the surgical airway. goals and objectives i will discuss: –brief history –general principles...
TRANSCRIPT

The Surgical Airway

Goals and Objectives• I will discuss:
– Brief history– General principles– Complications, acute and delayed– Indications– Routine management– Basic technique
• Hopefully you will gain:– Understanding of basic principles, procedures, risks, and
possible complications– Appreciation of indications and limitations of various
techniques

Tracheotomy in Popular Culture
• M*A*S*H (TV) - Father Mulcahy performs a tracheotomy on a patient whose swollen tongue prevents him from breathing
• House M.D. Several episodes (including the pilot) include tracheotomies - often in great detail
• Scrubs episode (“My Drive-By”), Dr. Turk used a knife from a nearby taco stand to perform a trach on a man choking on a burrito
• Jerico (pilot episode), Jake Green performs emergency trach on a young girl who sustained a neck injury

Tracheotomy or Tracheostomy?
• Used interchangeably (incorrectly?) to designate an opening in the anterior neck into the trachea
• Tracheotomy: The incision made into the trachea
• Tracheostomy: Surgical creation of a stoma through which air may pass to the lungs, bypassing the upper airway (implies suturing skin edges to trachea)
History of Tracheostomy
• Long, and until recently maligned– Earliest buried in legend
• Pictured on Egyptian tablets circa 3600 B.C.• Sacred Hindu book Rig Veda, written between 2000 and
1000 B.C. “The bountiful one who can cause the windpipe to reunite when the cervical cartilages are cut across.”
• Asclepiades (b 124 BC) generally considered first to carry out the procedure
• Galen and Aretaeus, 2nd and 3rd centuries A.D. - first detailed reports
• Originally used for emergency management of upper airway obstruction (limited success)

History of Tracheostomy
• “Arteria aspera” or “rough artery” - “Cartilage does not heal” - Hippocrates
• Known as the “Scandal of surgery” and “A semi-slaughter” throughout the middle ages
• No surgeon’s account until Brasavola (1500 - 1570) described his successful surgical management of Ludwig’s Angina in 1546.
• Surgical attempts feared - only 28 successful tracheotomies were reported from 1546 - 1833.



* C. Jackson, Laryngoscope 1909
History of Tracheostomy
• 1718 Lorenz Heister coined the term tracheotomy• Did not become respectable until Bretonneau and
Trousseau popularized for diptheria in the early 19th century, 25% success rate was excellent at that time
• Chevalier Jackson, modern incarnation in early 20th century, standardized technique, reduced operative mortality from 25% to 2%, proscription against incising cricoid, 1st ring, or below 5th ring*
C. Jackson, Laryngoscope, 1909, 1921
C. Jackson, Laryngoscope, 1909, 1921
• “The profession hesitates longer to advise tracheotomy than it did 50 years ago.”
• “The percentage of mortality is almost as high as of stab wounds inflicted with homicidal intent.”
• “In the hands of the most skillful and experienced the incision is usually badly placed; in the hands of the unskilled or excitable, serious accidents have occurred, such as the opening of the esophagus or a large vessel.”
• “Between the skin and the trachea, in the middle line, there is no large vessel, and no important structure. There should be no more mortality from the operation per se than from opening of superficial abscesses by an incision of equal length.”

History of Tracheostomy
• Wilson 1932 - management of airway, toilette, respiratory paralysis (Polio)
• Galloway 1950s, further expanded indications - head injury, severe chest injury, barbiturate intoxication, post-surgical airway control
• 1960s-70s, neonatal support, development of synthetics, improved tubes, low pressure/high volume cuffs greatly reduced morbidity
* Stauffer JL, Am J Med 1981
Not a Slam Dunk
• “Modern” mortality rate 2-5%• Complication rate 14-66%*
– Study design– Definition of complication– Patient follow-up
• Increased risk of complications in:– Emergency situations– ICU patients– Children and infants




Pediatric Tracheostomy
• Consistently associated with a greater mortality and complication rate
• Inverse relationship of age/size to mortality
• Pre-term and very low birth weight infants have a mortality ~ 11% related to tracheotomy
• Not so much from procedure as care issues:– Decanulation– Tube plugging– Poor pulmonary toilette

Complications of Tracheostomy
• Generally convenient though not entirely accurate to categorize by interval from procedure to onset
• Continuum - overlap– Early
• Operative
• Immediate post-op
– Late

