the well-leg countertraction method details of technique
TRANSCRIPT

THE WELL#LEG COUNTERTRACTION METHOD DETAILS OF TECHNIQUE*
ROGER ANDERSON, M.D., F.A.C.S.
SEATTLE, WASH.
F RACTURES of the lower extremity utihty in both operative and non-operative and the peIvis can now be treated by a work, acting in the capacity of a fracture new method of skeleta1 traction which, table, besides serving its main function as a
FIG. IA. FIG. IB.
FIG. I. A. Fractured shaft of right femur with shortening and externa1 rotation. B. Reduction is accompIished and maintained even in sitting posture. Note that hip on injured side has been
puIIed downward by traction, forcing it into abduction, because countertraction on we11 side has displaced that hip ipwards into add&ion.
though simpler in apphcation, obtains better resuIts. The principle depends upon the utiIization of the we11 leg alone for countertraction. As neither ropes nor weights have any part in the reduction process, the weII-Ieg spIint by means of its unique leverage attachment makes possibIe the combination of skeIeta1 traction with weII-Ieg countertraction (Fig. 2). The con- struction of the splint is so perfected that, once set in operation, disarrangement is impossibIe, even with whee1 chair ambula- tion. This method reduces essentially the amount of after-care, and provides a safe mode of handIing chiIdren, the seniIe and the feebIe-minded.
This method of treatment is applicabIe to a11 fractures of the femur, incIuding the neck, intertrochanteric, subtrochanteric, the shaft and the distal third; its use extends to uniIatera1 fractures and injuries of the peIvis and a11 fractures of the tibia requiring traction. The apparatus has a
reduction agent. It provides traction and immobilization for conditions of non-union, maI-union, reconstruction and bone- Iengthening operations, and aIso for pre- ooerative and oostooerative fixation for sloliosis. l
Immediate reduction, now recognized as essentiaIIy a first principIe of fracture treat- ment, is feasibIe by this method; and since IocaI anesthesia is the genera1 order there is Iess danger in obtaining earIy reduction, and consequently the avoidance of pro- Ionged shock, pain and undue sweIIing. The mechanism of the spIint is simple, yet so perfected that reduction may be ex- peditiousIy carried out. Very littIe equip- ment is required besides spIint, steriIe set-up and pIaster materiaIs, even for the most serious case.
l Anderson, Roger. New method of empIoying skeIeta1 traction. Nortbwest Med., 30: 444-448, 1931.
New method for treating fractures, utiIizing the we11 Ieg for countertraction. Surg. Gynec. Obst., 54: zo7-zIg, February, 1932.
* Submitted for publication August 2, 19x2.
36
NEW SERIES VOL. XVIII, No. I Anderson-WeII-Leg Countertraction American JOUWI of surgery 37
In theory and in practice the counter- tract.ion splint is the very essence of inde- pendence. The great freedom of movement ahowed the patient couId not be effected were the apparatus not an entity in itseIf, working in conjunction with no other agent than the human body. The basic feature of this method is an unaIterabIe traction force, which operates regardIess of move- ment of patient, and thus since the ap- paratus is attached to neither bed nor frame, it permits the daiIy use of the wheeI- chair. This resuIts in economic as we11 as physioIogic advantages: an institution needs Iess expensive roentgenoIogic equip- ment if the patient can be moved for the taking of fiIms; a shortened period of hospitaIization is required when the trans- fer home may be safeIy made if subsequent radiographs revea1 good position. Move- ment is the keynote for maintaining me- taboIism at par and decreasing circuIatory and puImonary compIications, benelits directIy enhanced by the use of backrest and trapeze. The fact that countertraction is not obtained by Iowering the head of the bed, as the we11 Ieg aIone supplies a11 countertraction, accrues to these benefits. This freedom from restraint, change of position on bed or transportation by wheeI- chair to soIarium, so increases the patient’s genera1 resistance that he feeIs optimistic, not onIy concerning the prognosis of his case, but aIso regarding the ski11 of the surgeon, a cycIe continuously reacting to everyone’s weIfare.
APPLICATION
A hypodermic of >+$i grain morphine suIphate or without. scopoIamine, grain Maa to grain ?Baa, is usuaIIy given on entrance to the hospital. A roentgeno- graphic examination requiring two views or stereoscopic fiIms generaIIy precedes treatment, but the patient need not be taken from the cart on which he entered the hospita1 for either the fiIms or the appIica- tion of the spIint. To decrease the pain and to Iessen trauma the assistant shouId gentIy puI1 on the Ieg during any necessary
manipulation; both Iegs should be washed and any wounds dressed, preparatory to reduction.
