the patient interview
TRANSCRIPT
Chapter 1
Learning Objectives
• Explainthebasiccommunicationskillsneededwhenperformingapatientinterview.• Describethecomponentsofthepatientinterview.• Conductathoroughmedicationhistory.• Compareandcontrastthedifferentpatientinterviewapproachesinvariousclinicalsettings.• Adapttheinterviewtechniquebasedontheneedsofthepatient.
ThePatientInterview
Sneha Baxi Srivastava, PharmD, BCACP
• ActiveListening• Rapport• Empathy• Open-EndedQuestions• LeadingQuestions• ProbingQuestions• NonverbalCommunication• ChiefComplaint• HistoryofPresentIllness
• PertinentPositive• PertinentNegative• PastHistory• MedicationHistory• FamilyHistory• PersonalandSocialHistory• ReviewofSystems• PhysicalExam• QuEST/SCHOLAR-MAC
Key terms
intrOductiOn
The patient interview is the primaryway of obtaining comprehensive informationaboutthepatientinordertoprovideeffectivepatient-centeredcare,andthemedica-tionhistorycomponent is thepharmacist’sexpertise.Amethodologicalapproach isused toobtain information from thepatient, usually startingwithdetermining thepatient’schiefcomplaint,alsoknownasthereasonforthehealthcarevisit,andthen

delving further intoanexplorationof thepatient’s specificcomplaintandproblem.A comprehensive patient interview includes inquiring about the patient’s medical,medication,social,personal,andfamilyhistory,aswellasathoroughreviewofsystemsandpossiblyaphysicalexamination.Themedicationhistory is thepartof thepatient interview thatprovides the
pharmacist theopportunity toutilizehis orher expertise byprecisely collectingeachcomponentofthemedicationhistory(however,amedicationhistorymayalsobe collected independent of a comprehensive patient interview). The questionsthat you ask the patient, aswell as the technique used,will enable you to learnexactlyhow,when,andwhyapatienttakeseachmedication,aswellasaboutanyadverse reactions, allergies, or issueswithmedication cost the patientmay haveexperienced.Theapproachtothepatientinterviewandmedicationhistorywillchangebased
onthesettinginwhichyouarepracticing.Forexample,ifthesettingisacommunitypharmacyandyouare responding toaproblemthatmayallow for self-care,yourquestionswillbedirectedatmeticulouslycharacterizingthepatient’scomplaintandobtainingspecific informationthatwill influenceyourassessmentandplanforthepatient.However,ifyouareinahospital,thefocusoftheinterviewmayneedtobemodifiedbasedonthepatient’sconditionandtheparticularunitordepartment inwhichheorsheisbeingcaredforsothatthepatient’sneedsmaybemet.Regardless of the setting, your goal during the interviewwill be to provide
patient-centered care; this can be accomplished by combining your pharmaco-therapeutic knowledge with a solid foundation of excellent communication andpatient-interviewing skills. Excelling in these communication skills is a learnedtechniquethattakestimeandpracticetomaster.Oncetheseskillsareemployedinpractice, the relationship that is developed with the patient is often stronger,allowing for the patient to have increased confidence and trust in your role asahealthcareprovider.Thepurposeofthischapteristodescribethevariouscomponentsofthecompre-
hensivehealthhistoryandtoprovideanoverviewoftheskillsandtechniquesrequiredwhencommunicatingwiththepatient.Thischapterwillfocusonthebestpracticestofollowwhencollectinginformationfromthepatient.
cOmmunicatiOn sKiLLs
Communicationskillsarethefundamentallinkbetweenthepharmacist’sexpertiseaboutdrugsandhisorhercontributiontoprovidingexcellentpatient-centeredcare.Althoughcommunicatingwithapatientmayseemlikeasimpletask,itactuallytakes
2 chapter 1 / the patient interview

practiceandknowledgetocommunicatewiththepatientinamannerthatencour-agesrespectforthehealthcareproviderandthatenablesthepharmacisttoobtainanaccurateandcompletehistory.Somepractitionersareabletonaturallycommu-nicatewithpatientsmore effectively,whereasothershavedifficulty communicat-ingwithpatientsdue to a varietyof reasons, including theirpersonality, comfortlevel, and confidence.However, regardless of one’s natural abilities, communica-tionskillsandquestioningtechniques,especiallywhenitcomestocommunicatingwithpatients,arelearnedandtaketimetodevelop.Avarietyofexcellentin-depthresourcesdescribecommunicationskills.Thischapterexaminesthemostpertinentskills required to conduct a comprehensive medication history. These skills andquestioningtechniquesinclude:
• Activelistening• Empathy• Buildingrapport• Open-endedquestions• Closed-endedquestions• Leadingquestions• Silence• “Why”questions• Nonverbalcommunicationcues
active Listening
Thefirstcommunicationskilltobemasteredislistening,specificallyactivelisten-ing.Listeningisdefinedashearingwhatisbeingsaid,whereasactive listeningisadynamicprocessthatincludesbothhearingwhatisbeingsaidaswellasprocessingand interpreting thewords that are spoken (and/or unspoken) to understand thecompletemessage that is being delivered.Whereas listening is a passive process,activelisteningrequiresthelistenertoconsciouslychoosetogivethepatientatten-tionandconcentrationthatisfreeofdistractionsandinterruptions,bothexternalandinternal.External distractions are the easier of the two to avoid. External distractions
include ringing telephones, flickering computer screens, and other infringing per-sonaland/orotherduties.Theseexternaldistractionscanbeavoidedbyinteractingwithyourpatientinaplacethatisfreeofsuchdistractions.Internal distractions occur for two major reasons: (1) many matters, unre-
latedtothepatient in frontofyou,mayoccupyyourmindand(2) it isdifficult
communication skills 3

to perceivewhat the patient is sayingwithout tainting his or hermessagewithyourpersonaljudgment.Thefirstreasoncanbeaddressedbymakingaconsciousefforttoconcentratesolelyonyourinteractionwiththepatient.Thisismoredif-ficult toaccomplish than it sounds,but,withpractice, turningon the“listeningswitch”inyourmindwillbecomeeasier.1Thesecondreasonismoredifficulttoaddress, because instinct often leads us to judge or evaluatewhat the patient issaying based on our own frame of reference. Biases, prejudices, and judgmentscloudthemessagethatisbeingdeliveredbythepatient,which,inturn,affectthepatientinteraction,andpossiblyclinicaloutcomes.2Forexample,asyouprepareforapatientwhohasbeenreferredtoyouforsmokingcessationcounseling,youread in several progressnotes that thepatient “refuses to giveup smoking.”Asyoumeetwiththatpatient,inyourmindyoumaybethinkingthat“it’ssodifficulttogiveupsmokingandmostpeopledon’treallywanttogiveupsmoking”basedonyourpreviousencounterswithotherpatients.Afterreadingthepatient’snotes,your preconceptionmay be strengthened. Therefore, as your patient is talkingabout reasonswhy it is difficult for him to quit smoking, yourmind is hearingwhatisbeingsaidbutisinterpretingitasexcusesratherthanreasonsthatyoumaybeabletoaddresswiththepatienttoassisthiminquittingsmoking.Onewaytoovercome internal distractions is by being present in themoment, during yourpatientvisit,addressingyourpatient’scurrentconcernswithoutfocusingonyourpreconceivednotions.
empathy
empathyisdefinedasthe“intellectualidentificationwithorvicariousexperiencingofthefeelings,thoughts,orattitudesofanother.”3Thetermsempathyandsympathyareoftenconfused.Sympathyiswhenyoufeelsorryforthepatientbutdonotfeelthesameemotionsorarenotinthesamesituation,whereasempathyiswhenyouplaceyourselfinyourpatient’ssituationandrespondbasedoneithersimilarpersonalexperiencesorthroughvicariousunderstanding.Whenyouexpressempathy,itallowsyourpatienttofeelasthoughyouunderstandhisorheruniqueexperienceandthatyouareapplyingyourexpertisetothepatientasanindividual.Empathycanbeshowninseveralways,andeachwaywilldependuponthepartic-
ularpatientaswellasthesituation.Forexample,noddingyourhead,makingastate-ment,oraskingafollow-upquestioncanshowempathy.2Additionally,itisimportanttodistinguishbetween an empathetic statement and the assumption that youknowexactlywhatthepatientisfeeling.Forexample,sayingtoyourpatientwhohasbeen
4 chapter 1 / the patient interview

diagnosedwithcancer,“Iknowjusthowyouarefeeling.Mygrandfatherhadcanceranditwassuchashocktoallofus.Atfirst,hewasjustsooverwhelmedandupset”maymakethepatientfeellikeyouarenottrulylisteningtoher,butratherassumingthatshewillrespondlikeanyoneelsewithacancerdiagnosis.Itmaybebettertosay,“Iknow fromsomepersonalexperiences that findingoutaboutcancercanbeveryoverwhelming.Howareyoufeeling?”Althoughthereisnoonewaytoshowempathy,focusingonthekeyfactorsofallowingpatientstofeelunderstoodwhilemaintainingtheuniquenessoftheirexperience(s)mayallowforabetterpatientinteraction.
building rapport
Thefirstimpressionyoumakeonyourpatientwillweighontherestofthepatientinterviewaswellasaffectyourrelationshipwiththepatient.Buildingagoodrapport sets thetoneforthe interviewandallowsthepatienttofeelcomfortablewithyou,therebymaking the lines of communicationmore open and honest. Patientsmaysometimeswithholdinformationiftheyfeeluncomfortableoranxiousaboutsharingtheircomplaintsbecauseofalackoffeelingrespected,feelingasthoughtheirwordsarenotbeingheard,orquitesimplynotknowingwhoyouareandwhatyourroleisintheircare.Therefore,startingtheinterviewbygreetingthepatientbyname,makingsureyouarepronouncingthepatient’snamecorrectly,askinghowheorshepreferstobeaddressed,andaddingatitletohisorhername,ifpreferred,willindicateyourinterestinthepatientandshowthatyoucare.Youshouldalsogiveyournameandtitleandthenbrieflydescribethepurposeoftheinterview.Forexample,youcouldsay,“HelloMrs.Smith,mynameisAnkurKumar.Iamthepharmacistwhoispartofyourmedicalteam,andIamheretoaskyouafewquestionsaboutwhatbroughtyoutothehospitalanddiscussthemedicationsyouhavebeentakingathome.”Ifthereareothersintheroom,youshouldgreeteachpersonintheroom,andthenaskyourpatientforpermissiontocontinuewiththeinterviewinthepresenceofothers.Forexample,youmaysay,“Ihaveafewquestionsforyou,Mrs.Smith.Isitokayformetospeaktoyouwithyourfamily/friendsintheroomorwouldyouprefertobealonewhilewetalk?”Evenifyouhavemetthepatientbefore,youmaywanttoremindthepatientof
yourrole,especially ifyouare inahospitalsettingwherethepatientmaybeover-whelmedbythemanyprovidersparticipatinginhisorhercare.4Makingappropri-ate introductions, interacting respectfullywith the patient, andmaking the patientfeelcomfortablewillbuildexcellentrapport, leadingtoastrongfoundationforthepatient–pharmacistrelationship.
communication skills 5

