the nicu – while life-saving, is nothing like the womb ... · pdf filegavage feeding...
TRANSCRIPT

9/8/16
1
Family-CenteredDevelopmentalCare:Suppor6ngA9achment
intheNICU
Raylene Phillips, MD, FAAP, FABM, IBCLC
Loma Linda University Children’s Hospital
I have no conflicts of interests
and nothing to disclose
TheNICU–whilelife-saving,isNOTHINGlikethewomb!
� Bright and loud sounds � Frequent touch – often painful
� IV line placements and blood draws � Intubation and suctioning
� Gavage feeding tube insertions
� X-rays, ultrasounds, and eye exams � Daily physical examinations
� Frequent assessments of vital signs � Bathing and weighing
� Separation from mother
Separa6onfromMother
AParent’sViewoftheNICU“Where is my baby?”
“Whereismymother?”

9/8/16
2
Parentsare“PrematureParents”� Who often feel guilty, usually helpless and
always terrified for the life of their prematurely born baby
Mother-InfantDyad
Asinglepsychobiologicalorganism
� “There is no such thing as an infant. The infant and maternal care together form a unit.” Winnicott, 1965
�
MaternalBonding� “When a baby is born, a mother is born”
� Mother is totally focused on caring for baby to the exclusion of everything else � “Primary maternal preoccupation” Winnicott
� Neuronal mechanisms regulate maternal behavior � Medial preoptic area of the hypothalamus � Projections to the mesocorticolimbic dopaminergic
system
Diaz-Rossello NeoReviews 2008
A9achmentHormones� Attachment is biological primed
� Biochemical bonding/attachment activators in our neuronal reward circuitry � Trigger maternal caregiving
� Increased by skin-to-skin contact � Oxytocin
� Vasopressin � Prolactin
� Dopamine
� Estrogen � Endogenous opiod peptides
Fetal brain development From CONCEPTION fetal brain growth is influenced by genes (the DNA) But from the beginning, brain growth
is an active process.
N. Bergman
Fetal brain development By 20 weeks gestational age all organ structures are formed Brain growth occurs
by parallel development of structure & function (Hugo Lagercrantz 2004)
Brain development depends on experiences !!
N. Bergman
(Shore, 2001)

9/8/16
3
Fetal Brain Development
40 wks
28 wks 22 wks 14 wks 10 wks
32 wks
“Cri6calPeriod” Window of opportunity in early life when a child’s brain is exquisitely primed
to receive sensory input
in order to develop more advanced
neural systems
AmygdalaandBrainDevelopment� Areas of the amygdala...are in a critical period of
maturation...in the first two months after birth � Amygdala - Limbic System
� Emotional learning � Memory modulation � Activation of sympathetic
nervous system
� Skin-to-skin contact activates the amydala via the prefrontal-orbital pathway
Schore, Infant Mental Health Journal, 2001
TouchandBrainDevelopment
� The fetus has well developed senses of: � Touch, proprioception, smell
� These senses connect directly to the amygdala via the prefrontal-orbital pathway, the first and essential part of an efficiently regulated and
organized right brain.
Schore, Infant Mental Health Journal, 2001
TouchandBrainDevelopment
• “In early postnatal life, maintenance of critical levels of tactile input … is important for normal brain maturation. “
Schore 2001
� “... the baby must spend most of its time in its mother’s arms to get the full benefit of her sensory environment…”
White,ClinicsinPerinatology,2004
Face-to-face communication Eye-to-eye orientations Voice-ear interactions Hand/facial movements/touch
Active Brain Development ( brain wiring)
Baby - Mother Communication

9/8/16
4
A newborn has a basic biological need for contact with mother
9/8/16
5
A9achmentandRegula6on
� “Attachment relationships are formative because they facilitate the development of the brain’s
self-regulatory mechanism.”
Fonagy & Target, Psychoanalytic Inquiry, 2002
NeurologicallyImmatureAt birth the human infant is the LEAST neurologically mature primate of all, and the most reliant on physiological regulation by the caregiver for the longest period of time.
McKenna
MotherisBaby’sRegulator� “The dyadic interaction between the newborn and the mother constantly controls and modulates the newborn’s exposure to environmental stimuli and thereby serves as a regulator of the developing individual’s internal homeostasis.”
Ovt-scharoff , Neuroscience, 2001
A9achmentandBrainDevelopment
� “The regulatory function of the newborn-mother interaction may be an essential promoter to ensure the normal development and maintenance
of synaptic connections during the establishment
of functional brain circuits.”
Ovt-Scharoff , Neuroscience, 2001