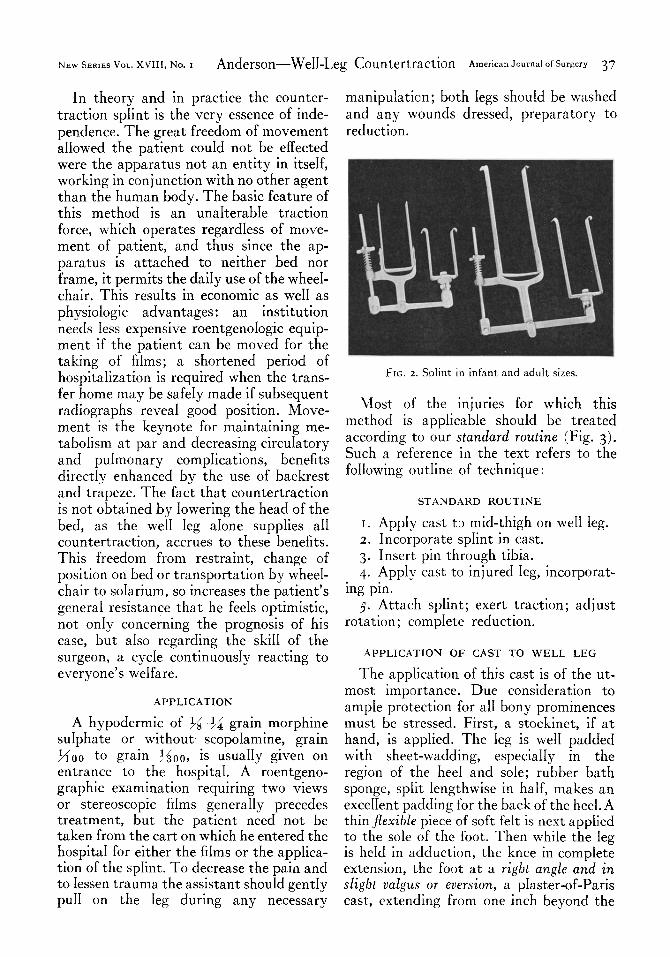
FIG. 2. SpIint in infant and adult sizes.
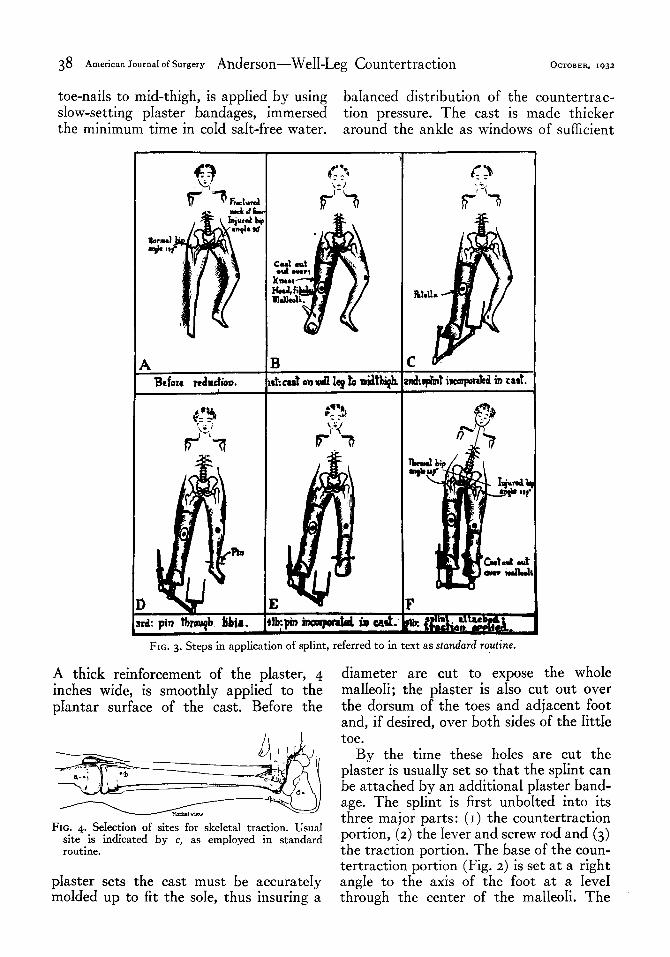
Most of the injuries for which this method is appIicabIe shouId be treated according to our standard routine (Fig. 3). Such a reference in the text refers to the folIowing outIine of technique :
STANDARD ROUTINE
I. AppIy cast to mid-thigh on we11 Ieg. 2. Incorporate spIint in cast.
3. Insert pin through tibia.
4. Apply cast to injured Ieg, incorporat- ing pm.
3. Attach spIint; exert traction; adjust rotation; compIete reduction.
APPLICATION OF CAST TO WELL LEG
The application of this cast is of the ut- most importance. Due consideration to ampIe protection for a11 bony prominences must be stressed. First, a stockinet, if at hand, is appIied. The Ieg is we11 padded with sheet-wadding, especiaIIy in the region of the hee1 and sole; rubber bath sponge, spIit Iengthwise in haIf, makes an exceIIent padding for the back of the heel. A thin flexible piece of soft feIt is next appIied to the sole of the foot. Then whiIe the Ieg is heId in adduction, the knee in complete extension, the foot at a right angle and in slight valgus or ever&on, a pIaster-of-Paris cast, extending from one inch beyond the
38 American Journal of Surgery Anderson-We&Leg Countertraction OCTOBER, ,932
toe-naiIs to mid-thigh, is apphed by using baIanced distribution of the countertrac- sIow-setting pIaster bandages, immersed tion pressure. The cast is made thicker the minimum time in coId saIt-free water. around the ankIe as windows of sufficient
Bcfotr reduction
FIG. 3. Steps in application of splint, referred to in text as standard routine.
A thick reinforcement of the plaster, 4 inches wide, is smoothIy appIied to the pIantar surface of the cast. Before the
FIG. 4. Sehtion of sites for skeIeta1 traction. Usual site is indicated by c, as empIoyed in standard routine.
pIaster sets the cast must be accurateIy moIded up to fit the soIe, thus insuring a
diameter are cut to expose the whoIe maIIeoIi; the piaster is aIso cut out over the dorsum of the toes and adjacent foot and, if desired, over both sides of the IittIe toe.
