the prevalence of psychiatric illness among continuing-care patients under the care of departments...
TRANSCRIPT

INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY. VOL 4 227-233 (1989)
THE PREVALENCE OF PSYCHIATRIC ILLNESS AMONG CONTINUING-CARE PATIENTS
UNDER THE CARE OF DEPARTMENTS OF GERIATRIC MEDICINE
JOHN BOND, ANN ATKINSON AND BARBARA A. GREGSON
Senior Lecturer in Sociology, Health Care Research Unit. 21 Chremont Phce, l lw University, Newcastle upon ljne, NE24AA. UK
Research Associate, Policy Services Unit, Newcastle City Council, Civic Centre, Newcastle upon ljne, NE2 8QN, UK Research Associate, Health Care Research Unit, 21 Chuemont Pklce, nte University, Newcastle upon ljne, NE2 4AA.
UK
SUMMARY Between 1983 and 1987,568 patients in three centres, who were under the care of consultant physicians with a special interest in elderly people, were referred to a randomized controlled trial as part of the evaluation of the three experimental NHS nursing homes. All patients referred to the trial were defined by the referring consultant as ‘long-stay’ or ‘continuing-care’ patients. The mental state of patients was assessed as part of the baseline assessments undertaken at entry to the trial. Two methods of assessment were used. First, the presence of organic psychiatric disorders and of affective disorders and psychoneuroses was assessed using the Survey Psychiatric Assessment Schedule. Second, the presence of ‘confusion’ was estimated using the the modified Crichton Royal Behavioural Rating Scale. The prevalence of organic psychiatric conditions was found to be 72% and of affective disorders and psychoneuroses 40%. This substantial proportion of people with psychiatric illness has major implications for the training of both medical and nursing staff working in non-psychiatric hospitals.
KEY WORDS-Depression: occurence in old age, dementia: occurence in old age, geriatric medicine, institutional care.
INTRODUCTION
The United Kingdom was one of the first industrial- ized countries to provide a specialist service for the medical care of the elderly people (Brocklehurst, 1975; Hall, 1988). Throughout the UK this service takes a variety of forms but, in general, medical departments which specialize in the care of elderly people set out to provide a service for a defined population and to offer a comprehensive range of facilities (Andrews and Brocklehurst, 1987). The majority of such departments care for their patients in district general hospitals and non-psychiatric long-stay hospitals.
The prevalence of psychiatric illness in old age has been widely estimated for both community and institutional populations (Kay and Bergman, 1980;
Crown copyright reserved.
Henderson and Kay, 1984; Bond, 1987; Brayne and Ames, 1988). However, only two British studies report the prevalence of psychiatric illness in non- psychiatric long-stay hospitals. A study of elderly people resident in geriatric wards in Newcastle upon Tyne (n=62) undertaken in 1960 found that 70% of patients had an organic psychiatric disorder and 15% an affective disorder or psychoneurosis (Kay et al., 1964). A Scottish population survey undertaken in 1976, which included a census of all elderly people staying overnight in non-psychiatric long-stay hospitals (n=102), estimated that 70% of patients had an organic psychiatric disorder and 27% an affective disorder (Bond and Carstairs, 1982; Bond, 1987).
Data presented in this article update these estimates, providing estimates of prevalence for 568 ‘long-stay’ patients referred to a three-centre randomized controlled trial as part of the evalua- tion of the three experimental NHS nursing homes (Bond, 1984).
0885-623O/ 89/ O40227-O73OS.O0 8 1989 by John Wiley & Sons, Ltd.
