the needs of hearing impaired children's parents who attend to auditory verbal...
TRANSCRIPT
The needs of hearing impaired children’s parentswho attend to auditory verbal therapy-counselingprogram
Esra Yucel a,*, Deray Derim b, Demet Celik c
International Journal of Pediatric Otorhinolaryngology (2008) 72, 1097—1111
www.elsevier.com/locate/ijporl
aDepartment of Otorhinolaryngology, Hacettepe University, Audiology and Speech Pathology Section,Ankara, TurkeybDepartment of Otorhinolaryngology, Lefkosa Dr. Burhan Nalbantoglu Hospital, CypruscDepartment of Otorhinolaryngology, Gulhane Military Medical Academy Hospital, Ankara, Turkey
Received 13 November 2007; received in revised form 26 March 2008; accepted 27 March 2008Available online 12 May 2008
KEYWORDSHearing impaired;Children;Parents;Needs
Summary
Objective: Exploring the information and support needs of parents with hearingimpairment in habilitation process. The effects of variables such as duration ofhearing aid use and habilitation (duration of intervention) and the number of hearingimpaired individuals in family are also considered during the evaluation.Methods: Sixty-five parents of children between 24 and 348 months of age (median:80) participated in this study by returning the completed in The Family Needs Survey.Age at diagnosis of deafness varied from 1 to 84 months of age (median: 16). Theduration of hearing aid use was 8—252 months (median: 24) and the duration ofintervention was 2—176 months (median: 36). In view of the fact that the familydynamics might have effects on the type and amount of the needs of parents, thenumber of siblings (none, two or more siblings) and the presence of hearing impairedindividuals apart from their child was also explored.Results: The parental needs with regard to different topics such as general informa-tion, hearing loss, communication–—services and educational resources, family andsocial support, childcare and community services, financial were evaluated sepa-rately. The needs of parents participating in a multi-dimensional Auditory—Verbalintervention program differed by their preferential demands. The duration of inter-vention was found significantly correlated with the amount of information needsrelated with other conditions their children may have, explaining their children’shearing problem to others, locating good baby-sitters and day-care programs for theirchildren and transportation ( p � 0.05). It was also found that the long-termedcontinuing intervention generates additional psychotherapeutic, social and financial
* Corresponding author. Tel.: +90 312 305 10 68.E-mail address: [email protected] (E. Yucel).
0165-5876/$ — see front matter # 2008 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijporl.2008.03.020

1098 E. Yucel et al.
needs for the parents. No significant correlation was found between hearing impairedindividuals existence with the type and amount of family needs ( p > 0.05).Conclusion: These findings support the positive effect of persistent and long-termAuditory—Verbal therapy and Counseling approach which incorporates parents asinalienable members in all rehabilitation process. Creating an adequate and appro-priate educational environment by considering individualized needs and familydynamics in a long term and persistent Auditory—Verbal therapy and Counselingapproach are all equally important. In addition to a team approach to management,with parents taking a major role in the habilitation process, and all these will lead to amuch better outcome.# 2008 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Parents of hearing impaired children usually feelswamped and unqualified managing their child’srehabilitative process in a beneficial manner. Thisanxiety in their own abilities is often exhibited asaffliction. Several researchers have described thebenefits of early diagnosis and intervention of hear-ing loss in early childhood [1,2]. This is usually interms of speech and language development. Theheightened interest on identification and noticeabledevelopment of speech and language has at timesovershadowed the partnership of parents and familyin the rehabilitation process of the deaf and hard ofhearing child. There is little research evidence as tothe role that parents actually play in support of theirchild’s development. However, all researcherswould agree that the role of the parent is critical.The level of parental involvement, quality, quantityand timing of care services children receive is essen-tial to their psychosocial and academic develop-ment and ultimately the quality of life theyachieve [3,4].
Omondi et al. [5] has presented the results ofparental awareness of hearing impairment in theirschool-going children and healthcare seeking beha-vior. His findings indicate the prospective prime roleof parents in surveillance and management of child-hood hearing impairment. Also, he suggested that afamily-centered and inclusive approach to bothassessment and habilitation process of children withhearing impairment (with or without co-disabilities)is a practical strategy to harness resources withinthe family and formal care settings. In order toestablish an efficient parent and family contributionin the habilitation process, principally the level andthe content of their acquaintance with their needsand their role in the development of their hearingimpaired child should be explored. Besides, there isalso an existing belief that balancing the desires ofparents and the opinions of professionals may be oneof the most difficult challenges facing those in re-habilitation as parents may demand more account-
ability and individuality to obtain services that morespecifically address their desires as they acquiregreater knowledge and interest in their children’seducation [6]. However, the power and impact ofcollaboration by a team of specialists which includesparents as equal partners cannot be overestimated.It also seems important to us to examine the parentsof children with hearing impairment with regard topossible specific peculiarities, as in clinical practiceparents and their respective requirements will beconfronting the specialist in the field of rehabilita-tive audiology as well as all the other professionalgroups participating in the habilitation process.
The parents of a normal child have the respon-sibility to meet the needs of their child and preparean appropriate environment for their child’s healthygrowth and development. The parent of a disabledchild, however, in addition to these responsibilities,is also burdened with additional responsibilities,such as teaching the skills and practicing the habi-litation programs. For this reason the parents ofdisabled children requires additional needs [7,8].The aim of this study is to explore the informationand support needs of parents need when dealingwith hearing impairment in their habilitation pro-cess. The effects of variables such as duration ofhearing aid use, habilitation (duration of interven-tion) and the number of hearing impaired individualsin family are also considered during the evaluation.
