the use of cannabis-based medicinal …...the use of cannabis-based medicinal products (cbmps) in...
TRANSCRIPT

THE USE OF CANNABIS-BASED MEDICINAL PRODUCTS (CBMPS) IN EPILEPSY
BY DR SAOIRSE O’SULLIVAN Professor at the University of Nottingham and Science Lead of the CMC

2The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Glossary 3
Introduction 4UK Legislative context 4Current guidelines for CBMP in Epilepsy 4
Introductiontocannabisandcannabinoids 5
Introductiontotheendocannabinoidsystem 5
Cannabidiol 6 Flavonoids and terpenes 6 Isolate versus full spectrum CBD 6 The entourage hypothesis 7
CurrentlylicensedCBMPmedicines 7
CBMPuseinepilepsy 8
Scientificandclinicalevidence 8 Animal data and mechanisms of action of cannabidiol 8 Animal data and mechanisms of action of other phytocannabinoids 8 Summary of clinical trial data with CBMPs in epilepsy 9 Effective doses and delivery mechanisms in Epilepsy 10 Bioavailability 11 Potential drug-drug interactions (DDIs) 11 Side effects 11 Registered and ongoing trials with CBMPs in epilepsy 11 Cannabis-based medicines and driving 13
Patienttestimonies 14
Clinician’stestimonies 18 Professor David Neubauer 18 Zeid Mohamedali 18
Summary 19
Acknowledgements 19
Contents

3The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
AEA: anandamide, the first identified endogenous (made in our body) cannabinoid
Bioavailability: the ability of a medicine to get into our bloodstream
CB1: the first identified cannabinoid receptor
CB2: the second identified cannabinoid receptor
CBD: cannabidiol, phytocannabinoid that does not cause a high
CBMPs: Cannabis-based medicinal products
Clinicaltrial: an investigation of the effectiveness of a medicine, usually in comparison to
placebo and/or standard care (controlled)
DDI: drug-drug interactions, when one medicine interferes with the action of another
medicine
Dronabinol: synthetic THC, licensed in the US
Epidiolex: pure CBD produced as a medicine licensed in epilepsy in the US
Nabilone: a structural analogue of THC, licensed in the US and UK
Primaryendpoint: the main outcome of a clinical trial the investigators hypothesise will be
positively changed by a medicine (usually a pain rating in this subject area)
RCT: randomised controlled trial, the gold standard of clinical research
Sativex: CBD:THC in a 1:1 ratio licensed internationally for spasticity in MS, also known as
nabiximols
Secondaryendpoint: additional supportive or important outcomes of a clinical trial the
investigators think will be positively changed by a medicine (often includes quality of life
scores)
Sublingually: a medicine taken under the tongue, common for CBMPs
THC: Δ9-tetrahydrocannabinol, an abundant metabolite of the Cannabis plant that causes
the ‘high’
Glossary

4The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Introduction
UK Legislative context
In the summer of 2018, Home Secretary Sajid Javid announced the UK would be making medicinal cannabis available after receiving advice from Professor Dame Sally Davies, Chief Medical Officer for England and Chief Medical Adviser to the UK government, that cannabis-based medicinal products should be moved out of a Schedule 1 classification. On November 1, 2018, cannabis-based medicinal products (CBMPs) were rescheduled to allow lawful prescription as unlicensed medicines by specialist doctors (consultants)1. The Home Office definition of a CBMP is as follows:
• the product is or contains cannabis, cannabis resin, cannabinol or cannabinol derivatives
• the product must be produced for medicinal use in humans
• it must be a product that is regulated as a medicinal product or an ingredient of a medicinal product
Current guidelines for CBMPs in Pain
The government asked for interim guidance on the medicinal use of CBMPs in epilepsy from the British Paediatric Neurology Association (BPNA). Their report states that ‘There is good quality clinical evidence that CBD has an anti-epileptic effect in two
severe epilepsy syndromes (Dravet Syndrome and Lennox-Gastaut Syndrome) and evidence from open-label studies and animal studies that it is likely to have an anti-epileptic effect in the epilepsies in general’.2
The BPNA welcomes the rescheduling of CBPMs but recommend that the products undergo randomised clinical trials for efficacy and safety. Their report recommends that ‘Prescription of a non-licensed cannabis-based product for medicinal use should be used as a treatment of last resort for children who meet the following three criteria:
• Have an epilepsy that has proven intractable to treatment with conventional licensed anti-epileptic drugs given at therapeutic doses
• Have not responded to the ketogenic diet or for whom the diet is inappropriate
• Are not candidates for epilepsy surgery
They ‘advise that pure CBD (Epidiolex®) should be the default choice when considering prescription of a CBPM in intractable epilepsy in children’ and they ‘do not recommend prescribing other non-licensed cannabis-based products for medicinal use’.
The National Institute for Health and Care Excellence (NICE) is currently defining the final guidelines which will be published no later than October 2019. The scope of the NICE recommendations will include all people with severe treatment-resistant epilepsy3.
