the treatment of mg: state of the art may 2010 gil i. wolfe, m.d. univ. of texas southwestern...
TRANSCRIPT
The Treatment of MG: The Treatment of MG: State of the ArtState of the Art
May 2010May 2010
Gil I. Wolfe, M.D.Gil I. Wolfe, M.D.Univ. of Texas Southwestern Univ. of Texas Southwestern
Medical CenterMedical Center
Dallas, TXDallas, TX

Therapy goals in MGTherapy goals in MG
Return patients to normal functionReturn patients to normal function Achieve remissionAchieve remission Minimize side effectsMinimize side effects
Individualize therapyIndividualize therapy Disease severity and distributionDisease severity and distribution Rate of progressionRate of progression Lifestyle and career choicesLifestyle and career choices Coexisting diseaseCoexisting disease Patient age and sexPatient age and sex Cost considerationsCost considerations
Symptomatic Rx: Anticholinesterase Symptomatic Rx: Anticholinesterase agentsagents
PyridostigminePyridostigmine Initiate at 30-60 mg 3-4 Initiate at 30-60 mg 3-4
times a day initiallytimes a day initially Clinical response in 15-30 Clinical response in 15-30
min lasting 3-4 hrsmin lasting 3-4 hrs tt1/2 1/2 200 min (60 mg)200 min (60 mg) Peak plasma levels in 1-2 Peak plasma levels in 1-2
hrshrs Monitoring levels not usefulMonitoring levels not useful
Individualize dosingIndividualize dosing Dosing >120 mg every 3 hrs Dosing >120 mg every 3 hrs
unlikely to be helpfulunlikely to be helpful

Anticholinesterase agentsAnticholinesterase agents
Countering muscarinic side effectsCountering muscarinic side effects Glycopyrrolate 1 mgGlycopyrrolate 1 mg Hyoscyamine sulfate 0.125 mgHyoscyamine sulfate 0.125 mg Atropine 0.4 mgAtropine 0.4 mg Loperamide 2-4 mg (OTC)Loperamide 2-4 mg (OTC)
Can be given prn or on fixed schedule in Can be given prn or on fixed schedule in concert with pyridostigmine dosesconcert with pyridostigmine doses

ACE in MuSK Ab+ MGACE in MuSK Ab+ MG
Anticholinesterase Anticholinesterase responsesresponses
Non-responsivenessNon-responsiveness Hypersensitivity-sx Hypersensitivity-sx
worsenworsen Intolerance-severe Intolerance-severe
cholinergic AEscholinergic AEs No improvementNo improvement
MuSKMuSK
Ab +Ab +
SeronegSeroneg AchRAchR
Ab +Ab +
ACE non-ACE non-responseresponse
10/1410/14
71%71%
4/224/22
18%18%
13/7313/73
18%18%
ACEACE
hypersenshypersens3/143/14 1/221/22 0/730/73
ACE ACE intoleranceintolerance
4/144/14 2/222/22 13/7313/73
No improve-No improve-
mentment4/144/14 1/221/22 0/730/73
Tensilon Tensilon test +test +
5/105/10 16/1916/19 32/3332/33
PyridostigPyridostig
responseresponse3/143/14 21/2221/22 71/7371/73
Hatanaka et al. Neurology2005;65:1508
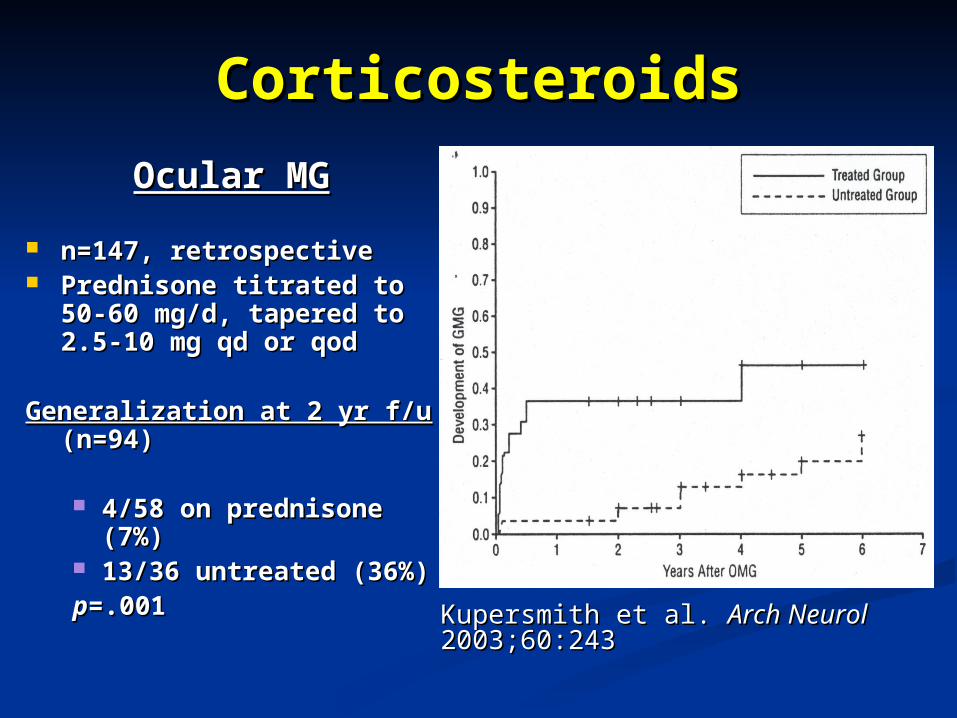
CorticosteroidsCorticosteroids
Ocular MGOcular MG
n=147, retrospectiven=147, retrospective Prednisone titrated to 50-60 Prednisone titrated to 50-60
mg/d, tapered to 2.5-10 mg mg/d, tapered to 2.5-10 mg qd or qodqd or qod
Generalization at 2 yr f/uGeneralization at 2 yr f/u (n=94) (n=94)
4/58 on prednisone (7%)4/58 on prednisone (7%) 13/36 untreated (36%)13/36 untreated (36%)pp=.001=.001
Kupersmith et al. Kupersmith et al. Arch NeurolArch Neurol 2003;60:243 2003;60:243
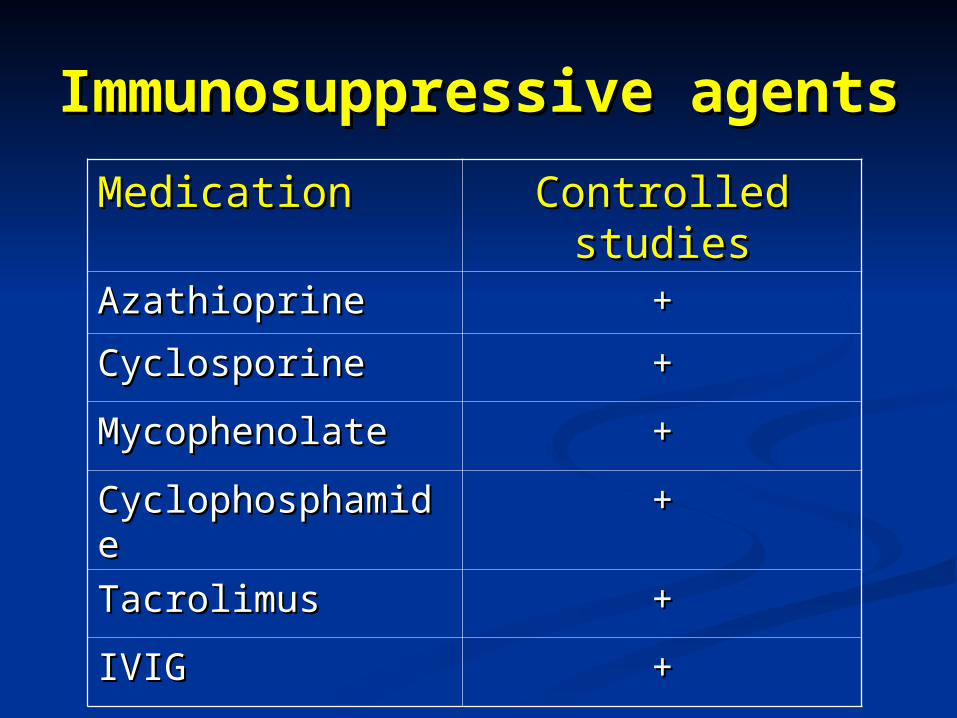
Immunosuppressive agentsImmunosuppressive agents
MedicationMedication Controlled studiesControlled studies
AzathioprineAzathioprine ++
CyclosporineCyclosporine ++
MycophenolateMycophenolate ++
CyclophosphamideCyclophosphamide ++
TacrolimusTacrolimus ++
IVIGIVIG ++