By the time these hoIes are cut the pIaster is usuaIIy set so that the spIint can be attached by an additional pIaster band- age. The splint is first unboIted into its three major parts: (I) the countertraction portion, (2) the Iever and screw rod and (3) the traction portion. The base of the coun- tertraction portion (Fig. 2) is set at a right angIe to the axis of the foot at a IeveI through the center of the malIeoIi. The

NEW SERIES VOL. XVIII, No. I Anderson-WeII-Leg Countertraction American Journal of SW~~Y 39
ffexibIe sides of the stirrup are bent by APPLICATION OF CAST TO INJURED LEG
hand to fit the cast, an equa1 amount of space being Ieft on each side between
The cast is applied to the injured Ieg with
the stirrup and the maIIeoIi to prevent the foot heId at a right angIe. The cast
pressure.
TECHNIQUE OF PIN INSERTION
When the skin over the fractured ends has been washed and shaved, it is scrubbed with ether and painted with iodine. Later remova of the iodine with aIcoho1 or the use of weaker soIutions eIiminates the possibiIity of burns. The area around the ends of the fragments is anesthetized by direct injection of 20 to 40 C.C. of 2 per cent novocaine, as used by BohIer. The ankle from 6 inches above the joint to severa inches beIow is simiIarIy prepared, after which 2 per cent novocaine is injected into the skin and down into the periosteum on each side of the tibia. The gIoves are then changed and the field draped with toweIs, in readiness for the insertion of the pin.
A seven-inch soIid Steinmann pin of stainIess steel, diameter ss inch, with a four-sided, sharp-pointed end is preferred. The pin is inserted from the media1 aspect straight through the center of the tibia, FIG. 5. These agents plus sptint and pIaster materia1 are
on a level two fingers’ breadth superior to 0nIy requisites for usua1 fracture case.
the tip of the internal malleolus (Fig. 4). This occasions no preIiminary incision of extends from one inch beyond the toenaiIs the skin, or drihing of the bone for, if the up to a IeveI 5 inches beIow the knee joint, pin is sharp, it can be forced through by firmIy incorporating the pin (Fig. 3~ ). rotary hand-pressure aIone (Fig. 3 D). The Ieg is first we11 padded with sheet- A three-inch steriIe gauze sponge is spiked wadding and a four-inch plaster reinforce- over the pin, down against the skin on each ment is appIied to the soIe of the foot and side, another piece of gauze about $$ by 1% the cast cut out over both malIeoli. inches being twisted around the pin-ends to The perforations of the traction stirrup absorb any moisture running down the pin are now connected with the pin-ends, and contaminating the wounds. The drapes those holes seIected which permit the spIint are removed and excess iodine is washed off to set up most compactly against the with aIcoho1. Sheet-wadding, 3 inches in pIantar portion of the cast (Fig. I). The width, wrapped over the pin and around traction portion is fastened to the cast the Ieg, suffices to hoId the dressing cIose by pIaster bandage, the pin-ends protected to the skin, bandage or adhesive being by ordinary corks before being covered entireiy unnecessary. No other prophyIactic with pIaster. Therefore, unless informed against infection is required except to of the transfixion, the patient shouId be Ieave the wounds entirely aIone throughout entireIy unaware of the pin unti1 its the period of immobiIization. removal.

FIG. 6~. FIG. 6~. FIG. 6c.
of ed.
F
A. B.
cast. C.
FIG. 6~. FIG. 6~. :IG. 6. Steps of standard routine. Patient, sixty-five years of age, has fractured neck of right femur.
Cast to we11 Ieg. D. Incorporation of pin in cast. Countertraction portion of splint incorporated in E. Traction portion of splint attached to cast
injured leg. Traction and rotation have been appIi Pin inserted through Iower end of tibia. Fracture now reduced.
I[401

NEW SERIES VOL. XVIII, No. I Anderson-WeII-Leg Countertraction American journal of surgery 4 I
After boIting together the component and feet of the patient are drawn to either
parts of the apparatus, the next step is to the Ieft or right side of the tabIe, corre- generate traction force by screwing down sponding to the same side as that of the
FIG. 7A. FIG. 7~.
FIG. 7. hirs. L. C. Comminuted fracture of Ieft acetabuIum and left ischium with central dispIacement of head !into pelvis, non-reducible by either manipulation or by Buck’s extension.
A. Before reduction. B. After reduction with splint. Patient was removed without pain to x-ray room and, as this fiIm shows, there
was no disturbance of reduction.
FIG. 8~. FIG. 8~.
FIG. 8. hlrs. I. LaF., aged fifty-eight years. Fractured neck of Ieft femur, which was not detected for seven weeks and, therefore, received no treatment. Patient even tried to walk on it.
A. Before reduction. B. FiIm taken day foIIowing appIication of splint.
the traction nut (Fig. 3 F). Correct aIign- injury, whiIe the hips are dispIaced toward ment, by either interna or externa1 rota- the opposite side of the tabIe. This position, tion, is obtained by operating the rotation if maintained in bed, permits the spine, nut (Fig. I). When the lever arm is drawn paradoxical as it may seem, to set at right down to a right angle with the longitudinal angIes on the peIvis. axis of the legs, suficient traction has usually At this time, or within a short whiIe, been exerted. Meanwhile both the head reduction shouId be checked by radio-

42 American Journal of surgery Anderson-WeII-Leg Countertraction OCTOBER, 1932
graphs, and traction and rotation changed as indicated. A few hours after the patient is returned to his room, the cast shouId
FIG. g. Patient, with fracture of Ieft hip, was up within a few days after appIication of spIint.
the trapeze freeIy; in a day or so he wiI1 be abIe to raise himself up for necessities of toilet. If the patient with a hip fracture is not in a condition of shock, the wheeI- chair is often provided as earIy as the second or third day. The subject with heart troubIe can safely be ahowed to sIeep in a sitting or recIining position; patients with hip and intertrochanteric fractures may be turned on the abdomen daiIy.