1 https://www.gov.uk/government/news/government-announces-that-medicinal-cannabis-is-legal2 https://www.bpna.org.uk/userfiles/BPNA_CBPM_Guidance_Oct2018.pdf3 https://www.nice.org.uk/guidance/gid-ng10124/documents/final-scope

5The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Introduction to cannabis and cannabinoids
The Cannabis sativa plant produces hundreds of chemicals which are concentrated in structures called glandular trichomes on the flower of the plant. These chemicals are known as cannabinoids; or more specifically, phytocannabinoids, because they come from the plant. Usually, the most abundant phytocannabinoid found in cannabis flowers is Δ9-tetrahydrocannabinol (THC). THC normally comprises about 10-18% of the chemicals depending on the cannabis plant strain. This is the psychotropic (mood altering) chemical that produces the responses in our body that you might be familiar with; euphoria (feeling high), wanting to eat, effects on memory and analgesia (the ability to relieve pain). Normally, the next most abundant cannabinoid is cannabidiol (CBD). CBD is the chemical that makes you feel mellow and reduces anxiety, and is evidenced to be useful in a wide range of disorders such as epilepsy, schizophrenia, post-traumatic stress disorder (PTSD) and stroke.
The definition of a cannabinoid can involve chemicals other than those phytocannabinoids that come from the plant, and can include chemicals that are similar to phytocannabinoids and that bind to the cannabinoid receptors in our body. This includes synthetic cannabinoids that are manufactured artificially (these may be structurally similar or identical to phytocannabinoids or structurally diverse such as street “spice”) and endocannabinoids, chemicals that are produced within our bodies to control a range of processes.
Introduction to the endocannabinoid system
Initial scientific thinking was that cannabis had a non-specific effect on the function of cells in our body. However, approximately 30 years ago, it was discovered that there are particular proteins (termed receptors) on the surface of our cells that recognise and bind cannabinoids, resulting in a change in the function of these proteins, leading to the effects we recognise when people consume Cannabis preparations. The first receptor discovered was called the cannabinoid receptor 1 (CB1). Activation of CB1 is the way THC brings about most of its biological effects such as euphoria, appetite stimulation and analgesia. The CB1 receptor is found all over the body, but has particularly high levels across the brain.
The second cannabinoid receptor, called cannabinoid receptor 2 (CB2) was discovered a couple of years later. It is expressed particularly in cells of the immune system. Levels of this receptor are increased in many tissues, however, when there is damage or infection.
After the discovery of cannabinoid receptors in our body, people began to investigate whether we produce chemicals within our body that bind to these receptors, and quickly discovered a molecular derived from fatty acids called arachidonoylethanolamine (also known as anandamide, AEA). AEA is similar to THC in that it can activate both CB1 and CB2. A second compound called 2-arachidonoylglycerol (2-AG, also activates CB1 and CB2) was also found soon afterwards. These compounds were termed ‘endocannabinoids’ and we now know that these represent two families of endocannabinoids which are formed through independent pathways in our bodies.

6The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
4 https://www.who.int/medicines/access/controlled-substances/CannabidiolCriticalReview.pdf
The endocannabinoid system is involved in almost every biological function in the body, in the central nervous system but also in all organs; dysregulation of the endocannabinoid system contributes to many disease states including pain.
Cannabidiol
CBD is the second most abundant phytochemical found in the cannabis plant. It is found in the plant as its acidic precursor, cannabidiolic acid (CBDA), which is converted to CBD with light, heat and time. Unlike THC, CBD does not have psychotropic effects. This is because it doesn’t activate the CB1 receptor in the brain. CBD also does not activate the CB2 receptor, making it very different to THC. From a pharmacology (the study of how drugs work) point of view, CBD is a really interesting chemical because it interacts with many different protein receptors and enzymes in the body, which may help to bring about the many beneficial effects of CBD. CBD is already available as a medicine in the drug Sativex(R) (1:1 ratio of THC: CBD, licensed for spasticity in MS) and as Epidiolex (R) (Pure CBD, licensed for epilepsy). According to a report by the World Health Organisation4, ‘in its pure state, cannabidiol does not appear to have abuse potential or cause harm’ and that ‘CBD is generally well tolerated with a good safety profile’. WHO also recognised the potential of CBD as a medicine in several disorders.
Flavonoids and terpenes
As well as the phytocannabinoids produced by the cannabis plant, other chemicals are also found, including flavonoids, cannaflavins and terpenes.
Although we know less about these chemicals than we do about phytocannabinoids, there is some evidence to suggest that these compounds have therapeutic properties which add to, or potentially even synergise with, those of the phytocannabinoids.
There are about 20 flavonoids produced by the cannabis plant, and these can have their own biological effects including anti-inflammatory, antioxidant, anti-fungal, ant-tumoral and anti-bacterial properties. The important flavonoids produced by the cannabis plant include cannflavine A, cannflavine B, cannflavine C, vitexin, isovitexin, apigenin, kaempferol, quercetin, luteolin and orientin.
Terpenes are plant essential oils and there are more than 200 terpenes found in cannabis. Terpenes are responsible for the smell, taste, and colour of cannabis. Some of the important terpenes produced by the cannabis plant include (but are not limited to) onene, ß-caryophyllene, linalool, limonene, pinene, humelene, and B-myrcene. Like flavonoids, terpenes have their own biological effect and are suggested to be anti-inflammatory and neuroprotectant. ß-caryophyllene has also been shown to activate the CB2 receptor.
