the role of overactive bladder treatment
TRANSCRIPT

THE ROLE OF OVERACTIVE BLADDER TREATMENT
Prof. Junizaf, SpOG(K)
Division of UrogynecologyDepartment of Obstetrics and Gynecology
School of Medicine, University of Indonesia/Dr. Cipto Mangunkusumo Hospital
Jakarta, Indonesia




Toilet dependence

Overactive Bladder (OAB)

What is Overactive Bladder (OAB)Overactive Bladder (OAB) is a “symptom syndrome suggestive of lower urinary tract dysfunction”It is specifically defined as:
Urgency, with or without urge incontinence, Usually with frequency and nocturia
Standardisation Subcommittee of the International Continence Society (ICS)
OAB is used in the absence of proven infection or other obvious pathology
Usually suggestive of detrusor overactivity, but can be due to other urethro-vesical dysfunction.
Abrams P, Cardozo L, Fall M et al Neurourol Urodyn 2002;21:167-178

International Continence Society definitions
Urgency A sudden compelling desire to pass urine, which is difficult to defer
Incontinence Any involuntary leakage of urine
Frequency Voiding too often – usually defined as 8 or more times in 24 hours
Nocturia Waking more than once at night to void
Abrams P, Cardozo L, Fall M et al Neurourol Urodyn 2002;21:167-178

Impact of OABImpact of OAB
Emotional effects Disruption to activities of daily
life
Economic
embarrassmentshamesocial withdrawal
♫proximity to toilets is important
♫reduced fluid intake
♫avoidance of sexual intimacy
♫loss of independence
♦ spend on incontinence pads
♦ loss of employment♦ direct costs of
laundry

Normal Detrusor Function during Filling Cystometry (CMG)
Normal detrusor function allows bladder filling with little or no change in pressure. No involuntary phasic contractions occur despite provocation.
Abrams P, Cardozo L et al Neurourol Urodyn 2002;21:167-178 (Page 173L)

Filling Cystometry (CMG) (Normal)
Namiki M, 1998


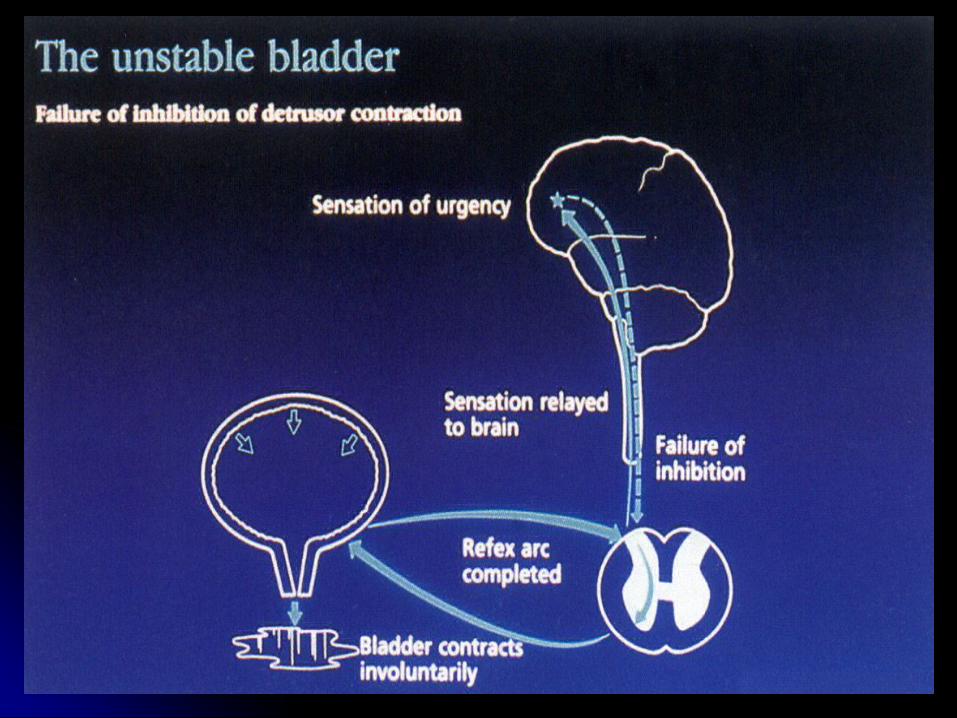
Involuntary Detrusor Involuntary Detrusor ContractionsContractions(Abnormal)(Abnormal)
Namiki M, 1998


