the northwest territories’ - nhlc / cnls learned_leith_dc coleman.pdfrequirements for renal...
TRANSCRIPT
cfhi-fcass.ca
The Northwest Territories’ Experience Leading Improvement in Chronic Disease Management
National Health Leadership Conference Panel Session
June 2nd 1:30 pm – 3:00 pm

Northwest Territories (NWT) Context
5.2% of the population was living with diabetes in 2009
Between 2008/2009 and 2010/2011, diabetic patients accounted for 9% of unique
patients, 16% of bed days and 15% of overall costs
Between 2008 and 2011, renal disease accounted for more than 2,000 bed days/year at an estimated cost of $5.2 million
Uncoordinated approach to renal care and inability to properly identify the precise stage of renal disease in each patient
Mental health service delivery often involves multiple authorities at various levels
Processes and procedures for patient referral and information sharing among
various agencies have historically been unaligned
2
Adapted from Doucet & Beatty (2010); Northwest Territories Health and Social Services (2012); Department of Health Victoria, Australia; Northwest Territories Health and Social Services (2011); Ministry of Health and Long-Term Care (2007).

Tackling Chronic Disease: NWT Chronic Disease Management (CDM) Project
• Launched in September 2010
• Partnership between the NWT Department of Health and Social Services (DHSS) and the Canadian Foundation for Healthcare Improvement (CFHI)
• Focus on the management and prevention of chronic disease through improvement projects (IPs) that informed a roadmap for sustainable change
3

Northwest Territories System Objectives
• Develop an integrated CDPM strategy
• Develop capacity for implementation and change management
• System improvement using tracer projects and scale lessons learned
4

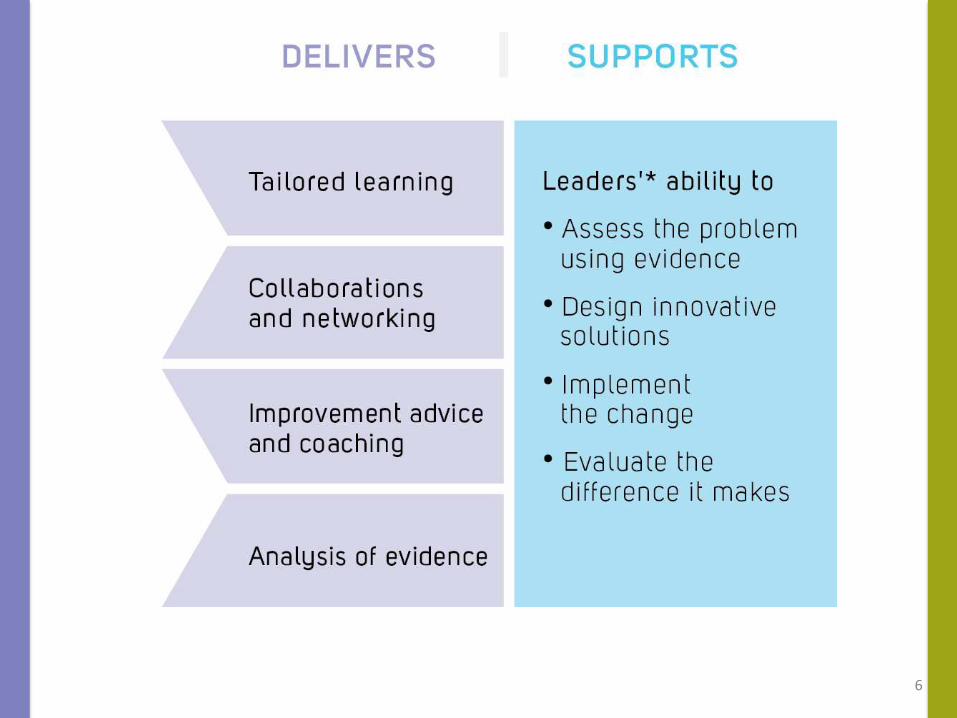
CFHI Improvement Model
5
6

Levers for accelerating healthcare improvement™
7
In press, to be published in spring 2014.

