the work setting of diabetes nursing specialists in the netherlands: a questionnaire survey
TRANSCRIPT

The work setting of diabetes nursing specialists in
the Netherlands: A questionnaire survey
Tilja I.J. van den Berg a, Hubertus J.M. Vrijhoef b,c, Gladys Tummers a,Jan A. Landeweerd a, Godefridus G. van Merode a,*
a University of Maastricht, Faculty of Health, Medicine & Life Sciences, Department of Health Organisation,
Policy and Economics, The Netherlandsb University Hospital Maastricht, Department of Integrated Care, The Netherlands
c University of Maastricht, Faculty of Health, Medicine & Life Sciences, Department of Health Care Studies,
Section Nursing Science, The Netherlands
Received 26 April 2007; received in revised form 11 December 2007; accepted 18 December 2007
www.elsevier.com/ijns
Available online at www.sciencedirect.com
International Journal of Nursing Studies 45 (2008) 1422–1432
Abstract
Aim: The aim of this study is to explore whether the work organisation of diabetes specialist nurses (DSNs) differs significantly
from nurses working in hospital and nursing home and if so, does this difference result in positive or negative consequences
regarding work and health.
Background: In traditional health care settings, nurses exhibit a high level of environmental uncertainty and low decision-
making authority, which has a negative effect on psychological reactions towards work. In professional nursing, specialisation,
e.g. diabetic nursing, is a current trend in many countries. Therefore, insight into the determinants of the work situation of
nursing specialists is becoming increasingly relevant.
Methods: Comparisons were made between 3 different samples: 1204 nurses employed by 15 hospitals, 1058 nurses employed
by 14 nursing homes, and 350 diabetes nurses working in other health care settings throughout the Netherlands. Data concerning
organisation, work aspects, and psychological reactions were measured via questionnaires. Variances between the groups were
analysed with ANCOVA, besides hierarchical multiple regression analysis was applied.
Findings: Environmental uncertainty scored lower amongst diabetes nurses when compared to nurses working in the other two
types of health care settings. Social support and role conflict scored low for diabetes nursing specialists who simultaneously
perceived autonomy and role ambiguity highest. Diabetes nursing specialists also scored highest on intrinsic work motivation
and job satisfaction and lowest for psychosomatic health.
Conclusion: Except for social support and role ambiguity, diabetic nurses rate their [work] organisation, [work] aspects and
psychological [work] reactions more positively than nurses employed in other health care settings.
# 2007 Elsevier Ltd. All rights reserved.
Keywords: Diabetes nurse; Work organisation; Work pressure; Emotional exhaustion
* Corresponding author at: University of Maastricht, Department
Hope (Health Organisation, Policy and Economics), Faculty of
Health Sciences, P.O. Box 616, 6200 MD Maastricht, The Nether-
lands. Tel.: +31 43 388 1727; fax: +31 43 367 0960.
E-mail address: [email protected]
(G.G. van Merode).
0020-7489/$ – see front matter # 2007 Elsevier Ltd. All rights reserved
doi:10.1016/j.ijnurstu.2007.12.003
What is already known about the topic?
� T
.
he work organisation of nurses employed in hospitals
differs from nurses employed in nursing homes, more
specifically, environmental uncertainty.

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–1432 1423
� R
elations between work organisation, aspects, and psy-chological attitude are for the most part in line with the
Job Demand Control model regardless of the type of
health care setting.
What this paper adds
� D
iabetes specialist nurses rate their [work] organisation,[work] aspects and psychological [work] reactions more
positively than nurses employed in other health care
settings.
� T
he transition of work tasks and a high specialisation ofnurses have a positive influence on the psychological
reactions when compared to those nurses employed in
more traditional health care settings.
� I
n the diabetes specialist nurses’ workplace, there was nosignificant relation between environmental uncertainty
and psychological reactions.
1. Introduction
Throughout the past 10 years, the diabetes specialist
nurse (DSN) has developed into an indispensable profes-
sional, administering complex care to patients with diabetic.
This nursing specialisation evolved as an answer to staff
shortages in charge of providing care as well as to the
necessity for improvement of the quality of care. Nowadays,
the transfer of tasks between doctors and nurses and sub-
stitution of doctors by nursing specialists are well accepted
in the care for patients with chronic diseases such as diabetes
mellitus (Vrijhoef et al., 2001).
In the Netherlands the work tasks performed by the DSN
can be summarised as follows: direct patient care (medical
history, physical examination, interpretation of laboratory
results, recording findings, and prevention of complica-
tions); co-ordination and organisation of care (identification
of shortcomings, referral to and communicating with other
health care-providers) and the advancement of expertise
(educating patients, other health care-providers and the
nurses themselves). Compared to general nurses, DSNs have
one of the highest qualification levels for nursing care and
are accepted nursing specialists who are focused on diabetes
care and who possess distinctive skills in this area of practice
(Vrijhoef et al., 2002).
In the Netherlands (Vrijhoef et al., 2002), USA (Valen-
tine et al., 2003), the UK (Winocour et al., 2002), and New
Zealand (Kenealy et al., 2004) the role of the DSN increases
while they enhance their position within the diabetes team
(Sigurdardottir, 1999).
According to the DSN job profile, one can expect that the
work setting of the DSN differ significantly, when compared
with nurses working in a hospital or nursing home. Since the
work organisation is of great importance to psychological
attitude, it is relevant to explore what the differences in work
organisation are and whether these differences result in
positive or negative outcomes, directly or mediated through
work aspects on psychological work reactions.
2. Theoretical perspectives on organisations, work,
and psychological work reactions
In this study, two theoretical perspectives are utilized for
the selection of work organisation, work aspects, and psy-
chological reactions, namely, the contingency approach of
organisations (Child, 1977; Galbraith, 1977; Lawrence and
Lorsch, 1967), and the Demand-Control-Support (DCS)
model (Johnson and Hall, 1988; Karasek, 1979; Karasek
and Theorell, 1990).
According to the contingency approach, design decisions
depend on environmental conditions. In addition, organisa-
tional effectiveness is achieved by organisations whose
structural characteristics, i.e. centralisation, formalisation,
and standardisation (Child, 1977; Gutek, 1990; Pennings,
1998) best match the demands of the environment or context,
i.e. environmental uncertainty (Fry and Slocum, 1984; Pen-
nings, 1998; Perrow, 1970; Rundall and Hetherington,
1988).