2. Materials and methods
2.1. Subjects
Sixty-five parents with low or middle socio-economicstatus were drawn at random among whom joined inthe parent—child counseling run by the HacettepeUniversity Auditory—Verbal therapy and CounselingProgram in Turkey. This Program is dedicated tomaximizing the success of every child who receiveseither hearing aid or cochlear implant. The programprovides numerous services for patients and for the
The needs of hearing impaired children’s parents 1099
therapeutic and educational programs that servehard of hearing or deafened children. It also offerscounseling sessions dedicated to the parents of newlydiagnosed children with hearing loss. These includean explanation of communication choices, provisionof local and national informational resources, andconsultation to address concerns and questionsregarding communication development in childrenwith hearing aids or cochlear implants. Educationalaudiologists provide pre-implant/pre-hearing aidevaluation of current speech, language and auditoryskills. They also serve as a resource, by providingconsultation, evaluation, and in-service presenta-tions, to educational and therapeutic programswhich request assistance in the provision of appro-priate rehabilitation services to children in theircare. Children cannot develop a functional commu-nication system, if the only intervention they receiveis in a therapy room, therefore specific speech,language and auditory goals should be targeted dailyin the child’s home environment. In the HacettepeProgramparents andcaregivers areexpected tobeanactive participant in the child’s rehabilitation. Chil-dren’s primary caregivers arepresumed tobe thefirstand most important teacher’s of the child’s life.Therefore, parent training primarily takes part inthe program. Professionals involved with a child inthe aural rehabilitation program also create a systemwhich allows for consistency and coordination ofservices. We work hard to develop and maintain astrong working relationship with the therapeutic andeducational professionals, who work with ourpatients. Our program provides consultation ser-vices, as well as in-service trainings, for private
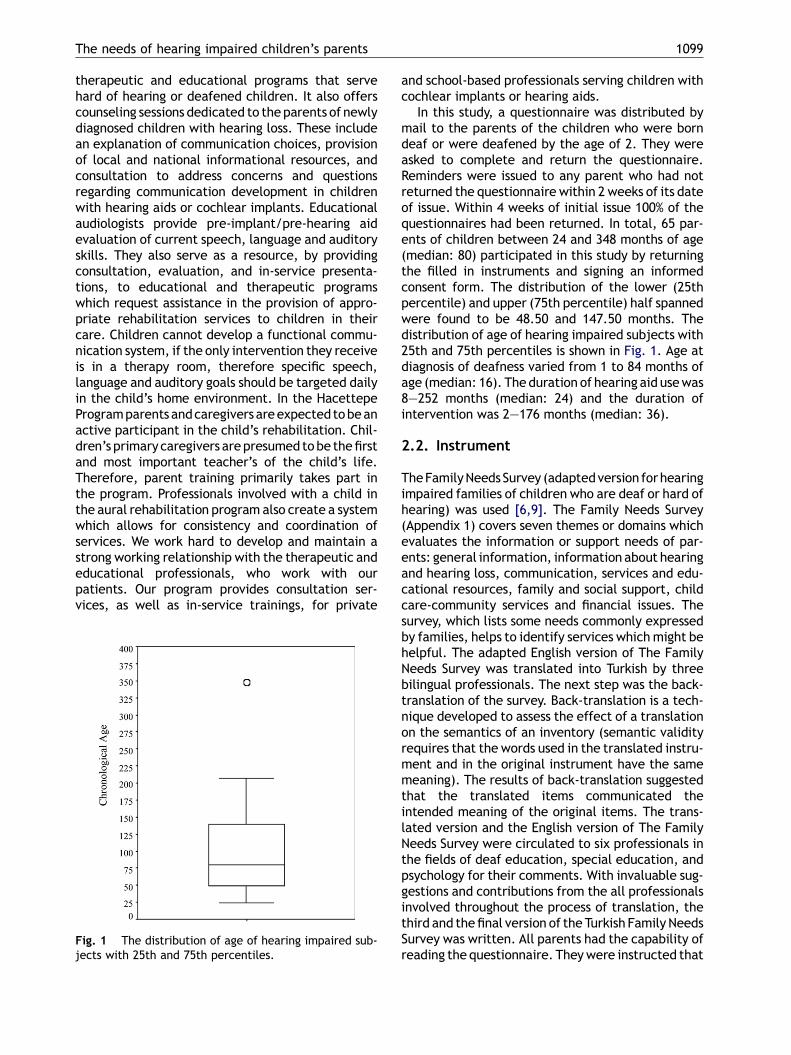
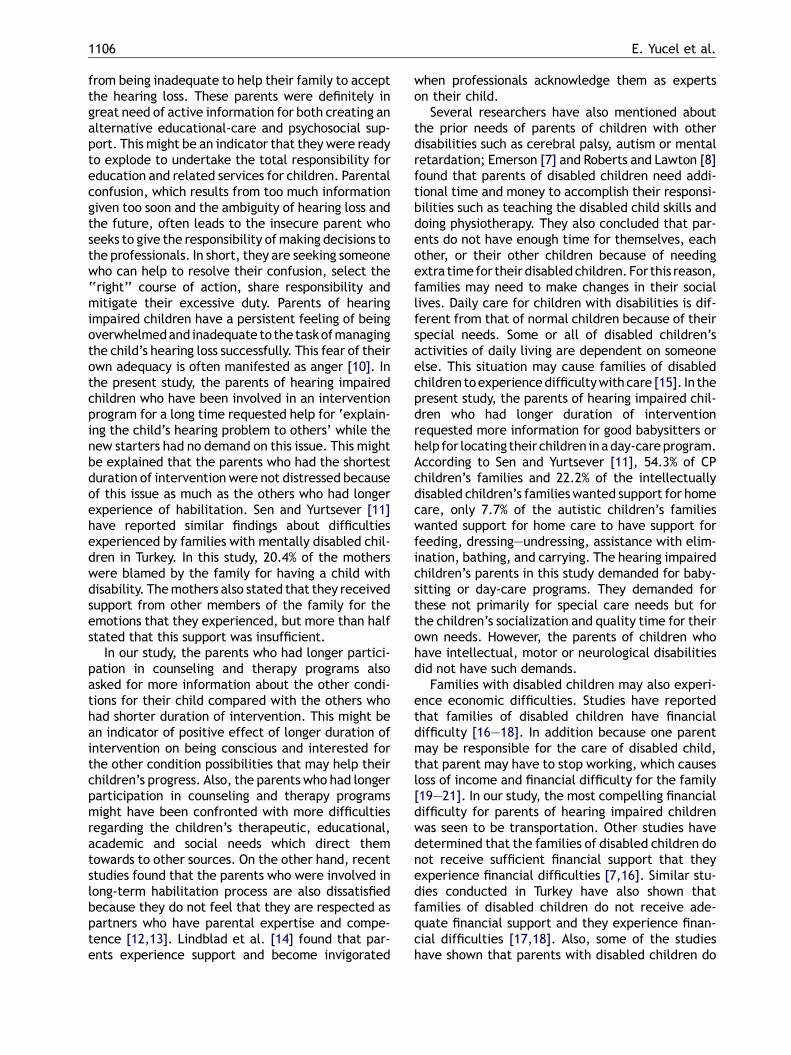
Fig. 1 The distribution of age of hearing impaired sub-jects with 25th and 75th percentiles.
and school-based professionals serving children withcochlear implants or hearing aids.
In this study, a questionnaire was distributed bymail to the parents of the children who were borndeaf or were deafened by the age of 2. They wereasked to complete and return the questionnaire.Reminders were issued to any parent who had notreturned the questionnaire within 2 weeks of its dateof issue. Within 4 weeks of initial issue 100% of thequestionnaires had been returned. In total, 65 par-ents of children between 24 and 348 months of age(median: 80) participated in this study by returningthe filled in instruments and signing an informedconsent form. The distribution of the lower (25thpercentile) and upper (75th percentile) half spannedwere found to be 48.50 and 147.50 months. Thedistribution of age of hearing impaired subjects with25th and 75th percentiles is shown in Fig. 1. Age atdiagnosis of deafness varied from 1 to 84 months ofage (median: 16). Theduration of hearing aid usewas8—252 months (median: 24) and the duration ofintervention was 2—176 months (median: 36).
2.2. Instrument
TheFamilyNeeds Survey (adaptedversion forhearingimpaired families of children who are deaf or hard ofhearing) was used [6,9]. The Family Needs Survey(Appendix 1) covers seven themes or domains whichevaluates the information or support needs of par-ents: general information, information about hearingand hearing loss, communication, services and edu-cational resources, family and social support, childcare-community services and financial issues. Thesurvey, which lists some needs commonly expressedby families, helps to identify services whichmight behelpful. The adapted English version of The FamilyNeeds Survey was translated into Turkish by threebilingual professionals. The next step was the back-translation of the survey. Back-translation is a tech-nique developed to assess the effect of a translationon the semantics of an inventory (semantic validityrequires that the words used in the translated instru-ment and in the original instrument have the samemeaning). The results of back-translation suggestedthat the translated items communicated theintended meaning of the original items. The trans-lated version and the English version of The FamilyNeeds Survey were circulated to six professionals inthe fields of deaf education, special education, andpsychology for their comments. With invaluable sug-gestions and contributions from the all professionalsinvolved throughout the process of translation, thethird and thefinal version of the Turkish Family NeedsSurvey was written. All parents had the capability ofreading the questionnaire. Theywere instructed that

1100 E. Yucel et al.
it would be helpful if they would check the topics forwhich they would like more information or to discusswith amemberof staff from theprogram.Therewerefour choices (no, not sure, yes-discuss, yes-info) fromwhich they were expected to choose themost appro-priate answer in each statement. If they had suffi-cient understanding of the information they havealready had they were asked to mark ‘no’. However,if they were not sure either about the level or if theywanted any further information, they were asked tochoose ‘not-sure’. If they believed that they hadsome information andwanted to discuss it, theyweresupposed to choose ‘yes-discuss’. If they felt totallyuninformed and curious, they were supposed tochoose ‘yes-info’. Some of the survey statementswere not compatible with the rehabilitation systemin Turkey. Parentswere asked to answer only the 30 of38 statements to see if they would like to get moreinformation or to discuss this topic with a member ofstaff from the counseling program. Because thefamily dynamics might be effective on the typeand amount of the needs of parents, the number ofsiblings (none, twoormore siblings) and thepresenceof hearing impaired individuals were also enquired.
2.3. Statistical analysis
Data was analyzed using SPSS-10 (SPSS Inc., Chi-cago, IL). The statistical significance of differencesbetween more than two-independent groups wasassessed by Kruskal—Wallis one-way analysis of var-iance by ranks and chi-square test for numeric andcategorical data, respectively. Kruskal—Wallis Z-test was used for multiple-comparison. Significancelevel alpha was taken 0.05.
