the reversal trial reversing atherosclerosis with aggressive lipid lowering
TRANSCRIPT

The REVERSAL TrialThe REVERSAL TrialReversing Atherosclerosis With Aggressive Lipid LoweringReversing Atherosclerosis With Aggressive Lipid Lowering

Atherosclerosis: A Progressive ProcessAtherosclerosis: A Progressive Process
Disease progression
PHASE I: Initiation PHASE II: Progression PHASE III: Complication
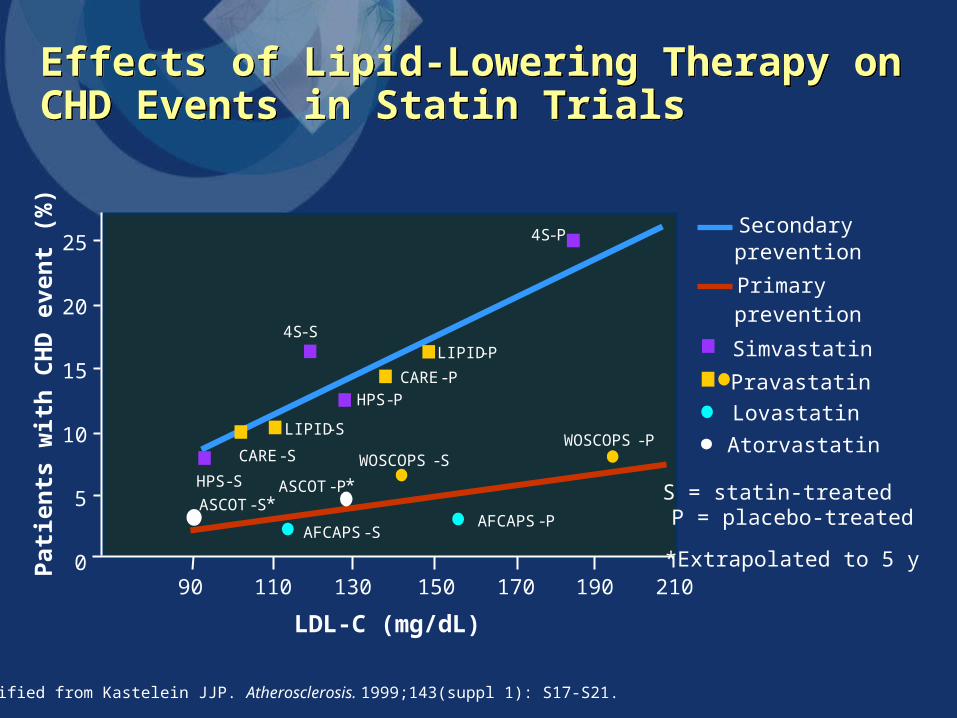
Effects of Lipid-Lowering Therapy on CHD Events in Statin TrialsEffects of Lipid-Lowering Therapy on CHD Events in Statin Trials
25
20
15
10
5
0
Pat
ien
ts w
ith
CH
D e
ven
t (%
)
90 110 130 150 170 190 210
S = statin-treated P = placebo-treated
*Extrapolated to 5 y
4S-P
CARE-P
LIPID-P4S-S
WOSCOPS-SWOSCOPS-P
AFCAPS-PAFCAPS-S
LIPID-S
CARE-S
Primary prevention
Simvastatin
Pravastatin
Lovastatin
Modified from Kastelein JJP. Atherosclerosis. 1999;143(suppl 1): S17-S21.
HPS-S
HPS-P
Atorvastatin
ASCOT-S*ASCOT-P*
Secondary prevention
LDL-C (mg/dL)

What Is REVERSAL?What Is REVERSAL?
• Multicenter, randomized, double-blind, active- controlled trial
• Comparing the effects of atorvastatin 80 mg/d with pravastatin 40 mg/d administered for 18 months
• Using IVUS to measure progression of atherosclerosis

Effects of Lipid Lowering With Statins on Progression of CHDEffects of Lipid Lowering With Statins on Progression of CHD
0
0.01
0.02
0.03
0.04
0.05
0.06
-40 -30 -20 -10 0 10
MARS
MAAS
CCAIT
PLAC I
REGRESS
LCAS
MARS MAAS
LCAS
CCAIT
PLAC I
LDL-C reduction (%)
Pro
gre
ssio
n (
ML
D d
ecre
ase)
, m
m/y
REGRESS
Drug Placebo