After-care is at the minimum; very little is required except perhaps to cut out over the hee1, the IittIe toe or the dorsum of the foot, or to spIit the upper rim of the cast. A11 or most of the anterior portions of both casts may be removed as conditions direct. The nurses and the patient aIso shouId be instructed to massage the knee joints and to move the knee-caps daiiy. It is advisable to repeat the roentgenograms as indicated.
FIG. IOA. FIG. IOB.
FIG. IO. Mrs. E. H. Comminuted right intertrochanteric fracture. A. Before reduction. B. X-rays taken immediateIy after appIication, according to standard routine.
be cut out over the posteroIatera1 aspect If subsequent radiographs in both views of the head of the fibuIa and the anterior or stereos verify good position, the patient side of the knee joint. may be removed home.
AFTER-CARE TIME AND MANNER OF REMOVING PIN
The patient is not onIy permitted to No attempt shouId be made to dress sit up but encouraged to do so and to use the pin-wounds from the time of the

NEW SERIES VOL. XVIII,‘No. 1 Anderson-We&Leg Countertraction American Journal of Surgery 43
insertion unti1 the remova of the pin, tures, seven to nine weeks; subtrochanteric whether this be a one-month or a four- fractures, seven to ten weeks; fractures month interva1. of the femoral shaft, five to ten weeks:
FIG. IIA
FIG. IIB. FIG. IIC.
FIG. II. Baby B., fifteen months old. Fractured shaft of right femur; application of spIint and perfect reduction obtained by Dr. L. G. Woodford.
A. Before reduction. B. After reduction. c. Final result.
The time of removal of the pin depends upon such factors as the age of the patient, the Iocation and type of fracture and caIIus formation. In generaI, the foIIowing sched- ule for the period of traction is adhered to: fractures of the peIvis, four to six weeks; fractures of the neck of the femur, tweIve to fourteen weeks; intertrochanteric frac-
fractures of the dista1 third, five to ten weeks; fractures of the tibia, four to tweIve weeks; and operative’cases, six to eighteen weeks.
The patient is unconscious of a secureIy incorporated pin; hence pain in this region is usualIy occasioned by Iooseness of the pin in the cast, a condition caIIing for
44 American Journal of Surgery Anderson-Well-Leg Countertraction OCTOBER, 1932
correction. In fact most patients are unaware of even the presence of the pin, when covered by a cast. Because of the
removed with aIcoho1, but if any iodine escapes beyond the pin-wound, the cast shouId be further cut and the iodine
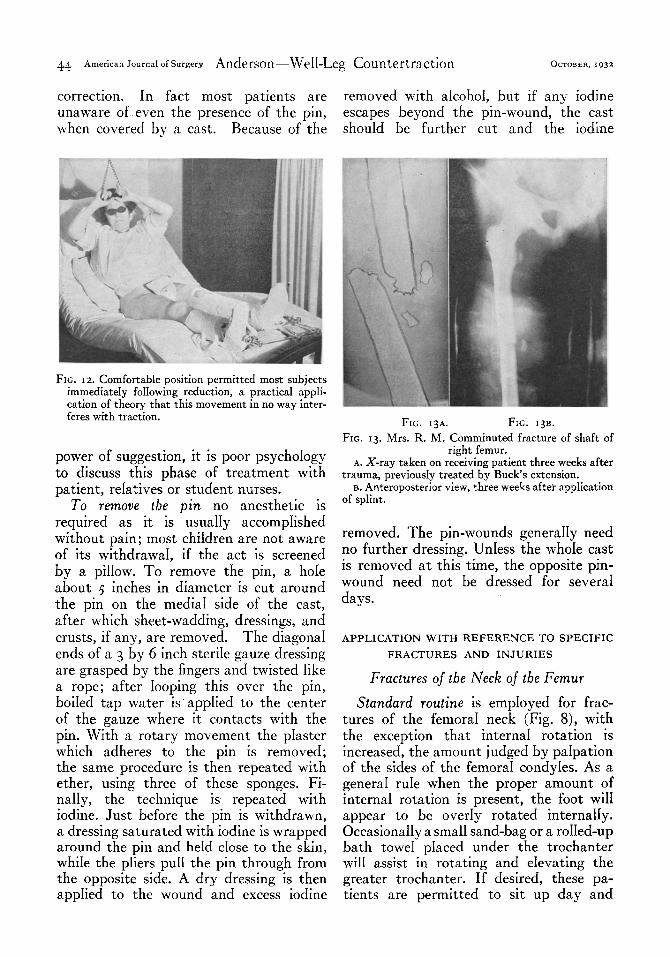
FIG. 12. ComfortabIe position permitted most subjects immediateIy foIIowing reduction, a practica1 appIi- cation of theory that this movement in no way inter- feres with traction.
power of suggestion, it is poor psychoIogy to discuss this phase of treatment with patient, reIatives or student nurses.
To remove the pin no anesthetic is required as it is usualIy accompIished without pain; most chiIdren are not aware of its withdrawa1, if the act is screened by a piIIow. To remove the pin, a hoIe about 5 inches in diameter is cut around the pin on the media1 side of the cast, after which sheet-wadding, dressings, and crusts, if any, are removed. The diagona1 ends of a 3 by 6 inch steriIe gauze dressing are grasped by the fingers and twisted Iike a rope; after Iooping this over the pin, boiIed tap water is appIied to the center of the gauze where it contacts with the pin. With a rotary movement the pIaster which adheres to the pin is removed; the same procedure is then repeated with ether, using three of these sponges. Fi- naIIy, the technique is repeated with iodine. Just before the pin is withdrawn, a dressing saturated with iodine is wrapped around the pin and heId close to the skin, whiIe the pIiers puI1 the pin through from the opposite side. A dry dressing is then appIied to the wound and excess iodine
FIG. 13~. FIG. 13~.