3. Results
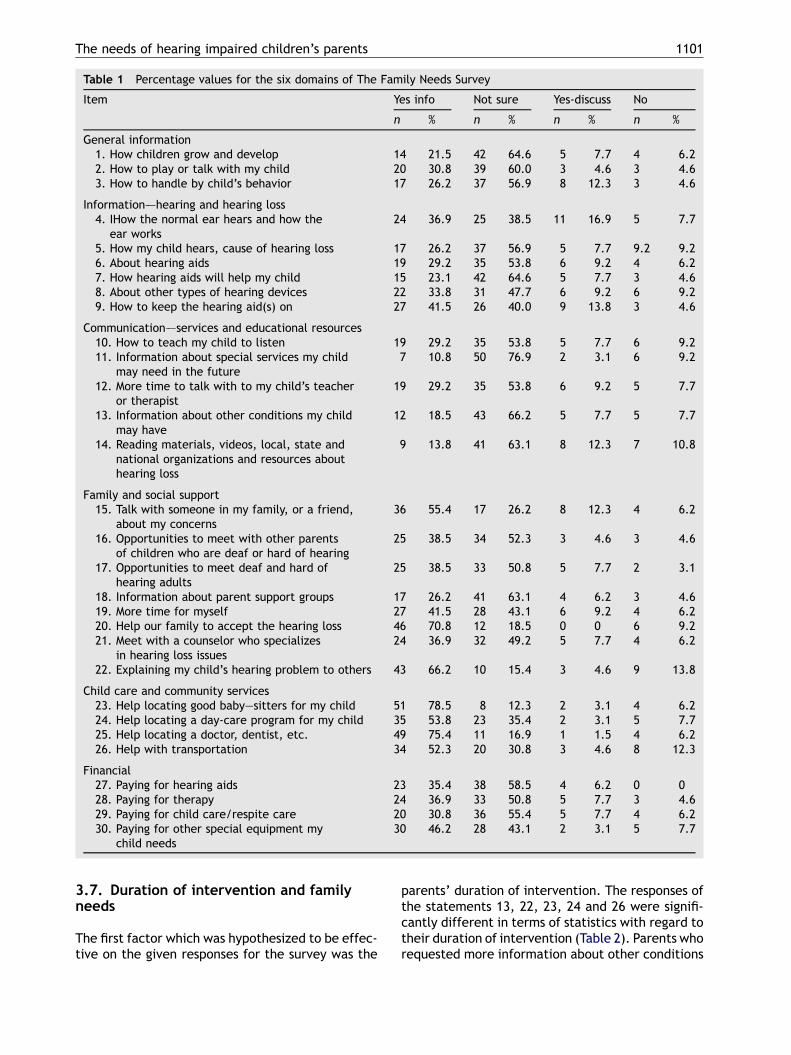
Each question from six domains of The Family Needssurvey was evaluated separately and the results arepresented in Table 1.
3.1. General information
The first part of the survey was based on generalinformation such as the growth and development ofthe child, playing—talking abilities, and the strate-gies to handle the child’s behavior. 21.5% of theparents have requested more information about thegrowth and development of their child. 64% of themstated that they were not sure if their knowledgewas adequate or not. 60% were uncertain about theaccuracy of their playing—talking abilities. 56.9%felt unconfident while they were trying to handlethe child’s behavior. 30.8 and 26.2% felt the need for
information on how to play and talk and handle thebehavior while interacting with their children.
3.2. Information–—hearing and hearingloss
Considering the statements related with hearingand hearing loss 36.9% requested and 38.5% werenot sure of their present knowledge about the func-tion of normal ear and hearing. 53.8% also feltunsure about how their children hear, and the causeof hearing loss and 64.6% felt unsure about thefunction of hearing aids. Most of the parents(47.7%) lacked knowledge of the other types ofhearing devices and 41.5% requested new informa-tion related to ‘how to keep the hearing aid(s) on’.
3.3. Communication–—services andeducational resources
53.8% were unsure if they receive adequate andeffective methods for teaching their children tolisten. 76.9% were unsure about the informationon special services which the child may need infuture. Only 29.2% asked for more time to talk withthe therapist and 66.2% were uncertain aboutwhether to get more information about other con-ditions that the child may have or not. Moreover,63.1% of them indicated that they might get furtherinformation about reading materials, video andseveral types of organizations about hearing loss.
3.4. Family and social support
55.4% of the parents expressed their need to talk tosomeone in the family or to a friend about theirconcerns. 70.8% requested help for their family tohelp them to accept the hearing loss and 66.2% werein need of assistance while explaining their chil-dren’s hearing problem to others.
3.5. Child care and community services
In this section 78% need help locating good baby-sitters or a day-care program (53.8%) for their hear-ing impaired children. 75.4% asked for informationon how to locate a doctor and a dentist. 52.3%demanded support with transportation.
3.6. Financial
Most of the parents were unsure about their presentsituation on how to pay for the hearing aids (58%),for therapy (50.8%) and for child or respite care(55.4%). Whereas, 46% needed help with paying forother special equipment their children needed.
The needs of hearing impaired children’s parents 1101
Table 1 Percentage values for the six domains of The Family Needs Survey
Item Yes info Not sure Yes-discuss No
n % n % n % n %
General information1. How children grow and develop 14 21.5 42 64.6 5 7.7 4 6.22. How to play or talk with my child 20 30.8 39 60.0 3 4.6 3 4.63. How to handle by child’s behavior 17 26.2 37 56.9 8 12.3 3 4.6
Information–—hearing and hearing loss4. IHow the normal ear hears and how the
ear works24 36.9 25 38.5 11 16.9 5 7.7
5. How my child hears, cause of hearing loss 17 26.2 37 56.9 5 7.7 9.2 9.26. About hearing aids 19 29.2 35 53.8 6 9.2 4 6.27. How hearing aids will help my child 15 23.1 42 64.6 5 7.7 3 4.68. About other types of hearing devices 22 33.8 31 47.7 6 9.2 6 9.29. How to keep the hearing aid(s) on 27 41.5 26 40.0 9 13.8 3 4.6
Communication–—services and educational resources10. How to teach my child to listen 19 29.2 35 53.8 5 7.7 6 9.211. Information about special services my child
may need in the future7 10.8 50 76.9 2 3.1 6 9.2
12. More time to talk with to my child’s teacheror therapist
19 29.2 35 53.8 6 9.2 5 7.7
13. Information about other conditions my childmay have
12 18.5 43 66.2 5 7.7 5 7.7
14. Reading materials, videos, local, state andnational organizations and resources abouthearing loss
9 13.8 41 63.1 8 12.3 7 10.8
Family and social support15. Talk with someone in my family, or a friend,
about my concerns36 55.4 17 26.2 8 12.3 4 6.2
16. Opportunities to meet with other parentsof children who are deaf or hard of hearing
25 38.5 34 52.3 3 4.6 3 4.6
17. Opportunities to meet deaf and hard ofhearing adults
25 38.5 33 50.8 5 7.7 2 3.1
18. Information about parent support groups 17 26.2 41 63.1 4 6.2 3 4.619. More time for myself 27 41.5 28 43.1 6 9.2 4 6.220. Help our family to accept the hearing loss 46 70.8 12 18.5 0 0 6 9.221. Meet with a counselor who specializes
in hearing loss issues24 36.9 32 49.2 5 7.7 4 6.2
22. Explaining my child’s hearing problem to others 43 66.2 10 15.4 3 4.6 9 13.8
Child care and community services23. Help locating good baby—sitters for my child 51 78.5 8 12.3 2 3.1 4 6.224. Help locating a day-care program for my child 35 53.8 23 35.4 2 3.1 5 7.725. Help locating a doctor, dentist, etc. 49 75.4 11 16.9 1 1.5 4 6.226. Help with transportation 34 52.3 20 30.8 3 4.6 8 12.3
