the use of exparel in abdominal-wall field blocks … · low-dose infusion with surgical transverse...
TRANSCRIPT

EXPAREL is indicated for single-dose infiltration in adults to produce postsurgical local analgesia and as an interscalene brachial plexus nerve block to produce postsurgical regional analgesia. Safety and efficacy have not been established in other nerve blocks.
Please see Important Safety Information throughout and refer to accompanying full Prescribing Information.
THE USE OF EXPAREL IN ABDOMINAL-WALL FIELD BLOCKS
IndicationEXPAREL is indicated for single-dose infiltration in adults to produce postsurgical local analgesia and as an interscalene brachial plexus nerve block to produce postsurgical regional analgesia. Safety and efficacy have not been established in other nerve blocks.
Important Safety Information EXPAREL is contraindicated in obstetrical paracervical block anesthesia.
Adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via infiltration were nausea, constipation, and vomiting; adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via interscalene brachial plexus nerve block were nausea, pyrexia, and constipation.
If EXPAREL and other non-bupivacaine local anesthetics, including lidocaine, are administered at the same site, there may be an immediate release of bupivacaine from EXPAREL. Therefore, EXPAREL may be administered to the same site 20 minutes after injecting lidocaine.
EXPAREL is not recommended to be used in the following patient population: patients <18 years old and/or pregnant patients.
Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease.
Warnings and Precautions Specific to EXPARELAvoid additional use of local anesthetics within 96 hours following administration of EXPAREL.
EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks other than interscalene brachial plexus nerve block, or intravascular or intra-articular use.
The potential sensory and/or motor loss with EXPAREL is temporary and varies in degree and duration depending on the site of injection and dosage administered and may last for up to 5 days, as seen in clinical trials.
Warnings and Precautions for Bupivacaine-Containing ProductsCentral Nervous System (CNS) Reactions: There have been reports of adverse neurologic reactions with the use of local anesthetics. These include persistent anesthesia and paresthesia. CNS reactions are characterized by excitation and/or depression.
Cardiovascular System Reactions: Toxic blood concentrations depress cardiac conductivity and excitability which may lead to dysrhythmias, sometimes leading to death.
Allergic Reactions: Allergic-type reactions (eg, anaphylaxis and angioedema) are rare and may occur as a result of hypersensitivity to the local anesthetic or to other formulation ingredients.
Chondrolysis: There have been reports of chondrolysis (mostly in the shoulder joint) following intra-articular infusion of local anesthetics, which is an unapproved use.
Methemoglobinemia: Cases of methemoglobinemia have been reported with local anesthetic use.
6 millionpatients have received non-opioid EXPAREL
since 201220
Visit www.EXPAREL.com to learn more.
Please refer to accompanying full Prescribing Information.For more information, please visit www.EXPAREL.com or call 1-855-RX-EXPAREL (793-9727).References: 1. Gadsden J, Ayad S, Gonzales JJ, Mehta J, Boublik J, Hutchins J. Evolution of transversus abdominis plane infi ltration techniques for postsurgical analgesia following abdominal surgeries. Local Reg Anesth. 2015;8:113-117. 2. Young MJ, Gorlin AW, Modest VE, Quraishi SA. Clinical implications of the transversus abdominis plane block in adults. Anesthesiol Res Pract. 2012;2012:731645. doi:10.1155/2012/731645. 3. Børglum J, Jensen K. Abdominal surgery: advances in the use of ultrasound-guided truncal blocks for perioperative pain management. In: Derbel F, ed. Abdominal Surgery. Rijeka, Croatia: InTech; 2012:69-94. 4. Niraj G, Kelkar A, Powell R. Ultrasound-guided subcostal transversus abdominis plane block. International Journal of Ultrasound and Applied Technologies in Perioperative Care. 2010;1(1):9-12. 5. Go R, Huang YY, Weyker PD, Webb CA. Truncal blocks for perioperative pain management: a review of the literature and evolving techniques. Pain Manag. 2016;6(5):455-468. 6. Ultrasound-guided transversus abdominis plane and quadratus lumborum blocks. New York School of Regional Anesthesia website. https://www.nysora.com/regional-anesthesia-for-specifi c-surgical-procedures/abdomen/ultrasound-guided-transversus-abdominis-plane-quadratus-lumborum-blocks. Accessed April 23, 2019. 7. Detton AJ. Grant’s Dissector. 16th ed. Philadelphia, PA: Wolters Kluwer; 2017:109. 8. Rafi AN. Abdominal fi eld block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024-1026. 9. McDonnell JG, O’Donnell BD, Farell T, et al. Transversus abdominis plane block: a cadaveric and radiological evaluation. Reg Anesth Pain Med. 2007;32(5):399-404. 10. Webster K. Ultrasound guided rectus sheath block-analgesia for abdominal surgery. Update Anaesth. 2010;26:12-17. 11. Favuzza J, Brady K, Delaney CP. Transversus abdominis plane blocks and enhanced recovery pathways: making the 23-h hospital stay a realistic goal after laparoscopic colorectal surgery. Surg Endosc. 2013;27(7):2481-2486. 12. Chen CK, Tan PC, Phui VE, Teo SC. A comparison of analgesic e� cacy between oblique subcostal transversus abdominis plane block and intravenous morphine for laparoscopic cholecystectomy. A prospective randomized controlled trial. Korean J Anesthesiol. 2013;64(6):511-516. 13. Harish R. Low-dose infusion with “surgical transverse abdominis plane (TAP) block” in open nephrectomy. Br J Anaesth. 2009;102(6):889-890. 14. Hutchins J, Delaney D, Vogel RI, et al. Ultrasound guided subcostal transversus abdominis plane (TAP) infi ltration with liposomal bupivacaine for patients undergoing robotic assisted hysterectomy: a prospective randomized controlled study. Gynecol Oncol. 2015;138(3):609-613. 15. Børglum J, Maschmann C, Belhage B, Jensen K. Ultrasound-guided bilateral dual transversus abdominis plane block: a new four-point approach. Acta Anaesthesiol Scand. 2011;55(6):658-663. 16. Bhakta A, Glotzer O, Ata A, Tafen M, Stain S, Singh P. Analgesic e� cacy of laparoscopic guided transverse abdominis plane block using liposomal bupivacaine in bariatric surgery. Am J Surg. 2018;215(4):643-646. 17. Yarwood J, Berrill A. Nerve blocks of the anterior abdominal wall. Cont Educ Anaesth Crit Care Pain. 2010;10(6):182-186. 18. Elsharkawy H. Ultrasound-guided quadratus lumborum block: how do I do it? American Society of Regional Anesthesia and Pain Medicine website. https://www.asra.com/pain-resource/article/48/ultrasound-guided-quadratus-lumborum-blo. Accessed April 1, 2019. 19. Chetwood A, Agrawal S, Hrouda D, Doyle P. Laparoscopic assisted transversus abdominis plane block: a novel insertion technique during laparoscopic nephrectomy. Anaesthesia. 2011;66(4):317-318. 20. Data on fi le. 5903. Parsippany, NJ: Pacira BioSciences, Inc.; October 2019.

