the relationship between positive development and psychopathology during the transition to...
TRANSCRIPT

Journal of Adolescence 35 (2012) 701–712
Contents lists available at SciVerse ScienceDirect
Journal of Adolescence
journal homepage: www.elsevier .com/locate/ jado
The relationship between positive development and psychopathologyduring the transition to adulthood: A person-centred approach
Meredith O’Connor a,*, Ann Sanson b, Mary T. Hawkins b, Craig Olsson c, Erica Frydenberg a,John W. Toumbourou c, Primrose Letcher b
aMelbourne Graduate School of Education, The University of Melbourne, AustraliabDepartment of Paediatrics, The University of Melbourne, AustraliacDeakin University and Murdoch Childrens Research Institute, Centre for Adolescent Health, Australia
Keywords:Positive developmentPsychopathologyEmerging adulthoodPerson-centred analysis
* Corresponding author. Department of PaediatricTel.: þ61 03 9345 5537.
E-mail address: [email protected] (M. O’Conn
0140-1971/$ – see front matter � 2011 The Foundadoi:10.1016/j.adolescence.2011.10.006
a b s t r a c t
The transition to adulthood is characterised by potential for both positive developmentand problem outcomes such as psychopathology, yet little is known about relationshipsbetween the two. Given the diversity of pathways observed during this transition period,there is likely to be significant heterogeneity in young people’s experiences of theseoutcomes. Drawing on data from 1158 19–20 year olds in the Australian TemperamentProject and using latent profile analysis, we identified six subgroups. For most, higherpositive development was associated with lower psychopathology and vice versa. Onegroup (33.6%) was high across all positive development measures and low on psychopa-thology, and another (47.7%) average in both areas. The remaining four groups were low onpositive development but differentiated by average psychopathology (4.7%), high inter-nalising (5.5%), and moderate (7.2%) and severe (1.3%) externalising problems. Tailoredintervention strategies that address both the promotion of competence and prevention ofproblem outcomes are needed.� 2011 The Foundation for Professionals in Services for Adolescents. Published by Elsevier
Ltd. All rights reserved.
The transition to adulthood is characterised by exploration of social roles and worldviews, without clear normativeexpectations of how this period should be traversed (Arnett, 2000). It has been described as a window of opportunity forpositive change, as well as a period in which the incidence of risk behaviours and mental health problems is relatively high(Smart & Sanson, 2005). However, an unresolved question is how best to conceptualise the relationship between positivedevelopment and problem outcomes such as psychopathology during this period. This question has important implications;for example, whether the same interventions can be expected to reduce problem outcomes and enhance positive functioning.Given the diversity of pathways observed during this transition period (Arnett, 2000), it is likely that the nature of thisrelationship varies across groups of young people, and variable-centred findings examining average relationships couldtherefore be misleading. This paper takes a person-centred approach to examining the relationship between positivedevelopment and psychopathology during the transition to adulthood, to identify subgroups of young people with similarexperiences of positive and problem outcomes.
s, The University of Melbourne, Royal Children’s Hospital, Flemington Road, Parkville 3052, Australia.
or).
tion for Professionals in Services for Adolescents. Published by Elsevier Ltd. All rights reserved.
M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712702
Defining positive development
Our multidimensional model of positive development at 19–20 years (Hawkins, Letcher, Sanson, Smart, & Toumbourou,2009) incorporates perspectives on developmental psychopathology (Masten & Curtis, 2000), life course and life spanpsychology (Lerner, 2006), and social capital theory (Whitley & McKenzie, 2005). The model identifies five importantdomains of positive development that are relevant across demographic circumstances and contexts of functioning. The firstdomain, social competence, underpins successful social relationships (Gresham, Sugai, & Horner, 2001). The second domain,life satisfaction, reflects a sense of contentment and feelings of congruency betweenwants or needs and accomplishments orresources (Keyes &Waterman, 2003). The third and fourth domains, trust and tolerance of others and trust in authorities andinstitutions, are important aspects of social capital that reflect an individual’s attachment to the community and their capacityto work harmoniously with people from different backgrounds (Putnam, 1995). The fifth domain, civic engagement, refers toan individual’s willingness to take up the role of being a citizen, and is central to political socialization and a successfuldemocratic society (Flanagan & Sherrod, 1998). This model has been shown to be a robust measure of positive developmentduring the transition to adulthood.
Positive development and psychopathology during the transition to adulthood
A remaining area of contention concerns the relationship between positive development and problem outcomes such aspsychopathology. The nature of this relationship may differ during the transition to adulthood from other developmentalperiods: the lack of strict social norms allows a broader range of individual differences to be expressed (Arnett, 2000), andintensified identity exploration raises the possibility that negative outcomes, such as high levels of substance use, couldcoincide with positive outcomes, such as identity development (Arnett, 2005). There are several competing hypotheses in theliterature about this relationship; specifically, that positive development and psychopathology may be 1) poles of a singleunderlying dimension, 2) separate but inversely related constructs, or 3) variably related depending on the specificdimensions examined. The empirical support for each of these hypotheses will next be examined.
Poles of a single dimensionThe medical model assumes that positive and negative mental health outcomes reflect a single underlying dimension
(Keyes, 2007), and this assumption has been carried forward in several empirical models of positive development during thetransition to adulthood. For example, Gambone, Klem, and Connell’s (2002) model of positive functioning includes theabsence of a range of negative outcomes (such as not being a drug user), in addition to the presence of numerous positivedimensions of functioning (such as employment). Looking at progress towards meeting developmental tasks, Schulenberg,Bryant, and O’Malley (2004) examined positive youth outcomes such as being involved with a peer group, as well asavoiding negative outcomes (e.g., substance use). Similarly, Masten et al.’s (1995) model of “competence” at 20 years includesthe presence of positive outcomes such as academic achievement, as well as the absence of antisocial behaviour. In contrast tothe former two studies, Masten et al. (1995) empirically tested their model, and found it to fit their data well. Hence, despitethe fact that this assumption is implicit in a number of models, few studies have empirically tested it.
