hypothermia in
OHCA with Shockable Rhythm
N Engl J Med 2002;346:557-63
• Melbourne, Australia
• September 1996 and June 1999
• Randomized controlled trial
• Patients:
– Ventricular Fibrillation
– ROSC with persistent coma
• Exclusion criteria:
– Cardiogenic shock (SBP < 90 mm Hg despite epinephrine infusion)
– Other possible causes of coma (drug overdose, head trauma, or cerebrovascular
accident)

5/29/2015
14
Methods
Hypothermia (n=43)
Normothermia
(n=34)
• At discharge, outcomes:
• Favorable neurologic outcome
• Mortality
N Engl J Med 2002;346:557-63
Hypothermia Protocol• Cold packs (ambulance) + ice packs (ED/ICU)
• Midazolam + Vecuronium PRN for shivering
• Optimal ventilator and hemodynamic support
• Thrombolytic for AMI/Heparin for ACS
• Lidocaine to prevent recurrent ventricular arrhythmias
• Target temperature of 33°C for 12h
• Passive rewarming over 8h
N Engl J Med 2002;346:557-63
ICU
Target temp 33C
Rewarmed
24h18h12h0h-2h
ROSC
5/29/2015
15
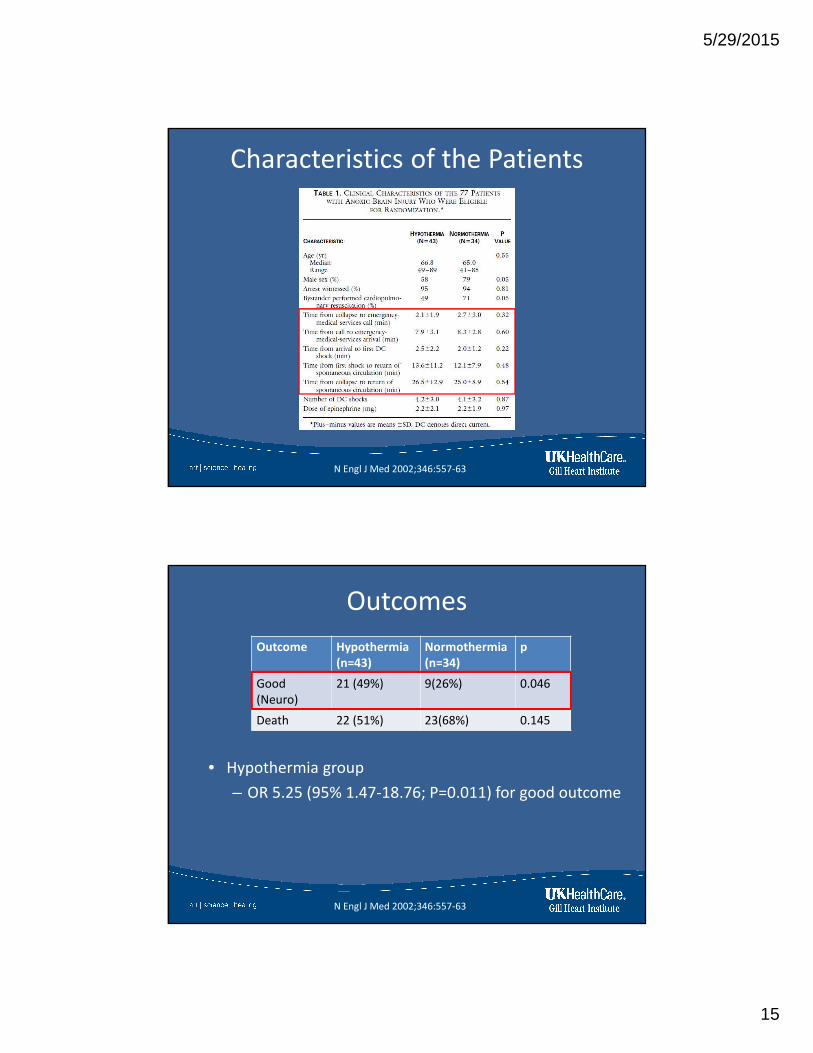
Characteristics of the Patients
N Engl J Med 2002;346:557-63
Outcomes
N Engl J Med 2002;346:557-63
Outcome Hypothermia
(n=43)
Normothermia
(n=34)
p
Good
(Neuro)
21 (49%) 9(26%) 0.046
Death 22 (51%) 23(68%) 0.145
• Hypothermia group
– OR 5.25 (95% 1.47-18.76; P=0.011) for good outcome