2
Abdominal-wall field blocks are part of a multimodal strategy for postsurgical pain management1
• Abdominal-wall field blocks use a local anesthetic to provide effective regional analgesia for a range of procedures2
• Transversus abdominis plane (TAP) field blocks provide analgesia to the anterior abdominal wall and involve administration of a local anesthetic into the fascial plane between the transversus abdominis and internal oblique muscles1
• Approaches to abdominal-wall field blocks have been evolving — The TAP block was originally described as a landmark-guided field block based on the lumbar triangle1
— Ultrasound-guided TAP blocks allow visualization of the needle and local anesthetic in the plane1
— Additional approaches have been and continue to be developed, including subcostal TAP, 4-point TAP, rectus sheath blocks, and quadratus lumborum (QL) blocks1,3
• TAP blocks can be administered by the anesthesiologist or the surgeon2
Important Safety InformationEXPAREL is contraindicated in obstetrical paracervical block anesthesia.
Adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via infiltration were nausea, constipation, and vomiting; adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via interscalene brachial plexus nerve block were nausea, pyrexia, and constipation.
Abdominal-wall field blocks can achieve sensory block in one of several areas
QL block
Rectus sheath block
Bilateral 4-point TAP block
Subcostal TAP block
Classic TAPblock
Comparison of sensory blocks achieved
Classic TAP block4
Yellow semicircle over the lower abdomen (dermatomes T10 to L1)
Subcostal TAP block4
Can vary, but approximately the shaded gray in the upper abdominal quadrant (dermatomes T6 to T10-T12)
Bilateral 4-point TAP block5
Green shape overlapping the areas of coverage of classic and subcostal TAPs (dermatomes T6 to T12)
Rectus sheath block5
Narrow black oval over abdominal midline (dermatomes T6 to T12)
QL block6
Large purple circle over abdominal midline (dermatomes T4 to L1)
[1/Gadsden 2015/p113/par1/ln8-12]
[2/Young 2012/p1/col1/par1/ln1-7]
[1/Gadsden 2015/p113/par1/ln10-12,p114/col2/par1/ln1-5]
[1/Gadsden 2015/p114/col1/par2/ln1,2][1/Gadsden 2015/p114/col2/par2/ln1-8]
[1/Gadsden 2015/p115/col1/par1/ln3-15][3/Borglum 2012/p72/Fig2/rows3,6]
[2/Young 2012/p3/col2/par2/ln1-5]
[4/Niraj 2010/p9/col2/par2/ln1-6]
[4/Niraj 2010/p11/col1/par5/ln2-5, 9-11]
[5/Go 2016/p2/col1/par2/ln23-29]
[5/Go 2016/p11/Table1/row6]
[6/NYSORA/p1/para1/ln11-13]

Please refer to accompanying full Prescribing Information.
3
Thoracoabdominal nerves
T7
T8
T9
T10
T11
Subcostal nerve (T12)
Iliohypogastric nerve (L1)
Ilioinguinal nerve (L2)
Superior epigastric artery
Inferior epigastric artery
Transversusabdominismuscle
Image used with permission from Abdominal Best Infi ltration Practices and International Guidelines Central. Artwork created by Kellie M. Holoski, 2016.
Ultrasound-guided infiltration of the appropriate nerves can achieve a range of sensory blocks7
Target the appropriate nerves to achieve the desired abdominal-wall field block
Important Safety Information (continued)If EXPAREL and other non-bupivacaine local anesthetics, including lidocaine, are administered at the same site, there may be an immediate release of bupivacaine from EXPAREL. Therefore, EXPAREL may be administered to the same site 20 minutes after injecting lidocaine.
EXPAREL is not recommended to be used in the following patient population: patients <18 years old and/or pregnant patients.
Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease.
[7/Detton/p109/Fig4.15]
Please refer to accompanying full Prescribing Information.