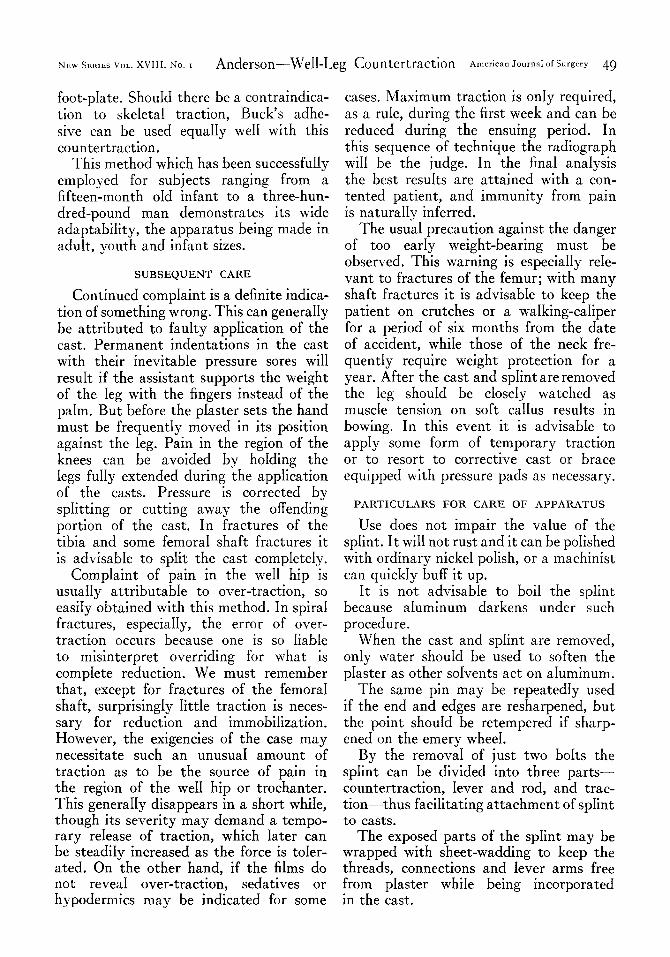
FIG. 13. Mrs. R. M. Comminuted fracture of shaft of right femur.
A. X-ray taken on receiving patient three weeks after trauma, previousIy treated by Buck’s extension.
B. Anteroposterior view, three weeks after apprication of spIint.
removed. The pin-wounds generaIIy need no further dressing. UnIess the whoIe cast is removed at this time, the opposite pin- wound need not be dressed for severa days.
APPLICATION WITH REFERENCE TO SPECIFIC
FRACTURES AND INJURIES
Fractures of the Neck of the Femur
Standard routine is empIoyed for frac- tures of the femora1 neck (Fig. 8), with the exception that interna rotation is increased, the amount judged by paIpation of the sides of the femora1 condyIes. As a genera1 ruIe when the proper amount of interna rotation is present, the foot wiII appear to be overIy rotated internaIIy. OccasionaIIy a smal1 sand-bag or a roIIed-up bath towe pIaced under the trochanter wil1 assist in rotating and eIevating the greater trochanter. If desired, these pa- tients are permitted to sit up day and

NEW SERIES VOL. XVIII, No. I Anderson-WeII-Leg Countertraction American JOUST of Surgery 15
night, and within a day or so are accorded the use of the wheeI-chair.
Intertrochanteric Fractures
Since fractures of the neck require Iittle Treatment here is aIso according
standard routine (Fig. IO), except that ; to it is
FIG. 14. Original method of treating supracondybr fractures.
traction, each week the force may be safeIy decreased up to that point whereby aIignment is stiI1 maintained, thus insuring pressure contact between the fractured surfaces. Over-traction with its dangers, especiaIIy non-union, must be guarded against, the radiograph being the supreme arbiter in regard to retaining end-to-end contact and preserving the normal cervica1 angle. Stereoroentgenograms have been regarded as the desired test but CIayton Johnson’s Iateral technique gives additiona check. If these principIes are cIoseIy adhered to, better end-results with fewer cases of non-union wiI1 be attained, for this system controls these factors as does no other method.
usuaIIy best to fix the thigh in externa1 rotation, the degree determined by study of stereoscopic or Iateral roentgenograms. In the cornminuted variety, especiaIIy where the Iesser trochanter has been fractured off and puIIed upward by the iIiopsoas muscIe, approximation of the fragments may necessitate a sitting posi- tion day and night in bed or wheel-chair. Some of these cases require eIevation of the legs on a pile of piIIows or box. This ffexion assists in reduction; but perfect reduction of the Iesser trochanter is un- necessary as the main objective is union of the femora1 shaft, and good function can be obtained without norma reposition of a11 fragments.

46 American Journd of Surgery Anderson-We&Leg Countertraction OCTOBER, 1932
Free use of trapeze and wheel-chair, even on the day of reduction, and shortened hospitahzation are not incompatibIe with excehent results.
Subtrochanteric Fractures
In these fractures standard routine is deviated from, as the pin is forced through the center of the femur at a IeveI g inch above or superior to the medica condyIe. Transfixion shouId be approximateIy straight through, but if the pin does not emerge at about the same IeveI on the opposite side, it is occasionaIIy best to withdraw and reinsert it, checking by Mm if necessary.