The DCS model (Johnson and Hall, 1988; Karasek et al.,
1981; Karasek and Theorell, 1990) is an extension of
Karasek’s Job Demand-Control (JD-C) model (Karasek,
1979). Both the JD-C and the DCS models are aimed at
generating a more profound insight into psychosocial risk
factors at work (Karasek, 1979). Following Tummers et al.
(2002), role stressors, i.e. role conflict and role ambiguity,
were added to the framework. Since these stressors may
cause job dissatisfaction and feelings of job-related strain
(Tummers et al., 2002). The relation between these theoretic
perspectives was investigated in previous research (Tum-
mers et al., 2006).
2.1. Organisational characteristics
Both structural (e.g. decision authority) and environmen-
tal characteristics (e.g. complexity and environmental uncer-
tainty) can be used to represent the work organisation in
nursing.
Complexity of care refers to such patient characteristics
as changes in a patient’s health and environmental char-
acteristics. The patient mix on a unit encompasses the
composition with regards to the specialities and patient
diversity. Diversity implies that the differences amongst
patients’ are caused by the type of disease and the level of
health problems. Diabetes management is characterised by
its complex nature and the complex health care needs of
the patients with diabetic (El Fakiri et al., 2003). Aside
from the health status of patients with type 2 diabetes, it is
even more complex with 60% of patients suffering from
co-morbidity (Charman, 2000). Whether or not this com-
plex health status leads to a complex work organisation is
unknown.

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–14321424
Furthermore, nursing units are characterised by high
environmental uncertainty or unpredictable circumstances.
In general, uncertainty indicates that there is a differentiation
between the amount of information required and the amount
of information already held by the organisation (Galbraith,
1973). In this study environmental uncertainty refers to
workflow uncertainty. As we know, nurses working in a
chronic health care setting (nursing home) exhibit signifi-
cantly lower environmental uncertainty than nurses working
in an acute health care setting (hospital) (van den Berg et al.,
2006). In general, diabetes care is not acute, but chronic by
nature. Therefore, the setting wherein diabetes care is admi-
nistered is expected to result in diminished environmental
uncertainty compared to those working in a hospital.
Decision-making authority relates to the way in which
the authority to make such decisions as ‘who is going to do
what and when’ is distributed among members of a ward
(Bodt and Van Tuijl, 1988). The concept of decision-
making authority, as applied in this study, refers to the
performance of various tasks, and the decentralisation of
decision-making. Since DSNs usually work independently,
it is most likely that decision-making authority is highest.
High environmental uncertainty and minimal decision-
making authority has a negative effect on such psycholo-
gical reactions as emotional exhaustion, intrinsic work
motivation, psychosomatic health, and job satisfaction
(Tummers et al., 2002).
The aim of this study is to explore whether the work
organisation of DSNs differs significantly from nurses work-
ing in hospital and nursing home and if so, does this
difference result in positive or negative consequences
regarding work and health. Therefore two research questions
were formulated. The first research question addressed
whether differences in work organisation, work aspects,
and psychological reactions existed between DSNs, hospital
or nursing home care. The second research question relates
to the relationship between work organisation, work aspects,
and the psychological reactions of nurses connected to the
three different settings. This question was divided into three
Fig. 1. Researc
sub-questions, as represented by Lines A, B1, B2 and C in the
research model (Fig. 1):
� L
h m
ine A demonstrates the relationship between character-
istics of the work organisation and work aspects.
� L
ine B questions whether the relationship between thecharacteristics of the work organisation and psychological
attitude is a direct relationship (B1) or an indirect one, via
the work aspects (B2), which means that the work char-
acteristics may be regarded as mediator variables.
� L
ine C represents the third sub-question, the relationshipbetween work aspects and psychological reactions.
Since the use of contingency theory in nursing is relatively
new, there are no validated questionnaires available concern-
ing environmental uncertainty, complexity, and decision-
making authority. Previous research showed insufficient psy-
chometric properties of the complexity scale in the nursing
home sample (Cronbach’s alpha was .32) (van den Berg et al.,
2006), the research question of how to improve the concep-
tualisation of work organisation was addressed as well.
3. Methods
3.1. Design and procedure
In this cross-sectional study nurses working in 15 ran-
domly selected general hospitals, 14 randomly selected
nursing homes, and 825 DSNs in the Netherlands were
asked whether they were willing to participate, after permis-
sion of the institutions director. Questionnaires were dis-
tributed in a sealed envelope together with a letter that
explained the purpose of the study and anonymity proce-
dures. After completing the questionnaires, subjects were
asked to return them in an enclosed return envelope. Parti-
cipants had been employed for at least 3 months. In the
general hospital and nursing home sample all nurses com-
plying with this criteria were included.
odel.

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–1432 1425
An approval by the Ethics Committee was not necessary.
Subjects filled in an informed consent in order to approve the
use of data for scientific research. Because all data was
retrieved from self-assessed questionnaires and no human
body tissues or species were obtained, ethical approval was
not necessary.
3.2. Samples and response
Data were collected in three samples, collected at dif-
ferent times over a period of 2 years:
Hospital nurses: One thousand eight hundred fifty-five
(1855) questionnaires were distributed among nurses from
15 hospitals. In total 1253 questionnaires were returned (a
response rate of 68%). The sample size was 1204 (nursing
staff employed for a period of less than 3 months were
excluded from the sample). The sample consisted of 1019
women (85%). The mean age of the hospital nurses was 35.7
years (S.D. = 8.7). The mean job experience was 15.5 years
(S.D. = 8.6), while the working time on the unit was 6.8
years (S.D. = 6.2).
Nursing home caregivers: One thousand eight hundred
forty-six (1846) questionnaires were distributed among
nurses from 14 nursing homes. In total 1139 questionnaires
were returned (response rate 62%). The sample size was
1058 (nursing staff employed for a period of less than 3
months were excluded from the sample). The sample con-
sisted of 963 women (94%). The mean age of the nursing
home caregivers was 35.8 years (S.D. = 9.7). The mean job
experience was 12.6 years (S.D. = 8.4), while the mean
working time on the unit was 4.6 years (S.D. = 4.8).