9/8/16
6
TheParen6ngEnvironmentandBrainDevelopment
� “There is now solid evidence that the parenting environment influences the neural connections
that underlie infant behavior. “
Dawson 1994
Attachment and Brain Structure
“Early interpersonal events positively and negatively impact the
structural organization of the brain.”
“The brain is designed to be sculpted into its final configuration by the effects of early experiences. These experiences are embedded in the attachment relationship. “
Schore, Infant Mental Health Journal, 2001
A9achmentasBrainOrganizer� “If the attachment relationship is indeed a major
organizer of brain development… then the determinants of attachment relationships are important far beyond the provision of a fundamental sense of safety or security.”
Fonagy, Attachment and Human Development, 2005.
What Can We Do in the NICU?
� To support infants
� To support parents
� To help support emotional connections
� To help heal the wounds of mother-infant separation
Family-CenteredCare� An approach to planning, delivery, and evaluation of
healthcare that supports partnerships among patients, families, and healthcare team.
� It is founded on the principle that the family plays a
vital role in ensuring the health and well-being of the infant.
� Over time, the family has the greatest influence on an infant’s health and well-being.
American Hospital Association Institute for Family Centered Care
GoalsofFamily-CenteredCare
� To reunite the family � To resume interrupted parent-infant bonding
Ø To support parents in their role as the most important caregivers for their infant
9/8/16
7
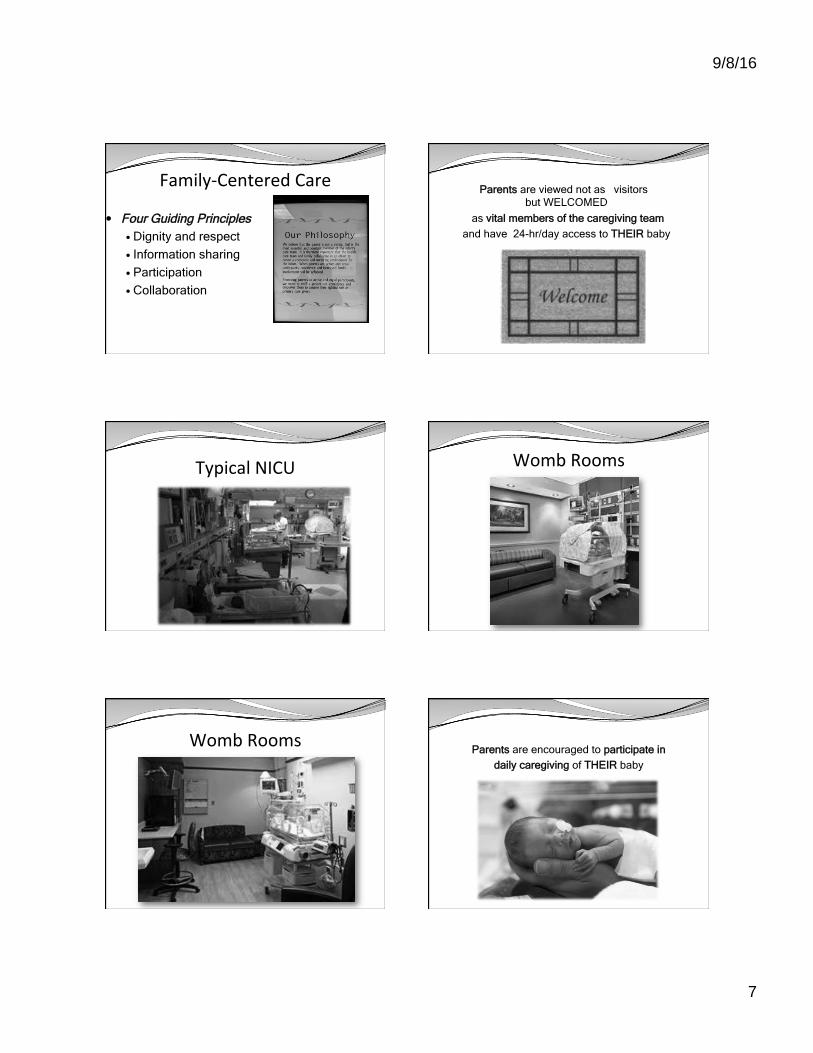
Family-CenteredCare
� Four Guiding Principles � Dignity and respect
� Information sharing
� Participation
� Collaboration AmericanHospitalAssociation InstituteforFamilyCenteredCare
Parents are viewed not as “visitors” but WELCOMED
as vital members of the caregiving team
and have 24-hr/day access to THEIR baby
TypicalNICU WombRooms
WombRoomsParents are encouraged to participate in
daily caregiving of THEIR baby