Distinct but inversely correlated factorsThe positive youth development field tends to conceptualise positive development and poor functioning as distinct
dimensions with an inverse association (Silbereisen & Lerner, 2007). According to this hypothesis, individuals who are high inpositive development are relatively problem free, whereas those who are high in problem outcomes are low in positivedevelopment and unable to interact in positive ways with their environment (Jelicic, Bobek, Phelps, Lerner, & Lerner, 2007).Hence, interventions focussing on promoting positive development should reduce negative outcomes and the need to investin problem-based interventions (Silbereisen & Lerner, 2007).
More convincing support has been found for this hypothesis. For example, O’Connor et al. (2011) found that a structuralequation model in which positive development and psychopathology at 19–20 years were distinct but moderately correlatedfactors was a good fit for the data and a better fit than other plausible models. Hawkins, Catalano, Kosterman, Abbott, and Hill(1999) examined the effects of amulti-level intervention delivered inprimary school. At age 18, the intervention group showedboth higher levels of positive outcomes, including school bonding and academic achievement, and lower levels of problembehaviours, such as heavy drinking, thus suggesting that the same intervention influenced both outcomes. Similarly, Oesterle,Hill, Hawkins, and Abbott (2008) found that positive functioning in adolescence significantly decreased the likelihood of lateralcohol use disorders at ages 21 and 24. However, some adolescent findings using person-centred analyses (e.g., Phelps et al.,2007; Zimmerman, Phelps, & Lerner, 2008) have led Lerner and colleagues to temper this hypothesis somewhat, suggestingthat for a minority of adolescents, problem outcomes may occur in the context of high positive development (Lerner, 2009).
Dimension-specific relationshipsA third position on the relationship between positive development and psychopathology is that these constructs are
related in complex and varied ways, with some facets of positive development related to, and others independent of, negativeoutcomes. For example, Kosterman et al. (2005) examined correlations between problem outcomes (crime and substanceuse), and dimensions of positive functioning (e.g., volunteerism) when participants were 21 years old. The observed

M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712 703
correlations were highly variable in strength and statistical significance. Thus, aspects of positive and problems outcomesappeared variably related depending on the specific dimensions examined. However, this position is mostly atheoretical,arising only from empirical findings.
Antecedents of positive and problem outcomes
In addition to describing the nature of transitions to young adulthood, insights into the predictors of healthy transitionswould provide a basis for innovation in prevention and health promotion across this period. A number of developmentalantecedents are likely to be associated with different experiences of positive and problem outcomes during the transition toadulthood. For example, connectedness in youth social environments (such as the family, community, and peer group) isa basic human need that is essential for both well-being and mental health outcomes (Ryan & Deci, 2001). Similarly, self-regulation (indicated by factors such as control of emotional expression) has been described as a cornerstone of develop-ment (Shonkoff & Phillips, 2000). Higher socioeconomic background and female gender have also been consistently asso-ciatedwithmore adaptive outcomes (Mossakowski, 2008; Phelps et al., 2007). In a previous study, we have reported evidencefor the unique contributions of all of these factors (social connectedness, emotional regulation, gender, and SES) to positivedevelopment during the transition to adulthood inmultivariate analyses (O’Connor et al., 2011). Hence, these factors are likelyto represent an important set of predictors of profiles of developmental outcomes in emerging adulthood.
The current study
The first aim of the study is to provide insight into the relationship between positive development and psychopathologyover the transition to adulthood. Most previous research examining this question has taken a variable-centred approach,which seeks to identify processes common to all members of a group; however, results can be misleading if they reflect theaverage of a number of different underlying relationships. Person-centred analyses aim to identify groups or types of indi-viduals who share particular attributes or relations among attributes, emphasising diversity rather than central tendency(Magnusson, 2003). Given the diversity of pathways observed during this transition period (Arnett, 2000), we hypothesizedthat person-centred analysis would reveal heterogeneity in the relations between positive development and psychopa-thology, evidenced by the identification of a number of underlying groups.
The second aim of the study was to examine the relationship between antecedents known to be important for positive andproblem outcomes and profiles of development during the transition to adulthood. We hypothesized that adolescent factorsreflecting social connectedness (indicated by the quality of relationships with peers, parents, school, and community), and thecapacity for self-regulation (indicated by emotional control), would be associatedwith better outcomes.We also hypothesizedthat higher socioeconomic status (SES) background and female gender would predict membership in more adaptive groups.
To examine these two questions, we draw on data from the Australian Temperament Project (ATP), which provides a rareopportunity to examine both functioning during the transition to adulthood and antecedent characteristics.
Method
Participants and procedure
The ATP has followed the psychosocial development of a community sample from infancy to adulthood: a representativesample of 2443 infants was recruited through selectedMaternal and Child Health Centres across both urban and rural areas inthe State of Victoria, Australia, during a twoweek period in 1983. Using mail surveymethodology, 15 waves of data have beencollected over the past 28 years from parents, primary school teachers, maternal and child health nurses, and from the age of11 onwards, the young people themselves (see Prior, Sanson, Smart, & Oberklaid, 2000).
Participants in the current study were the 1158 participants who completed the thirteenth survey at age 19–20 years, andthus had data on positive development and psychopathology at this time. Questionnaire booklets weremailed to participants,together with reply-paid, addressed envelopes in which to return them. Participants were 647 females and 511 males, rep-resenting 77% of the young people who were still enrolled in the study at 19–20 years.
Approximately two-thirds of the cohort was still enrolled in the study after 20 years. Attrition has been slightly higher infamilies experiencing socioeconomic disadvantage and among families with parents not born in Australia. However, therewere no substantial differences between the retained and non-retained subgroups at 19–20 years on child characteristicsassessed in infancy. Hence, although attrition has led to a slight under-representation of young people from families living insocio-economically disadvantaged circumstances, the study continues to include childrenwith awide range of capacities andcharacteristics, and attrition is unlikely to be a significant influence on the results.
Materials
Positive developmentThe measure used to assess dimensions of positive development during the transition to adulthood was developed by
Hawkins et al. (2009) using AMOS 7.0 SEM confirmatory factor analysis (SPSS, 2006). The positive development construct
M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712704
incorporates the five domains of social competence, life satisfaction, trust and tolerance of others, trust in authorities andorganizations and civic action and engagement, all assessed by self report at 19–20 years. All first order constructs loadedmeaningfully on the second-order positive development construct (from .30 to .68), and all second-order loadings weregender invariant. Themodel provided an excellent fit for the data (RMSEA¼ .05, CFI¼ .94). Using model-based imputation onthe final positive development model, latent factor scores were computed for each first order construct and these scores areused in the following analyses. The components of these scores are described below.