5/29/2015
16
Hemodynamics and Adverse Effects
N Engl J Med 2002;346:557-63
• No significant differences between the two groups with
respect to the frequency of adverse events
• Europe, March 1996 - January 2001
• Multicenter (9 centers in 5 countries) , randomized, controlled
trial
• Patients:
– Witnessed cardiac arrest
– Ventricular Fibrillation or ventricular tachycardia
– Collapse - CPR by EMS < 15min.
– Collapse - ROSC, < 60 min
• Excluded:
– Temp < 30OC, comatose before the cardiac arrest (drugs), response to
verbal commands after ROSC, MAP < 60mmHg , persistent
hypoxemia, coagulopathy
N Engl J Med 2002;346:549-56
5/29/2015
17
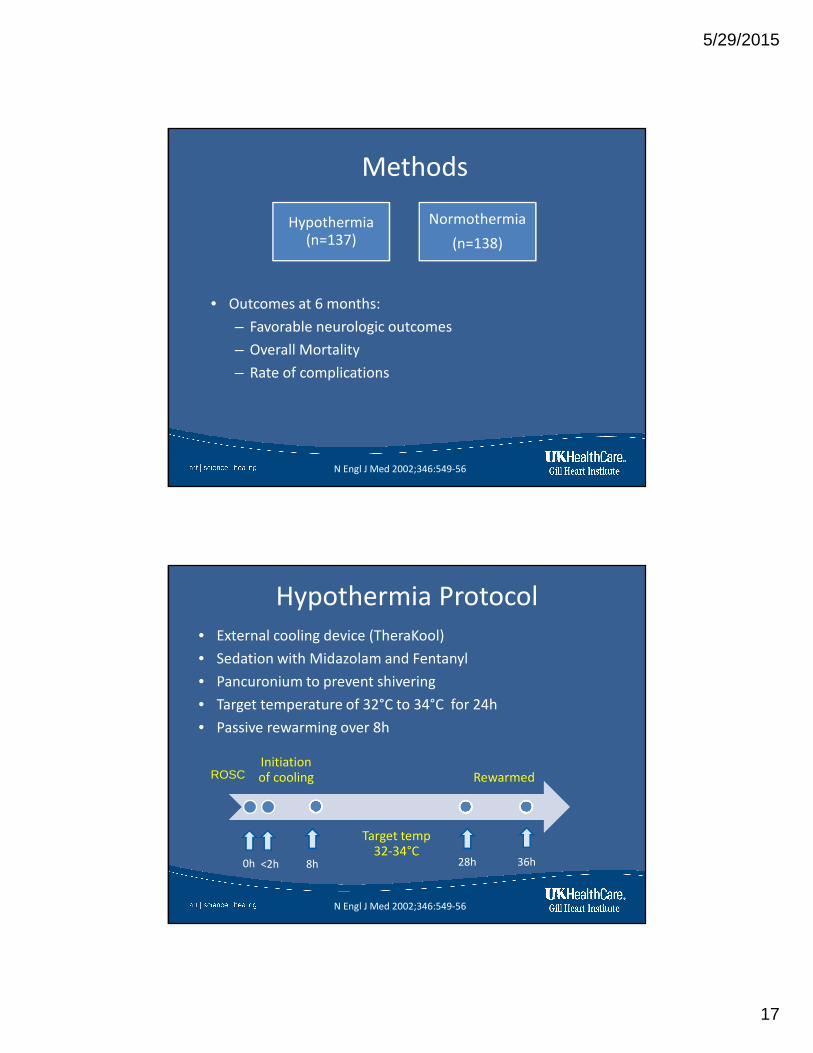
• Outcomes at 6 months:
– Favorable neurologic outcomes
– Overall Mortality
– Rate of complications
N Engl J Med 2002;346:549-56
Hypothermia (n=137)
Normothermia
(n=138)
Methods
Hypothermia Protocol
• External cooling device (TheraKool)
• Sedation with Midazolam and Fentanyl
• Pancuronium to prevent shivering
• Target temperature of 32°C to 34°C for 24h
• Passive rewarming over 8h
Initiation of cooling
Target temp 32-34°C
Rewarmed
36h28h8h<2h0h
ROSC
N Engl J Med 2002;346:549-56