DSN: Eight hundred fifty-two (852) questionnaires were
distributed to DSNs in the Netherlands, 350 of which were
returned (response rate 41%). The sample consisted of 325
Table 1
Results reliability analysis for all three samples
Cronbach’s alpha
Sample 1 (general hospital)
Characteristics of the work organisation
Environmental uncertainty 0.8
Decision authority 0.7
Complexity 0.7
Work aspects
Autonomy 0.8
Workload 0.9
Social support at work 0.8
Role ambiguity 0.7
Role conflict 0.7
Psychological work reactions
Emotional exhaustion 0.9
Intrinsic work motivation 0.7
Psychosomatic health 0.8
Job satisfaction 0.9
women (93%). The mean age was 42.9 years (S.D. = 7.9).
The mean job experience was 5.82 years (S.D. = 4.6).
3.3. Questionnaire
The following variables were measured by question-
naires as part of a direct mailing. Results of reliability
analysis are shown in Table 1.
3.4. Characteristics of the work organisation
Environmental uncertainty contains items referring to
workflow and task uncertainty. One example is: ‘‘There are
daily emergency admittances on this unit’’.
Decision authority was measured in the DSN sample by
means of 3 items, ranging from 1 ‘‘totally disagree’’ to 5
‘‘totally agree’’. In the samples taken from the hospital
nurses and nursing home caregivers, the decision-making
authority scale consisted of five items. The Cronbach’s alpha
was 0.7 in the sample of hospital nurses, and 0.6 in the
sample of nursing home caregivers. Using the three-item
version – as was the case with the sample conducted of the
DSN – Cronbach’s alpha was 0.7 in the sample of hospital
nurses and 0.4 in the sample of nursing home caregivers.
Since the decision-making authority scale is in the devel-
opmental stages, descriptive questions of the work setting
were inserted to determine which improvements could be
achieved. The Pearson correlations were then calculated
between the descriptive and subjective decision-making
authority items. It can be concluded that decision-making
authority is unrelated to working in a multidisciplinary team,
the size of a multidisciplinary team, team supervisor, direct
supervisor and method used to record tasks and authorities.
Unfortunately reliability analysis on the data of the DSN
population was unsatisfactory and yielded a Cronbach’s
Sample 2 (nursing home) Sample 3 (DSN)
0.5 0.8
0.4 0.1
0.3 0.3
0.8 0.9
0.9 0.9
0.8 0.7
0.7 0.7
0.7 0.7
0.9 0.9
0.7 0.7
0.8 0.8
0.9 0.9

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–14321426
alpha of 0.1. Considering the insufficient psychometric
properties ‘decision-making authority’ was omitted from
the analyses.
Complexity was measured by means of eight items. In
both the hospital and nursing home samples, complexity was
measured by means of ten items on a five-point response
scale. Since Cronbach’s alpha emerged as unsatisfactory in
the nursing home sample, the ‘‘complexity’’ scale was
amended for use in the DSN sample. Descriptive questions
were introduced as a means of increasing the psychometric
quality, for example, questions concerning the diversity of
the patient population and the number of specialisation
fields. Then Pearson correlations were calculated between
the descriptive and subjective complexity items. This
revealed that the descriptive items had an elevated correla-
tion with the mean complexity score and the majority of
single complexity items. Furthermore, it was discovered that
when nurses are only specialised in diabetes, complexity
increases, the result of more complex and specialised tasks
being performed, for example, insulin treatment. Unfortu-
nately, Cronbach’s alpha proved inadequate in the DSN
population with (0.4) and without descriptive questions
(0.3).
In order to increase the methodological quality of the
scale in the future, a factor analysis was performed for the
complexity scale. It was concluded that a two-factor struc-
ture is the most suitable. The first factor merely consists of
items subjecting nurse specific skills. For example, ‘‘Does
the patient need emotional support and psychological help?’’
and ‘‘Do you establish patient insulin treatment instituting?’’
The second factor merely consists of situation dependent
complexity. For example, ‘‘What are the expectations in a
high risk situation?’’ and ‘‘How many care givers do you
have to deal with besides the operational doctor?’’ Con-
sidering the insufficient psychometric properties ‘complex-
ity’ was omitted from the analyses.
3.5. Work characteristics
Autonomy was measured by means of 10 items on a 5-
point response scale ranging from 1 ’very little opportunity’
to 5 ’very much opportunity’. This scale was derived from
the Maastricht Autonomy Questionnaire, abbreviated MAQ,
and was developed by De Jonge et al. (1993). Respondents
were asked to rate their work situations as to the opportu-
nities it offers for autonomy. An example of an item is: ‘‘The
opportunity that the work offers to leave your workplace
whenever you want’’.
Workload was measured by means of an 8-item ques-
tionnaire, also developed by De Jonge et al. (1993) and
ranging from 1 ’never’ to 5 ’always’. The scale consists of
both quantitative and qualitative demanding aspects in the
working situation, like working under time pressure, work-
ing hard, and strenuous work (De Jonge et al., 1993). An
example item is: ‘‘In the unit where I work, there is too little
time to finish the work’’.
Social support at work ( from colleagues and senior
nursing officer) was measured by means of a 10-item scale,
derived from a Dutch questionnaire on organisational stress
(‘‘Vragenlijst Organisatie Stress-Doetinchem’’—VOS-D;
Bergers et al., 1986). An item example is: ‘‘To what extent
can you count on your colleagues, when you have difficulties
in your work?’’ The items were scored on a 4-point response
scale format, ranging from 1 ‘‘never’’ to 4 ‘‘always’’.
3.6. Psychological work reactions
Emotional exhaustion was measured by means of the
Dutch version of the Maslach Burnout Inventory (MBI
(Maslach and Jackson, 1986)): the MBI-NL (Cox et al.,
1993; Maslach, 1993; Schaufeli and Van Dierendonck,
1993). The emotional exhaustion scale of the MBI-NL
consists of 8 items, ranging from 1 ‘‘never’’ to 7 ‘‘always’’.
An item example is: ‘‘I feel emotionally drained from my
work’’.
Intrinsic work motivation was measured by means of 6
items derived from a scale developed by Warr et al. (1979),
ranging form 1 ‘‘totally disagree’’ to 5 ‘‘totally agree’’. An
item example is: ‘‘My opinion of myself goes down when I
do this job badly’’.
