the relationship between social capital and depression during the transition to adulthood
TRANSCRIPT

The relationship between social capital and depression during thetransition to adulthoodajpy_4 26..35
Meredith O’Connor,1 Mary T. Hawkins,1 John W. Toumbourou,2 Ann Sanson,1 Primrose Letcher,1 andCraig A. Olsson3
1Department of Paediatrics, The University of Melbourne, 2School of Psychology, Deakin University, Melbourne, and3Murdoch Childrens Research Institute, Royal Children’s Hospital, and the University of Melbourne (PsychologicalSciences & Paediatrics), Parkville, Victoria, Australia
Abstract
Relatively high levels of depression are observed during the transition to adulthood. Hence, it is important to identify the factorsthat can reduce the incidence of depression at this time. Social capital is theorised to protect against depression by providinggreater access to support and psychological resources. Social capital incorporates both interpersonal relationships and broadercommunity-level factors. However, most research has focused on the influence of relationships with parents and peers in thedevelopment of depression in young people, with little attention given to the role of broader social capital factors relating toperceptions of and engagement with the wider community. Drawing on longitudinal data from the Australian TemperamentProject (ATP), this article examines the effects of close interpersonal relationships (with parents and peers) and broader,community-level aspects of social capital (trust and civic engagement) on depression during the transition to adulthood. Usinghierarchical multiple regression, alienation from peers was found to predict higher depression, whereas good communication withpeers was associated with a reduction of depressive symptoms. After controlling for the effects of close interpersonal relationships,trust in authorities and organisations made a significant contribution to the prediction of lower depression. Implications forintervention are discussed.
Key words: civic engagement, depression, emerging adulthood, political trust, social capital, social trust
Depression over the transition to adulthood is relatively
common, with a 1-month prevalence of around 20%
(Smart & Sanson, 2005), and a range of biological and
social risk factors have been identified (Badcock et al.,
2011; van Eekelen et al., 2011; Garber, 2006). Depression
is associated with impaired functioning across multiple
domains, including interpersonal relationships (Tanner
et al., 2007), work productivity, and educational outcomes
(Wittchen, Nelson, & Lachner, 1998), romantic involve-
ment and life satisfaction (Paradis, Reinherz, Giaconia, &
Fitzmaurice, 2006), and self-esteem (Reinherz, Giaconia,
Carmola Hauf, Wasserman, & Silverman, 1999). These
deficits occur at a time when young people are making
significant decisions about their educational, occupational,
and romantic lives which have lasting implications as they
move into adulthood (Arnett, 2000). Hence, it is important
to identify factors that reduce the incidence of depression
during this time.
Social capital may be one such protective factor. In general
terms, social capital refers to the networks of social ties
between individuals in a community (Portes, 1998; Putnam,
1995a). These ties are assumed to provide benefits at both the
individual and collective levels when the relationships that
make up these networks are reciprocal, trusting, and involve
positive emotions (Paxton, 1999). Generalised trust of others
in the community, and trust in institutions and organisations
are important aspects of social capital (Paxton, 1999; Putnam,
1995b). Civic engagement is also considered central to social
capital, and is often operationalised as involvement in volun-
tary organisations and volunteer work, both of which facili-
tate the development of social networks (Jennings & Stoker,
2004). Social capital can be conceptualised and measured at
both an individual and a group level (Brehm & Rahn, 1997),
with psychological research tending to focus on the former
and sociological research focusing on aggregate social capital.
Social capital incorporates both close interpersonal relation-
ships, or ‘proximal’ factors, as well as connections with the
broader community, or ‘distal’ factors (Bassani, 2007). It is
thought to reduce the incidence of depression through a
Correspondence: Meredith O’Connor, Dr, Department of Paediat-rics, The University of Melbourne, Royal Children’s Hospital, Flem-ington Road, Parkville, VIC 3052, Australia. Email: [email protected]
Received 2 June 2010. Accepted for publication 16 July 2010.© 2011 The Australian Psychological Society
Australian Journal of Psychology 2011; 63: 26–35doi:10.1111/j.1742-9536.2011.00004.x

number of pathways; for example, by increasing individuals’
exposure to positive emotional support, enhancing psycho-
logical resources such as self esteem, and buffering the nega-
tive effects of stressful life events (Phongsavan, Chey,
Bauman, Brooks, & Silove, 2006).
Investigations into the relationship between social capital
and depression over adolescence and the transition to adult-
hood have generally focused on the role of proximal rela-
tionships with peers and family members, with strong
empirical support found for the importance of these relation-
ships (for a review, see Campas, Hinden, & Gerhardt, 1995).
For example, Costello, Swendsen, Rose, and Dierker (2008)
recently examined trajectories of depression over adoles-
cence and early adulthood in a large US sample, and found
that strong connections with parents and peers predicted
membership in a non-depressed trajectory group.
In contrast, much less attention has been given to distal
aspects of social capital, such as social trust (or generalised
trust of others in the community), trust in institutions, and
civic engagement (Almedom, 2005; De Silva, McKenzie,
Harpham, & Huttly, 2005). Yet these aspects of social capital,
which relate to perceptions of and connections to the
broader community, are also likely to be important for
depression. For example, Erikson (1965) argued that under-
standing one’s roles and connections to the broader commu-
nity is important for healthy psychosocial development.
Furthermore, distal aspects of social capital are relatively
malleable (Jennings & Stoker, 2004) and hence represent
good targets for intervention. Broadly speaking, distal social
capital factors can be promoted through structural social
resources (i.e., characteristics of group members), and func-
tional social resources (i.e., the qualities of social interactions
within groups) (Bassani, 2007).
Of these distal aspects of social capital, civic engagement
has received the most attention as a potential protective
factor for depression. It has been suggested that civic engage-
ment, most often operationalised behaviourally as participa-
tion in extracurricular activities such as volunteering or
sports clubs and examined in adolescence, contributes to
healthy psychosocial functioning by providing young people
with the opportunity to build interpersonal competence,
feelings, of belonging, and strong relationships with their
school and peers (Mahoney, Cairns, & Farmer, 2003). Some
empirical support for this hypothesis has been found. For
example, Fredricks and Eccles (2006) found that, controlling
for achievement motivation levels, participation in sports
groups in year 11 concurrently predicted lower depression
and internalising problems, although involvement in school
clubs or prosocial activities did not.