Financial27. Paying for hearing aids 23 35.4 38 58.5 4 6.2 0 028. Paying for therapy 24 36.9 33 50.8 5 7.7 3 4.629. Paying for child care/respite care 20 30.8 36 55.4 5 7.7 4 6.230. Paying for other special equipment my
child needs30 46.2 28 43.1 2 3.1 5 7.7
3.7. Duration of intervention and familyneeds
The first factor which was hypothesized to be effec-tive on the given responses for the survey was the
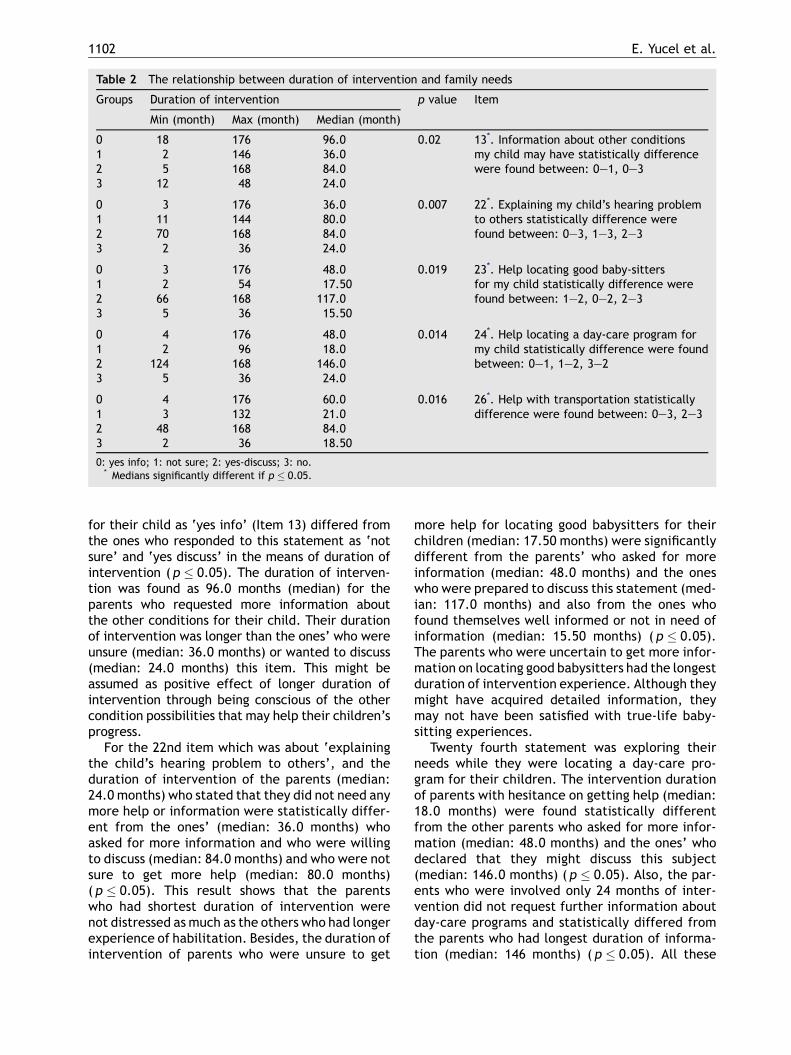
parents’ duration of intervention. The responses ofthe statements 13, 22, 23, 24 and 26 were signifi-cantly different in terms of statistics with regard totheir duration of intervention (Table 2). Parents whorequested more information about other conditions
1102 E. Yucel et al.
Table 2 The relationship between duration of intervention and family needs
Groups Duration of intervention p value Item
Min (month) Max (month) Median (month)
0 18 176 96.0 0.02 13*. Information about other conditionsmy child may have statistically differencewere found between: 0—1, 0—3
1 2 146 36.02 5 168 84.03 12 48 24.0
0 3 176 36.0 0.007 22*. Explaining my child’s hearing problemto others statistically difference werefound between: 0—3, 1—3, 2—3
1 11 144 80.02 70 168 84.03 2 36 24.0
0 3 176 48.0 0.019 23*. Help locating good baby-sittersfor my child statistically difference werefound between: 1—2, 0—2, 2—3
1 2 54 17.502 66 168 117.03 5 36 15.50
0 4 176 48.0 0.014 24*. Help locating a day-care program formy child statistically difference were foundbetween: 0—1, 1—2, 3—2
1 2 96 18.02 124 168 146.03 5 36 24.0
0 4 176 60.0 0.016 26*. Help with transportation statisticallydifference were found between: 0—3, 2—31 3 132 21.0
2 48 168 84.03 2 36 18.50
0: yes info; 1: not sure; 2: yes-discuss; 3: no.* Medians significantly different if p � 0.05.
for their child as ‘yes info’ (Item 13) differed fromthe ones who responded to this statement as ‘notsure’ and ‘yes discuss’ in the means of duration ofintervention (p � 0.05). The duration of interven-tion was found as 96.0 months (median) for theparents who requested more information aboutthe other conditions for their child. Their durationof intervention was longer than the ones’ who wereunsure (median: 36.0 months) or wanted to discuss(median: 24.0 months) this item. This might beassumed as positive effect of longer duration ofintervention through being conscious of the othercondition possibilities that may help their children’sprogress.
For the 22nd item which was about ‘explainingthe child’s hearing problem to others’, and theduration of intervention of the parents (median:24.0 months) who stated that they did not need anymore help or information were statistically differ-ent from the ones’ (median: 36.0 months) whoasked for more information and who were willingto discuss (median: 84.0 months) and who were notsure to get more help (median: 80.0 months)( p � 0.05). This result shows that the parentswho had shortest duration of intervention werenot distressed as much as the others who had longerexperience of habilitation. Besides, the duration ofintervention of parents who were unsure to get
more help for locating good babysitters for theirchildren (median: 17.50 months) were significantlydifferent from the parents’ who asked for moreinformation (median: 48.0 months) and the oneswho were prepared to discuss this statement (med-ian: 117.0 months) and also from the ones whofound themselves well informed or not in need ofinformation (median: 15.50 months) ( p � 0.05).The parents who were uncertain to get more infor-mation on locating good babysitters had the longestduration of intervention experience. Although theymight have acquired detailed information, theymay not have been satisfied with true-life baby-sitting experiences.
Twenty fourth statement was exploring theirneeds while they were locating a day-care pro-gram for their children. The intervention durationof parents with hesitance on getting help (median:18.0 months) were found statistically differentfrom the other parents who asked for more infor-mation (median: 48.0 months) and the ones’ whodeclared that they might discuss this subject(median: 146.0 months) ( p � 0.05). Also, the par-ents who were involved only 24 months of inter-vention did not request further information aboutday-care programs and statistically differed fromthe parents who had longest duration of informa-tion (median: 146 months) ( p � 0.05). All these
The needs of hearing impaired children’s parents 1103
findings support that the increment of interven-tion duration brings out the necessity to share theresponsibilities of child’s day care. Besides, theduration of intervention of the families whofound themselves well informed (median: 18.50months) about the transportation issues was sig-nificantly different from the ones who requiredmore information (median: 60.0 months) andthe ones who want to discuss this item (median:84.0 months) ( p � 0.05). These results alsoshow that the increment of duration of interven-tion causes financial difficulties especially fortransportation to reach the rehabilitation servicesfrequently.