Open- and closed-ended Questions
Open-ended questionsarequestionsthatrequirethepatienttoanswerwithmorethanasimpleyesornoornodofthehead,whereasclosed-ended questionsgener-allylimitthepatient’sresponsetoeitherayesornooranodofthehead.Ingeneral,open-endedquestioningisthepreferredtechniquetouseduringpatientinterviewstocompelthepatienttoprovidemorein-depthandinsightfulresponses.Becauseopen-endedquestionsdonotlimitthepatienttorespondingwithayesorno,theyencour-agethepatienttodisclosemoreinformation.Forexample,youcanstarttheinterviewbyaskinganopen-endedquestion,suchas“Howareyoufeelingtoday?”oraclosed-endedquestion,suchas“Areyoufeelingwelltoday?”Thefirstapproachallowsforthepatienttoanswerinfreeformandpossiblygiveyoumoredetailabouttheconditionofhisorherhealth,whereasthesecondwayleadsthepatienttoanswerwitheitherayesorno,therebylimitingtheinformationthatyouobtainfromthepatient.2This,inturn,mayleadtoarapidsequenceofmoreclosed-endedquestions.For example, if you ask the patient a closed-ended question such as, “Do you
take yourmedications as directed by your physician?” youwillmost likely receivearesponseof“yes.”Althoughthepatientmayindeedbetakingeachmedicationasdirectedbyhisorherphysician,youmaybemissingtheopportunitytodiscoverhowthepatientisactuallytakingeachmedication.Instead,ifyouaskthepatientanopen-endedquestion,suchas“Howareyoutakingthismedication?”theanswerwilllikelyincludemoredetails,suchasthedoseandfrequencyofthemedication.Bygatheringmore informationwith open-ended questioning, youmay learn that there are dis-crepanciesbetweenhowthepatientisactuallytakingthemedicationandhowithasbeenprescribed.Oftentimes,apatientanswers,“Yes,Iamtakingitasdirected,”butyouthendiscoverthatthisisnotthecase,perhapsasaresultofdishonestybutmorelikelybecausethepatientbelievesthatheorsheistakingthemedicationcorrectly.Theuseofopen-endedquestionsenablesyoutogathermoreinformationfromthepatientandtobemorecompleteandaccurateinyourassessment;this,inturn,leadstoappropriatepatient-specificcare.Closed-endedquestionsdoplayaroleincommunicatingwithapatient;however,
theuseofclose-endedquestionsshouldbespecifictotheinformationyouwanttocol-lect.Forexample,ifyouwouldliketoknowwhetherthepatienttookhisorherbloodpressuremedicationinthemorningtomoreaccuratelyassesshisorherbloodpressurereading,youmightask,“Didyoutakeyourbloodpressuremedicationsthismorning?”Additionally, you can use open-ended questions to determine the presence or
absenceofcertainsymptomsortofurtherexploreasymptomthatthepatientisexpe-riencing.Forexample,afteraskinganopen-endedquestionsuchas“Whatsymptoms
6 chapter 1 / the patient interview

areyoucurrentlyexperiencing?”andhearingtheresponse“Myheadhurts,”anappro-priateclosed-endedfollow-upquestionwouldbe“Isthepainbehindyoureyes?”
Leading Questions
Leading questionsarethosethatsuggestaparticularanswer.Thesequestionsleadapatienttoprovidearesponsethatheorsheperceivestobetheanswerthattheinter-viewerwantstohear.Anexampleofaleadingquestionis“Youdonotmissanydosesofyourmedication,doyou?”Byphrasingthequestioninthismanner,thepatientfeelsobligedtosay,“No,Idon’t”becausethequestionimpliesthatthepatientshouldnotbemissingdoses,and,ratherthancontradictingyourexpectation,thepatientmerelyagrees.Therefore,toobtainanaccurateresponsetoyourquestions,leadingquestionsshouldbeavoided.
silence
Theroleofsilenceduringyourinteractionwiththepatientismoresignificantthanyoumayrealize.Byallowingmomentsofsilenceafteraskingaquestion,thepatientis able to reflect upon your question and provide amore thoughtful and accurateresponse.However,silencemayalsoindicatethatthepatienthasnotunderstoodyourquestion.Nonverbalcueswillhelpyoudeterminethedifference.Youcanusenonver-balcuestogaugeeachpatientindependentlytodeterminetheappropriatelengthoftimetobesilentand/orwhentobreakthesilence.Determiningtheappropriatelengthofsilencetouseisdefinitelyanart.Ingeneral,thesilenceshouldbelongenoughtoprovidethepatientachancetogatherhisorherthoughtsbutnotsolongastomakethepatientfeeluncomfortable.
“Why” Questions
As you are interviewing your patient, avoiding “why” questions may prevent thepatientfromfeelingasthoughheneedstodefendhischoicesandactions.Althoughitmaybenecessarytolearnthereasoningbehindthepatient’schoicesandactions,thewordingthatyouusemayimpacttheresponse.Forexample,ifyoudesiretolearnwhyapatientismissingdosesofhydrochlorothiazide,insteadofasking“Whydoyoumissyourdoses?”youmightask“Whatcausesyoutomissyourdoses?”or“Whataresomereasonsformissingyourdosesofthehydrochlorothiazide?”Thedifferenceissubtle,butitmaybeenoughtoaffectthewaythepatientperceivesthequestion.Withthe“why”method,thepatientmayfeeltheneedtodefendhim-orherself,whereas
communication skills 7

the“what”methodallowsthepatienttoreflectonhisorherreasonswithoutfeelingasthoughyouareofferingjudgment.
nonverbal communication
Nonverbal communicationisthesendingofmessagestoorfromyourpatientwith-out theuseofwords.This typeofcommunicationplaysan important role inyourinteractionswithyourpatientsbecause it canbe aspowerful as thewords that arespoken.Nonverbalcommunicationincludestoneofvoice,choiceoflanguage,facialexpressions,bodypostureandposition,gestures,eyecontact,appearance,andoverallbehavior.1Apatient’sperceptionofnonverbalcommunicationmaybeinfluencedbyindividualandculturaldifferences.Therefore,youshouldbesensitivetoculturaldif-ferencespriortomakinginferencesaboutthepatientbasedonnonverbalcommunica-tion.table 1.1describesthevarioustypesofnonverbalcommunicationandprovidesexamplesfortoneofvoice,choiceoflanguage,andfacialexpression.
the issue of reliability
Duringthepatientinterview,youmustassessthereliabilityoftheinformationthatisbeingconveyedtoyou.Manyfactorsmayaffectapatient’sreliability,includingcer-tainpsychiatricconditions,impairedcognitivefunction,inadequatememoryrecall,orevenalackofunderstandingofthequestionsbeingasked.Therefore,itisimportanttoassessthepatient’sreliabilityduringtheinterview.Listeningforandrecognizingcluesthatthepatientmaynotberelayingaccurateinformation,nomatterthereason,takesexperience.Onewaytoaddresspotentialunreliabilityistocross-referencetheinformationfromavarietyofsources,includingthepatient’sprofile,medicalrecords,andinformationfromthepharmacy.Insomecases,itmaybenecessarytoincludeacaregiverorfamilymemberintheinterviewsession.ThiswouldneedtobedoneinamannerthatisconsistentwiththeHIPAAproceduresatyourinstitution.
the patient intervieW
Thepatient’sstoryisconsideredtobethekeytothemedical interview,andaskingtherightquestionsandactivelylisteningtothepatientcanbestobtainthisstory.Asyouinterviewthepatient,youwillcometorealizethatanorganizedapproachpro-vides a solid foundation, but youmust follow the patient’s story in the order it isbeingtoldversusthepatientansweringyourquestionsinapredeterminedorder.Thisbeingsaid, it isnecessary toknowthecoreelementsof thesystematicapproachto
8 chapter 1 / the patient interview

nonverbal communication
description
example
Tone of voice One may speak in a tone that is persuasive, assertive, passive, condescending, kind, patient, impatient, confident, or unconfident. Although the words that are spoken are important, the tone in which they are spoken may influence the patient’s interpretation of what is being said. Similarly, you may be able to assess how a patient is feel-ing or reacting based on his or her tone of voice. A patient may speak in a tone that sounds encouraged, dejected, sad, excited, angered, or confused. By understanding the patient’s tone, you may be able to adjust your interaction with the patient to improve communication.
“Smoking is harmful to your health.”
Practice saying this in various tones. The patient’s interpretation will vary based on your tone of voice. A conde-scending tone may cause the patient to feel as though you are talking “down” to him or her, such that the patient may not want to discuss this any fur-ther with you, which, in turn, may make you miss an opportunity for smoking cessation counseling. In contrast, say-ing this in a confident and assertive tone may cause the patient to at least hear what you are saying versus being offended by the way you have said it.
Choice of language
The language used may be simple or complex, clear or confusing, or easy or difficult to follow. The meaning of the words may be influenced by the language used.
“Detrimental effects on health have been caused by tobacco use. The studies have shown that smoking leads to death, can-cer, and hypertension. Choosing to cease smoking may lead to improvements in your well-being.”
The use of complex language that is more difficult to follow may not only cause the patient to be confused about the message that is being conveyed, but also to feel as though he or she cannot connect with you, lead-ing the patient to believe that you are disinterested in his or her care.
The following statement is better: “Smoking causes harm to the body, including high blood pressure, cancer, and even death. Choosing to quit smok-ing will help your health be better.”
tabLe 1.1 types of nonverbal communication
(Continues)
the patient interview 9

Facial expressions
Many facial expressions are pos-sible: smiling/frowning, looks of astonishment, disappointment, disapproval, surprise, shock, anger, fear, happiness, and sadness. These expressions may happen involun-tarily and convey strong messages. As a patient is speaking, it may be appropriate to smile, which could mean you are encouraging the patient to continue speaking, or it could indicate that you are amused. One may also look perplexed, indi-cating that either the patient or you need more clarity.
A patient says, “Sometimes, I take my mom’s blood pressure medications when I have a headache because that’s how I know that my pressure’s up.”
Upon hearing this, you may feel surprise, shock, and/or disapproval. Although these feelings may be justi-fied, allowing your facial expression to show these feelings may discourage the patient from divulging information to you because of embarrassment and chagrin. In contrast, looking perplexed as you ask the patient why he or she thinks a headache means that his or her blood pressure is high may encourage the patient to respond by explaining his or her reasoning to you.
Body posture and position
Sitting straight or slumped, relaxed or tense, and/or with hands crossed over body may indicate one’s desire to be a part of the conversation or it may reflect feel-ing nervous, anxious, or defensive. Sitting straight may convey confi-dence. In addition, the distance or space between you and the patient may indicate the balance between respect for personal space and being close enough to comfort-ably speak with the patient without barriers. Typically, finding a place to sit where you are close enough to reach the patient but not touching the patient is a good distance.
If the pharmacist is sitting slumped in a chair, the patient may perceive that there is a lack of interest on the part of the practitioner to be present at the patient visit. In the same vein, if the patient is slouching, it may indicate a lack of interest, and therefore rather than just continuing to give informa-tion to the patient, it may be better to pause, and ask the patient a reflective question such as, “What do you think about starting these new medications?”
Now, not only are the words clearer, but the patient’s ability to connect with you, because of increased understand-ing, may improve as well.
tabLe 1.1 types of nonverbal communication (Continued)
nonverbal communication
description
example
10 chapter 1 / the patient interview