AzathioprineAzathioprine Randomized, double-blind trial (n=34)Randomized, double-blind trial (n=34)
Palace et al. Palace et al. NeurologyNeurology 1998;50:1778 1998;50:1778
Azathioprine 2.5 mg/kg qd vs. placeboAzathioprine 2.5 mg/kg qd vs. placebo All patients received prednisoloneAll patients received prednisolone
1.5 mg/kg qod with 100 mg qod ceiling1.5 mg/kg qod with 100 mg qod ceiling At 2 & 3 yrs, prednisolone dose reduced in At 2 & 3 yrs, prednisolone dose reduced in
AZA group (AZA group (pp=0.02)=0.02) >80% reduction at 2 yrs>80% reduction at 2 yrs
Disease relapse rate lower in AZA group Disease relapse rate lower in AZA group ((pp=0.024)=0.024)
Side effects lower in AZA groupSide effects lower in AZA group

AzathioprineAzathioprinePalace et al.Palace et al.
placebo
AZA
p =0.02 at 24 mo
placebo
AZA

AzathioprineAzathioprine
Steroid-sparing effects Steroid-sparing effects (Palace et al.)(Palace et al.)
Lower median weight gain at 2,3 yrsLower median weight gain at 2,3 yrs Less dyspepsia, back pain at 1,2,3 yrsLess dyspepsia, back pain at 1,2,3 yrs 30% reduction in steroid dose by 15 mos30% reduction in steroid dose by 15 mos Temporal arteritis studies show 30% Temporal arteritis studies show 30%
reduction substantially reduces adverse reduction substantially reduces adverse eventsevents
Nesher et al. Nesher et al. Clin Exp RheumatolClin Exp Rheumatol 1997;15:303 1997;15:303 Rubinow et al. Rubinow et al. Ann OphthalmolAnn Ophthalmol 1984;16:258 1984;16:258

Mycophenolate mofetilMycophenolate mofetil
Blocks IMP dehydrogenase/purine synthesisBlocks IMP dehydrogenase/purine synthesis Selective inhibition of B & T lymphocytesSelective inhibition of B & T lymphocytes
Widely used in transplant medicineWidely used in transplant medicine Utility in MGUtility in MG
First-line agentFirst-line agent Steroid-sparing agentSteroid-sparing agent
Dosing Dosing 500 mg bid initially, increasing to 1000-1500 mg 500 mg bid initially, increasing to 1000-1500 mg
bid by 500-1000 mg increments every 2-4 wksbid by 500-1000 mg increments every 2-4 wks Can use tid regimen if diarrhea occursCan use tid regimen if diarrhea occurs

Mycophenolate mofetilMycophenolate mofetil Adverse eventsAdverse events
No major organ toxicityNo major organ toxicity Diarrhea, nausea, abdominal painDiarrhea, nausea, abdominal pain Infections Infections (PML)(PML) Peripheral edemaPeripheral edema Drug-induced feverDrug-induced fever Leukopenia Leukopenia
CBC q wk x 4, q2 wks x 4, then monthlyCBC q wk x 4, q2 wks x 4, then monthly Neoplasia (lymphoma)Neoplasia (lymphoma)
Primary CNS lymphoma after 3 yrs of treatmentPrimary CNS lymphoma after 3 yrs of treatmentVernino et al. Vernino et al. NeurologyNeurology 2005;65:639 2005;65:639
Lymphocytopenia (260/Lymphocytopenia (260/µL); CD4 158µL); CD4 158 Near complete resolution with d/c of MM, steroids, Near complete resolution with d/c of MM, steroids,
rituximabrituximab