The Expanded Chronic Care Model (ECCM)
8

Applying the Expanded Chronic Care Model (ECCM) to the CDM Project
• The ECCM shows how population health promotion and clinical health services can complement one another to improve the health of, and healthcare provided to, patients and communities.
• The IPs pinpointed specific aspects of each ECCM element where the Department believed improvements were achievable:
• Diabetes IP: Self-management support – the integration of self-management support into regular care
• Mental health IP: Decision support and information systems – clinical pathways and service agreements as coordination tools in health system design
• Renal IP: Health system design and decision support – the use of clinical practice guidelines in decision support and the use of the NWT’s new EMR information system as a patient database
9
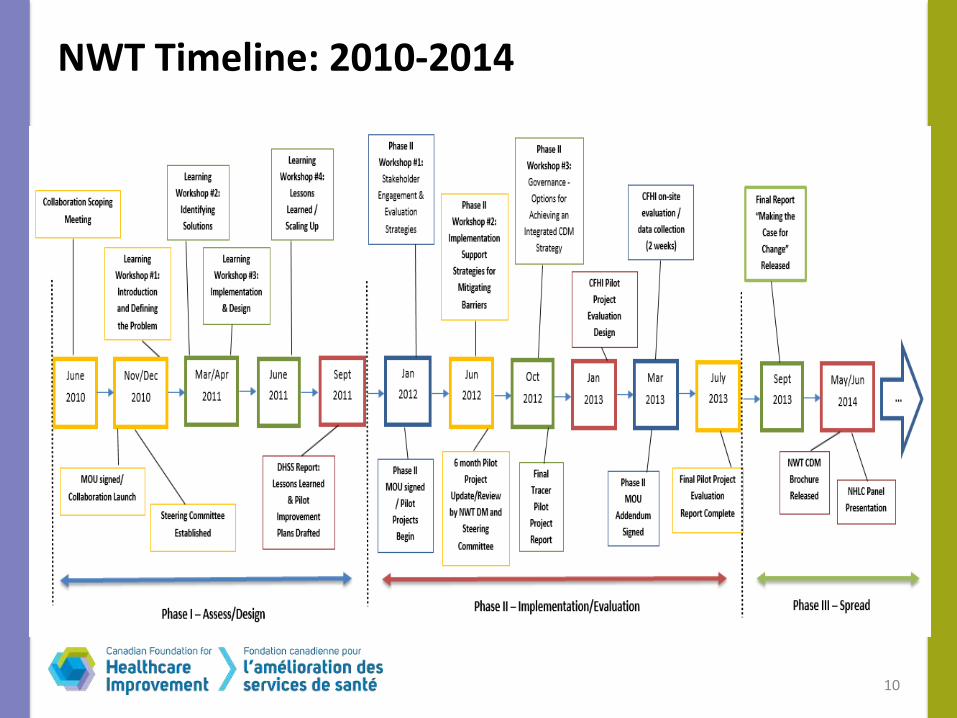
NWT Timeline: 2010-2014
10
Applying CFHI’s Approach to Healthcare Improvement to the NWT Context
Three project objectives were identified:
1. Develop and implement diabetes, renal disease and mental health IPs that maximize the use of resources and provide care based on evidence and informed practices.
2. Draw lessons from these projects to inform development of an integrated CDM strategy.
3. Strengthen capacity and self-reliance for the use of evidence.
11
Selecting the Three Improvement Projects (IPs)
12
Diabetes Project
• Goal: • Build primary
care teams’ capacity to provide self-management support (SMS) to type 2 diabetes patients
Renal Disease Project
• Goal: • Improve and
integrate the provision of renal care to NWT residents
Mental Health Project
• Goal: • Standardize
processes and procedures for referral and information sharing
Renal IP process
Initial problem identification:
• Perceived high prevalence of renal disease/dialysis rates
• Known high risk population for renal disease
• Poor ability to predict future resource requirements for renal replacement therapy given unclear rates of transition through stages of increasingly severe renal disease
13

Drilling down to the root causes: “how do we know what the problems really are?”
• Lack of system-wide data on incidence and prevalence of CKD by stage of disease
• No established processes for referral and follow-up of renal patients
• Inconsistent case definitions for renal disease across providers
• Lack of clinical guidance for primary care clinicians for early detection and follow up of CKD
• Patients were being lost to follow up due to turnover of care providers and multiple follow up paths.
14
Solutions
• Assembling a team of key stakeholders to inform best practice solutions
• Establishment of a Territorial Renal Care database
• Develop a single entry point to the NWT Renal Care Program for consistent referral, assessment and management of renal disease
• Algorithm for primary care decision support of early stage renal disease detection and management, including formalized case definitions
15