Isolate versus full spectrum CBD
CBD products can be pure CBD or CBD-rich extracts (also sometimes known as full spectrum CBD). Purified CBD will be as close as possible to just pure CBD with no other chemicals present. CBD-rich extracts will be predominantly CBD, but with other chemical entities such as other phytocannabinoids (which might include trace

7The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
5 https://www.epidiolex.com/6 https://bnf.nice.org.uk/drug/nabilone.html7 http://marinol.com/8 http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con2033379.pdf
amounts of THC), flavonoids and terpenoids. Purified CBD can come from either the hemp or marijuana plant, or be synthetically manufactured. CBD-rich extracts can derive from either the hemp or marijuana (more likely to contain THC), and thus the profile of the associated phytocannabinoids, flavonoids and terpenoids will be different between these two plants.
The entourage hypothesis
The entourage hypothesis is a proposed mechanism by which small quantities of other chemicals from the plant enhance the effect of the major chemicals (THC or CBD) of the plant. This could be the effect of multiple phytocannabinoids on each other, or the effect of flavonoids, cannaflavins and terpenes on phytocannabinoids, or both. This is still an under-investigated research area and it is not clear where the important synergistic relationships, if any, might lie. Clinically, no studies have looked at direct comparisons between pure phytocannabinoids and enriched extracts.
The term ‘entourage effect’ is also used in relation to the endocannabinoid system where there can be competition inhibition of endocannabinoids for their degradation enzymes which can indirectly increase endocannabinoids levels, and therefore indirectly cause CB1 and CB2 activation.
Currently licensed CBMP medicines
The Home Office definition of a CBMP represents an incredibly broad potential range of products which potentially complicates clinical decision making. We recommend that there are four types of CBMPs for which we have clinical trial evidence:
• CBD only products (such as Epidiolex5, which is licensed in the US for seizure reduction in epilepsy)
• THC only products (such as nabilone6 (a molecular similar to THC, licensed in the US and UK) and dronabinol7 (a synthetic version of THC, licensed in the US), which are licensed for HIV/AIDS induced anorexia and chemotherapy induced nausea and vomiting)
• Products that have a CBD:THC ratio of 1:1 (such as Sativex8, which is licensed internationally for spasticity in MS. However, it should also be recognised that Sativex also contains other plant products in small quantities)
• Whole flower products (such as Bedrocan Flos or similar flower products) which can be purchased with specific ratios of THC:CBD according to the patient’s preference
In epilepsy, CBD (pure or enriched extracts) and CBD:THC ratio products have been tested in patients.

8The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
CBMP use in epilepsy
There is a long history in the use of cannabis as a medicine for the reduction in seizures, first documented in 1843 by the physician W.B.O’Shaughnessy for benefits in infantile convulsions9. Clinical trial work in the late seventies/early eighties in Israel then demonstrated a particular potential benefit of CBD in epilepsy10. Over the next 30 years, several case reports, anecdotes and patient surveys supported the use of CBD to reduce seizures in epilepsy. The first randomised controlled trial (RCT) using the pure CBD product Epidiolex was published in 2015. As a result of several subsequent positive clinical trials with Epidiolex in more than 500 patients in total, this medicine was approved in the US for the treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome. In addition to pure CBD, artisanal preparations of CBD which contain other phytocannabinoids and phytocannabinoids are also widely used in patients with epilepsy. The scientific and clinical evidence behind the effectiveness of CBMPs in epilepsy is now discussed.
Scientific and clinical evidence
Animal data and mechanisms of action of cannabidiol
Cannabidiol is a compound with many molecular targets in the body (sometimes known as polypharmacology). Whilst it is not particularly
potent at any particular target (which is often the strategy with novel drug discovery), its ability to interact with many different enzymes, ion channels and receptors may underlie its ability to modulate seizures and other symptoms in epilepsy. Based on animal data, some of the proposed mechanisms of action of CBD in epilepsy include the following; some or all of which might be important in patient populations:
• TRPV1 desensitisation leading to normalisation of calcium levels
• Direct inhibition of calcium ion channels
• Serotonin receptor activation
• Opioid receptor inhibition
• Glycine receptor inhibition
• Sigma 1 receptor inhibition
• GPR55 (an orphan receptor) inhibition
• Increasing endocannabinoid levels (and thus CB1 or CB2 activation) by inhibiting their degradation
• Enhancement of the effects of typical anti-epileptic medication by inhibiting their breakdown
Animal data and mechanisms of action of other phytocannabinoids
Although the cannabinoid most recognised for anti-epileptic actions is CBD, other phytocannabinoids might also have beneficial effects in this area.