The pin is incorporated in the cast, which is extended just above the pin or to the groin, as conditions indicate. The cast on the we11 Ieg is usuaIly extended up to the groin, since these stubborn fractures may necessitate fastening specia1 pressure pads to this cast. 2 In many cases better apposition is accompIished by eIevation of the legs on piIIows or by a sitting posture.
Since the perforated sides of the traction stirrup sIip over the pin when the insertion is through the Iower tibia, one may seem to be confronted with an apparentIy too short stirrup when adapting the method to femora1 transfixion. This probIem has been solved by curving out the ends of the stir- rup so that it is bound and fastened so secureIy in the pIaster that it cannot be puIIed out. Hence traction puI1 is trans- mitted up to the pin by the solid interven- ing cast.
Fractures of the Shaft of the Femur
Technique foIIows standard routine with the foIlowing provisos: an 8-inch pin is inserted through the femur, while the cast on the we11 leg is occasionally extended to the groin (Fig. 13). The splint connection between stirrup and pin is made in the manner described under subtrochanteric fractures.
If difficulty is encountered in obtaining apposition, the dista1 fragment can be
* The subject of a paper to be later pubhshed.
directIy controhed by cutting out the cast from around the ends of the pin in order to permit direct readjustment of the frag- ment by manipuIation of the pin. After the desired position is attained, the pin is refastened by pIaster bandage. A pressure pad, attached after exposing the fracture site through the casts, is aIso instrumenta in effecting readjustment.2
AIthough the trapeze is permitted after the first few days, the use of the wheeI- chair is dependent upon caIIus formation.
Fractures of the Lower Third of the Femur
For this diffrcuIt cIass of fractures, which incIude the supracondyIar and intercondy- Iar, the technique is sIightIy aItered.3 After-care is practicaIIy the same as for shaft fractures. The folIowing steps in reduction are iIIustrated by Figure 14.
I. First, the pin is inserted through the dista1 end of the femur (Fig. 14~). Traction made upon the pin in an anterior direction forces the distal fragment of the femur into the same straight Iine with the tibia, bringing the knee into fuI1 extension (Fig.
I4C).
2. The cast is appIied from a IeveI 4
inches above the ankIe to I inch above the pin; this incorporates the pin and aIso holds the distal femoral fragment and the tibia in the same straight Iine (Fig. 14~).
3. After this segment of the cast is set, the foot is forced up to a right angle whiIe the cast is extended slightIy beyond the toenails (Fig. 14~). HoIes are then cut over the maIIeoIi.
4. The traction stirrup is incorporated in the dista1 end of the cast (Fig. 14~) ; trac- tion is then applied and rotation corrected.
5. The cast is finalIy extended from the pin to the groin (Fig. 14G)..
If the fracture extends T-shaped into the joint, the condyIar fragments must first be aligned before the transverse fracture is reduced. Should these fragments be widely separated from each other, the
3 Anderson, Roger. New method of treating femora1 fractures in the dista1 third. (In press.)

NEW SERIES VOL. XVIII, No. I A n d erson-WeII-Leg Countertraction American Journal of Surgery 47
medial or IateraI displacement is first After-care instructions reIevant to this corrected by a speciaIIy threaded pin, the cIass of fractures in&de the placing of a technica detaiIs being given in the author’s fracture-board beneath the mattress, and
FIG. 15. Reading from Ieft to right: Mrs. N. S., aged eighty-six years, with neck of femur fracture, was turned on stomach daiIy; Mrs. M. S. sat up day and night because of asthma; Mrs. M. M., with fracture of right hip, made daiIy use of wheeLchair; Master J. H., cornminuted fractures of middIe and upper third of right femur. Pin was inserted through d&a1 end of femur.
monograph as noted above. By inserting a pair of sIiding “sIeeves” the fragments are forced together and heId as in a vise.
Fractures of the Pelvis
Standard routine, as previousIy outIined, is the procedure for peIvic fractures. AIthough the method is suited for uni- IateraI fractures of the peIvis (Fig. 7), it may be used in biIatera1 fractures when the fractures are Iimited to ischium or pubic bones on the opposite side from that of the major peIvic fracture. In fact it can even be used in muItipIe fractures of the peIvis provided there has been no injury to that smaI1 area between the sacroiIiac joint and the acetabulum on the we11 side. In injury or disIocation of one sacroiIiac joint or in separation of the symphysis pubis, the sphnt has aIso proved successfu1.
a pad or baby-piIIow under the smaI1 of the back for support. In most cases these patients are neither permitted to sit up nor are they turned over during the first three to six weeks.
Fractures of the Tibia
Standard routine is empIoyed for al1 tibia1 fractures caIIing for continuous traction, but over-traction should be avoided since very IittIe force is needed for this type of fracture. If a compound wound extends too near the ankIe-joint, the pin is inserted through the OS caIcis.
For that cIass of tibia1 fractures which require traction for reduction onIy, pro- vided a snug-fitting cast be appIied for fixation, the spIint serves in the capacity of a fracture tabIe and is appIied in the foIIowing manner. Standard routine is adopted for the we11 Ieg; the pin is inserted above the ankIe or through the OS caIcis,

48 American Journal of Surgery Anderson-WeII-Leg Countertraction OcroaER, 1932
the cast on the injured Ieg extending just up to the fracture, incorporating the pin. The traction stirrup is then shpped over the pin and incorporated. If the ends extend above the cast they are turned back, thus permitting free adjustment of the upper fragment under traction.
The spIint is then assembIed and traction force exerted. Since the cast does not encompass the fracture site, the fragments may be manipuIated into position and the necessary rotation effected. After satisfactory reduction is accomplished, the cast is extended up 6 inches above the knee. Traction force may be subsequentIy re- leased; if roentgenographic examination shows that the fracture remains reduced, the weII-Ieg cast and splint may be removed, Ieaving the traction stirrup onIy in the cast of the injured member. Thus the apparatus has served as an orthopedic traction tabIe.
