the vascular exam jason davis, md. before the exam… obtain history acute vs. chronic symptoms...
TRANSCRIPT
The Vascular Exam
Jason Davis, MDJason Davis, MD

Before the Exam…Obtain historyAcute vs. Chronic symptomsDistribution of symptoms
Level(s) of extremity pain, etc.Aggravating, Relieving factors
Activity/rest, elevation/dependenceCo-morbid conditions, vitals
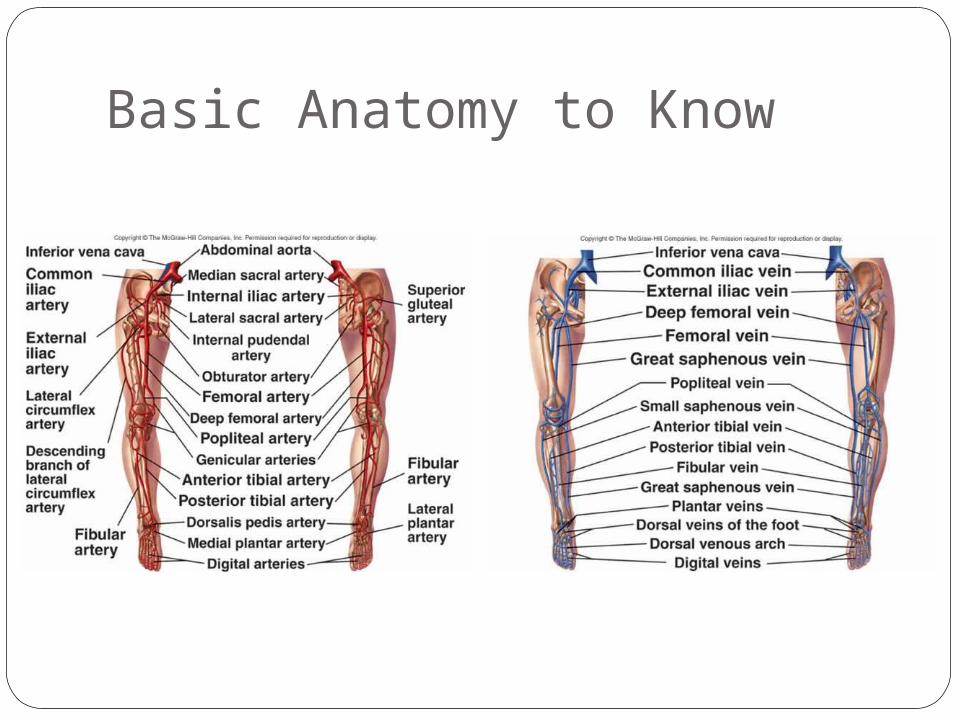
Basic Anatomy to Know