9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2490264/pdf/provmedsurgj00865-0001.pdf10 https://www.ncbi.nlm.nih.gov/pubmed/7413719
9The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
11 https://www.epilepsybehavior.com/article/S1525-5050(16)30579-0/fulltext12 http://ir.gwpharm.com/news-releases/news-release-details/gw-pharmaceuticals-announces-preliminary-results-phase-2a-study13 https://www.ncbi.nlm.nih.gov/pubmed/3025839814 https://www.ncbi.nlm.nih.gov/pubmed/30949046
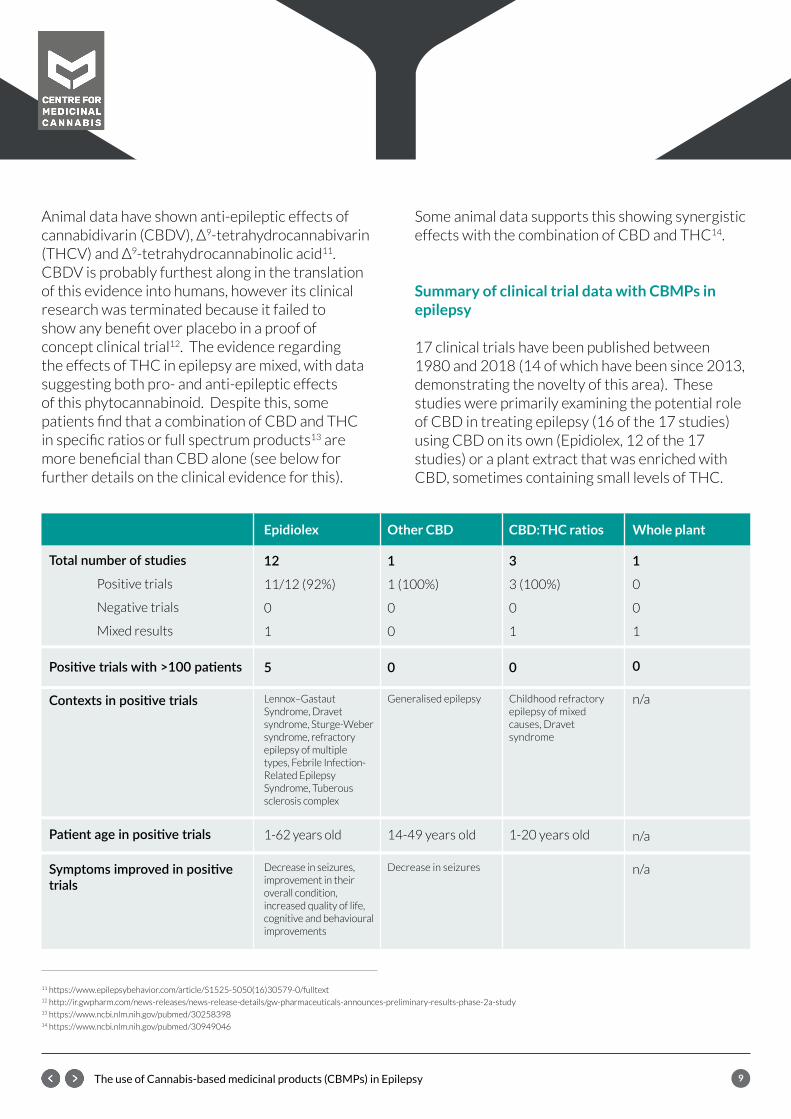
Animal data have shown anti-epileptic effects of cannabidivarin (CBDV), Δ9-tetrahydrocannabivarin (THCV) and Δ9-tetrahydrocannabinolic acid11. CBDV is probably furthest along in the translation of this evidence into humans, however its clinical research was terminated because it failed to show any benefit over placebo in a proof of concept clinical trial12. The evidence regarding the effects of THC in epilepsy are mixed, with data suggesting both pro- and anti-epileptic effects of this phytocannabinoid. Despite this, some patients find that a combination of CBD and THC in specific ratios or full spectrum products13 are more beneficial than CBD alone (see below for further details on the clinical evidence for this).
Some animal data supports this showing synergistic effects with the combination of CBD and THC14.
Summary of clinical trial data with CBMPs in epilepsy
17 clinical trials have been published between 1980 and 2018 (14 of which have been since 2013, demonstrating the novelty of this area). These studies were primarily examining the potential role of CBD in treating epilepsy (16 of the 17 studies) using CBD on its own (Epidiolex, 12 of the 17 studies) or a plant extract that was enriched with CBD, sometimes containing small levels of THC.
Totalnumberofstudies
Positive trials
Negative trials
Mixed results
Positivetrialswith>100patients
Contextsinpositivetrials
Patientageinpositivetrials
Symptomsimprovedinpositivetrials
Epidiolex
12
11/12 (92%)
0
1
5
Lennox–Gastaut Syndrome, Dravet syndrome, Sturge-Weber syndrome, refractory epilepsy of multiple types, Febrile Infection-Related Epilepsy Syndrome, Tuberous sclerosis complex
1-62 years old
Decrease in seizures, improvement in their overall condition, increased quality of life, cognitive and behavioural improvements
Other CBD
1
1 (100%)
0
0
0
Generalised epilepsy
14-49 years old
Decrease in seizures
CBD:THC ratios
3
3 (100%)
0
1
0
Childhood refractory epilepsy of mixed causes, Dravet syndrome
1-20 years old
Whole plant
1
0
0
1
0
n/a
n/a
n/a

10The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
A summary of the clinical trials examining the effects of CBMPs in epilepsy. Positive trials saw a significant change in the primary outcome of the trial and negative trials did not show a change in the primary outcome.