However, some cross-sectional studies suggest that partici-
pation in groups may be related to higher depression. Using
cluster analysis, Zarrett et al. (2009) drew on data from the
4-H study when participants were in grades 5 through 7 and
identified six clusters with different patterns of group par-
ticipation. The clusters of highly engaged youths, and youths
who were involved in performing arts but not in sporting
activities, had the highest levels of depression. The authors
suggested that the effect for the highly engaged youths may
reflect the negative consequences of ‘overscheduling’, such
as time management issues and parental pressure. In con-
trast, engagement in sports and religious activities, and in
sports only, predicted significantly lower levels of depression,
consistent with Fredricks and Eccles’ (2006) findings. Others
have found no relationship between depression and civic
engagement. For example, Pancer, Pratt, and Hunsberger
(2007) also used cluster analysis with a Canadian sample of
students in their final year of high school and identified four
groups: activists (who had wide ranging involvement in
political and community activities), helpers (who were
involved in helping individuals from their communities but
not in political activities), responders (who responded to but
did not initiate helping or political activities), and unin-
volved adolescents. The four groups did not significantly
differ in their levels of depression. Hence, the role of civic
engagement in the course of depression remains unclear.
There are also some indications that subjective experi-
ences of social trust may be related to lower depression.
Sucoff and Aneshensel (1996) drew on a US sample of ado-
lescents (12–17 years), and examined two aspects of subjec-
tive social capital, including perceptions of ‘ambient hazards’
(e.g., violent crimes, drive-by shootings), which might be
taken as the negative pole of social trust, and social cohesion
(e.g., perceiving people in the neighbourhood as friendly).
The sample was confined to Los Angeles County, where
neighbourhoods were highly stratified by socioeconomic
status and ethnicity. They found that, controlling for actual
neighbourhood characteristics, perceptions of ambient
hazards concurrently predicted higher depression, and per-
ceptions of social cohesion in the community predicted
lower depression.
In a study of the relationship between social trust and
depression in adulthood, Fujiwara and Kawachi (2008) drew
on data from a US twin sample of adults aged 25–75, and
found that higher levels of perceived social capital (including
social trust and sense of belonging) were related to a reduced
risk of developing depression during a 2–3-year assessment
interval (using participants’ retrospective reports of depres-
sive symptoms over this period). In contrast, behavioural
aspects of social capital, including volunteer work, were not
associated with depression over this period. Veenstra’s
(2005) Canadian study found similar results, with trust in
community members and political trust predicting lower
levels of depressive symptoms in adults, whereas volunteer-
ing did not.
A number of large cross-sectional studies have examined
the relationship of trust to general psychopathology rather
Social capital and depression 27
© 2011 The Australian Psychological Society

than specifically focusing on depression. McCullock (2001)
found that high perceived social capital (measured by items
relating to the participant’s neighbourhood) was related to
lower psychiatric morbidity for British adults. Ellaway,
Macintyre, and Kearns (2001), in a Scottish study, found
that perceived social cohesion in the neighbourhood was
positively related to mental health. Phongsavan et al. (2006)
sampled participants aged 16 and over (age range not
reported) living in Australia, and assessed community par-
ticipation, feelings of trust and safety, and neighbourhood
connections and reciprocity, and their relationships with
psychological distress. After controlling for demographic and
health related factors, lower trust, fewer neighbourhood
connections, and lower reciprocity predicted membership in
the high distress group. Moreover, in a large Swedish study
of adults aged 18–80, low social trust was found to predict
poorer psychological health even when social participation
was high (Lindstrom, 2004). However, the focus on general
psychopathology in these studies limits the inferences that
can be drawn in relation to depression.
THE CURRENT STUDY
The Australian Temperament Project (ATP) is a large-scale
longitudinal community-based study, which has followed
the development of a cohort of Australian children from
infancy to early adulthood. The current study draws on data
from the ATP to examine the effects of proximal and distal
aspects of social capital on depression during the transition
to adulthood. Proximal social capital factors are operationa-
lised as attachment to peers and parents, and distal social
capital are operationalised as social trust and tolerance of
diversity, trust in authorities and organisations, and civic
action and engagement.
We employ a hierarchical design whereby the unique
effects of distal social capital can be examined, controlling
for their shared variance with proximal social capital
factors. Whereas previous research has typically employed
ad hoc measures of distal social capital developed by ‘ret-
rofitting’ the social capital concept to items available in
large questionnaire studies (Almedom, 2005), we employ
well-validated and empirically tested measures. Further-
more, the current study specifically addresses depression,
rather than general psychological distress, thus aiding
interpretability of the findings and refining possible impli-
cations for intervention.
Based on the tenets of social capital theory, we hypoth-
esise that, as in previous literature, strong relationships with
parents and peers in adolescence will significantly reduce
depression in early adulthood. Furthermore, we hypothesise
that the distal social capital factors of trust in authorities and
organisations, as well as general trust of others in the com-
munity and tolerance of diversity, will also make a unique
contribution to reduced risk for depression. The analysis will
also seek to clarify the role of civic engagement as an aspect
of distal social capital, with an expectation of it having a
protective role on depression. We further hypothesise that
social capital will be particularly important for individuals
who experienced high levels of depressive symptoms in ado-
lescence and thus were at an increased risk for depression
during the transition to adulthood.
METHOD
Participants and procedure
Participants were young people enrolled in the ATP, a lon-
gitudinal study following the psychosocial development of a
community sample from infancy to adulthood. A represen-
tative sample of 2,443 infants was recruited through selected
Maternal and Child Health Centres across both urban and
rural areas in Victoria during a specified 2-week period in
1983. Using a mail survey methodology, 14 waves of data
have been collected over the past 25 years from parents,
primary school teachers, maternal and child health nurses,
and from the age of 11 onwards, the young people them-
selves (for further information, see Prior, Sanson, Smart, &
Oberklaid, 2000).
The current sample consisted of the 991 participants,
including 384 males and 607 females, who participated in
the 2006 wave and thus had data on depression at 23–24
years. Questionnaire booklets were mailed to participants,
together with reply-paid, addressed envelopes in which to
return them. One round of postal reminders was under-
taken, and was followed by a second mail-out of question-
naires to non-respondents. Finally, a round of telephone
reminders was undertaken. Missing data on antecedent vari-
ables ranged from 0% to 11.3%, with an average of 8.55%,
and was estimated using the Expectation Maximisation algo-
rithm (Enders, 2006).