3.7. Statistics
Background variables were analysed by using a descrip-
tive analysis. To gain insight into the work organisation,
aspects, and psychological reactions of DSNs in relation to
nurses employed in hospitals and nursing homes, multi-
variate analysis (ANCOVA) was carried out. Gender and age
were entered as covariates. Post hoc procedure Bonferroni
and Scheffe were used.
Hierarchical multiple regression analysis was applied in
order to investigate the relationships between: (a) character-
istics of the work organisation and work aspects, (b) char-
acteristics of the work organisation and psychological work
reactions, and (c) work characteristics and psychological
work reactions.
All the variables included in this study were standardised
to reduce problems of multi-colinearity. Two-way interac-
tion effects were tested by computing cross-product terms of
the standardised independent variables. Regression analyses
were presented separately for DSNs, hospital, and nursing
home settings.
To investigate which characteristics of work organisation
are predictable in terms of emotional exhaustion, intrinsic
work motivation, psychosomatic complaints, and job satis-
faction, hierarchical multiple regression analyses were per-
formed separately for each criterion variable. Because
gender and age were correlated with characteristics of the
work organisation, work aspects, and psychological reac-
tions, the analyses were controlled for the background
variables gender and age. The order of fit in the hierarchical
regression model was: (1) gender and age, (2) workload, (3)

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–1432 1427
autonomy, (4) social support, and (5) role ambiguity and role
conflict.
All analyses were carried out with the Statistical Package
for Social Sciences Version 11.0 for Windows (SPSS, 1999).
4. Results
4.1. Descriptives
The majority of DSNs (78%), worked in a multidisci-
plinary team, mean size 8.9 (S.D. = 6.0) members. Ninety
one percent (91%) were employed on a full-time basis. The
patient population under care was, in 7% of all cases,
‘‘younger than 18 years’’, in 45% of the cases the population
were ‘‘older than 18 years’’, and in 30% of the cases ‘‘the
patients were represented by all age groups’’. The majority
of DSNs were not specialised in any other field other than
diabetes (67%), but for those DSNs who are specialised in
other fields, the specialisation often extends to more than one
other specialisation. Registration of tasks and authorities
took place in 54% of all cases in ‘‘work description’’ or was
registered in more than one document (21%).
Table 2 demonstrates that nurses working in a general
hospital, nursing home or as DSN score significantly dif-
ferent in terms of work organisation, work aspects, and work
reactions, as determined by overall F-tests. No significant
differences in average score were found for emotional
exhaustion. Environmental uncertainty was significantly
lower in diabetes care than in both of the other settings.
DSNs exhibited the lowest workload in relation to the other
health care settings. Post hoc procedure Bonferroni and
Scheffe did not reveal any significant global differences
in mean score ( p = 0.1) for workload between DSN and
hospital nurses. In regard to autonomy, the DSN scored
highest in relation to the other health care setting. On the
Table 2
Univariate test results
Variables [number of items]
(x-point Likert scale)
Sample 1
(general hospital)
Mean (S.D.)
Environmental uncertainty [5] (5) 3.9 (.7)
Workload [10] (5) 3.3 (.5)
Autonomy [8] (5) 2.8 (.5)
Social support at work [10] (4) 3.2 (.3)
Social support supervisor [5] (4) 3.2 (.5)
Social support colleague [5] (4) 3.3 (.3)
Role ambiguity [4] (5) 2.1 (.5)
Role conflict [3] (5) 2.7 (.5)
Emotional exhaustion [8] (7) 2.2 (.7)
Intrinsic work motivation [6] (5) 4.0 (.5)
Psychosomatic health [21] (yes/no) 0.2 (.2)
Job satisfaction [21] (5) 3.5 (.4)
*p � 0.001.
contrary, the social support scores for the DSN were the
lowest in relation to the other health care settings. The DSN
scored highest for role ambiguity and lowest for role conflict.
DSNs scored highest in intrinsic work motivation and job
satisfaction, and lowest for psychosomatic ailments. There
were no significant differences in psychosomatic ailments
between the DSN and hospital nurses ( p = 0.2).
4.2. Relationships between organisational
characteristics and work aspects (Line A in Fig. 1)
Table 3 indicates relatively low percentages of the var-
iance (R2) in work aspects that were explained by work
organisation. In the DSN setting, environmental uncertainty
has a positive relation with role conflict (b = 0.2***) and
workload (b = 0.4***). From a work and health point of
view, environmental uncertainty is an indicator of negative
work characteristics (an increased workload, role conflict,
and reduced social support). In the nursing home setting,
environmental uncertainty indicates positive work aspects
(increased autonomy and less role ambiguity).
4.3. Relationships between organisational
characteristics and psychological work reactions (Line
B1 in Fig. 1)
Table 4 indicates that none of the psychological work
reactions were explained by environmental uncertainty in
the DSN setting. Emotional exhaustion was not predicted by
environmental uncertainty, in any of the settings. From a
work and health point of view, environmental uncertainty
was an indicator of positive (more intrinsic motivation) as
well as negative work reactions (more psychosomatic ail-
ments) in the hospital setting. In a nursing home setting,
environmental uncertainty has a positive influence, i.e.
higher intrinsic motivation and job satisfaction.
Sample 2
(nursing home)
Sample 3
(DSN)
F (overall)
Mean (S.D.) Mean (S.D.)
3.8 (.6) 3.7 (.7) 19.0*
3.4 (.6) 3.3 (.6) 13.8*
2.7 (.6) 3.3 (.7) 178.9*
3.3 (.3) 2.8 (.4) 270.0*
3.3 (.5) 2.7 (.5) 235.9*
3.3 (.4) 2.9 (.4) 143.5*
2.0 (.6) 2.1 (.6) 12.9*
2.5 (.6) 2.4 (.6) 28.5*
2.3 (.8) 2.2 (.8) 4.7
4.0 (.5) 4.1 (.5) 11.4*
0.2 (.2) 0.1 (.2) 13.2*
3.6 (.4) 3.7 (.4) 14.3*

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–14321428
Table 3
Relation between work organisation and work characteristics
Predictor Criterium Diabetes specialist/hospital nurse/nursing home
Beta (b) R2change
R2
1. Gender Workload .05/.12***/.00 .00/.01***/.00 .00/.01/.00
Age .05/.06*/.06
2. Environmental uncertainty .38***/.24***/.09** .15***/.06***/.01** .15/.07/.01
1. Gender Autonomy �.04/.10***/�.05 .02/.01**/.00 .02/.01/.00
Age .12*/.03/�.01
2. Environmental uncertainty .05/�.03/.08** .00/.00/.01** .02/.01/.01
1. Gender Social support �.01/�.00/.02 .00/.00/.00 .00/.00/.00
Age �.04/�.00/�.03
2. Environmental uncertainty �.08/�.07**/.06 .01/.01**/.00 .01/.01/.00
1. Gender Role ambiguity �.02/�.01/�.07* .00/.00/.00 .00/.00/.00
Age .02/�.05/�.00
2. Environmental uncertainty .03/.02/�.15*** .00/.00/.02*** .00/.00/.03
1. Gender Role conflict .00/�.04/�.03 .02*/.01***/.00 .02/.01/.00
Age �.12*/�.10***/�.01
2. Environmental uncertainty .24***/.14***/.01 .06***/.02***/.00 .07/.03/.00
*p � .05, **p � .01, ***p � .001.