Mycophenolate mofetilMycophenolate mofetil
Retrospective analysis of 85 MG ptsRetrospective analysis of 85 MG pts 14 pts considered “refractory”14 pts considered “refractory”
Meriggioli et al. Meriggioli et al. Neurology Neurology 2003;61:14382003;61:1438
OutcomesOutcomes 73% remission/minimal manifestation/improved73% remission/minimal manifestation/improved MMT/QMG scores improved significantlyMMT/QMG scores improved significantly 5/13 Class IV pts (38%) did not improve5/13 Class IV pts (38%) did not improve
Steroid doseSteroid dose Reduced by Reduced by >> 50% in 23 pts 50% in 23 pts Reduced by < 50% in 13 ptsReduced by < 50% in 13 pts Unchanged in 14 ptsUnchanged in 14 pts Increased in 1 ptIncreased in 1 pt

Mycophenolate mofetilMycophenolate mofetil
Retrospective analysis of 85 MG ptsRetrospective analysis of 85 MG pts Onset of action relatively rapidOnset of action relatively rapid
Improvement observed at 9-11 wksImprovement observed at 9-11 wks May take up to 40 wksMay take up to 40 wks
Maximal improvement at mean of 27 wksMaximal improvement at mean of 27 wks TolerabilityTolerability
5/85 pts discontinued5/85 pts discontinued GI intolerance (diarrhea)GI intolerance (diarrhea) No significant leukopeniaNo significant leukopenia
Meriggioli et al. Meriggioli et al. Neurology Neurology 2003;61:14382003;61:1438
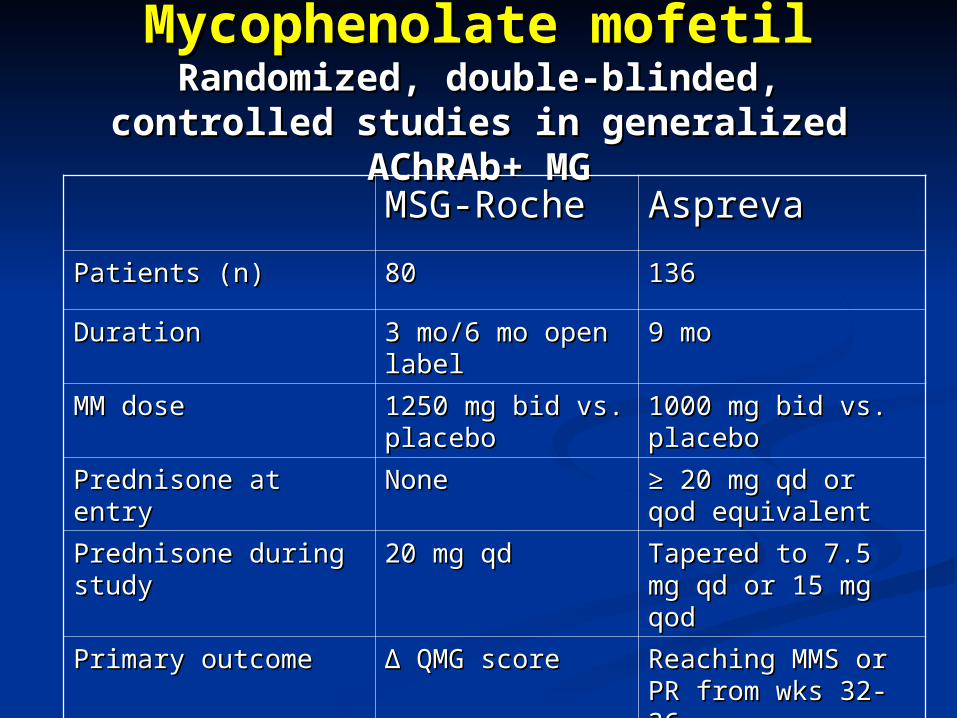
Mycophenolate mofetilMycophenolate mofetilRandomized, double-blinded, controlled Randomized, double-blinded, controlled
studies in generalized AChRAb+ MGstudies in generalized AChRAb+ MG
MSG-RocheMSG-Roche AsprevaAspreva
Patients (n)Patients (n) 8080 136136
DurationDuration 3 mo/6 mo open 3 mo/6 mo open labellabel
9 mo9 mo
MM doseMM dose 1250 mg bid vs. 1250 mg bid vs. placeboplacebo
1000 mg bid vs. 1000 mg bid vs. placeboplacebo
Prednisone at entryPrednisone at entry NoneNone ≥ ≥ 20 mg qd or qod 20 mg qd or qod equivalentequivalent
Prednisone during studyPrednisone during study 20 mg qd20 mg qd Tapered to 7.5 mg qd Tapered to 7.5 mg qd or 15 mg qodor 15 mg qod
Primary outcomePrimary outcome ΔΔ QMG score QMG score Reaching MMS or PR Reaching MMS or PR from wks 32-36 from wks 32-36

Mycophenolate mofetilMycophenolate mofetil MSG-Roche studyMSG-Roche study
n=39 on pred/placebo; 41 on pred/MMn=39 on pred/placebo; 41 on pred/MM No significant difference in No significant difference in ΔΔQMG at 3 moQMG at 3 mo
-4.4 on MM vs. -3.6 on placebo (p=0.71)-4.4 on MM vs. -3.6 on placebo (p=0.71) No significant difference in 2° outcomesNo significant difference in 2° outcomes
MG-ADL, MMT, SF-36, AChRAb levelsMG-ADL, MMT, SF-36, AChRAb levels MM was well toleratedMM was well tolerated
Diarrhea in 16%, infection in 13% in blinded phase on Diarrhea in 16%, infection in 13% in blinded phase on MMMM
Muscle Study Group. Muscle Study Group. NeurologyNeurology 2008;71:394 2008;71:394