Focusing on Renal IP Results
• Improved care delivery and increased early detection
• The number of known individuals with renal disease increased from 40 to 400, once new screening and referral processes were in place
• GPs have made most referrals prior to the project. Since the project, more than ¾ of referrals during the project came from other practitioners
• 40% of new dialysis start are individuals not previously known or followed by the renal clinic
Next Step: Develop a system wide approach and identify resource requirement and review of the clinical practice guidelines (2 year cycle)
16
Year New diabetic kidney disease cases (not
taking into account the potential for increased incident rates over time)
Estimated Renal Program numbers (based on new diabetic kidney disease
referrals alone)
Potential number of NWT patients progressing to ESRD*/year who will require RRT**, based on up to a 2% year over year progression rate
2013 70 350 “actual” new starts were 11
2014 70 420 up to 8.4 patients (in addition to the current 11 patients)= 19
2015 70 490 up to 9.8 patients = 29 patients
2016 70 560 up to 11.2 patients = 40 patients
2017 70 630 up to 12.6 patients = 53 patients
*ESRD: End stage renal disease **RRT: Renal replacement therapy
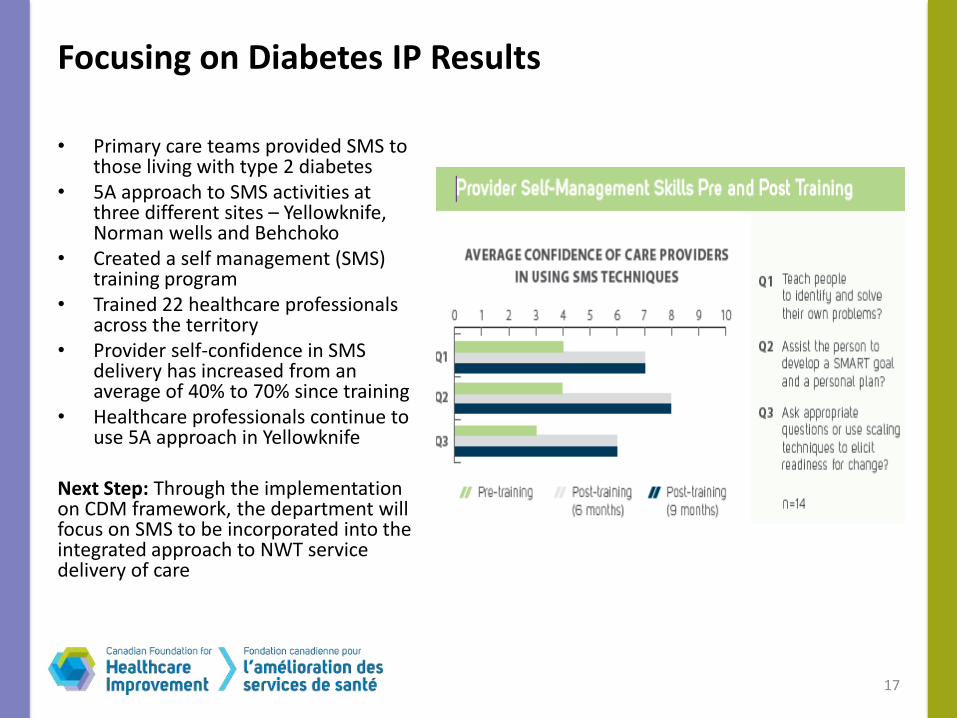
Focusing on Diabetes IP Results
• Primary care teams provided SMS to those living with type 2 diabetes
• 5A approach to SMS activities at three different sites – Yellowknife, Norman wells and Behchoko
• Created a self management (SMS) training program
• Trained 22 healthcare professionals across the territory
• Provider self-confidence in SMS delivery has increased from an average of 40% to 70% since training
• Healthcare professionals continue to use 5A approach in Yellowknife
Next Step: Through the implementation on CDM framework, the department will focus on SMS to be incorporated into the integrated approach to NWT service delivery of care
17