Gestures/movements
The use of gestures such as hand movements or nodding to show encouragement/understanding may be appropriate to complement your words; however the overuse of gestures, tapping of feet, or moving around may be distracting. If your patient is moving around too much or acting restless, it may indicate ner-vousness or discontent. In addition, touching a patient on the shoulder may show empathy or go together with making a point; however, some patients may feel uncomfortable with this. You need to assess the patient’s reaction to the touch to know the difference.
If you are a practitioner that lightly touches your patient’s shoulder or arm to emphasize a point or show empathy, and your patient pulls back or looks at you nervously, it may mean they are not comfortable with touch and therefore you should avoid touching the patient in the future. Additionally, if your patient appears to be moving around too much, you can ask the patient a question such as, “You seem to be pacing the room—what is on your mind?”
Eye contact If you keep glancing at your computer screen or your phone, it appears to the patient that you are not interested in what he or she is saying; however, maintaining continuous eye contact may make the patient uncomfortable. Addi-tionally, certain cultures consider eye contact to be a sign of respect whereas others think it is more respectful to not make direct eye contact. Therefore, you should take nonverbal cues from your patient to maintain the right amount of eye contact, understanding that a lack of eye contact does not nec-essarily indicate dishonesty.
As computerized medical records are becoming more prevalent, if you are reviewing and documenting informa-tion as the patient is speaking, it may make the patient feel as though you are not actively listening. During the visit, you can start by telling your patient that you will be documenting in the computerized medical record throughout the visit to prepare the patient. On the other hand, when the patient is answering your ques-tions, you should make eye contact and document this information at a later time.
apatientinterviewtoensurethatallofthecomponentsareaddressedandeventuallydocumentedand/orcommunicatedinanorganizedmannerthatisrecognizedbyallhealthcareprofessionals.Ithasbeenwelldocumentedinthemedicalfieldthateffec-tivecommunicationwithpatientsleadstobetterdiagnosisandtreatment,aswellasanimprovedprovider–patientrelationship.5Althoughmostofthisresearchisrelatedto
tabLe 1.1 (Continued)
the patient interview 11

physician–patientcommunications,itcaneasilytranslatetocommunicationsbetweenthepharmacistandthepatient.Thisisbecausepharmaceuticalcare,likethecarepro-videdbyaphysician,involves(1)curingapatient’sdisease,(2)eliminatingorreducingapatient’ssymptoms,(3)arrestingorslowingadiseaseprocess,and(4)preventingadiseaseorsymptoms.6Eventhoughapharmacistdoesnotmakediseasediagnoseslikephysiciansdo,apharmacistmustnonethelessevaluatetheinformationobtainedfromthepatientinterview,includingthepossibilityofcertaindiagnoses,toappropriatelycreateanassessmentandplan,whichmayincludeareferraltothepatient’sphysicianoranemergencyroomforfurtherevaluation.
components of the health history
Chief Complaint
Thechief complaint (CC) is the issueor issues that thepatient ispresentingwithandtheprimaryreasonforthevisit.Thisistypicallydocumentedinthepatient’sownwordsandisthereforequotedinthewrittenororalpresentation.Onewaytodeter-minethepatient’schiefcomplaintisbyasking,“Whatbringsyouheretoday?”Somepatientsmayhaveanactualcomplaint,whileatothertimestheymaybevisitingforageneralreason,suchastopickupaneworrefillprescriptionorforafollow-upvisit.Inthecaseofnoovertcomplaint,thechiefcomplaintmaybegoal-oriented,suchas“Iamheretopickupmyrefills,”“Iamheretodiscussmylabs,”or“Mydoctortoldmetoseeyouaboutmysugars.”4Attimes,thepatient’schiefcomplaintmayseemrela-tivelyminorcomparedtotheassessment;however,regardlessofthefinaldiagnosis,thechiefcomplaintshouldbethepatient’sprimarycomplaint.Forexample,apatientmaycomeincomplainingof“beingoutofhisfurosemide”and,uponevaluation,itmaybedeterminedthatthepatientisexperiencingacuteheartfailure.Thisassessmentandthesubsequentplanwillbediscussedelsewhereinyourdocumentation.
History of Present Illness
Thehistory of present illness (hpI)isthestoryoftheillness.7Thepharmacistwillfurtherexplorethechiefcomplaintaswellasanyotherpotentialproblemsbyaskingquestionsaboutanyrecentorremotehistorythatmayberelatedtothecurrentillness.ThegoaloftheHPIistoascertainacomplete,accurate,andchronologicalaccountoftheillnessfromthepatient.Sevenattributesneedtobeaddressedtoobtainawell-characterizeddescriptionofthecomplaintorsymptom:location,quality,quantityorseverity,timing,setting,factorsthataggravateorrelievethesymptoms,andassociatedmanifestations.2 table 1.2 describes each attribute inmore detail and provides an
12 chapter 1 / the patient interview

tabLe 1.2 seven attributes of a symptom
attribute
exploration
example for chief complaint of swelling
Location Specifics about where the symptom is occurring. In some cases, it is important to ask the patient if it is okay for you to inspect the area.
“Where is the swelling located?”
Quality Describe the symptom in terms of char-acterization. For example, if the patient is in pain, characterize the pain by using descriptive adjectives, such as stinging, shooting, or crushing.
“Describe the swelling. How much worse is it now than it normally is?”
Quantity/severity Quantify the severity of the symptom. If the symptom is pain, ask the patient to rate the pain on a scale of 1 to 10.
“Would you say that this swelling is causing your leg to be twice its normal size?”
Timing Find out when the symptom started and if there was anything occurring at the time to link it to the onset of the symptom. Also clarify how long the symptom has been occurring and the frequency of occurrence; that is, is it constant or intermittent?
“When did the swelling start? How long does it last? Is it worse at certain times during the day?”
Setting This includes addressing the possible cause of the symptom.
“Have you noticed what causes the swelling?”
Factors that aggravate or relieve the symptom
Determine what makes the symptom bet-ter or worse. Ask about any medications or nonpharmacologic therapies used to relieve the symptoms and their efficacy. Ask questions to find out what makes the symptom worse. For example, the symp-tom may be worsened by certain environ-mental conditions, exertion, or stress.
“What makes the swelling worse or better? Do you notice a difference in the morning versus when you have been on your feet dur-ing the day? What did you try for the swelling? How did it work?”
Associated manifestations
Note any other symptoms the patient is experiencing. Also ask about symptoms that may be a consequence of the primary symptom.
“What other symptoms do you have? Are you experienc-ing any shortness of breath or trouble walking?”
the patient interview 13

example.Asyoutalkwiththepatient,theflowoftheHPImaydependonwhatthepatientwantstotellyou;however,mostofthetimeallsevenattributesofasymptommustbeaddressedtocompletelycharacterizethepatient’scomplaintandtodeveloptheHPI.Forexample, if apatientcomplainsof a cough, it isnotnecessary toaskabout the “location”of the cough.However, if a patient complains of a headache,specifyingtheexact“location”ofthepain(i.e.,front,back,orsideofthehead)willassistintheassessment.AskingquestionsduringtheHPIisakintoputtingtogetherapuzzle.Apatient
whoistellingyoupartsofhisorherstorymaynotrealizewhichpartsarepertinent.Forexample,thepatientmaynotknowhowandwhatinformationneedstoberelayedtoyousothatyoucanmakeacompleteassessment.Itislikeapuzzleinthatyoumayknowwhat thecompletedpuzzlewill look like;however,youhave topickupeachpiece;examineitsshapeandcolorforhints,suchashavingaflatside,whichindicatesthatitisaborderpiece;andthenplaceitnearother“like”piecesuntilyouareabletofitallthepiecestogether.You,asthepharmacist,shouldstartthinkingofvariousquestionstoaskthepatientsothatthepatient’sresponses,orthepuzzlepieces,maybe put together to ascertain or rule out certain assessments. It is important to askopen-endedquestionsandappropriatelyfollowupinordertoobtaintherightpiecesofinformationtoputtogethertheHPI.Inthecaseofthepatientinterview,youwillbeassessingeachpieceofinformationforitsreliability,completeness,andrelevancetotheproblem.7 Asthedetailsoftheproblemarefurtherexplored,youneedtopro-cessandevaluatethis informationtofindthe linkamongsymptomssoappropriateassessmentmayoccur.7
Onewaytoascertainthis informationisbyfocusingonpertinentpositivesandnegatives,whichmaybethoughtofasthehintsthatwillleadtoyouputtingthepuzzletogether.Inadditiontoaskingthepatientopen-endedandfocusedquestionstolearnthecharacterizationsofhisorherchiefcomplaintorsymptom,theHPImayincludeadditionalquestionsthatfocusonthepresenceorabsenceofcertainsymptomsthatcouldberelatedtoyourdifferentialdiagnosisorthepatient’smedicalcondition.Youmayneedtoassessapatient’smedicalconditionduringthepatientinterviewevenifthepatientdoesnothaveanycomplaintsregardingthatmedicalcondition.Forexam-ple,inapatientwhohasheartfailure(HF),youmayneedtoaskaboutthepresenceorabsenceofcertainsymptomstodeterminewhetherthepatient’sHFiscontrolledorifthepatientisexperiencinganexacerbation.Therefore,youmayaskthepatientaboutsymptomsthatarepertinenttotheassessmentofHF,suchasthepresenceorabsenceofedema,theuseofextrapillowsatnighttoavoidlyingflat,andshortnessofbreath.Ifthepatienthasanyoftheaforementionedsymptoms,theywouldbetermed pertinent positives, or the presence of symptoms that are related to themedical
14 chapter 1 / the patient interview

