the vizient/aacn nurse residency program™ at …...the vizient/aacn nurse residency program at...
TRANSCRIPT
The Vizient/AACN Nurse Residency Program™
at UCLA Health System
The Journey of Your First Year Begins…Nurse Residency Program CoordinatorDr. Arika Duchene, DNP, RN-BC, CCRN
Updated May 2016, Jessica Phillips

General Overview
• The Journey Begins• Professional Practice• Evidence Based Practice• Challenges and Opportunities• Levels of Nursing Competency• Establishing Credibility• Communication• Getting Help and Getting Ahead• Diversity • Closing Comments
2

Learning Objectives• Describe what it means to be a UCLA nurse
• Explain the levels of nursing competency
• Verbalize effective strategies to establish credibility and facilitate productive
communication– “getting help and getting ahead”
• Identify dimensions of diversity in self, patients, and staff
• Apply evidence-based strategies related to cultural competence to effectively manage
clinical issues to ensure patient safety and high-quality outcomes of care for diverse
populations (to be initiated on your units)
• Identify appropriate language assistance services to achieve mutual understanding with the patient/family (to be
initiated on your units)
• Identify appropriate resources for patient care delivery and resource management (to be
initiated on your units)
3

The Journey Begins
• Today’s nurse assumes more autonomy and responsibility • Nursing is a dynamic profession where you will be faced with
challenges and opportunities on a daily basis• Due to the ever evolving changes and advances in healthcare,
nurses are called upon to use more advanced critical thinking, assessment, and technology skills
• Phase #1 was Nursing School– Theory and Knowledge • Phase #2 is NRP – Application of Previous and New Knowledge
4

Professional Nursing Practice
• What is a nursing professional practice model? • Why do we need a nursing professional practice model?
5
Professional Nursing Practice:The Maria O’Rourke Accountability Model - O5
1. Obligation2. Ownership3. Oversight4. Outcomes5. Opportunity
© 2012 Role-Based Practice Solutions. All Rights Reser

Challenges and Opportunities
• Large Group Brainstorm: What challenges/concerns do you face?
7

Challenges and Opportunities• Limited financial resources and school loans• High acuity/sick patients• Increased demands• Did I make the right decision/Is this the right career for me?• Can I handle the responsibility?• Separation from school/friends/family• No longer having the structure of school• Inexperience• Will the staff accept me?• Reality shock: crisis of identity when values and system in the
workplace do not match with what we learned in school (attrition rate of these nurses significantly high)
8

• This is normal !!!
• At the end of the shift, you will know more and be more experienced than you were at the beginning
• Maintain a journal and reflect on your process
• Make a long term plan and set small, realistic goals
• You are not expected to know everything
• You ARE expected to: ask questions, develop critical thinking, be accountable, take responsibility, and be an active participant
• Keep yourself open to opportunities to learn and grow
9
Challenges and Opportunities
Levels of Nursing Competency
• There are five levels of competency in clinical nursing practice:
• Novice – *where you are now*
• Advanced beginner
•Competent *(our goal at the year milestone)*• Proficient
• Expert
10

From Novice to Expert
11
Novice Nurse WHERE YOU ARE RIGHT NOW
• Nurse residents enter into the NRP with the requisite theoretical knowledge
• Need clinical/situational experience to apply intuition, clinical judgment, contextual knowledge of nursing practice and care delivery
• Nurses new in the profession function by rule-governed behavior• Will lack the ability to recognize and interpret information without situational
experiences that provide higher level skill acquisition
• Novice nurses’ learning is framed by their feelings about the experience in the context of the practice environment
12