4.4. Relationship between work characteristics and
psychological work reactions (Line C in Fig. 1)
Explained variances showed to be higher for emotional
exhaustion (R2 = .31) and job satisfaction (R2 = .43) com-
Table 4
Relation between organisational characteristics and psychological work r
Predictor Criterium
1. Gender Emotional exhaustion
Age
2. Environmental uncertainty
1. Gender Intrinsic work motivation
Age
2. Environmental uncertainty
1. Gender Psychosomatic complaints
Age
2. Environmental uncertainty
1. Gender Job satisfaction
Age
2. Environmental uncertainty
*p � .05, **p � .01, ***p � .001.
pared to intrinsic motivation (R2 = .05) and psychosomatic
complaints (R2 = .10) (Table 5).
Emotional exhaustion indicates a positive relation with
high workload, role conflict, and role ambiguity across all
settings. Job satisfaction was predicted by all measured work
eactions
Diabetes specialist/hospital nurse/nursing home
Beta (b) R2change
R2
�.00/�.02/�.00 .00/.00/.00 .00/.00/.00
.05/.00/�.01
.09/.05/�.01 .01/.00/.00 .01/.00/.00
.10*/.10***/.02 .02/.01***/.02*** .02/.01/.02
.05/.08**/.13***
�.02/.09**/.12*** .00/.01**/.01*** .02/.02/.03
.02/.04/.05 .00/.00/.00 .00/.00/.00
.06/�.01/.00
.10/.06*/�.03 .01/.04*/.00 .01/.01/.00
.07/.05/.01 .01/.01*/.00 .01/.01/.00
.01/.07*/�.01
�.07/�.05/.12*** .01/.00/.02*** .01/.01/.02
T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–1432 1429
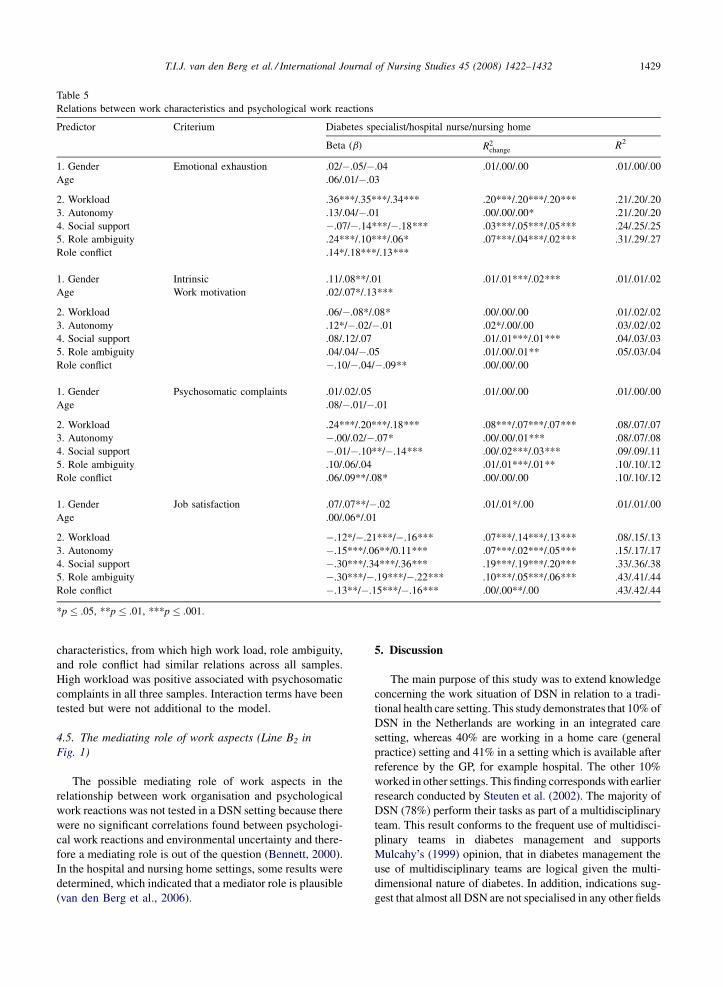
Table 5
Relations between work characteristics and psychological work reactions
Predictor Criterium Diabetes specialist/hospital nurse/nursing home
Beta (b) R2change
R2
1. Gender Emotional exhaustion .02/�.05/�.04 .01/.00/.00 .01/.00/.00
Age .06/.01/�.03
2. Workload .36***/.35***/.34*** .20***/.20***/.20*** .21/.20/.20
3. Autonomy .13/.04/�.01 .00/.00/.00* .21/.20/.20
4. Social support �.07/�.14***/�.18*** .03***/.05***/.05*** .24/.25/.25
5. Role ambiguity .24***/.10***/.06* .07***/.04***/.02*** .31/.29/.27
Role conflict .14*/.18***/.13***
1. Gender Intrinsic .11/.08**/.01 .01/.01***/.02*** .01/.01/.02
Age Work motivation .02/.07*/.13***
2. Workload .06/�.08*/.08* .00/.00/.00 .01/.02/.02
3. Autonomy .12*/�.02/�.01 .02*/.00/.00 .03/.02/.02
4. Social support .08/.12/.07 .01/.01***/.01*** .04/.03/.03
5. Role ambiguity .04/.04/�.05 .01/.00/.01** .05/.03/.04
Role conflict �.10/�.04/�.09** .00/.00/.00
1. Gender Psychosomatic complaints .01/.02/.05 .01/.00/.00 .01/.00/.00
Age .08/�.01/�.01
2. Workload .24***/.20***/.18*** .08***/.07***/.07*** .08/.07/.07
3. Autonomy �.00/.02/�.07* .00/.00/.01*** .08/.07/.08
4. Social support �.01/�.10**/�.14*** .00/.02***/.03*** .09/.09/.11
5. Role ambiguity .10/.06/.04 .01/.01***/.01** .10/.10/.12
Role conflict .06/.09**/.08* .00/.00/.00 .10/.10/.12
1. Gender Job satisfaction .07/.07**/�.02 .01/.01*/.00 .01/.01/.00
Age .00/.06*/.01
2. Workload �.12*/�.21***/�.16*** .07***/.14***/.13*** .08/.15/.13
3. Autonomy �.15***/.06**/0.11*** .07***/.02***/.05*** .15/.17/.17
4. Social support �.30***/.34***/.36*** .19***/.19***/.20*** .33/.36/.38
5. Role ambiguity �.30***/�.19***/�.22*** .10***/.05***/.06*** .43/.41/.44
Role conflict �.13**/�.15***/�.16*** .00/.00**/.00 .43/.42/.44
*p � .05, **p � .01, ***p � .001.
