the shoulder exam jeffrey rosenberg md residency program in family medicine montefiore hospital june...
TRANSCRIPT

The Shoulder Exam
Jeffrey Rosenberg MD
Residency Program in Family Medicine
Montefiore Hospital
June 2, 2005

Objectives
Learn the anatomy of the Shoulder joint so as to better understand shoulder pathology
Review the proper primary care based shoulder examination
Discuss shoulder pathology in relation to age of patient and mechanism of injury

Case #1
20 yo male who plays weekend softball p/w pain over the anterior lateral aspect of the rt. shoulder and lateral upper arm. No specific injury noted. C/o pain when combing hair and at nighttime. Exam sig. for nl anatomy, painful arc from 70-130 deg., nl rotator cuff strength. What could his diagnosis be?

Case #2
45 yo female p/w gradual onset of pain on top of left shoulder. Pt does remember a sign. fall several years ago onto the left arm and shoulder. C/o pain at night, and with raising arm above head. Exam shows mostly normal AROM and PROM. Tenderness over AC joint with mild protuberance. What could be the cause of this pain

Shoulder Bones

Glenoid Cavity

Acute Pain (<2 weeks)
Fracture if sig fall (esp in >50) Shoulder Instability:
Subluxation/Dislocation-fall with arm outstreched overhead
Acute rotator cuff tear-fall with arm abductedNeed quick diagnosis/treatment
AC joint separation (if falls onto side of shoulder)

Pathology for subacute/chronic often based on age of patient
Middle Aged (30-50): Impingement Syndrome, Partial rotator cuff tears Frozen shoulder
Older patient (>50): Complete RTC tear Degenerative Arthiritis-lots of stiffness Frozen shoulder-lots of stiffness Fracture after fall

Shoulder Exam
Start with anatomy. Symmetry of the shoulder, protuberance over AC joint, atrophy of muscles
Tenderness: Biceps Tendon, Lat and Post shoulder, AC joint, SC joint, Clavicle, Scapular Spine

Range of Motion
Measure ROM and feel for crepitus Flexion: move arm forward from body anteriorly
0-165 Extension: move arm backwards from body
posteriorly 0-60 Abduction: Abduct arm away from body. 0-170.
Note painful arc: 70-120 acromial imping. vs. 130-160 AC jt imping or arthritis

Range of Motion
EXTERNAL ROTATION: (nl 90 degrees) Lack of External Rotation with elbow/shoulder
in neutral equal Frozen Shoulder/GH arthritis External Rotation Strength from infraspinatus
REMEMBER for Abduction: Initial 20 degrees of motion from deltoid and ss 20-130 from supraspinatus 130-150 from rotation of scapula

Range of Motion
If motion limited, move passively Drop test: Passively Abduct; let go of arm ?
maintain abduction. If not: RTC likely completely torn!! Injection w/ lidocaine and repeat to make sure
Hold scapula and passively abd arm-Decreased movement equals joint restriction from frozen shoulder or GH arthritis.

Range of Motion
Cross Body Adduction: adduct arm across body. 0-50: Painful with AC joint pathology.
Internal Rotation: can be done in abduction or extension: measure by vertebrae of t-spine.

Rotator Cuff

Rotator Cuff Strength
Supraspinatus: Empty can test Infraspinatus and Teres
Minor: Hitch hiker test (ext rotation with elbow next to body)
Subscapularis: with arm internal rotation and extension, have patient move hand away from body

Impingement Syndrome
Impingement of RTC or bursa Inflammation/Swelling increase the size in a
tight space OR space gets smaller secondary to bony growth. Can progress to RTC tear.
Swelling ->Tendonitis and Fibrosis->Degeneration (Tendinosis) and Tears
Often Coexist/continuum

Subacromial Bursa

Impingement and the ACROMION

Impingement Syndrome
Symptoms: gradual onset, anterior-lateral pain, worse overhead, night time pain
Tender over ant or lateral shoulder. Crepitus and Pain with active abduction 60-120 degrees (painful arc). Normal Strength Neer and Hawkins Impingment tests painful.
If positive, could inject with lido,steroids and repeat. If sx resolve, impingement evident

Impingement Signs
Neer impingement sign. Forcibly flex arm fully above head to produce pain as humerus compressed Rotator cuff against coracoacromial arch

Impingement Signs
Hawkins sign: Abduct arm 90 deg., flex, and forcibly internally rotate arm. Pain sign for subacromial impingement or rotator cuff tendonitis.

Gleno-humeral Instability
Inability to keep humeral joint centered in glenoid socket: Sense of Slippage.
TUBS: Traumatic subluxation/dislocation Unilateral, involve tear of glenoid labrum-Bankart Lesion, needs Surgery
AMBRI: Atraumatic dislocation, Multidirectional, Bilateral, Rehab.