A modification of the weII-Ieg method, for quick appIication without the use of plaster bandages, wiI1 be reported on Iater. For this purpose we have designed an aIuminum countertraction sheI1, Iined with rubber, to fit the soIe of the aduIt foot and the posterior side of the leg where it is secured by straps. This device permits either wire or pin for skeIeta1 traction.
Mal-union, Non-union, Bone-lengthening, Hip and Reconstruction Operations
AIthough standard technique is cIoseIy adhered to in these operations, the pin may transfix the femur, with the cast extending 2 inches above the pin. Pin, cast and splint are generaIIy appIied a day or so previous to the operation, to afford opportunity for the cast to dry and for the patient to become accustomed to this position. Before commencing to operate, a fair amount of traction force is usuaIIy generated, and the circuIating nurse shouId be instructed how tq manipuIate the splint for further extension and rotation. The fact that the patient can be turned on his side or over on his abdomen for better operative exposure is a decided advantage,
especiaIIy so since it in no wise interferes with traction. By removing a singIe boIt one may have free use of the leg for wide manipuIation; the bolt can be quickIy reinserted when traction and immobiIiza- tion are again desired.
After the bone-graft is fastened in pIace and the skin sutured, in most cases the patient can be safeIy removed to bed. However, it may be necessary to extend the cast up to the groin over an operated femur. Under such conditions as in oId, unilatera1 congenita1 hips, where a new acetabuIum has been reconstructed, it may be advisable to extend the cast to the Iower Costa1 margin on the injured side in order to prevent the patient from sitting up. However, the,necessary trac- tion must be exerted before the body portion of cast is appIied. Some cases caI1 for operation through a Iarge opening cut in the cast; the scoIiotic spine responds to this type of treatment. It is cIearIy seen that the spIint and cast apportion- ment conforms to whatever surgica1 prob- Iem presents itself.
ScoIiosis, especially that of the Iumbar spine, whether idiopathic or secondary to poIiomyeIitis, can be sIowIy adjusted or corrected by means of this spIint. But the cast on the we11 Ieg is extended up over the body in the form of a spica cast, before any traction is appIied. This correc- tive agent can‘be empIoyed for some time before operation, which may be performed through a Iarge opening in the cast. On the other hand, fusion operation may be performed first. The spIint is Iater appIied according to standard routine with the extension of the cast upwards to the mid- dorsa1 region, after which traction, the corrective force, is exerted.
ADAPTATION AND SIZE OF SPLINT
The spIint has been so constructed that it works equaIIy we11 with other forms of skeIeta1 traction than the pin. Moreover, the pin, wire or tongs need or need not be incorporated in the cast; for the Tatter the sprint is equipped with an adjustabIe
NEW SERIES VOL. XVIII, No. 1 Anderson-Well-Leg Countertraction American Journal of Surgery 49
foot-plate. Should there be a contraindica- tion to skeletal traction, Buck’s adhe- sive can be used equaIIy we11 with this countertraction.
This method which has been successfully employed for subjects ranging from a fifteen-month oId infant to a three-hun- dred-pound man demonstrates its wide adaptabiIity, the apparatus being made in adult, youth and infant sizes.
SUBSEQUENT CARE
Continued complaint is a definite indica- tion of something wrong. This can generaIIy be attributed to faulty appIication of the cast. Permanent indentations in the cast with their inevitabIe pressure sores will result if the assistant supports the weight of the Ieg with the fingers instead of the palm. But before the pIaster sets the hand must be frequently moved in its position against the Ieg. Pain in the region of the knees can be avoided by hoIding the legs fully extended during the application of the casts. Pressure is corrected by splitting or cutting away the offending portion of the cast. In fractures of the tibia and some femoral shaft fractures it is advisabIe to split the cast completely.
CompIaint of pain in the we11 hip is usuahy attributabIe to over-traction, so easiIy obtained with this method. In spiral fractures, especiaIIy, the error of over- traction occurs because one is so Iiable to misinterpret overriding for what is compIete reduction. We must remember that, except for fractures of the femora1 shaft, surprisingIy Iittle traction is neces- sary for reduction and immobiIization. However, the exigencies of the case may necessitate such an unusua1 amount of traction as to be the source of pain in the region of the we11 hip or trochanter. This generaIIy disappears in a short whiIe, though its severity may demand a tempo- rary reIease of traction, which Iater can be steadiIy increased as the force is toIer- ated. On the other hand, if the films do not revea1 over-traction, sedatives or hypodermics may be indicated for some
cases. Maximum traction is onIy required, as a rule, during the first week and can be reduced during the ensuing period. In this sequence of technique the radiograph will be the judge. In the fina analysis the best resuIts are attained with a con- tented patient, and immunity from pain is naturally inferred.
The usua1 precaution against the danger of too early weight-bearing must be observed. This warning is especiaIly reIe- vant to fractures of the femur; with many shaft fractures it is advisabIe to keep the patient on crutches or a waIking-caliper for a period of six months from the date of accident, whiIe those of the neck fre- quently require weight protection for a year. After the cast and splint are removed the leg shouId be closely watched as muscle tension on soft caIIus resuIts in bowing. In this event it is advisabIe to apply some form of temporary traction or to resort to corrective cast or brace equipped with pressure pads as necessary.
PARTICULARS FOR CARE OF APPARATUS
Use does not impair the vaIue of the spIint. It will not rust and it can be polished with ordinary nickel polish, or a machinist can quickIy buff it up.
