the ross procedure: when and how? - penn medicine ross procedure: when and how? hans-h. sievers ......
TRANSCRIPT

1
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
The Ross Procedure:When and How?
Hans-H. Sievers
Department of Cardiac and Thoracic Vascular Surgery, University of Lübeck
Course Director: Joseph E. Bavaria, MD Co-Directors: Munir Boodhwani, MD, MMSc Prashanth Vallabhajosyula, MD, MS John Augoustides, MD
Conflict of interests:Royalties from Braun Melsungen for vascular prostheses
(Sinus prosthesis, curved prosthesis)

2
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
The problem, the calcified aortic valvein this case a type I L/R bicuspid aortic valve needing replacement

3
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Surgical goal
The surgical goal is to achieve normal conditions.
Therefore the native aortic valve is
the blueprint for a perfect aortic valve substitute.
Theoretically these criteria can be met most likely with the autologous pulmonary valve. Ross principle

4
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
The pulmonary autograft is autologous, living and has a similar development, anatomy and histology of the aortic valve giving reason to use the pulmonary valve for aortic valve replacement – The Ross operation
a) The autograft has no fibrous annulus. manageable (intra-annular implantation)
b) The pulmonary valve is transplanted from low pressure circulation to systemic pressure. adaptation seems possible
b) The pulmonary valve is surgically manipulated.
c) The Ross operation necessitates the replacement of the pulmonary valve with a homograft converting a one valve disease to a potential two valve problem. How big is the risk?
But there are some special issues to be considered:
5
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
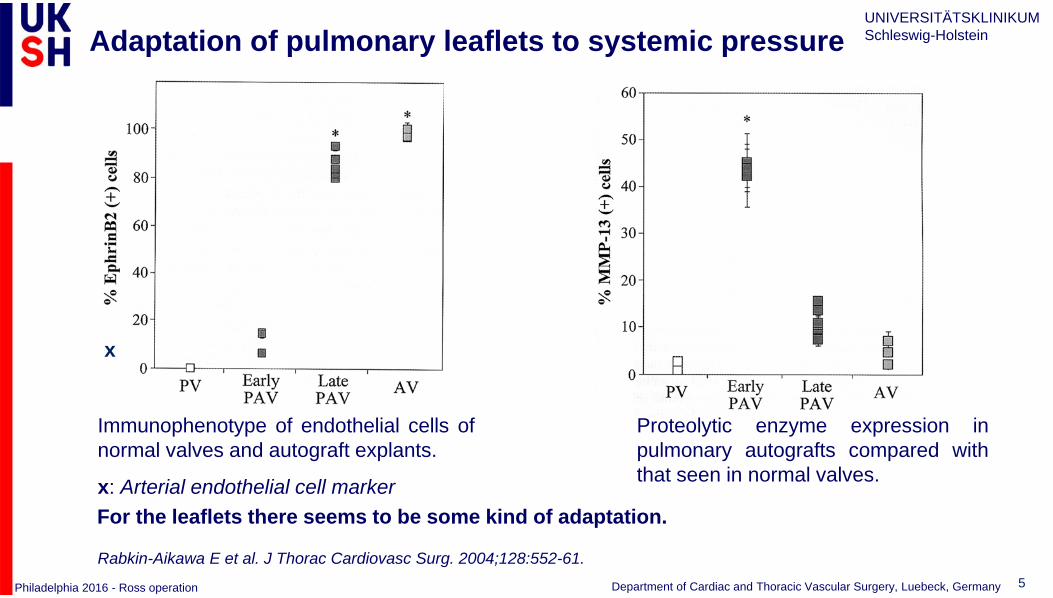
Proteolytic enzyme expression inpulmonary autografts compared withthat seen in normal valves.
Rabkin-Aikawa E et al. J Thorac Cardiovasc Surg. 2004;128:552-61.
Immunophenotype of endothelial cells ofnormal valves and autograft explants.
x: Arterial endothelial cell markerFor the leaflets there seems to be some kind of adaptation.
Adaptation of pulmonary leaflets to systemic pressure
x

6
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Ross Techniques in the Ross Registry (n=1945)
Subcoronaryn=797
SC
Root Replacementn=465
RR
Reinforced Root Replacement
n=611
RR+R
Root inclusionn=72
RI

7
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
8
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
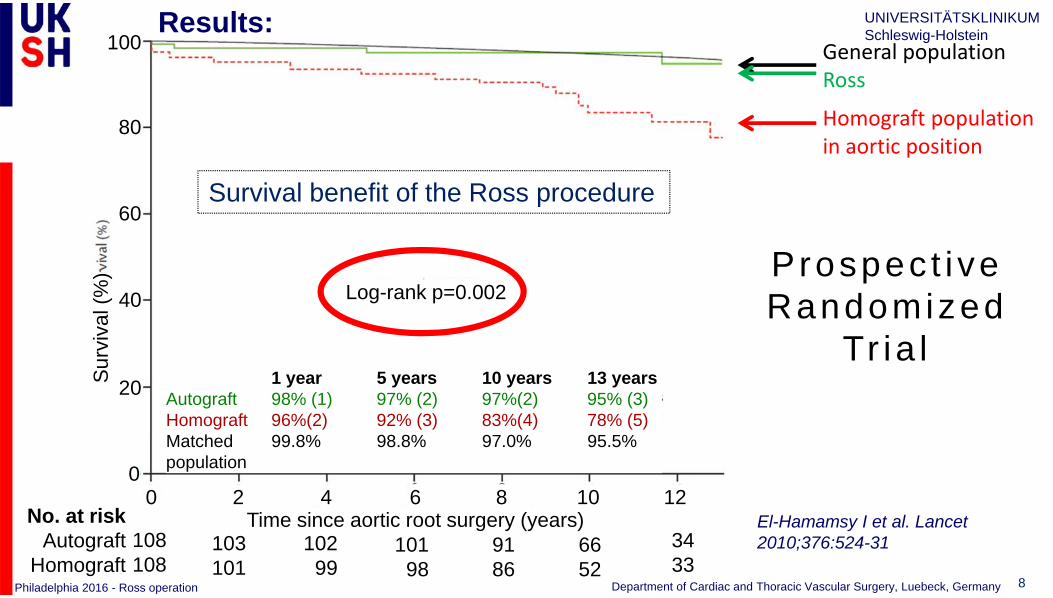
El-Hamamsy I et al. Lancet 2010;376:524-31
General populationRoss
Homograft populationin aortic position
Prospec t i ve Randomized
Tr ia l
100
80
60
40
20
0
0 2 4 6 8 10 12
1 year 5 years 10 years 13 yearsAutograft 98% (1) 97% (2) 97%(2) 95% (3)Homograft 96%(2) 92% (3) 83%(4) 78% (5)Matched 99.8% 98.8% 97.0% 95.5%population
Time since aortic root surgery (years)
Sur
viva
l (%
)
Log-rank p=0.002
108108
103101
10299
10198
9186
6652
3433
No. at riskAutograft
Homograft
0
Results:
Survival benefit of the Ross procedure