Received 18 November 1988 Accepted 9 February 1989

228 JOHN BOND, ANN ATKINSON AND BARBARA A. GREGSON
METHOD
Between 1983 and 1987, ‘long-stay geriatric’ patients were recruited to a pragmatic multicentred randomized controlled trial in three geographically dispersed ’centres. (Six centres were involved in the evaluation of the experimental NHS nursing homes but only centres A, C and E in which the homes were sited were included in this trial.) The purpose of the trial was to compare the outcomes of care for patients in continuing-care wards with residents in the experimental NHS nursing homes in order to assess whether NHS nursing homes could provide an appropriate alternative mode of care to that offered in conventional continuing-care wards. A full description of the implementation of this trial has been given elsewhere (Bond et al., I989a,b). In selecting subjects for the trial we identified the following operational criteria:
1. 2.
3.
4.
5 .
6.
7.
Patients should be aged 65 years or over. Patients should be under the care of a consultant physician with special interest in elderly people or referred to and assessed by him or her. Patients should be defined as ‘long-stay’ by the consultant physician. Patients’ last permanent residence should be within a defined catchment area. Patients should have been in hospital for at least 28 days for the present episode, but not for longer than two years. Patients should not be on a waiting list for alternative continuingcare accommodation such as a psychogeriatric bed. Patients were not eligible if they had been dis- charged permanently home after referral.
Administrative errors by the research team allowed 10 cases for which these criteria were vio- lated, particularly length of stay where six patients had been resident in hospital for longer than two years (Bond ef al., 1989b).
The characteristics of ‘long-stay’ patients vary between different hospitals and different wards (Atkinson et al., 1986). They are influenced by different factors but most notably the supply of alternative types of accommodation and comm- unity services mediated by the admission and dis- charge policies of various consultants. However, the population studied was fairly representative of admissions to British ‘long-stay’ non-psychiatric hospital beds.
Classijkation of mental state
An assessment of mental state was undertaken in two ways. First, the modified Crichton Royal Behavioural Rating Scale (CRBRS), which was completed by staff, was used to estimate the prevalence of ‘confusion’ (Wilkin and Jolley, 1979). Second, an % assessment of mental state was undertaken by interviewers using the Survey Psychiatric Assessment Schedule (SPAS) (Bond et al., 1980).
Crichton Royal Behavioural Rating Scale
The modified CRBRS consists of 10 items, five which reflect physical dependence (mobility, feed- ing, dressing, bathing, continence) and five which reflect mental disturbance (memory, orientation, communication, cooperation, restlessness). The scale has been used quite extensively in research and has proved to be reliable (Wilkin et al., 1978; Goldberg and Connelly, 1982; Willcocks et al., 1987). Ratings have been validated against clinical assessments showing the scale to be a good pre- dictor of the presence and severity of functional and mental impairment. Most specifically, the ‘confusion’ subscale (memory, orientation and communication) is a good indicator of the presence and seventy of a dementing illness (Wilkin and Jolley, 1979). Scores on the ‘confusion’ subscale are calculated by summing responses to the three components. Scores range from 0 to 11, a score of four or more indicating ‘moderate or severe confusion’.
The modified CRBRS is based on staff percep- tions, which were elicited through a structured inter- view with a lay interviewer. It is acknowledged that the derived ratings will therefore reflect institutional- ly ‘induced dependency’(Booth, 1985). That is, insti- tutions which encourage independence are more likely to assess subjects as being more physically and psychologically independent than those institu- tions which adopt a more ‘warehousing’ (Miller and Gwynne, 1972; Evers, 1981) or ‘custodial’ (Goff- man, 1961) approach.