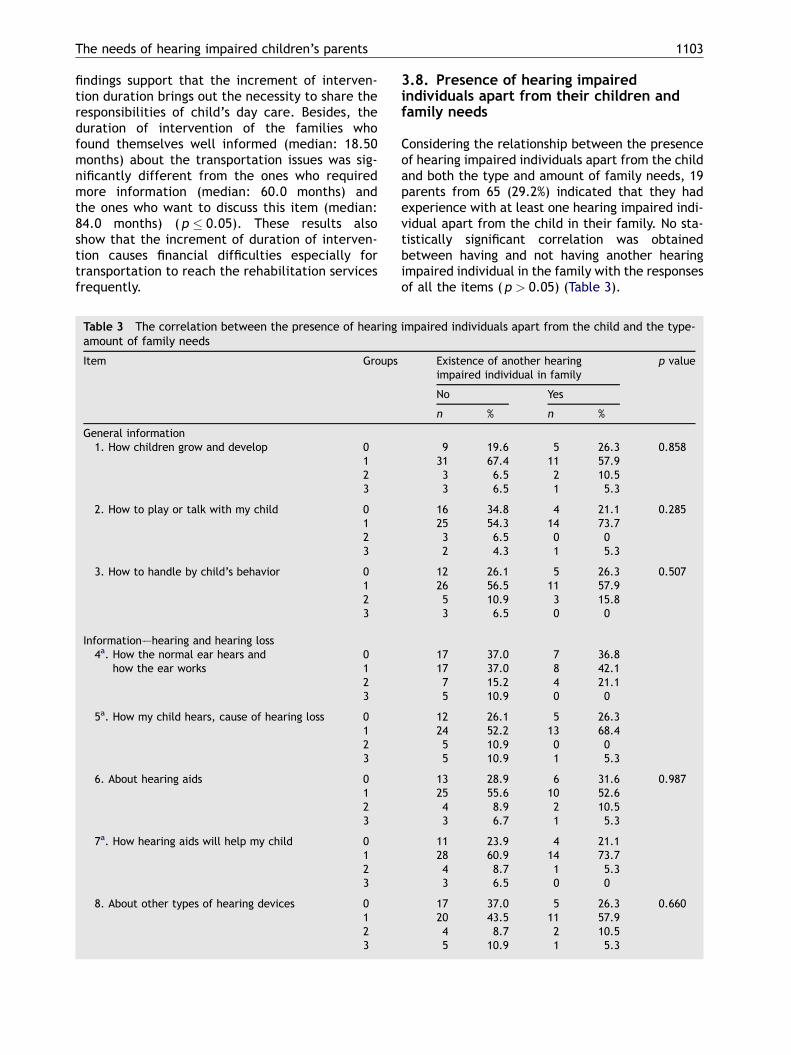
Table 3 The correlation between the presence of hearingamount of family needs
Item Groups
General information1. How children grow and develop 0
123
2. How to play or talk with my child 0123
3. How to handle by child’s behavior 0123
Information–—hearing and hearing loss4a. How the normal ear hears and
how the ear works0123
5a. How my child hears, cause of hearing loss 0123
6. About hearing aids 0123
7a. How hearing aids will help my child 0123
8. About other types of hearing devices 0123
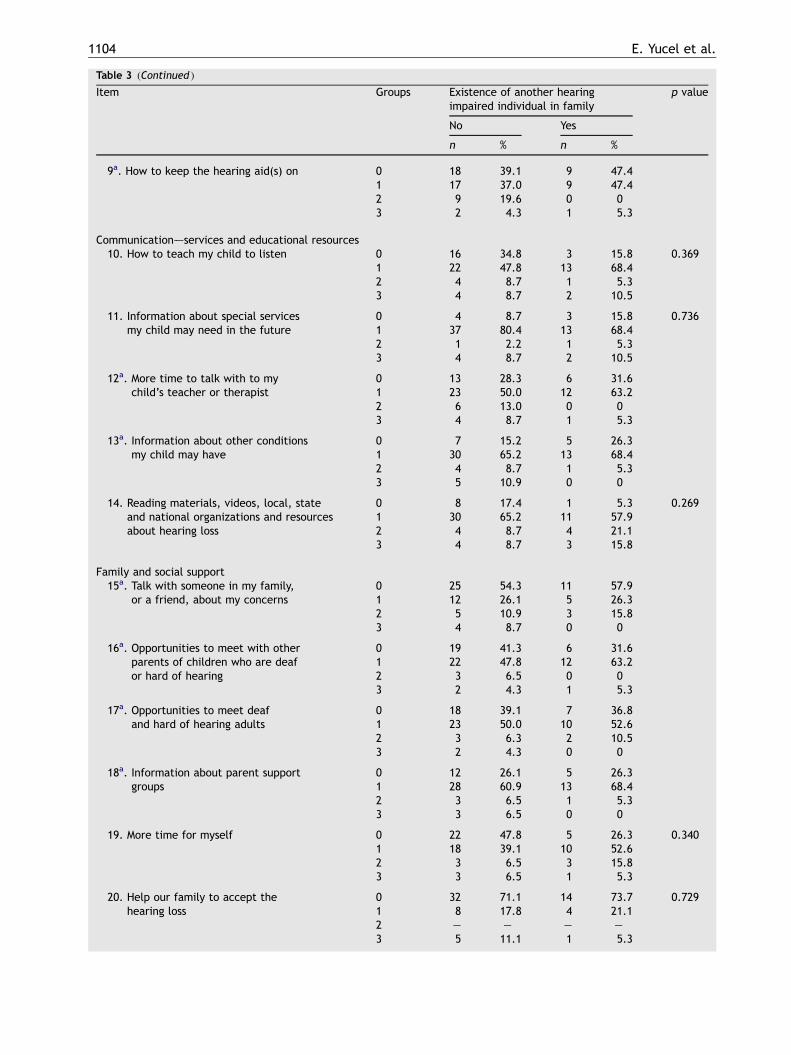
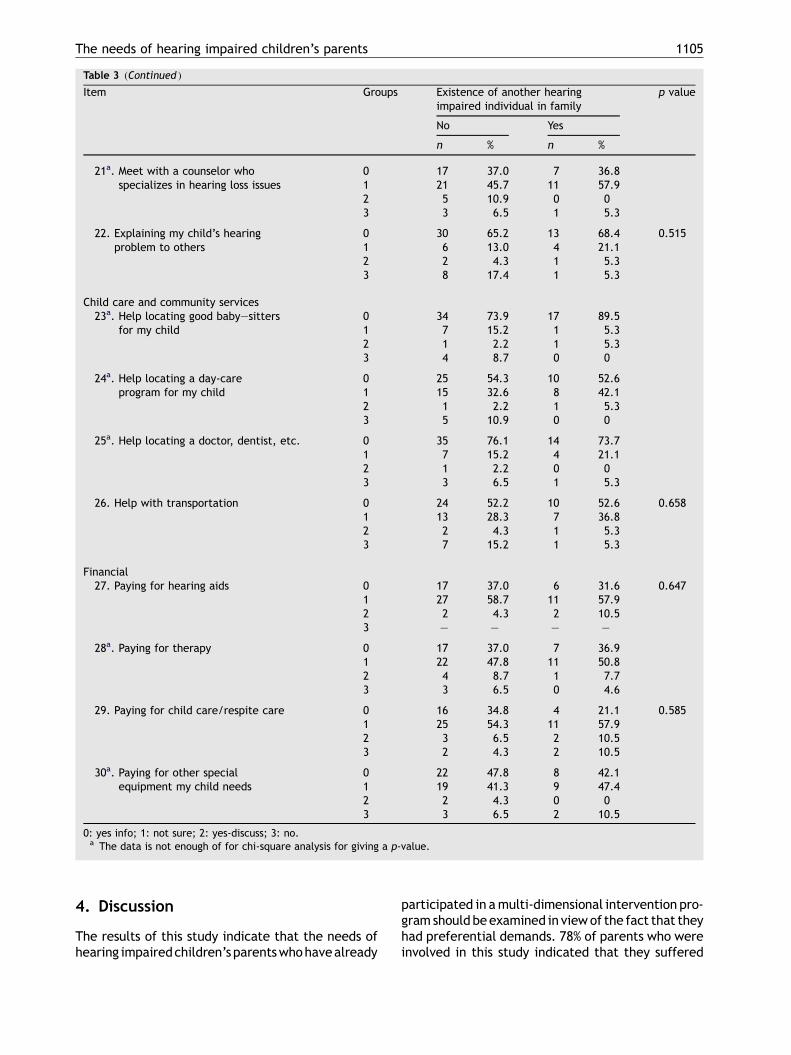
3.8. Presence of hearing impairedindividuals apart from their children andfamily needs
Considering the relationship between the presenceof hearing impaired individuals apart from the childand both the type and amount of family needs, 19parents from 65 (29.2%) indicated that they hadexperience with at least one hearing impaired indi-vidual apart from the child in their family. No sta-tistically significant correlation was obtainedbetween having and not having another hearingimpaired individual in the family with the responsesof all the items ( p > 0.05) (Table 3).