9
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Is the survival advantage bias? (Patient solution or real Ross-related?)
Probability of survival of the Ross patients compared with the general German population; 17 patients with <30 day mortality were excluded.
20 years registry results
Sievers HH et al. Eur J Cardiothorac Surg. 2016. 49; 1:212-218

10
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Autograft + Homograft Reoperation – Adult populationStratification by technique (n=1779, Registry1)
1 Sievers HH et al. Eur J Cardiothorac Surg. 2016.49:212-8.
XenograftFann et al. Curr OpinCardiol.2001;16:126-135.
SCRR+RRR
Ross
Age 51 - 60Age 41 - 50
Age 16 - 30
Age 31 - 40
Age (years):
45.1 ± 11.2 (SC)
45.7 ± 11.3 (RR-R)
40.3 ± 12.8 (RR)
LOR: ~ 1% / ptyear

11
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Projections for the Need for a ReoperationE.g. for a patient at 45 years of age at first operation the probability to be alive with ReOP at 75 years of age is 19%; to be alive without ReOP is 41%.
The probability to be dead without ReOP is 33% and to be dead with ReOP 7%.
Sievers HH et al. Eur J Cardiothorac Surg. 2016;49:212-8.

12
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Sievers HH et al. Eur J Cardiothorac Surg. 2016;49:212-218
(Left) The time course of transvalvular mean and maximum homograft gradients.(Right) Longitudinal probability of being in each pulmonary regurgitation grade with time.
Longitudinal probability of being in each autograft regurgitationgrade with time. AR: aortic regurgitation.
PI PS AI
AS: 3.5 mmHg mean dP

13
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Spatiotemporal velocity maps. Representative spatiotemporal velocity maps for 4 groups.Torii R et al. J Thorac Cardiovasc Surg 2012;143:1422-1428
Flow velocity through the aortic valve –Normal flow after the Ross-Procedure

14
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
She wrote: „After the Ross operation (previously mechanical valve) my life really began and became perfect with the uncomplicated birth of my daughter.“

15
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
ConclusionThe Ross operation up to 24 years
• is a complex operation, however the hospital mortality is relatively low (last 500 cases no death, 2 in all 700)
• is performed in selected patients, preferably with aortic stenosis, <55 years• provides excellent survival• provides near normal hemodynamics in the majority of patients (blood
pressure control!)• needs no anticoagulation, has no noise, low thromboembolism (minor and
major)• has a linear risk of reoperation of ~ 1% / ptyear (endocarditis)
Nevertheless the Ross operation does not provide 100% normal results, but what is better especially in young patients?

16
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Long-Term Outcomes of the Ross Procedure Versus Mechanical Aortic Valve Replacement: Propensity-Matched Cohort Study.Mazine A, David TE, Rao V, Hickey EJ, Christie S, Manlhiot C, Ouzounian M
What Are the Clinical Implications?
• The clinical implication of this study is that young and middle-aged adults requiring AVR may benefit from a Ross procedure.
• The long-term freedom from stroke and major hemorrhage should be considered in discussions of valve replacement options.
• Findings from this study suggest that in specialized centers, the Ross procedure represents an excellent option and should be considered for young and middle-aged adults undergoing AVR.
Circulation. 2016;134:576-85.major bleeding/stroke
Mazine A et al. Circulation. 2016;134:576-85.
17
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
Future of the Ross operation • The Ross operation remains a surgical challenge and does not have an easy time in our current
cardiovascular world (focus on TAVI, minimal invasive).Nevertheless the Ross operation will survive in experienced centres for special indications and in selected patients. Results can be improved:
- Standardization and optimization of operative techniques(SOP of all experienced centres, what have we learned?)
- PostOp blood pressure control- Awareness and prophylaxis of endocarditis- Improving of homograft (tissue engineering, interventional replacement)- Training programs (trainee school)
• In the meantime alternatives will improve:- New bioprostheses with longer durability and pressure gradient < 10 mmHG (surgery + product)
• Bioprosthesis first and later TAVI• Novel mechanical prostheses without anticoagulation• Whatever we do we must direct our decision making to a personalized treatment strategy (patient and
surgeon), and • It is our responsibility to follow all patients carefully and lifelong
18
UNIVERSITÄTSKLINIKUM Schleswig-Holstein
Philadelphia 2016 - Ross operation Department of Cardiac and Thoracic Vascular Surgery, Luebeck, Germany
- Thank you for your attention -