conditionthatisbeingassessed.Incontrast,ifthesesymptomsareabsent,theywouldbetermedpertinent negatives,ortheabsenceofsymptomsrelatedtothemedicalconditionbeingassessed.Askingthesefocusedquestionsaboutpertinentpositiveandnegativesymptomscontributestotheassessmentofheartfailureinthispatient.Anotherwaytousethetechniqueofaskingaboutpertinentpositivesandnega-
tivesistoruleoutorruleinpossiblediagnoses.Forexample,todetermineapossiblecause for thepolyuria (increasedurination)apatient isexperiencing,youwillneedto ask focusedquestions.First, you consider themost commoncausesofpolyuria,whichinclude,butarenotlimitedto,diabetesoraurinarytractinfection(UTI).Tofurtherexplorethereasonbehindthepolyuria,youwillaskaboutsymptomsthatarepresentineitherdiabetesoraUTI,includingpolydipsia(increasedthirst)andpoly-phagia(increasedhunger)ordysuria(painfulurination)andhematuria(bloodintheurine), respectively.Additionally,pertinentpositivesornegativesarenot limited tosymptoms butmay include other information obtained from the family history orpastmedicalhistory.Forexample, inapatientwithpolyuria, itwillbepertinenttofindoutifthefamilyhistoryissignificantfordiabetesorifthepatient’spastmedicalhistory(PMH)includesrecurrentUTIs.Inordertoaccuratelymakeadiagnosis,incollaborationwithamedicalprofessional, these findings fromthepatient interviewwouldneedtobecoupledwithdiagnostic tests, includingbloodworkand/orurineanalysis.Thepurposeofthisexampleistoillustratetheuseofquestionstodiscovereitherthepresenceorabsenceofpertinentfindingsthatassistinpaintinganaccurateandcompletepictureofthepatient’sstory.
Past History
Thepast historyincludesthepastmedicalhistory,surgicalhistory,historyofchild-hoodillnesses,andobstetric/gynecologichistory.Aspectsofhealthmaintenance,suchasimmunizationsandscreeningtests,shouldbeincludedaswell.4Wheninterviewingthepatient,alloftheseaspectsfallundertheumbrellaofpasthistory;however,upondocumentation,thesesectionsmaybeseparatedbytypeofpasthistory,suchasPMH,surgicalhistory,orhealthmaintenance/immunizations.Eachofthecomponentsofthepasthistoryshouldincludetheinformationdiscussedbelow.Aspharmacists,wedonotusuallyobtainacompletepasthistoryfromapatient;rather,werelyontheinforma-tiondocumentedbyamedicalstudent,resident,orphysician.However,sometimesitisappropriatetoaskthepatientaboutpartsofhisorherpasthistoryand/ortouseanyinformationgatheredpreviouslytodeterminetheappropriatecareforthepatient.Therefore,itisvitaltoknowthecomponentsofthepasthistoryandthequestionsthatneedtobeasked.
the patient interview 15

past medical history The PMHincludeschronicaswellaspastacutemedicalconditions, includingdiabetes,hypertension,hyperlipidemia,hepatitis,andasthma,aswellasanyhistoryofpneumonia,cancer,orLymedisease.OnewaytoaskpatientsabouttheirPMHis,“Whatmedicalconditionsdoyouhaveorhaveyoubeentoldyouhave?”Youmaynoticethataparticularpatientmayhaveseveralconditionsdocu-mented,butuponfurtherquestioningdeterminethatthepatientisnotincludingallofthem.Toensurecompleteness,youmayneedtoaskthequestioninvariouswaysand, at times,gentlyprobe.Forexample, if younotice that thepatient isnot surewhatyoumeanby“medicalconditions,”youmightask,“Doyouhaveanymedicalconditions,suchasdiabetesorhighbloodpressure?”Or,ifyounotethatthepatienthasalbuterolinhisorhermedicationprofilebuthasnotmentionedanypulmonary-relatedconditions,youmightask,“Whatareyoutakingthealbuterolfor?”
surgical history Thesurgicalhistoryshouldincludethetypeofoperation,whenitoccurred,andtheindicationfortheoperation.Youmightaskthepatient,“Whatsurgerieshaveyouhad?” and“Whendidyouhave this surgery?”Examplesof thesurgical history thatwouldbepertinent topharmacistswouldbe an assessmentofuncontrolled pain from a recent knee replacement surgery or the determinationofwhichvaccinesshouldbeavoidedinthepatientwhohashadasplenectomy.
childhood illnesses Pertinent childhood illnesses include measles, mumps,whoopingcough,chickenpox,rheumaticfever,scarletfever,andpolio.Youcouldaskthepatient,“Whatchildhoodillnesses,suchasmeaslesorchickenpox,didyouhaveasachild?”
Obstetric/gynecologic history The obstetric history includes the number ofpregnancies,includingdeliveries,miscarriages,andterminations,aswellastheyear,monthsgestation,complications,andinfantweightforeachpregnancy.Thegyneco-logichistoryincludesonsetofmenstruation,dateoflastperiod,useandtypeofbirthcontrol,andsexualfunction.Althoughthepharmacistdoesnottypicallygatherthishistory, someof this informationmaybepertinent topatientcareprovidedby thepharmacist.Forexample,knowledgeofaninfant’sbirthweightcanhelpyoudeter-minewhetherthemotherhasariskfactorfordiabetes,which,inturn,mayinfluencewhetheryouwouldrecommenddiabetesscreeningforthepatient.Onewaytogatherthisinformationwouldbetoaskdirectly,forexample,“Therearemanyriskfactorsfordiabetes,includingthebirthweightofyourchildren.Howmuchdidyourchil-drenweighwhentheywereborn?”or“Didanyofyourchildrenweigh9ormorepoundswhentheywereborn?”
16 chapter 1 / the patient interview

Anotherexampleofaskingquestionsrelatedtothegynecologichistoryisinthecommunity settingwhenapatient requestsPlanBOne-Step, andyoumustdeter-minewhetherPlanBOne-Stepisappropriateandwhatothercounselingmaybenec-essary.Inthissituation,youmightaskthepatientquestionssuchas,“Whendidtheunprotectedsexhappen?”“Toensurethatyouarenotpregnantnow,whenwasthedateofyourlastperiod?”or“Unprotectedsexcarriestheriskofsexuallytransmitteddiseases, andPlanBOne-Stepwill not prevent this.Are youworried about this?”SuchquestionsenableyoutoassesstheappropriatenessofPlanBOne-Stepandthepossibleneedforthepatienttoseekmedicalattention.
Health Maintenance/Immunizations
This part of themedical history includes information onwhat immunizations thepatienthasreceived,suchasinfluenza,pneumococcal,tetanus,andhepatitisB,aswellasthedatestheywereobtained.Basedonthisinformation,youcanthenrecommendanyneworbooster immunizations thepatientmayneed.Thedates and resultsofscreeningtests,suchasmammograms,Papsmears,andtuberculintests,shouldalsobeincluded.Informationondiabetesandcholesterolscreeningsmayalsobeincludedinthissection,eventhoughthesetestsarepartoftheobjectivedata.Thesescreen-ingteststypicallyoccurbecauseofrecommendationsfromguidelinesandaremeanttoallowforpreventativetreatmentsandearlydiagnosis;therefore,askingthepatientaboutthisduringthepasthistorycomponentofthepatientinterviewenablesyoutomakerecommendationsbasedontheinformationyouhavegathered.
Family History
The family history (Fh) ishealth informationabout thepatient’s immediaterela-tives.Theserelativesincludeparents,grandparents,siblings,children,andgrandchil-dren.Becausemanymedicalconditionshaveageneticcomponent,thepurposeofthefamilyhistoryistodeterminepotentialrisksfactorsforthepatient’scurrentandfuturehealth.Typically,relativessuchascousins,aunts,andunclesarenotincludedinthefamilyhistory;however,forcertainmedicalconditionsthatcarryahighgeneticlinkquestionsaboutthepatient’sfamilyhistorymaybeappropriate.7 When inquiring about familyhistory, you should askwhether thepersonwhose
history is beingprovided is alive or deceased; determine the presence or absenceofmedicalconditionssuchashypertension,coronaryarterydisease,hyperlipidemia,dia-betes, pulmonary diseases, cancers, or thyroid disorders; and gather information onthat person’s psychiatrichistory, addictions, or allergies. In addition, if theperson is
the patient interview 17

deceased,ascertaintheageatdeathandthecauseofdeath.4Itisimportanttoincludethis specific informationbecause itmaydetermine certain risk factors apatientmaycarry.Forexample,ifapatient’sfatherdiedattheageof45secondarytoamyocardialinfarction,thepatientthenhasariskfactorforcoronaryarterydisease.Thisriskfactor,inconjunctionwithotherpertinenthistory,willdeterminethepatient’sgoallowdensitylipoprotein(LDL)anddrugtherapynecessarytoachievethisgoal.Onewaytodeter-minethepatient’s familyhistory is toask,“Areyourparentsandgrandparentsalive?Whatwasthecauseofdeath?Atwhatagedidtheypassaway?”Ageneralquestion,suchas“Whathealthconditionsdoordidyourparents/grandparents/childrenhave?”maybesufficient,butsometimesitmaybenecessarytoaskamorefocusedquestion,suchas“Doordidyourparentsorgrandparentshaveheartdiseaseordiabetes?”
Personal and Social History
Thepersonal and social history (Sh) is thepartofthe interviewwherewelearnabout thepatient’s life, includinghealthbehaviors andpersonal choices.Thebasicsocial history consists of asking the patient about past and present use of tobacco,alcohol,andillicitsubstances.Ifthesearecurrentlyconsumed,youshouldinquireastohowmuchandhowofteneachisutilized.Inaddition,ifapatientisaformeruserofanyofthesesubstances,itisvitaltoaskthepatientatsubsequentvisitsifheorsheremainsabstinentorifrelapsehasoccurred.Becausemanyofthethesequestionscanbeverypersonalandsomepatientsmaybereluctanttosharesuchinformation,eitheroutofembarrassmentor fearofbeing judged,youshouldask thesequestionswithsensitivityandrespect.However,itisimportanttobedirectsothatpatientsrealizethesequestionsareimportantwithregardtotheircare.
tobacco use You should ask patients if they currently smoke or if they havesmoked in thepast.Forboth former andcurrent tobaccousers, you should ask atwhatage theystarted (andquit);what formof tobacco theyuseorused, includingcigarettes,chewingtobacco,and/orcigars;andquantify theamount.Forcigarettessmokers,youshouldaskhowmanycigarettesorpackstheysmoke(orsmoked)perday.Onewaytoaskthisquestionis,“Howoftendoyouusetobaccoproducts?”Byasking this question in an open-ended manner, patients who consider themselvessocial smokersmaybemore likely todisclose informationabout their tobaccouse.Hadyouasked,“Doyousmoke?”thesesamepatientsmaybemorelikelytosaynobecausetheydonotsmokeoften.
alcohol use Similartotobaccouse,youwanttoaskapatient,“Howoftendoyoudrinkalcohol?”Youalsowantpatientstoquantifytheamounttheydrinkandhowoften
18 chapter 1 / the patient interview