Social competencewas assessed with three subscales derived from Smart and Sanson (2003), including empathy (5 items,a ¼ .78, e.g., ‘I show my concern for others when they experience difficulties’), responsibility (4 items, a ¼ .72, e.g., ‘I can berelied on to do things right’), and self control (3 items, a¼ .60, e.g., ‘I can assert my opinionwithout arguing or fighting’). Itemswere rated on a 5-point Likert scale ranging from ‘never’ to ‘always’.
Life satisfaction was measured by two subscales adapted from the National Survey of Families and Households (Sweet &Bumpass, 2002), including a) satisfaction with achievement and life directions (3 items, a ¼ .83, e.g., ‘How satisfied areyou with what you are accomplishing?’), and b) satisfaction with personal and social life (5 items, a ¼ .75, e.g., ‘How satisfiedare you with your social life?’). Items were rated on a 4-point scale from ‘very satisfied’ to ‘not at all satisfied’.
Trust and tolerance of otherswasmeasured using 3 single items derived from Stone and Hughes (2002, pp.1–64) relating totrust in people in the neighbourhood, trust in Australians, and tolerance of different ethnic groups (e.g., ‘Most people in yourneighbourhood can be trusted’; a ¼ .55). Ratings were made on a 5-point scale from ‘disagree completely’ to ‘agreecompletely’.
Trust in authorities and organizations was measured by three scales, two derived from Flanagan and Longmire (1995)measuring trust in authorities, and one from Stone and Hughes (2002, pp. 1–64) measuring trust in organizations. Thescales comprised a) confidence in police (5 items, a ¼ .83, e.g., ‘How much confidence do you have in the police to treateveryone fairly’ rated on a 4-point scale from ‘a great deal’ to ‘none at all’), b) confidence in the courts (5 items, a ¼ .87, e.g.,‘Howmuch confidence do you have in the ability of the courts to impose fair sentences’ rated on the same scale), and c) trustin organizations (8 items, a¼ .83), reflecting confidence that various organizations/institutions can be relied on to act in a fairor reasonable manner (e.g., government, the media), using a 4-point scale from ‘not at all confident’ to ‘very confident’.
Civic action and engagement was measured by three scales derived from Stone (2001, pp. 1–38) and Stone and Hughes(2002, pp. 1–64) tapping a) participation in community activities over the past year (10 items, a ¼ .58, e.g., ‘In the past 12months how often have you attended a public meeting’ rated from ‘not at all’ to ‘5 times or more’), b) participation in groups(9 items, a ¼ .65, e.g., ‘sporting, recreation, or hobby groups’ rated as ‘yes’ or ‘no’ to participation in the last year), and c)donations to groups (9 items, a ¼ .60, e.g., ‘church groups’ rated as ‘yes’ or ‘no’ to donations made in the past year).
PsychopathologyThe measure used to assess internalising and externalising problems was developed by O’Connor et al. (2011) also using
confirmatory factor analysis. Themodel replicatedKrueger, Caspi,Moffitt, andSilva’s (1998)model of psychopathologyat 18–21years, and incorporates the twodomainsof internalising andexternalisingproblems, bothassessedbyself report at 19–20years.The internalising problems latent factor was indicated by depression, anxiety, and stress, reflecting general internalisingpathology (Henry & Crawford, 2005), and the externalising problems latent factor was indicated by antisocial behaviour,problematic alcohol use, and problematic marijuana use. Internalising and externalising problems were allowed to freelycovary. Standardized loadings ranged from .43 to .86 and were all significant at p < .001. The latent correlation between theinternalising and externalising factors was estimated to be .26 (p< .001). Gender invariance was examined and all differenceswere trivial inmagnitude.Themodelwasanexcellentfit byallmeasures examined (RMSEA¼ .04;AGFI¼ .99). As for thepositivedevelopmentmodel, latent factor scores were computed usingmodel-based imputation on the final model and these imputedvalues were used as the internalising and externalising scores. The components of these two scores are described below.
Internalising problemswere assessed by Lovibond and Lovibond’s (1995) Depression Anxiety Stress (DASS) scales. The DASSassessed the subscales of a) depression (e.g., ‘I felt that I had nothing to look forward to’; a¼ .89), b) anxiety (e.g., ‘I felt scaredwithout any good reason’; a¼ .77), and c) stress (e.g., ‘I found it hard towind down’; a¼ .83). Each subscale comprised 7 itemsrated on a 4-point Likert scale from ‘did not apply’ to ‘applied very much/most of the time’ over the past month.
Externalising problems were assessed by a) antisocial behaviour, which was measured according to the frequency ofengaging in 13 antisocial acts (e.g., ‘Get into physical fights with other people’) taken from Elliot and Ageton (1980), where1¼ never and 6¼10þ times over the last year (a¼ .70); b) problematic alcohol use assessed by frequency of harms associatedwith use (10 items, e.g., ‘Get so drunk youwere sick or passed out’; a¼ .79); and c) problematicmarijuana usemeasuredwith 5items relating to harms associated with use (e.g., ‘Felt irritable or depressed when it wasn’t available’; a ¼ .79). Participantsrated both b) and c) according to frequency over the past year, where 0 ¼ never, 1 ¼ once or twice, and 2 ¼ more often.
Key antecedents of positive developmentSocioeconomic status (SES) was measured according to parent reports at 4–8 months, as a composite of both parents’
occupational level and educational level (Broom, Jones, & Zubrzycki,1974; Brotherton, Kotler, & Hammond,1979). This infancymeasure was chosen for two reasons: the stability of SES across time (e.g., r ¼ .9 across the first three waves), and our interestin antecedent predictors. Parents also indicated their child’s gender at this time.
Emotional controlwasmeasured by self report at 15–16 years. The ATP-devised scale encompassed 10 items (e.g., ‘I am ableto keep my feelings under control’) rated on a 6-point scale from ‘never’ to ‘always’ (a ¼ .70).