impaired individuals apart from the child and the type-
Existence of another hearingimpaired individual in family
p value
No Yes
n % n %
9 19.6 5 26.3 0.85831 67.4 11 57.93 6.5 2 10.53 6.5 1 5.3
16 34.8 4 21.1 0.28525 54.3 14 73.73 6.5 0 02 4.3 1 5.3
12 26.1 5 26.3 0.50726 56.5 11 57.95 10.9 3 15.83 6.5 0 0
17 37.0 7 36.817 37.0 8 42.17 15.2 4 21.15 10.9 0 0
12 26.1 5 26.324 52.2 13 68.45 10.9 0 05 10.9 1 5.3
13 28.9 6 31.6 0.98725 55.6 10 52.64 8.9 2 10.53 6.7 1 5.3
11 23.9 4 21.128 60.9 14 73.74 8.7 1 5.33 6.5 0 0
17 37.0 5 26.3 0.66020 43.5 11 57.94 8.7 2 10.55 10.9 1 5.3
1104 E. Yucel et al.
Table 3 (Continued )
Item Groups Existence of another hearingimpaired individual in family
p value
No Yes
n % n %
9a. How to keep the hearing aid(s) on 0 18 39.1 9 47.41 17 37.0 9 47.42 9 19.6 0 03 2 4.3 1 5.3
Communication–—services and educational resources10. How to teach my child to listen 0 16 34.8 3 15.8 0.369
1 22 47.8 13 68.42 4 8.7 1 5.33 4 8.7 2 10.5
11. Information about special servicesmy child may need in the future
0 4 8.7 3 15.8 0.7361 37 80.4 13 68.42 1 2.2 1 5.33 4 8.7 2 10.5
12a. More time to talk with to mychild’s teacher or therapist
0 13 28.3 6 31.61 23 50.0 12 63.22 6 13.0 0 03 4 8.7 1 5.3
13a. Information about other conditionsmy child may have
0 7 15.2 5 26.31 30 65.2 13 68.42 4 8.7 1 5.33 5 10.9 0 0
14. Reading materials, videos, local, stateand national organizations and resourcesabout hearing loss
0 8 17.4 1 5.3 0.2691 30 65.2 11 57.92 4 8.7 4 21.13 4 8.7 3 15.8
Family and social support15a. Talk with someone in my family,
or a friend, about my concerns0 25 54.3 11 57.91 12 26.1 5 26.32 5 10.9 3 15.83 4 8.7 0 0
16a. Opportunities to meet with otherparents of children who are deafor hard of hearing
0 19 41.3 6 31.61 22 47.8 12 63.22 3 6.5 0 03 2 4.3 1 5.3
17a. Opportunities to meet deafand hard of hearing adults
0 18 39.1 7 36.81 23 50.0 10 52.62 3 6.3 2 10.53 2 4.3 0 0
18a. Information about parent supportgroups
0 12 26.1 5 26.31 28 60.9 13 68.42 3 6.5 1 5.33 3 6.5 0 0
19. More time for myself 0 22 47.8 5 26.3 0.3401 18 39.1 10 52.62 3 6.5 3 15.83 3 6.5 1 5.3
20. Help our family to accept thehearing loss
0 32 71.1 14 73.7 0.7291 8 17.8 4 21.12 — — — —3 5 11.1 1 5.3
The needs of hearing impaired children’s parents 1105
Table 3 (Continued )
Item Groups Existence of another hearingimpaired individual in family
p value
No Yes
n % n %
21a. Meet with a counselor whospecializes in hearing loss issues
0 17 37.0 7 36.81 21 45.7 11 57.92 5 10.9 0 03 3 6.5 1 5.3
22. Explaining my child’s hearingproblem to others
0 30 65.2 13 68.4 0.5151 6 13.0 4 21.12 2 4.3 1 5.33 8 17.4 1 5.3
Child care and community services23a. Help locating good baby—sitters
for my child0 34 73.9 17 89.51 7 15.2 1 5.32 1 2.2 1 5.33 4 8.7 0 0
24a. Help locating a day-careprogram for my child
0 25 54.3 10 52.61 15 32.6 8 42.12 1 2.2 1 5.33 5 10.9 0 0
25a. Help locating a doctor, dentist, etc. 0 35 76.1 14 73.71 7 15.2 4 21.12 1 2.2 0 03 3 6.5 1 5.3
26. Help with transportation 0 24 52.2 10 52.6 0.6581 13 28.3 7 36.82 2 4.3 1 5.33 7 15.2 1 5.3
Financial27. Paying for hearing aids 0 17 37.0 6 31.6 0.647
1 27 58.7 11 57.92 2 4.3 2 10.53 — — — —
28a. Paying for therapy 0 17 37.0 7 36.91 22 47.8 11 50.82 4 8.7 1 7.73 3 6.5 0 4.6
29. Paying for child care/respite care 0 16 34.8 4 21.1 0.5851 25 54.3 11 57.92 3 6.5 2 10.53 2 4.3 2 10.5
30a. Paying for other specialequipment my child needs
0 22 47.8 8 42.11 19 41.3 9 47.42 2 4.3 0 03 3 6.5 2 10.5
0: yes info; 1: not sure; 2: yes-discuss; 3: no.a The data is not enough of for chi-square analysis for giving a p-value.
4. Discussion
The results of this study indicate that the needs ofhearing impairedchildren’s parentswhohavealready
participated in amulti-dimensional intervention pro-gram should beexamined in viewof the fact that theyhad preferential demands. 78% of parents who wereinvolved in this study indicated that they suffered
1106 E. Yucel et al.
from being inadequate to help their family to acceptthe hearing loss. These parents were definitely ingreat need of active information for both creating analternative educational-care and psychosocial sup-port. This might be an indicator that theywere readyto explode to undertake the total responsibility foreducation and related services for children. Parentalconfusion, which results from too much informationgiven too soon and the ambiguity of hearing loss andthe future, often leads to the insecure parent whoseeks to give the responsibility ofmaking decisions tothe professionals. In short, they are seeking someonewho can help to resolve their confusion, select the‘‘right’’ course of action, share responsibility andmitigate their excessive duty. Parents of hearingimpaired children have a persistent feeling of beingoverwhelmedand inadequate to the taskofmanagingthe child’s hearing loss successfully. This fear of theirown adequacy is often manifested as anger [10]. Inthe present study, the parents of hearing impairedchildren who have been involved in an interventionprogram for a long time requested help for ‘explain-ing the child’s hearing problem to others’ while thenew starters had no demand on this issue. This mightbe explained that the parents who had the shortestduration of intervention were not distressed becauseof this issue as much as the others who had longerexperience of habilitation. Sen and Yurtsever [11]have reported similar findings about difficultiesexperienced by families with mentally disabled chil-dren in Turkey. In this study, 20.4% of the motherswere blamed by the family for having a child withdisability. Themothers also stated that they receivedsupport from other members of the family for theemotions that they experienced, but more than halfstated that this support was insufficient.
In our study, the parents who had longer partici-pation in counseling and therapy programs alsoasked for more information about the other condi-tions for their child compared with the others whohad shorter duration of intervention. This might bean indicator of positive effect of longer duration ofintervention on being conscious and interested forthe other condition possibilities that may help theirchildren’s progress. Also, the parents who had longerparticipation in counseling and therapy programsmight have been confronted with more difficultiesregarding the children’s therapeutic, educational,academic and social needs which direct themtowards to other sources. On the other hand, recentstudies found that the parents who were involved inlong-term habilitation process are also dissatisfiedbecause they do not feel that they are respected aspartners who have parental expertise and compe-tence [12,13]. Lindblad et al. [14] found that par-ents experience support and become invigorated
when professionals acknowledge them as expertson their child.
Several researchers have also mentioned aboutthe prior needs of parents of children with otherdisabilities such as cerebral palsy, autism or mentalretardation; Emerson [7] and Roberts and Lawton [8]found that parents of disabled children need addi-tional time and money to accomplish their responsi-bilities such as teaching the disabled child skills anddoing physiotherapy. They also concluded that par-ents do not have enough time for themselves, eachother, or their other children because of needingextra time for their disabledchildren. For this reason,families may need to make changes in their sociallives. Daily care for children with disabilities is dif-ferent from that of normal children because of theirspecial needs. Some or all of disabled children’sactivities of daily living are dependent on someoneelse. This situation may cause families of disabledchildren toexperiencedifficultywith care [15]. In thepresent study, the parents of hearing impaired chil-dren who had longer duration of interventionrequested more information for good babysitters orhelp for locating their children inaday-careprogram.According to Sen and Yurtsever [11], 54.3% of CPchildren’s families and 22.2% of the intellectuallydisabled children’s families wanted support for homecare, only 7.7% of the autistic children’s familieswanted support for home care to have support forfeeding, dressing—undressing, assistance with elim-ination, bathing, and carrying. The hearing impairedchildren’s parents in this study demanded for baby-sitting or day-care programs. They demanded forthese not primarily for special care needs but forthe children’s socialization and quality time for theirown needs. However, the parents of children whohave intellectual, motor or neurological disabilitiesdid not have such demands.