4
Performing a classic TAP block in abdominal surgeries
Performing a bilateral subcostal TAP block in abdominal surgeries
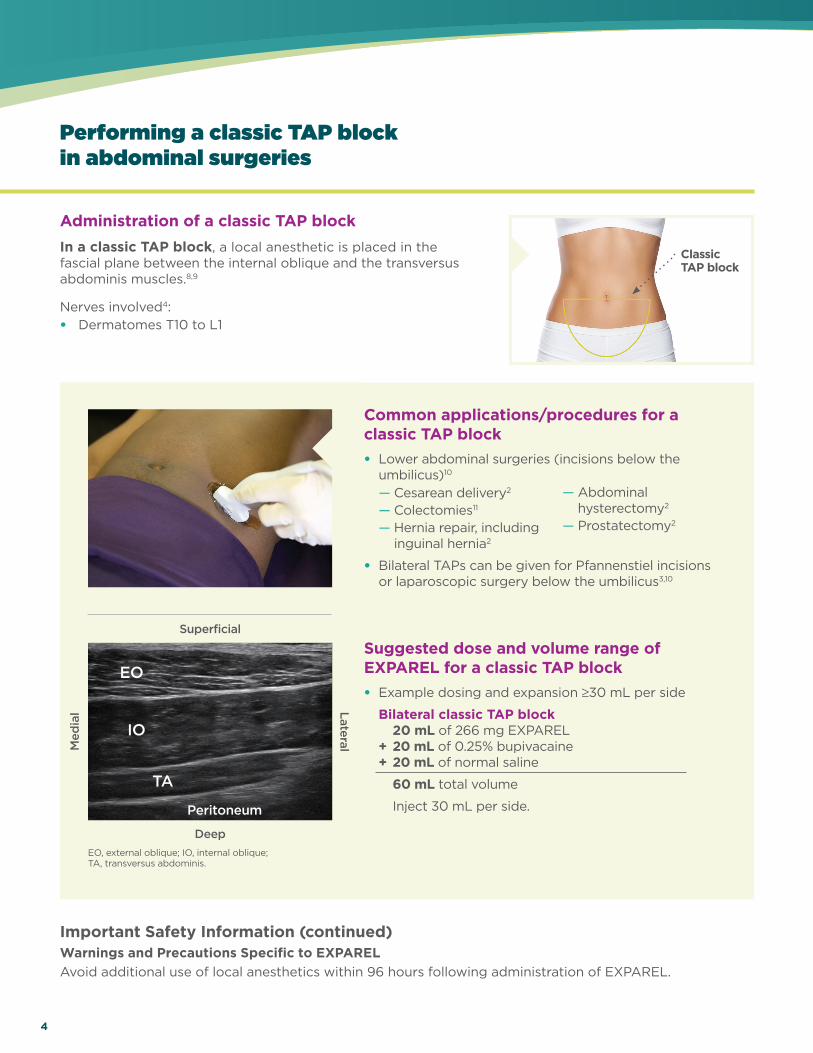
Common applications/procedures for a classic TAP block• Lower abdominal surgeries (incisions below the
umbilicus)10
— Cesarean delivery2
— Colectomies11
— Hernia repair, includinginguinal hernia2
• Bilateral TAPs can be given for Pfannenstiel incisions or laparoscopic surgery below the umbilicus3,10
Administration of a bilateral subcostal TAP block In a subcostal oblique TAP block, a local anesthetic is placed between the rectus abdominis and the posterior rectus sheath or between the rectus abdominis and the transversus abdominis.5
Nerves involved4:• Dermatomes T6 to T10-T12
Med
ial
Superficial
EO, external oblique; IO, internal oblique; TA, transversus abdominis.
Deep
Administration of a classic TAP block In a classic TAP block, a local anesthetic is placed in the fascial plane between the internal oblique and the transversus abdominis muscles.8,9
Nerves involved4:• Dermatomes T10 to L1
Classic TAP block
Important Safety Information (continued)Warnings and Precautions Specific to EXPAREL (continued)EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks other than interscalene brachial plexus nerve block, or intravascular or intra-articular use.
The potential sensory and/or motor loss with EXPAREL is temporary and varies in degree and duration depending on the site of injection and dosage administered and may last for up to 5 days, as seen in clinical trials.
Important Safety Information (continued)Warnings and Precautions Specific to EXPARELAvoid additional use of local anesthetics within 96 hours following administration of EXPAREL.
Suggested dose and volume range of EXPAREL for a classic TAP block• Example dosing and expansion ≥30 mL per side
Bilateral classic TAP block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 20 mL of normal saline
60 mL total volume
Inject 30 mL per side.
— Abdominalhysterectomy2
— Prostatectomy2
Med
ial
RA, rectus abdominis.
Lateral
Superficial
Deep
EO
IO
TA
Peritoneum
RA
TA
Peritoneum
[8/Ra� 2001/p1025/col3/par1/ln1-4][9/McDonnell 2007/p399/col2/par2/ln1,2, p400/col1/par1/all, p401/col1/par1/ln1-8]
[11/Favuzza 2013/p2483/col1/par2/ln1-6]
[10/Webster 2010/p14/col1/par2/ ln5-6]
[3/Borglum 2012/p72/Table2/col1/row1; col2/Fig2][10/Webster 2010/p14/col1/par2/ln5-6]
4/Niraj 2010/p9/col2/par2/ln1-6
[2/Young 2012/p5/Table1/rows9,14]
[2/Young 2012/p5/Table 1/rows5,10,13; p6/Table1 cont/row12; p7/Table1 cont/row2]
[2/Young 2012/p7/Table1/row1]
[2/Young 2012/p7/Table 1/row4]

5
Please refer to accompanying full Prescribing Information.