9/8/16
8
HelpingParentsCOPE� Creating Opportunities for Parent Empowerment
� Designed to make parent-infant interactions a more positive experience
� Enhance parent mental health outcomes
� Parents report significantly less stress in the NICU
� Less depression and anxiety
� More positive interactions with infants
� Infants had 3.8 days shorter NICU length of stay
� VLBW infants (less than 1500 g at birth) had 8 days shorter length of stay
Melnyk BM,, Pediatrics 2006
ParentSupportOrganiza6ons
Na6onalPerinatalAssocia6on� InterdisciplinaryRecommendationsforthePsychosocialSupportofNICUParents
JofPerinatology,2015
www.nationalperinatal.org
Suppor6ngParents
� Welcome them daily to baby’s bedside � Acknowledge ambivalence of their feelings
� Encourage time just to be with THEIR baby
� Empower them to do daily cares – be a parent
� Teach infant massage
� Inform about risks for PTSD and depression
� Provide resources for professional help and support
Suppor6ngBabiesTalking to Babies
Myriam Szejer, MD
Telling babies their stories is healing
Suppor6ngBabiesHolding Babies
Holding with your heart
Transport babies

9/8/16
9
Suppor6ngBabiesHolding Babies
Holding with your eyes
Charlie's baby
Suppor6ngBabiesHolding Babies
Holding with your hands
Steven’s dads
Suppor6ngBabiesHolding Babies
Holding with your arms
Daniel’s Mom
Suppor6ngMothersandBabiesTogether
In Family-Centered Care skin-to-skin contact is
actively encouraged and facilitated
Natural Habitat for Newborns

9/8/16
10
Natural Habitat for Newborns Natural Habitat for Newborns
TheNaturalHabitatforHumanNewbornMammals
Prof Peter Hartmann, UWA
ThermalSynchronyDuringSkin-to-SkinContact
� Temperature of mother’s chest will increase
by 2 degrees Celsius if baby is too cool.
� Temperature of mother’s chest will decease
by 1 degree Celsius
if baby is too hot.
IndividualizedThermalSynchrony
Each breast independently regulates baby’s temperature
ThermalSynchronyChallenge?

9/8/16
11
HistoryofKangarooMotherCare
(KMC)LATE KMC Drs Rey & Martinez
1979 - Bogota, Colombia BIRTH KMC Dr. Nils Bergman, Agneta Jurisoo 1987 - Manama, South Africa
N. Bergman
Manama, South Africa
Birth Weight: 1000 - 1500 g
Survival before KMC 10% Survival with KMC 50%
Weight gain per day 30 g/day
Breastfeeding rate 100% N. Bergman
PERCENTAGE SURVIVAL BY BIRTH-WEIGHT
0
20
40
60
80
100
<1000g 1000g 1100g 1200g 1300g 1400g 1500g 1600g 1700g 1800g 1900g
Birth weight intervals
Pe
rce
nta
ge
su
rviv
ed
KMC babies Pre-KMC babies
Manama, South Africa
N. Bergman
Is KMC as safe as incubators for preterm infants
immediately after birth?
First Randomized Controlled Trial to compare
KANGAROO MOTHER CARE
and CONVENTIONAL
INCUBATOR CARE
For preterm infants from birth to 6 hrs of life
Primary Hypothesis Skin-to-skin contact with Kangaroo Mother Care (KMC) from birth is superior to conventional method of care with incubator (CMC) for low birthweight infants ONLY the HABITAT differed KMC = Kangaroo Mother Care CMC = Conventional Method of Care
N. Bergman

9/8/16
12
Subjects ( n = 34) KMC CMC Mean weight 1813 g 1866 g Mean GA 34.2 w 35.3 w Approp’ GA 65% 64% Male 60% 50% N. Bergman
SCRIP SCORE 2 1 0 Heart rate
Regular
Deceleration
to 80-100
Rate <80 or >200 bpm
Respiratory rate
Regular
Apnoea <10s, or periodic breathing
Apnoea >10s Tachypnoea
>80 pm
Oxygen saturation
Regular >87%
Any fall to 80
– 87%
Any fall below
80%
Stability of Cardio-Respiratory system In Preterm Infants Fischer et al, 1988
Score allocated for a five-minute period of continuous observation with maximum score of 6 for each period
N. Bergman
RandomizedControlledTrialMother(KMC)vs.Incubators(CMC)
Kangaroo Mother Care (KMC)
Stable at 6 hours of life
Unstable at 6 hours of life Conventional Method of Care (CMC)
Birth Weight 1200-2200 g
4
5
6
60min 90min 120min 150min 180min 210min 240min 270min 300min 315min 330min 345min 360min
BIRTH RCT - SCRIP SCORES
KMC CMC
Bergman, Acta Paediatrica, 2004
Percent of Infants with 100% SCRIP Stability Scores
KMC CMC 1200 g to 2200 g
1- 6 hr 56% 11%
@ 6 hr 100% 46%
1200 g to 1800 g
1- 6 hr 44% 0%
@ 6 hr 100% 25%
Bergman Acta Paediatrica, 2004
Stabilisation first 6 hours, average hourly SCRIP score
5.1
5.2
5.3
5.4
5.5
5.6
5.7
5.8
5.9
6
6.1
2nd 3rd 4th 5th 6th
KMC allKMC <1800CMC allCMC <1800
INCUBATORS DE-STABILIZE Premature Newborns
N. Bergman
CONCLUSION
KMC started from birth is superior to incubator
for infants 1200 – 2199 g with respect to
stabilization as defined by basic physiological parameters
(HR, RR, Ox sats, apnea)