Basic Anatomy to Know

Basic Anatomy to Know
Elements of Vascular Exam
Inspect, Palpate, AuscultateSkin pallor/rubor, mottling/ cyanosis,
temperature, atrophy, hair distributionMotor function and sensory examTissue loss, ulcerationsPulse +/- doppler exam
Always compare each w/ contralateral
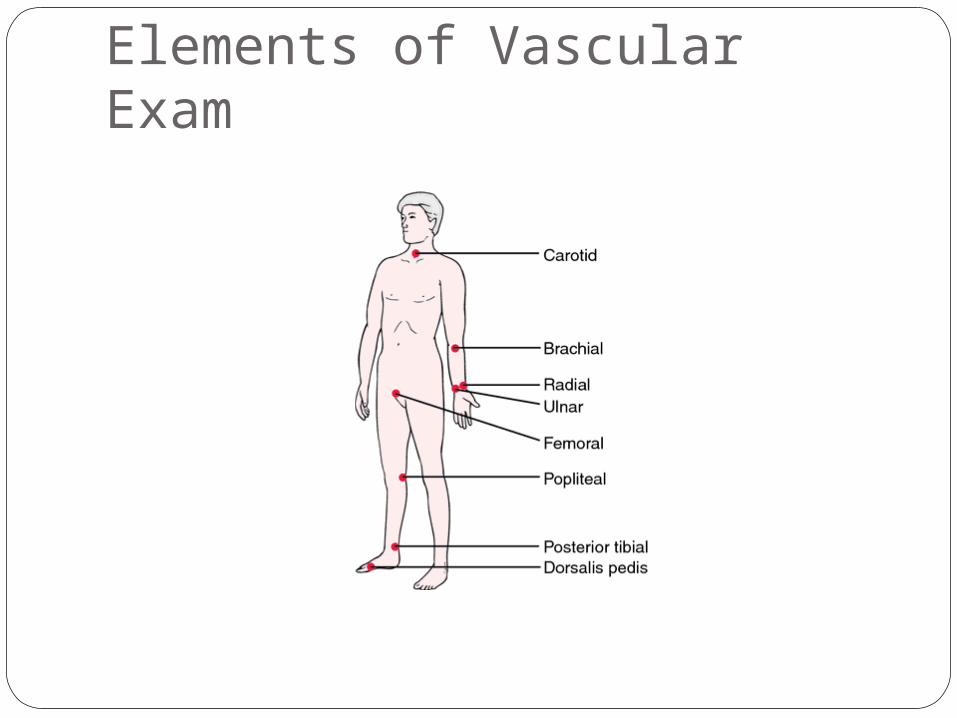
Elements of Vascular Exam
Vascular Exam tips
■ Doppler signals are NOT Pulses– Palpable pulses include carotid, brachial, radial,
ulnar, femoral, popliteal, dorsalis pedis, posterior tib
■ Bruits vs. Thrills: Audible vs. Palpable■ Characterization of Pulses
– Character (bounding, thready), Rate, Rhythm■ Characterization of Doppler Signals
– Triphasic, Biphasic, Monophasic
Trauma / Hypovolemia■ If you can palpate:
– Radial pulse, then SBP is >70 - 80– Femoral + Carotid, then SBP >50 - 70– Carotid only, then SBP >40 - 60
■ NEVER rely on pulses alone for hypovolemia assessment
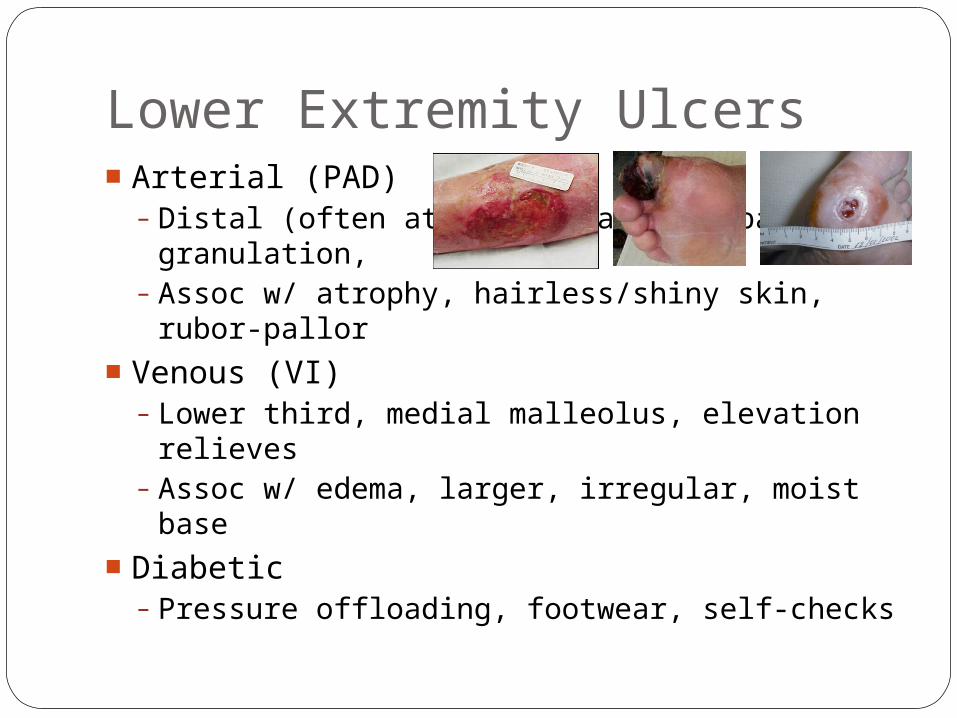
Lower Extremity Ulcers■ Arterial (PAD)
– Distal (often at toes), painful, pale granulation,
– Assoc w/ atrophy, hairless/shiny skin, rubor-pallor
■ Venous (VI)– Lower third, medial malleolus, elevation
relieves– Assoc w/ edema, larger, irregular, moist base
■ Diabetic– Pressure offloading, footwear, self-checks
Common Vascular Problems■ Peripheral arterial disease
– Thrombotic (DM, atherosclerosis)– Embolic (atrial fibrillation, Aneurysms)
■ Venous insufficiency■ DVT, thrombophlebitis■ Carotid artery stenosis■ Compartment Syndrome■ Trauma
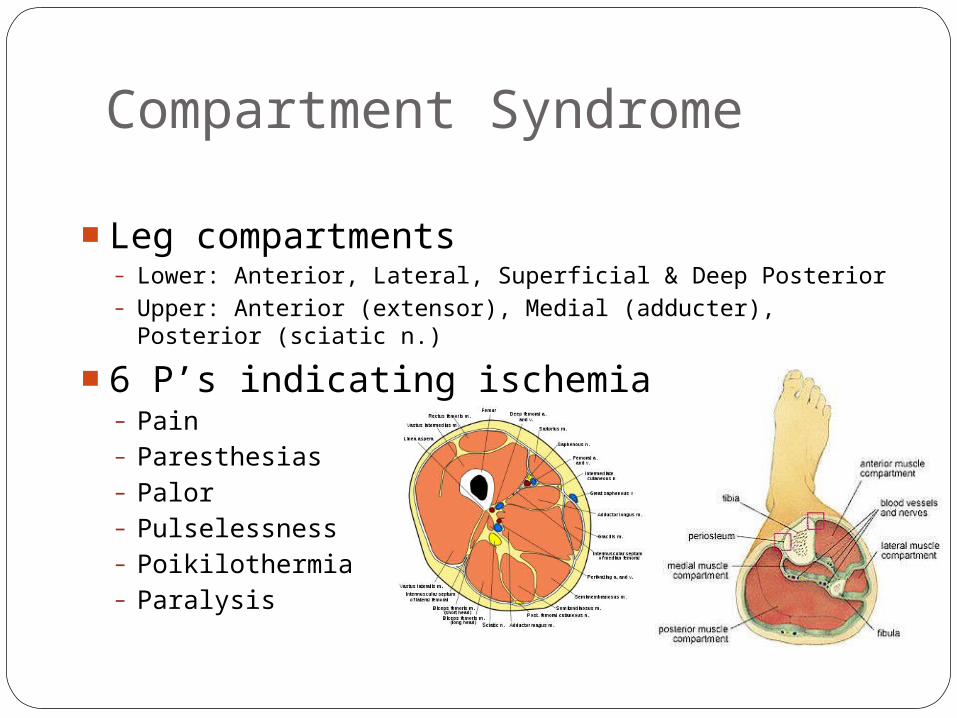
Compartment Syndrome
■ Leg compartments– Lower: Anterior, Lateral, Superficial & Deep Posterior– Upper: Anterior (extensor), Medial (adducter), Posterior
(sciatic n.)
■ 6 P’s indicating ischemia– Pain– Paresthesias– Palor– Pulselessness– Poikilothermia– Paralysis