Advanced Beginner NurseLess than 1 year experience
• Graduate nurses will move into this next phase when they can demonstrate acceptable performance and have enough experience to begin detecting patterns of patient response
• Still not able to take in the entire situation without getting overwhelmed by the volume of information
• Will start to be able to detect clinical signs to judge the relative importance of a particular clinical finding to the patient condition
• Are all aspects of a patient condition regarded as equally important?
• Areas of opportunity: time management, priority setting, planning, and organization in the delivery of care
13
Competent Nurse
• During the first year of practice our goal is to become competent!!!
• To master necessary skills and have the ability to efficiently cope with the many constituents of care delivery
• Differentiate between what is most important and what can be delayed
• Process of moving through stages to competent can depend on:• Background and experience of the resident
• Type of institution
• Degree of complexity of the patient population in the work environment
• Focus of the NRP (one year): guiding/supporting development of skills, aspect recognition, and coping mechanisms
14
Proficient Nurse Expert Nurse• 3-5 years• Some may never reach this level• Perceives the situation as a whole• Their perspective is not thought out,
but “presents” itself based upon experience and situations
• Learns from experience• Guided by subtle nuances in patient’s
status• Understands how plans need to be
modified in response to variations
• >=5 years of experience• Some may never reach this point• Capturing the description of expert
performance is difficult • Work from a deep instinctive, intuitive
level of understanding• Expert does things because it “feels
right” • Due to experience, expert has an
intuitive grasp of the situation, zeroes in on the key problem/issue without wasting time or effort on irrelevancy
15

Quick Recap
• Where should you be in the five levels of nursing competency by the end of this yearlong program?
• What two key objectives do you have to meet to be at this level?
16

Credibility – What is it?
17
• Professionals must intentionally establish and maintain • You do not automatically gain credibility and respect
Establishing Credibility
• Being knowledgeable and committed to life-long learning
• Professionalism – personal appearance and conduct
• Open to new ideas, feedback, and approaches
• Accept responsibility and accountability for actions
• Admitting personal mistakes and knowledge gaps
• Builds an atmosphere of trust and respect
• Clear communication - show interest, be present, ask questions
• Round with team and interdisciplinary collaboration
• Networking with others
18
Communication
• Nurses are responsible for communicating with other members of the healthcare team to safely and effectively manage patient care
• NRP will assist nurse residents to develop effective communication strategies, including:
• Transmission of patient’s plan of care and changes in condition• Approaching physicians and other health care providers and actively listening to the information communicated
• Communication within the established chain of command• Establishment of credibility within your unit/department
• Let’s start with a few examples:
19

Assertive Communication• There are six main characteristics of assertive communication:
• Eye contact: demonstrates interest, shows sincerity
• Body posture: congruent body language will improve the significance of the message
• Gestures: appropriate gestures help to add emphasis
• Voice: a level, well-modulated tone convincing and acceptable, not intimidating
• Timing: use your judgment to maximize receptivity and impact
• Content: how, where, and when you choose to comment more is important than WHAT
• The importance of "I" statements• Part of being assertive involves the ability to express your needs and feelings• Indicates ownership, does not attribute blame, focuses on behavior and its effect, is direct and
honest, and contributes to the growth of your relationship with each other• CUS – I am concerned, uncomfortable, and don’t feel it is safe…• "I feel frustrated when you are late for meetings. I don't like having to repeat information
20

Communication Barriers
• Lack of structure and standardization for communication• Differences in authority, culture, gender, and race• Healthcare team members may have different
communication styles• Many physicians seem to favor “bulleted” summaries or “headlines”
• Non-physician team members often use detailed, descriptive narratives – for example nurse to nurse handoff report
• Do we have a common language - effective/efficient, standardized, mirrors nursing/scientific process in healthcare?
21
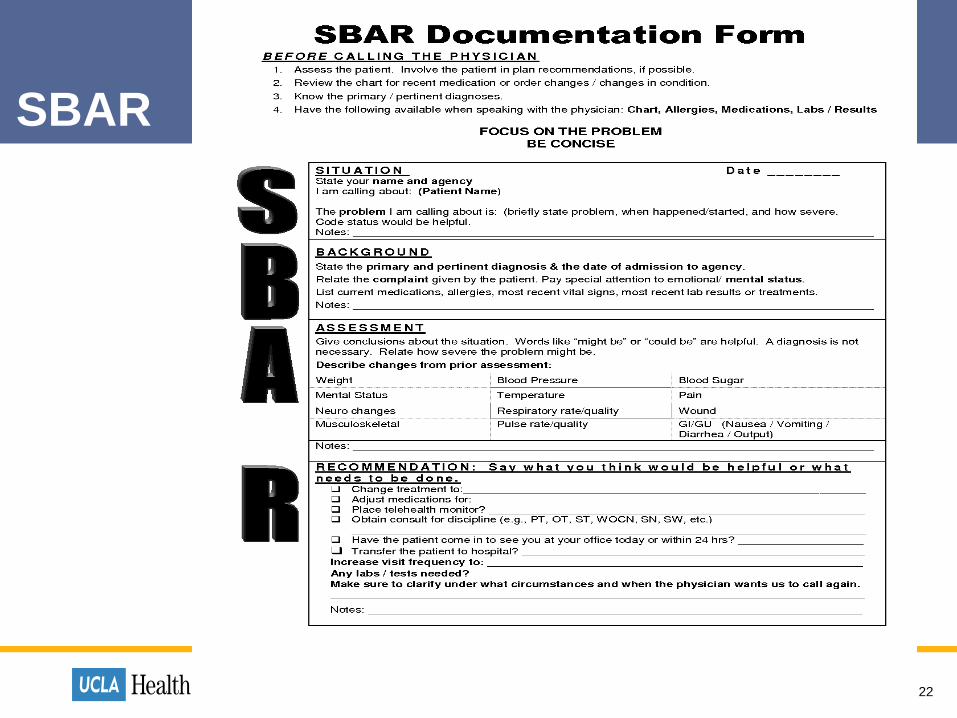
SBAR
22