theydrink.Itisnecessarytoaskspecificquestions,becausealthoughonedrinkistech-nicallyconsideredtobe12ouncesofbeer,5ouncesofwine,or1.5ouncesofliquor,apatient’sdefinitionof “onedrink”mayvary.Youcouldask thepatient, “Whatdoyoutypicallydrink?”“Howmuchwine/beer/liquordoyouhaveeveryday?”or“Howmanydaysaweekdoyoudrink?”Togathermoreinformationaboutwhatonedrinkmeanstothepatient,specificallyask,“Howmuchliquordoyouputinonedrink?”
illicit substances use Patientsmayhesitatetoanswerquestionsaboutillicitdrugusehonestlybecausetheyareafraidofnegativeconsequences.Itwillhelpifyouarestraightforwardandnonjudgmentalwhenaskingaboutillicitsubstanceuse.Onewaytoaskthisquestionis,“Doyoucurrentlytake,orhaveyoutakeninthepast,anyillicitdrugs?Ifso,whichones?”Remindthepatientthatheorsheshouldfeelcomfortabledisclosingthis informationtoyoubecauseyouareseekingthis informationforthepurposeofprovidingpatientcareandthatyouwillnotreporttheuseofany illicitdrugstolawenforcementauthorities.
Inadditiontopastandpresenttobacco,alcohol,andillicitsubstancesuse,amorecompletepersonalhistoryalsoincludeseducationallevel,compositionofthefamilyoforiginandthecurrenthousehold,personalinterests,andadditionallifestyleinfor-mation,suchasdietaryhabits,caffeineintake,exercisehabits,andanassessmentoftheactivitiesofdailyliving(ADL)todeterminebaselinefunction,especiallyindis-abledorolderpatients.4
Review of Systems4
Thereview of systems (rOS)isasystematic,head-to-toeevaluationofthepresenceorabsenceofsymptoms.Itincludesthepresenceofanysymptom,evenonethatthepatientmaynothavedeemedtobesignificantormayhaveforgottenbecauseofhisorherfocusonthechiefcomplaint.Generally,themedicalstudent,resident,orphysiciancompletes thecomprehensiveROSquestioning;however,pharmacistsmayneed toaskapatientaboutthepresenceorabsenceofpertinentsymptomsrelatedtothepres-entillness.Becauseofthis,itisnecessarytounderstandwhatisincludedintheROS.Additionally,pharmacistsmayalsobepartofamedicalteam,andthereforeshouldbeawareofallofthecomponentsofapatientintervieweveniftheyarenottheonesask-ingthequestions.Priortostartingthispartoftheinterview,letthepatientknowthatyouwillbeaskingseveralquestionstoassessanypotentialsymptomsheorshemaybeexperiencing.Oftentimes,someofthesesystemsmaybeaddressedconcurrentlywithanotherpartoftheinterview.Forexample,aftercheckingthepatient’sbloodpressure,youmayaskifthepatienthashadanydizzinessorpalpitations.
the patient interview 19

Physical Examination
Thecomprehensivephysical examination (pe)ismostoftencompletedbyamedicalstu-dent,resident,orphysician.Theyaretaughttodeveloptheirownsystematicapproachtoensureathoroughandaccuratephysicalexam.Thecomprehensivephysicalexamincludesmeasurementofvitalsignssuchasheight,weight,temperature,bloodpressure,andpulse,aswellastheobservation,inspection,andpalpationofthepatient’sbodyfromheadtotoe.Althoughphysiciansoftencompletethispartofthepatientassessment,pharmacistsarealsoskilledatcompletingpartsofthephysicalexam.Thesepartsinclude,butarenotlim-itedto,measuringvitalsignsandinspectingandpalpatingpartsofthebodyrelatedtothepatient’scomplaint.Forexample,apharmacistmayassesstheseverityoflowerlegedemabyinspectingandpalpatingtheareaofswelling.Additionally,pharmacistsmayconductmentalstatusexaminationsorassesstheeffectsofastrokebyexaminingthepatientforfacialdroop,armdriftorstrength,andspeechabnormalities.8
medicatiOn histOry
Themedication historyisavitalcomponenttothepatientinterviewandistheareawherethepharmacistwilldedicatethemosttime.Medicationsincludeprescriptionandover-the-counter(OTC)drugsaswellasherbalproducts.Themedicationhistoryprovidesinsightintothepatient’scurrentandpastmedications,adversedrugreactionsorallergies,adherence,thepatient’sownunderstandingabouthisorhermedications,andanyotherconcernsapatientmayhaveregardinghisorhermedications.9Askingpertinentquestionswithasystematicapproach,utilizingappropriatetechnique,andactively listening to thepatientwill enable you to collect a thorough and accuratemedicationhistory.This,inturn,willenableyoutoidentify,prevent,and/orresolveanyactiveorpotentialdrug-relatedproblems.Additionalreasonstoobtainanaccuratemedicationhistoryincludethefollowing:10
• Rulinginoroutadrug-relatedadverseeffect• Preventingdrug–drug,drug–food,ordrug–diseaseinteractions• Monitoringforclinicalsignsthatmaybemaskedduetoadrug• Evaluating laboratory findings appropriately, as certaindrugsmay affect theresults
• Preventingprescribingerrors
Additionally, the inclusionof a thoroughOTCmedication andherbal producthistoryisvitalforthefollowingreasons:
• It verifies that the patient is choosing the appropriateOTCmedication orherbalagentandthatitisbeingtakencorrectly.
20 chapter 1 / the patient interview

• Itgivesyoutheopportunitytoassessforanydrug–drugordrug–diseaseinter-actionsthatmaybeoccurringwithanOTCorherbalproduct.
• ItwillgiveyoutheopportunitytocounselandeducatethepatientaboutOTCmedicationsandherbalproducts,becausesomecarrymorerisksthanbenefits.
For example, a patientwho is takingwarfarinmay also tell you she is taking ibu-profen200mgtwicedailyforarthritispain.Thisinformationprovidesyouwithanopportunitytoassessthepatient’sarthritispainandinquireaboutwhatotheragentshave been tried to treat the pain.After evaluating the patient, youmaydeterminethat acetaminophen is themore appropriate drug for this patient.Youwould thencounselregardingtheincreasedriskofbleedingassociatedwithconcomitantwarfarinandibuprofenuse,aswellasrecommendacetaminophen,beingsuretoincludeallthecomponentsofself-carecounselingdescribedlaterinthischapter.
components of a medication history
Toeffectivelyandefficientlyconductamedicationhistory,appropriatetraining,edu-cation,andpracticearenecessary.Youshouldknowallthequestionsthatneedtobeasked,thevariouswaysinwhichthequestionsmaybeasked,theappropriateuseofinterviewtechniques,andthemanysourcesofinformationthatshouldbeutilized.9 Itisnecessarytoknowthecontentsandsignificanceofthevariouscomponents
ofamedicationhistory.Thissectionprovidesexamplesofhowtoaskthequestionsrelated to the medication history along with the explanation of each component;however, it is importanttorealizethattheseexamplesdemonstrate justonewaytoask questions, and youmight find that your own communication style lends itselftoa differentwayofaskingthequestions.Youmust findawayofhavinganaturaldiscussionwiththepatientthatworksforyou,andthiswilltakealotofpractice.
Introduction
Priortostartingthemedicationhistory,youshouldintroduceyourselfbytellingthepatientand/orcaregiveryournameandtitle.Besuretoconfirmthepatient’sidentitywithatleastonepatientidentifier,suchasthepatient’sbirthday,telephonenumber,or home address. Additionally, you should describe the purpose of themedicationhistory,tellthepatienttheamountoftimeyouexpectthatitwilltaketoconductthemedicationhistory,andobtainpermissiontocollecttheinformation.Thefollowingisasampledialoguefortheintroduction:“Hello,mynameisShaan
Smith,andIamapharmacystudent.Beforewegetstarted,IwouldliketomakesureIamspeakingwiththerightperson.MayIgetyourfullnameandaddress,please?”
medication history 21

Once the patient’s identity has been confirmed, you could continue by saying,“Iwillbetakingamedicationhistoryfromyoutoday.ThismeansthatIwillbeask-ingyouquestionsaboutall themedicationsyouarecurrently takingandget someinformationaboutmedicationsyoumayhavetakeninthepastandanysideeffectsorallergiesyoumayhave.Allofthisshouldtakeabout10to15minutes.Wouldthatbealrightwithyou?”
Medication History
Aftertheintroduction,youwillneedtoobtaininformationonalloftheprescriptionandOTCmedicationsaswellasanyherbalproductsthepatientiscurrentlytaking.Additionally,youmayneedtospecificallyaskthepatientabout inhalers, injections,OTCproducts,andherbalmedications,becausepatientsoftentimesforgettomen-tionthese thingsbecause they tendtoonly thinkof“pills”whenaskedabout theirmedications.Foreachmedication,youwillneed todetermine theproduct’sname, strength,
dose, indication, frequency, timingof administration,durationofuse, and thepre-scribingphysician.Theinformationcanbegatheredinanumberofdifferentways,andthemethodyouusemaydependontheclinicalsetting.Thebestwaytoobtainthis information in a planned encounter is via the “brown bag”method. Prior toyourplannedmeeting,askthepatienttobringinallofhisorhermedicationbottles,including prescription andOTCmedications and herbal supplements.During themeeting,askaboutthedose,indication,frequency,timingofadministration,anddura-tionoftheuse.Bylookingatthebottles,youwillalreadyknowthenameandstrengthofthemedicationaswellastheprescribingphysician.Eventhoughthedirectionsarewrittenonthelabel,youshouldaskthepatienthowheorsheistakingaparticularmedication,becausetheremaybediscrepanciesbetweenthewrittendirectionsandhowthepatientactuallytakesthemedication.Anothermethodistolookatawrittenlistofmedicationsthatiseitherkeptby
thepatientor foundinthemedicalchart.Sometimesapatientmaysay,“Iamtak-ing everything that you have on your list” when you start asking them questionsabouttheirmedications.Onewaytoaddressthisisbyexplainingthepurposeofthemedication history. For example, you could tell the patient, “Although I do havethemedicationslistedinmychart,itwouldbegoodtogothrougheachmedicationonebyonetoensurethatmylistisaccurateandtrulyshowswhatyouaretakingnow.”Anotheroptionistosimplyaskthepatientaboutall themedicationsheorshe
istaking.Unfortunately,patientsdonotalwaysrememberthenames,doses,orhowtheyaretakingtheirmedication;accordingly,thismethodmaynotproducethemost
22 chapter 1 / the patient interview

completemedicationhistory.Withthepatient’spermission,youcancallthepatient’spharmacyorprimarycarephysiciantoobtainthemostcurrentmedicationlist,oryoucanevencallthepatient’shometospeakwithsomeonewhocanreadtheinformationfromthemedicationbottles.If apatient ispresenting to theemergencyroomor is inahospitalwhere it is
notpossibletolookatthepatient’smedicalchart,youshouldaskthepatient,familymember,orcaregiverifheorshehasawrittenlist.Ifsuchalistisnotavailable,obtainpermissiontocallthepharmacy,primarycarephysician,and/orthepatient’shome,asdiscussedpreviously.Regardlessofthemethodutilizedtocompleteamedicationhistory,theinforma-
tionthatneedstobecollectedisthesame.Thevariouscomponentsofthemedicationhistoryarelistedbelow.Thesecomponentsarethesameforeachmedication,includ-ingprescriptionandOTCmedicationsandherbalproducts.
medication name Thenameofthemedicationcanbelocatedonthelabelorthemedicationlist.Onewaytoobtainthisinformationistoask,“Whatarethenamesofthemedicationsthatyouarecurrentlytaking?”Whenobtainingthisinformation,makesuretodetermineifthemedicationisextendedrelease(ER),longacting(LA),sustainedrelease(SR),or immediaterelease(IR),andwhetherthepatient istakingthebrandnameorgenericversion.Forexample,ifapatientstatesthatheorsheistakingmetoprolol,youmustdetermineif it istartrateorsuccinate.Withregardtogenericversusbrandname, for somemedicationswithnarrowtherapeutic indexes,suchaslevothyroxineorwarfarin,changingbetweenmanufacturersmaycausefluc-tuationsindruglevelsintheblood;therefore,includingmanufacturerinformationisbeneficial.Ifapatientdoesnotknowthisinformation,anotherwaytoaskthisques-tionis,“Doesyourlevothyroxinetabletlookthesameasitalwayshas?”
strength and dose Informationforstrengthanddoseisalsofoundonthelabeloronamedicationlist.Youcanalsoaskthepatient,“Whatisthedoseofthemedica-tionyouaretaking?”Makesuretoincludeinformationforboththestrengthanditscorrespondingunits.Forexample,levothyroxine50mcgormetoprololER50mg.
Frequency Although this information isoften included in thedirectionswrittenonthelabel,youshouldaskthepatient,“Howoftendoyoutakethismedication?”Insomecases,thepatientmaybetakingthemedicationdifferentlythanwrittenonthelabel.Thiscouldoccurforseveralreasons.Forexample,apatientmayhavebeentoldbyhisorherphysiciantodoubleorlessenthedose,orthepatientmayhavemisreadthedirectionsorbeconfusedaboutthecorrectwaytotakeit.
medication history 23