M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712 705
Relationship with peerswas measured at 17–18 years according to the mean of the Communication (e.g., “My friends sensewhen I’m upset about something”), Trust (e.g., “My friends accept me as I am”), and Alienation (reverse scored, e.g., “Myfriends don’t understand what I’m going through these days”) subscales of the Inventory of Parent and Peer Attachment(Armsden & Greenberg, 1987). Responses were made by the teenager on a 4-point scale ranging from ‘always/almost always’to ‘never/almost never’.
Relationship with parentswasmeasured as the mean of theWarmth (e.g., “Senses when I’mupset about something”), Trust(e.g., “Considers my point of view when we discuss things”), and Alienation (reverse scored; e.g., “Doesn’t understand me”)subscales of the same inventory (a ¼ .83).
The School bonding scale (O’Donnell, Hawkins, & Abbott, 1995) was self-completed at 17–18 years. The scale (9 items,a ¼ .88, e.g., ‘I look forward to going to school’) was rated on a 5-point scale where 1 ¼ always and 5 ¼ never/almost never.
The community orientation scale asked participants at 17–18 years to rate the likelihood of their involvement in threeactivities (e.g., ‘Work to improve conditions in your local community’) in the future, with responses made on a 4-point scaleranging from ‘not likely’ to ‘extremely likely’ (a ¼ .61).
Analytic approach
Latent Profile Analysis (LPA), conducted with Mplus (Muthén & Muthén, 2010), was used to identify groups with similarexperiences of positive and problem outcomes. LPA is a model-based statistical method for identifying unmeasured classmembership among participants using continuous indicator variables (Lanza, Flaherty, & Collins, 2003). LPA has a number ofadvantages over related techniques such as cluster analysis, including more objective methods for choosing the number ofgroups to extract from the data.
To determine the optimal number of profiles to extract from the data in the current analysis, four fit statistics were used tocompare models. The Akaike Information Criterion (AIC) and size-adjusted Bayesian Information Criterion (BIC) provide anindex of relative model fit, with lower values reflecting better fit (Schermelleh-Engel, Moosbrugger, & Muller, 2003; Schwarz,1978). The Lo–Mendell–Rubin Adjusted Likelihood Ratio Test (LMRT; Lo, Mendell, & Rubin, 2001) compares the specifiedmodel to a model with one less class; significant p values indicate that the specified solution is significantly better than thereducedmodel. The entropy index determines the accuracy of classifying people into their respective class, with higher valuesindicating better fit (Muthén, 2006).
Multivariate Analysis of variance (MANOVA; Scheffe, 1999) with post-hoc comparisons, conducted with SPSS version 19(SPSS, 2010), was used to examine group differences in variables included in the analysis and across antecedent factors.
Results
Identification of groups
The current LPA uses seven continuous variables, including the five positive development dimensions and the twopsychopathology dimensions, to identify underlying groups of young peoplewith similar experiences of positive and problemoutcomes. Missing data was low (averaging <1%) and was estimated using the Expectation-Maximization (EM) Algorithm(Enders, 2006). Intercorrelations between variables used in the analyses are presented in Table 1.
The plausibility of 3- to 7-class solutions was investigated, and Table 2 shows the fit of eachmodel according to the variousfit measures. The 3-, 4-, 5- and 6-class solutions were consecutively better fitting models than their predecessor with one lessclass. The LMRT indicated that a 7-class model did not provide a significantly better fit than the 6-class solution. Hence, the 6-class solution was deemed the best fitting model.
The mean scores of each class on the dimensions of positive development and psychopathology were used to interpretthe groups (see Table 3 and Fig. 1; scores were converted to z scores to aide interpretation). Participants in the first class werehigh in all dimensions of positive development and low in psychopathology, and hence could be described as Thriving(n ¼ 389, 33.6%). The second group had average levels of positive development and psychopathology, and could be describedasWell-adjusted (n ¼ 552, 47.7%). The third group could be described as Idling (n¼ 55, 4.7%): they were average in their levelsof psychopathology, yet they were also low on all positive development dimensions. The fourth group had markedly higherlevels of internalising problems, as well as low levels of life satisfaction, and hence could be described as Internalising(n ¼ 64, 5.5%). Another group showed moderately high levels of externalising pathology, combined with low positivedevelopment, and could be described as Moderate externalising (n ¼ 83, 7.2%). Finally, the small Severe externalising groupshowed very high levels of externalising pathology and very low positive development (n ¼ 15, 1.3%). MANOVA revealeda significant multivariate effect of group membership on the dimensions included in the model (F(7, 1150) ¼ 735.2, p < .001),and univariate F-tests showed significant group differences for each positive development and psychopathology dimension,as shown in Table 3.
Relationships of groups to antecedent factors
Next, the relationships between the sixgroups and theantecedent factors of genderand socioeconomic status in infancy, andemotional control, peer relationships, parent relationships, school bonding, and community orientation in adolescence were
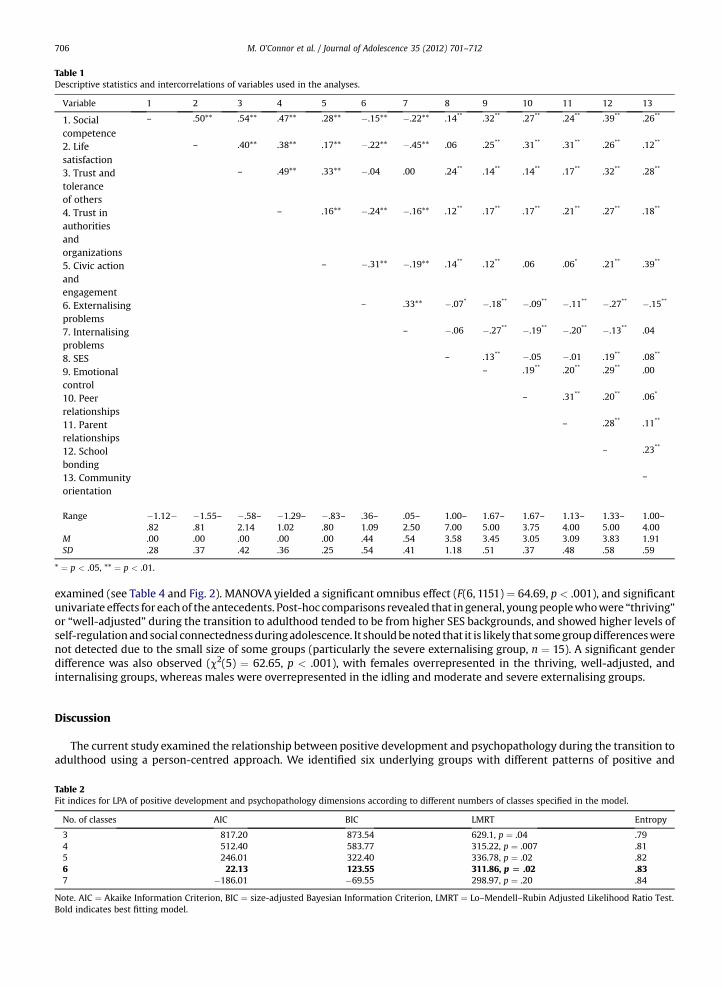
Table 1Descriptive statistics and intercorrelations of variables used in the analyses.