Mycophenolate mofetilMycophenolate mofetil Aspreva studyAspreva study
n=88 on pred/placebo; 88 on pred/MMn=88 on pred/placebo; 88 on pred/MM n=144 completed studyn=144 completed study
No significant different in reaching treatment response of No significant different in reaching treatment response of MMS/PRMMS/PR 44.3% on MM vs. 38.6% on placebo (p=0.541)44.3% on MM vs. 38.6% on placebo (p=0.541)
No significant difference in 2° outcomesNo significant difference in 2° outcomes QMG, MG-ADL, SF-36, global assessmentsQMG, MG-ADL, SF-36, global assessments Trend for greater prednisone dose reduction, decline in AChRAb, Trend for greater prednisone dose reduction, decline in AChRAb,
hospitalizations if on MM, but not significanthospitalizations if on MM, but not significant MM overall well toleratedMM overall well tolerated
Headache (12%), nausea (9%) most common side effectsHeadache (12%), nausea (9%) most common side effects One death related to study drug (pneumonia in MM group)One death related to study drug (pneumonia in MM group)
Sanders et al. Sanders et al. NeurologyNeurology 2008;71:400 2008;71:400

What did we learn about MMF What did we learn about MMF from these two studies?from these two studies?
MM is not better than prednisone alone as initial MM is not better than prednisone alone as initial treatment in mild-moderate MG, and has no treatment in mild-moderate MG, and has no steroid-sparing effect within the timeframe of steroid-sparing effect within the timeframe of these studies (up to 36 wks)these studies (up to 36 wks)
It may take longer than predicted to show benefit It may take longer than predicted to show benefit from MMfrom MM
Prednisone is more effective than predicted, and Prednisone is more effective than predicted, and at a lower dose than expectedat a lower dose than expected
Exacerbations after prednisone may also occur Exacerbations after prednisone may also occur at lower doses than expectedat lower doses than expected

Tacrolimus (FK506)Tacrolimus (FK506)
Same pharmacologic class as cyclosporineSame pharmacologic class as cyclosporine Less nephrotoxicLess nephrotoxic Utility in MGUtility in MG
Monotherapy (not “first-line”)Monotherapy (not “first-line”) Steroid-sparing agentSteroid-sparing agent
Effects seen after 1-2 monthsEffects seen after 1-2 months DosingDosing
3-5 mg/d3-5 mg/d