Frequency of a prn medication Obtaining the actual frequency of a PRN(i.e., asneeded)medicationenablesyou to assesswhether thepatient is taking themedicationappropriatelyandwhetherthediseasestateisbeingmanagedeffectively.Onewaytodeterminethisfrequencyistoaskthepatient,“Inatypicalday(orweek),howmanytimesdoyoutakethismedication?”or“Howmanytabletsdoyoutakeatatimeandhowoftendoyoutakethem?”Forexample,ifapatientstatesthatheorsheistakingalbuterolmostdaysoftheweekforshortnessofbreath,itisimportanttoaskthepatientwhatcausestheshortnessofbreath,howmanyinhalationsaretakenatonetime,howmanytimesadaythemedicationistaken,andwhatthetimeintervalisbetweendoses.Thisenablesyoutoensurethatthepatientisatorbelowthemaxi-mumdosageandpotentiallyassesstheseverityofthepatient’sasthma,which,inthisexample,maywarrantadditionalmedications.
timing To determine the timing of medication administration, you can ask thepatient,“Whendoyoutakethismedication?”Ifitisamedicationrequiringdosingatmultipletimesduringtheday,becertaintoascertaintheamountoftimebetweendoses.Forexample,ifapatientsaysthatheorshetakesatwice-dailymedicationwithbreakfastanddinner,youshouldask,“Whattimeisbreakfastanddinner?”becausethemedica-tionmayrequire12hoursbetweendosesbuttheamountoftimebetweenthepatient’sbreakfastanddinnermaybeonly8hours.Anotherreasonthattimingiskeyisbecausesomemedicationsneedtobetakenatcertaintimesofdayorinrelationtoameal.Forexample,somestatinsaremosteffectivewhentakenintheevening,whereasothermedi-cationsneedtobegivenonanemptystomachorseparatedfromotherdrugs.Determinationoftimingisespeciallyimportantforapatientwhoisbeingadmit-
tedtothehospital.Itisnecessarytoobtainthetimingofeachmedicationsothatthissameschedulecanbefollowedinthehospital.Also,thetimeofthelastdoseofeachmedication is vital to ensure that apatientdoesnot receive an additionaldoseof amedicationonthedayofadmissionthatheorshemayhavealreadytakenthatmorn-ingathome.Onewaytoavoidthisistohavetheprescriberspecifywhenthefirstdoseofeachmedicationisduewhenwritingtheinitialmedicationordersonadmission.
indication Inquiring about the indication for each medication enables you toassessthepatient’sunderstandingofhisorhermedicationsandtoprovidepatient-specificeducation.Youcandeterminetheindicationbyaskingthepatient,“Whatareyoutakingthismedicationfor?”
adverse reactions Adversereactionsarealsoknownasside effectsorintolerances.Askthepatient,“Whatsideeffectsareyouexperiencingwithanyofyourmedications?”
24 chapter 1 / the patient interview

Youcanalsouseaclosed-endedquestion,suchas“Doyouthinkanyofyourmedica-tionsarecausingyoutofeelanythingoutoftheordinary?”Sometimesapatientmaycomplainofa symptomthat isactuallyanadversereaction.Other times,apatientmay link the start of an adverse effectwith the start of amedication. Asking thisquestioninageneralwayallowsthepatienttoreflectonormentionanywayheorshemayhavebeenfeelingdifferentlywithoutrealizingthatamedicationcouldbecausingthereaction.Additionally,itisimportanttogetdetailedinformationabouttheadversereactionsothatyoucanassesstheseverityof theadversereactionanddeterminethenextcourseofaction,whichmay includediscontinuingthemedica-tion,addingamedicationtocounteracttheadverseeffects,and/orobtaininglabora-torytestsorrecommendingfurthertestingtodeterminethecauseorseverityoftheadversereaction.
past medication use At times, it canbehelpful to findoutwhatmedicationsthepatienthastakeninthepast.Forexample,certainpatientswithdiabetesneedtobeonanangiotensin-convertingenzymeinhibitor (ACE-I)suchas lisinopril.Afterconductingthemedicationhistory,youmaydiscoverthatthepatientisnottakinganACE-Ieventhoughtheguidelinesrecommendthis.Priortodiscussingthiswiththepatient’s physician, you should inquirewhether the patient has taken anACE-I inthepast.Forexample,youmightaskaprobing question,suchas“Haveyoutakenanymedicationsforbloodpressureorforyourkidneys inthepast?”or“Haveyoutakenabloodpressuremedicationinthepastthatmaysoundlikethereisa‘pril’attheendof thename, suchas lisinoprilorenalapril?”Anotherway toexaminepastmedications is by cross-referencing the information that thepatienthas given youwithhis orherpharmacy and/ormedical chart.Youmaydiscover that thepatientmaynotbeonanACE-Idue toanadversereaction in thepastorbecauseofcostissues.However,youmightalsodiscoverthatthepatienthasneverbeenonanACE-inhibitor,inwhichcaseyouwouldevaluateforanycontraindicationsandpotentiallydiscussaddingsuchamedicationwiththepatient’sphysician.
medication adherence Akeycomponenttothemedicationhistoryisanassess-mentofmedicationadherence.Asthesayinggoes,amedicationonlyworkswellifitisbeingtaken.Assumingthatapatientistakingthemedicationisnotalwaysasafeassumption.Therefore, it is important to ask the patient howmanydoses of eachmedicationaremissed,whatthereasonsareformissingdoses,andwhatthepatientdoesifadoseismissed.Youcouldaskthepatient,“Howoftendoyoumissdosesofanyofyourmedications?”or“Inthelastweek,howmanydosesdidyoumissofyourmedications?Whichmedications?Whatcausedyoutomissthosedoses?Whatdid
medication history 25

youdowhenyourealizedthatyouforgottotakethemedication?”Byaskingthesequestions,youarelearninghowadherentapatientistothemedicationregimenandwhatmaybecausingthepatienttomissdoses.Theinformationyougainaboutadherencewillenableyoutobettertargetyour
medication counseling.For example, youmay learn that apatient is taking adailymedicationeveryotherdaybecauseofthehighcostorbecauseoffeelingsofdizzinesswheneverheor she takes it.Onceyouunderstand thepatient’s reasoning,youcanmakeappropriateadjustmentstotheregimen,ifnecessary.Forexample,ifthepatientisunabletoaffordthedrug,youmaybeabletorecommendalessexpensivethera-peuticalternative;ifthereasonformisseddosesisduetoanadversereaction,furtherevaluationiswarrantedtodeterminewhethertheadversereactionistrulybecauseofthemedicationorpossiblyduetoanotherreason.Additionally,youmaylearnthatapatientmerely forgets to taketheeveningdoseofa twice-dailymedication.Inthiscase,youcanseeifaonce-dailyoptionisavailableorprovidesuggestionstoimprovethepatient’sabilitytorememberthedose,suchasusingacellphonealarmorleavingthemedicationnexttothebed.Inanycase,priortomakinganyrecommendations,itisimportanttothoroughly
exploreapatient’slevelofadherenceandreasonsforlackofadherence.Inaddition,whenaskingaboutadherence,youwanttomakesurethepatientdoesnotfeellikeheorsheisbeingscoldedorreprimanded.Besuretoaskwithoutjudgmentandavoidleadingquestionssuchas“Youdon’tmissanydoses,right?”
allergies Inquiringaboutanyallergies thepatientmayhaveexperiencedatanypointinhisorherlifeisjustasimportantaslearningaboutallthemedicationsthepatientistaking.Askthepatientaboutanyallergiestomedicationsorfoodsandtodescribewhattypeofreactionoccurred.Youmustdeterminetheallergytrigger;thetypeofreaction, includingitsseverity;andhowtheallergicreactionwasresolved.Thisinformationwillhelpyoudeterminewhetherthereactionistrulyanallergyorratheranadverseeffect.Youcouldaskthepatient,“Whatallergiesdoyouhave?”Aclosed-endedquestionwouldbe,“Doyouhaveanyallergiestoanymedicationsyouhavetakenoranyfoods?”Onceyoudeterminewhichallergiesthepatienthas,you should ask, “What happenedwhen you took thatmedication?What did youneedtodotomakethereactiongoaway?”Bydocumentingallofthisinformation,youcandeterminewhichmedicationstoavoidinthefuturebasedoncross-reactivitythatmayoccurbetweendifferentclassesofdrugsorbecauseoftheseverityofthereaction.Forexample,ifapatientsaysthatsheisallergictoamoxicillinandrefusestotakeiteveragaininthefuturebecauseofthestomachachesheexperienced,theninthefutureyoumaybelikelytorecommendacephalosporin;however,ifthereaction
26 chapter 1 / the patient interview