characteristics, from which high work load, role ambiguity,
and role conflict had similar relations across all samples.
High workload was positive associated with psychosomatic
complaints in all three samples. Interaction terms have been
tested but were not additional to the model.
4.5. The mediating role of work aspects (Line B2 in
Fig. 1)
The possible mediating role of work aspects in the
relationship between work organisation and psychological
work reactions was not tested in a DSN setting because there
were no significant correlations found between psychologi-
cal work reactions and environmental uncertainty and there-
fore a mediating role is out of the question (Bennett, 2000).
In the hospital and nursing home settings, some results were
determined, which indicated that a mediator role is plausible
(van den Berg et al., 2006).
5. Discussion
The main purpose of this study was to extend knowledge
concerning the work situation of DSN in relation to a tradi-
tional health care setting. This study demonstrates that 10% of
DSN in the Netherlands are working in an integrated care
setting, whereas 40% are working in a home care (general
practice) setting and 41% in a setting which is available after
reference by the GP, for example hospital. The other 10%
worked in other settings. This finding corresponds with earlier
research conducted by Steuten et al. (2002). The majority of
DSN (78%) perform their tasks as part of a multidisciplinary
team. This result conforms to the frequent use of multidisci-
plinary teams in diabetes management and supports
Mulcahy’s (1999) opinion, that in diabetes management the
use of multidisciplinary teams are logical given the multi-
dimensional nature of diabetes. In addition, indications sug-
gest that almost all DSN are not specialised in any other fields

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–14321430
other than diabetes (67%). This supports the finding by
Vrijhoef et al. (2002), that the DSN is highly specialised
and purely focused on diabetic care.
Some limitations must be taken into account in this study.
First, the cross-sectional design does not permit exploration
of causal relationships between work and organisational
characteristics and psychological work reactions. Neverthe-
less, the results are still of interest as they give a first insight
in influence of differences in work setting on psychological
work reactions. Second, the psychometric quality of the
organisational work characteristics was very poor. In the
DSN sample reliability analysis showed unsatisfactory
Cronbach’s alphas for decision authority and complexity.
Both variables were omitted from the analysis. The two
scales were not appropriate to measure aspects of the con-
tingency theory in nursing. Third, no non-response analyses
could be performed. The response in the DSN sample (41%)
was quite lower than in the hospital (68%), and nursing home
sample (62%). One explanation could be that nurses working
in general hospitals and nursing homes were informed by the
managers during the ward meeting about the research topic
and purpose, the data collection procedure, and the research
report. Whereas DSNs were directly invited to participate in
the study without mediation of the manager.
In general, differences in work organisation, work char-
acteristics, and psychological work reactions were significant,
although the differences were small. In regard to the work
organisation, this study revealed that the environmental uncer-
tainty is low amongst DSN in comparison to hospital nurses
and nursing home caregivers. Apparently, in the field of
diabetes nursing, more knowledge concerning workflow or
when ‘‘the inputs’’ will arrive, i.e. patient inflow exists. The
findings were as expected. In principle, the patient [visit]
schedule is known and care needs are relatively predictable.
From a work and health point of view, relatively positive
results were found regarding the work aspects of the DSN in
relation to nurses working in general hospitals and nursing
homes. For example, DSNs scored lowest on workload and
role conflict, and highest on autonomy. Despite, again it
should be mentioned differences were only minor, except
for autonomy. DSNs regard autonomy higher than hospital
nurses or nursing home caregivers. The DAWN study (Simi-
nerio et al., 2007) showed, regarding responsibilities, that
specialist nurses functioned at a more advanced level and
reported taking a more active role in facilitating both self-
management and medication management than generalist
nurses did. In Brown et al., 2001 it was mentioned that
diabetes educators express frustration over the limited author-
ity they have in caring for patients with diabetic . Despite this
frustration, the fact that they work on an independent basis is a
likely factor in the high score for autonomy, compared with
nurses working in other health care settings. Working inde-
pendently probably attributes to the low scores for social
support (from both supervisors and colleagues). Operational
tasks are performed rather independently. Personal feedback
and support is only obtained during the meetings of the
multidisciplinary team. This finding is in agreement with a
study among nurse consultants (Woodward et al., 2005) in
which specialised nurse consultants felt less social support
from their immediate colleagues than non-specialised nurse
consultants felt. This lack of social support could be decreased
by focussing on the emotional nature of support from peers
and colleagues than that of a physical presence. The knowl-
edge that the nurse can share with a peer or a manager while
alone at work under difficult circumstances should be
strengthened (Neal-Boylan, 2006). The high scores for role
ambiguity may be explained by the fact that the function of a
DSN is in the developmental stage where roles increase and
are amended. Registration of tasks and responsibilities were
available in such documents as task description (54% of all
registrations), function profile (10%) or protocol (10%).
Apparently, the registration of tasks and responsibilities are
in all likelihood, not sufficient enough to compensate this
dynamic role development.