TacrolimusTacrolimus
16 wk open trial in 16 wk open trial in thymectomized generalized thymectomized generalized MG (n=19)MG (n=19)
Konishi et al. Konishi et al. Muscle Muscle NerveNerve 2003;28:570 2003;28:570
QMG improved in 13/19QMG improved in 13/19 Fell at least 3 pts in 7/19 Fell at least 3 pts in 7/19
(used 27 pt version)(used 27 pt version) Therapy continued for 2 Therapy continued for 2
yrs in 12/19yrs in 12/19 Efficacy maintainedEfficacy maintained
Adverse eventsAdverse events No change in serum CrNo change in serum Cr Increased HbA1c in one ptIncreased HbA1c in one pt
TacrolimusTacrolimus n=212 in open studyn=212 in open study
Ponseti et al. Ponseti et al. Ann NY Acad SciAnn NY Acad Sci 2008;1132:254 2008;1132:254
Dose: 0.1 mg/kg/d adjusted to 7-8 ng/mlDose: 0.1 mg/kg/d adjusted to 7-8 ng/ml Assessments x4 in first month, then at Assessments x4 in first month, then at
least every 3 monthsleast every 3 months Mean f/u 49.3 moMean f/u 49.3 mo OutcomesOutcomes
Muscle strengthMuscle strength QMGQMG MGFA post-intervention statusMGFA post-intervention status
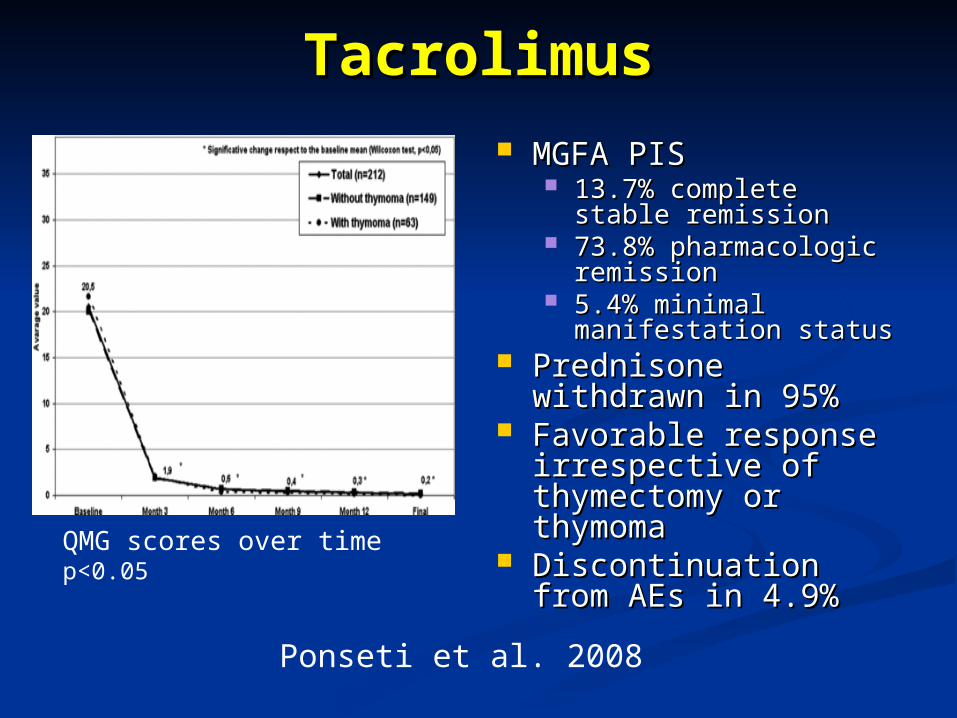
TacrolimusTacrolimus
MGFA PISMGFA PIS 13.7% complete stable 13.7% complete stable
remissionremission 73.8% pharmacologic 73.8% pharmacologic
remissionremission 5.4% minimal manifestation 5.4% minimal manifestation
statusstatus Prednisone withdrawn in Prednisone withdrawn in
95%95% Favorable response Favorable response
irrespective of irrespective of thymectomy or thymomathymectomy or thymoma
Discontinuation from AEs Discontinuation from AEs in 4.9%in 4.9%
QMG scores over timep<0.05
Ponseti et al. 2008
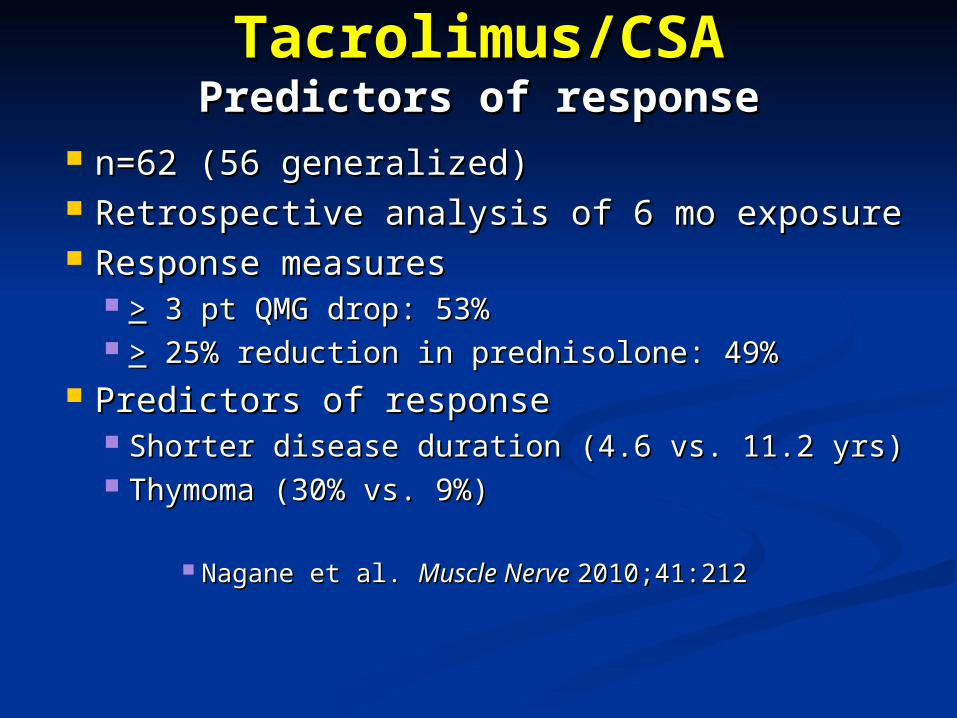
Tacrolimus/CSATacrolimus/CSAPredictors of responsePredictors of response
n=62 (56 generalized)n=62 (56 generalized) Retrospective analysis of 6 mo exposureRetrospective analysis of 6 mo exposure Response measuresResponse measures
>> 3 pt QMG drop: 53% 3 pt QMG drop: 53% >> 25% reduction in prednisolone: 49% 25% reduction in prednisolone: 49%
Predictors of responsePredictors of response Shorter disease duration (4.6 vs. 11.2 yrs)Shorter disease duration (4.6 vs. 11.2 yrs) Thymoma (30% vs. 9%)Thymoma (30% vs. 9%)
Nagane et al. Nagane et al. Muscle Nerve Muscle Nerve 2010;41:2122010;41:212
TacrolimusTacrolimus Adverse eventsAdverse events
HyperglycemiaHyperglycemia HypertensionHypertension HeadacheHeadache HyperkalemiaHyperkalemia NephrotoxicityNephrotoxicity Nausea/vomiting/diarrheaNausea/vomiting/diarrhea InfectionInfection LymphomaLymphoma
Drug interactions similar to CSADrug interactions similar to CSA MonitoringMonitoring
BUN/Cr, glu, KBUN/Cr, glu, K++, trough drug levels (<10 ng/ml) , trough drug levels (<10 ng/ml) Every 2-4 weeks initially, then less frequentlyEvery 2-4 weeks initially, then less frequently
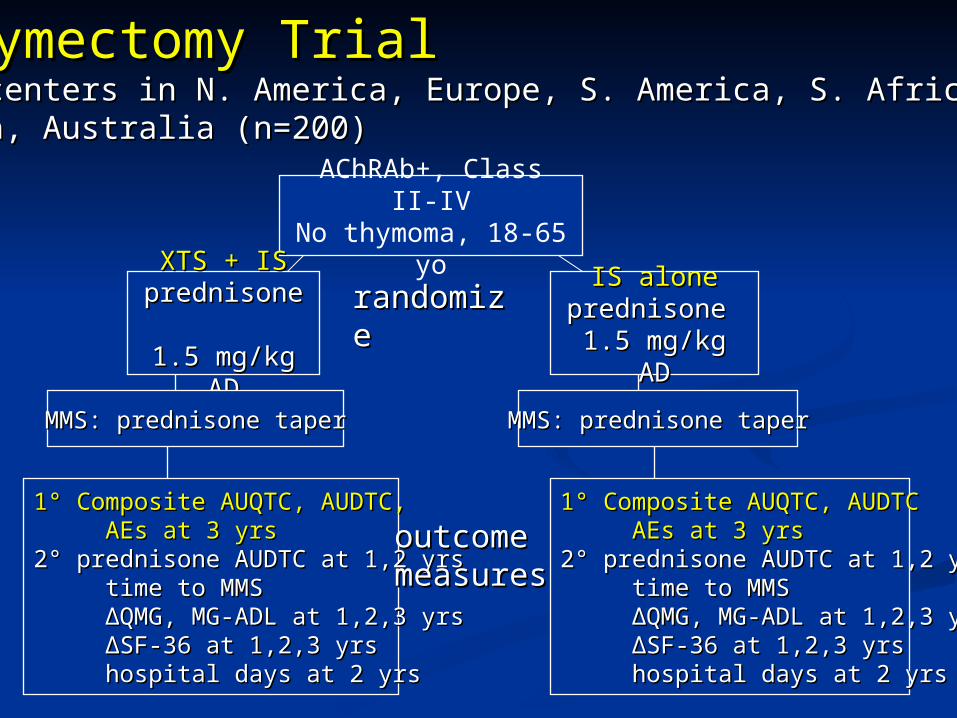
AChRAb+, Class II-IVNo thymoma, 18-65 yo
XTS + ISXTS + ISprednisone prednisone
1.5 mg/kg AD1.5 mg/kg AD
IS aloneIS aloneprednisone prednisone
1.5 mg/kg AD1.5 mg/kg AD
MMS: prednisone taperMMS: prednisone taper MMS: prednisone taperMMS: prednisone taper
1° Composite AUQTC, AUDTC,1° Composite AUQTC, AUDTC, AEs at 3 yrsAEs at 3 yrs2° prednisone AUDTC at 1,2 yrs2° prednisone AUDTC at 1,2 yrs time to MMStime to MMS ∆ ∆QMG, MG-ADL at 1,2,3 yrsQMG, MG-ADL at 1,2,3 yrs ∆ ∆SF-36 at 1,2,3 yrsSF-36 at 1,2,3 yrs hospital days at 2 yrshospital days at 2 yrs
1° Composite AUQTC, AUDTC1° Composite AUQTC, AUDTC AEs at 3 yrsAEs at 3 yrs2° prednisone AUDTC at 1,2 yrs2° prednisone AUDTC at 1,2 yrs time to MMStime to MMS ∆ ∆QMG, MG-ADL at 1,2,3 yrsQMG, MG-ADL at 1,2,3 yrs ∆ ∆SF-36 at 1,2,3 yrsSF-36 at 1,2,3 yrs hospital days at 2 yrshospital days at 2 yrs
randomizerandomize
outcomeoutcomemeasuresmeasures
Thymectomy TrialThymectomy Trial79 centers in N. America, Europe, S. America, S. Africa, 79 centers in N. America, Europe, S. America, S. Africa, Asia, Australia (n=200)Asia, Australia (n=200)
New/future approachesNew/future approaches RituximabRituximab TerbutalineTerbutaline Monarsen/EN101Monarsen/EN101 Etanercept Etanercept Rowin et al. Rowin et al. NeurologyNeurology 2004;63:2390 2004;63:2390
TNFTNFαα receptor blocker receptor blocker 6/11 patients improved in pilot study (8 completed 6-6/11 patients improved in pilot study (8 completed 6-
month trial)month trial) 2/11 worsened, one requiring urgent PE2/11 worsened, one requiring urgent PE
Upregulation of TNFUpregulation of TNFαα levels levels Eculizimab Eculizimab
Monoclonal Ab, blocks C5 activationMonoclonal Ab, blocks C5 activation Phase II randomized DBPC crossover trialPhase II randomized DBPC crossover trial
MethotrexateMethotrexate Phase II DBPC trial Phase II DBPC trial
RituximabRituximab Monoclonal Ab to CD20Monoclonal Ab to CD20 Improvement within several weeks in case Improvement within several weeks in case
reportsreports Zaja et al. 2000; Wylam et al. 2003; Gajra et al. 2004Zaja et al. 2000; Wylam et al. 2003; Gajra et al. 2004
Benefit in ongoing studies/pilot trials in Benefit in ongoing studies/pilot trials in AChR/MuSK+ MGAChR/MuSK+ MG n=19 totaln=19 total Initial dosing 375 mg/mInitial dosing 375 mg/m2 2 q1-2 wks for 4 wks q1-2 wks for 4 wks Maintenance: none or 375 mg/mMaintenance: none or 375 mg/m2 2 q4-10 wksq4-10 wks Onset in 4-12 wksOnset in 4-12 wks
Rojas-Garcia et al., Tandan et al., Gardner et al., Rojas-Garcia et al., Tandan et al., Gardner et al., Frenay et al. (2008 AAN abstracts)Frenay et al. (2008 AAN abstracts)