ScreeningScreeningvisit*visit*
Atorvastatin 80 mg/d
Pravastatin 40 mg/d
REVERSAL: Study DesignREVERSAL: Study Design
Design: Prospective, multicenter, randomized, double-blind trial
Setting: 34 community and tertiary-care hospitals in the USA
Double-blind period
18-month follow-up with IVUS*Includes baseline IVUS
PlaceboPlaceborun-inrun-inphasephase
Randomization
654 patients
REVERSAL: Study ObjectiveREVERSAL: Study Objective
To compare the effects of aggressive lipid-lowering therapy (atorvastatin 80 mg/d) vs moderate lipid-lowering therapy (pravastatin 40 mg/d)
on percent change in TAV using IVUS imaging of the coronary arteries in patients with CHD

REVERSAL: Why Was Pravastatin 40 mg Used?REVERSAL: Why Was Pravastatin 40 mg Used?
• REVERSAL is the first active-controlled, cholesterol- lowering, coronary atherosclerosis progression trial
• Previous large-scale trials used placebo as a comparator
• Pravastatin has an indication to slow progression of atherosclerosis based on angiographic studies
– PLAC I: 264 patients for 3 y vs placebo
– REGRESS: 885 patients for 2 y vs placebo
• 40 mg was the highest approved dose of pravastatin at the initiation of REVERSAL

REVERSAL: Patient PopulationREVERSAL: Patient Population
• Inclusion criteria:
– Patients requiring diagnostic coronary angiography for a clinical indication
– Aged 30-75 y
– LDL-C 3.2 mmol/L (125 mg/dL) but 5.4 mmol/L (210 mg/dL)
– TGs < 6.8 mmol/L (600 mg/dL)
• Angiographic inclusion criteria:
– Angiographic evidence of CHD defined as 1 lesion with 20% reduction in lumen diameter in any coronary artery
50% reduction in lumen diameter of the left main coronary artery
– The vessel undergoing IVUS evaluation (the “target” vessel) should have 50% stenosis throughout a segment of minimum length 30 mm

REVERSAL: Patient PopulationREVERSAL: Patient Population
• Exclusion criteria:
– Target vessel was considered suitable only if the artery had not undergone PTCA or CABG surgery
– Left ventricular ejection fraction of < 0.4
– Moderate or more severe CHF
– Clinically significant valvular heart disease
– Uncontrolled hypertension
– Second- or third-degree heart block
– Sustained ventricular tachyarrhythmia or an implantedcardiac defibrillator
– Known major hematologic, neoplastic, metabolic, gastrointestinal, or endocrine dysfunction
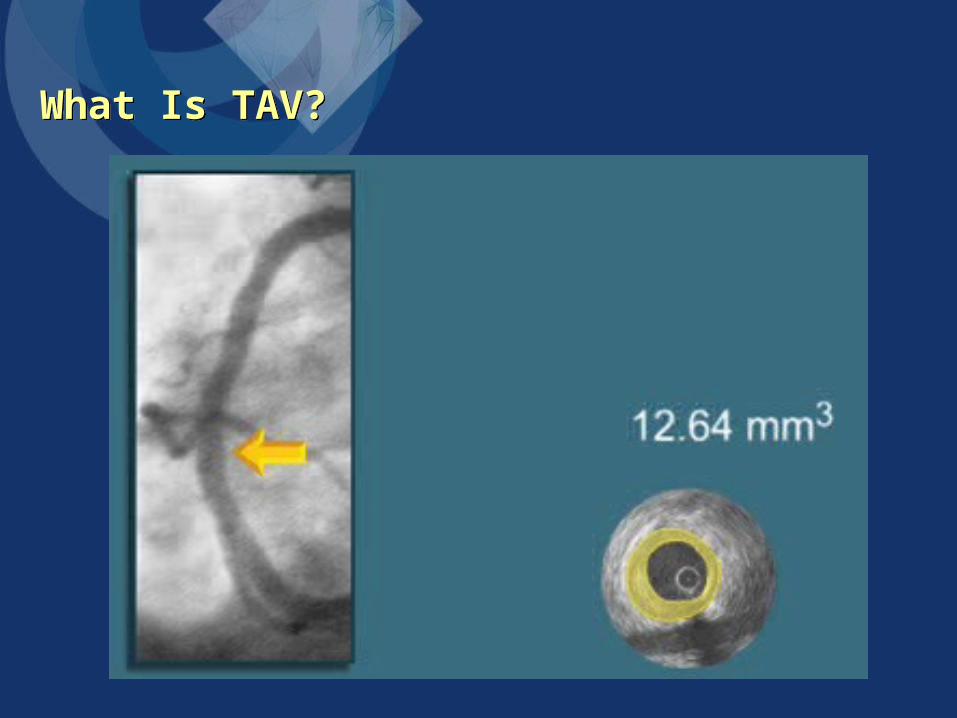
What Is TAV?What Is TAV?