Complications of Tracheostomy
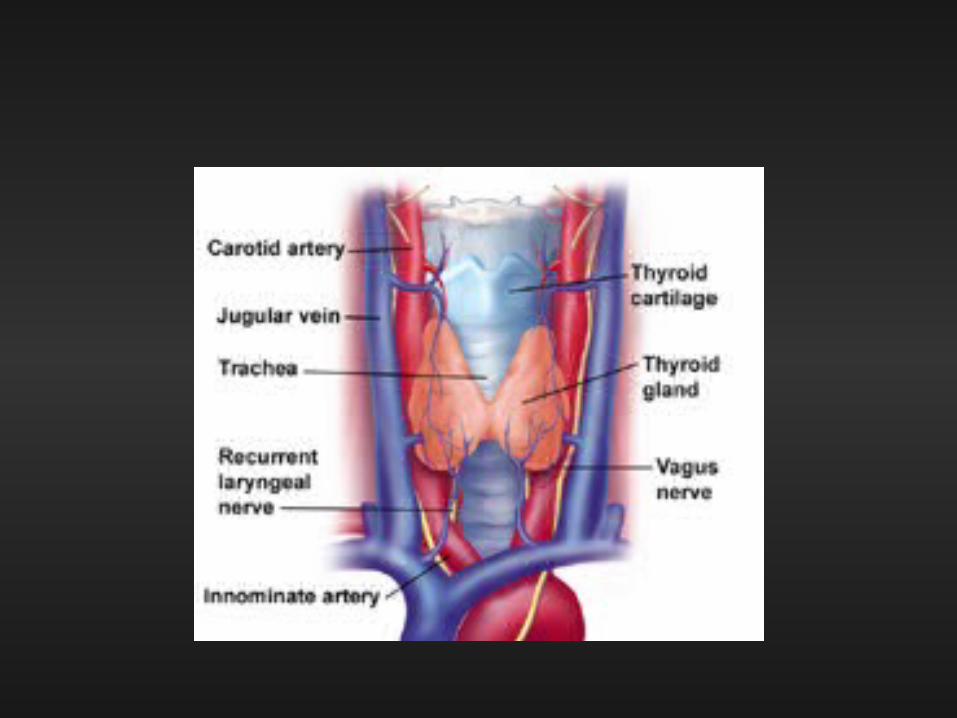
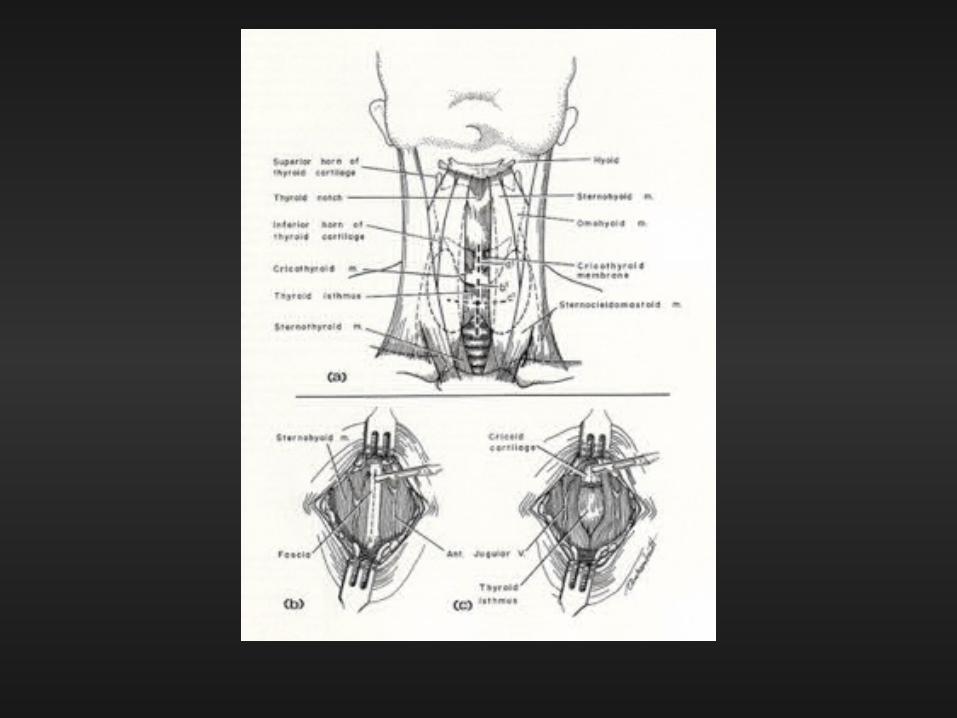
• Intra-operative– Hemorrhage
• ~ 5% rate of intra-op (or immediate post-op) hemorrhage
• Major rare but even minor can interfere with identification and access
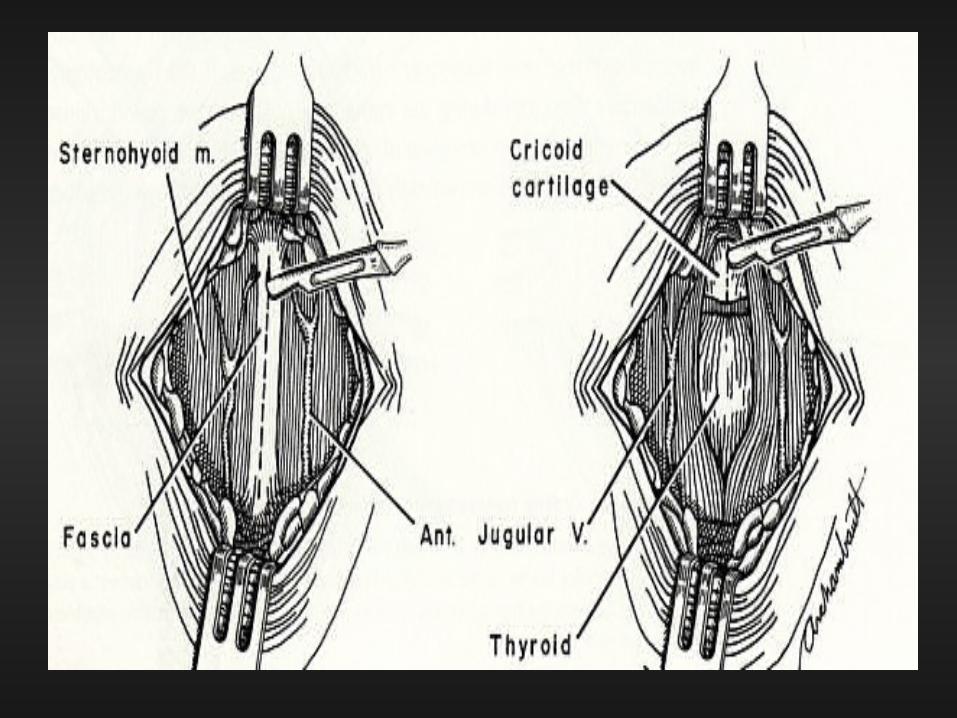
• Most commonly an error in surgical technique (one of