Survey psychiatric assessment schedule
The reliability and development of the SPAS for use by lay interviewers has been described elsewhere (Bond el a/., 1980). The SPAS is a highly structured version of the Geriatric Screening Schedule (GSS),
PSYCHIATRIC ILLNESS AMONG CONTINUING-CARE PATIENTS 229
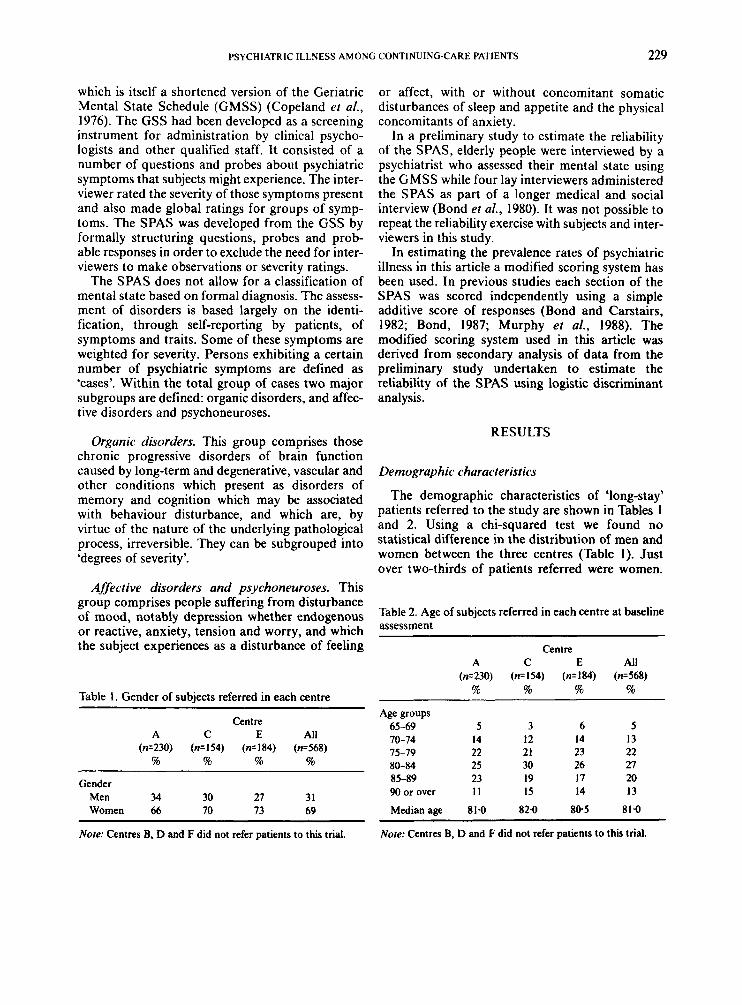
which is itself a shortened version of the Geriatric Mental State Schedule (GMSS) (Copeland ef al., 1976). The GSS had been developed as a screening instrument for administration by clinical psycho- logists and other qualified staff. It consisted of a number of questions and probes about psychiatric symptoms that subjects might experience. The inter- viewer rated the severity of those symptoms present and also made global ratings for groups of symp- toms. The SPAS was developed from the GSS by formally structuring questions, probes and prob- able responses in order to exclude the need for inter- viewers to make observations or severity ratings.
The SPAS does not allow for a classification of mental state based on formal diagnosis. The assess- ment of disorders is based largely on the identi- fication, through self-reporting by patients, of symptoms and traits. Some of these symptoms are weighted for severity. Persons exhibiting a certain number of psychiatric symptoms are defined as ‘cases’. Within the total group of cases two major subgroups are defined: organic disorders, and affec- tive disorders and psychoneuroses.
Organic disorders. This group comprises those chronic progressive disorders of brain function caused by long-term and degenerative, vascular and other conditions which present as disorders of memory and cognition which may be associated with behaviour disturbance, and which are, by virtue of the nature of the underlying pathological process, irreversible. They can be subgrouped into ‘degrees of severity’.
Affective disorders and psychoneuroses. This group comprises people suffering from disturbance of mood, notably depression whether endogenous or reactive, anxiety, tension and worry, and which the subject experiences as a disturbance of feeling
Table 1. Gender of subjects referred in each centre
Centre A c E All
(n=230) ( ~ 1 5 4 ) (n=184) ( ~ 5 6 8 ) % % % %
Gender Men 34 30 21 31 Women 66 70 13 69
or affect, with or without concomitant somatic disturbances of sleep and appetite and the physical concomitants of anxiety.