Variable 1 2 3 4 5 6 7 8 9 10 11 12 13
1. Socialcompetence
– .50** .54** .47** .28** �.15** �.22** .14** .32** .27** .24** .39** .26**
2. Lifesatisfaction
– .40** .38** .17** �.22** �.45** .06 .25** .31** .31** .26** .12**
3. Trust andtoleranceof others
– .49** .33** �.04 .00 .24** .14** .14** .17** .32** .28**
4. Trust inauthoritiesandorganizations
– .16** �.24** �.16** .12** .17** .17** .21** .27** .18**
5. Civic actionandengagement
– �.31** �.19** .14** .12** .06 .06* .21** .39**
6. Externalisingproblems
– .33** �.07* �.18** �.09** �.11** �.27** �.15**
7. Internalisingproblems
– �.06 �.27** �.19** �.20** �.13** .04
8. SES – .13** �.05 �.01 .19** .08**
9. Emotionalcontrol
– .19** .20** .29** .00
10. Peerrelationships
– .31** .20** .06*
11. Parentrelationships
– .28** .11**
12. Schoolbonding
– .23**
13. Communityorientation
–
Range �1.12�.82
�1.55–.81
�.58–2.14
�1.29–1.02
�.83–.80
.36–1.09
.05–2.50
1.00–7.00
1.67–5.00
1.67–3.75
1.13–4.00
1.33–5.00
1.00–4.00
M .00 .00 .00 .00 .00 .44 .54 3.58 3.45 3.05 3.09 3.83 1.91SD .28 .37 .42 .36 .25 .54 .41 1.18 .51 .37 .48 .58 .59
* ¼ p < .05, ** ¼ p < .01.
M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712706
examined (see Table 4 and Fig. 2). MANOVA yielded a significant omnibus effect (F(6, 1151) ¼ 64.69, p < .001), and significantunivariate effects for eachof the antecedents. Post-hoc comparisons revealed that in general, youngpeoplewhowere “thriving”or “well-adjusted” during the transition to adulthood tended to be from higher SES backgrounds, and showed higher levels ofself-regulationandsocial connectednessduringadolescence. It shouldbenoted that it is likely that somegroupdifferenceswerenot detected due to the small size of some groups (particularly the severe externalising group, n ¼ 15). A significant genderdifference was also observed (c2(5) ¼ 62.65, p < .001), with females overrepresented in the thriving, well-adjusted, andinternalising groups, whereas males were overrepresented in the idling and moderate and severe externalising groups.
Discussion
The current study examined the relationship between positive development and psychopathology during the transition toadulthood using a person-centred approach. We identified six underlying groups with different patterns of positive and
Table 2Fit indices for LPA of positive development and psychopathology dimensions according to different numbers of classes specified in the model.
No. of classes AIC BIC LMRT Entropy
3 817.20 873.54 629.1, p ¼ .04 .794 512.40 583.77 315.22, p ¼ .007 .815 246.01 322.40 336.78, p ¼ .02 .826 22.13 123.55 311.86, p [ .02 .837 �186.01 �69.55 298.97, p ¼ .20 .84
Note. AIC ¼ Akaike Information Criterion, BIC ¼ size-adjusted Bayesian Information Criterion, LMRT ¼ Lo–Mendell–Rubin Adjusted Likelihood Ratio Test.Bold indicates best fitting model.

Table 3Group means for the six classes according to positive development and psychopathology dimensions.
Variable Thriving(1)
Well-adjusted(2)
Idling(3)
Internalising(4)
Moderateexternalising(5)
Severeexternalising(6)
UnivariateF-test
M SD M SD M SD M SD M SD M SD F-value Significant groupdifferences
Social competence .85 .61 �.26 .68 �1.47 .95 �.22 .99 �.66 .94 �2.33 1.03 215.52** All except 2–4Life satisfaction .74 .68 �.18 .75 �1.12 .80 �1.29 1.15 �.27 .98 �1.57 1.14 147.35** All except 2–5, 3–4Trust and tolerance
of others.81 .68 �.23 .70 �1.96 .68 �.17 .83 �.60 .95 �1.25 1.08 206.70** All except 2–4
Trust in authoritiesand organizations
.74 .75 �.21 .77 �1.40 .86 �.19 .88 �.65 .90 �1.99 1.17 141.34** All except 2–4, 3–6
Civic action andengagement
.50 1.11 �.26 .77 �.65 .56 .04 1.03 �.14 .98 �.45 1.38 37.15** All except 2–4,2–6, 4–6
Internalising problems �.39 .63 �.17 .68 .36 .91 2.54 .88 .51 .97 1.47 1.40 209.38** All except 3–5Externalising problems �.37 .41 �.22 .48 .09 .60 .14 .50 2.08 .66 5.39 1.14 721.25** All except 3–4
Note: Descriptive statistics are based on z scores.** ¼ p < .01.
M.O
’Connoret
al./Journal
ofAdolescence
35(2012)
701–712
707

Fig. 1. Levels of positive development and psychopathology dimensions according to group.