Approximately two-thirds of the cohort is still enrolled in
the study after 23 years. Table 1 shows characteristics of the
retained sample at the 14th data collection wave as compared
with the original sample upon recruitment, and demonstrates
that proportionately more families from a lower socioeco-
nomic status (SES)-background, and families with parents
who were not born in Australia, have been lost to the study.
Statistical comparisons of the retained and non-retained sub-
samples confirmed these sociodemographic differences and
also indicated that the retained subgroup of children was
significantly ‘easier’ in temperament style in infancy than
non-retained subgroup (t(2441) = -2.63, p = .01), although
this difference was very small in magnitude (retained sub-
group M = 1.71, SD = 0.68; non-retained subgroup M = 1.75,
SD = 0.71). However, there were no significant differences
28 M. O’Connor et al.
© 2011 The Australian Psychological Society

between the retained and non-retained subgroups on behav-
ioural problems during infancy (t(2432) = -1.25, p = .21, ns).
The sample continues to include young adults with a broad
range of attributes and from diverse circumstances, although
it contains fewer families experiencing socioeconomic disad-
vantage than at the commencement of the study and hence is
likely to slightly underestimate the effect of family socio-
economic disadvantage.
Materials
Depression was measured at 13–14 and 15–16 years using the
Short Mood and Feelings Questionnaire (Angold et al.,
1995), which includes 12 items (e.g. ‘I don’t enjoy anything
at all) rated on a 3-point scale from ‘rarely or never’ to ‘very
often’. Internal reliability was high at both 13–14 (a = 0.80)
and 15–16 years (a = 0.85), and depression was highly cor-
related across these two time points r = 0.61 (p < .001).
Hence, in order to provide a more robust measure tapping
persistent problems with depression, a composite score was
created from self-reported depression at 13–14 and 15–16
years by standardising and averaging the two scores. Depres-
sion during the transition to adulthood (at 23–24 years) was
measured with the depression subscale of the Depression
Anxiety Stress Scales (Lovibond & Lovibond, 1995). This
measure included seven items relating to depressive symp-
toms, such as ‘I couldn’t seem to experience any positive
feelings’ (a = 0.90). Items were rated on a 4-point scale
ranging from ‘did not apply’ to ‘applied very much/most of
the time’ over the past month.
Proximal social capital at 17–18 years was assessed via self-
report measures of relationships with parents and peers using
subscales of the Inventory of Parent and Peer Attachment
(Armsden & Greenberg, 1987). Aspects of the parent–
adolescent relationship measured were: trust (eight items,
e.g., ‘Considers my point of view when we discuss things’;
a = 0.86), communication (seven items, e.g., ‘Senses when
I’m upset about something’; a = 0.89), and alienation (four
items, e.g., ‘Doesn’t understand me’; a = 0.75). Parallel mea-
sures of peer relationships were used, including: trust (four
items, e.g., ‘My friends accept me as I am’; a = 0.84), com-
munication (four items, e.g., ‘My friends sense when I’m
upset about something’; a = 0.70), and alienation (four
items, e.g., ‘My friends don’t understand what I’m going
through these days’; a = 0.64). Ratings were made on a
4-point scale from ‘always/almost always’ to ‘never/almost
never’.
Distal social capital factors were assessed by three measures
developed by Hawkins, Letcher, Sanson, Smart, and Toum-
bourou (2009) using AMOS 7.0 SEM confirmatory factor
analysis (SPSS Inc., Chicago, IL; Arbuckle & Wothke, 2006)
as part of a larger model of positive adaptation. These three
measures included trust and tolerance of others, trust in
authorities and organisations, and civic action and engage-
ment, all assessed by self-report at 19–20 years. The mea-
surement models of each of these constructs fit the data
very well, and all indicators contributed meaningfully to
their respective latent constructs. The overall model pro-
vided a very good fit for the data (RMSEA = 0.05,
CFI = 0.94). Using model-based imputation in AMOS on
the final model, latent factor scores were computed for each
of the first-order constructs (including trust and tolerance
of others, trust in authorities and organisations, and civic
action and engagement). The components of these scores
are described below.
Three items derived from Stone and Hughes (2002) relat-
ing to trust in people in the neighbourhood, trust in Austra-
lians, and tolerance of different ethnic groups were used to
assess trust and tolerance of others. These were ‘Most people in
your neighbourhood can be trusted’, ‘Having people from
different ethnic and cultural backgrounds makes Australia a
better place’, and ‘Thinking about Australia, most people can
be trusted’. These three items were rated on a 5-point scale
from ‘disagree completely’ to ‘agree completely’.
Trust in authorities and organisations was measured by items
derived from Flanagan and Longmire (1995) and Stone and
Hughes (2002) tapping participants’ confidence in police
(five items, a = 0.83, e.g., ‘How much confidence do you
have in the police to treat everyone fairly’ rated on a scale
where 1 = a great deal, 2 = some, 3 = little, and 4 = none at
all), confidence in the courts (five items, a = 0.87, e.g., ‘How
much confidence do you have in the ability of the courts to
impose fair sentences’ rated on a scale where 1 = a great
deal, 2 = some, 3 = little, and 4 = none at all), and trust in
organisations (eight items, a = 0.83, e.g., ‘the media’ rated
according to how confident the participant is that the organi-
sation can be relied on to act in a fair or reasonable manner,
Table 1 Comparison of retained sample and original cohort oncharacteristics at recruitment in 1983
Domain Original cohort Retained 2006
SES Quartile in 1983Highest 26.7% 32.1%Medium-high 29.2% 30.3%Medium-low 24.4% 23.5%Lowest 19.8% 14.2%
Mother’s country of birthAustralian 79.9% 83.9%UK 6.0% 5.6%Other 14.1% 10.6%
Father’s country of birthAustralian 73.3% 77.1%UK 7.3% 6.9%Other 19.4% 16.0%
Infant behaviour problems Mean 1.73 (SD 0.69) 1.71 (SD 0.68)Infant easy-difficult
temperament factorMean 2.46 (SD 0.63) 2.43 (SD 0.63)
Social capital and depression 29
© 2011 The Australian Psychological Society

with ratings made on a scale from 1 = not at all confident to
4 = very confident).