REVERSAL: Primary Efficacy ParameterREVERSAL: Primary Efficacy Parameter
The percent change from baseline in TAV for all slices of anatomically comparable segments of the target coronary artery
as measured by IVUS

REVERSAL: Selected Secondary Efficacy Parameters REVERSAL: Selected Secondary Efficacy Parameters
• Nominal change from baseline in TAV
• Change from baseline in PAV
• Change from baseline in lipid parameters
• Change from baseline in CRP

Age* (y)
Male (%)
White (%)
BMI* (kg/m2)
Current smoker (%)
Diabetes (%)
Hypertension (%)
TC* (mmol/L [mg/dL])
LDL-C* (mmol/L [mg/dL])
TG* (mmol/L [mg/dL])
HDL-C* (mmol/L [mg/dL])
55.8 ± 9.8
71
90
30.5 ± 6.5
26
20
68
6.0 ± 0.9][231.8 ± 34.2]
3.9 ± 0.7 [150.2 ± 27.9]
2.2 ± 1.2 [197.2 ± 95.7]
1.1 ± 0.3 [42.3 ± 9.9]
Characteristic Atorvastatin 80 mg(n = 253)
REVERSAL: Baseline CharacteristicsREVERSAL: Baseline Characteristics
56.6±9.2
73
87
30.5±5.6
27
18
70
6.0 ± 0.9 [232.6 ± 34.1]
3.9 ± 0.7 [150.2 ± 25.9]
2.2 ± 1.1 [197.7 ± 105.6]
1.1 ± 0.3 [42.9 ± 11.4]
Pravastatin 40 mg(n = 249)
*Mean ± SD.

*P < 0.001 vs pravastatin.
Data are mean percent change from baseline to 18-month follow-up.
-40
-30
-20
-10
0
10
Atorvastatin
Change From Baseline in Lipid Parameters Change From Baseline in Lipid Parameters
-50
Ch
ang
e fr
om
bas
elin
e (%
)
TC LDL-C
-25.2
-18.4
5.6
-6.8
-46.3*
-34.1*
2.9
-20.0*
TGs HDL-C
Pravastatin