Detrusor Overactivity (DO)Detrusor overactivity is a urodynamic observation characterised by involuntary detrusor contractions during the filling phase which may be spontaneous or provoked.
1. Neurogenic detrusor overactivity When there is a relevant neurogical condition This term replaces the term “detrusor hyperreflexia”
2. Idiopathic detrusor overactivity When there is no defined cause →Non-neurogenic This term replaces the term “detrusor instability”
Unstable detrusor (what is called Unstable bladder, =Detrusor instability) in the previous version (1989) →Deleted
Abrams P, Cardozo L et al Neurourol Urodyn 2002;21:167-178 (Page 173 L&R)


OAB is Nearly as Common as Arthritis and Sinusitis
05
10152025303540
Chronic
sinusitis
1
Hay fever/
Allergic rhinitis
1
High cholesterol1
Chronic
bronchitis1
Diabetes1
Arthriti
s1
Heart disease1
Asthma1
1. National Center for Health Statistics. Vital health stat 10;1994. 2. Stewart W et al. World J Urol. 2002. Available at: http://link.springer.de/link/service/journals/00345.
Mill
ions
Overactive
Bladder2

Prevalence of urge vs stress incontinence
Booth C and Pascoe D Hospital Pharmacy 2002; 9: 65-68
WOMEN MEN
Urge IncontinenceStress Incontinence
Mixed Incontinence

THE GLOBAL BURDEN OF OAB:USA
Overall, 16,5% of the population aged > 18 years (~ 33 million people) had symptoms of OAB
Prevalence of OAB increases with age
*>micturitions per day Stewart W et al World J Urol. 2002 Available athttp://link.springer.de/link/service/journale/00345
N=5,204MenWomen
Age (years)10-24 25-34 35-44 45-54 55-64 65-74 75+
0
5
10
15
20
25
30
35
40
Prev
alen
ce (%
)

*>8 micturitions per day or nucturia 2x
THE GLOBAL BURDEN OF OAB:EUROPE
Overall, 16,5% of the population aged > 40 years in 6 European countries have symptoms of OAB
Prevalence of OAB increases with age
Milson I et al BJU Int. 2001;87:760-766
N=16,776MenWomen
Age (years)
40-44 45-49 50-54 55-59 60-64 65-69 70-740
51015
2530
35
40
45
Prev
alen
ce (%
)20
75+

53% of Asian Women Have Symptoms of OAB
65
55
21 21
0
10
20
30
40
50
60
70
Urgency Frequency Incontinence PercentSeeking
Treatment
Perc
ent o
f Wom
en
with
OA
B S
ympt
oms
Questionnaire survey of 5,502 women from 11 countries in AsiaUrgency and frequency are the most common LUTS
● OAB is undertreated
Lapitan MC, Chye PL. Int Urogynecol J Pelvic Floor Dysfunct. 2001;12:226-231.

Storage Symptoms and Incontinence
UUI:“OAB wet”
(6.1%)
“OAB dry”urgency
frequencynocturia (10.3%)
SUI: stress urinary incontinenceUUI: urge urinary incontinence
Mixed SUI/UUI (2.7%)SUI
In a recent US survey (n = 5204),16.5% of individuals in the general population met the criteria for OAB
Stewart W et al. World J Urol. 2002. Available at: http://link.springer.de/link/service/journals/00345.

FrequencyUrgency
Overactive bladder
Urge incontinence
SYMPTOM OVERACTIVE BLADDER

1. HISTORY2. PHYSICAL EXAMINATION3. LABORATORY TEST4. URINARY DIARY5. URODYNAMICS
DIAGNOSTIC OVERACTIVE BLADDER (OAB)

Fantl JA et al. Agency for Healthcare Policy and Research;1996; AHCPR Publication No. 96-0686.
1. LABORATORY TESTS Urinalysis
to rule out hematuria, pyuria, bacteriuria, glucosuria, proteinuria
Blood work as appropriate glucoseprostate specific antigenothers

1. URINARY DIARY
Time Drinks Urination Accidental Leaks Did you feel a strong
urge to go?
What were you doing at the time?
What kind?
How much?
How many times?
How much? (fill in amount:
small, medium, large)
How much? (fill in amount:
small, medium, large)
Sneezing, exercising, having sex, lifting, etc.
Sample coffee 2 cups 12 large large yes laughing
6–7 AM
7–8 AM
8–9 AM
9–10 AM
10–11 AM
11–12 PM
12–1 PM
1–2 PM
2–3 PM
3–4 PM
4–5 PM
Your Daily Bladder DiaryThis diary will help you and your healthcare team. Bladder diaries help show the causes of bladder control trouble. The “sample” line (below) will show you how to use the diary.
Your name: J. Doe Date: March 31, 2003
DIAGNOSTIC INCONTINENCE URINE