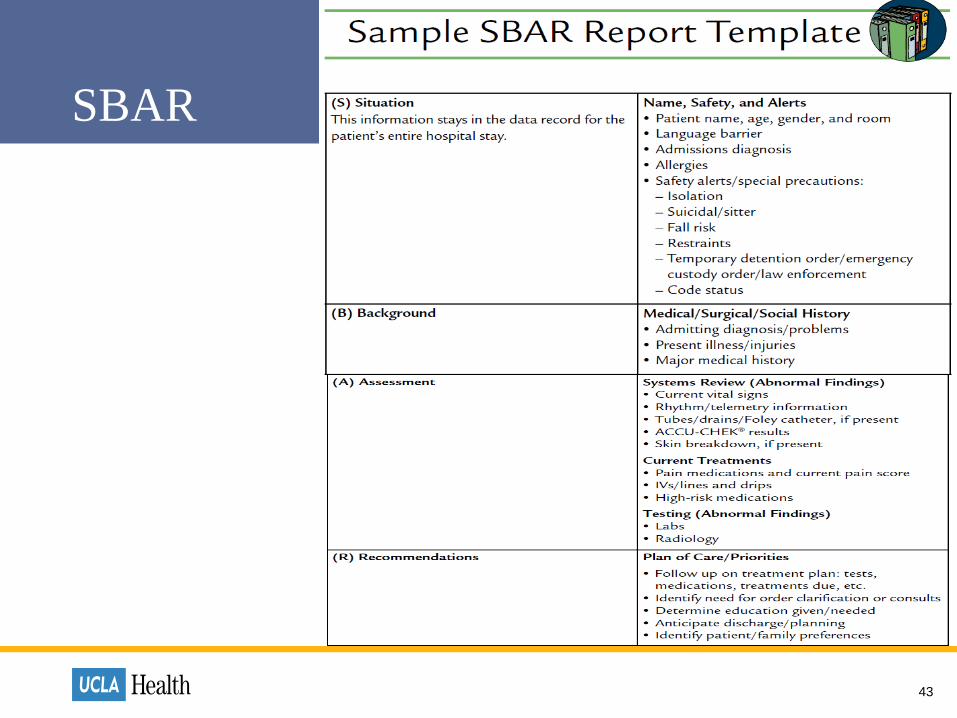
SBAR• S – Situation - What is the immediate problem/situation?
• Example: Hello Dr. Smith. I am Nurse Happy from the Z unit. I’m calling about Mr. Jones who is experiencing a severe deterioration in his respiratory status.
• B – Background - What is the relevant background to the issue/problem?
• Example: He’s a 75 y.o. admitted with SOB due to severe COPD. He had a needle biopsy this afternoon. He has become increasingly SOB over the last 10 minutes.
• A – Assessment - What are your conclusions about the present situation?
• Example: His breath sounds are diminished on the R side, compared to earlier. V/S are…..with an increased RR from 22 to 34, Saturation is…I think he may have a pneumothorax…
• R – Recommendation - What can be done to correct the problem?
• Example: I recommend initial imaging and increased oxygenation…
23