totheamoxicillinwasanaphylaxis,youwouldmostlikelyavoidcephalosporinsduetotheriskofcross-reactivity.
closing the interview
Aswithallpatientinteractions,closingthemedicationinterviewincludesassessingthepatient’sunderstanding,providinganopportunityforthepatienttoaskyouquestions,anddiscussing any follow-upplans.Because thepurposeof themedicationhistoryisprimarilyforyoutogatherinformation,assessingthepatient’sunderstandingwillonlyoccurifissueswereidentifiedduringthemedicationhistoryandcounselingwasprovided.Ifthisoccurred,youmaychoosetoutilizetheteach-backmethod,whichmeansyouaskthepatienttorepeattheeducationthatyouhaveprovidedsothatyoucanassessthepatient’sunderstandingandcorrectanymisunderstandingsthepatientmayhavehad.Alwaysaskifthepatienthasanyquestions.Evenifquestionswereaskedthrough-
out the interview, it is still necessary togive thepatient a chance to ask anyotherquestionsthatmayhavearisenorthatmayhavebeenleftunanswered.Afteraddressinganyquestions,letthepatientknowwhetherfollow-upisneces-
sary.Thiswilldependonwhatoccurredduringthemedicationhistoryandthesettingwherethesessiontookplace.Forexample,ifchangesweremadetothepatient’smed-icationregimen,youmayneedtoscheduleafollow-upappointment.Ifyouwerecon-ductingamedicationhistoryatahealthfair,youmaytellthepatienttofollowupwithhisorherphysicianinaspecifiedamountoftimeorphonethephysicianifyouhaveamedicationconcernthatcannotwait.Additionally,ifamedicationhistoryoccurredinthehospital,youshoulddocumentyourfindingsinthemedicalrecordsothatthemedical teamhasyourcompletemedicationhistoryandcanaddressany issuesanddiscussfollow-upneedsduringthedischargeprocess.Ifyouwillbeinvolvedinthepatient’scareatthehospitalorinasettingthatthepatientmayneedtogetintouchwithyou,besuretoincludeyourcontactinformation.Thefollowingisanexampleofhowyoumightcloseaninterview:“Thankyoufor
alltheinformationyouhavegivenme.Iwillbesuretodocumentthisinyourmedi-calrecord.Beforeyougo,Ijustwantedtomakesurethatwediscussedhowtotakeyouralbuterolinhalerproperly.Wouldyoumindshowingmehowyouwilluseyourinhalerwhenyougethome?”Thepatientshouldthenshowyouhisorhertechnique.You should thenmake anynecessary corrections andhave thepatientdemonstrateusageonceagaintoensurethatthetechniqueisbeingperformedcorrectly.Youcouldthenask,“Whatquestionsdoyouhaveforme?”Afteraddressingallofthepatient’squestions,youmightsay,“Well,itwasgreatmeetingyou.Pleasecallthepharmacy
medication history 27

ifyouhaveanyquestions.Ournumber isonyour label.”Ifyouareat thehospitalandyouareonlyhavingaone-timeinteractionwithyourpatient,youcansay,“Well,thankyouagain for completing themedicationhistory. Iwillbe sure to share thisinformationwiththemedicalteam.Ifanyquestionscomeup,pleasebesuretoasksomeoneonthemedicalteam.”
the patient intervieW in the cOmmunity setting
Manypatientspresent toacommunitypharmacywithself-carecomplaints seekingrecommendationsforanOTCmedication.Priortomakingarecommendation,thepharmacistmustfirstspeakwiththepatientabouthisorherchiefcomplaintsothatanappropriateplancanbedetermined.Thepatientencounterinthecommunitysettinggenerallyoccursinoneoftwo
ways:eitherthepatientpresentstothepharmacycounterseekingadviceorthephar-macist or pharmacy student notices the patient perusing the aisles and approacheshimorher.Ineithercase,thepatientinterviewthatshouldtakeplaceisthesameinordertoappropriatelyassessthesituationandcreateacompleteplan.First,thephar-macistorpharmacystudentshould introducehimselforherself,ask forpermissiontoassesstheproblemandprovideadvice,and/ortellthepatientthatheorshewillbeaskingquestionspriortomakinganyrecommendations.Second,manyquestionsmustbeasked inordertoproperlyassess thepatient. Incontrast toanambulatorycaresetting,boththepharmacistandpatientareusuallyrestrictedintheamountoftimetheycanspendexploringthecomplaintanddiscussingtherecommendationinacommunitypharmacysetting.However,evenwiththetimeconstraints,appropriatequestioningmustoccurinordertoadvisethepatientappropriately.Severalmethodshavebeendevelopedandmnemonicscreatedtoassistthepharmacistinaskingques-tionsaboutthepatient’schiefcomplaintinamethodologicalmanner.Mnemonics include WWHAM, AS METTHOD, CHAPS-FRAPS, Basic 7,
PQRST, and QuEST/SCHOLAR-MAC (table 1.3).11,12 Although each of theseapproaches is valuable in providing amethodologicalmeans of patient assessment,unfortunatelynoneofthemincludeallthequestionsthatneedtobeaddressed.Forexample,manyof themethods donot include a determinationofwho the patientactuallyis,whichisimportantbecauseinsomecasestheindividualaskingyouaques-tionaboutamedicationisnotthepersonwhowillactuallybetakingit.Inaddition,theonlymethodthatdescribeswhattodofollowingtheassessmentistheQueSt/SChOLar-MaCmethod.11 Forexample,sayyouhaveapatientwhopresentstothecounterwithabottleof
acetaminophenandasks,“HowmanyshouldItakeformypain?”Priortoanswering
28 chapter 1 / the patient interview
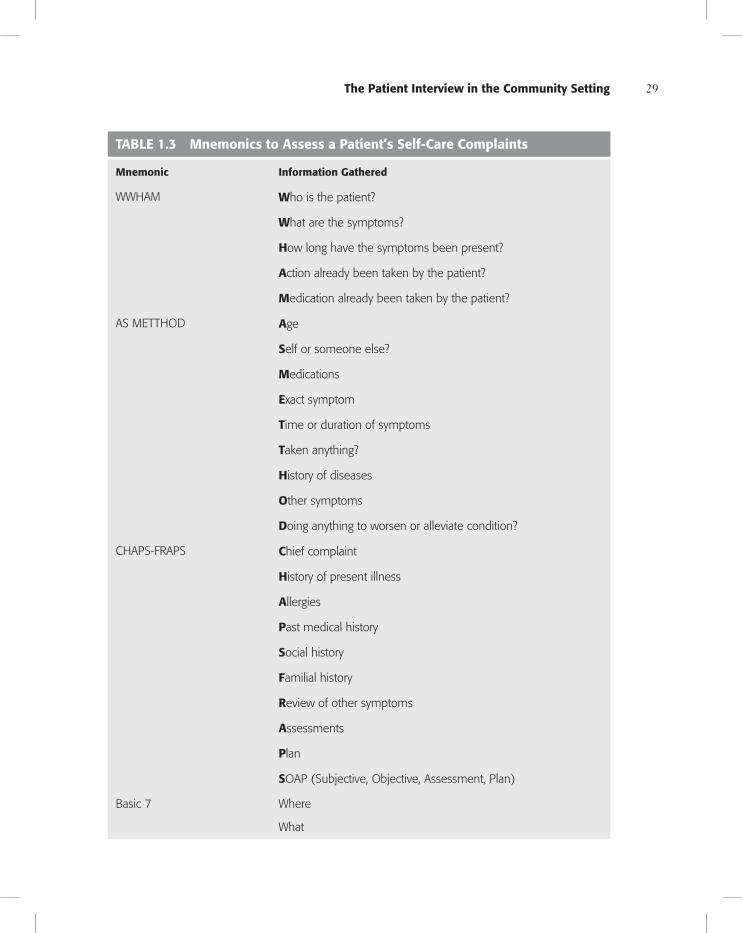
tabLe 1.3 mnemonics to assess a patient’s self-care complaints
mnemonic information gathered
WWHAM Who is the patient?
What are the symptoms?
how long have the symptoms been present?
action already been taken by the patient?
medication already been taken by the patient?
AS METTHOD age
self or someone else?
medications
exact symptom
time or duration of symptoms
taken anything?
history of diseases
Other symptoms
doing anything to worsen or alleviate condition?
CHAPS-FRAPS chief complaint
history of present illness
allergies
past medical history
social history
Familial history
review of other symptoms
assessments
plan
sOAP (Subjective, Objective, Assessment, Plan)
Basic 7 Where
What
the patient interview in the community setting 29

Quality
Severity
Timing
Context
Modifying factors
Associated symptoms
PQRST palliation and provocation
Quality and quantity
region and radiation
signs and symptoms
temporal relations
QuEST Quickly and accurately assess the patient
establish that the patient is an appropriate self-care candidate
suggest appropriate self-care strategies
talk with the patient
SCHOLAR-MAC symptoms
characteristics
history
Onset
Location
aggravating factors
remitting factors
medications
allergies
conditions
Sources: Buring SM, Kirby J, Conrad WF. A structured approach for teaching students to counsel self-care patients. Am J Pharm Educ. 2001;71(1):8; Berardi RR, McDermott JH, Newton GD, et al. Handbook of nonprescription drugs: An interactive approach to self-care. 14th ed. Washington, DC: American Pharmacists Association; 2004.
tabLe 1.3 mnemonics to assess a patient’s self-care complaints (Continued )
mnemonic information gathered
30 chapter 1 / the patient interview

withthedosinginformation,itisyourdutytoascertainthatthepatientisselectingthecorrectmedication.Youcandothisbesaying,“Hello,mynameisAriJones,andIamthepharmacystudentworkinghere.BeforeIansweryourquestion,wouldyoumindifIaskyouafewquestionstoensurethatthemedicationyouhaveselectedisthemostappropriatemedicationforyou?”Oncepermissionhasbeengrantedtocontinuewiththeinterview,youneedtoaskwhothemedicationisfor,becausethepersonwhoarespeakingwithmayhavecometothepharmacytoseekadviceforsomeoneelse,suchasachild,parent,orfriend.Therefore,youshouldask,“Whoisthisfor?”Thenextfewquestionswillberelatedtofindingoutwhatthesymptomisand
characterizingit.Mostlikelyyouwillstartbyasking,“Whatsymptomsdoyouhave?”Oncethepatienttellsyouwhichsymptomsarepresent,itwillbeyourresponsibilitytodeterminewhetheryouneedtoaskmoreprobingquestionstodeterminethechar-acteristicsoftheparticularsymptomandanyotherassociatedsymptoms.Returningtotheacetaminophenexample,ifthepatientstatesthatthemedicationisforhimandthatheneedsitforpain,youwillneedtoaskafewmorequestions.Thesequestionsmightincludethefollowing:
“Whereisthepainlocated?”“Howlonghasthepainbeengoingon?”“Whendidthepainstart?”“Isthepainradiatingtoanywhereelse?”“Doesanythingmakethepainbetterorworse?”“Whathaveyoutriedforthepainalready?Howmuchdidithelp?”“Onascaleof1to10,with1beingtheleastpainand10beingtheworstpain,howwouldyourateyourpain?”
Thesequestionsshouldbeaskedonebyoneandaltereddependingonthepatient’sanswer.Additionally,youarealsoresponsibleforunderstandingthediseaseprocessofthe
symptomandwhatpertinentpositivesandnegativesyouneedtoassess.Forexample,ifthepatientstatesthathispainisinhishead,youneedtoknowthequestionstoasktoeitherruleinorruleoutaheadacheduetoamigraine.Appropriatequestionsinthissituationcould include,butarenot limitedto,“Doyouhaveanysensitivitytolight?”and“Doyouhaveanyothersymptoms,suchasnausea?”Youwill alsoneed todetermineotherpatient-specific factors, suchas age, sex,
weight (especially forachild),PMH,allergies,pregnancy status, andbreastfeedingstatus.Keepinmindthatcollectinginformationforallofthesefactorsisnotneces-saryforeverypatientoreverycomplaint;however,onehastohavetheknowledgetodeterminewhichfactorsarepertinenttocollectineachspecificsituation.
the patient interview in the community setting 31