Jackson’s major contributions - meticulous midline dissection)
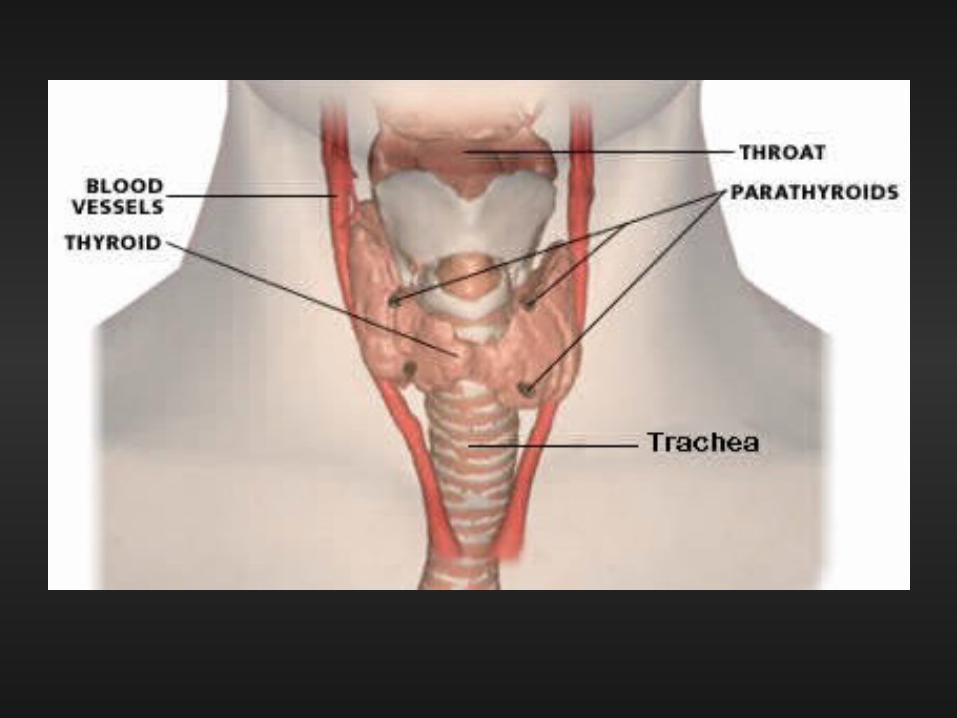
• Frequent sites:– Anterior jugular veins
– Thyroid isthmus
– High innominate artery
– Thyroid ima artery
Complications of Tracheostomy
• Intra-operative– Inability to identify trachea– Recurrent nerve injury– Tube misplacement
• Into bronchus
• Outside tracheal lumen