Performing a classic TAP block in abdominal surgeries
Performing a bilateral subcostal TAP block in abdominal surgeries
Lateral
Common applications/procedures for a classic TAP block• Lower abdominal surgeries (incisions below the
umbilicus)10
— Cesarean delivery2
— Colectomies11
— Hernia repair, includinginguinal hernia2
• Bilateral TAPs can be given for Pfannenstiel incisions or laparoscopic surgery below the umbilicus3,10
Administration of a bilateral subcostal TAP block In a subcostal oblique TAP block, a local anesthetic is placed between the rectus abdominis and the posterior rectus sheath or between the rectus abdominis and the transversus abdominis.5
Nerves involved4:• Dermatomes T6 to T10-T12
Subcostal TAP block
Classic TAP block
Important Safety Information (continued)Warnings and Precautions Specific to EXPAREL (continued)EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks other than interscalene brachial plexus nerve block, or intravascular or intra-articular use.
The potential sensory and/or motor loss with EXPAREL is temporary and varies in degree and duration depending on the site of injection and dosage administered and may last for up to 5 days, as seen in clinical trials.
Important Safety Information (continued)Warnings and Precautions Specific to EXPARELAvoid additional use of local anesthetics within 96 hours following administration of EXPAREL.
Suggested dose and volume range of EXPAREL for a classic TAP block• Example dosing and expansion ≥30 mL per side
Bilateral classic TAP block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 20 mL of normal saline
60 mL total volume
Inject 30 mL per side.
Common applications/procedures for a subcostal TAP block• Upper abdominal surgeries (incisions above the
umbilicus)10
• Can be added to a classic TAP block for coverage above and below the umbilicus3
Suggested dose and volume range of EXPAREL for a subcostal TAP block• Example dosing and expansion ≥30 mL per side
Bilateral subcostal TAP block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 20 mL of normal saline
60 mL total volume
Inject 30 mL per side.
— Laparoscopic cholecystectomy12
— Nephrectomy13
— Colorectal3
— Upper midline laparotomy4
— Laparoscopic/robotic surgery14
— Hysterectomy14
— Abdominalhysterectomy2
— Prostatectomy2
Med
ial
RA, rectus abdominis.
Superficial
Deep
RA
TA
Peritoneum
[5/Go 2016/p3/col2/par1/ln3-7]
[4/Niraj 2010/p11/col1/par5/ln2-5, 9-11]
[10/Webster 2010/p14/col1/par2/ln6-7][12/Chen 2013/p512/col1/par1/ln7-13][13/Harish 2009/p889/col2/par1/ln2-5][3/Borglum 2012/p75/par2/ln1-6][4/Niraj 2010/p10/col2/Fig2][14/Hutchins 2015/p612/col1/par3/all][14/Hutchins 2015/p612/col1/par3/all][3/Borglum 2012/p/p72/Table2/col2/row1]

Please refer to accompanying full Prescribing Information.
6
Performing a bilateral 4-point TAP block in major abdominal surgeries
Performing a rectus sheath block in midline incisions
Med
ial
Superficial
Deep
Med
ial
Superficial
Deep
Common applications/procedures for a bilateral 4-point TAP block • Major abdominal surgeries (combination block
anesthetizes entire abdominal wall) — Laparoscopy15
— Laparotomy15
— Abdominal wall repair15
— Colorectal3
— Bariatric16
Administration of a bilateral 4-point TAP blockIn a 4-point TAP block, a local anesthetic is placed at the 4 injection sites used for a bilateral classic TAP block and subcostal TAP block.1
Nerves involved5:• Dermatomes T6 to T12
Administration of a rectus sheath blockIn a rectus sheath block, a local anesthetic is placed in the posterior border of the rectus abdominis muscle and the rectus sheath.17
Nerves involved5:• Dermatomes T6 to T12
Bilateral 4-point TAP block
Bilateral 4-point TAP block
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Cardiovascular System Reactions: Toxic blood concentrations depress cardiac conductivity and excitability which may lead to dysrhythmias, sometimes leading to death.
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing ProductsCentral Nervous System (CNS) Reactions: There have been reports of adverse neurologic reactions with the use of local anesthetics. These include persistent anesthesia and paresthesia. CNS reactions are characterized by excitation and/or depression.
Suggested dose and volume range of EXPAREL for a 4-point TAP block• Example dosing and expansion ≥20 mL per side
Bilateral 4-point TAP block 20 mL of 266 mg EXPAREL + 40 mL of 0.25% bupivacaine + 20 mL of normal saline
80 mL total volume
Inject 20 mL per site.
Lateral
RARA
Peritoneum
Rectus sheath
EO
IO
TA
Peritoneum
[1/Gadsden 2015/p115/col1/par1/ln12-15]
[5/Go 2016/p11/Table1/row6]
[15/Borglum 2011/p659/col1/par2/ln9-12][15/Borglum 2011/p659/col1/par2/ln9-12][15/Borglum 2011/p659/col1/par2/ln9-12][3/Borglum 2012/p75/par2/ln1-6][16/Bhakta/p644/col2/par4/ln1-9/Table3, p645/Table4]
[15/Borglum 2011/p661/col2/par2/ln1-3]

7
Please refer to accompanying full Prescribing Information.
Performing a bilateral 4-point TAP block in major abdominal surgeries
Performing a rectus sheath block in midline incisions
Med
ial
Superficial
Deep
Common applications/procedures for a bilateral 4-point TAP block • Major abdominal surgeries (combination block
anesthetizes entire abdominal wall) — Laparoscopy15
— Laparotomy15
— Abdominal wall repair15
— Colorectal3
— Bariatric16
Common applications/procedures for a rectus sheath block• Midline incisions, including17
— Umbilical hernia repairs — Incisional hernia repairs
Administration of a rectus sheath blockIn a rectus sheath block, a local anesthetic is placed in the posterior border of the rectus abdominis muscle and the rectus sheath.17
Nerves involved5:• Dermatomes T6 to T12
Bilateral 4-point TAP block
Bilateral 4-point TAP block
Rectus sheathblock
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Cardiovascular System Reactions: Toxic blood concentrations depress cardiac conductivity and excitability which may lead to dysrhythmias, sometimes leading to death.