5/29/2015
18
Temperature Curves
• ROSC-initiation of cooling : 105 min.
• ROSC- target temp 8h
N Engl J Med 2002;346:549-56
N Engl J Med 2002;346:549-56
Characteristics of the Patients

5/29/2015
19
Neurologic Outcomes
• Therapeutic Mild Hypothermia � Favorable Neurologic Outcome
N Engl J Med 2002;346:549-56
Cerebral Performance Category
� CPC 1 (good recovery)
� CPC 2 (moderate disability)
Survival
59%
45%P=0.02
N Engl J Med 2002;346:549-56
• Therapeutic Mild Hypothermia � Improved Survival

5/29/2015
20
Complications
N Engl J Med 2002;346:549-56
• Complication rate did not differ significantly between the
two groups
Therapeutic Hypothermia in OHCA
with Non-shockable Rhythm

5/29/2015
21
• Brussels, Belgium
• Randomized controlled trial
• Asystole or pulseless electrical activity (PEA)
• Remained unconscious after ROSC
• Target temp 34°C for 4h
• Helmet device
Resuscitation 51 (2001) 275–281
• Lactate and O2 extraction
ratio were significantly lower
in the hypothermia group
Resuscitation 51 (2001) 275–281
Outcome Hypothermia
(n=16)
Normothermia
(n=14)
Death 13 (81%) 13(92%)

5/29/2015
22
Circulation. 2011;123:877-886
• 19 sites (Europe), 2003-2005, observational, registry
• Lower mortality in the hypothermia group in patients with
PEA/asystole as first rhythm
Circulation. 2011;123:877-886
• Paris, France, 2000-2009, prospective cohort
• No difference in outcomes in patients with PEA/asystole as
first rhythm

5/29/2015
23
Therapeutic Hypothermia after
In-hospital Cardiac Arrest
Circulation. 2011;123:877-886
• 19 sites (Europe), 2003-2005, observational, registry
• No difference in outcomes for patients with in-hospital
arrest

5/29/2015
24
Guidelines
Circulation. 2003;108:118-121
Resuscitation 57 (2003) 231/235
5/29/2015
25
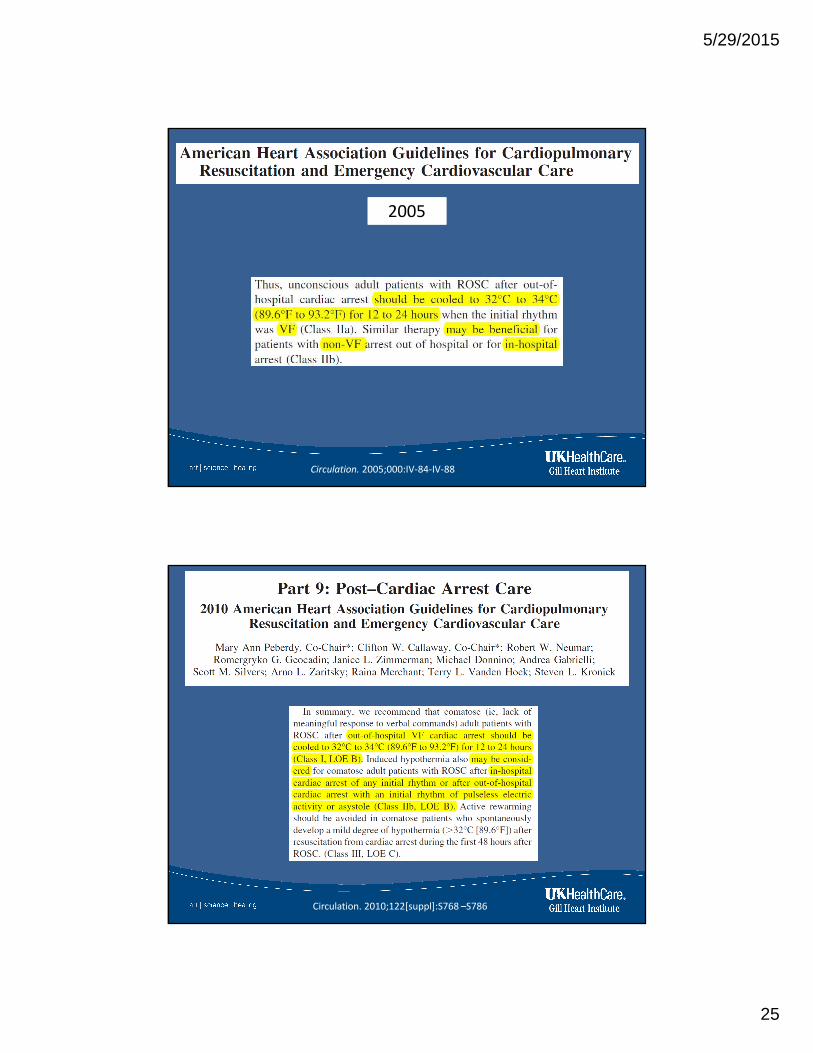
20052005
Circulation. 2005;000:IV-84-IV-88
Circulation. 2010;122[suppl]:S768 –S786