* Rabuzzi DD, Laryngoscope 1971
Complications of Tracheostomy
• Intra-operative– Pneumothorax / pneumomediastinum
• Adults 2-5%
• Peds up to 17% (70% in children < 2 years old*)
• Exact cause not always apparent
• Generally accepted mechanism - forceful inspiration leads to high negative intra-thoracic pressure - pathway through wound edges into mediastinum - air trapping / rupture through pleura
• Direct injury to apical pleura (esp in children due to “high position”)
• Rupture of lung bleb
• Surgical technique / errors

* Barlow DW, Otol Rhinol Laryngol 1994
Complications of Tracheostomy
• Intra-operative– Pneumothorax / pneumomediastinum
• Prevention - meticulous operative technique– Maintain midline dissection– Minimize amount of dissection– Airway control - ET tube or rigid bronchoscope (less negative
pressure and better identification of trachea)– Avoid tight closure / packing
• Evaluation - the role of the post-op CXR– Historically routine in all– Children, “difficult”, or emergent, displaced tube, signs or
symptoms of intra-thoracic complication*

Complications of Tracheostomy
• Intra-operative– Fires
• One of the most common causes of operative fires
• High O2 concentrations
• Electrocautery
– Post obstructive pulmonary edema

Complications of Tracheostomy
• Tube obstruction / decannulation– Common
• Impingement on posterior tracheal wall
• Displacement (partial or total) into mediastinum
• Blood clot
• Mucous plug
• Most serious post-op complication in children - decannulation in first 24 hours - 25% mortality
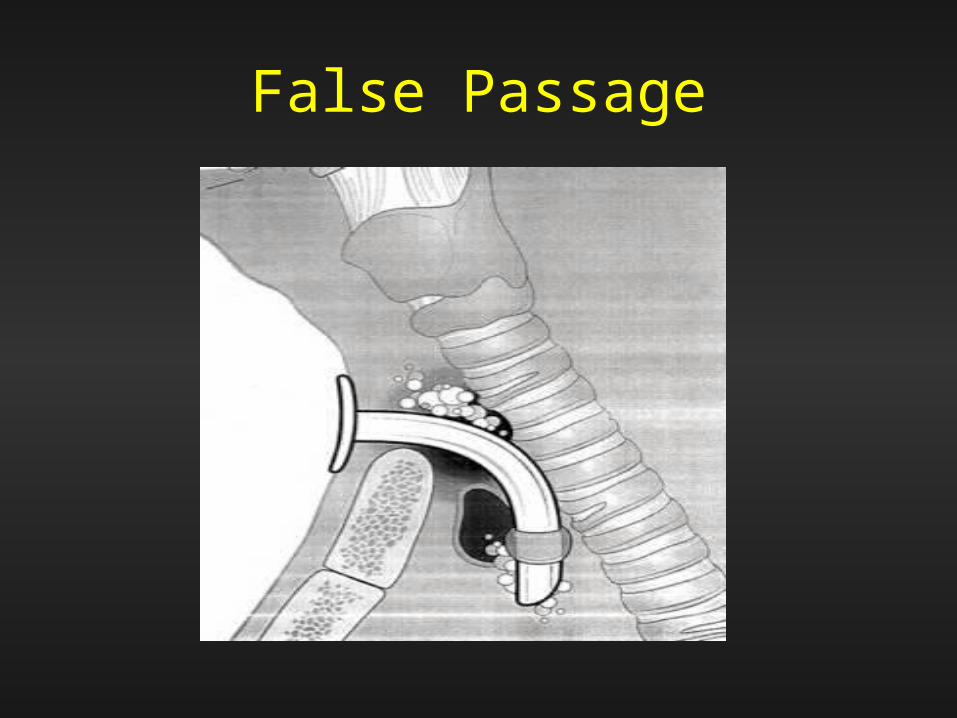
False Passage

Complications of Tracheostomy
• “Infection”– Clean contaminated wound– Incidence of infection highly dependent upon
criteria– Reported rates of stomal infections 3-36%– True cellulitis / purulence 3-8%– Stomal infections usually indolent, mild
cellulitis/granulation - respond to local care– Serious infections, mediastinitis, fasciitis, abscess,
clavicular osteomyelitis rare

* Sasaki CT, Laryngoscope 1979
Complications of Tracheostomy
• “Infection”– Bacterial colonization, 75% pseudomonas within
10 days– Stomal cultures meaningless– Antibiotic prophylaxis highly controversial
• Most feel not efficacious and only selects for resistant organisms
• Infectious contribution to sub-glottic stenosis*
– Local wound care• Ascetic acid (0.25% to 0.5%)

* Weymuller EA, Ann Otol Rhinol Laryngol 1983
Late Complications
• Tracheal damage– Direct pressure necrosis from cuff or tip of tube– Capillary flow occluded at 30 - 50 mm Hg*– Tube / cuff can exert > 400 mm Hg*
• “Modern” tubes 25 mm Hg
– Mucosal ulceration -> cartilage exposure -> bacterial colonization/invasion -> necrosis -> fibrosis with contraction / stricture / malacia
– Alternatively, progressive tracheal dilation“Increasing the tube size is not the answer!”


Late Complications
• Tracheal damage– Typical stenosis at cuff or tip site, 1 to 3.5 cm
below stoma– 0.5 to 4.0 cm in length– Granulation at site of tube fenestration– Stenosis at stoma - excessive traction on trach tube
by connecting tubing or patient motion (much less frequent now due to light, flexible connectors, etc., but vigilance still needed)
* Bryant LR, Am J Surg 1978
Late Complications
• Tracheal damage– Stomal stenosis - role of tracheal incision– In children - vertical incision in trachea - do not
remove cartilage– In adults
• Vertical tracheal incisions or incisions incorporating first ring or cricoid increase risk
• “Excessive” cartilage removal• Transverse, “H” incisions, Bjork flaps better• “Incisions that disturb anatomy least are best.”*
* Jones JW, Ann Surg 1977
Late Complications
• Massive hemorrhage from vessel erosion– Dramatic– Usually erosion into innominate artery, right carotid
reported– Tracheal necrosis from erosion/infection, usually at distal
end of tube– Associated with “low” placement of tube (“not below 5th
ring”) and/or “high” innominate artery– 0.4% to 4.5%– 50% “sentinel bleed” ( > 10ml p 24 hours)– Peak incidence 1-2 weeks p surgery, 72% in first 3 weeks*
* Jones JW, Ann Surg 1977
Late Complications
• Massive hemorrhage - Management – Suspicion mandates tube removal, flexible scope exam– Angiography not helpful and may dangerously delay
definitive treatment– Protect airway / Control bleeding - “Prompt tamponade”
• Finger pressure - successful in 89%*• Tube balloon - 85%*
– Fluid resuscitation– Surgical intervention
• Resection of artery and muscle flap best• Attempt at repairing/grafting artery > 85% mortality• Of 175 documented cases in 1991 - only 24% long term survivors
Late Complications
• Tracheo-esophageal fistula– Rare, “0.1%” - “I’ve never seen one other than
tumor”– Not as dramatic as tracheo-innominate fistula but
same potential morbidity/mortality– Incidental damage at time of surgery - rare– Pressure necrosis of party wall by trach tube and
stiff NG tube– Poor perfusion

Late Complications
• Tracheo-esophageal fistula– Increased tracheal secretions, coughing, esp. with
feedings• N.B. all patients with trachs aspirate!
– Gastric distention, paralytic ileus from insufflation– Dx.
• Contrast esophagram
• Endoscopy (usually simplest flex via trach stoma)

Late Complications
• Tracheo-esophageal fistula– No evidence these ever close spontaneously– Virtually 100% mortality if not addressed
surgically• Direct closure with muscle flap interposition
• Staged closure
• Esophageal diversion

Late(er) Complication
• Ugly scars
• Persistent tracheocutaneous fistula
• Vertical vs. horizontal skin incisions?