In regard to work and health, positive results attributed to
work aspects are also identified in work reactions. This has
resulted in the highest scores being allocated to intrinsic
work motivation and work satisfaction, and the lowest scores
being allocated to psychosomatic health.
The specialised tasks of the DSN could be positive for the
experience of stress as the inability to use all of their skills on
the job was reported to cause stress in nursing home nurses
(Lapane and Hughes, 2007). Yet, equivalent univariate
analyses indicated that there were no significant differences
of emotional exhaustion between the three health care
settings examined in this study. In Charman (2000), it
was reported that DSN were at high risk of emotional
exhaustion because of their perfectionist character and the
psychosocial stressors they regularly deal with. However,
these risk factors are not specifically associated to DSN, but
rather to the nursing profession in general.
With regard to the second aim of the study, it was
disclosed that in the DSN setting, environmental uncertainty
was positive in relation to workload and role conflict. Work
organisation characteristics, decision-making authority, and
complexity could not be investigated, as the psychometric
quality of these, were not acceptable. No direct relation
exists between environmental uncertainty and the psycho-
logical work reactions. As a result, any possibility of a
mediating role of work characteristics is out of the question.
With regard to the relationship between the work character-
istics and psychological work reactions, it can be concluded
that workload was an important predictor of emotional
exhaustion and psychosomatic complaints in all three sam-
ples. From the psychological work reactions job satisfaction
was best predicted by the work characteristics, which is in
line with findings of Rafnsdottir et al. (2004) among nurses
in geriatric care. With exceptions to the negative association
between autonomy and social support with job satisfaction
in the DSN sample, results are in line with the DCS model.
Work organisation environmental uncertainty forecast
negative work characteristics (more workload and role con-

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–1432 1431
flict, less social support) in the DSN and hospital setting.
This was not true in the nursing home setting: environmental
uncertainty was a forewarning of more autonomy and less
role ambiguity. In the nursing home setting environmental
uncertainty forecast positive psychological work reactions
(more intrinsic motivation and job satisfaction). In the
hospital setting relations between environmental uncertainty
and psychological work reactions were contradictory.
These contradictory findings can probably be attributed
to the unsatisfactory psychometric quality of the work
organisation variables. Moreover, in all health care settings,
explanatory variances were low. In the DSN sample these
varied from .01 to .43.
6. Conclusions
The work of a DSN can be distinguished by certain
characteristics. From an organisational point of view, the
work setting is characterised by low environmental uncer-
tainty in comparison with nurses employed in the other two
health care settings (hospital and nursing home). Further-
more, the work of the DSN can be characterised by high
autonomy and role ambiguity, low workload, social support,
and role conflict. Relations between organisational charac-
teristics, work aspects, and psychological work reactions
indicated conflicting results due to differing psychometric
qualities of the environmental uncertainty variable. DSNs
scored most positive in regard to psychological work reac-
tions. It can be concluded that differences in the work
organisation through transition of work tasks and high
specialisation of nurses has a positive influence on the
psychological work reactions in comparison with a more
traditional health care setting.
Continued improvement of the work situation of DSNs
should focus on decreasing role ambiguity and increasing
social support. Since the nurse practitioner is the future trend
in health care (Reay et al., 2003), e.g. the DSN, it might be
expected that transition of work tasks and high specialisation
of advanced nurses or nurse practitioners have a positive
influence on psychological work reactions in comparison
with a more traditional health care setting.
Recommendations for additional work suggest a need for
the optimal measurement of organisational characteristics.
As this study reveals, scales for organisational characteris-
tics require improvement and should even be combined with
objective data related to variances in patient flow, patient
mix, and role differentiation.
References
Bennett, J.A., 2000. Mediator and moderator variables in nursing
research: conceptual and statistical differences. Res. Nurs.
Health 23, 415–420.
Bergers, G.P.A., Marcelissen, F.H.G., Wolff, Ch.J.de., 1986. VOS-
D: Vragenlijst Organisatie Stress-D: handleiding (in Dutch).
Katholieke Universiteit Nijmegen, Nijmegen.
Bodt, J.H.I., Van Tuijl, F.J.M., 1988. Aworkgroup model for nursing
wards. In: Wallis, D., de Wolff, C.J. (Eds.),Stress and Organiza-
tional Problems in Hospitals. Implications for Management. The
University Press, Cambridge, pp. 191–221.
Brown, A.W., Wolff, K.L., Elasy, T.A., Graber, A.L., 2001. The role
of advanced practice nurses in a shared care diabetes practice
model. Diabetes Educ. 27 (4) 492–496, 498–500, 502.
Charman, D., 2000. Burnout and diabetes: reflections from work-
ing with educators and patients. J. Clin. Psychol. 56 (5),
607–617.
Child, J., 1977. Organization: A Guide to Problems and Practice.
Harper & Row, London.
Cox, T., Kuk, G., Leiter, M.P., 1993. Burnout, health, work stress
and organizational healthiness. In: Schaufeli, W.B., Maslach,
C., Marek, T. (Eds.), Professional Burnout: Recent Develop-
ments in Theory and Research. Taylor & Francis, Washington,
DC, pp. 177–197.
El Fakiri, F., Foets, M., Rijken, M., 2003. Health care use by patients
with diabetic in the Netherlands: patterns and predicting factors.
Diabetes Res. Clin. Pract. 61, 199–209.
Fry, L.W., Slocum, J.W., 1984. Technology, structure, and work-
group effectiveness: a test of a contingency model. Acad.
Manage. J. 27 (2), 221–246.
Galbraith, J., 1973. Designing Complex Organizations. Addison-
Wesley Publishing Company, Reading, MA.
Galbraith, J., 1977. Organizational Design. Addison-Wesley, Read-
ing, MA.
Gutek, B.A., 1990. Work group structure and information technol-
ogy: a structural contingency approach. In: Galegher, J., Kraut,
R.E., Egido, C. (Eds.), Intellectual Teamwork: Social and Tech-
nological Foundations of Cooperative Work. Lawrence Erlbaum
Associates, Hillsdale, NJ, pp. 63–78.
Johnson, J.V., Hall, E.M., 1988. Job strain, work place, social
support, and cardiovascular disease: a cross-sectional study of
a random sample of the Swedish working population. Am. J.
Public Health 78, 1336–1342.
