the uk's four national health services after devolution: divergence without structure...
TRANSCRIPT

THE UK'S FOUR NATIONAL HEALTH SERVICES AFTER DEVOLUTION: Divergence without structure
Presentation by Alan Trenchto European Union Centre of Excellence,
Dalhousie University, Halifax, 20 October 2014

The NHS before devolutionEstablished 1948, but never homogeneous • local/regional variations within England (and
Wales) • Responsibility of Welsh Office from 1964 • Separate legislation and structures in Scotland
and N Ireland from outset – Partly a recognition of different laws and
administrative arrangements • In N Ireland, in effect a gift; part of delivering a
GB welfare state that couldn’t be funded from NI’s tax base

The NHS, devolution and LabourA signal and totemic Labour achievement Labour the party most ‘trusted’ with the NHS Devolution similarly delivered by and through
Labour after embrace in 1990s (though supported by others earlier)
But no thought to how the NHS would work after devolution – it was simply to ‘be devolved’
No UK-led declaration about NHS goals or principles at all; no endorsement of these until 2009 (and then echoing a S/W/NI one of 2008)which lets the Con-Lib Dem Coalition off the hook ...

What devolution was and did Enacted 1998 Different arrangements for Scotland, Wales, Northern
Ireland But embodied ideas of self-rule for key functions, including
health, education, personal social services, local government, aspects of environment and transport
Particularly for Wales, a process more than an event: – Shift from executive to legislative devolution
Westminster retaining legal authority to legislate for all of UK – not used by (constitutional) convention– concurrent legislation – no exclusive legislative competences
And England left wholly out of the picture

Devolution and the four NHSs• Devolution not meant to create ‘policy laboratories’;
impact on policy incidental • If intention was to create a ‘bulwark against the Tories’,
it failed to do that too – not part of the design • Rather, a spinning-out and democratisation of the
existing forms of administrative devolution • Perhaps underpinned by an assumption that devolved
governments would do much the same, just closer to the public
• If ever there were a case of the law of unintended consequences ...
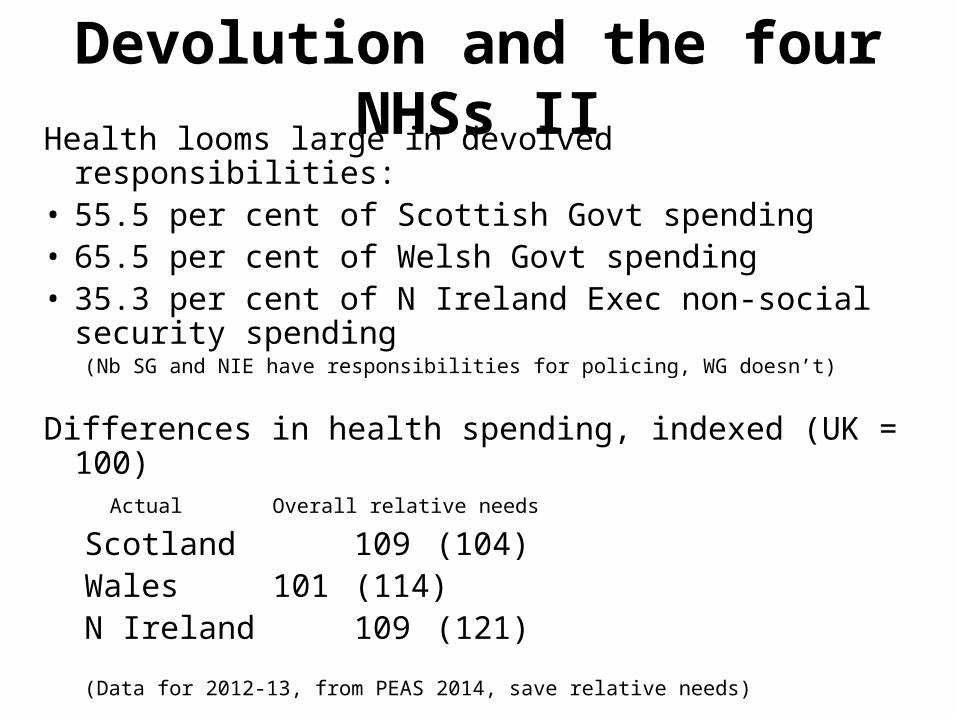
Devolution and the four NHSs IIHealth looms large in devolved responsibilities: • 55.5 per cent of Scottish Govt spending • 65.5 per cent of Welsh Govt spending • 35.3 per cent of N Ireland Exec non-social security
spending (Nb SG and NIE have responsibilities for policing, WG doesn’t)
Differences in health spending, indexed (UK = 100) Actual Overall relative needs
Scotland 109 (104) Wales 101 (114) N Ireland 109 (121)
(Data for 2012-13, from PEAS 2014, save relative needs)

Post-devolution policy: Scotland • Dominated by professionals and professionalism • Dismantled purchaser-provider split • Innovations: free prescriptions, free long term care for
the elderly – Seen as being at ‘English expense’
• Trials of elected local health boards • Strengths in bio-science research – Dolly the sheep • Endemic health problems, especially cancer and heart
disease, especially the West of Scotland