In a preliminary study to estimate the reliability of the SPAS, elderly people were interviewed by a psychiatrist who assessed their mental state using the GMSS while four lay interviewers administered the SPAS as part of a longer medical and social interview (Bond et al., 1980). It was not possible to repeat the reliability exercise with subjects and inter- viewers in this study.
In estimating the prevalence rates of psychiatric illness in this article a modified scoring system has been used. In previous studies each section of the SPAS was scored independently using a simple additive score of responses (Bond and Carstairs, 1982; Bond, 1987; Murphy et al., 1988). The modified scoring system used in this article was derived from secondary analysis of data from the preliminary study undertaken to estimate the reliability of the SPAS using logistic discriminant analysis.
RESULTS
Demographic characteristics
The demographic characteristics of ‘long-stay’ patients referred to the study are shown in Tables 1 and 2. Using a chi-squared test we found no statistical difference in the distribution of men and women between the three centres (Table 1). Just over two-thirds of patients referred were women.
Table 2. Age of subjects referred in each centre at baseline assessment
Centre A C E All
( ~ 2 3 0 ) ( ~ 1 5 4 ) (n=184) ( ~ 5 6 8 ) % % % %
Age groups 65-69 5 3 6 5 10-14 14 12 14 13 15-19 22 21 23 22 80-84 25 30 26 21 85-89 23 19 17 20 90 or over 11 I5 14 13 Median age 81.0 82.0 80.5 81.0
~
Note: Centres B, D and F did not refer patients to this trial. Note: Centres B, D and F did not refer patients to this trial.

230
156
104
P 2 3 n
52
0 -
JOHN BOND, ANN ATKINSON AND BARBARA A. GREGSON
*
-
-
-
( 1 CENTRE A (n- 230)
Fig. I . Length of stay of referred subjects at baseline assessment
Using a Kruskal-Wallis one-way analysis of variance on the ungrouped data we found no significant differences in age between the three centres (Table 2). The median age of patients referred was 81.0.
Fig. 1 is drawn as box-and-whisker plots of the length of stay in hospital for the present episode of ‘long-stay’ patients at referral to the study. The upper and lower quartiles of the data are portrayed by the top and bottom of the rectangle and the median is the horizontal line within the rectangle. The area of each box is proportional to the number of patients in each centre and the lines extend from the ends of the box to the upper and lower values. Using a Kruskal-Wallis one-way analysis of variance on the ungrouped data we found that the length of stay of referred patients in centre A was significantly shorter than centres C and E (p < 0.0001). This probably reflects a difference in policies practised by referring doctors rather than differences in the type of ‘long-stay’ patient referred.
Functional ability
Fig. 2 shows box-and-whisker plots of the functional ability subscale (mobility, feeding, dressing and bathing) from the modified CRBRS for referred patients. Using a Kruskal-Wallis one-
I CENTRE C (ru 153)
CENTRE E (n. 183)
way analysis of variance on the ungrouped data we found that functional ability scores were higher, representing higher frailty, in centres A and C than in centre E (p < 0.0001). The range of scores obtained show that ‘long-stay’ patients referred to the study were very physically frail. For example, 62% of all patients were bedfast or chairfast and a further 23% required assistance with walking. Differences in the distribution of scores between centre reflect the way that patients were referred to the study in centre E (Bond et al. 1989b).
Mental state
Tables 3 and 4 show the mental state of referred patients as assessed by fieldworkers using the SPAS. Data are not available for 164 patients for whom assessment was not possible because of mental or physical frailty. Using a chi-squared test we found no significant differences in the pre- valence of organic or affective psychiatric disorders between the three centres. Forty per cent of assessed patients were identified as having an affective dis- order or psychoneurosis and 72% as having an organic disorder. Seventeen per cent were identified as having no psychiatric illness.