Civic action and engagement was measured by items derived
from Stone (2001) and Stone and Hughes (2002) tapping
participation in community activities, participation in
groups, and donations to groups, over the past year. Partici-
pation in community activities was measured according to
10 items asking participants to indicate how often they had
participated in certain activities over the past year. For
example, ‘In the past 12 months have you attended a public
meeting’ rated on a scale where 1 = not at all, 2 = 1–2 times,
3 = 3–4 times, and 4 = five times or more (a = 0.58). Partici-
pation in groups was measured according to nine items
asking participants to indicate whether they ‘participated,
attended events or meetings’ for nine groups such as ‘sport-
ing, recreation, or hobby groups’ and ‘self-help or support
group’ (rated according to yes or no response and scaled to
indicate ‘yes’; a = 0.65). Donations to groups were measured
according to whether participants ‘donated money, time,
etc.’ to the same nine community groups (rated according to
yes or no response and scaled to indicate ‘yes’; a = 0.60).
RESULTS
Descriptive statistics and intercorrelations between variables
examined in the study are presented in Table 2. Correlations
were generally small to moderate, with the strongest asso-
ciations observed between depression at the two time points,
and variables within the domains of relationships with peers,
relationships with parents, and distal social capital factors.
A hierarchical multiple regression analysis was performed
with depression at 23–24 years as the dependent variable.
Gender and adolescent depression were entered in the first
step to control for their effects, as both have been associated
with early adult depression in previous research (Piccinelli &
Wilkinson, 2000; Simons, Rohde, Kennard, & Robins, 2005).
Given its relationship to social capital (Lin, 1982), family
socioeconomic status was also initially included as a control
but had no significant effects, and hence was removed from
the model. Proximal social capital variables (i.e., parent and
peer relationships) were entered in the second step, and
distal social capital variables (trust and tolerance of others,
trust in authorities and organisations, and civic action and
engagement) were entered in the third step. The fourth step
contained interaction terms reflecting peer and parent rela-
tionship predictors by adolescent depression. The fifth, final
step included interaction terms between adolescent depres-
sion and broader social capital factors. All variables were
centred prior to the analysis in order to reduce multicol-
linearity and aid interpretation of interaction effects
(Tabachnick & Fidell, 2001).
The final model (see Table 3) accounted for a significant
16.90% of the variance in depression at 23–24 years (F(20,
970) = 9.85, p < .001). In the first step, female gender and
adolescent depression emerged as significant antecedents of
depression in early adulthood, explaining 12% of the vari-
ance (Fchange(2,988) = 65.01, p < .001). Adolescent depres-
sion remained a significant predictor in each of the
subsequent steps. Close relationship variables were entered
in the second step and contributed an additional 3% to the
variance accounted for (Fchange(6,982) = 5.01, p < .001). Peer
alienation emerged as a significant antecedent of higher
levels of depression in early adulthood and remained signifi-
cant in subsequent steps. The distal social capital factors
entered in the third step contributed a modest but significant
1% to the proportion of variance accounted for (Fchange
(3, 979) = 4.93, p = .002); trust in authorities and organisa-
tions emerged as a significant predictor, with higher levels
of trust predicting lower depression, and this remained
Table 2 Descriptive statistics and intercorrelations between depression and social capital variables
Variable 1 2 3 4 5 6 7 8 9 10 11
1. Early adulthood depression – 0.33** -0.17** -0.15** 0.25** -0.16** -0.18** 0.21** -0.16** -0.20** -0.022. Adolescent depression – -0.24** -0.06 0.39** -0.22** -0.30** 0.36** -0.17** -0.22** 0.003. Peer trust – 0.41** -0.45** 0.15** 0.20** -0.15** 0.15** 0.16** 0.044. Peer communication – -0.35** 0.29** 0.13** -0.07* 0.13** 0.14** 0.065. Peer alienation – -0.18** -0.22** 0.39** -0.05 -0.13** 0.026. Warmth/communication with mother – 0.70** -0.58** 0.17** 0.20** 0.11**7. Trust with mother – -0.61** 0.17** 0.22** 0.058. Alienation from mother – -0.08* -0.18** 0.029. Trust and tolerance of others – 0.49** 0.30**
10. Trust in authorities and organisations – 0.14**11. Civic action and engagement –
Mean 0.47 0.00 3.03 2.94 1.79 2.97 3.35 2.10 0.02 0.01 0.02Standard deviation 0.53 0.91 0.28 0.64 0.49 0.61 0.44 0.56 0.34 0.23 0.40Minimum 0 -1.34 1.75 1 1 1 1 1 -1.29 -0.83 -0.58Maximum 3 3.49 4 4 3.50 4 4 4 0.91 0.66 2.14
*p < .05, **p < .01.
30 M. O’Connor et al.
© 2011 The Australian Psychological Society
significant in subsequent steps. In the fourth step, the inter-
actions between adolescent depression and peer and parent
relationship variables contributed a modest but significant
1% to the variance accounted for (Fchange(6,973) = 2.55,
p = .02). A significant interaction was observed between
adolescent depression and peer communication. When
interactions between adolescent depression and distal social
capital factors were entered in the fifth step, the change in
the proportion of variance accounted for was non-significant
(Fchange(3,970) = 0.18, p = .91, ns), and hence this step was
removed from the analysis.