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing ProductsCentral Nervous System (CNS) Reactions: There have been reports of adverse neurologic reactions with the use of local anesthetics. These include persistent anesthesia and paresthesia. CNS reactions are characterized by excitation and/or depression.
Suggested dose and volume range of EXPAREL for a 4-point TAP block• Example dosing and expansion ≥20 mL per side
Bilateral 4-point TAP block 20 mL of 266 mg EXPAREL + 40 mL of 0.25% bupivacaine + 20 mL of normal saline
80 mL total volume
Inject 20 mL per site.
Suggested dose and volume range of EXPAREL for a rectus sheath block• Example dosing and expansion ≥20 mL per side
Bilateral rectus sheath block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine
40 mL total volume
Inject 20 mL per side.
Lateral
RA
Peritoneum
Rectus sheath
[17/Yarwood 2010/p183/col2/par7/ln1,2,p184/col1/par1/ln1,2]
[5/Go 2016/p2/col1/par2/ln23-29]
[17/Yarwood 2010/p183/col2/par5/ln4-5]
Please refer to accompanying full Prescribing Information.
8
Performing a QL block in more extensive abdominal surgeries
Performing TAP blocks in abdominal laparoscopic procedures
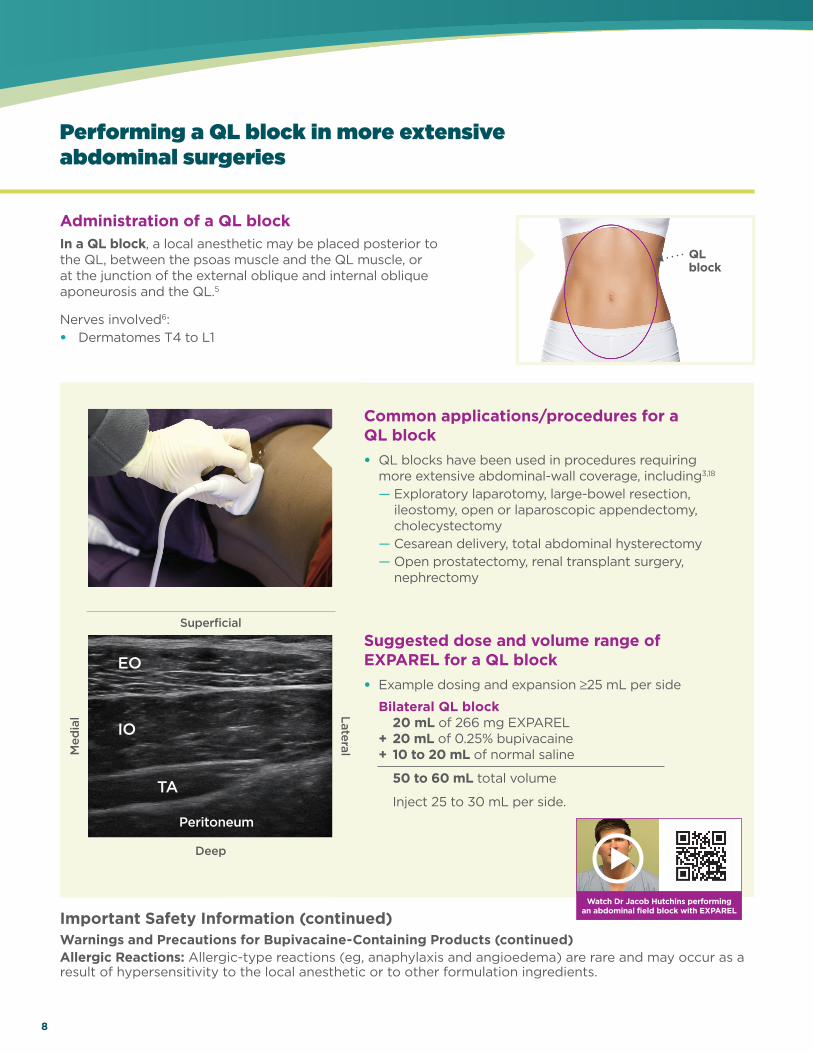
Administration of a QL block In a QL block, a local anesthetic may be placed posterior to the QL, between the psoas muscle and the QL muscle, or at the junction of the external oblique and internal oblique aponeurosis and the QL.5
Nerves involved6:• Dermatomes T4 to L1
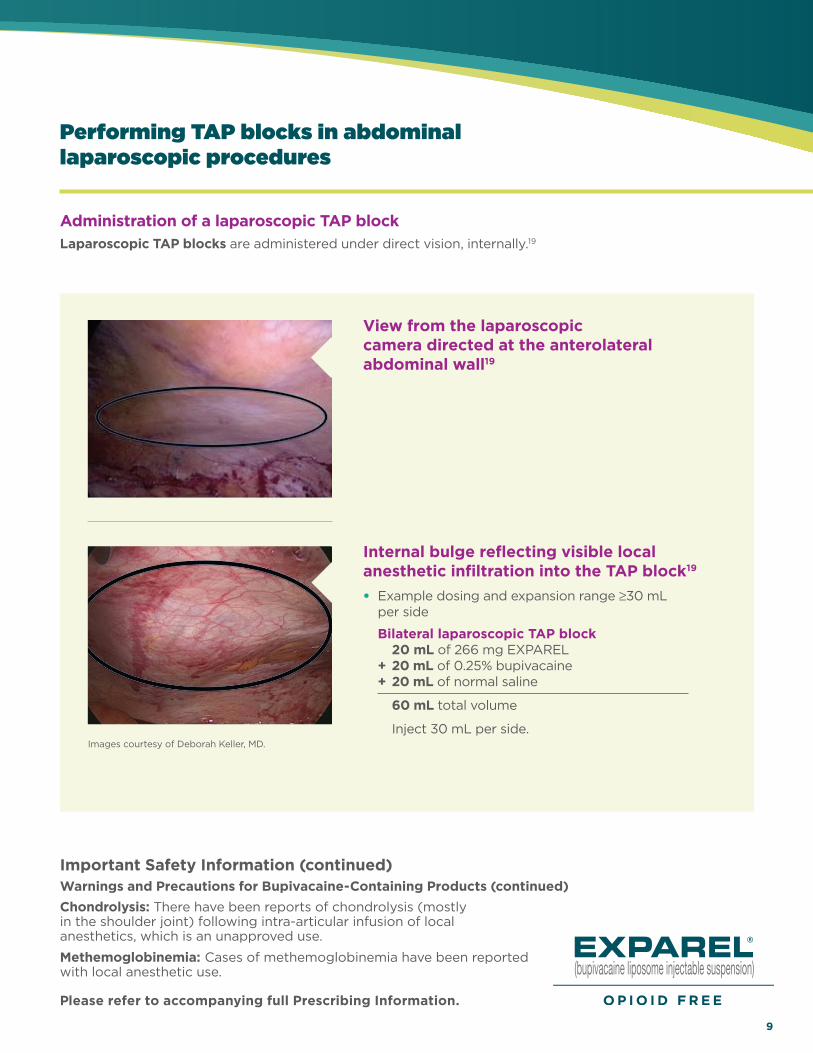
Administration of a laparoscopic TAP block Laparoscopic TAP blocks are administered under direct vision, internally.19
Med
ial Lateral
QLblock
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Chondrolysis: There have been reports of chondrolysis (mostly in the shoulder joint) following intra-articular infusion of local anesthetics, which is an unapproved use.
Methemoglobinemia: Cases of methemoglobinemia have been reported with local anesthetic use.
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Allergic Reactions: Allergic-type reactions (eg, anaphylaxis and angioedema) are rare and may occur as a result of hypersensitivity to the local anesthetic or to other formulation ingredients.
Suggested dose and volume range of EXPAREL for a QL block• Example dosing and expansion ≥25 mL per side