2.7*
Pravastatin
Significant atheroscleroticprogression from baseline
-0.4†
Atorvastatin
No significant change frombaseline; atheroscleroticprogression was stopped
Primary End Point: Percent Change in TAVPrimary End Point: Percent Change in TAVC
han
ge
in T
AV
(%
)
-1
0
1
2
3
*Progression vs baseline (P = 0.001); †No change vs baseline (P = 0.98).
P = 0.02
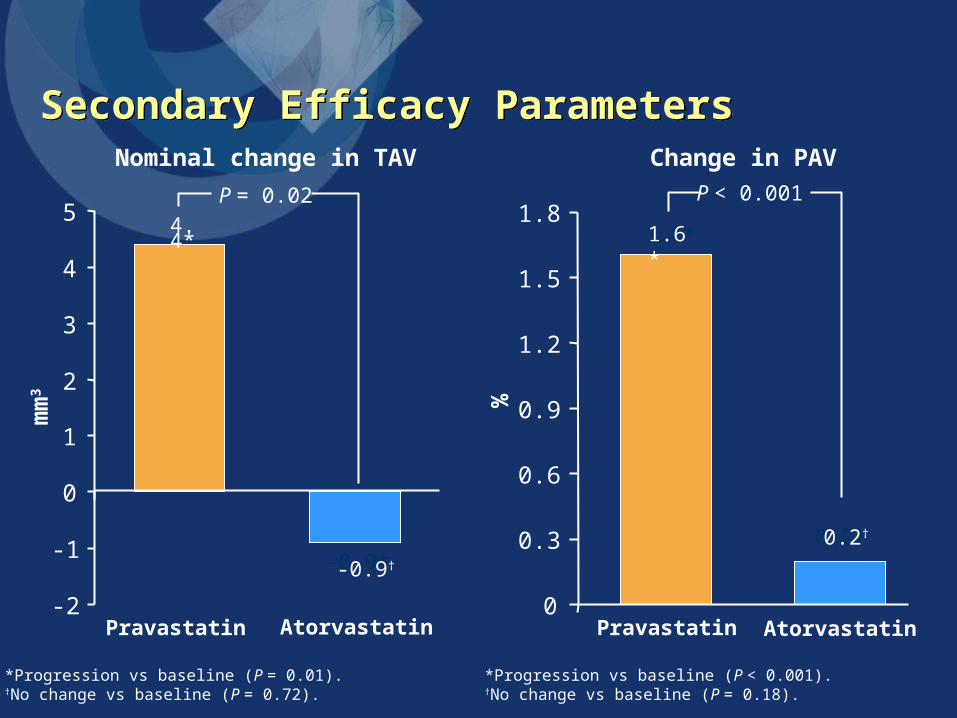
0.2†
Atorvastatin
1.6*
PravastatinAtorvastatin
4.4*
Pravastatin
Nominal change in TAV
*Progression vs baseline (P = 0.01).†No change vs baseline (P = 0.72).
0
0.3
0.6
0.9
1.2
1.5
1.8
*Progression vs baseline (P < 0.001).†No change vs baseline (P = 0.18).
Change in PAV
-2
-1
0
1
2
3
4
5
-0.9†
P = 0.02 P < 0.001
%
mm
3
Secondary Efficacy ParametersSecondary Efficacy Parameters
-0.9†
1.6*
0.2†
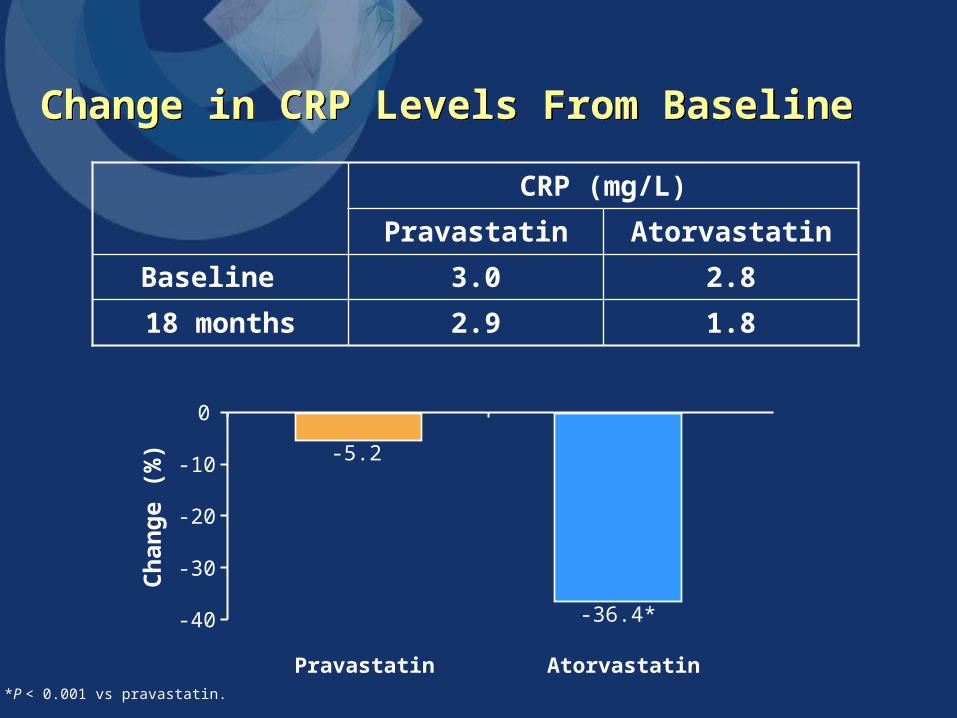
-36.4*
Atorvastatin
-5.2
Pravastatin
Change in CRP Levels From Baseline Change in CRP Levels From Baseline C
han
ge
(%)
*P < 0.001 vs pravastatin.
-40
-30
-20
-10
0
1.82.918 months
2.83.0Baseline
AtorvastatinPravastatin
CRP (mg/L)