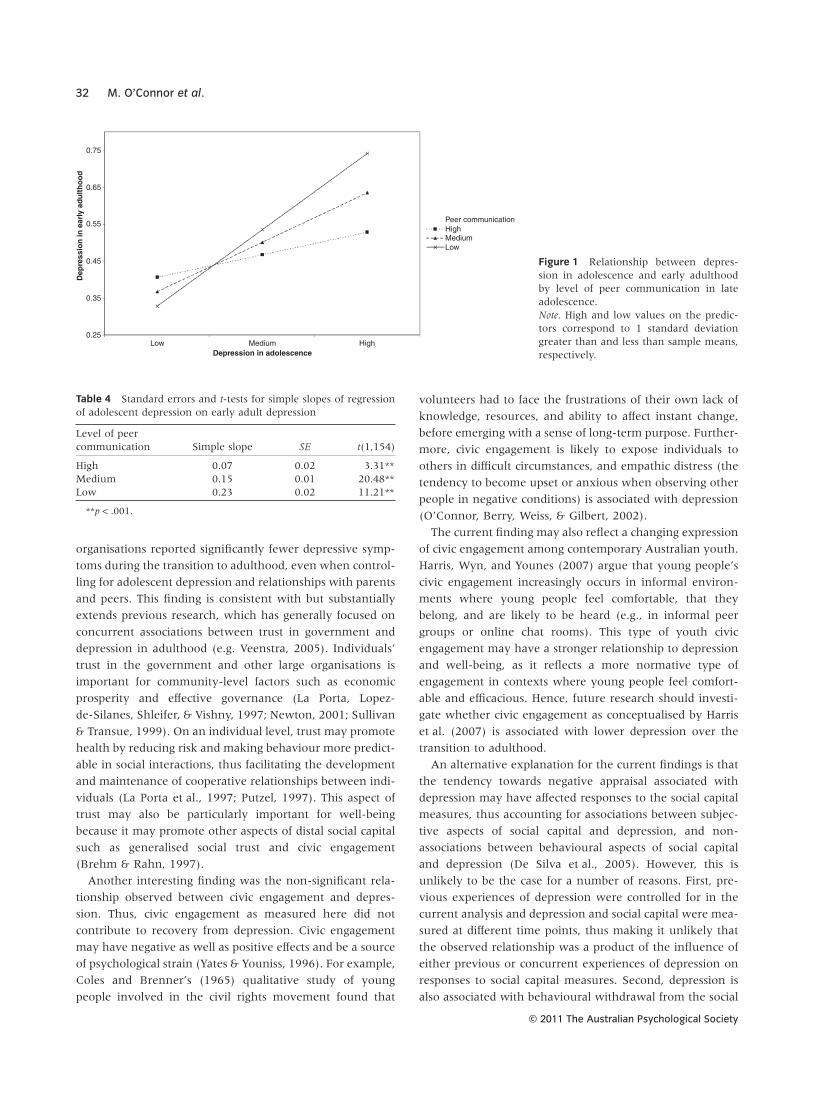
The nature of the significant adolescent depression by peer
communication interaction was probed further. The results
were plotted using ModGraph (Jose, 2008) and are pre-
sented in Fig. 1. The simple slopes (see Table 4) were signifi-
cantly different from zero at low, medium, and high levels
of peer communication. As can be seen from Fig. 1, those
with high adolescent depression and low peer communica-
tion had the highest levels of adult depression, whereas at
low levels of adolescent depression, peer communication
appeared to have less effect on adult depression. Hence,
higher levels of peer communication appeared to have a
stronger protective effect for those who were higher in ado-
lescent depression.
DISCUSSION
The current study examined the protective effects of both
proximal and distal social capital factors on depression
during the transition to adulthood. Depression over adoles-
cence and early adulthood showed high continuity, with
depression in adolescence emerging as the strongest predic-
tor of later depression. As expected, relationships with peers
during adolescence were also relevant to later depression.
Independently of proximal social capital and experiences of
depression in adolescence, trust in authorities and organisa-
tions further predicted lower levels of depression. Hence,
aspects of both proximal and distal social capital were asso-
ciated with reduced depression during the transition to
adulthood.
Consistent with a large body of previous research
(Campas et al., 1995), peer relationships in adolescence
were significantly related to depressive symptoms during
the transition to adulthood. Those adolescents who were
alienated from their peers, or had experienced previous
depressive symptoms and had poor communication with
their peers, were particularly at risk for later depression.
The salience of peer relationships in adolescence as com-
pared to relationships with parents, which did not signifi-
cantly predict later depression in the current study, was also
evident and is consistent with previous findings, suggesting
that peer attachment during adolescence may be relatively
more influential for depression than parent attachment
(e.g., Laible, Carlo, & Raffaelli, 2000). The results further
demonstrate—again replicating a large body of research
(e.g. Simons et al., 2005)—the considerable risk posed by
experiences of adolescent depression for later depression
during the transition to adulthood.
Unique to the current study is the finding that
young people who were more trusting of authorities and
Table 3 Hierarchical linear regression predicting depression inearly adulthood from adolescent depression and social capital factors
Variable B SE B b
Step 1Gender -0.09 0.03 -0.08**Adolescent depression 0.21 0.02 0.35**
Step 2Gender -0.05 0.04 -0.05Adolescent depression 0.16 0.02 0.27**Peer trust -0.03 0.07 -0.01Peer communication -0.05 0.03 -0.06Peer alienation 0.11 0.04 0.10**Parent trust -0.05 0.05 -0.04Parent communication 0.01 0.04 0.01Parent alienation 0.05 0.04 0.05
Step 3Gender -0.02 0.04 -0.02Adolescent depression 0.14 0.02 0.24**Peer trust -0.01 0.07 -0.01Peer communication -0.05 0.03 -0.06Peer alienation 0.11 0.04 0.10**Parent trust -0.03 0.05 -0.02Parent communication 0.01 0.04 0.01Parent alienation 0.05 0.04 0.05Trust and tolerance of others -0.10 0.06 -0.06Trust in authorities and organisations -0.19 0.08 -0.08*Civic action and engagement 0.02 0.04 0.02
Step 4Gender -0.04 0.04 -0.03Adolescent depression 0.15 0.02 0.25**Peer trust 0.00 0.07 0.00Peer communication -0.05 0.03 -0.06Peer alienation 0.10 0.04 0.09*Parent trust -0.03 0.06 -0.03Parent communication 0.00 0.04 0.00Parent alienation 0.06 0.04 0.06Trust and tolerance of others -0.11 0.06 -0.07Trust in authorities and organisations -0.17 0.08 -0.07*Civic action and engagement 0.03 0.04 0.02Peer trust ¥ adolescent depression 0.07 0.07 0.04Peer communication ¥ adolescent
depression-0.13 0.04 -0.14**
Peer alienation ¥ adolescentdepression
-0.01 0.04 -0.01
Parent trust ¥ adolescent depression 0.01 0.06 0.01Parent communication ¥ adolescent
depression0.04 0.04 0.05
Parent alienation ¥ adolescentdepression
0.01 0.05 0.02
R2 = 0.12 for Step 1 (p < .001); DR2 = 0.03 for Step 2 (p < .001);DR2 = 0.01 for Step 3 (p = .002); DR2 = 0.01 for Step 4 (p = .02).
*p < .05, **p < .01.