5/29/2015
26
Circulation. 2010;122[suppl]:S768 –S786
Clinical Use
5/29/2015
27
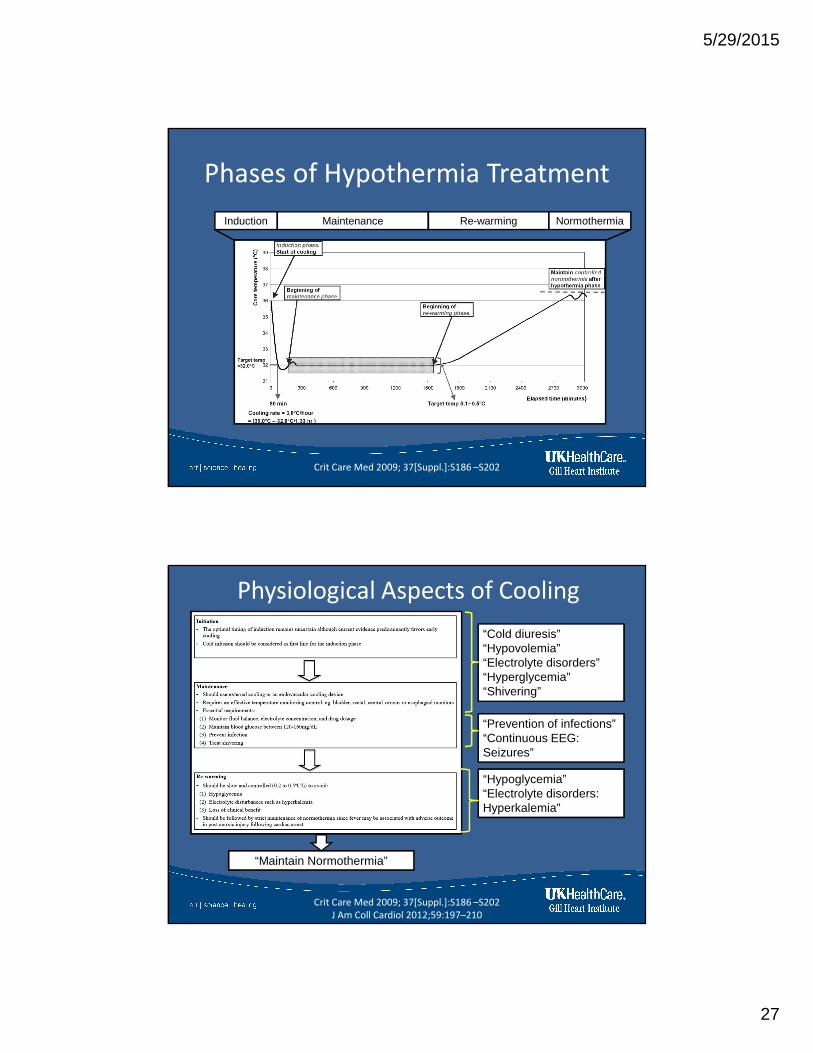
Phases of Hypothermia Treatment
Crit Care Med 2009; 37[Suppl.]:S186 –S202
Induction Maintenance Re-warming Normothermia
Physiological Aspects of Cooling
“Cold diuresis”“Hypovolemia”“Electrolyte disorders”“Hyperglycemia”“Shivering”
“Prevention of infections”“Continuous EEG: Seizures”
“Hypoglycemia”“Electrolyte disorders: Hyperkalemia”
“Maintain Normothermia”
Crit Care Med 2009; 37[Suppl.]:S186 –S202
J Am Coll Cardiol 2012;59:197–210