88% of clinical trials in epilepsy were successful using any CBMP and 92% were successful when using CBD alone (usually in the form of Epidiolex). Although Epidiolex now has FDA approval specifically for Lennox-Gastaut syndrome and Dravets syndrome, CBD was able to significant reduce seizures across many other forms of epilepsy in both children and adults. As well as seizure reduction, these studies showed a significant improvement in the overall condition of patients, increased quality of life, and cognitive and behavioural improvements.
3 observational/retrospective studies using a fixed CBD:THC ratio of either 20:1 or 50:1 showed seizure reductions in their patient populations, advocating that randomised controlled trials using these novel ratios should be undertaken.
A paper published in September 2018 examined the potential clinical benefits of CBD-rich Cannabis extracts (i.e. those containing other chemicals from the plant but in low quantities) over purified CBD in treatment-resistant epilepsy15. In this observational analysis, they report that patients treated with CBD-rich extracts reported lower average dose (6.1 mg/kg/day) than those using purified CBD (27.1 mg/kg/day). They also report that the mild and severe adverse effects of the products were more frequent in those containing purified CBD than in CBD-rich extracts. The authors conclude that ‘CBD-rich extracts seem to present a better therapeutic profile than purified CBD, at least in this population of patients with refractory epilepsy. The roots of this
difference is likely due to synergistic effects of CBD with other phytocompounds (aka Entourage effect), but this remains to be confirmed in controlled clinical studies’. However, it is important to emphasise that the trials being compared are not of similar design; the trials with purified CBD (Epidiolex) were randomised controlled trials in larger patient numbers, while those with CBD-rich extracts were often uncontrolled, observational studies. Head to head clinical trials comparing pure CBD against CBD-rich extracts are urgently required to test this.
Effective doses and delivery mechanisms in Epilepsy
In trials that have used epidiolex, patients were generally started at 2–5 mg/kg and titrated up by 2–5 mg/kg per week to a maximum dose of 25 mg/kg/day. Other studies with CBD have gone to a maximum of 50 mg/kg. The average effective dose of epidiolex is about 20mg/kg/day in Dravet and Lennox-Gastaut syndromes. The route of delivery in all trials with CBD has been orally, as a solution (Epidiolex) or as a sublingual oil (with CBD-rich extracts). Various CBD:THC ratios that have been tested clinically have also been delivered orally in an oil. These studies had lower average doses (6 mg/kg/day). In an observation study16, 17 patients transferred successfully from oil extract to inhaled CBMP. Transfer or addition of inhaled CBD-enriched cannabis caused additional improvement (20–40%) in 6 of these patients. Further studies are required to test whether inhalation is a better or equally efficacious mechanism of CBD administration in patients.
SmokingCBMPsisnotallowedunderthenewlegislation.
15 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6143706/16 https://www.sciencedirect.com/science/article/pii/S0387760418301128
11The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Bioavailability
Phytocannabinoids have low oral bioavailability (which means that they don’t easily get into our bloodstream when taken orally) because they are highly lipophilic (fat loving) compounds. Some suggested mechanisms to improve phytocannabinoid drug delivery. In the future this could mean lower doses of CBMPs such as CBD are required (perhaps for example by inhalation). Several studies suggest that CBMPs including CBD are better absorbed in the body when taken after food, and are therefore usually recommended to be taken with food when administered orally17.
Potential drug-drug interactions (DDIs)
The patient information sheets for Epidiolex contains moderately strong statements regarding drug drug interactions (DDI). This can require dose titration up or down of other co-administered drugs because of the ability of CBD to interfere with the metabolism (breakdown) of anti-epileptic medicines in the liver. DDIs have been reported with Epidiolex and medicines that are metabolised by the liver enzymes CYP2C19 and CYP3A4, where CBD inhibits the metabolism of medicines normally broken down by these liver enzymes. Increased plasma levels of clobazam, rufinamide, topiramate, zonisamide, and eslicarbazepine have been reported18. Generally, patients have had to reduce the dosage of medications that have been inhibited by CBD, and this is most common with Clobezam and Valproate. There is also one case report of a DDI with CBD and warfarin, possibly because of competitive inhibition at CYP2C9 or CYP3A4.
Side effects
In the published clinical trials, CBMPs were usually well tolerated by epileptic patients although side
effects were frequent. The most common side effects (remembering most of these are pure CBD studies) were sleepiness/sedation, fever, decreased appetite/weight loss, diarrhoea and nausea/vomiting. Side effects can be resolved by dose reduction. Sometimes the side-effects observed with CBD medications are actually due to side effects of concurrent medication that is now at higher plasma concentrations because of the inhibition of metabolism by CBD. This is particularly true of concomitant use of Valproate and CBD and side-effects associated with liver function leading to raised liver enzymes19. The BPNA20 recommend that ‘liver function tests should be taken at baseline, 2-weeks post the initiation of therapy and 2-weeks after each increment in dose. They should then be performed at regular intervals or on the occurrence of a clinically relevant event’.
