the never ending battle of dengue crisis - moh.gov.my never ending battle of dengue crisis professor...
TRANSCRIPT
The Never Ending Battle of Dengue Crisis
Professor Lucy LumDepartment of Paediatrics
Faculty of MedicineUniversity of Malaya
11TH MOH –AAM SCIENTIFIC MEETING, 12 August 2015
1

Dengue in Malaysia: Incidence: 1999-2014
1 Adapted from data obtained directly from the Vector Borne Diseases Control Sector, Disease Control Division, MOH; 2. Lam SK, Trop. Med. 1993.35: 195-200.; 3 Al-Muhandis N, Hunter PR, 2011. PLoS Negl Trop Dis 5(8): e1278.; 4 World Health Organization Western Pacific Regional Office based on data provided by the Member States 2014 data from MoH Malaysia
0
20,000
40,000
60,000
80,000
100,000
120,000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Rep
ort
edo
f d
engu
e ca
ses
↑159%
2

DENGUE DEATH MALAYSIA 1997 – 2014
52
82
37
45
50
99
72
10
2 107
92
98
112
88
134
36
35
92
0
20
40
60
80
100
120
140
160
199
7
199
8
199
9
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
8
200
9
201
0
201
1
201
2
201
3
Nu
mb
er
of
De
ath
Year
132%
215
20143

Dengue in Malaysia: 2014
108,698
Reported Cases
45,653 Hospitalized
Cases
215
Deaths
4
41% Hospitalization

Malaysia: As of 4 July 2015,
• 59,365 cases of dengue with 165 deaths.
• 33.4% higher compared with the same reporting period of 2014
Number of dengue cases per week 2014-2015, Department of Health, Malaysia 5

Measures to cope with increased patient load
• Full blood count analysers in most health clinics and emergency departments in major hospitals
• Dengue Combo kit NS-1Ag, IgM/IgG testing made available
• Extended working hours of health clinics to relieve the patient load of ED in major hospitals.
• Opening of wards for influx of patients
• Training in case management has been intensified at several levels of health care.
• Volunteers ….
6
Out-patient Clinic, Klang Valley
7

Patients’ long wait
8

Survive95-99.5%
Die0.5 - 5%
Infection Incidence ~ 5% / year
Asymptomatic 75%
Symptomatic 25%
Dengue fever95-99%
Severe dengue1-5%
Adapted from Vaccine 2004; 22: 1275-1280
Natural History of DENV Infections
9

Dengue among ASEAN countries in 2013:Cases, Deaths and Case fatality rate
Country Reported Cases
(deaths)
Case fatality rate
(CFR%)
Cambodia 16,722 (53) 0.35%
Philippines 166,107 (528) 0.32%
Lao PDR 44,171 (95) 0.22%
Malaysia 43,346 (92) 0.21%
Thailand 150,934 (136) 0.09%
Vietnam 60,588 (38) 0.05%
Singapore 22,205 (7) 0.03%
Data from WHO (SEARO) and (WPRO)
0.28% in 2015
10

Acknowledgements
This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials were contributed by the Ministry of Health, Singapore, the United States Centers for Disease Control and Prevention, and the University of Malaya Medical Centre.
Dengue Clinical Management
MODULE 4: Clinical Course of Disease
MODULE 5: Case Classification and Differential Diagnosis
MODULE 6: Patient Assessment & EvaluationMODULE 7: Outpatient Management
MODULE 8 A – D: IV Fluid therapy

Training in case management
12%
88%
Medical Personnel
Trained (8) Untrained (58)
12

Regular /Compulsory
Dengue Training
Program For Doctors - 2015
13

REALITY
• Dengue Deaths are preventable
• It is not possible to predict the course of illness
• Daily ambulatory follow-up during the febrile phase is necessary to avoid unnecessary admissions and detect patients going into severe dengue
• The most important prognostic factor for severe dengue is a TRAINED and WELL REHEARSED MEDICAL AND NURSING TEAM
14