9/8/16
13
KMC is
safer!
N. Bergman
Mothers are Superior to Incubators
in stabilizing healthy preterm infants at birth
Bergman Acta Paediatrica, 2004
Skin-to-Skin Contact Promotes Normal Sleep Patterns
� STS contact increases � Quiet sleep � REM sleep � Normal sleep cycles
Ludington-Hoe, Pediatrics 2006
IncreasesWeightGain� STS contact associated with increased weight gain
Sieratzi, Lancet, 1996, Charpak, Ruiz-Pelaez, & Figueroa, 2005, London, 2006
DecreasedLengthofStay� STS contact associated with shorter hospital stays
Sieratzi, Lancet, 1996, Charpak, Ruiz-Pelaez, & Figueroa, 2005, London, 2006
IncreasesImmuneProtec6on� STS contact increases antibodies in mother’s milk � Decreases incidence and severity of nosocomial infections
Hurst, Journal of Perinatology, 1997, Conde-Argudelo, Diaz- Rossello, & Belizan, 2003

9/8/16
14
Enteromammary Immune System
Lawrence & Lawrence, 5th ed, 1999, pg 166.
IncreasesBreastmilk� STS contact increases breastmilk production by
increasing prolactin levels
Ludington-Hoe, 1996, Mohrbacher & Stock, 2003
IncreasesBreasXeeding� Preterm infants can practice breastfeeding anytime � Goal: Feeding at the breast before discharge
ProlongsBreasXeeding� STS contact increases breastfeeding duration
At Discharge After Discharge
Ludington-Hoe, 1996, Mohrbacher & Stock, 2003
IncreasesParents’Confidence� STS contact increases parent’s confidence and sense of
competence in handling tiny infant
Uvnas-Moberg, 2003, Tessier et al., 1998, Kirsten, Bergman, & Hann, 2001 Conde-Agudelo, Diaz-Rossello, & Belizan, 2003;
Con6nues“Gesta6on”OutsideWomb
� STS contact brings babies back in contact with their mothers

9/8/16
15
HelpsMothersCopewithGrief� STS contact helps mothers cope with grief from loss of
term pregnancy and normal term infant
� Helps to “complete gestation”
PromotesBondingandA9achment
Uvnas-Moberg,2003,Tessieretal.,1998,Kirsten,Bergman,&Hann,2001,Conde-Agudelo,Diaz-Rossello,&Belizan,2003
DadsNeedToBondToo EvenFutureDads
Forprematureinfants…skin-to-skincontactisESSENTIAL
–notanop6onalac6vity!
Skin-to-SkinContactonMechanicalVen6la6on

9/8/16
16
Skin-to-SkinContactonHighFrequencyJetVen6la6on
“JAKOB” Photo story on
www.kangaroomothercare.com/photo.htm
Born 24 w EGA 593 g Continuous SSC since 25 w On VENTILATOR for BPD 1300 g at time of photo
N. Bergman
N. Bergman
“JAKOB”
Same technology NEW HABITAT
N. Bergman

9/8/16
17
253/7wGA,625g–5daysoldHighFrequencyJetVen6la6on “We’reinthistogether.”
AFamiliarHeartbeatMommyisHere
9MonthsOld(6monthsPMA)

9/8/16
18
A new awakening ...
A “New” Paradigm” ...
N. Bergman
Humanity
ANDTechnology

9/8/16
19
Humanity
ANDTechnology
Baby Stohm, 780g
N. Bergman
OurNICUWorld� Sometimes feels like a dark place
� Filled with tiny traumatized fetuses struggling to live � And anxious traumatized parents struggling to cope
AwarenessBringsLight
� That all babies, no matter how small, know their mothers
� That supporting a baby’s emotional connection with mother (and father) makes a difference in short- and long-term outcomes
SharedKnowledgeInspiresCourage
� It takes courage to initiate and sustain change � The support of others with shared knowledge inspires
courage
CommunityIncreasesStrength� Supporting each other as caregivers in the NICU,
increases the strength and effectiveness of our efforts
Togetherwecanmakeadifference

9/8/16
20
TogetherwecanchangetheworldOnebabyandonefamilyata6me!
Thankyou
A person’s a person no matter how small
Dr. Seuss