Bilateral QL block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 10 to 20 mL of normal saline
50 to 60 mL total volume
Inject 25 to 30 mL per side.
Images courtesy of Deborah Keller, MD.
Watch Dr Jacob Hutchins performing an abdominal field block with EXPAREL
Deep
Superficial
Common applications/procedures for a QL block• QL blocks have been used in procedures requiring
more extensive abdominal-wall coverage, including3,18
— Exploratory laparotomy, large-bowel resection, ileostomy, open or laparoscopic appendectomy, cholecystectomy
— Cesarean delivery, total abdominal hysterectomy — Open prostatectomy, renal transplant surgery,
nephrectomy
Peritoneum
EO
IO
TA
[5/Go 2016/p6/col1/par2/ln14-21]
[6/NYSORA/p1/para1/ln11-13]
[3/Borglum 2012/p82/par1/ln1-4][17/Eisharkawy 2015/p2/Indications/par1/ln1,2/bullets 1-3]
9
Please refer to accompanying full Prescribing Information.
Performing a QL block in more extensive abdominal surgeries
Performing TAP blocks in abdominal laparoscopic procedures
Administration of a laparoscopic TAP block Laparoscopic TAP blocks are administered under direct vision, internally.19
View from the laparoscopic camera directed at the anterolateral abdominal wall19
Internal bulge reflecting visible local anesthetic infiltration into the TAP block19
• Example dosing and expansion range ≥30 mL per side
Bilateral laparoscopic TAP block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 20 mL of normal saline
60 mL total volume
Inject 30 mL per side.
QLblock
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Chondrolysis: There have been reports of chondrolysis (mostly in the shoulder joint) following intra-articular infusion of local anesthetics, which is an unapproved use.
Methemoglobinemia: Cases of methemoglobinemia have been reported with local anesthetic use.
Important Safety Information (continued)Warnings and Precautions for Bupivacaine-Containing Products (continued)Allergic Reactions: Allergic-type reactions (eg, anaphylaxis and angioedema) are rare and may occur as a result of hypersensitivity to the local anesthetic or to other formulation ingredients.
Suggested dose and volume range of EXPAREL for a QL block• Example dosing and expansion ≥25 mL per side
Bilateral QL block 20 mL of 266 mg EXPAREL + 20 mL of 0.25% bupivacaine + 10 to 20 mL of normal saline
50 to 60 mL total volume
Inject 25 to 30 mL per side.
Images courtesy of Deborah Keller, MD.