Registered and ongoing trials with CBMPs in epilepsy
The use of CBMPs in epilepsy is still in its infancy and many clinical trials to further our knowledge in this area are underway across the world, including trials in types of epilepsy other than Lennox-Gastaut syndrome or Dravet syndrome, in young and adult patient. These are listed in the below table. Some of the novel CBMPs that are being clinically tested (and may be licensed in the future as medicines) in epilepsy include:
• INS011-14-030, a pure, synthetic CBD developed by Insys Therapeutics
• PTL101, a hard capsule pure CBD product developed by PhytoTech Therapeutics
• CanniMed 1:20, a CBD:THC 20:1 ratio product provided as an oil-based suspension made by CanniMed Therapeutics Inc
• TIL-TC150, a cannabis plant extract produced by Tilray, containing 100 mg/mL CBD and 2 mg/mL THC (50:1 ratio)
17 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6223703/18 https://onlinelibrary.wiley.com/doi/full/10.1111/epi.1385219 https://www.mdpi.com/1420-3049/24/8/145920 https://www.bpna.org.uk/userfiles/BPNA_CBPM_Guidance_Oct2018.pdf

12The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
A list of registered and on-going clinical trials with CBMPs in epilepsy.

13The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Cannabis-based medicines and driving
If you are an adult and someone who is eligible to drive under the DVLA regulations21, it may be relevant to you to know the rules about CBMPs and driving. It is an offence to drive whilst impaired through drugs (whether due to non-medical use of drugs or due to legitimate use of medicines) in Section 4 of the Road Traffic Act 1988. There is also a new offence which refers to driving, attempting to drive or being in charge of a vehicle with a specified controlled drug in the body, in excess of a specified limit (Section 5A of the Road Traffic Act 1988 as amended in April 2013), which includes THC set at a very low limit.
It is a driver’s responsibility to decide whether they consider their driving is, or they believe might be, impaired on any given occasion. Based on existing best practice, current advice given to patients about issues related to ‘medicines and driving’ typically covers the following points, as relevant to each case:
1. Not to drive if any symptoms or signs develop suggesting that their driving may be impaired, such as experiencing sleepiness, poor coordination, impaired or slowed thinking, dizziness, or visual problems.
2. Not to drive at certain times when the risk may be temporarily increased, for example, when first starting, or when first increasing or reducing the dose of, a medicine that may potentially impair their driving.
3. To take particular care in circumstances that may increase the risk of their driving being impaired whilst taking their medicine, and to avoid driving if this occurs.
4. To be aware that alcohol taken in combination with other impairing drugs can substantially increase the risk of accidents.
It should be remembered that some of the side-effects of CBD are dizziness and drowsiness, so patients should take responsibility with CBD products and driving. If you are stopped by the police, a new ‘medical defence’ can be raised for the offence if drivers are taking medication as directed and found to be over the limit and not impaired22.
21 https://www.gov.uk/epilepsy-and-driving22 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/325275/healthcare-profs-drug-driving.pdf

14The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Patient testimonies
Olivia Glennie
‘Hello my name is Olivia Glennie and I was diagnosed with Epilepsy, when I was 16 years old. My seizures include absences, myoclonic and tonic clonic. My doctor at the time decided to put me on the drug Epilim, which I stayed on for 3 years. Struggling to come to terms with my health as a rebellious teen, I stopped taking my medication altogether for 2 years out of my own free will.A random grand mal seizure occurred when I was 21, and was advised to go back onto medication but this time on lamotrigine. I had an aggressive skin reaction and was then introduced to try Keppra.
Keppra is my current medication and I have been taking it for the last 6 and a half years. The side effects for me included a foggy mind, deteriorated memory, irrational mood swings, anxiety, headaches and tiredness. I decided to talk to others away from my doctor to see what they can advise to help. So became fully committed to improving my lifestyle, diet and general wellbeing.
A year and a half ago I had the pleasure of being introduced to Chelsea Leyland through a friend from school. My friend mentioned she had managed to control her epilepsy by weening off her drugs using a natural substance, CBD. Her story inspired me and encouraged me to reach out and find out more. Everything we discussed was relatable, same side effects, same struggles, it was such a heart warming moment to finally speak to someone who truly understand the mindset of an epileptic. Being carefully warned ‘what works for one, doesn’t work for everyone’, I still wanted to take the plunge and try and see if CBD was a possibility for me too. So I started the process gradually, taking each day as it comes. Staying on my 2000mg keppra daily while taking 2-3 drops of CBD in the morning and night.
After 6 weeks I started to decrease my medication be 500 mg replacing it with a quarter pipette of 15 mg CBD. Letting my body get used to this new amount I noticed quite quickly how clear my thoughts were becoming, the ability to concentrate became easier and the headaches were fading. After 4 months I took my Keppra down again another 500 mg this time replacing half a pipette with 30 mg. This time I noticed a much more balanced general mood. I didn’t have to try so hard to keep my true feelings together – I just felt as though my moods were normalising.
Another 500 mg down of Keppra after another 4 months, I felt really strange. Not because of the CBD but because of so much of the drugs leaving my system, I was relearning myself as a normal human after compressing these irritational feelings for so long, and now I no longer had to. I was getting better. The drugs had been in my system for so long my body felt overwhelmed when so much had left.
Recently, I have halved again to my lowest yet. I am currently on 250mg of Keppra and am taking 50 mg of CBD only a quarter pipette.My side effects I’ve noticed have been tiredness but that is all so far. It has been extremely uplifting to find something that is able to neutralise all the other side effects.