After asking allof thequestions to assess thepatient’s self-care complaint, youneedtodeterminethenextcourseofactionforyourpatient.TheQuESTmnemonicincludes eachpartof the self-care counselingprocess.11The first partof themne-monic,Qu, stands for “quickly and accurately assessing the patient.” Youmay dothisbyassessingthesevenattributesofasymptom,asdiscussedintheHPIsection.SimilarlytheSCHOLARmethodisalsousedtoobtainmoredetailaboutthepatient’scomplaint.Themnemonicstandsforsymptoms,characteristics,history,onset,loca-tion,aggravatingfactors,andremittingfactors.ThenextletterinQuEST,E,standsfor“establishthatthepatientisanappropri-
ateself-carecandidate.”Thisoccursbyutilizingtheinformationthepatienthasgivenyouandcombiningitwithyourownknowledgeaboutdiseasestatemanagement.Forexample,ifapatienthasasthmaandiscomplainingofacoldthatiscausingshortnessofbreath,youshouldestablishthatthispatientisacandidateforself-care.The S stands for “suggest appropriate self-care strategies.” Once it has been
determinedthatthepatientisaself-carecandidate,meaningthatthepatientwillbeabletotreattheconditioncompletelyoratleastpartlywithoutareferraltoanotherhealthcareprovider,self-carestrategiesshouldbeformulated.TheT stands for “talkwith thepatient.”Asobvious as thismay seem, it is an
importantsteptorecognize,becausetalkingwiththepatientactually includespro-viding comprehensive patient education. Such education will include the self-carestrategy,includingbothnonpharmacologicandpharmacologicagents;theappropri-atedose,frequency,andmaximumdurationofthedrugregimen;howtoadministerandstorethedrug;adverseeffectsandwhattodoincasetheyoccur;whenandhowmuchreliefcanbeexpected;andfinally,whatthepatientshoulddoiftheconditionworsensordoesnotimprove.Similartootherpatientencounters,thepatient’sunder-standingoftheinstructionsshouldbeassessedandquestionsfromthepatientshouldbesolicitedandanswered.12Additionally,regardlessofwhichmethodyouchoosetoutilize forassessing thepatient’s self-carecomplaint in thecommunity setting,youneedtoensurethatyouareaskingallthepertinentquestions,eveniftheyarenotinthemnemonic.
the patient intervieW in the acute care setting
Thepatientinterviewintheacutecaresettingincludesthesameelementsasacom-prehensivepatienthealthhistoryandmedicationhistory.Thedifferenceisinhowtheinterviewisconducted,whichwillbedeterminedbyafewsetting-andpatient-specificfactors,includingthehospitalareainwhichtheinterviewistakingplace,suchasanemergencyroom(ER),ageneralmedicinefloor,oranintensivecareunit,aswellas
32 chapter 1 / the patient interview

thepatient’slevelofalertness.Therefore,yourroleinthepatientinterviewprocessaswellasthepatient’sconditionwilldeterminehowyouwillbeabletoconducttheinterviewandonwhichelementsyouwillfocus.Intheacutecaresetting,itisimportanttotailortheinterviewbasedonitspurpose.
Forexample,intheERthepharmacist’spurposeofperformingamedicationhistorymaybetodeterminewhetherthecauseofthevisittotheERisdrug-related.There-fore,youwillneedtofocusonlearningallthemedicationsthatthepatienthastakenbyaskingthepatientand/orcaregiverorfamilymemberaboutthepatient’smedicationsaswellasbylookingatalistofmedicationsthatthepatientmayhavebroughtwithhimorherorcallingthepharmacytoobtainthisinformation.Dependingonthesitu-ation,theexactstrengths,dosing,andadherencemaynotbeasimportantifthepatientisincriticalcondition;however,oncethepatienthasstabilizedandiseitherbeingsenthomeortoanotherpartofthehospital,itmaybenecessarytocompleteathoroughmedicationhistory toensure thatmedicationerrorsdonotoccur.Forexample, if apatientwithahistoryofasthmaarrivesattheERcomplainingofshortnessofbreath,youshouldaskthepatientwhichmedicationsheorsheiscurrentlytakingforasthmaaswellasdeterminethepatient’sadherencetotheregimen.Adherenceinthiscaseisimportantbecauseitenablesyoutoassessthepossiblecausesoftheasthmaexacerba-tion, includingthelackofadherenceor improperuseofaninhaler.Incontrast, ifapatientcomestotheERcomplainingofchestpain,youshouldnotaskwhetherthepatienthasbeenadherenttoherstatintherapyorifsheiscurrentlysmoking,becausealthough the lackof adherence to a lipid-lowering agent and/or smokingmayhavecontributedtothepatient’spossibleheartattack,thiswouldnotbethetimetoaddressit.However,oncethepatient’schestpainhasbeenaddressedandtreated,assessmentsandcounselingabouttobaccouseandmedicationadherenceshouldoccur.If thepatient is in the intensive careunit, youmayneed toobtain a complete
medication history to ensure that all of the patient’smedical conditions are beingaddressed.However,after the initial comprehensivemedicationhistory,whichmaybeobtained fromeither a familymemberor caregiverorby calling thepharmacy,yourinteractionswiththepatientmaybemorefocusedonspecificpatientcaremea-sures.Forexample,ifthepatientisbeinggivenpainmedicationandisconsciousandalert,yourinterviewmayfocusonfurtherexploringhowthepatient’spainisbeingmanagedandwhatsymptomsheorsheisexperiencingthatarerelatedtothepainandthepainmedication.Ifthepatientisonthegeneralfloorofthehospital,yourinterviewwillbedifferent
basedonthedayofhospitalizationandyourroleinthepatient’scare.Forexample,onthefirstdaythepatientisadmittedtothehospital,themedicalteamwillhaveconductedacomprehensivehealthhistory,anditmaybeyourroletocompleteacomprehensive
the patient interview in the acute care setting 33

medicationhistory.Onsubsequentdays,youmaybe interactingwithyourpatient todiscussongoingtreatmentsandtoaddressanycurrentcomplaints.Evenifamedicationhistoryisnotconductedonthefirstdayofadmittance,itisvitalthatacomprehensivemedicationhistoryisobtainedanddocumentedatsomepointduringthehospitalstay.
chapter summary
Thepatientinterview,includingthecomprehensivehealthandmedicationhistory,isfundamentalinprovidingexcellentandaccuratepatientcare.Thelearningandappli-cationofcommunicationskillsandtechniqueswillallowforapatientencounterthatischaracterizedbyrespectaswellasofferyoutheopportunitytolearnaboutpatient-specific problems, thereby making your assessment, plan, and approach uniquelypatient-centered.Additionally,useofastructuredapproachandframeworktoobtainallthepertinentinformationfromthepatientenablesyoutorelyonasetfoundationevenasyoudirecttheconversationaccordingtotheuniquenuancesofeachparticularpatient.Awarenessofthesettinginwhichyouareconductingthepatientinterviewandknowingthepurposeoftheinterviewwillenableyoutogathertheinformationyouneed tomakeanaccurate assessment andplan,which is essential toprovidinghigh-quality,patient-centeredcare.
take home messages
• Communication skills are the fundamental link between the pharmacist’sexpertiseaboutdrugsandhisorhercontributiontoprovidingexcellentpatient-centeredcare;thesecommunicationskillsmustbelearnedanddeveloped.
• Utilizing the various structured approaches to obtain information from thepatientallowsforyoutoassurethatallthepertinentinformationhasbeengath-ered.Simultaneously,actively listeningduringthepatient interviewwillgiveyoutheopportunitytolearnaboutpatient-specificproblems.
• The approach to the patient interview in a community settingmay be briefversus a comprehensivevisit thatoccurs in theambulatoryor acutecare set-ting;howeverpertinentinformationmustbecollectedtoprovideanappropriateassessmentandplan.
• Thehealthhistoryofapatientremainsthesameregardlessofthepatient-caresetting;howeverthedifferencesareinhowtheinterviewisconducted,patient-specificfactors,andsetting-specificfactors.Itisnecessarytomodifyyourapproachtothepatientinterviewinordertoprovideappropriatepatientcareinanysetting.
34 chapter 1 / the patient interview

revieW QuestiOns
1. Whatarethecomponentsofthecomprehensivepatientinterview? 2. Whatarethecomponentsofthemedicationhistory? 3. DescribetheQuEST/SCHOLAR-MACmethod. 4. Whatisthedifferencebetweenaleadingquestionandaprobingquestion? 5. Describethedifferencesbetweenconductingamedicationhistoryforapatient
intheemergencyroomversus thepatient inan intensivecareunitversus thepatientonageneralmedicinefloor.
reFerences
1. HugmanB.Healthcare communication.Philadelphia:PharmaceuticalPress;2009;80–82. 2. BergerBA.Communication skills for pharmacists.3rd ed.Washington,DC:AmericanPharmacists
Association;2009;25–29. 3. Empathy. Available at: http://dictionary.reference.com/browse/empathy. Accessed June 17,
2012. 4. BickleyLS.Bates’ guide to physical examination and history taking.9th ed.Philadelphia:Lippincott
Williams&Wilkins;2007;1–95. 5. KaplanCB,SiegelB,Madill JM,EpsteinRM.Communicationandthemedical interview—
strategiesforlearningandteaching.J Gen Intern Med. 1997;12(2). 6. ASHP Statement on Pharmaceutical Care.Medication therapy and patient care:Organiza-
tion and delivery of services-statements. Available at: www.ashp.org/doclibrary/bestpractices /orgstpharmcare.aspx.AccessedJune3,2012.
7. Walker HK, HallWD, Hurst JW, eds.Clinical methods: The history, physical, and laboratory examinations. 3rd ed. Boston: Butterworths; 1990. Available at: www.ncbi.nlm.nih.gov/books /NBK201/.AccessedFebruary7,2013.
8. Guidelinesfortheearlymanagementofadultswithischemicstroke.Availableat:http://stroke .ahajournals.org/content/38/5/1655.full#cited-by.AccessedJune3,2012.
9. EllingtonAM,BarnettCW,JohnssonDR,NykampD.Currentmethodsusedtoteachthemed-icationhistoryinterviewtodoctorofpharmacystudents.Am J Pharm Educ. 2002;66:103–107.
10. FitzGerald RJ. Medication errors: The importance of an accurate drug history. Br J Clin Pharmacol.2009;67:671–675.
11. BuringSM,KirbyJ,ConradWF.Astructuredapproachforteachingstudentstocounselself-carepatients.Am J Pharm Educ. 2001;71(1):8.
12. BerardiRR,McDermottJH,NewtonGD,etal.Handbook of nonprescription drugs: An interactive approach to self-care.14thed.Washington,DC:AmericanPharmacistsAssociation;2004;3–37.
references 35