*Regression vs baseline (P = 0.049). †Regression vs baseline (P < 0.001).
P = 0.01
-4.2†
-5
-4
-3
-2
-1
0
-1.2*
AtorvastatinPravastatin
mm
3Nominal Change in TAV for 10-mm Vessel Subsegment With Greatest Disease SeverityNominal Change in TAV for 10-mm Vessel Subsegment With Greatest Disease Severity
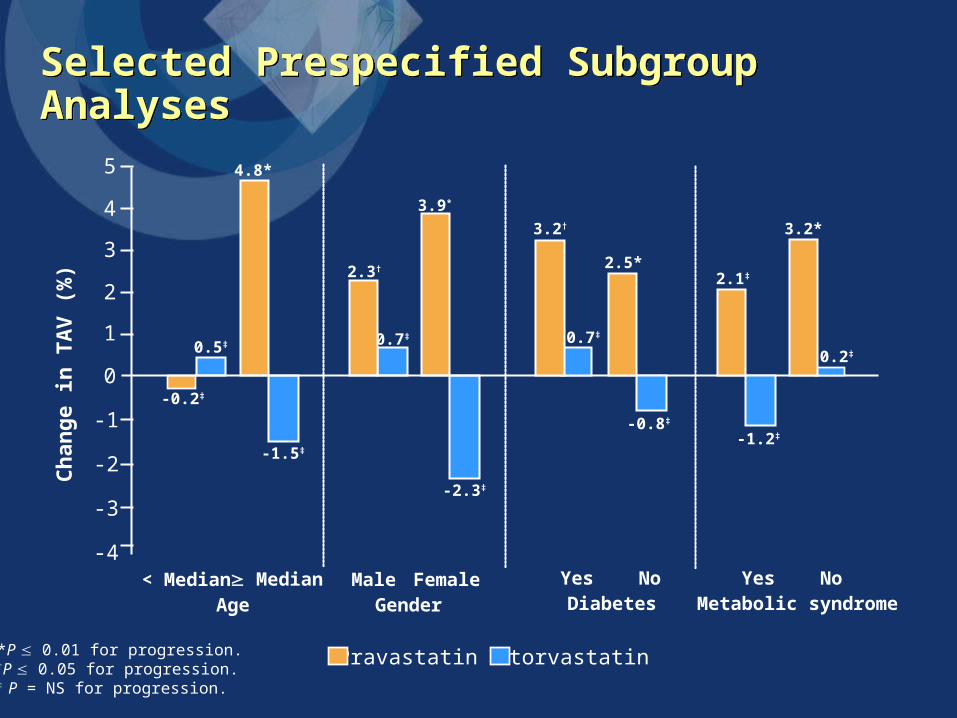
0.5‡
-1.5‡
0.7‡
-2.3‡
AtorvastatinPravastatin
< Median Median Male FemaleAge Gender
-0.2‡
4.8*
2.3†
3.9*
Ch
ang
e in
TA
V (
%)
*P 0.01 for progression.†P 0.05 for progression.‡ P = NS for progression.
Yes No Yes NoDiabetes Metabolic syndrome
0.7‡
-0.8‡
-1.2‡
0.2‡
3.2†
2.5*2.1‡
3.2*
0
1
2
3
4
5
-1
-2
-3
-4
Selected Prespecified Subgroup AnalysesSelected Prespecified Subgroup Analyses

Percent Change in TAV Among Patients Reaching NCEP ATP III GoalPercent Change in TAV Among Patients Reaching NCEP ATP III Goal
*Progression vs baseline (P = 0.01); †No change vs baseline (P = 0.93).
Significant atherosclerotic progression from baseline occurred even among pravastatin patients reaching NCEP ATP III goal
Ch
ang
e in
TA
V (
%)
Pravastatin
0
1
21.9*
3
-0.9†
Atorvastatin
-1
Subgroup reaching NCEP ATP III goal (< 2.59 mmol/L [100 mg/dL])161/249 (65%) pravastatin patients (mean LDL-C = 2.27 mmol/L [87.5 mg/dL])246/253 (97%) atorvastatin patients (mean LDL-C = 1.75 mmol/L [67.7 mg/dL])

Comparison of LDL-C Reduction and Change in Atheroma VolumeComparison of LDL-C Reduction and Change in Atheroma Volume
% change in LDL-C
20
15
10
5
0
-5
-10
-15Ch
ang
e in
ath
ero
ma
volu
me
(mm
3 )
-80 -70 -60 -50 -40 -30 -20 -10 0 10 20
Both treatment groups (n = 502)
Regardless of the agent used, an LDL-C reduction of at least 50% was required to halt progression
The dashed lines indicate upper and lower 95% CIs for the mean values.Nissen SE, et al. JAMA. 2004;291:1071-1080.