Post-devolution policy: Wales• Several structural policies: – Early 00s: the ‘local govt’ approach: co-terminosity of Local
Health Boards with local govt areas (-> 22 boards: too many, too small)
– 2009: consolidation into 7 boards, commissioning from NHS Trusts
• But no purchaser-provider split or internal competition • Policy innovations: free prescriptions, opt-out (deemed
consent) regime for organ donation – ‘Welsh organs for English patients’?
• Limited service innovations – walk in centres, NHS Direct, etc
Post-devolution policy: Wales II• Priority on public health at expense of hospitals and
GPs: -> lengthened waiting lists, acute (and ongoing) political embarrassment
• Welsh health care as stick for UK Conservatives to beat Labour with

Post-devolution policy: N Ireland• Policy really isn’t the point of politics in Northern Ireland
– and policy making is hard (cross-community consent) • No major changes to services or service delivery • Though free prescriptions introduced • Financial problems arising from immobility in the
Executive and inflexibility of budget/Programme for Govt – Emergent waiting list problems
• Moral causes: notably abortion

Post-devolution policy: England• Embrace of the purchaser-provider split and internal
market • Plus use of performance management and targets• When this goes wrong: Mid-Staffs • Use of NICE to approve drugs, technology on VFM
grounds • And since 2010 fragmentation with no local contracting
units, just aggregations of GPs buying services – from hospitals operating as commercial units, which may be in private or public sector
• Confusing public and private, and putting framework beyond control of any government or actor – Like the railways?
Financing the devolved NHS • Health care (and other devolved services) are funded
through the Barnett formula • A block grant, which can be freely allocated as the
devolved govt sees fit • Which varies according to changes in spending on
‘comparable functions’ in England • So if £100 million more is spent on health in England,
devolved govts get a population share of 99.1% of that • But the underlying baseline has never been reviewed (it’s
just a cumulation of earlier incremental decisions) • So the grant bears no relation to need (or any other
logical factor) • And devolved govts have little or no tax-setting powers/
responsibilities of their own

Financing the devolved NHS II • Moreover, the formula assumes devolved governments
(are happy to) have essentially the same model of public services as England– They can vire money within the grant, but changes in England
will force devolved govts either to do something similar or make cuts elsewhere
• The exception is Scotland – which is generously funded – The overfunding amounts to about 20% of the Scottish Govt’s
grant; nearly £1000 per person per year • The UK Coalition’s austerity programme protected
spending on health and schools (the two biggest areas of devolved responsibility) – So sheltered devolved budgets, and increasing divergence
from English levels – But forcing greater cuts elsewhere

Policy performance and the NHS • 2014 Nuffield Trust study details differences between
the ‘four NHSs’ • And concludes these make little difference to overall
levels or quality of treatment • Money makes the difference: explaining why health
services improved in 2000s, not since 2010 • Contrast to Nuffield’s earlier (2008) study – found
England performed better as ... It tried to measure performance
• New study notes the data problems in comparing what is going on – Is that a surprise? Why collect data that will help embarrass
you?

The UK-wide functions of the Dept of Health
• 0.9 per cent of health spending is ‘non-comparable’, i.e. UK wide
• Remaining DH functions – External aspects of contagious disease control – Supervision of the (main) medical professions and their
regulation – The organ donation and transplant system and the ‘organ
pool’ – Licensing and regulation of medicines (to extent not EMEA) –
funded by industry through licence fees • Committee on Safety of Medicines
– Medical costs for visitors from other EU and EEA countries
Intergovernmental relations? What intergovernmental relations?
• UK IGR depends on the ‘Joint Ministerial Committee’, which has various formats including an annual plenary meeting of Prime Minister and First Ministers
• Format on Health met in 2000-01, mostly ‘shared experiences’, then stopped
• In principle, health covered by JMC (Domestic) since 2008. No evidence health has in fact figured in those proceedings
• Otherwise, issues dealt with ad hoc, bilaterally, at variety of levels – with minimum of transparency

Anomalies of devolution • Different treatments available in different places – Mainly drugs – NICE guidance only binding in England, followed
in Wales too, only considered in Scotland • Different organ donation regimes in Scotland, Wales,
England-&-N-Ireland • The qualified right to free healthcare in another part of
the UK – Arising in relation to patients from N Ireland travelling to
England for abortions, but wider implications – So free treatment is limited to treatments available where you
reside? – A residence right, not a UK citizenship right

Anomalies of devolution II • Cross-border payments and the absence of routinised
payment mechanisms – Significant for Wales: c. 5000 more English patients registered
with Welsh GPs than vice versa, but c 6000 more Welsh patients receiving in- and out-patient treatments in England than vice versa
– Significant holes in budgets at individual hospital trust level

The NHSs into the future I A collection of major policy problems • Demographic problems: ageing population– Particularly severe in Scotland – The relationship between health and social care for the elderly:
joining up provision? Funding? • Funding, given that – and political commitments to
protect (English) NHS funding in real terms, which assumes cost growth can be met by ‘efficiency savings’ – With increasing use of private providers in England, at expense
of staff pay and conditions? – Elsewhere, if not by same, from other policy areas?
• Fragmentation of professions, emergence of differential pay and conditions

The NHSs into the future II • The NHS retains its totemic significance, which also
makes it highly contentious politically: – witness the Scottish referendum and importance of ‘vote for
independence to stop the Scottish NHS being privatised’ – And political use of Welsh poor performance by Westminster
Conservatives • But policy fragmentation is advanced. Hard to see how it
can be halted. • Framework legislation?
a) to consolidate NHS providing universal care free at the point of use, and b) reciprocal citizenship rights to access it?
• How to accommodate different policy preferences? Fiscal devolution? – Is point of devolution to reconcile autonomy and solidarity, or
simply allow difference and divergence?

Read more on the Devolution Matters blog:
http://devolutionmatters.wordpress.com/