Back to Basics: History taking
15

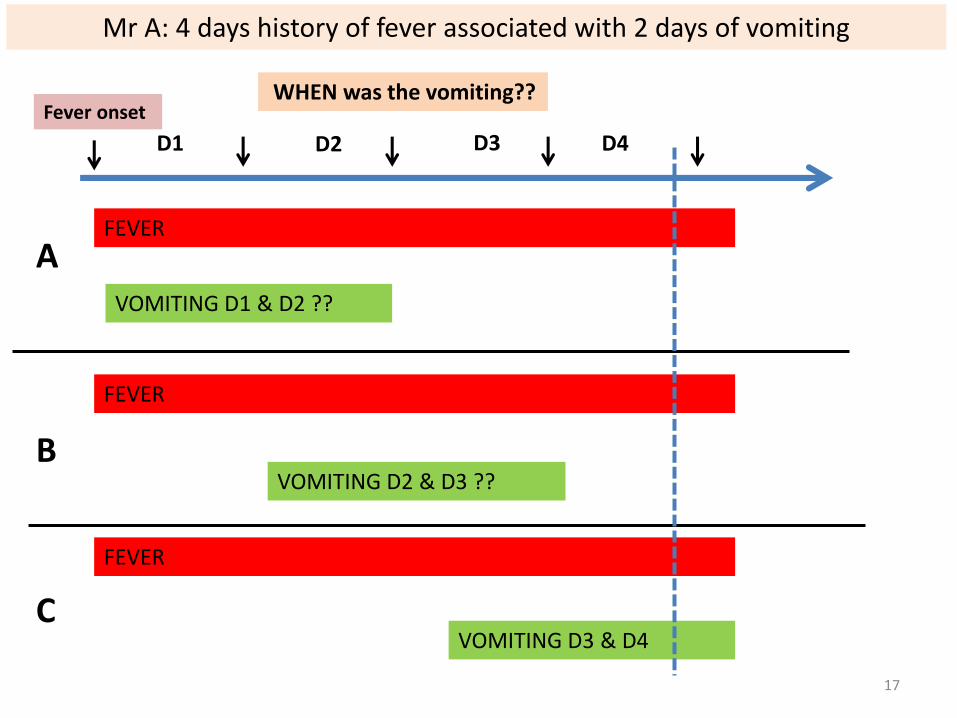
Mr A, came to ED on D4 of illness,referred from GP as ?Dengue Fever
S/B ED MO: Fever 4 days associated with vomiting 2 days, • No abdominal pain• No bleeding• Diagnosis: Dengue Fever, ordered FBC, referred medical
S/B Medical MO: Fever 4 days associated with vomiting 2 days, • No abdominal pain• No bleeding• Diagnosis: Acute Gastroenteritis
Questions? Same patient with same complaints,2 doctors, 2 different diagnosis. WHY?
16
VOMITING D3 & D4
FEVER
C
FEVER
VOMITING D1 & D2 ??
A
B
FEVER
VOMITING D2 & D3 ??
Mr A: 4 days history of fever associated with 2 days of vomiting
D1 D2 D3 D4
Fever onset WHEN was the vomiting??
17

The Changing Faces of Dengue
• Co-morbid conditions – diabetes mellitus, hypertension, pregnancy, hemolytic diseases
• Treatment with non-steroidal, antibiotics
18
• NS1-Ag +ve: Early Intravenous fluid therapy
• Treating the diagnosis vs treating the patient
Malarial parasite positive => antimalarial treatment

16 year old girl, Day 3 of fever
Presented to Primary Care with high fever, 39oC.Headache, myalgia for 2½ days.Poor appetite and reduced fluid intakeDrank ½ glass of milk that morningPassed scanty urineThis morning started to have epigastric pain.
Is the epigastric pain a warning sign?
Yes
No
Not sure
The day before, had poor appetite and reduced oral intake.Drank less than 3 glasses of water
Saw a GP, who suspected she might have dengue, because neighbourhood fogging last week, asked to return for blood test next day.
What other questions would you ask?
19

Medications cause “warning signs”
Erythromycin, Mefenemic acid Erythromycin, Sodium Diclofenac
20