* Fisher SR, Laryngoscope 1991
Persistent Tracheocutaneous Fistulae
• Difficulty with phonation, skin irritation from secretions, susceptibility to respiratory infections, dysphagia
• 3.3 - 29%
• Directly related to duration of cannulation
• 70% if cannulation > 16 weeks*
• Surgical closure, most simple, some frustrating


Vertical vs. Horizontal Skin Incisions
• Horizontally– Cosmetically better?
• Vertical– Less bleeding or bleeding less likely– Tube can “seek its own level”– Helps keep you in the midline?





Laryngeal Function
• Inhibited by tracheostomy• Limitation of laryngeal elevation prevents supra-
glottic closure• Dysphagia from tube/cuff pressure on posterior
tracheal wall• Adductor reflex threshold increase• Diminished -> absent abductor activity (phasic
activity returns in 3-5 minutes with airflow - implications for periodic plugging of tube)
• Increased aspiration

Indications for Tracheostomy
• Decreasing– Improved endotracheal airway management /
expertise– Better training– Better equipment
• Tubes
• Cuffs
• Flexible endoscopes

Indications for Tracheostomy
• Respiratory obstruction• Secretion / Foreign body retention• Respiratory insufficiency / support
“If you think about doing a tracheotomy, do it (sooner rather than later)”
vs.“If you think about doing a tracheotomy, intubate and think again”

Indications for Tracheostomy
• Respiratory obstruction– Trauma
• Facial fractures• Laryngotracheal injuries
– Laryngeal / pharyngeal surgery– Head and neck surgery – Foreign bodies– Irritants/corrosives– Infections (esp. supraglottic)– Congenital anomalies– Angio-edema– Laryngeal dysfunction– Cysts, neoplasms– OSA

Indications for Tracheostomy
• Secretory retention– Obstruction of the trachea or lower airway
– Alveolar hypoventilation
• Respiratory insufficiency– Presently the most common indication for tracheostomy is
in the elderly /ventilator dependent patient with cardio-pulmonary deficiencies
Obstructive Sleep Apnea and Tracheostomy
• Effective but radical?
• Permanent stoma
• Dynamic stoma, Eliashar

Advantages of Tracheostomy
• Emergency control of airway
• Sparing further direct laryngeal injury from trans-laryngeal tube
• Facilitating care– Oral– Tracheo-bronchial toilette
• Increasing patient mobility - more secure tube
• Faster transfer from ICU / hospital
Advantages of Tracheostomy
• Improved comfort• Speech• Facilitating oral nourishment• Psychological• Better and more flexible airway control - long
term ventilation• Assisting weaning• Decreased “work” of breathing
Disadvantages of Tracheostomy
• A hole in my neck?
• Surgical procedure (remember all those complications?)
• Lack of understanding / discomfort of care givers
• Skilled care placement

Patient Selection
• Who?
• When?
• Where?
• How?

Timing of Elective Tracheostomy
• Adult– Controversy still exists concerning ideal time of
conversion from trans-laryngeal intubation to tracheostomy
– Consideration of complications:• Cuff / tip - same with both• Laryngeal - trans-laryngeal only• Stomal - tracheostomy only• Surgical - tracheostomy only• Other - sinusitis, lip, commissure, etc.

Timing of Elective Tracheostomy
• Currently accepted guidelines (adult)– If anticipated need < 10 days, use trans-laryngeal
route– If > 21 days, perform tracheostomy– Obviously large middle ground
• Individual circumstances
• Frequent evaluation
• Communication (team, family, etc.)
– Once decision made, expeditious performance

Logistics of Elective Tracheostomy
• OR vs. Bedside
• “Open” vs. “Percutaneous”
• Operating room - costly, scheduling, moving patients, IVs, hyperal, monitors, Foleys, Chest tubes, etc. - require multiple people, elevators, hallways, etc.
• Bedside - safety?, less support




Operating Room vs. Bedside
• Contra-indications for bedside– Pediatric– Unprotected airway– Emergent, acute obstruction (if time)– Neck mass (large goiter, tumor, high innominate)– Short, thick neck / non-palpable landmarks– Cricoid at or below sternal notch (some say less
than 3 cm above notch)– Coagulopathy (relative)

Open vs. Percutaneous
• Contra-indications for percutaneous, virtually the same
– Pediatric
– Unprotected airway
– Emergent, acute obstruction
– Neck mass (large goiter, tumor, high innominate)
– Short, thick neck / non-palpable landmarks
– Cricoid at or below sternal notch (some say less than 2 cm above notch)
– Coagulopathy (less relative)

Cricothyroidotomy

Cricothyroidotomy
• 1921, C. Jackson, “No end of laryngeal stenosis is the result of these high operations.” - effectively abolished this procedure
• 1976, Grow & Brantigan re-introduce - reporting lower complication rates - flawed, poor f/u
• Numerous f/u studies - avoid in acute laryngeal pathology, professional or high voice demand patients

J. Thorac Cardiovasc Surg 71:72-81:1976

Surgery, 217 – 221, Feb 1982

Cricothyroidotomy
• While operative simplicity is an advantage, higher incidence of laryngeal, subglottic, and tracheal complications and more difficult surgical repair make this procedure undesirable except in emergency situations
• In controlled situations in cadavers only 33% of non-surgeons were able to successfully cannulate the trachea via cricothyroidotomy