15The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Getting support from a doctor was something I really needed but every time I tried to speak with someone they said they are unable to offer any advise. So it ended up being something I had to take into my own hands with the support of others around me who it had worked for. I hope sometime soon this matter will change, as CBD has been life changing for me and could be also for so many others.’
Anonymous
‘When I was 15, I was diagnosed with a low threshold to epilepsy after collapsing at school and suffering from repeated Grand Mal (Tonic clonic seizure) in 2015. After which I was placed on Carbamazepine for 2 years (2 x 100mg/day). After remaining seizure free I was slowly weaned off the medication. Before I started taking this medication, I was a straight “A” student, being placed in all of the top sets at school. My GCSE results were Average marks at mainly C’s. I also gained weight within a year of taking them and my periods were very erratic. I found it hard to focus and was very emotional. After stopping taking the medication at age 18 my weight dropped, my periods became regular and I performed in my A levels better than expected. I have regularly recreationally used cannabis flower from the age of 16, following the advice from my Father. From that point I have smoke the cannabis he has grown for me. In 1996, information about medicinal cannabis was almost impossible to obtain. To even think about mentioning it to the doctors was out of the question.
In 2009 I started a part-time PhD and helped to set up a new company in 2013. During the writing up stage of my PhD in 2016 gave up smoking cannabis. In the summer of 2016, 20 years tonic clonic seizure free, I had another Grand mal (Tonic Clonic seizure) banged my head and ended up in hospital. I remained in denial that it was a seizure, as I did not want to lose my driving licence. It was not until January 2017, that I was able to see a neurologist, after no tests since the age of 15, told me very rudely that I was epileptic, I had always been epileptic and to start taking Levetiracetam. At which point I began religiously self-medicating with cannabis flower, smoking it. After gaining two more neurologist opinions (One private the other NHS) and having ECG performed and MRI’s, which were clear I was allowed to drive again. The second NHS neurologist recommended further investigation with sleep deprivation studies. Still being in denial at this point and having not experienced any more seizure. I dismissed them.
In 2017 I decided to get fit and was going to run a half marathon on Halloween, for the charity JOEL. In the September prior to this I again gave up smoke cannabis. 2 days after the half marathon I had a Grand Mal (Tonic Clonic seizure) at work, which was witness by my work colleague.
I finally came out of denial. Once I did this, I began researching the disease more and I accepted that I had been having partial/auras seizures for years. Which increased when I had stopped smoking cannabis over the years. I have spoken to a number of doctors and had mixed reactions. This I have only done recently due to the change in scheduling. One very interested in what I had to say (my current neurologist), other very dismissive. All would not recommend it.
16The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Some of what could be described as mild side effects when smoking high THC strains include: Mild paranoia which makes me anti-social when using high THC strains, forgetfulness, unable to use a motor vehicle, dry mouth, increase appetite. In 2017 I discovered CBD oil, which I now use on a morning and will smoke cannabis flower with high THC on a night. CBD did not work alone, as the auras/partials started again when I stopped smoking cannabis with THC in.‘
Ed Granger
‘I have suffered with Grand Mal seizures for 20 years, for 17 of those years I have told every health professional I meet that natural, organic, full spectrum cannabis is the answer for me. I was ignored but I persisted and was forced to use inferior/unregulated/ potentially dangerous criminally sourced product. I am convinced had I not defied criticism and risked years of criminalization and self medicated I’d most likely have suffered a huge amount more brain damage than was “removed” from me in 2016. At the height of my epilepsy I was recorded as having up to 70 partial seizures a day. I now seizure daily, with grand mals reduced to once every few months. My seizure frequency is only fully controlled with full spectrum cannabis but the institution I have to trust to care for me have never listened to me, while alienating my truth. For years, at great cost and criminal risk to my family I have used cannabis to control these and stop them from formulating into life threatening Tonic clonic seizures, something the prescribed medicine has NEVER managed to achieve. Had I not been using cannabis for so many years I’m sure it could be proven that I’d likely have suffered huge amounts more irreversible neurological and physical damage.
I’m now in a position where I can see and feel the cycle of pharmaceutical tolerance coming again as it has done for some many years now and I refuse to put myself and my wife and children through the well travelled road of outdated care options available to me in this country. My “care” team refuse to help me safely come off the medications. The meds don’t agree with me, have never controlled my illness and constantly test my brains hardwired complexities while twisting my biological and neurological balance. Most frustrating, and farcical is I know a mixture/variety of organic cannabinoids work for me, I’ve been saying it for over a decade!! Sadly to do this and know I can be guaranteed my life saving medicine I would have to leave the U.K.’
17The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Eugenie Eley
‘I was first diagnosed with epilepsy at the age of 14 in 2006, after suffering a grand mal seizure on a fairground ride at school. As both my Mother and Aunt were also diagnosed with epilepsy at similar ages my first seizure wasn’t treated as a ‘random’ seizure. From then on I suffered grand mal seizures and auras every few weeks, mainly when I was tired or asleep. They lasted from 30 seconds to 2 minutes. I would lose all consciousness and even when conscious it would take a while for me to start remembering anything from who I am, where I was, how old I was, what day it was etc. I was diagnosed with myoclonic epilepsy, with no abnormalities shown on my brain scan or on any other tests. I now believe that I was experiencing auras and petite mal seizures from a much younger age, I just was not aware of what was happening.