Table 5 shows the prevalence of ‘confusion’ as indicated by scores on the confusion subscale of the CRBRS. Using a chi-squared test there was no signi-

PSYCHIATRIC ILLNESS AMONG CONTINUINGCARE PATIENTS 23 1
lnmm
t CENTRE lnm 1541
Fig. 2. Functional ability scores of referred subjects at baseline assessments
ficant difference in the prevalence of ‘confusion’ between the three centres. Fifty-five per cent of patients were assessed as ‘moderately or severely confused’.
DISCUSSION
The data reported in this article concern patients referred to a randomized controlled trial of the
Table 3. Severity of any organic psychiatric disorder for subjects referred in each centre at baseline assessment
Centre A C E All
( ~ 1 6 1 ) ( ~ 1 0 7 ) ( ~ 1 3 6 ) (n=404) % % % %
No organic 26 36 25 28
Mild organic 36 26 26 30 disorder
disorder
Severe organic 38 38 49 42 disorder
Notes: I. Mental frailty could not be assessed for 164 ‘long-stay’patients who were not interviewed. 2. Centres B, D and F did not refer patients to this trial.
i ENTREE lnm I 8 4 1
three experimental NHS nursing homes. The purpose of the three experimental NHS nursing homes is to offer an alternative mode of continuing care to that provided in conventional long-stay or continuing-care wards for patients currently under the care of consultant physicians with a special interest in elderly people. Thus patients referred to the study were defined as ‘long-stay’ or ‘continuing- care’ patients by individual consultant physicians.
The data presented show that ‘long-stay’ patients were all physically frail. Over 70% were also found to have a psychiatric illness: 30% were assessed, using the SPAS, as having a mild organic disorder and a further 42% a severe organic disorder. Assess-
Table 4. Presence of an affective disorder or psycho- neurosis for subjects referred in each centre at baseline assessment
~
Centre A C E All
(n=ISS) ( ~ 1 1 8 ) ( ~ 1 2 5 ) ( ~ 3 9 8 ) % % % %
No affective 57 56 69 60
Some affective 43 44 31 40 disorder
disorder
Note: Centres B, D and F did not refer patients to this trial.

232 JOHN BOND, ANN ATKINSON AND BARBARA A. GREGSON
Table 5. Presence of severe or moderate confusion as determined by the modified Crichton Royal Behavioural Rating Scale for subjects referred in each centre at baseline assessment
Centre A C E All
(n=230) ( ~ 1 5 4 ) ( ~ 1 8 3 ) (n=567) % % % %
None or mild 45 48 41 45 confusion (0-3)
severe confusion (4 or more)
Moderate or 55 52 59 55
Notes: I . For one ‘long-stay’ patient no assessment of ‘confusion’ was provided by nursing staff. 2. Centres B, D and F did not refer patients to this trial.
ments made by nursing staff using the confusion subscale of the CRBRS suggest that some 55% of patients were ‘moderately or severely confused’. Also, 40% of patients were assessed using the SPAS as having an affective disorder or psychoneurosis.
The prevalence of ‘moderate or severe confusion’ as assessed by the confusion subscale of the CRBRS (55%) is higher than the prevalence of moderate or severe organic disorders as assessed by the SPAS (42%). This difference in prevalence reflects the emphases of the two methods of assess- ment: whereas the CRBRS emphasizes the be- havioural consequences of an organic impairment as assessed by staff, the SPAS measures cognitive performance of patients through personal inter- views. It also reflects the absence of an assessment, using the SPAS, for 30% of patients. Forty-four per cent of patients interviewed compared with 83% of patients not interviewed were assessed as ‘moder- ately or severely confused’ using the confusion subscale of the CRBRS.
One of the disadvantages of using the SPAS or the CRBRS is in identifying a main diagnosis when there is an overlap between the two groups of disorders assessed, a weakness shared by a number of assessment methods. However, for the purposes of estimating prevalence and assessing population changes they provide a more cost-effective method of data collection than formal psychiatric inter- views and diagnosis (Bond, 1987).