M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712708
problem outcomes. The presence of these groups not only points to the importance of understanding individual differencesduring the transition to adulthood, but also highlights the value of consideringmore tailored approaches to program design tooptimise health promotion gains.
The positive youth development literature proposes that positive development and psychopathology share an inverserelationship (Silbereisen & Lerner, 2007), and this inverse relationship held for most young people in the current study, withthe thriving, well-adjusted, and externalising groups all showing a pattern of results characterised by higher positivedevelopment/lower psychopathology or vice versa, or average levels of both domains in the case of the well-adjusted group.Person-centred analysis revealed that there were exceptions to this general trend for the smaller proportion of participants inthe idling and internalising groups. For example, young people in the idling group had average levels of psychopathology,despite being uniformly low in positive development. This finding is consistent with several adolescent studies which foundmultiple patterns in the intersections of trajectories of positive development and psychopathology over time (Lewin-Bizanet al., 2010; Phelps et al., 2007; Zimmerman et al., 2008).
Furthermore, the identification of the “idling” group strongly supports the positive youth development position that“problem free is not fullyprepared” (Pittman&Fleming,1991: p. 3). Youngpeople in the idling groupwere relativelyuntroubledbypsychopathology, yet theywereunsatisfiedwith their lives, lowin social competencies, andpoorlyadjusted to authority.Ourfindings are compelling in suggesting that the absence of mental illness does not ensure the presence of well-being, andreiterates the importanceofmovingbeyondapurelydeficit-based viewofwhat constitutes “good”development (Keyes, 2007).
Little support was found for other conceptualisations of the relationship between positive development and psychopa-thology. The results do not show the completely inverse relationship predicted by the medical model assumption thatpositive functioning and mental health problems form poles of a single underlying dimension. Similarly, there was relativelylittle variability in the relationships between specific dimensions of positive and negative functioning, offering little supportto Kosterman et al.’s (2005) findings.
Relationships of groups to antecedent factors
The current study also demonstrates that the observed subgroups could be differentiated by antecedent factors. Theimportance of emotional control was consistent with the identification of self-regulation as critical for healthy development(Shonkoff & Phillips, 2000). Parent and peer relationships, as well as positive relationships with school over adolescence alsodifferentiated the groups: attachment theory suggests that positive relationships provide young people with a secure andconsistent support system from which they can develop trusting relationships with others and explore their environment

Table 4Group means, SDs and F-values for the six classes according to key predictors of positive development.
Variable Thriving(1)
Well-adjusted(2)
Idling(3)
Internalising(4)
Moderateexternalising(5)
Severeexternalising(6)
UnivariateF-test
M SD M SD M SD M SD M SD M SD F-value Significant groupdifferences
SES .21 1.03 �.06 .97 �.50 .83 �.14 .94 �.07 1.01 �.41 1.04 7.80** 1–2, 1–3, 2–3Emotional control .33 .96 �.06 .92 �.24 1.14 �.62 1.06 �.40 .95 �.86 1.00 21.13** 1–all, 2–4, 2–5, 2–6,Relationship with peers .30 .96 �.09 .93 �.44 1.22 �.41 1.26 �.11 .87 �.34 1.11 13.45** 1–all except 6Relationship with parents .32 .88 �.09 1.01 �.46 1.06 �.38 1.13 �.11 .89 �.91 1.03 16.71** 1–all, 2–6, 5–6School bonding .31 .80 .01 .91 �.51 1.21 �.40 1.32 �.54 1.13 �1.82 1.40 47.38** All except 2–4, 3–4, 3–5,
3–6, 4–5, 5–6Community orientation .32 1.01 �.14 .93 �.66 .75 .41 1.15 �.33 .93 �.61 .62 21.92** All except 1–4, 2–5, 2–6,
3–5, 3–6, 5–6
Note: Descriptive statistics are based on z scores.* ¼ p < .05, ** ¼ p < .01.
M.O
’Connoret
al./Journal
ofAdolescence
35(2012)
701–712
709

Fig. 2. Levels of key adolescent predictors according to group.
M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712710
(Bretherton &Munholland, 1999). An orientation towards working for the community also differentiated between those whowere relatively well adapted and those who were idling or experiencing externalising problems. Interestingly, however, theinternalising group also had significantly higher levels of community orientation than other groups. This is consistent withprevious research suggesting that behaviours such as volunteering are associated with both benefits to development andsome psychological strain (e.g., Zarrett et al., 2009). As expected, the demographic factors of higher family socioeconomicstatus (SES) and female gender were generally associated with more adaptive outcomes.
Limitations
Certain limitations of the current study warrant consideration. When examining the relationship of the groups todemographic and antecedent factors, we were constrained by the data available and hence were unable to control for earlierpositive development or the antecedent factors at 19–20 years. This limits our capacity to make inferences about causation.The modest reliability of some measures used in the study (with alpha coefficients ranging from .60 to .89) is an additionallimitation. However, the structural equation modelling methodology used to derive the positive development and psycho-pathology scores is likely to have addressed this to a large extent, through its capacity to remove error variance. Finally, therespondents retained in the sample at 19–20 years were somewhat higher in socioeconomic status and less ethnically diversethan the original sample which may limit generalisability, although the retained sample continued to include participantsfrom a wide range of backgrounds and circumstances.
Implications
Although a generally inverse relationship between positive development and psychopathology held for the majority ofparticipants, there were subgroups showing different patterns of functioning. In regards to model development, this suggeststhat low psychopathology is likely to be a poor indicator of positive development for at least some young people. In regards tointervention, our findings suggest that some specific and distinct developmental pathways may operate in relation to positiveand problem outcomes, supporting calls for programs that promote and maintain positive mental health to complimentdeficit-focused interventions. Given the diversity identified by the person-centred analyses, the current findings also supportZimmerman et al.’s (2008) warning against a “cookie cutter” or generic approach and the need for tailored intervention. Forexample, the idling groupwould benefit from interventions that focus predominately on building their competencies,whereasthe internalising and externalising groups would benefit from interventions to address their mental health symptoms.