RituximabRituximab Refractory MG Refractory MG (n=6 females, AChR or MuSK-Ab)(n=6 females, AChR or MuSK-Ab)
Unable to lower immunosuppressionUnable to lower immunosuppression Uncontrolled on immunosuppressionUncontrolled on immunosuppression Intolerable side effectsIntolerable side effects
1-4 cycles (q1-4 cycles (q 4-12 mos)4-12 mos) 375 mg/m375 mg/m2 2 weekly infusionsweekly infusions
ResultsResults 4/6 pts asymptomatic4/6 pts asymptomatic 1 pt with diplopia1 pt with diplopia 1 pt with dysarthria1 pt with dysarthria No significant side effectsNo significant side effects
Zebardast et al. Zebardast et al. Muscle Nerve Muscle Nerve 2010;41:3752010;41:375
RituximabRituximab AEsAEs
Skin: pruritis to pemphigus/Stevens-JohnsonSkin: pruritis to pemphigus/Stevens-Johnson Nausea, vomitingNausea, vomiting HeadacheHeadache Anemia, leukopenia, thromocytopeniaAnemia, leukopenia, thromocytopenia Chest painChest pain >25 PML cases in SLE/hematological >25 PML cases in SLE/hematological
malignancy patientsmalignancy patients Premedicate with acetaminophen, Premedicate with acetaminophen,
diphenhydraminediphenhydramine

Monarsen/EN101Monarsen/EN101
Antisense oligonucleotide to AchE Antisense oligonucleotide to AchE mRNAmRNA
Oral agentOral agent Prevents translationPrevents translation
mRNA susceptible to degradationmRNA susceptible to degradation Clinical effectiveness up to 72 hoursClinical effectiveness up to 72 hours
Sussman. Sussman. Drug Disc TodayDrug Disc Today 2003;8:516 2003;8:516