Comparison of LDL-C Reduction and Change in Atheroma VolumeComparison of LDL-C Reduction and Change in Atheroma Volume
20
Ch
ang
e i
n a
ther
om
a vo
lum
e (m
m3)
% change in LDL-C
15
10
5
0
-5
-15
-20
Pravastatin group (n = 249) Atorvastatin group (n = 253)
-80 -70 -60 -50 -40 -30 -20 -10 0 10 20 -80 -70 -60 -50 -40 -30 -20 -10 0 10 20
Patients receiving pravastatin who experienced LDL-C reductions > 50% continued to show disease progression
The progression rate at any level of LDL-C reduction was lower with atorvastatin than with pravastatin
The dashed lines indicate upper and lower 95% CIs for the mean values.Nissen SE, et al. JAMA. 2004;291:1071-1080.

Safety—AEsSafety—AEs
Pravastatin 40 mg (n = 327)
Atorvastatin 80 mg (n =
327)
1 (0.3%)1 (0.3%)Stroke, n (%)
2/316 (0.6%)2/311 (0.6%)AST > 3 ULN, n (%)
5/316 (1.6%)7/311 (2.3%)ALT > 3 ULN, n (%)
0/316 (0%)
7 (2.1%)
1 (0.3%)
0/311 (0%)CPK > 10 ULN, n (%)
Laboratory abnormality
4 (1.2%)MI, n (%)
1 (0.3%)Death (any cause), n (%)
Cardiovascular end point
• Rates of CV end points were similar between groups• Rates of liver- and muscle-enzyme abnormalities were low and similar between groups

Safety—Drug DiscontinuationsSafety—Drug Discontinuations
22 (6.7)21 (6.4)Drug discontinuation, n (%)
Pravastatin 40 mg (n = 327)
Atorvastatin 80 mg (n =
327)
2 (0.6)0 Cancer, n (%)
04 (1.2) ALT/AST < 3 ULN, n (%)
2 (0.6)0 Chest pain, n (%)
1 (0.6)
5 (1.5)
12 (3.4)
5 (1.5) Other, n (%)
3 (0.9) Abdominal complaint, n (%)
9 (2.8) Musculoskeletal complaint, n (%)

Summary and Conclusions Summary and Conclusions
• First large-scale trial to compare the impact of 2 statins on atherosclerotic disease progression by using IVUS, a more sensitive approach than QCA, to measure plaque burden
• There was no change in TAV in the atorvastatin 80-mg group, indicating that atorvastatin stopped the progression of atherosclerosis
• Atorvastatin significantly impacted LDL-C, TGs, and the biomarker CRP to a greater extent than did pravastatin
• The safety profile of atorvastatin 80 mg was comparable to that of pravastatin 40 mg
Treatment with atorvastatin stopped further progression of atherosclerosis
• LIPITOR (atorvastatin calcium) is indicated as an adjunct to diet to reduce elevated total cholesterol, LDL-cholesterol, apo B, and TG levels and to increase HDL-cholesterol in patients with primary hypercholesterolemia (heterozygous familial) or combined hyperlipidemia.
• In clinical trials, the most common adverse events were constipation,
flatulence, dyspepsia and abdominal pain, headache, nausea, myalgia, asthenia, diarrhea, insomnia.
• LIPITOR is contraindicated in patients with hypersensitivity to any component of this medication; in patients with active liver disease or unexplained persistent elevation of serum transaminases; myopathy; in women during pregnancy, in nursing mothers, and in women of child-bearing potential not using appropriate contraceptive measures.
• Liver function tests should be performed before the initiation of treatment, at 6 and 12 weeks after initiation of therapy or elevation in dose, and periodically thereafter. LIPITOR should be used with caution in patients who consume substantial quantities of alcohol and/or have a history of liver disease. LIPITOR therapy should be discontinued if markedly elevated CPK levels occur or myopathy is diagnosed or suspected.

0
פתח תקוה 7063, ת.ד. 8 בית ניאופרם, רח' השילוח ניאופרם בע"מ49170,
-E, 03 9373716, פקס.03 9373737 טל-mail:[email protected]
LIPITOR is available in 10-mg, 20-mg, 40-mg, and 80-mg film-coated tablets, administered once daily.
For further information please see prescribing information.
•Lip01FE05