Future directions
Anenduring area for futurediscussion and research is theneed for betterdeveloped theory (Phelps et al., 2007), as this is notonlyanempirical questionbut alsoa conceptual issue. Inparticular, therehasbeen little theoretical discussionof theunderlyingprocesses that might account for the observed relationships between positive and negative outcomes. Hence, although thecurrent findings provide empirical support for some positions, further discussion of the underlying mechanisms is needed.

M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712 711
Future research should also examine the relationship between positive development and psychopathology longitudinally,to provide insight into how these outcomes relate across time. Given the diversity of young people’s demographic profilesover this period (Arnett, 2000), it would also be of interest to examine how the identified groups differ in relation to theirconcurrent life circumstances. The nuances in the relationship between positive development and psychopathology observedin the current study could not have been discerned using a traditional, variable-centred approach, suggesting that futureresearch should integrate both variable- and person-oriented methods.
Conclusions
We took a person-centred approach to the question of how positive development and psychopathology relate over thetransition to adulthood. The person-centredmethodology revealed a number of underlying groupswith different experiencesof positive development and psychopathology, which could be differentiated by antecedent factors. Consistent with theheterogeneity of young people’s pathways towards adulthood, the trend for positive development and psychopathology to benegatively correlated was generally apparent, but did not hold for all young people. The results suggest the importance ofdistinct intervention strategies for promoting positive development and reducing psychopathology, as neither focus is likelyto be sufficient in isolation.
Acknowledgments
The ATP study is managed by the Australian Institute of Family Studies, and is a collaboration between the University ofMelbourne, Royal Children’s Hospital, and the Australian Institute of Family Studies; further information available at www.aifs.com.au/atp. Funding for this analysis was provided by a project grant from the Australian Research Council (Investiga-tors Professor Ann Sanson, Dr. Craig Olsson and Ms Diana Smart). Professor John Toumbourou and Dr. Craig Olsson aresupported by Victorian Health Promotion Foundation Research Fellowships. We acknowledge all collaborators who havecontributed to the Australian Temperament Project, especially Ms. Diana Smart and Professors Margot Prior and FrankOberklaid. Wewould also like to thank all families involved in the ATP for their time and invaluable contribution to the study.
References
Armsden, G., & Greenberg, M. (1987). The inventory of parent and peer attachment: individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16, 427–454.
Arnett, J. (2000). Emerging adulthood: a theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480.Arnett, J. (2005). The developmental context of substance use in emerging adulthood. Journal of Drug Issues, 35, 235–254.Bretherton, I., & Munholland, K. (1999). Internal working models in attachment relationships: a construct revisited. In J. Cassidy, & P. Shaver (Eds.),
Handbook of attachment: Theory, research, and clinical applications. New York: Guilford Press.Broom, L., Jones, F., & Zubrzycki, J. (1974). Opportunity and attainment in Australia. Canberra: ANU Press.Brotherton, P., Kotler, T., & Hammond, S. (1979). Development of an Australian index of social class. Australian Psychologist, 14, 77–83.Elliot, S., & Ageton, S. (1980). Reconciling race and class differences in self-reported and official estimates of delinquency. American Sociological Review, 45,
95–110.Enders, C. (2006). A primer on the use of modern missing-data methods in psychosomatic medicine research. Psychosomatic Medicine, 68, 427–436.Flanagan, C., & Sherrod, L. (1998). Youth political development: an introduction. Journal of Social Issues, 54, 447–456.Flanagan, T., & Longmire, D. (1995). National opinion survey of crime and justice. Huntsville, TX: Sam Houston State University, Criminal Justice Centre.Gambone, M., Klem, A., & Connell’s, J. (2002). Finding out what matters for youth: Testing key links in a community action framework for youth development.
Philadelphia: Youth Development Strategies, Inc., and Institute for Research and Reform in Education.Gresham, F., Sugai, G., & Horner, R. (2001). Interpreting outcomes of social skills training for students with high-incidence disabilities. Exceptional Children,
67(3), 331–344.Hawkins, J., Catalano, R., Kosterman, R., Abbott, R., & Hill, K. (1999). Preventing adolescent health-risk behavior by strengthening protection during
childhood. Archives of Pediatrics and Adolescent Medicine, 153, 226–234.Hawkins, M., Letcher, P., Sanson, A., Smart, D., & Toumbourou, J. (2009). Positive development in emerging adulthood. Australian Journal of Psychology, 61(2),
89–99.Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in
a large non-clinical sample. British Journal of Clinical Psychology, 44(2), 227–239.Jelicic, H., Bobek, D., Phelps, E., Lerner, R., & Lerner, J. (2007). Using positive youth development to predict contribution and risk behaviors in early adolescence:
findings from the first two waves of the 4-H study of positive youth development. International Journal of Behavioral Development, 31(3), 263–273.Keyes, C. (2007). Promoting and protecting mental health as flourishing. A complementary strategy for improving national mental health. American
Psychologist, 62, 95–108.Keyes, C., & Waterman, M. (2003). Dimensions of well-being and mental health in adulthood. In M. Bornstein, L. Davidson, C. Keyes, & K. Moore (Eds.), Well-
being. Positive development across the life course (pp. 477–497). Mahwah, NJ: Lawrence Erlbaum.Kosterman, R., Hawkins, J., Abbott, R., Hill, K., Herrenkohl, T., & Catalano, R. (2005). Measures of positive adult behavior and their relationship to crime and
substance use. Prevention Science, 6, 21–33.Krueger, R., Capsi, A., Moffitt, T., & Silva, P. (1998). The structure and stability of common mental disorders (DSM-III-R): a longitudinal-epidemiological
study. Journal of Abnormal Psychology, 107(2), 216–227.Lanza, S., Flaherty, B., & Collins, L. (2003). Latent class and latent transition analysis. In J. Schinka, & W. Velicer (Eds.), Handbook of psychology: Research
methods in psychology, Vol. 2 (pp. 663–685). Hoboken, NJ: John Wiley and Sons.Lerner, R. (2006). Developmental science, developmental systems, and contemporary theories of human development. In R. Lerner, & W. Damon (Eds.),
Handbook of child psychology (6th ed.).. Theoretical models of human development, Vol. 1 (pp. 1–17) Hoboken, NJ: John Wiley & Sons.Lerner, R. (2009). The positive youth development perspective: theoretical and empirical bases of a strengths-based approach to adolescent development.