Cricothyroidotomy
• Maybe? The emergency procedure of choice
• Stabilization / definition of anatomy KEY!
• Patient positioning: sniffing position
• Surgeon position:– Stand on dominant hand side– Scalpel in dominant hand (assume right)
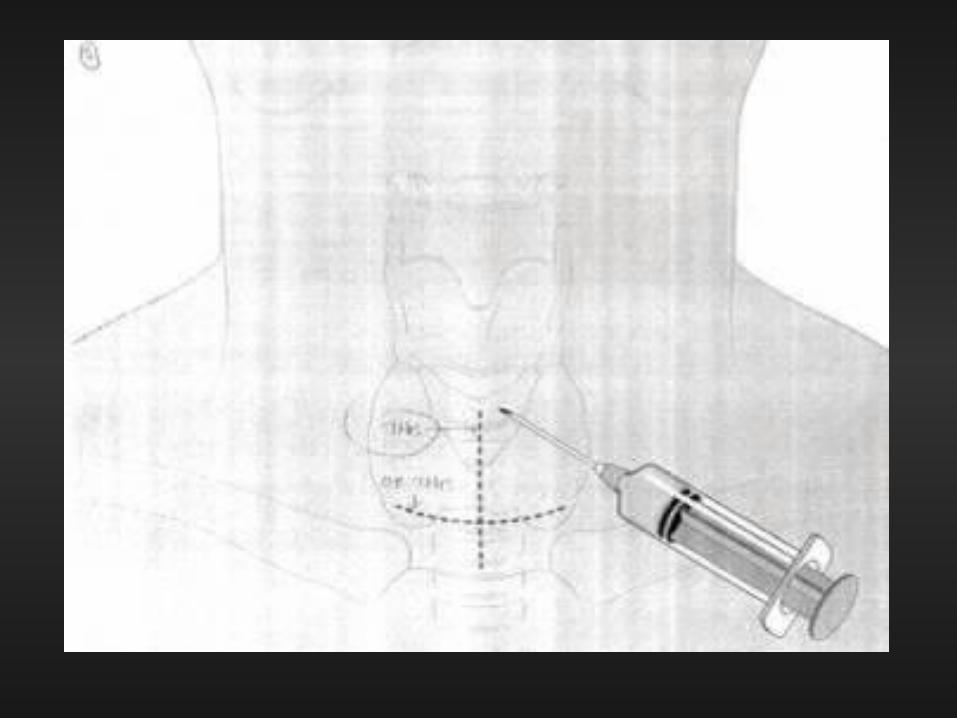
Landmarks

Landmarks
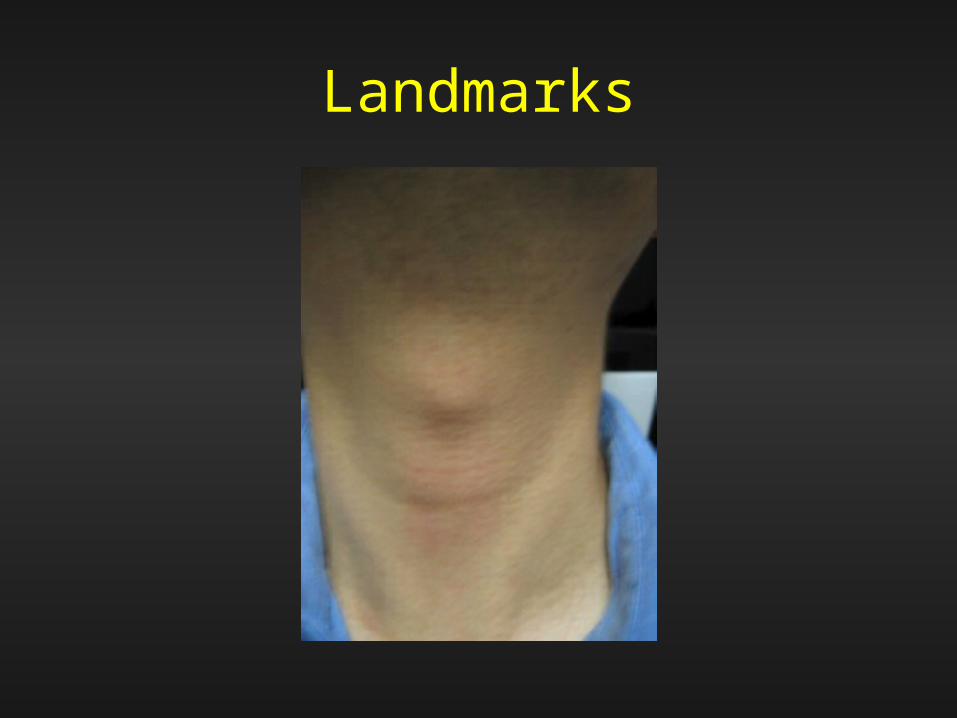
Landmarks
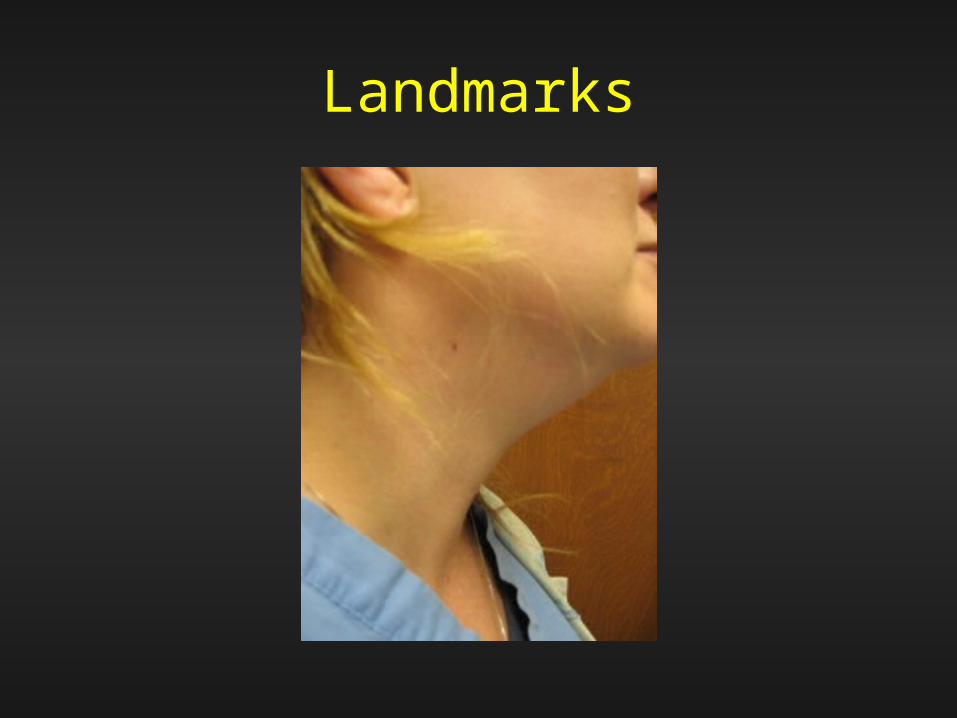
Landmarks