Social capital and depression 31
© 2011 The Australian Psychological Society
organisations reported significantly fewer depressive symp-
toms during the transition to adulthood, even when control-
ling for adolescent depression and relationships with parents
and peers. This finding is consistent with but substantially
extends previous research, which has generally focused on
concurrent associations between trust in government and
depression in adulthood (e.g. Veenstra, 2005). Individuals’
trust in the government and other large organisations is
important for community-level factors such as economic
prosperity and effective governance (La Porta, Lopez-
de-Silanes, Shleifer, & Vishny, 1997; Newton, 2001; Sullivan
& Transue, 1999). On an individual level, trust may promote
health by reducing risk and making behaviour more predict-
able in social interactions, thus facilitating the development
and maintenance of cooperative relationships between indi-
viduals (La Porta et al., 1997; Putzel, 1997). This aspect of
trust may also be particularly important for well-being
because it may promote other aspects of distal social capital
such as generalised social trust and civic engagement
(Brehm & Rahn, 1997).
Another interesting finding was the non-significant rela-
tionship observed between civic engagement and depres-
sion. Thus, civic engagement as measured here did not
contribute to recovery from depression. Civic engagement
may have negative as well as positive effects and be a source
of psychological strain (Yates & Youniss, 1996). For example,
Coles and Brenner’s (1965) qualitative study of young
people involved in the civil rights movement found that
volunteers had to face the frustrations of their own lack of
knowledge, resources, and ability to affect instant change,
before emerging with a sense of long-term purpose. Further-
more, civic engagement is likely to expose individuals to
others in difficult circumstances, and empathic distress (the
tendency to become upset or anxious when observing other
people in negative conditions) is associated with depression
(O’Connor, Berry, Weiss, & Gilbert, 2002).
The current finding may also reflect a changing expression
of civic engagement among contemporary Australian youth.
Harris, Wyn, and Younes (2007) argue that young people’s
civic engagement increasingly occurs in informal environ-
ments where young people feel comfortable, that they
belong, and are likely to be heard (e.g., in informal peer
groups or online chat rooms). This type of youth civic
engagement may have a stronger relationship to depression
and well-being, as it reflects a more normative type of
engagement in contexts where young people feel comfort-
able and efficacious. Hence, future research should investi-
gate whether civic engagement as conceptualised by Harris
et al. (2007) is associated with lower depression over the
transition to adulthood.
An alternative explanation for the current findings is that
the tendency towards negative appraisal associated with
depression may have affected responses to the social capital
measures, thus accounting for associations between subjec-
tive aspects of social capital and depression, and non-
associations between behavioural aspects of social capital
and depression (De Silva et al., 2005). However, this is
unlikely to be the case for a number of reasons. First, pre-
vious experiences of depression were controlled for in the
current analysis and depression and social capital were mea-
sured at different time points, thus making it unlikely that
the observed relationship was a product of the influence of
either previous or concurrent experiences of depression on
responses to social capital measures. Second, depression is
also associated with behavioural withdrawal from the social
Figure 1 Relationship between depres-sion in adolescence and early adulthoodby level of peer communication in lateadolescence.Note. High and low values on the predic-tors correspond to 1 standard deviationgreater than and less than sample means,respectively.
Low
0.75
0.65
0.55
0.45
0.35
0.25Medium
Depression in adolescence
Dep
ress
ion
in e
arly
ad
ult
ho
od
High
Peer communicationHighMediumLow
Table 4 Standard errors and t-tests for simple slopes of regressionof adolescent depression on early adult depression
Level of peercommunication Simple slope SE t(1,154)
High 0.07 0.02 3.31**Medium 0.15 0.01 20.48**Low 0.23 0.02 11.21**
**p < .001.
32 M. O’Connor et al.
© 2011 The Australian Psychological Society

environment (American Psychiatric Association, 2000), and
hence a relationship between decreased behavioural aspects
of social capital (i.e., civic action and engagement) and
depression is equally plausible, yet was not observed. Third,
trust and tolerance of others is also a subjective aspect of
social capital, but did not significantly predict depression,
again suggesting that negative appraisal associated with
depression is an insufficient explanation for the observed
results.
A limitation of the current study that warrants consider-
ation relates to the direction of effects between social capital
and depression; that is, whether social capital reduces
depression or depression reduces social capital (De Silva
et al., 2005). Almost all previous research in this area has
been cross-sectional, making it impossible to infer the direc-
tion of effects. In the current study, social capital was mea-
sured as an antecedent of depression, and earlier experiences
of depression were controlled for in the analyses, thus sup-
porting the hypothesised direction of effects from social
capital to depression. However, we were unable to entirely
resolve this question as social capital was not measured in
adolescence, and thus earlier social capital could not be
controlled for in the model. Hence, this possibility requires
exploration in future research. It should also be noted that
the effect sizes observed in relation to the social capital
factors were relatively modest, although the analysis was
stringent in controlling for other highly influential factors,
most notably adolescent depression.
Future research should examine the possibility of non-
linear relationships between depression and trust. At very
high levels, social capital may impede successful functioning
(Putzel, 1997). For example, right wing authoritarianism, a
personality trait characterised by a high degree of trust in
and submissiveness to authorities (Altemeyer, 1996), has
been consistently associated with prejudiced attitudes
towards out-groups (e.g. Laythe, Finkel, & Kirkpatrick,
2002). Furthermore, the potential role of context in moder-
ating the relationship between trust and depression requires
further investigation. A certain degree of mistrust may be
required and may be functional in negotiating an environ-
ment of high crime and violence (Bradley, 1997). Some level
of mistrust may also be adaptive on a societal level. Chanley,
Rudolph, and Rahn (2000), for example, argue that scepti-
cism about the government’s actions ‘is undoubtedly
healthy in a representative democracy’ (p. 240).
The current findings have a number of implications for
policy and intervention. The findings reinforce the impor-
tance of facilitating strong peer relationships during adoles-
cence and, given the risk posed by adolescent depression for
later depression, the importance of early intervention in
addressing mental health problems. The findings further
suggest that the promotion of trust in society’s important
authorities and organisations—such as through increased
community involvement and social connectedness (Glaeser,
Laibson, Scheinkman, & Soutter, 1999)—may also provide
some protective benefits for depression. However, trust is
not a purely subjective phenomenon (Brehm & Rahn,
1997), and individuals’ expectations of trust are facilitated
by the ‘trustworthiness of the social environment’
(Coleman, 1988: p. 119). For example, Chanley et al.’s
(2000) time series analysis found that the state of the
economy, scandals associated with Congress, and increasing
public concern about crime significantly contributed to
declining levels of trust in the US government over the
1980s and 1990s. Hence, responsible conduct from govern-
ment and other important social bodies is also important for
creating a trustworthy environment that promotes young
people’s emotional well-being.