21

Day 116 Feb
Fever onset Fever, MyalgiaHeadacheDecreased oral intake
Temp 39.2oCGood perfusion
Encourage oral fluid
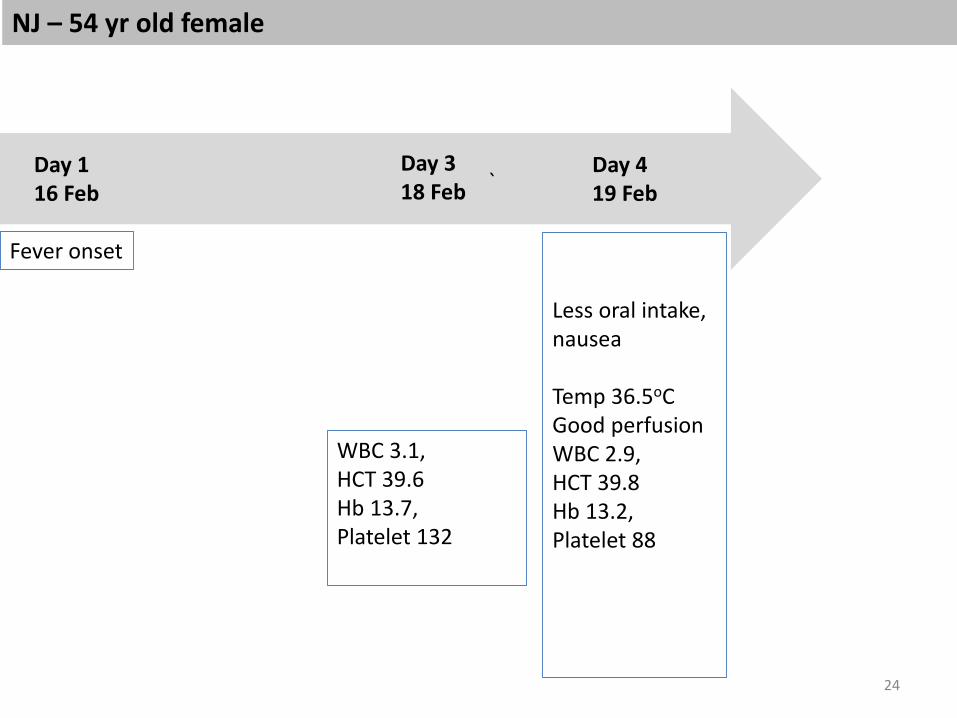
NJ – 54 yr old female
22
Day 217 Feb

Day 318 Feb
NJ – 54 yr old female
23
Dizziness,HeadacheDecreased oral intake
Temp 37.9oCGood perfusionWBC 3.1,HCT 39.6 Hb 13.7, Platelet 132
Encourage oral fluid
`
Fever onset
Less oral intake, nausea
Temp 36.5oCGood perfusionWBC 2.9, HCT 39.8 Hb 13.2,Platelet 88
Encourage oral fluid
NJ – 54 yr old female
24
Day 419 Feb
Day 116 Feb
WBC 3.1,HCT 39.6 Hb 13.7, Platelet 132
Day 318 Feb

Timeline: Trajectory
Day 1 Day 2 Day 3 Day 416 Feb 17 Feb 18 Feb 19 Feb
Fever onset Fever, MyalgiaHeadacheDecreased oral intake
Temp 39.2oCGood perfusion
Encourage oral fluid
Dizziness,HeadacheDecreased oral intake
Temp 37.9oCGood perfusionWBC 3.1,HCT 39.6 Hb 13.7, Platelet 132
Encourage oral fluid
Less oral intake, nausea
Temp 36.5oCGood perfusionWBC 2.9, HCT 39.8 Hb 13.2,Platelet 88
Encourage oral fluid
NJ – 54 yr old female
25

Timeline: Trajectory
Day 1 Day 2 Day 3 Day 416 Feb 17 Feb 18 Feb 19 Feb
Fever onset Fever, MyalgiaHeadacheDecreased oral intake
Temp 39.2oCGood perfusion
Encourage oral fluid
Dizziness,HeadacheDecreased oral intake
Temp 37.9oCGood perfusionWBC 3.1,HCT 39.6 Hb 13.7, Platelet 132
Encourage oral fluid
Less oral intake, nausea
Temp 36.5oCGood perfusionWBC 2.9, HCT 39.8 Hb 13.2,Platelet 88
Encourage oral fluid
Dizziness,
not eaten anything for past 3 days.Temp 36.7oCPoor perfusionWBC 2.6, HCT 46.2,Hb 15.2,
Platelet 56
Dengue shock syndrome
NJ – 54 yr old female
26
Day 520 Feb

Back to Basics:
History taking: Impact of disease on food and fluid intake
27
The 3 Golden Questions:
1. Drinking – volume, type
2. Pass Urine – frequency
3. Activities