Since all-patients assessed were physically frail and over 70% were also mentally frail, these data
suggest a strong association between mental and physical frailty in old people, something which has been monitored in a number of other studies (Kay and Bergmann, 1966; Bond and Carstairs, 1982; Ouslander, 1982; Gurland et al., 1983; Bond, 1987). This association has at least two implications for policies concerning the continuing care of elderly people.
At oresent most DeDartments of Geriatric Medi- cine in the United Kingdom are separate from those Departments of Psychiatry which provide a specialist service for elderly people. Andrews and Brocklehurst (1987) in their recent study of geriatric medicine reported no examples of specialist psychiatric services which were integral to the medical services for elderly people. In some areas separate specialist psychiatric services for elderly people are not available (Wattis, 1988). Given the presence of both physical and mental frailty among the majority of ‘long-stay’ patients, future policy developments should encourage the integration of these two specialities along the lines of the service provided in Nottingham (Arie and Jolley, 1982), so that all patients with both physical and psychiatric illness might receive the specialist services required.
The second implication of these data is for the education and training of medical, nursing and therapy staff. Each of these groups are currently exposed to the care of elderly people during training, but the emphasis is towards acute physical medicine and rehabilitation. These data indicate the need to place greater emphasis during training on the problems of both mental and physical frailty in old age by ensuring that staff receive experience of working with continuing-care patients.
ACKNOWLEDGEMENTS
The study was funded by the Department of Health. We would like to thank those physicians who collaborated with us by referring patients to the study: Dr A. K. Admani, Dr A. J. Anderson, Dr W. G. T. Annan, Dr A. J . Balouch, Dr M. J . Clarke-Williams, Dr J . R. Cox, Dr J. A. H. Grunstein, Dr R. S. Gulati, Dr M. D. John, Dr L. Jones, Dr P. H. Ritchie, Dr P. S. Wilkins and Dr R. P. Williams. We are also grateful to the nursing staff in each of these authorities for their assistance in the collection of patient data. We would like to acknowledge the help of other members of the pro- ject team who assisted: Pam Ackroyd, Senga Bond,

PSYCHIATRIC ILLNESS AMONG CONTINUING-CARE PATIENTS 233
Eva Brown, Joyce Crawley, Cam Donaldson, Margaret Fall, Joan Gray, Margaret Hally, Janet James, Lesley Speakman, David Newell, Judy Thompson and Lora Wake. Finally, we would also like t o thank those patients who so freely contri- buted t o this study.
REFERENCES
Andrews, K. and Brocklehurst, J. (1987) British Geriatric Medicine in the 1980s. King Edward’s Hospital Fund, London.
Arie, T. D. H. and Jolley, D. J. (1982) Making services work: Organisation and style of psychiatric services. In The Psychiatry of Later Life. (R. Levy and F. Post Eds). Blackwell, Oxford, pp. 222-251.
Atkinson, D. A., Bond, J. and Gregson, B. A. (1986) The dependency characteristics of older people in long- term institutional care. In Dependency and Inter- dependency in Old Age - Theoretical Perspectives and Policy Alternatives. (C. Phillipson, M. Bernard and P. Strang Eds). Croom Helm, London, pp. 257-269.
Bond, J. (1984) Evaluation of long-stay accommodation for elderly people. In Gerontology: Social and Behavioural Perspectives. (D. B. Bromley Ed.). Croom Helm, London, pp. 88-101.
Bond, J. (1987) Psychiatric illness in later life. A study prevalence in a Scottish population. Int. J. Gerzizr. Psychiat. 2,39-57.
Bond, J., Atkinson, A., Gregson, B. A. and Newell, D. J. (1989a) Pragmatic and explanatory trials in the evaluation of the experimental NHS nursing homes. Age Ageing 18,89-95.
Bond, J., Gregson, B. A., Atkinson, A. and Newell, D. J. (1989b) The implementation of a multi-centred ran- domised controlled trial in the evaluation of the experimental NHS nursing homes. Age Ageing 18,
Bond, J., Brooks, P., Carstairs, V. and Giles, L. (1980) The reliability of a survey psychiatric assessment schedule for the elderly. Brit. J. Psychiat. 137, 148-162.