I was not put on any medication when diagnosed. I was told that it was something I would grow out of and was mostly likely due to hormonal changes in my body and there was no need for drugs. I visited a Kinesiologist who prescribed me a concoction of natural supplements; I experienced no seizures whilst taking it. After I stopped taking it around 2007 I did experience some seizures, however they got less and less, around one every few months until eventually it was one or two a year. They were almost always when I had a lack of sleep, I had stayed up too late, I was woken up suddenly or I was hung-over.
In 2011 my Mother passed away, the trauma of this combined with the stress of starting University reignited my seizures and I was having at least one or two a week. I saw a new neurologist and was put on 1000mg Keppra twice a day. I have now been on Keppra for 7 years, taking the same dosage.
Although I have not been able to come off or reduce Keppra, CBD has helped me in so many ways. I appreciate I cannot determine the exact results as I am still taking both of them but I do know that CBD has given me a better quality of sleep, my brain doesn’t seem so fogged over. My anxious feelings are fewer and easily controlled. I have more confidence in the fact that I can take CBD with me everywhere in case I feel funny. I don’t even experience auras anymore. However, my immunity and blood count are still so poor. In an ideal world I would like to come off Keppra and only medicate with CBD. However, there is a lack of professional support in this process. Perhaps it is a lack of education but also a lack of willingness or belief. How can it be that I am taking a drug to treat my epilepsy with one of the main side affects being my main trigger? I understand my body more than anyone else and I can feel the damage being caused. I currently have no medical support in moving over from Keppra to CBD and I am too afraid to do it on my own. Living with epilepsy is tough enough; I would like the fittest, healthiest body whilst doing so.’

18The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
Clinician’s testimonies
Professor David Neubauer
Head of Department of Child, Adolescent and Developmental Neurology at University Children’s Hospital, Ljubljana.
‘We have been prescribing CBD for patients (children and adolescents) with resistant epilepsies since the beginning of 2015, and now we have a cohort of around 150 patients (in our paper, published in March last year there is a series of only 67 patients). We have some patients who are taking artisanal (home-made) cannabis for epilepsies, cerebral palsy, ADHD, Tourette and autism with quite good response, however the experiences with them are quite anecdotal.’
Zeid Mohamedali
‘I have limited experience in treating epilepsy. I have treated patients with seizure disorders with poor control on their anti-seizure medications. Here are some treatment pearls that I would include:
1. Start with low CBD dose of 2mg/kg BID and titrate up every 5days by 1mg/kg BID until I get to max of 10mg/kg BID
2. I leave them on the anti-seizure medications until they are stable and I work with the neurologists throughout the process to reduce the traditional medications
3. Be aware that higher doses of CBD can interfere with other medications (including sz medications)- monitor levels where needed
4. Be aware that many CBD extracts come from chemovars that are high in Myrcene and therefore at high dose of CBD will be sedating- if this side effects gets to be too much, then changing source of CBD can be helpful. Finding out which chemovar was used for the extraction and picking one with lower Myrcene (currently not possible since most LPs use a mix of chemovars to derive the CBD oil). I encourage families to add Limonene (citrus fruits like lemons, oranges, grapefruits, limes and pomelos) to the diet to help off-set sedation
5. Some patients with epilepsy have some behavioral issues – a low dose of THC (about 0.5 to 1mg) BID can help with the behavior, but also may aid in an entourage effect with the CBD. Keep in mind that higher doses of THC in some patients will have pro-sz activity

19The use of Cannabis-based medicinal products (CBMPs) in Epilepsy
6. THCA can be beneficial and not intoxicating- not much evidence yet
7. Patient can consider augmenting their treatment with Linalool from lavender, mint, cinnamon, and coriander as a terpene since there are animal models for this and it is harmless when added to the diet.’
Summary
There is good evidence for use of CBMPs in the treatment of epilepsy, especially with the pure CBD oral product Epidiolex (average dose about 20 mg/kg) which has positive results in seizure reduction in several randomised controlled trials including both children and adults of various types of epilepsy. The BPNA advise the use of this product as a treatment of last resort for children for whom other medications, diets or surgery are not appropriate. Pure CBD is generally well tolerated, although interactions with other anti-epileptic medications may lead to raised liver enzymes that should be monitored. There is some evidence that CBD enriched products or those containing small quantities of THC may be more beneficial than pure CBD (lower doses required with fewer side effects) although this remains to be conclusively
established. However, there are many ongoing clinical trials that will answer some of these questions. Patient testimonies suggest that CBMPs are more preferably to traditional anti-epileptics which often have severe side effects, and patients report being able to reduce the dose of anti-epileptics. In clinical trials CBMPs are added onto current care, and as yet, no studies have examined any potential superiority or non-inferiority of CBMP compared to traditional anti-epileptics.
Acknowledgements
We would like to acknowledge the peer review, advice and suggestions that we received in the assembly and production of this report from patients and clinicians, charities, and the core members of the CMC.