In summary, this study demonstrates that young peoples’
confidence that important social organisations and authori-
ties will act fairly and responsibly is related to their experi-
ences of depression during the transition to adulthood, even
when controlling for the qualities of their relationships with
family and peers, and depression in adolescence. Given that
adolescent depression was the strongest predictor of later
depression, the findings also direct attention to the impor-
tance of early intervention, and the importance of strong
peer relationships, especially for those who have experi-
enced depressive symptoms in adolescence. These findings
suggest a number of potential avenues for intervention to
reduce depression during the transition to adulthood.
REFERENCES
Almedom, A. M. (2005). Social capital and mental health: An inter-disciplinary review of primary evidence. Social Science & Medicine,61(5), 943–964.
Altemeyer, B. (1996). The authoritarian specter. Cambridge, MA:Harvard University Press.
American Psychiatric Association. (2000). Diagnostic and StatisticalManual of Mental Disorders. (text revision, 4th ed.). Washington,DC: American Psychiatric Association.
Angold, A., Costello, E. J., Messer, S. C., Pickles, A., Winder, F., &Silver, D. (1995). Development of a short questionnaire for use inepidemiological studies of depression in children and adolescents.International Journal of Methods in Psychiatric Research, 5, 237–249.
Arbuckle, J., & Wothke, W. (2006). Amos 7.0 user’s guide. Chicago, IL:SPSS Inc.
Armsden, G. C., & Greenberg, M. T. (1987). The Inventory of Parentand Peer Attachment: Individual differences and their relation-ship to psychological well-being in adolescence. Journal of Youthand Adolescence, 16, 427–454.
Arnett, J. (2000). Emerging adulthood: A theory of developmentfrom the late teens through the twenties. American Psychologist,55(5), 469–480.
Badcock, P. B., Moore, E., Williamson, E., Berk, M., Williams, L. J.,Bjerkeset, O. . . . Olsson, C. A. (2011). Gene-environment inter-action in prediction of neuroticism: Risk attributable to the jointaction of the DRD4 exon III 7-repeat allele and low maternalcare. Australian Journal of Psychology, 63(1), 18–25.
Social capital and depression 33
© 2011 The Australian Psychological Society

Bassani, C. (2007). Five dimensions of social capital theory asthey pertain to youth studies. Journal of Youth Studies, 10(1),17–34.
Bradley, C. (1997). Generativity-stagnation: Development of astatus model. Developmental Review, 17, 262–290.
Brehm, J., & Rahn, W. (1997). Individual level evidence for thecauses and consequences of social capital. American Journal ofPolitical Science, 41(3), 999–1023.
Campas, B., Hinden, B., & Gerhardt, C. (1995). Adolescent devel-opment: Pathways and processes of risk and resilience. AnnualReview of Psychology, 46, 265–293.
Chanley, V., Rudolph, T., & Rahn, W. (2000). The origins and con-sequences of public trust in government: A time series analysis.Public Opinion Quarterly, 64, 239–256.
Coleman, J. (1988). Social capital in the creation of human capital.American Journal of Sociology, 94, S95–120.
Coles, R., & Brenner, J. (1965). American youth in a social struggle:The Mississippi summer project. American Journal of Orthopsychia-try, 35, 909–926.
Costello, D., Swendsen, J., Rose, J., & Dierker, L. (2008). Risk andprotective factors associated with trajectories of depressed moodfrom adolescence to early adulthood. Journal of Consulting andClinical Psychology, 76(2), 173–183.
De Silva, M., McKenzie, K., Harpham, T., & Huttly, S. (2005). Socialcapital and mental illness: A systematic review. Journal of Epide-miology and Community Health, 59(8), 619–627.
Ellaway, A., Macintyre, S., & Kearns, A. (2001). Perceptions of placeand health in social contrasting neighbourhoods. Urban Studies,38(12), 2299–2316.
Enders, C. (2006). A primer on the use of modern missing-datamethods in psychosomatic medicine research. Psychosomatic Medi-cine, 68, 427–436.
Erikson, E. (1965). Childhood and society. Harmondsworth, UK:Penguin.
Flanagan, T. J., & Longmire, D. R. (1995). National opinion survey ofcrime and justice. Huntsville, TX: Sam Houston State University,Criminal Justice Centre.
Fredricks, J. A., & Eccles, J. S. (2006). Is extracurricular participationassociated with beneficial outcomes? Concurrent and longitudi-nal relations. Developmental Psychology, 42, 698–713.
Fujiwara, T., & Kawachi, I. (2008). A prospective study ofindividual-level social capital and major depression in the UnitedStates. Journal of Epidemiology and Community Health, 62, 627–633.
Garber, J. (2006). Depression in children and adolescents: Linkingrisk research and prevention. American Journal of Preventive Medi-cine, 6, 104–125.
Glaeser, E., Laibson, D., Scheinkman, J., & Soutter, C. (1999). Whatis social capital? The determinants of trust and trustworthiness. Cam-bridge, USA: National Bureau of Economic Research.
Harris, A., Wyn, J., & Younes, S. (2007). Young people and citizen-ship: An everyday perspective. Youth Studies Australia, 26(3),19–27.
Hawkins, M., Letcher, P., Sanson, A., Smart, D., & Toumbourou, J.(2009). Positive development in emerging adulthood. AustralianJournal of Psychology, 61(2), 89–99.
Jennings, M., & Stoker, L. (2004). Social trust and civic engagementacross time and generations. Acta Politica, 39, 342–379.
Jose, P. (2008). Modgraph-I: A programme to compute cell means for thegraphical display of moderational analyses (Version 2.0). Wellington,New Zealand: Victoria University of Wellington.
La Porta, F., Lopez-de-Silanes, F., Shleifer, A., & Vishny, R. (1997).Trust in large organisations. The American Economic Review, 87(2),333–338.
Laible, D. J., Carlo, G., & Raffaelli, M. (2000). The differential rela-tions of parent and peer attachment to adolescent adjustment.Journal of Youth and Adolescence, 29, 45–59.
Laythe, B., Finkel, D., & Kirkpatrick, L. (2002). Predicting prejudicefrom religious fundamentalism and right-wing authoritarianism:A multiple-regression approach. Journal for the Scientific Study ofReligion, 40(1), 1–10.
Lin, N. (1982). Social resources and instrumental action. InP. Marsden & N. Lin (Eds.), Social structure and network analysis(pp. 131–145). Beverly Hills, CA: Sage.