Landmarks


Landmarks
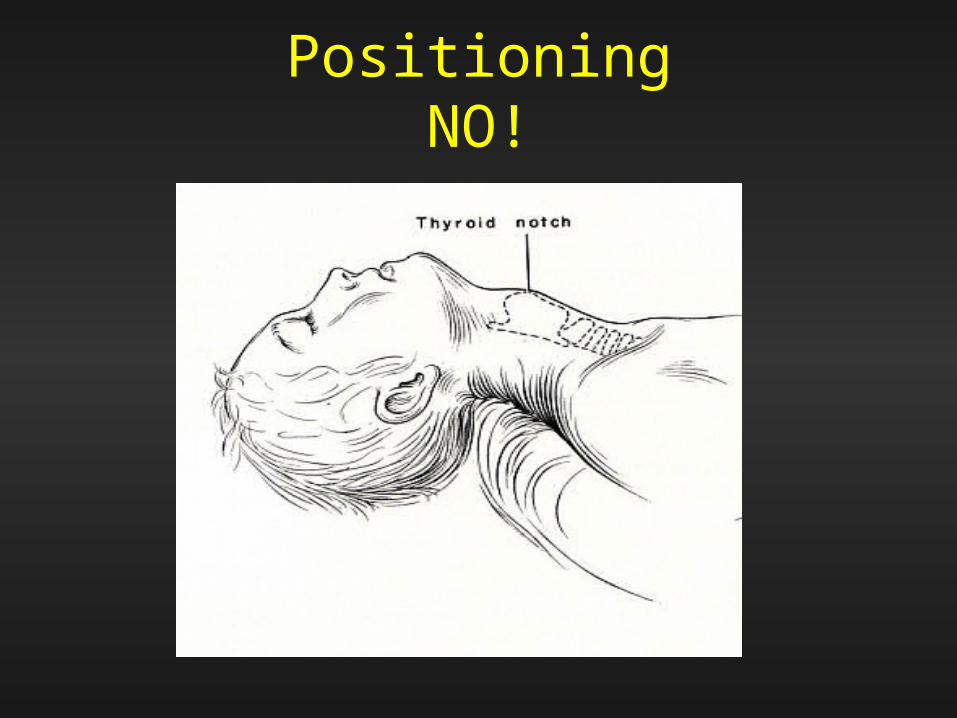
PositioningNO!

Cricothyroidotomy
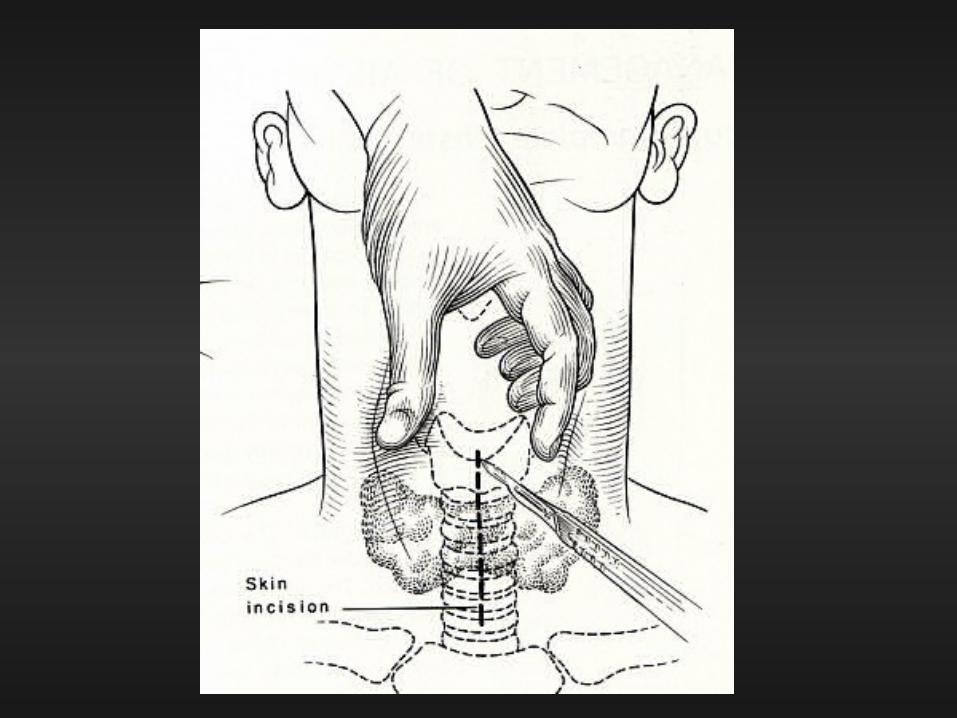
• Technique: – Left little finger toward chin– Left thumb on placed on right side of thyroid-cricoid
complex– Left third finger placed on the left side of the complex– Index finger, pointing caudal, palpates the cricoid– The thyro-cricoid complex is firmly held between the
thumb and third fingers (left hand) - a 3-4 cm vertical incision is made in the midline with caudal end over but not past the cricoid - single stroke to underlying cartilage