Gleno-humeral Instability
Sling 6 weeks (external rotation best): Recurrent Dislocation dependant on age/sport
Need lots of PT-if no help-surgery If occurs > 2 times, reoccurs almost 100%-
needs surgery especially if young/active Subtle instability -> secondary impingement in
overuse situation (swimming, pitching, tennis, etc). Fatigue causing migration of head
Gleno-humeral instability
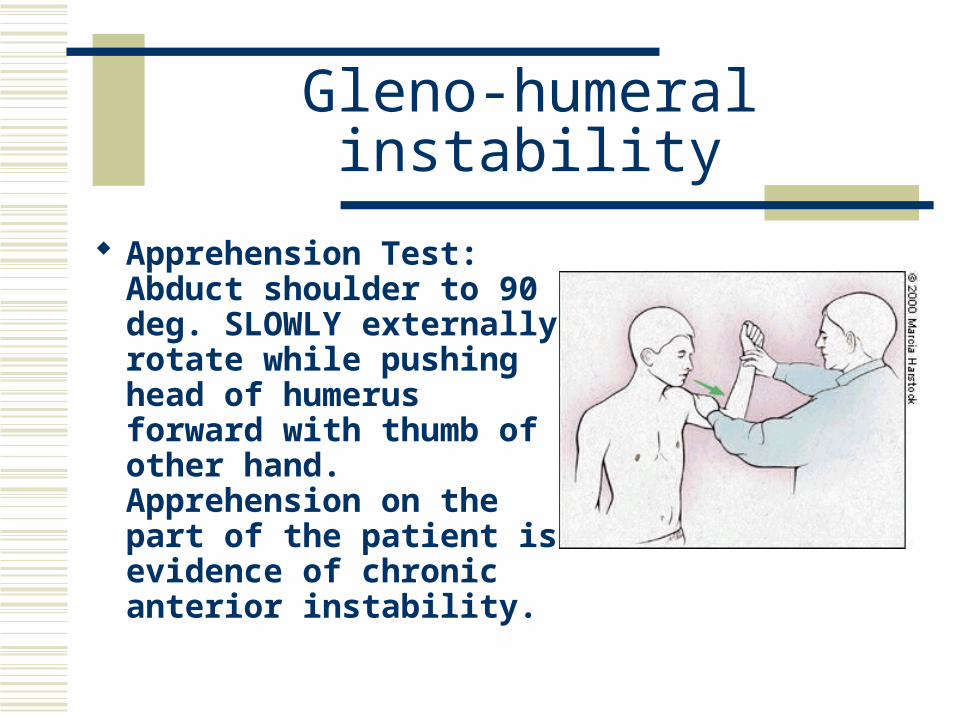
Apprehension Test: Abduct shoulder to 90 deg. SLOWLY externally rotate while pushing head of humerus forward with thumb of other hand. Apprehension on the part of the patient is evidence of chronic anterior instability.
Gleno-humeral Instability
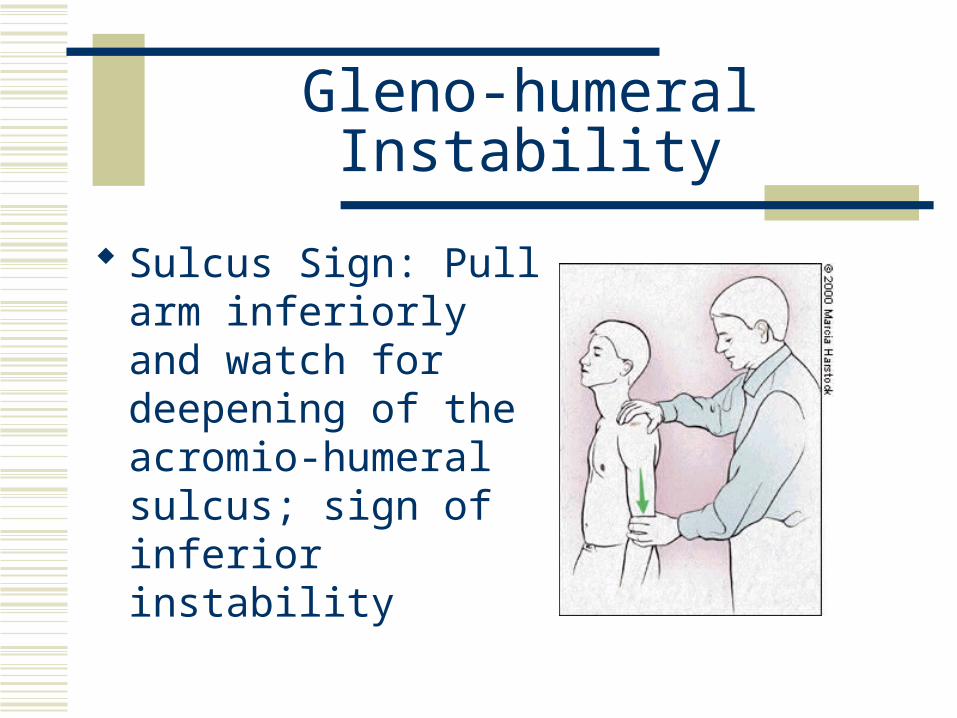
Sulcus Sign: Pull arm inferiorly and watch for deepening of the acromio-humeral sulcus; sign of inferior instability

Don’t Forget about the Neck
Investigation of shoulder complaints is not complete without investigation of the cervical spine:
Palpate cervical spine
Check DTR’s, sensation and strength
Spurlinigs Sign

Radiography
Acutely: Episode of Dislocation S/p trauma with AC joint/Clavicle Pain After fall in older patient (>60) with decreased
ROM

Radiography
Chronically: Frozen Shoulder >50 (to see in GH OA) Acromion View : increases likelihood of
significant. RTC Pathology

Radiography
MRI: Useful for evaluating for Rotator Cuff Tears (partial/complete)-I order them if patient not better with steroid injection/still have weakness
If looking for labral tear-Need intra-articular Gadolinium