Watch Dr Jacob Hutchins performing an abdominal field block with EXPAREL
Common applications/procedures for a QL block• QL blocks have been used in procedures requiring
more extensive abdominal-wall coverage, including3,18
— Exploratory laparotomy, large-bowel resection, ileostomy, open or laparoscopic appendectomy, cholecystectomy
— Cesarean delivery, total abdominal hysterectomy — Open prostatectomy, renal transplant surgery,
nephrectomy
[19/Chetwood 2011/p317/col2/par3/ln12-15]
[19/Chetwood 2011/p317/Fig1]
[19/Chetwood 2011/p317/Fig2]

10
Dosing considerations • Size of the surgical site• Volume needed to cover the width and depth of site• Patient factors that could impact safety of an
amide local anesthetic
• Maximum dose should not exceed 266 mg (20 mL)• Intended for single-dose administration only
Determine the right volume to cover the surgical site• Consider the size of the surgical site and the neuroanatomy• Expand the volume to disperse liposomes throughout the
surgical site• Enough multivesicular liposomes must be available at the
pain receptors to continuously release bupivacaine, ensuringlong-lasting analgesia
• TAP blocks require large volumes of local anesthetic to obtain reliable blockade
• For large surgical sites, the 266 mg (20 mL) vial of EXPAREL can be expanded with normal saline or lactated Ringer’s solution up to a total volume of 300 mL
Procedure Incisions Expanded volume
Open hysterectomy Intraumbilical midline incision T10 to L1 60 mL (TAP)
Small-bowel resection with primary anastomosis, ileostomy takedown, and removal of left subfascial port
Laparoscopic ports 60 mL (20 mL infiltration; 40 mL TAP)
Open abdominal-wall reconstruction
25-cm inverted-T incision with resection of skin and soft tissue
150 mL (50 mL infiltration; 100 mL field block)
Laparoscopic sleeve gastrectomy 2-cm incision in right midabdomen (15-mm trocar); 1.2-cm incision 8 cm above the umbilicus in the midline (10-mm trocar for camera); 0.7-cm incisions in left upper quadrant (5-mm trocar) in subxiphoid space (liver retractor) and in left lower quadrant (5-mm trocar)
220 mL (≈60 mL infiltration; ≈160 mL TAP)
Example expansion volumes are based on case reports that represent the individual experience of clinicians, and are intended to demonstrate their methodology for using EXPAREL in specifi c soft-tissue procedures. Pacira BioSciences, Inc. recognizes that there are alternative methodologies for administering local anesthetics, as well as individual patient considerations, when selecting the dose for a specifi c procedure.
Examples of expansion volumes by TAP procedure
Important Safety Information (continued)EXPAREL is contraindicated in obstetrical paracervical block anesthesia.
Image used with permission from Je� rey Gadsden, MD.
Dosing and administration information for EXPAREL
[PI/p2/section 2.2/¶1/bullets 1-3]
[PI/p2/section 1/¶1]
[PI/p2/section2.1/bullet4]
[20/Lee 2015/p2/col1/Figure 1]
[PI/p2/Sec2.2/bullet1]
[PI/p2/Sec2.2/bullet2,p19/Sec11/par1/ln3-4][PI/p19/Sec11/par1/ln3-4]
Data supported as extrapolation of PI,per Medical Reviewer

Please refer to accompanying full Prescribing Information.
11
OR
EXPAREL266 mg(20 mL)
+ Up to 30 mL of 0.5% bupivacaine HCl
150 mg total
30mL
Bupivacaine HCI0.5%
+ Up to 60 mL of 0.25% bupivacaine HCl
150 mg total
60mL
Bupivacaine HCI0.25%
• Admixing may impact the pharmacokinetic/pharmacodynamic properties of EXPAREL; the effect is concentration dependent
For early analgesic coverage, administer with bupivacaine HCl • Bupivacaine HCl may be administered immediately before EXPAREL or admixed in the same syringe
• Keep a 1:2 ratio of the milligram dose of bupivacaine HCl to EXPAREL. In determining the ratio, consider — One 20 mL vial of EXPAREL contains 266 mg of free-base bupivacaine, which is molar equivalent to
300 mg of bupivacaine HCl
— One 30 mL vial of 0.5% bupivacaine contains 150 mg of bupivacaine HCI
Example of admixing
Important Safety Information (continued)Adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via infiltration were nausea, constipation, and vomiting; adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via interscalene brachial plexus nerve block were nausea, pyrexia, and constipation.
If EXPAREL and other non-bupivacaine local anesthetics, including lidocaine, are administered at the same site, there may be an immediate release of bupivacaine from EXPAREL. Therefore, EXPAREL may be administered to the same site 20 minutes after injecting lidocaine.
[PI/p3/Sec2.4/bullet2]
[PI/p3/Sec2.4/bullet2,p4/par1]
[PI/p2/Sec2.2/par1/ln1-2,p4/Sec3/bullet1]Data supported as extrapolation of PI, per Medical Reviewer.
[PI/p3/Sec2.4/bullet2]
[PI/p1/col2/Drug Interactions/bullet2,p3/Sec2.4/bullet2]
EXPAREL is indicated for single-dose infiltration in adults to produce postsurgical local analgesia and as an interscalene brachial plexus nerve block to produce postsurgical regional analgesia. Safety and efficacy have not been established in other nerve blocks.
Please see Important Safety Information throughout and refer to accompanying full Prescribing Information.
THE USE OF EXPAREL IN ABDOMINAL-WALL FIELD BLOCKS
IndicationEXPAREL is indicated for single-dose infiltration in adults to produce postsurgical local analgesia and as an interscalene brachial plexus nerve block to produce postsurgical regional analgesia. Safety and efficacy have not been established in other nerve blocks.
Important Safety Information EXPAREL is contraindicated in obstetrical paracervical block anesthesia.
Adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via infiltration were nausea, constipation, and vomiting; adverse reactions reported with an incidence greater than or equal to 10% following EXPAREL administration via interscalene brachial plexus nerve block were nausea, pyrexia, and constipation.
If EXPAREL and other non-bupivacaine local anesthetics, including lidocaine, are administered at the same site, there may be an immediate release of bupivacaine from EXPAREL. Therefore, EXPAREL may be administered to the same site 20 minutes after injecting lidocaine.
EXPAREL is not recommended to be used in the following patient population: patients <18 years old and/or pregnant patients.
Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease.
Warnings and Precautions Specific to EXPARELAvoid additional use of local anesthetics within 96 hours following administration of EXPAREL.
EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks other than interscalene brachial plexus nerve block, or intravascular or intra-articular use.