MonarsenMonarsenArgov et al. Argov et al. NeurologyNeurology 2007;69:699 2007;69:699
Open-label study Open-label study (n=16, 1 protocol violation)(n=16, 1 protocol violation) 500 500 µµg/kg/d x 3dg/kg/d x 3d AEs monitored for 1 monthAEs monitored for 1 month
ResultsResults 13/15 with improved QMG on day 413/15 with improved QMG on day 4 Mean Mean ΔΔQMG -6.13 pts (baseline 14.9)QMG -6.13 pts (baseline 14.9) Effects last 24-48 hrs after doseEffects last 24-48 hrs after dose 4 pts on Monarsen for 4 weeks maintained improvement 4 pts on Monarsen for 4 weeks maintained improvement
2 resumed pyridostigmine2 resumed pyridostigmine
AEsAEs 56% with transient dry mouth/eyes56% with transient dry mouth/eyes
Treatment of MGTreatment of MGSpecial scenariosSpecial scenarios
MG crisisMG crisis Hold anticholinesterases Hold anticholinesterases Plasma exchange (50cc/kg x 4-Plasma exchange (50cc/kg x 4-
6 exchanges)6 exchanges) IVIGIVIG
PregnancyPregnancy Pyridostigmine, steroids, PE, Pyridostigmine, steroids, PE,
IVIGIVIG
Ocular MGOcular MG Ptosis: crutches, tape, Ptosis: crutches, tape,
blepharoplastyblepharoplasty Diplopia: alternate patching, Diplopia: alternate patching,
prisms, surgeryprisms, surgery

Treatment of ocular symptomsTreatment of ocular symptomsRetrospective analysisRetrospective analysis
Corticosteroids vs. AChE inhibitorsCorticosteroids vs. AChE inhibitors n=35n=35 Rx: 14 epochs with AChE inhibitors, 27 epochs with Rx: 14 epochs with AChE inhibitors, 27 epochs with
corticosteroids (median prednisone dose 20 mg qd)corticosteroids (median prednisone dose 20 mg qd) Outcome: ocular items from QMGOutcome: ocular items from QMG ResultsResults
Ocular QMG improvement favored corticosteroids (3.6 Ocular QMG improvement favored corticosteroids (3.6 vs. 1.1 pt change; vs. 1.1 pt change; pp=0.0021)=0.0021)
Symptom resolution in 70% of steroid epochs vs. 29% Symptom resolution in 70% of steroid epochs vs. 29% AChE inhibitors epochsAChE inhibitors epochs
AEsAEs IGT in 67%IGT in 67% Reduced bone density in 20%Reduced bone density in 20%
Bhanushali, Wuu & Benatar. Bhanushali, Wuu & Benatar. NeurologyNeurology 2008;71:1335 2008;71:1335