Bond, J. and Carstairs, V. (1982) Services for the Elderly: A Survey of the Characteristics and Needs of a Popula- tion of 5000 Old People. Scottish Health Service Studies No. 42. Scottish Home and Health Depart- ment, Edinburgh.
Brayne, C. and Ames, D. (1988) The epidemiology of mental disorder in old age. In Mental Health Problems in Old Age. (B. Gearing, M. L. Johnson and T. Heller, Eds.) Wiley, Chichester.
Brocklehurst, J . C. (Ed.) (1975) Geriatric Care in Advanced Societies. MTP, Lancaster.
Copeland, J . R. M., Kelleher, M. J., Kellett, J. M., Gourlay, A. J. et al. (1976) A semi-structured clinical interview for the assessment of diagnosis of mental
96-102.
state in the elderly: The Geriatric Mental State Schedule 1. Development and reliability. Psychol. Med. 6,439499.
Evers, H. K. (1981) The creation of patient careers in geriatric wards: Aspects of policy and practice. SOC. Sci. Med. 15A, 581-588.
Goffman, E. (1961) Asylums: Essays on the Social Situation of Mental Patients and Other Inmates. Anchor, New York.
Goldberg, E. M. and Connelly, N. (1982) The Effective- ness of Social Care for the Elderly. Heinemann. London.
Gurland, B., Copeland, J., Kuriansky, J., Kelleher, M., Sharpe, L. et al. (1983) The Mind and Mood of Ageing. Mental Health Problems of the Community Elderly in New York and London. Croom Helm, London.
Hall, M. (1988) Geriatric medicine today. In The Ageing Population. Burden or Challenge? (Wells, N. and Freer, C. Eds). Macmillian, London.
Henderson, A. S. and Kay, D. W. K. (1984) The epidemiology of mental disorders in the aged. In Handbook of Studies on Psychiatry and Old Age. (D. W. K. Kay and G. D. Burrows Eds). Elsevier, Amsterdam.
Kay, D. W. K., Beamish, P. and Roth, M. (1964) Old age mental disorders in Newcastle upon Tyne 1. Brit. J. Psychiat. 110, 146-158.
Kay, D. W. K. and Bergman, K. (1966) Physical dis- ability and mental health in old age. J. Psychosom. Res. 19, 3-12.
Kay, D. W. K. and Bergman, K. (1980) Epidemiology of mental disorders among the aged in the community. In Handbook of Mental Health and Ageing. (J. E. Birren and E. R. B. Sloan Eds). Prentice-Hall, Englewood Cliffs.
Miller, E. J. and Gwynne, G. V. (1972) A Life Apart. A Pilor Study of Residential Institutions for the Physical- ly Handicapped and the Young Chronic Sick. Tavi- stock, London.
Murphy, E., Smith, R., Lindesay, J. and Slattery, J. (1988) Increased mortality rates in late-life depression. Brit. J. Psychiat. 152, 347-353.
Ouslander, J. G. (1982) Illness and psycho-pathology in the elderly. Psychiat. Clin. N. America 5, 145-158.
Wattis, J. P. (1988) Geographical variations in the provision of psychiatric services of old people. Age Ageing 17, 171-180.
Wilkin, D. and Jolley, D. J. (1979) Behaviour Problems Among Old People in Geriatric Wards, 1976-1978. Research Report No. 1. Departments of Psychiatry and Community Medicine, University of Manchester.
Wilkin D., Mashiah, T. and Jolley, D. J. (1978) Changes in the behavioural characteristics of elderly popula- tions of local authority homes and long-stay hospital wards, 1976-1978. Brit. Med. J. 2, 127441276,
Willcocks, D., Peace, S. and Kellaher, L. (1987). Private Lives in Public Places. Tavistock, London.