5/29/2015
28
Physiologic Effects and Complications
• Shivering
• Cardiovascular manifestations
• Hyperglycemia
• Electrolyte disorders
• Bleeding
• Alterations in drug metabolism
• Risk of Infections
Crit Care Med 2009; 37[Suppl.]:S186 –S202
J Am Coll Cardiol 2012;59:197–210
Cooling Techniques

5/29/2015
29
Conventional Cooling Systems
• Cold saline, crushed ice or ice bags
• Easiest and effective way to induce hypothermia
• Not so effective in maintaining target temperature
Resuscitation (2007) 73, 46—53
Surface Cooling Systems• Circulating cold fluid or cold air through blankets/pads
wrapped around the patient
• Easy to apply and rapid initiation of treatment
• Maintenance of temperature may be difficult
• Shivering is more common
• Complication: Skin burns/irritation
Critical Care (2015) 19:103

5/29/2015
30
Intravascular Cooling Systems• Percutaneously placed central venous catheters
• Circulating cool or warm saline in a closed loop through the
catheter’s balloon
• Less shivering compared to surface devices
• Complication: Thrombosis
Critical Care (2015) 19:103
• No difference in outcomes between the groups
Resuscitation 81 (2010) 1117–1122

5/29/2015
31
• Endovascular cooling
– Longer time within the target temperature range
– Less temperature fluctuation
– Better control during rewarming
– Less overcooling
– Less failure to reach the target temperature
Resuscitation 81 (2010) 1117–1122
Implementation
5/29/2015
32
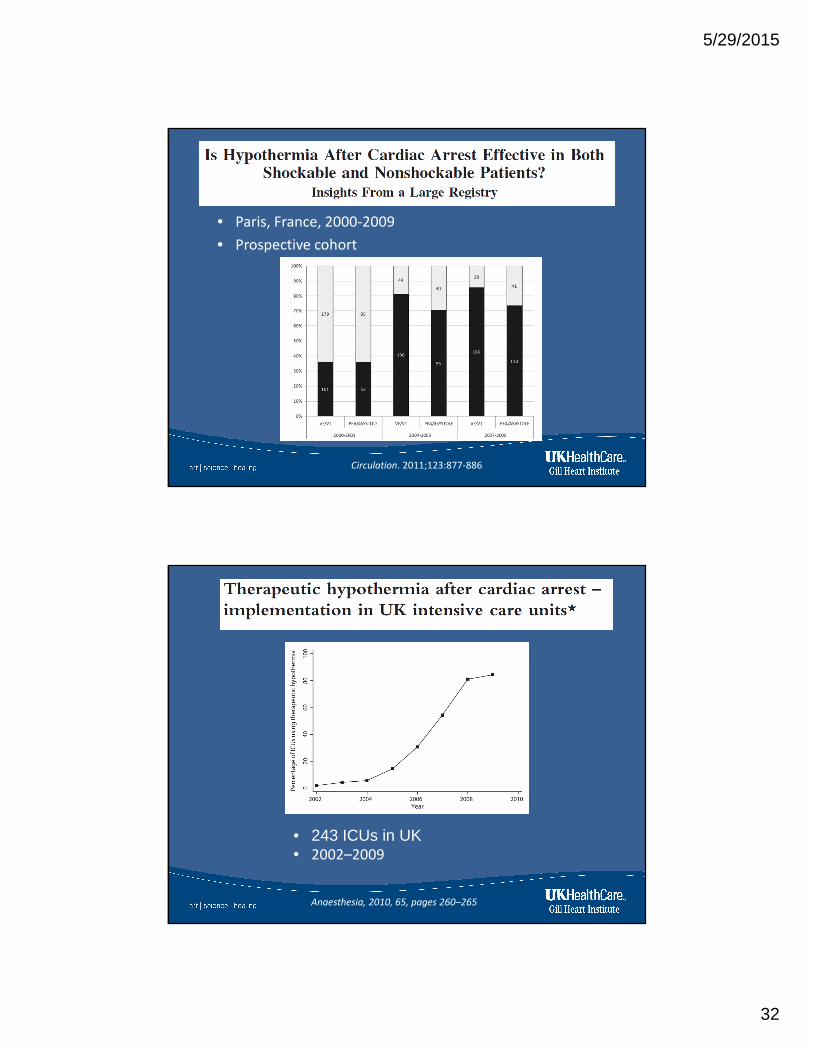
Circulation. 2011;123:877-886
• Paris, France, 2000-2009
• Prospective cohort
• 243 ICUs in UK• 2002–2009
Anaesthesia, 2010, 65, pages 260–265