CONTOH DAFTAR HARIAN BERKEMIHKARTU CATATAN BUANG AIR KECIL Tgl
Hari ke-I y y y y m m d d
Interval waktu Buang air kecilBiasa
Mengompol Keinginan buang air kecil
Keadaan
Tengah malam –1.00
1.00-2.00
2.00-3.00
3.00-4.00
4.00-5.00
5.00-6.00
6.00-7.00
7.00-8.00
8.00-9.00
9.00-10.00
10.00-11.00
12.00-13.00
13.00-14.00
14.00-15.00
16.00-16.00
16.00-17.00
17.00-18.00
18.00-19.00
19.00-20.00
20.00-21.00
21.00-22.00
22.00-23.00
23,00-24.00


OVERACTIVE BLADDER TREATMENT
Conservative Bladder training Pharmacothrapy

Current approaches to OAB treatment
Drugs licensed for OAB symptoms
Antimuscarinics are currently first-line therapy for OAB (eg tolterodine, oxybutynin [also has antispasmodic action], trospium, propiverine)
Antispasmodics (eg flavoxate, oxybutynin [also has antimuscarinic action])
Other drugs used off-licence for OAB symptoms
Alpha blockers (eg doxazosin)Beta agonists (eg tarbutaline)Antidepressants (eg imipramine)Prostaglandin synthesis inhibitors (eg indomethacin)Vasopressin analogues (eg desmopressin)Miscellaneous (eg baclofen)
Non-pharmacological methods
Bladder retraining
Pelvic floor exercises
Andersson KE, Chapple C, Wein A World J Urol 2001; 19: 294-8Garely AD and Burrows LJ Expert Opin Pharmacother 2002; 3(7):827-33
The challenge is to eliminate bladder overactivity without interfering withthe function of other organ systems and without disturbing normal micturition

PHARMACOLOGIC THERAPYAntimuscarinic agents are the mainstay for treating OABOAB symptoms are relieved by inhibition of involuntary bladder
contractions increased bladder capacity
Treatment can be limited by side effects such as dry mouth, GI effects (eg, constipation), and CNS effects

Antimuscarinic drugsMainstay of treatment for OABInclude:Oxybutynin TolterodineFlavoxatePropiverineTrospium
Exerts bladder relaxation through antimuscarinic activityAlso known as anticholinergics

Muscarinic Receptors
Five pharmacologically defined receptors, M1- M5
Sigala et al 2002Predominance of M2 and M3 receptors Yamaguchi et al 1996, Sigala et al 2002M2 receptors predominanc 3:1 over M3 receptorsMuscarinic receptors found≈ Urotelial cells≈ Suburotelial nerves≈ Interstitial cells≈ Chess-Williams 2002, Gillespie et al 2003

Lack of bladder selectivity results in anti-cholinergic adverse events in other organs: Salivary glands: dry mouth GI tract: constipation, nausea and vomiting, diarrhoea Eyes : blurred vision CNS : drowsiness, headache Heart : palpitations Skin : dryness
Anticholinergic side effects

MUSCARINIC RECEPTOR DISTRIBUTION

OxybutyninTertiary amine that undergoes considerable first-pass metabolismPotent muscarinic receptor antagonist with some degree of selectivity for M3, M4, and M1 receptorsLocal anesthetic as well as smooth muscle relaxant effects at doses higher than those used in clinical practiceLower doses used to improve tolerability profile
Broadley, Kelly. Molecules. 2001;6:142-193.

TolterodineDeveloped specifically for overactive bladderMuscarinic receptor antagonist nonselective for the M1 to M5 receptorsOrgan selective for bladder over salivary glandsClinically proven to have fewer side effects than oxybutynin
Nilvebrant L et al. Life Sci. 1997;60:1129-1136.Abrams P et al. Br J Urol. 81.801-810.

Summary1. Overactive Bladder (OAB) is a “symptom syndrome suggestive of
lower urinary tract dysfunction”. It is specifically defined as Urgency, with or without urge incontinence, Usually with frequency and nocturia
1. Overactive Bladder syndrome (OAB) is highly prevalent condition that adversely affects the quality of life (QOL) of many individualy
1. Current approaches to OAB treatment, is Antimuscarinics (eg tolterodine, oxybutynin, trospium, propiverine) and Non-pharmacological methods (Bladder retraining Pelvic floor exercises)
Abrams P, Cardozo L, Fall M et al Neurourol Urodyn 2002;21:167-178
THAK YOU