The potential sensory and/or motor loss with EXPAREL is temporary and varies in degree and duration depending on the site of injection and dosage administered and may last for up to 5 days, as seen in clinical trials.
Warnings and Precautions for Bupivacaine-Containing ProductsCentral Nervous System (CNS) Reactions: There have been reports of adverse neurologic reactions with the use of local anesthetics. These include persistent anesthesia and paresthesia. CNS reactions are characterized by excitation and/or depression.
Cardiovascular System Reactions: Toxic blood concentrations depress cardiac conductivity and excitability which may lead to dysrhythmias, sometimes leading to death.
Allergic Reactions: Allergic-type reactions (eg, anaphylaxis and angioedema) are rare and may occur as a result of hypersensitivity to the local anesthetic or to other formulation ingredients.
Chondrolysis: There have been reports of chondrolysis (mostly in the shoulder joint) following intra-articular infusion of local anesthetics, which is an unapproved use.
Methemoglobinemia: Cases of methemoglobinemia have been reported with local anesthetic use.
6 millionpatients have received non-opioid EXPAREL
since 201220
Visit www.EXPAREL.com to learn more.
Please refer to accompanying full Prescribing Information.For more information, please visit www.EXPAREL.com or call 1-855-RX-EXPAREL (793-9727).References: 1. Gadsden J, Ayad S, Gonzales JJ, Mehta J, Boublik J, Hutchins J. Evolution of transversus abdominis plane infi ltration techniques for postsurgical analgesia following abdominal surgeries. Local Reg Anesth. 2015;8:113-117. 2. Young MJ, Gorlin AW, Modest VE, Quraishi SA. Clinical implications of the transversus abdominis plane block in adults. Anesthesiol Res Pract. 2012;2012:731645. doi:10.1155/2012/731645. 3. Børglum J, Jensen K. Abdominal surgery: advances in the use of ultrasound-guided truncal blocks for perioperative pain management. In: Derbel F, ed. Abdominal Surgery. Rijeka, Croatia: InTech; 2012:69-94. 4. Niraj G, Kelkar A, Powell R. Ultrasound-guided subcostal transversus abdominis plane block. International Journal of Ultrasound and Applied Technologies in Perioperative Care. 2010;1(1):9-12. 5. Go R, Huang YY, Weyker PD, Webb CA. Truncal blocks for perioperative pain management: a review of the literature and evolving techniques. Pain Manag. 2016;6(5):455-468. 6. Ultrasound-guided transversus abdominis plane and quadratus lumborum blocks. New York School of Regional Anesthesia website. https://www.nysora.com/regional-anesthesia-for-specifi c-surgical-procedures/abdomen/ultrasound-guided-transversus-abdominis-plane-quadratus-lumborum-blocks. Accessed April 23, 2019. 7. Detton AJ. Grant’s Dissector. 16th ed. Philadelphia, PA: Wolters Kluwer; 2017:109. 8. Rafi AN. Abdominal fi eld block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024-1026. 9. McDonnell JG, O’Donnell BD, Farell T, et al. Transversus abdominis plane block: a cadaveric and radiological evaluation. Reg Anesth Pain Med. 2007;32(5):399-404. 10. Webster K. Ultrasound guided rectus sheath block-analgesia for abdominal surgery. Update Anaesth. 2010;26:12-17. 11. Favuzza J, Brady K, Delaney CP. Transversus abdominis plane blocks and enhanced recovery pathways: making the 23-h hospital stay a realistic goal after laparoscopic colorectal surgery. Surg Endosc. 2013;27(7):2481-2486. 12. Chen CK, Tan PC, Phui VE, Teo SC. A comparison of analgesic e� cacy between oblique subcostal transversus abdominis plane block and intravenous morphine for laparoscopic cholecystectomy. A prospective randomized controlled trial. Korean J Anesthesiol. 2013;64(6):511-516. 13. Harish R. Low-dose infusion with “surgical transverse abdominis plane (TAP) block” in open nephrectomy. Br J Anaesth. 2009;102(6):889-890. 14. Hutchins J, Delaney D, Vogel RI, et al. Ultrasound guided subcostal transversus abdominis plane (TAP) infi ltration with liposomal bupivacaine for patients undergoing robotic assisted hysterectomy: a prospective randomized controlled study. Gynecol Oncol. 2015;138(3):609-613. 15. Børglum J, Maschmann C, Belhage B, Jensen K. Ultrasound-guided bilateral dual transversus abdominis plane block: a new four-point approach. Acta Anaesthesiol Scand. 2011;55(6):658-663. 16. Bhakta A, Glotzer O, Ata A, Tafen M, Stain S, Singh P. Analgesic e� cacy of laparoscopic guided transverse abdominis plane block using liposomal bupivacaine in bariatric surgery. Am J Surg. 2018;215(4):643-646. 17. Yarwood J, Berrill A. Nerve blocks of the anterior abdominal wall. Cont Educ Anaesth Crit Care Pain. 2010;10(6):182-186. 18. Elsharkawy H. Ultrasound-guided quadratus lumborum block: how do I do it? American Society of Regional Anesthesia and Pain Medicine website. https://www.asra.com/pain-resource/article/48/ultrasound-guided-quadratus-lumborum-blo. Accessed April 1, 2019. 19. Chetwood A, Agrawal S, Hrouda D, Doyle P. Laparoscopic assisted transversus abdominis plane block: a novel insertion technique during laparoscopic nephrectomy. Anaesthesia. 2011;66(4):317-318. 20. Data on fi le. 5903. Parsippany, NJ: Pacira BioSciences, Inc.; October 2019.
©2019 Pacira BioSciences, Inc.Parsippany, NJ 07054 PP-EX-US-4903 11/19