Handoff Tips• Handoffs occur whenever there is a transfer of care from
one healthcare provider to another, all handoffs are opportunities for patient harm, handoffs most risky include:
• Patient discharge home/nursing home• Patient transfer between units• Nursing shift change• Physician transfer of care
• Effective handoffs:• Allow participants the opportunity to ask questions• Incorporate read/repeat back as needed to confirm or clarify• Have minimal interruptions to limit distractions and errors• Should be accurate and up-to-date with supporting historical information
24

Communication Tips: Medical Provider• Check with Preceptor/Charge Nurse/Lead Nurse first
• Know what the patient needs and what you want from physician
• Actively contribute to patient’s plan of care
• Take a deep breath, be comfortable approaching/calling physician• Identify self, unit, patient and diagnosis
• Have all the necessary data available in easily accessible format when you call – part of this data would be your assessment
• Review current orders, progress notes, nursing notes, PMH, medications
• Summarize patient problems/assessment cues (use SBAR)
• Know existing protocols used by hospital/service/physician
25

Unit Director and CNSGetting Help and Getting Ahead
• Ask for help • Meet on a regular basis
• Find out what they expect from you• Ask for feedback and guidance
• Use the Chain of Command• Use your resources appropriately
• Show good work ethic • Be on time, show up when scheduled, be a team player• Do your job, positive attitude, be accountable, be honest
• Develop and maintain mature and professional relationships• “Nothing about without”
26
PreceptorsGetting Help and Getting Ahead
• Make a connection Get to know your Preceptor
• Discuss/review the orientation goals for the day
• Ask for help, guidance, show interest, take initiative, be an active learning, ask questions, listen to learn, observe
• Be professional and courteous, show appreciation
• Set up regular meetings to discuss progress, time management
• Ask about a resource person if preceptor is not available
• Do your homework Read up on things before and after…
• Maintain outstanding work habits, be a role model
• Be visible and participate in huddles, meetings, committees
• Self-reflect and self-care will be key
27
• Introduce yourself to others and make a connection
• Ask questions, offer help, be present, thank others who help you
• Treat everyone in a professional and respectful manner
• Remember there is a “big picture” on your unit, not just your patients
• Praise and acknowledge other people when opportunity arises
• Socialize and build camaraderie with your team members
• Try and figure out who are the informal leaders and make a connection with them, take initiative to learn/observe/take part
• Try to avoid/not participate in negativity, gossip, and distractions
28
Being a Team PlayerGetting Help and Getting Ahead

Patients, Families & NeighborsGetting Help and Getting Ahead
• Business of “Human Caring,” healing humankind one patient at a time
29
Developing YOUR CareerGetting Help and Getting Ahead
• What’s in your job description and performance evaluation?
• Do you know the hospital policies/procedures?
• Do you know the practice guidelines for the area?
• Are you familiar with the Nurse Practice Act?
• Do you know your unit and nursing chain of command?
• Do you know the Joint Commission and Department of Public Health regulations?
• What about the magnet model components?
• Are you affiliated with any professional organizations?
• Do you have an updated resume or curriculum vitae?
• What are YOUR short term and long term plans/goals?
30

Evidence Based Practice Culture
31

Evidence Based Practice Culture
32

Evidence Based Practice Project • Goals : Explore a topic using Evidence-Based Practice methods and to describe how that evidence can
be used to advance nursing practice. You will You have 12 months to complete your project.
• General Instructions: Each Nurse Resident will ideally participate on a team. Teams are comprised of
members of your cohort. We recommend teams of 3 nurse residents. You may work alone if necessary.
• Topics will need approval from your unit director/supervisor/CNS. Topics should be related to quality
improvement/performance, patient safety, HCAHPS composite scores, nursing sensitive indicators (i.e.,
falls, HAPU, medication errors, CLABSI, CAUTI, specimen mislabeling) and should be clinically relevant in
your area. Lastly, choose something the group is interested in. PATIENT OUTCOMES
• Final projects must include a literature review of a minimum of 3 current references preferably published
within the past 5 years.
• Poster presentation sessions will be part of your final session – Graduation Day. All members of
the team must present. Teams will defend their project for guests attending the graduation.
33
• Use your resources:• Staff and faculty counseling, Circle of Caring, Ethics of Caring, UD/CNS/Preceptor
34
Preventing BurnoutGetting Help and Getting Ahead
Concepts of Diversity – the Kaleidoscope
• Diversity encompasses several dimensions that are characterized by physical differences, personal preferences, or life experiences of an individual. It includes acknowledging, understanding, accepting, valuing, and celebrating differences among people
• Meeting the challenge - rapidly changing and increasingly diverse patient population is more important than ever
• Exploring diversity within the health care team and within the context of the nurse-patient relationship will be key
35