Clinical Scenario #1■ Routine 5pm ED consult for cellulitis.
Clinical Scenario #1
■ Routine 5pm ED consult for cellulitis. ■ You see before leaving within your hrs■ On arrival, 78yo male w/ DM, CAD, +tobacco■ Also, hx of “irregular HR” with INR of 1.1■ Rt foot cooler than Lt, no palp Rt DP or PT■ Acute onset severe pain started 3hrs ago■ Embolectomy and anticoagulation
■ Don’t forget fasciotomy

Clinical Scenario #2■ New consult for non-healing ulcer, evaluate
for peripheral arterial bypass.

Clinical Scenario #2■ New consult for non-healing ulcer, evaluate
for peripheral arterial bypass.■ Obese 63yo M dialysis w/ DM, HTN■ Legs down in chair, severely edematous■ Advised to elevate and compression
garments, but does not b/c uncomfortable■ Non-tender medial malleolar ulcer x3 wk■ B/L DP and PT are palpable

Clinical Scenario #3
■ Stat consult to 3A for r/o compartment sx.■ 39yo F s/p cardiac cath via L radial artery■ Cath performed for cough, was normal■ After sheath removed, arm doubled in size■ Nurses want to know when pt going to OR
Clinical Scenario #3
■ Stat consult to 3A for r/o compartment sx.■ 39yo F s/p cardiac cath via L radial artery■ Cath performed for sneezing, found normal■ After sheath removed, arm doubled in size
■ Direct pressure applied, bleeding ceased■ Palpable distal pulses were appreciated■ Neurovascular exam intact w/ serial
exams■ Arm elevated to facilitate venous return

Berger’s Pet Peaves■ No overnight pre-op IVF unless dehydration
established or elderly pt AND afternoon case■ Reglan for N/V unless obstruction, espec DM
■ Zofran ONLY if nausea refractory to Reglan■ Only attg name on consents except as witness
■ Residents can, however, sign blood consents■ SCD’s for AAA’s only (NOT CEA’s, bypasses, etc)■ Vaseline gauze, NEVER iodoform gauze■ Do NOT elevate extremities after access cases
■ Increases steal symptoms and neuropathy■ Peri-op edema will resolve, heart level adequate
■ Dextran x24hrs for all CEA’s EXCEPT Berger’s
Vascular Studies■ Duplex
■ Doppler
■ B-mode doppler
■ ABI/PVR (LEADs)