5/29/2015
33
National Trends in the Use of Postcardiac Arrest
Therapeutic Hypothermia and Hospital Factors
Influencing Its Use
Ther Hypothermia Temp Manag.
2015 Mar;5(1):48-54. Epub 2015 Jan
2007 2010
Hospitals using TH 4.60% 22.16%
Patients received
TH0.34% 2.49%
0%
5%
10%
15%
20%
25%
• Across 2007–2010, in United States
National Trends in the Use of Postcardiac Arrest
Therapeutic Hypothermia and Hospital Factors
Influencing Its Use
Ther Hypothermia Temp Manag.
2015 Mar;5(1):48-54. Epub 2015 Jan
Significant hospital factors associated with TH utilization
were:
• Large hospitals
• Urban location, northeast or west regions
• Teaching hospitals
• Non-safety net hospitals
• Increasing year
• Hospitals with higher annual cardiac arrest volume

5/29/2015
34
Survival During The Last Decade
Survival following OHCA
• In Denmark , Danish Cardiac Arrest Registry
• Patients with OHCA , 2001 - 2010
JAMA. 2013;310(13):1377-1384

5/29/2015
35
Survival following OHCA
J Intern Med 2013; 273: 572–583.
• Get with the Guidelines Resuscitation Registry
• 374 hospitals in the US, 2000 - 2009
N Engl J Med 2012;367:1912-20

5/29/2015
36
Interventions In Resuscitation
Over The Last Decade
• Bystander CPR
• Increased use of AED
• High quality compressions: compression-only
• Good chest compressions and minimal “hands-off time”
• Early revascularization (PCI)
• Improved post-resuscitation care
• Use of ‘track and trigger systems’ to detect patients
deterioration (Rapid Response Team)
• Mild Therapeutic Hypothermia
N Engl J Med 2012;367:1912-20.
Targeted Temperature Management
Post Cardiac Arrest

5/29/2015
37
N Engl J Med 2013;369:2197-206
• Randomized trial, Nov 2010 - Jan 2013
• 36 ICUs in Europe and Australia
• Patients:
– OHCA, unconscious at presentation to the hospital
• Exclusion:
– ROSC to screening > 240 minutes(4h)
– Unwitnessed arrest with asystole as the initial rhythm
– Suspected or known acute intracranial hemorrhage or
stroke
– Body temperature of less than 30°C
N Engl J Med 2013;369:2197-206

5/29/2015
38
• Outcomes at 6 months:
– Neurologic outcomes
– Overall Mortality
33°C
(n=473)
36°C
(n=466)
Methods
N Engl J Med 2013;369:2197-206
TTM Protocol• Method of cooling:
– Intravascular cooling catheter (24%)
– Surface cooling system (76%)
• 33°C vs 36°C for a total of 28h
• After 28h gradual rewarming to 37°C (0.5°C/hour)
• Maintain < 37.5°C until 72 h after the cardiac arrest
N Engl J Med 2013;369:2197-206
0h
Randomization
28h
Rewarming
36h

5/29/2015
39
Temperature Curves
• P<0.001 for separation of curves
N Engl J Med 2013;369:2197-206
Characteristics of the Patients
N Engl J Med 2013;369:2197-206