Types of Diversity 1. Ethnicity2. Culture (patterns of behavior that include language, thoughts,
communications, actions, customs, beliefs, values, beliefs regarding health practices, decision making)
3. Gender4. Lifestyle5. Religion6. Socioeconomic status7. Age/generation8. Sexual orientation9. Physical appearance10. Physical and/or mental capabilities11. Health literacy
36

Dimensions of Diversity
• Patient/family/community preferences, values• Coordination and integration of care• Information, communication, and education• Physical comfort and emotional support• Involvement of family and friends• Transition and continuity
37
Similarities and DifferencesSelf, Patients/Families, and Staff• Understanding that diverse cultural, ethnic, and social backgrounds function as sources of patient, family,
and community values
• Seeing health care situations “through patients’ eyes”
• Respecting and encouraging individual expression of values, preferences, and expressed needs
• Valuing the patient’s expertise with own health and symptoms
• Seeking learning opportunities with patients who represent aspects of human diversity
• Recognizing personally held attitudes about working with patients from different ethnic, cultural, and
social backgrounds
• Willingly supporting patient-centered care for individuals and groups whose values differ from own
• Seeking to understand one’s personally held values and beliefs about the management of pain or
suffering
38
Evidence Based Strategies - Diversity
• Eliciting patient values, preferences, and expressed needs as part of clinical interview, implementation of care plan, and evaluation of care
• Communicating patient values, preferences, and expressed needs to other members of health care team
• Verbalizing importance of delivering patient-centered care with sensitivity and respect for the diversity of human experience
• Using knowledge of psychological, spiritual, social, developmental, and physiological models of pain and suffering
39
Nursing Workforce Diversity
• According to a 2013 survey conducted by the National Council of State Boards, the RN
population is comprised of: White/Caucasian 83%, African American 6%, Asian 6%, Latino
3%, American Indian/Alaskan Native & Hawaiian/Pacific Islander 1%
• Of practicing registered nurses, 90% are female and 10% are male
• Marital status - 74% are married
• According to a 2013 survey conducted by the National Council of State Boards of Nursing
and The Forum of State Nursing Workforce Centers, 55% of the RN workforce is age 50/>,
avg. age of the RN population is 47.0, up slightly from 46.8 in 2004
• US population 65> - 13.3%
• Disabilities – some level 56.7 million (18.7%), 65> yrs. 49.8%
• Language – 20% of US population uses a language other than English
40

Calling All Generations
• A nurse manager, desperate for more staff, telephones 4 of her nurses to ask whether they will pull an extra shift.
• The first nurse says, "What time do you need me?”• The second nurse says, "Call me back if you can't find anyone else.”• The third nurse says, "How much will you pay me?”• The fourth nurse says, "Sorry, I have plans. Maybe next time.”
• The "traditionalists" (also called the "veterans") – before 1945• The "baby boomers" ("boomers") – 1946 - 1964• The "X generation" ("Xers") – 1965 - 1980• The "Millennials" (also known as the "Y-generation/nexters") – 1980 – 2006
41