It is not advisable to boil the splint because aIuminum darkens under such procedure.
When the cast and splint are removed, only water should be used to soften the pIaster as other soTvents act on aluminum.
The same pin may be repeatedly used if the end and edges are resharpened, but the point should be retempered if sharp- ened on the emery wheel.
By the remova of just two boIts the spIint can be divided into three parts- countertraction, Iever and rod, and trac- tion-thus faciIitating attachment of spIint to casts.
The exposed parts of the spIint may be wrapped with sheet-wadding to keep the threads, connections and Iever arms free from pIaster whiIe being incorporated in the cast.

50 American Journal of Surgery Anderson-We&Leg Countertraction OCTOBER, 1932
IMPORTANT TECHNICAL CONSIDERATIONS
I. HoId the we11 Ieg in adduction at the hip whiIe applying the cast.
2. HoId the we11 foot at right angIes with the foot in sIight valgus (eversion or pronation of the foot).
3. Pad the soIe of the we11 foot with thin, soft, jlexible felt and with a goodIy amount of sheet-wadding. A four-inch re- inforcement of pIaster shouId be smoothIy appIied over the entire pIantar surface of the cast on the we11 foot; this should be moulded accurateIy to fit the soIe.
4. Cut suficiently Iarge openings in the cast over the maIIeoIi of both injured and uninjured ankIes before incorporating the spIint.
5. The cast shouId be cut out Iater over the posteroIatera1 aspect of the head or heads of the fibuIae.
6. Pain or troubIe with the we11 Ieg is usuaIIy attributabIe to careIess appIication of the cast. Continued compIaint demands a change of cast. Pain in the region of the we11 hip is usuaIIy indicative of too rapid or too much traction. In most cases when the Iever arm is drawn down at a right
angIe with the Iongitudinal axis of the Ieg, the requisite amount of traction has usuaIIy
been exerted. 7. Avoid over-traction, especiaIIy in frac-
tures of the femora1 neck, by checking
with repeated roentgenograms. Over-trac- tion is a frequent cause of non-union.
8. Remember the warning of the Co- operative Committee on Fractures : “ It is the doctor behind the splint and not the spIint that counts in the treatment
of fractures.”
REFERENCES OF DR. WATSON*
6. EURICH, F. W., and PHILLIPS, J. Acute phlegmon- 18. NEUHOFF, H., and COHN, I. Abdominal puncture
ous gastritis. Lancet, r : 910, 1921. in diagnosis of acute intraperitonea1 disease.
7. FINK, E. B. PhIegmonous gastritis. Boston M. und Ann. Surg., 83: 454-462, 1926.
S. J., 175: 795, 1916. rg. OWEN, D. R. Acute phIegmonous gastritis. Lancer,
8. GERSTER, J. C. A. Phlegmonous gastritis. Ann. I : 865, 1926.
Surg., 85 : 681-682, 1927. 20. PAUGCER, H. Beitrag zur Gastritis PhIegmonosa.
g. GERSTER, J. C. A. Phlegmonous gastritis. Med. Deutscbe Ztscbr. j. Cbir., 210: 368-380, 1928.
Rec. of N. Y., 95: 502, IgIg. 21. RANKIN, F. W., and MILLER, C. D. Intramural
IO. LAWRENCE, J. S. Phlegmonous gastritis. Boston M. and S. J., 195: 800-803, 1926.
II. LEHNHOFF, H. J. PhIegmonous gastritis. J. A. 22.
M. A., 68: 966, 1917. 12. MOYNIHAN, B. Acute phIegmonous gastritis. Brit.
J. Surg., IO: 43, 1922. 23.
13. MONGIN, R. Phlegmonous gastritis. Vracb. dielo., 2: 326, 1928.
abscess of the Iesser curvature of the stomach. Mayo Clinic Bull., May 6, 1931, p. 278.
ROSE and CARLESS. Acute phlegmonous gastritis. ManuaI of Surg. Ed. IO, N. Y., Wood, 1922, p. 1102.
14. MACAULEY, C. J. Acute phIegmonous gastritis. 24.
Brit. J. Surg., IO: 38-42, 1922. 15. MEYER, K. A., BRAMS, W. A., and GUY, C. PhIeg-
25.
monous gastritis (anatomica and cIinicaI study 26, of two cases). Surg. Gynec. Obst., 44: 301-307,
1927. 16. MORTON, J. J., and STABINS, S. J. PhIegmonous 27.
gastritis of baciIIus aerogenes capsuIatus (B. weIchii) origin. Ann. Surg., 87: 848-854, 1928. 28.
17. NOVAK, E. Circumscribed phIegmonous gastritis (submucous abscess of stomach). J. A. M. A., 29. 73: 1038, rgrg.
ROBSON and MOYNIHAN. SurgicaI Treatment of Diseases of the Stomach. Ed. 2, N. Y., Wood,
1904, PP. 463-496. REXFORD, E. PhIegmonous gastritis. Trans. Am
Surg. A.&n., 25: 472. 1927. ROBB, D. PhIegmonous gastritis. J. Coil. Surg.,
Australasia, 3: 122-123, 1930. SCHAEFER, V. Gastritis phIegmonosa mit subseroser
eitriger Lymphangitis. Bruns. Beitr. z. clin. Cbir., 146: 526-529, 1929.
SHATARA, F. I. PhIegmonous gastritis. J. A. M. A., 71: 2130, 1918.
WEINSTEIN, M. L., and KLEIN, J. PhIegmonous gastritis. Ann. Surg., 86: 534-539, 1927.
WESTABROOK, R. W. Phlegmonous gastritis. Long Island M. J., IO: 525, 1916.
*Continued from p. 122.