MuSK Ab+ MG Treatment ResponseMuSK Ab+ MG Treatment Response Pasnoor et al. Pasnoor et al. Muscle & Nerve Muscle & Nerve 2010;41:3702010;41:370
52/53 pts required 52/53 pts required ≥2 ≥2 forms of therapyforms of therapy
5 Rx categories5 Rx categories PyridostigminePyridostigmine PrednisonePrednisone IS agentsIS agents PEPE IVIGIVIG
ImprovementImprovement MGFA Class 0MGFA Class 0 CSR/PR/MMSCSR/PR/MMS MGFA classification: ≥2 MGFA classification: ≥2
class improvementclass improvement
Rx Rx categoriescategories
% of pts% of pts
(n=53)(n=53)
55 3636
44 2323
33 2121
22 1919
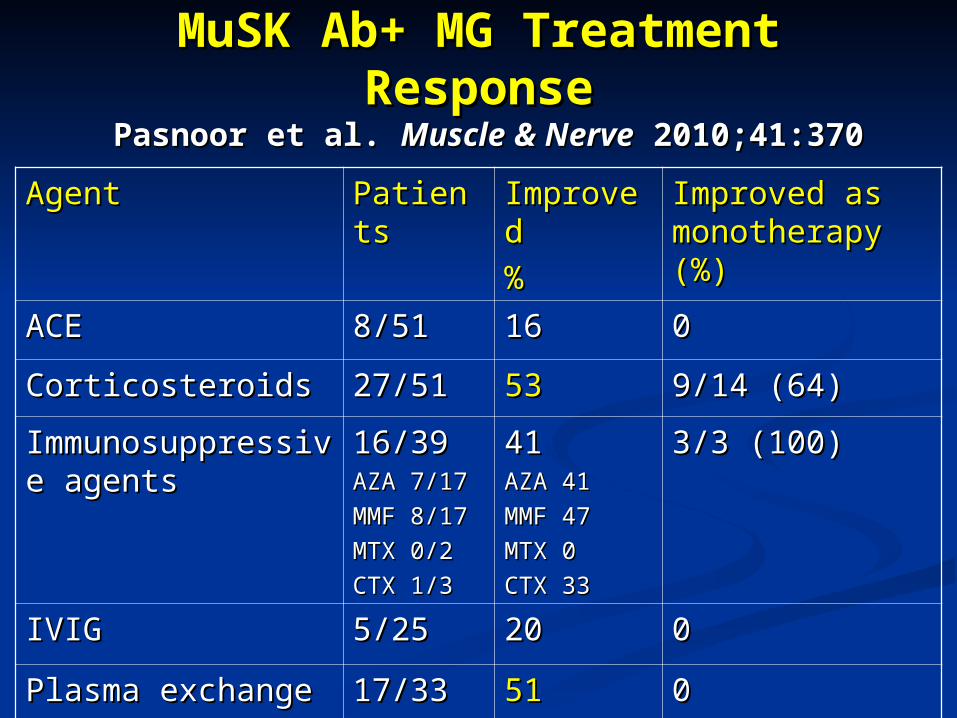
MuSK Ab+ MG Treatment ResponseMuSK Ab+ MG Treatment Response Pasnoor et al. Pasnoor et al. Muscle & NerveMuscle & Nerve 2010;41:370 2010;41:370
AgentAgent PatientsPatients ImprovedImproved
%%
Improved as Improved as monotherapy (%)monotherapy (%)
ACEACE 8/518/51 1616 00
CorticosteroidsCorticosteroids 27/5127/51 5353 9/14 (64)9/14 (64)
Immunosuppressive Immunosuppressive agentsagents
16/3916/39AZA 7/17 AZA 7/17
MMF 8/17MMF 8/17
MTX 0/2MTX 0/2
CTX 1/3CTX 1/3
4141AZA 41AZA 41
MMF 47MMF 47
MTX 0MTX 0
CTX 33CTX 33
3/3 (100)3/3 (100)
IVIG IVIG 5/255/25 2020 00
Plasma exchangePlasma exchange 17/3317/33 5151 00
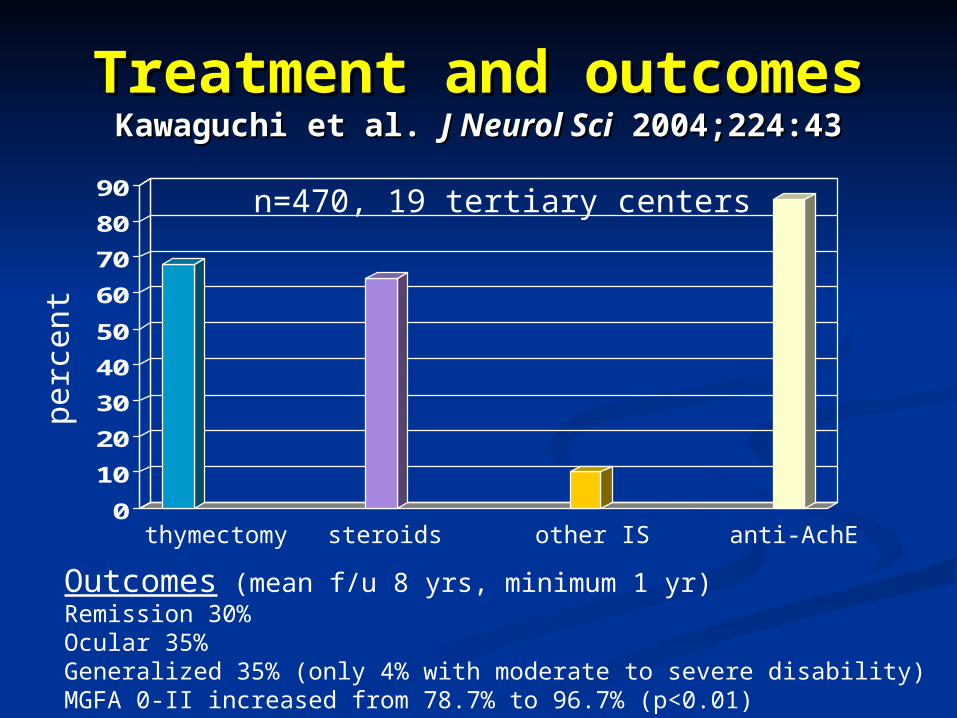
Treatment and outcomesTreatment and outcomesKawaguchi et al. Kawaguchi et al. J Neurol SciJ Neurol Sci 2004;224:43 2004;224:43
0
10
20
30
40
50
60
70
80
90n=470, 19 tertiary centers
thymectomy steroids other IS anti-AchE
Outcomes (mean f/u 8 yrs, minimum 1 yr)Remission 30%Ocular 35%Generalized 35% (only 4% with moderate to severe disability)MGFA 0-II increased from 78.7% to 96.7% (p<0.01)
perc
ent

MG vignetteMG vignette 69 yo former rodeo professional from Brooklyn, 69 yo former rodeo professional from Brooklyn,
NY with MGNY with MG Refractory bulbar symptomsRefractory bulbar symptoms
DysarthriaDysarthria DysphagiaDysphagia
Prior treatmentsPrior treatments Mestinon 60 mg tid to qidMestinon 60 mg tid to qid Prednisone diabetes, weight gainPrednisone diabetes, weight gain
Unable to taper below 40 mg qodUnable to taper below 40 mg qod Transsternal thymectomy (no thymoma)Transsternal thymectomy (no thymoma) Failed IVIGFailed IVIG No response to azathioprine ( LFTs), mycophenolateNo response to azathioprine ( LFTs), mycophenolate Requiring plasma exchange q 1-2 wks for disease controlRequiring plasma exchange q 1-2 wks for disease control
Lives on ranch 100 miles from UT SouthwesternLives on ranch 100 miles from UT Southwestern

Initiate and adjust pyridostigminefor maximal control
Options include:-Initiate pred alone or with steroid-sparing agent-Initiate MM or AZA as monotherapy, keeping in mind AZA's slow onset -Consider thymectomy
Continue pyridostigmine;Consider thymectomy
In remission
Not improved
-Initiate slow pred AD taper with objective of smallest dose that maintains improved status-Steroid-sparing agents can be tapered slowly over time as tolerated
Options include:-Initiate cyclosporine-Initiate IVIG or PE-Plan on thymectomy when stable
-Stop taper, initiate incremental increases in agent that has been lowered-High-dose steroids may need to be reinitiated
In case of relapse Improved
Not improved
Improved/ in remission
Not improved
Options include:-Long-term PE or IVIG-Cyclophosphamide-Tacrolimus-Rituximab
Treatment algorithm in generalized MGTreatment algorithm in generalized MG
Not in remission
Improved/ in remission

Lifetime Course of MGLifetime Course of MGGrob et al. Grob et al. Muscle NerveMuscle Nerve 2008;37:141 2008;37:141
David Grob, MD, 1919-2008David Grob, MD, 1919-2008
Transternal thymectomy Transternal thymectomy effect on remissioneffect on remission 1940-571940-57
Significant effect (20% Significant effect (20% vs. 10%)vs. 10%)
1958-19651958-1965 Similar remission and Similar remission and
improvement rates improvement rates 1966-20001966-2000
Slightly higher mortality Slightly higher mortality and lower remission and lower remission rates in thymectomy rates in thymectomy groupgroup
P values vs. 1940-57