Cricothyroidotomy
• Technique (2)– Insert forefinger (left hand) into wound and palpate the
space between the thyroid cartilage and cricoid– Keeping your forefinger in the wound - palpate the inferior
edge of the thyroid cartilage – Turn the scalpel from vertical to horizontal, place it along
the index finger into the cricothyroid space– Push it into the airway– To open the airway - twist the knife with the sharp edge
against the cricoid– Hold in place until suitable stent (tube) can be inserted


Cricothyroidotomy

Charles Vaugh MD, 2005
Cricothyroidotomy
• “Start to finish takes less than 5 seconds”
• Critical elements are fixing the airway in the midline, locating the cricoid - both done with surgeons non-dominant hand
• “Can be done blindfolded - or in the dark”

Open TracheostomyBasic Technique
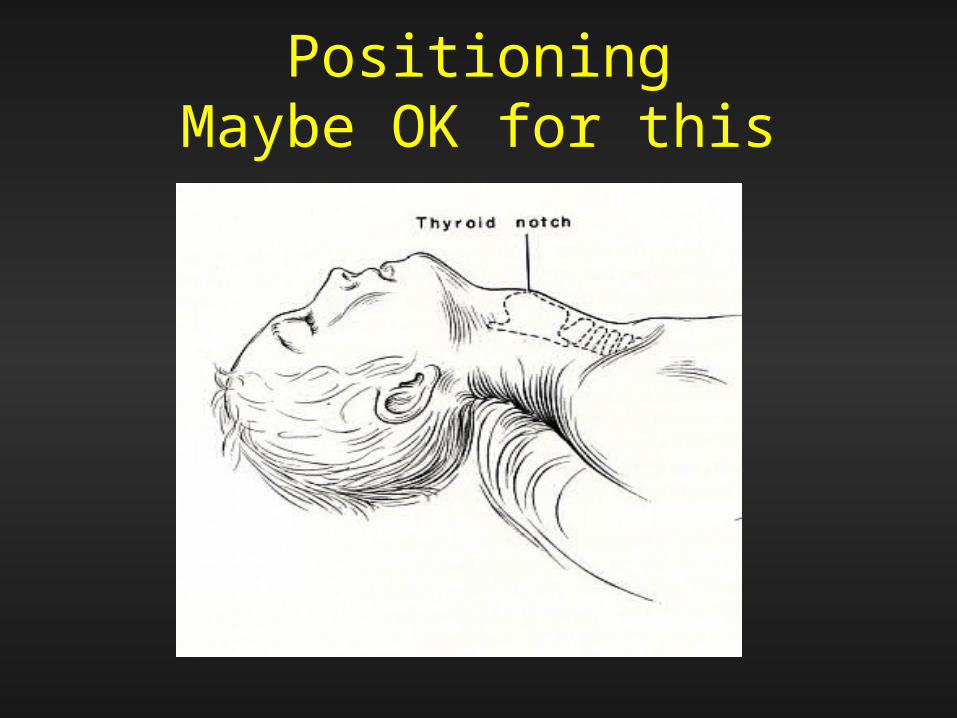
PositioningMaybe OK for this
MIDLINE!MIDLINE!MIDLINE!




T-Tubes

T-Tube

Summary
• Usually sick or injured
• In an emergency - any landing (airway) you walk away from… keep your head, know your anatomy!
• “Minor surgery” with potential for disaster
• Meticulous technique - MIDLINE - MIDLINE - MIDLINE!
• Teamwork





Thatcher GW, Laryngoscope 2003
Obstructive Sleep Apnea and Tracheostomy
• Thatcher and Maisel 2000– Retrospective study - 79 patients followed 3 months to 20
years – 70 men, 9 women– Age 25 - 70 years, mean 47 y/o– RDI 45 - 146, mean 81– “Eliminated” OSA in all– 16 patients decannulated– 14 deaths
• 2 related to trach - one postop MI, one tracheo-innominate fistula• 5 cardiopulmonary, 2 postop unrelated surgery, 1aspiration
Thatcher GW, Laryngoscope 2003
Obstructive Sleep Apnea and Tracheostomy
“Severe obstructive sleep apnea and its comorbid conditions are effectively treated by tracheostomy. …Significant morbidity and mortality are low. Chances of obstructive sleep apnea resolution allowing decannulation remain poor.”