Families with disabled children may also experi-ence economic difficulties. Studies have reportedthat families of disabled children have financialdifficulty [16—18]. In addition because one parentmay be responsible for the care of disabled child,that parent may have to stop working, which causesloss of income and financial difficulty for the family[19—21]. In our study, the most compelling financialdifficulty for parents of hearing impaired childrenwas seen to be transportation. Other studies havedetermined that the families of disabled children donot receive sufficient financial support that theyexperience financial difficulties [7,16]. Similar stu-dies conducted in Turkey have also shown thatfamilies of disabled children do not receive ade-quate financial support and they experience finan-cial difficulties [17,18]. Also, some of the studieshave shown that parents with disabled children do

The needs of hearing impaired children’s parents 1107
not receive subsidies because they are unaware ofthe available services or believe that they are noteligible [22,23]. Most of the parents who wereinvolved in the present study also stated that theywere unsure about the present information on pay-ing for the hearing aids (58%), for therapy (50.8%)and for child or respite care (55%). In Turkey, thefamilies who have hearing impaired children usuallydo not have sufficient information on hearing lossand available intervention services. For hearingimpaired children, pediatricians or otorhinolaryn-gologists usually do not provide right guidance andassistance to the families. As a result of theseconditions, the families usually lose their precioustime for identification of the hearing loss, gettingthe appropriate amplification and enrolling to thesuitable intervention for the child. There are alsosome other additional factors which may contributeto the delays for identification and intervention ofhearing loss, such as; the difficulties for reaching thespecialized health services, caused by the regionwhere the families live, and by the socio-economicstatus of the families. The low socio-economic sta-tus and low level of awareness of the families, andthe delays for obtaining a hearing aid device causedby economic limitations are the major factors thatmay contribute to the prolongation of the intervalbetween amplification and intervention. Moreover,the limited number of intervention centers maycause additional difficulties for the enrollment inintervention to the children who had already ampli-fied. These results highlight the need of Turkishinformative sources for early identification, hearingaids-cochlear implants, financial opportunities,intervention or rehabilitation services, schoolsand other educational systems.
The benefits of early diagnosis and intervention inhearing loss in early childhood have been described inthe literature, usually in terms of speech and lan-guagedevelopment. There is little research evidenceas to the role that parents actually play in support oftheir child’s development, although all researcherswould agree that the role of theparent is critical. Thepresence of a child with hearing loss puts significantpressures on the family with hearing parents and canbe a continuous source of potential stress [24,25].Parents’ emotional response and how they cope withthis stress will affect both family adjustment andchild outcomes. Parents who are in emotional crisisbecause of thediagnosis of deafnessmaynot have thepsychological energy to fully connect or communi-cate with their child [26]. While these differencesmay reflect parents’ adaptation to communicatingwith a child with hearing loss, the style of interactionmay be related to the mothers’ level of coping withhearing loss. Feelings of powerlessness and incompe-
tence resulting from a diagnosis of hearing loss maynegatively impact early parent—child interaction[27,28]. The literature also points to the positiveinfluences on child development by parents whocan cope and adjust to the psychological stress pre-cipitated by the diagnosis. Research has indicatedthat competence, achievement, and adjustment inboth preschool and school-age children who are deafand hard of hearing are related to successful familyadjustment [24,29]. Beyond provision with a hearingaid or a cochlear implant, subsequent long-termrehabilitation plays a decisive role for the audio-lingual development of the children involved. Thisconcerns the families of hearing impaired children,particularly their parents.
In this study, the majority of parents (43 from 65,66.2%) were clearly expressed that they were inneed of more information in ‘‘explaining theirchild’s hearing problem to others’’ and (46 from65, 70.8%) ‘‘Helping their family to accept thehearing loss’’. This finding might be reflecting theirincurability of solitariness while they are strugglingfor the hearing impaired child’s social, educationaland communicative needs. Thus, there is great needto provide public and school personnel with infor-mation regarding the special needs of children withhearing impairment in social, educational commu-nication settings. Several steps can be taken byrehabilitation programs to improve the educationalservices their patients receive in educational set-tings. Importantly, rehabilitation center personnelshould provide continuing education to profes-sionals in their region. Target audiences for suchlearning include early interventionists, pediatri-cians, teachers, teachers of the hearing-impaired,students, speech-language pathologists, and audiol-ogists. Auditory—Verbal Therapy program personnelare in a good position to provide such information asthey are the ones who remain most current regard-ing the changing needs of such children. Addition-ally, Auditory—Verbal Therapy Program audiologistsand speech language pathologists should encourageparents to have several aspects of their child’s carewritten into the child’s records. Audiology servicesshould include knowledgeable fitting and trouble-shooting of assistive listening devices, troubleshoot-ing of the speech processor, and maintenance of thehearing aid. Speech and language services shouldinclude therapy aimed at improving the child’s abil-ity to use spoken language as well as a plan tomonitor progress as it relates to other children withcochlear implants as well as to children with normal-hearing. Lastly, it is important for the Auditory—Verbal Therapy Program to communicate regularlywith the child’s school, circle of friends andacquaintances. One way to facilitate communica-

1108 E. Yucel et al.
tion is to encourage school personnel to visit thecenter to observe the child during rehabilitationand evaluation appointments. Additionally, parentsshould be encouraged to videotape the child’s ses-sions and share such documents with school person-nel. Providing information to and communicatingwith the child’s educational setting will enablecochlear implant programs to provide children withthe best possible chance for success with a hearingaid or a cochlear implant [30].
In this study, the duration of intervention wasfound significantly correlated with the amount ofinformation needs related with other conditionstheir children may have, explaining their children’shearing problem to others, locating good baby-sit-ters and day-care programs for their children, andtransportation. Although these findings support thepositive effect of persistent and long-term Audi-tory—Verbal therapy and Counseling approach whichincorporates parents as inalienable members in allrehabilitation it should also be underlined that theincrement of duration of intervention also inducesparents for psychotherapeutically support, finan-cial, day-care and baby-sitting needs in continuinglong-term habilitation process. For this reason, it isalso clearly emphasized that the subsidiary needs ofparents should not be ignored while intensivelydealing with the child’s Auditory—Verbal, commu-nication development. Besides, as it was speculatedin this study that early detection and intervention ofhearing loss might shorten the duration of interven-tion it should also be considered that additionalneeds of parents with hearing impaired childrenwould also reduced. This relation may highlightthe importance of early detection and interventionprograms once more. Also some of the confoundingissues such as the relationship between duration ofintervention and the both the time since diagnosisand age of the child may also play a part in theadditional conditions which becomemore obvious toparents. Further studies considering these issueswill enlighten the additional family needs.
It was also expected that having experience withanother hearing impaired individual in the familyapart from their hearing impaired child would be
related with family needs. However, no significantrelationship was found between hearing impairedindividuals existence with the type and amount offamily needs. This finding might be explained as allindividuals in a family have distinctive function andcourse of existence which might not be exemplaryfor the others. However, it might be also consideredthat the parents were not aware that they mighteffectively use the course of existence of the otherhearing impaired individual whom might be helpfulwhile providing what they needed or desired fortheir children’s rehabilitative process.