Lindstrom, M. (2004). Social capital, the miniaturisation of commu-nity and self-reported global and psychological health. SocialScience & Medicine, 59, 595–607.
Lovibond, P., & Lovibond, S. (1995). The structure of negative emo-tional states: Comparison of the Depression Anxiety Stress Scales(DASS) with the Beck Depression and Anxiety Inventories.Behaviour Research and Therapy, 33, 335–343.
Mahoney, J., Cairns, B., & Farmer, T. (2003). Promoting interper-sonal competence and educational success through extracurri-cular activity participation. Journal of Educational Psychology, 95,409–418.
McCullock, A. (2001). Social environments and health: Cross sec-tional national survey. British Medical Journal, 323, 208–209.
Newton, K. (2001). Trust, social capital, civil society, and democracy.International Political Science Review, 22(2), 201–214.
O’Connor, L. E., Berry, J. W., Weiss, J., & Gilbert, P. (2002). Guilt,fear, submission, and empathy in depression. Journal of AffectiveDisorders, 71(1–3), 19–27.
Pancer, S., Pratt, M., & Hunsberger, B. (2007). Community andpolitical involvement in adolescence: What distinguishes theactivists from the uninvolved? Journal of Community Psychology,35(6), 741–759.
Paradis, A. D., Reinherz, H. Z., Giaconia, R. M., & Fitzmaurice, G.(2006). Major depression in the transition to adulthood: Theimpact of active and past depression on young adult functioning.The Journal of Nervous and Mental Disease, 194(5), 318–323.
Paxton, P. (1999). Is social capital declining in the United States? Amultiple indicator assessment. American Journal of Sociology,105(1), 88–127.
Phongsavan, P., Chey, T., Bauman, A., Brooks, R., & Silove, D.(2006). Social capital, socio-economic status and psychologicaldistress among Australian adults. Social Science & Medicine, 63(10),2546–2561.
Piccinelli, M., & Wilkinson, G. (2000). Gender differences in depres-sion. British Journal of Psychiatry, 177, 486–492.
Portes, A. (1998). Social capital: Its origins and applications inmodern sociology. Annual Review of Sociology, 24, 1–24.
Prior, M., Sanson, A., Smart, D., & Oberklaid, F. (2000). Pathwaysfrom infancy to adolescence: Australian Temperament Project 1983–2000. Melbourne, Victoria, Australia: Australian Institute ofFamily Studies.
Putnam, R. (1995a). Bowling alone: America’s declining socialcapital. Journal of Democracy, 6, 65–78.
Putnam, R. (1995b). Tuning in, tuning out: The strange disappear-ance of social capital in America. PS: Political Science and Politics, 28,664–683.
Putzel, J. (1997). Accounting for the ‘dark side’ of social capital:Reading Robert Putnam on democracy. Journal of InternationalDevelopment, 9(7), 939–949.
Reinherz, H., Giaconia, R., Carmola Hauf, A., Wasserman, M., &Silverman, A. (1999). Major depression in the transition to adult-hood: Risks and impairments. Journal of Abnormal Psychology,108(3), 500–510.
Simons, A., Rohde, P., Kennard, B., & Robins, M. (2005). Relapseand recurrence prevention in the treatment for adolescents withdepression study. Cognitive and Behavioral Practice, 12, 240–251.
Smart, D., & Sanson, A. (2005). What is life like for young Austra-lians today, and how well are they faring? Family Matters, 70,46–53.
34 M. O’Connor et al.
© 2011 The Australian Psychological Society

Stone, W. (2001). Measuring social capital: Towards a theoreticallyinformed measurement framework for researching social capital infamily and community life. (Working Paper No. 24). Melbourne,Victoria, Australia: Australian Institute of Family Studies.
Stone, W., & Hughes, J. (2002). Social capital: Empirical meaning andmeasurement validity. (Working Paper No. 27). Melbourne, Victo-ria, Australia: Australian Institute of Family Studies.
Sucoff, C., & Aneshensel, C. (1996). The neighborhood context ofadolescent mental health. Journal of Health and Social Behavior, 37,293–310.
Sullivan, J., & Transue, J. (1999). The psychological underpinningsof democracy: A selective review of research on political toler-ance, interpersonal trust, and social capital. Annual Review ofPsychology, 50, 625–650.
Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics(4th ed.). Boston: Allyn & Bacon.
Tanner, J., Reinherz, H., Beardslee, W., Fitzmaurice, G., Leis, J., &Berger, S. (2007). Change in prevalence of psychiatric disordersfrom ages 21 to 30 in a community sample. The Journal of Nervousand Mental Disease, 195(4), 298–306.
van Eekelen, J. A. M., Olsson, C. A., Ellis, J. A., Ang, W.,Hutchinson, D., Zubrick, S. R., & Pennell, C. E. (2011). Identifi-cation and genetic determination of an early life risk dispositionfor depressive disorder: Atypical stress-related behaviour in earlychildhood. Australian Journal of Psychology, 63(1), 6–17.
Veenstra, G. (2005). Location, location, location: Contextual andcompositional health effects of social capital in British Columbia,Canada. Social Science & Medicine, 60, 2059–2071.
Wittchen, H., Nelson, C. B., & Lachner, G. (1998). Prevalence ofmental disorders and psychosocial impairments in adolescentsand young adults. Psychological Medicine, 28, 109–126.
Yates, M., & Youniss, J. (1996). A developmental perspective oncommunity service during adolescence. Social Development, 5,85–111.
Zarrett, N., Fay, K., Li, Y., Carrano, J., Phelps, E., & Lerner, R.(2009). More than child’s play: Variable- and pattern-centredapproaches for examining effects of sports participation on youthdevelopment. Developmental Psychology, 45(2), 368–382.
AUTHOR NOTE
The Australian Temperament Project (ATP) study is led and
managed by the Australian Institute of Family Studies, and
further information is available from the ATP website
(http://www.aifs.com.au/atp). Funding for this analysis was
supported through grants from the Australian Research
Council. Professor Toumbourou is supported by a Victorian
Health Promotion Foundation Senior Research Fellowship.
We wish to acknowledge the work of Professors Margot Prior
and Frank Oberklaid, and Diana Smart, along with other
collaborators who have contributed to the ATP. We would
also like to sincerely thank the participating families for their
loyal support of the study.
Social capital and depression 35
© 2011 The Australian Psychological Society