28

42 years old, female, 60 kg; 22 Dec, Fever onset 19 Dec
Fever 3 days, associated with nausea, abdominal pain, body aches
PE
Temp: 38oC
BP: 120/70 mmHg
PULSE: 78 /min
Throat: mildly injected
Lungs clear
CVS: Normal
Abdomen: soft,
increased bowel sounds
INVESTIGATION: FULL BLOOD COUNT
Hb: 13.5 g/dl (11.5-16.5)
HCT: 44.1% (35-55)
RBC: 6.03 x106/mm (3.5-5.5)
MCV: 72 mm (75-100)
MCH: 22 pg (25-35)
MCHC: 29.0 (31-38)
PLATELET: 40 x103/mm (150-400)
WBC: 5.8 x103/mm (3.5-11)
IMPRESSION: VIRAL FEVER TRO DENGUE FEVER
MANAGEMENT: REFER TO HOSPITAL
What other questions would you ask?
What is the diagnosis based on FBC? Guess her baseline HCT?
What is the implication?
Been to GP on 20 Dec, Diclofenac x2days
29
16:30 @ the GP

Back to Basics: The Physical Examination
30

Pearls in clinical examination of dengue patients
The “5-in-1 maneuver” magic touch – CCTV-R
Hold the patient’s hand to evaluate peripheral perfusion.
1.
Colour
2.
Capillary refill
3.
Temperature
4.
Pulse Volume
5.
Pulse Rate
Save life in 30 seconds by recognizing shock

Percussion technique: pleural effusion
32“Fluid finds its own level”: Place percussed finger parallel to fluid level, starting from anterior to mid-axillary and then posterior axillary lines.

Back to Basics: Fluid & Electrolyte therapy
• Oral & IV fluid therapy
• Resuscitation – intravenous therapy
• Rehydration – oral + intravenous
• Maintenance – oral + intravenous
• Not one size fits all!
• See patients not only in real time, but work out the illness trajectory
33


Crowd along veranda of Kukum Clinic, Solomon Islands
35

Coconut – natural rehydrating fluid

Increasing awareness of oral hydration
Encourage drinking aliquots of 50 ml or less in patients with nausea
37

Empowering parents to document intake & output chart
Mother’s documentation of her child’s oral intake, type of drinks, urine frequency
38

After training in Dengue clinical management
Doctor’s entry:Oral fluid intake, urine outputCCTVR
Actions:Stop IVFEncourage oral fluids – coconut water
39

40
After training:
Nurse entry at Dengue Desk Triage counter in NRH:
Date of onset of fever, Risk factors, 3 golden questions, CCTVR

Summary
Biggest dengue epidemic in Malaysia
A lot of resources have been channeled; no sign of slowing down
Training in WHO Dengue case management:Back to Basics in clinical practiceLow-tech, high touch approach
Gate-keeping at frontlineTriage in limited resources
The most important prognostic factor for severe dengue is aTRAINED and WELL REHEARSED MEDICAL AND NURSING TEAM

危機
是有危險又有機會的時刻
42
Dengue Crisis

Year 2003 (n=352)
(Pre-intervention)
2005 + 2006 (n=1943)
(Post-intervention)
P value
CLINICAL PARAMETERS
Available data on any haemorrhage 349 (99.1) 1931 (99.4) 0.875
Presence of any haemorrhage 202 (57.4) 1111 (57.2) 0.875
GI Bleed 16 (4.6) 112 (5.8) 0.523
Available data on plasma leakage 126 (35.8) 1393 (71.7) <0.001
Presence of plasma leakage 40 (11.4) 650 (34.4) <0.001
Available data on peripheral perfusion 46 (13.1) 537 (27.6) <0.001
Presence of hypoperfusion 40 (11.4) 457 (23.5) <0.001
Hypotension or narrowed pulse pr 75 (21.5) 190 (9.8) <0.001
Ratio of hypoperfusion to hypotension 0.53 2.41
LABORATORY PARAMETERS
Highest HCT before IVF (%) 43 (40 – 47) 45.7 (42-49) <0.001
Highest HCT throughout admission (%) 44 (41-48.75) 46.0 (42-50) 0.001
Lowest WBC (x109/L) 2.8 (2.0-3.9) 2.7 (1.9-3.7) 0.183
Lowest platelet count (x109/L) 31 (18-53) 30 (16-47) 0.672
TREATMENT
Days on IVF 3 (2-4) 2.5 (2-3.0) <0.001
Platelet transfusion 75 (21.7) 174 (9.0) <0.001
Plasma transfusion 21 (6.1) 50 (2.6) 0.003
Blood transfusion 6 (1.7) 21 (1.1) 0.555
Use of antibiotics 44 (12.5) 180 (9.3) 0.046
OUTCOME
LOS (days) 4 (3.0-5.0) 3 (3.0-4.0) <0.001
Intensive Care Unit Admission 20 (5.8) 49 (2.5) 0.002 43

Thank you for your Attention!
44