In C. Snyder, & S. Lopez (Eds.), Oxford handbook of positive psychology (pp. 149–164). New York: Oxford University Press.Lewin-Bizan, S., Lynch, A., Fay, K., Schmid, K., McPerran, C., Lerner, J., et al. (2010). Trajectories of positive and negative behaviors from early- to middle-
adolescence. Journal of Youth and Adolescence, 39, 751–763.Lo, Y., Mendell, N., & Rubin, D. (2001). Testing the number of components in a normal mixture. Biometrika, 88, 767–778.

M. O’Connor et al. / Journal of Adolescence 35 (2012) 701–712712
Lovibond, S., & Lovibond, P. (1995). Manual for the depression anxiety stress scales (2nd ed.). Sydney: Psychology Foundation.Magnusson, D. (2003). The person approach: concepts, measurement models, and research strategy. In S. Peck, & W. Roeser (Eds.), New directions for child
and adolescent development: Person-centered approaches to studying development in context. San Francisco: Jossey-Bass.Masten, A., Coatsworth, J., Neemann, J., Gest, S., Tellegen, A., & Garmezy, N. (1995). The structure and coherence of competence from childhood through
adolescence. Child Development, 66(6), 1635–1659.Masten, A., & Curtis, W. (2000). Integrating competence and psychopathology: pathways toward a comprehensive science of adaptation in development.
Development and Psychopathology, 12, 529–550.Mossakowski, K. N. (2008). Dissecting the influence of race, ethnicity, and socioeconomic status on mental health in young adulthood. Research on Aging,
30(6), 649–671.Muthén, B. (2006). Should substance use disorders be considered as categorical or dimensional? Addiction, 101, 6–16.Muthén, L., & Muthén, B. (2010). Mplus user’s guide (6th ed.). Los Angeles, CA: Muthen & Muthen.O’Connor, M., Sanson, A., Hawkins, M., Toumbourou, J., Letcher, P., & Frydenberg, E. (2011). Differentiating three conceptualisations of the relationship
between positive development and psychopathology during the transition to adulthood. Journal of Adolescence, 34, 475–484.O’Donnell, J., Hawkins, J., & Abbott, R. (1995). Predicting serious delinquency and substance use among aggressive boys. Journal of Consulting and Clinical
Psychology, 63, 529–537.Oesterle, S., Hill, K., Hawkins, J., & Abbott, R. (2008). Positive functioning and alcohol-use disorders from adolescence to young adulthood. Journal of Studies
on Alcohol and Drugs, (January), 100–111.Phelps, E., Balsano, A., Fay, K., Peltz, J., Zimmerman, S., Lerner, R., et al. (2007). Nuances in early adolescent developmental trajectories of positive and
problematic/risk behaviors: findings from the 4-H study of positive youth development. Child and Adolescent Psychiatric Clinics of North America, 16,473–496.
Pittman, K., & Fleming, W. (1991). A new vision: Promoting youth development. Testimony by Karen J. Pittman before the house select committee on children,youth, and families. Washington, DC: Centre for Youth Development and Policy Research.
Prior, M., Sanson, A., Smart, D., & Oberklaid, F. (2000). Pathways from infancy to adolescence: Australian temperament project 1983–2000. Melbourne, Victoria:Australian Institute of Family Studies.
Putnam, R. (1995). Tuning in, tuning out: the strange disappearance of social capital in America. PS: Political Science and Politics, 28(4), 664–683.Ryan, R. M., & Deci, E. L. (2001). On happiness and human potentials: a review of research on hedonic and eudaimonic well-being. Annual Review of
Psychology, 52, 141–166.Scheffe, H. (1999). The analysis of variance. Canada: John Wiley & Sons.Schermelleh-Engel, K., Moosbrugger, H., & Muller, H. (2003). Evaluating the fit of structural equation models: tests of significance and descriptive goodness-
of-fit measures. Methods of Psychological Research Online, 8(2), 23–74.Schulenberg, J., Bryant, A., & O’Malley, P. (2004). Taking hold of some kind of life: how developmental tasks relate to trajectories of well-being during the
transition to adulthood. Development and Psychopathology, 16, 1119–1140.Schwarz, G. (1978). Estimating the dimension of a model. The Annals of Statistics, 6(2), 461–464.Shonkoff, J. P., & Phillips, D. A. (2000). Fromneurons to neighborhoods: The science of early childhood development. Washington, DC, US: National Academy Press.Silbereisen, R., & Lerner, R. (2007). Approaches to positive youth development: a view of the issues. In R. Silbereisen, & R. Lerner (Eds.), Approaches to
positive youth development (pp. 3–30). UK: Sage.Smart, D., & Sanson, A. (2003). Social competence in young adulthood, its nature and antecedents. Family Matters, 64, 4–9.Smart, D., & Sanson, A. (2005). What is life like for young Australians today, and how well are they faring? Family Matters, 70, 46–53.Stone, W. (2001). Measuring social capital: Towards a theoretically informed measurement framework for researching social capital in family and community life
(Working Paper No. 24). Melbourne, Victoria: Australian Institute of Family Studies.Stone, W., & Hughes, J. (2002). Social capital: Empirical meaning and measurement validity (Working Paper No. 27). Melbourne, Victoria: Australian Institute
of Family Studies.Sweet, J. A., & Bumpass, L. L. (2002). The national survey of families and households – Waves 1, 2, and 3: Data description and documentation. Madison, WI:
Center for Demography and Ecology, University of Wisconsin-Madison.Whitley, R., & McKenzie, K. (2005). Social capital and psychiatry: review of the literature. Harvard Review of Psychiatry, 13, 71–84.Zarrett, N., Fay, K., Li, Y., Carrano, J., Phelps, E., & Lerner, R. (2009). More than child’s play: variable- and pattern-centred approaches for examining effects of
sports participation on youth development. Developmental Psychology, 45(2), 368–382.Zimmerman, S., Phelps, E., & Lerner, J. (2008). Positive and negative developmental trajectories in U.S. adolescents: where the positive youth development
perspective meets the deficit model. Research in Human Development, 5(3), 153–165.