Jonge, J., Landeweerd, J.A., Nijhuis, F.J.N., 1993. Construction and
Validation of the Questionnaire for the ‘Job Autonomy Project’
(in Dutch). Maastricht: Bedrijfsgezondheidszorg studies: Uni-
versity of Maastricht, Maastricht.
Karasek, R.A., 1979. Job demands, job decision latitude, and
mental strain: implications for job redesign. Adm. Sci. Q.
24, 285–308.
Karasek, R.A.J., Theorell, T., 1990. Healthy Work: Stress, Produc-
tivity and the Reconstruction of Working Life. Basic Books,
New York.
Karasek, R.A., Baker, D., Marxer, F., Ahlbom, A., Theorell, T.,
1981. Job decision latitude, job demands, and cardiovascular
disease: a prospective study of Swedish men. Am. J. Public
Health 71, 694–705.
Kenealy, T., Arroll, B., Kenealy, H., Docherty, B., Scott, D., Scragg,
R., Simmons, D., 2004. Diabetes care: practice nurse roles,
attitudes and concerns. J. Adv. Nurs. 48 (1), 68–75.
Lapane, K.L., Hughes, C.M., 2007. Considering the employee point
of view: perceptions of job satisfaction and stress among nursing
staff in nursing homes. J. Am. Med. Dir. 8 (1), 8–13.
Lawrence, P.R., Lorsch, J.W., 1967. Organization and Environment.
Managing Differentiation and Integration. Division of Research,

T.I.J. van den Berg et al. / International Journal of Nursing Studies 45 (2008) 1422–14321432
Graduate School of Business Administration, Harvard Univer-
sity, Boston.
Maslach, C., 1993. Burnout: a multidimensional theory of burnout.
In: Schaufeli, W.B., Maslach, C., Marek, T. (Eds.), Professional
Burnout: Recent Developments in Theory and Research. Taylor
& Francis, Washington, DC, pp. 177–197.
Mulcahy, K., 1999. Architects of the diabetes team. Diabetes Educ.
25 (2), 161–162.
Neal-Boylan, L., 2006. An analysis of the differences between
hospital and home healthcare nurse job satisfaction. Home
Healthc. Nurse 24 (8), 505–512.
Pennings, J.M., 1998. Structural contingency theory. In: Drenth,
P.J.D., Thierry, H., de Wolff, C.J. (Eds.), Handbook of Work
and Organizational Psychology. Psychology Press/Erlbaum,
Hove, England, pp. 39–60.
Perrow, C., 1970. A framework for the comparative analysis of
organizations. Am. Sociol. Rev. 32, 194–208.
Rafnsdottir, G.L., Gunnarsdottir, H.K., Tomasson, K., 2004. Work
organization, well-being and health in geriatric care. Work 22,
49–55.
Reay, T., Golden-Biddle, K., Germann, K., 2003. Challenges in
leadership strategies for managers of nurse practitioners. J. Nurs.
Manage. 11 (6), 396–403.
Rundall, T.G., Hetherington, R.W., 1988. The social structure of
work groups. In: Shortell, S.M., Kaluzny, A.D. (Eds.), Health
Care Management: A Text in Organization Theory and Beha-
viour. John Wiley & Sons, New York, pp. 5–37.
Schaufeli, W.B., Van Dierendonck, D., 1993. The construct validity
of two burnout measures. J. Organ. Behav. 14, 631–647.
Sigurdardottir, A.K., 1999. Nurse specialists’ perceptions of their
role and function in relation to starting an adult diabetic on
insulin. J. Clin. Nurs. 8 (5), 512–518.
Siminerio, L.M., Funnell, M.M., Peyrot, M., Rubin, R.R., 2007. US
Nurses’ perceptions of their role in diabetes care: results of the
cross-national diabetes attitudes wishes and needs (DAWN)
study. Diabetes Educ. 33, 152–162.
Statistical Package For Social Sciences, Version 11 Chigago, IL,
1999.
Steuten, L.M., Vrijhoef, H.J., Spreeuwenberg, C., Van Merode,
G.G., 2002. Participation of general practitioners in disease
management: experiences from the Netherlands. Int. J. Integr.
Care 2, e24 Epub March 1 2002.
Tummers, G.E.R., Landeweerd, J.A., Van Merode, G.G., 2002. Work
organisation, work characteristics and the psychological effects on
nurses in the Netherlands. Int. J. Stress Manage. 9 (3), 183–206.
Tummers, G.E.R., Van Merode, G.G., Landeweerd, J.A., 2006.
Organizational characteristics as predictors of nurses’ psycho-
logical work reactions. Organ. Stud. 27 (4), 559–584.
Valentine, V., Kulkarni, K., Hinnen, D., 2003. Evolving roles: from
diabetes educators to advanced diabetes managers. Diabetes
Educ. 29 (4), 598–602 598–602, 604, 606 passim.
van den Berg, T.I.J., Landeweerd, J.A., Tummers, G.E.R., van
Merode, G.G., 2006. A comparative study of organisational
characteristics, work characteristics and nurses’ psychological
work reactions in a hospital setting and nursing home setting. Int.
J. Nurs. Stud. 43, 491–505.
Vrijhoef, H.J., Diederiks, J.P., Spreeuwenberg, C., Wolffenbuttel,
B.H., 2001. Substitution model with central role for nurse
specialist is justified in the care for stable type 2 diabetic
outpatients. J. Adv. Nurs. 36 (4), 546–555.
Vrijhoef, H.J., Diederiks, J.P., Spreeuwenberg, C., Wolffenbuttel,
B.H., van Wilderen, L.J., 2002. The nurse specialist as main
care-provider for patients with type 2 diabetes in a primary care
setting: effects on patient outcomes. Int. J. Nurs. Stud. 39 (4),
441–451.
Warr, P.B., Cook, J., Wall, T.D., 1979. Scales for the measurement
of some work attitudes and aspects of psychological well-being.
J. Occup. Psychol. 52, 129–148.
Winocour, P.H., Ford, M., Ainsworth, A., 2002. Association of
British Clinical Diabetologists (ABCD): survey of specialist
diabetes care services in the UK, 2000. 2. Workforce issues,
roles and responsibilities of diabetes specialist nurses. Diabetic
Med. 19 (Suppl. 4), 27–31.
Woodward, V.A., Webb, C., Prowse, M., 2005. Nurse consultants:
organizational influences on role achievement. J. Clin. Nurs. 15,
272–280.