5. Conclusion
The results of this study demonstrate a need on thepart of parents of hearing impaired children forpsychosocial support. This framework introducesthe requirement for differentiated, patient andailment oriented treatment concepts. This will benecessary and should be developed according toevidence obtained in close collaboration betweenpediatric audiologists and psychosocial specialists.The targets identified for this study focus on broadersocial and rehabilitative support for hearingimpaired children and their families. They highlightthe need for multi-agency working and illustrate theimportance of parental involvement in planning newservices and suggesting responsive changes to exist-ing provision. There is still work to do, in connectionwith other professionals working on education,social services and health to ensure the best matchbetween parental priorities and services offered.Forming a sufficient and proper educational envir-onment, providing support services such as speechand language therapy are crucial. In addition tothese, considering the needs of individuals andfamily dynamics in a long term and constant Audi-tory—Verbal therapy and Counseling approach areall equally significant. Besides these, a teamapproach to management, with parents’ great helpin the habilitation process is of great importance.Finally, all the items stated above will result in amuch better outcome.
The needs of hearing impaired children’s parents 1109
Appendix A. Family Needs Survey
Topics No Not sure Yes-discuss Yes-info
General information1. How children grow and develop2. How to play or talk with my child3. How to teach my child4. How to handle by child’s behavior
Information–—hearing and hearing loss1. How the normal ear hears and how the ear works2. How my child hears, cause of hearing loss3. About hearing aids4. How hearing aids will help my child5. About other types of hearing devices6. How to keep the hearing aid(s) on
Communication1. How to teach my child to listen2. How will the hearing loss affect my child’s ability
to learn to talk3. How language develops4. About sign language5. How my child will communicate6. How I can communicate with my child
Services and educational resources1. Information about special services available
for my child2. Information about special services my child
may need in the future3. More time to talk with to my child’s teacher
or therapist4. Information about other conditions my child
may have5. Reading materials, videos, local, state and
national organizations and resources abouthearing loss
Family and social support1. Talk with someone in my family, or a friend,
about my concerns2. Opportunities to meet with other parents of
children who are deaf or hard of hearing3. Opportunities to meet deaf and hard of hearing
adults4. Information about parent support groups5. More time for myself

1110 E. Yucel et al.
Appendix A(Continued )Topics No Not sure Yes-discuss Yes-info
6. Help our family to accept the hearing loss7. Meet with a counselor who specializes in hearing
loss issues8. Explaining my child’s hearing problem to others
Child care and community services1. Help locating good baby—sitters for my child2. Help locating a day-care program for my child3. Help locating a doctor, dentist, etc.4. Help with transportation
Financial1. Paying for hearing aids2. Paying for therapy3. Paying for child care/respite care4. Paying for other special equipment my child needs5. Paying for food, housing, medical care, clothing,
or transportation
Please list other topics or information that you feel would be helpful to receive or discuss.
References
[1] K.S. Sirimanna, Management of the hearing impaired infant,Semin. Neonatol. 6 (2001) 511—519.
[2] Y.S. Sininger, K.J. Doyle, J.K. Moore, The case for earlyidentification of hearing loss in children: auditory systemdevelopment, experimental auditory deprivation and devel-opment of speech perception and hearing, Pediatr. Clin.North Am. 46 (1) (1999) 1—14.
[3] P.H. Dworkin, Detection of behavioral, developmental andpsychosocial problems in pediatric care practice, Curr. Opin.Pediatr. 5 (5) (1993) 531—536.
[4] C. Flexer, Facilitating Hearing and Listening in Young Chil-dren, Singular Publishing Group, Inc., San Diego, 1994, pp.1—19.
[5] D. Omondi, C. Ogol, S. Otieno, I. Macharia, Parental aware-ness of hearing impairment in their school-goingchildren and healthcare seeking behavior in Kisumu district,Kenya, Int. J. Pediatr. Otorhinolaryngol. 71 (2007) 415—423.
[6] C.D. Johnson, P.V. Benson, J.B. Seaton, Relationshipwith Families; Educational Audiology Handbook,Singular Publishing Group, Inc., San Diego, 1997 , pp.141—150.
[7] E. Emerson, Mothers of children and adolescents with intel-lectual disability: social and economic situation, mentalhealth status, and the self-assessed social and psychologicalimpact of the child’s difficulties, J. Intellect. Disabil. Res. 47(Pt 4—5) (2003) 385—399.
[8] K. Roberts, D. Lawton, Acknowledging the extra care par-ents give their disabled children, Child: Care, Health Dev. 27(2001) 307.
[9] R.J. Baily, Simeonsson, Family Needs Survey, FPG ChildDevelopment Institute, The University of North Carolina,Chapel Hill, 1990.
[10] W.E. Kurtzer, D. Luterman, Families and children with hear-ing loss: grief and coping, Ment. Retard. Dev. Disabil. Res.Rev. 9 (2003) 232—235.
[11] E. Sen, S. Yurtsever, Difficulties experienced by families withdisabled children, J. Spec. Pediatr. Nurs. 12 (October (4))(2007) 238—252.
[12] K. Balling, M. Mc Cubbin, Hospitalised children with chronicillness: parental care giving needs and valuing parentalexpertise, J. Pediatr. Nurs. 16 (2001) 110—119.
[13] H. Fisher, The needs of parents with chronically sick chil-dren: a literature review, J. Adv. Nurs. 36 (2001) 600—607.
[14] B.M. Lindblad, B.H. Rasmussen, P.O. Sandman, Being invi-gorated in parenthood: parent’s experiences of being sup-ported by professionals when having a disabled child, J.Pediatr. Nurs. 20 (4) (2005) 288—297.
[15] S. Siklos, K.A. Kerns, Assessing the diagnostic experiences ofa small sample of parents of children with autism spectrumdisorders, Res. Dev. Disabil. 28 (1) (2006) 9—22.
[16] K. Christina, S. Patricia, Stress in families of children withdisability: a review of risk and resistance, J. Ment. Health 1(3) (1992) 32—46.
[17] K. Gokcan, Expectations of families with disabled children.Retrieved June 25, 2007, from http://www.sosyalhizmetuz-mani.org/ozurlucocukaileleri.htm, 2002.
[18] A. Mutlu, N. Demir, M. Kerem, A. Livanelioglu, Examinationof problems faced by families with a child with cerebralpalsy, Health Public 13 (2) (2003) 56—59.
[19] H. Cavusoglu, Child Health Nursing, 6th ed., Bizim Com-pany, Ankara, Turkey, 2002.
[20] A.N. Karancı, Living with Difficulties, 1st ed., TurkishPsychologists Society Publications, Ankara, Turkey, 1997.
[21] A. Taanlia, L. Syrjala, J. Kokkoken, M.R. Jarvelin, Coping ofparents with physically or intellectually disabled children,Child: Care, Health Dev. 28 (1) (2002) 73—86.
[22] D. Blau, E. Tekin, The determinants and consequences ofchild care subsidies for single-mother (discussion paper383), Institute for the Social Labor, Bonn Germany, 2001.
[23] A.B. Shlay, M. Weinraub, M. Harmon, H. Tran, Barriers tosubsidies: why low-income families do not use child caresubsidies, Soc. Sci. Res. 33 (2004) 134—157.
[24] P.T. Feher, Stress and coping in families with deaf children, J.Deaf Stud. Deaf Educ. 1 (1996) 155—166.
[25] R. Calderon, M. Greenberg, Stress and coping in hearingmothers of children with hearing loss: factors affectingmother and child adjustment, Am. Ann. Deaf. 144 (1999)7—16.
[26] S.A. Leighi, Parent bonding in clinically depressed deaf andhard-of-hearing adults, J. Deaf. Stud. 4 (1999) 28—35.

The needs of hearing impaired children’s parents 1111
[27] R.H. MacTurk, K.P. Meadow-Orlans, L.S. Koester, Social sup-port; motivation, language, and interaction; a longitudinalstudy ofmothers and deaf infants, Am. Ann. Deaf. 138 (1993)19—25.
[28] B.B. Johnson, M.S. Leher, Concepts Premises in Family SchoolRelationships, Pre College National Mission Programs, Gallau-det University, Washington, DC, 1996.
[29] M.T. Greenberg, Family stress and child competence: theeffects of early intervention for families with deaf infants,Am. Ann. Deaf. 128 (1983) 407—417.
[30] T.A. Zwolan, D.L. Sorkin, Parental perspectives on educa-tional services for children with cochlear implants, Int.Congr. Ser. 1273 (2004) 401—404.
Available online at www.sciencedirect.com