5/29/2015
40
Characteristics of the Patients
N Engl J Med 2013;369:2197-206
Outcomes
• No outcome difference between the two groups
N Engl J Med 2013;369:2197-206
5/29/2015
41
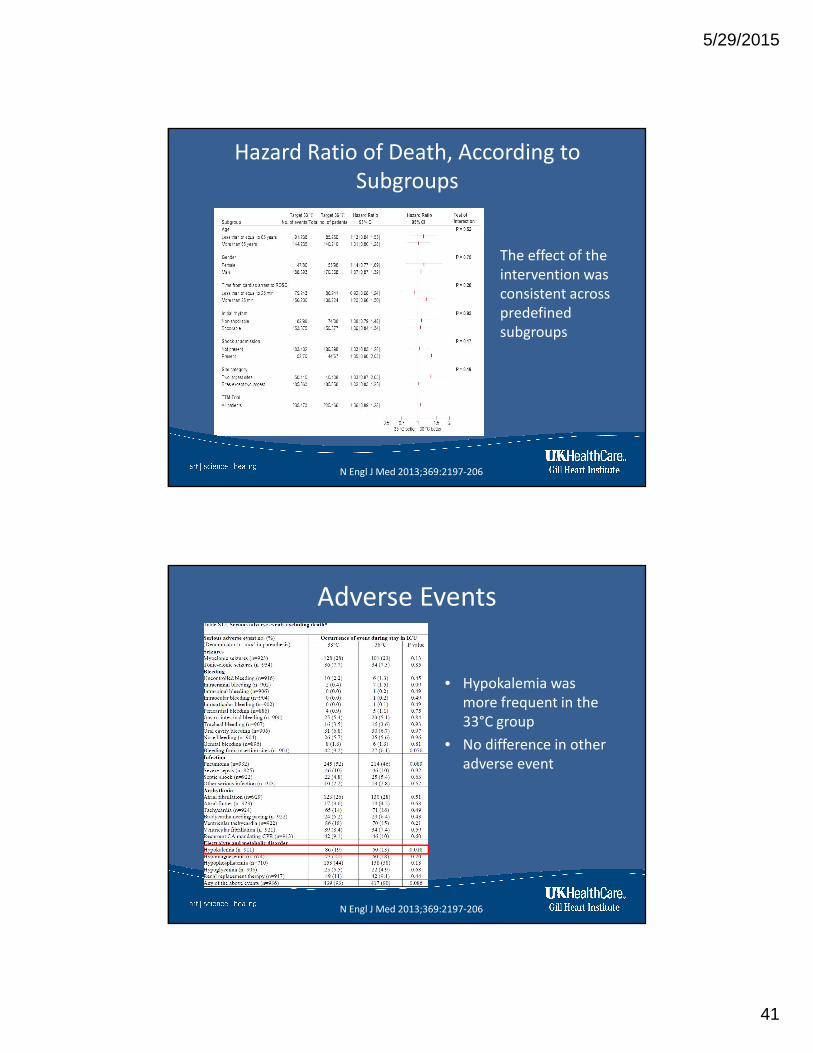
Hazard Ratio of Death, According to
Subgroups
The effect of the
intervention was
consistent across
predefined
subgroups
N Engl J Med 2013;369:2197-206
Adverse Events
• Hypokalemia was
more frequent in the
33°C group
• No difference in other
adverse event
N Engl J Med 2013;369:2197-206

5/29/2015
42
• Comatose patients after OHCA with initial NSR continue to
have a poor prognosis
• No effect of TTM at 33 ◦C compared to 36 ◦C in these patients
Resuscitation 89 (2015) 142–148
Conclusions

5/29/2015
43
Normothermia vs. TTM
Normothermia
(HACA)
Mortality in Landmark Trials
HACA
(2002)
Bernard
(2002)
TTM
(2013)
Normothermia
(37-38°C)55% 68%
32-34°C 41% 51% 50%
36°C 48%
• Fever is independently associated with an
increased risk of adverse outcome

5/29/2015
44
• In comatose post cardiac arrest patients:
– FEVER correlates with worse outcomes and should be avoided
– Hypothermia significantly mitigates/prevents destructive processes following ischemia/reperfusion brain injury
– Targeted temperature management of 36°C for 28h seems to offer equal benefits as a targeted temperature of 33°C
– This intervention should be started within 4h from ROSC
Take home messages …..
• Patients who mostly benefit from this
intervention:
– Witnessed cardiac arrest
– Bystander performed CPR (< 5 min)
– Shockable rhythm
– ACLS started < 15 min
– ROSC < 40 min
Take home messages …..

5/29/2015
45
Thanks
Gill Heart Institute