Focusing on Mental Health IP Results
• Developed standardized referral and information sharing pathways
• Improved information exchange between practitioners throughout the patient transfer process
• Facilitated integration between services (improved patient handoffs / discharges)
• Offered orientation through telehealth to new users
• Improved awareness of services and key players, reducing gaps in care (improved continuity of care)
• Increased communication and role clarity among providers
Next Step: The pathways are now part of Mental health Action Plan: A Shared Path Towards Wellness – The Mental Health and Addictions Action Plan, 2012-2015.
• A plan to implement pathways across NWT is being developed.
18
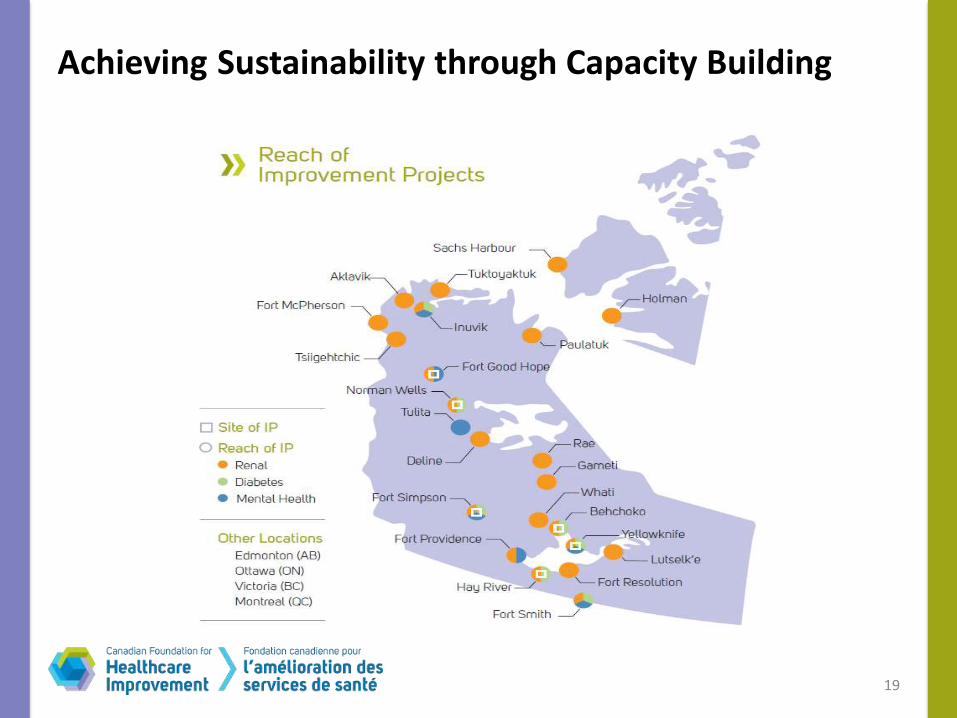
Achieving Sustainability through Capacity Building
19
From IPs to Recommendations: Key Lessons from the NWT Experience
1. Self-management support should become standard practice for all primary care staff in NWT.
2. Adopt standardized policies and pathways for clinical referral and information sharing.
3. Support the use of integrated case management practices for patients with complex chronic care needs.
4. Integrate the use of evidence-based, standardized clinical practice guidelines for other chronic diseases.
5. Establish clear guidelines and pathways for patient consent and information sharing.
6. Establish standardized data collection and monitoring for all CDM initiatives.
7. Align future CDM work with the development of a territorial clinical information system.
20
Current Status
• Adopted the use of the Expanded Chronic Care Model (ECCM) and developed a draft CDM framework
• Ongoing revision and implementation of Territory-wide clinical standards
• An unintended result: identified need for system-level approval process and a Territorial Clinical Standards Committee established
21

Reflections from the NWT
22

Breakout Session
1. In light of the six levers for healthcare improvement, reflect on the care that is currently being provided in your organization:
• What are your organization’s strengths? What are potential areas of improvement?
2. How do you intend to go from the care you’re currently providing to the care you want to be providing?
23

Turning it Over to the Audience
• Think about an example of an improvement activity in your organization that you participated in and describe, in 3 minutes, the following:
1) What worked and why?
2) What did not work and why?
24

Resources
• CFHI. (2013). Making the Case for Change: Advancing the NWT Chronic Disease Management Strategy.
• Department of Health Victoria, Australia. Chronic disease management audit tools: A fact sheet for primary care partnerships. Retrieved from: http://www.health.vic.gov.au/ pch/downloads/factsheet02.pdf.
• Doucet, G., Beatty, M. (2010). The Cost of Diabetes in Canada: The Economic Tsunami. Canadian Journal of Diabetes. Retrieved from: http://www.diabetes.ca/documents/forprofessionals/CJD--March_2010--Beatty.pdf
• Ministry of Health and Long-Term Care. (2007). Preventing and managing chronic disease: Ontario’s framework. Retrieved from: http://www.health.gov.on.ca/en/pro/programs/cdpm/pdf/framework_full.pdf
• Northwest Territories Health and Social Services. (2011). Renal disease improvement project phase I report (Unpublished).
• Northwest Territories Health and Social Services. (2012).Chronic Disease Management in the Northwest Territories Interim Report (Unpublished). Yellowknife, NWT: Government of Northwest Territories.
25

cfhi-fcass.ca
Thank you
For further information please contact CFHI:
Erin Leith [email protected]
26