Priority Setting
42
SBAR
43
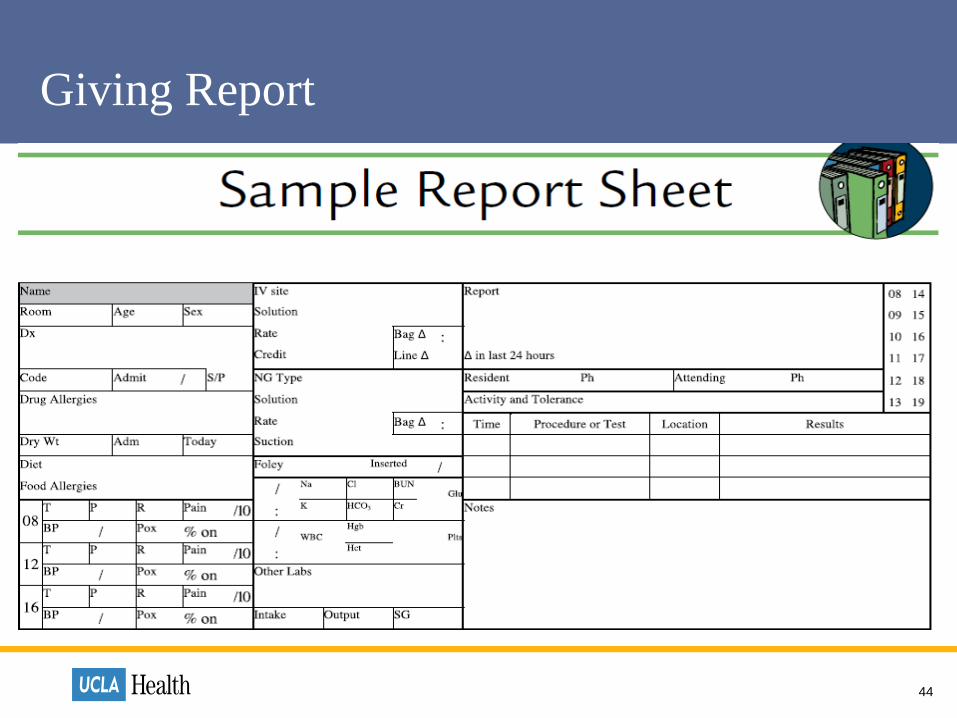
Giving Report
44

Professional Nursing Portfolio
45
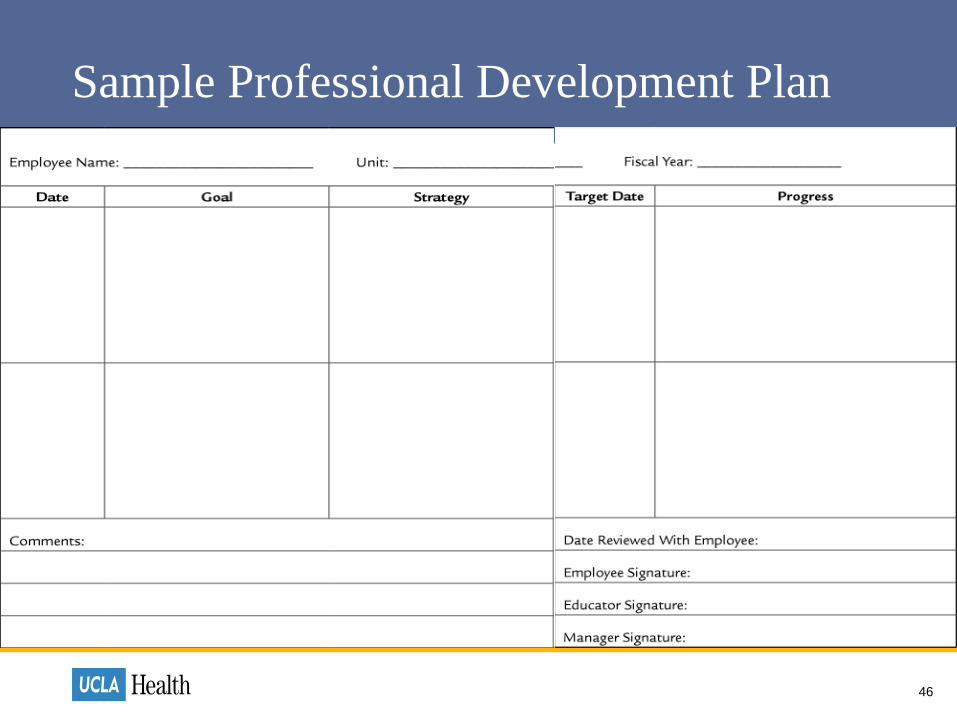
Sample Professional Development Plan
46
Closing Comment
47
Map it Out…What does it mean to be a ?
48
UCLA Nurse
Getting Help and Getting Ahead

References
• Benner, P. et al (1996). Expertise in nursing practice: Caring, clinical judgment, and ethics. New York, NY: Springer Publishing.
• Benner, P. (1984). From novice to expert: Excellence and power in clinical nursing practice. Menlo Park, CA: Addition-Wesley Publishing Company.
• Daley, B. (1999). Novice to expert: An exploration of how professionals learn. Adult Education Quarterly, 49, 133-148.
49