the molecular genetic analysis of diabetic … 2017.pdf · the molecular genetic analysis of...
TRANSCRIPT
THE MOLECULAR GENETIC ANALYSIS OF
DIABETIC FOOT WOUNDS
ERIN E KLEIN, DPM, MSSARAH E HALLER, DPM; BRETT J WAVERLY, DPM;
LOWELL WEIL, DPM; ADAM E FLEISCHER, DPM, MPH
WEIL FOOT & ANKLE INSTITUTE
DES PLAINES, ILLINOIS, USA
DISCLOSURES
Consultant for BESPA
Primary author on three ACFAS granted studies
Nothing related to the current presentation

TENANTS OF GOOD WOUND CARE
Evaluate and manage blood flow to the extremity
Evaluate and manage deep infection (i.e. osteomyelitis)
Offload
Medical management of systemic conditions
CONTROL THE BIOBURDEN OF THE WOUND

BIOFILM – AN INTRODUCTION
What is biofilm?
A thin, slimy film of bacteria that
adheres to a surface.
Can include bacteria, yeast, algae
and mold.
Tooth plaque
Why are we so interested in this?
Community of bacteria
TRADITIONAL CULTURES VS MOLECULAR ANALYSIS
Aim to identify organisms in a wound
Organisms must be ALIVE when they arrive at the lab
Amenable to growth on a plate/agar
May favor the hardiest micro-organisms
16s amplicon sequencing (next gen sequencing)
Organisms can be alive or dead when they arrive at the lab
Can identify ALL organisms in a biofilm or in a wound
PURPOSE
The purpose of this study is to:
Analyze the content of biofilm utilizing 16s amplicon technology
Identify any common factors between wounds
METHODS
Consecutive patients were included
History of diabetes
Foot ulceration that has been present for 4 weeks (or longer) that has
NOT responded standard wound care treatment
Excluded
Any other type of wound (i.e. venous wounds, pressure ulcers, arterial
wounds in patients without diabetes, traumatic wounds, post operative
wounds)
SPECIMEN COLLECTION
Wound debridement Sterile instrumentation
Biofilm sent to the lab
Level 1 Analysis 10 most common organisms
Level 2 Analysis Biofilm compared to an extensive national database
2% threshold to report
Results compiled in data base Included chart review of potentially connected problems

SPECIMEN COLLECTION
Wound debridement Sterile instrumentation
Biofilm sent to the lab
Level 1 Analysis 10 most common organisms
Level 2 Analysis Biofilm compared to an extensive national database
2% threshold to report
Results compiled in data base Included chart review of potentially connected problems

SPECIMEN COLLECTION
Wound debridement Sterile instrumentation
Biofilm sent to the lab
Level 1 Analysis 10 most common organisms
Level 2 Analysis Biofilm compared to an extensive national database
2% threshold to report
Results compiled in data base Included chart review of potentially connected problems

SPECIMEN COLLECTION
Wound debridement Sterile instrumentation
Biofilm sent to the lab
Level 1 Analysis 10 most common organisms
Level 2 Analysis Biofilm compared to an extensive national database
2% threshold to report
Results compiled in data base Included chart review of potentially connected problems
RESULTS
74 wounds in 53 patients
30 males; 23 females
38 left feet; 33 right feet
40 patients with one wound
34 patients with multiple wounds
Average age: 54.6 + 7.9 (range: 33 – 89)
HbA1C – 7.5% + 1.9% (range 5.1 – 12.4%)

RESULTS
Previous amputations – 3 BKA; 2 TMA; 2 partial 1st ray
Charcot – 4 cases all in quiescent stage
Expiration – 3 patients (4 wounds) were deceased at the time of
analysis

RESULTS – SMOKING STATUS
11%
13%
76%
Current Smoker
Former Smoker
Never Smoked
RESULTS – BLOOD FLOW AND INFECTION
Dichotomous vascular disease
All patient had some evidence of vascular disease
ABI were either >1.1 or <0.4
All patients were referred to vascular surgery/interventional radiology as part of their
treatment
Underlying osteomyelitis
41 positive
33 negative
No differences noted in bacterial species, quantity of microorganisms, type of
organisms or resistance patterns
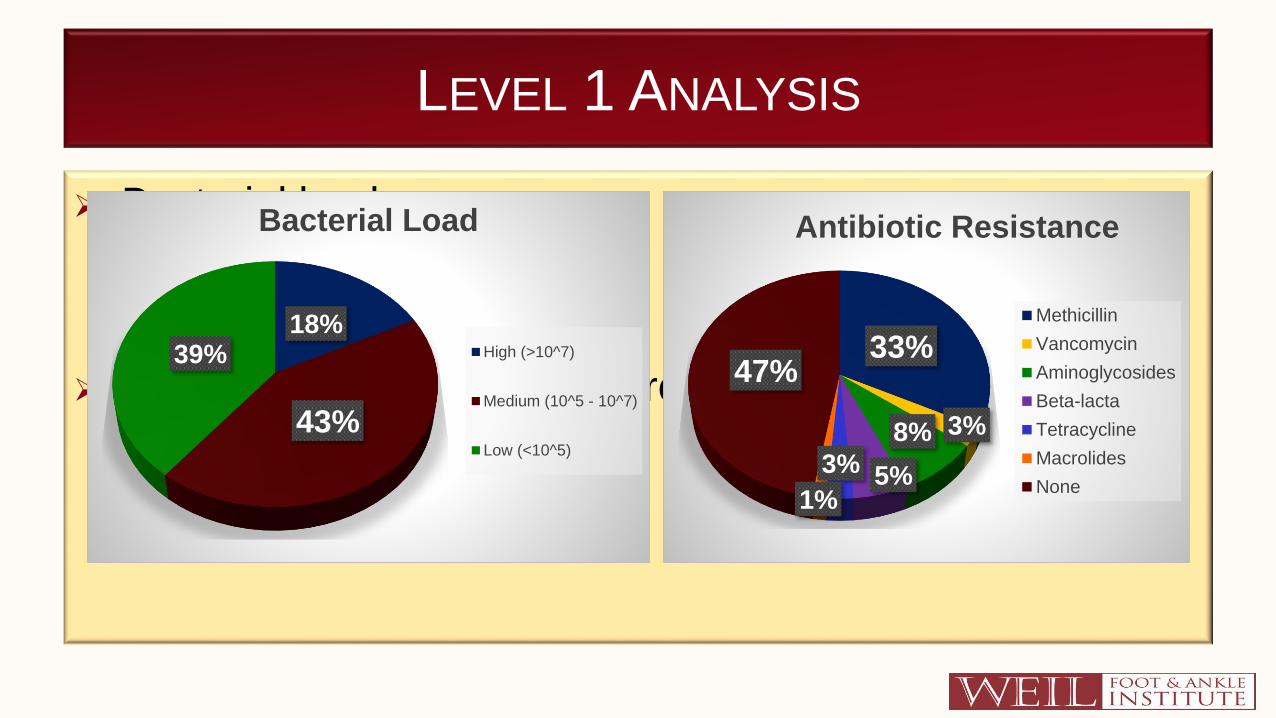
LEVEL 1 ANALYSIS
Bacterial load
Gene markers for antibiotic resistance
18%
43%
39%
Bacterial Load
High (>10^7)
Medium (10^5 - 10^7)
Low (<10^5)
33%
3%8%
5%3%
1%
47%
Antibiotic Resistance
Methicillin
Vancomycin
Aminoglycosides
Beta-lacta
Tetracycline
Macrolides
None
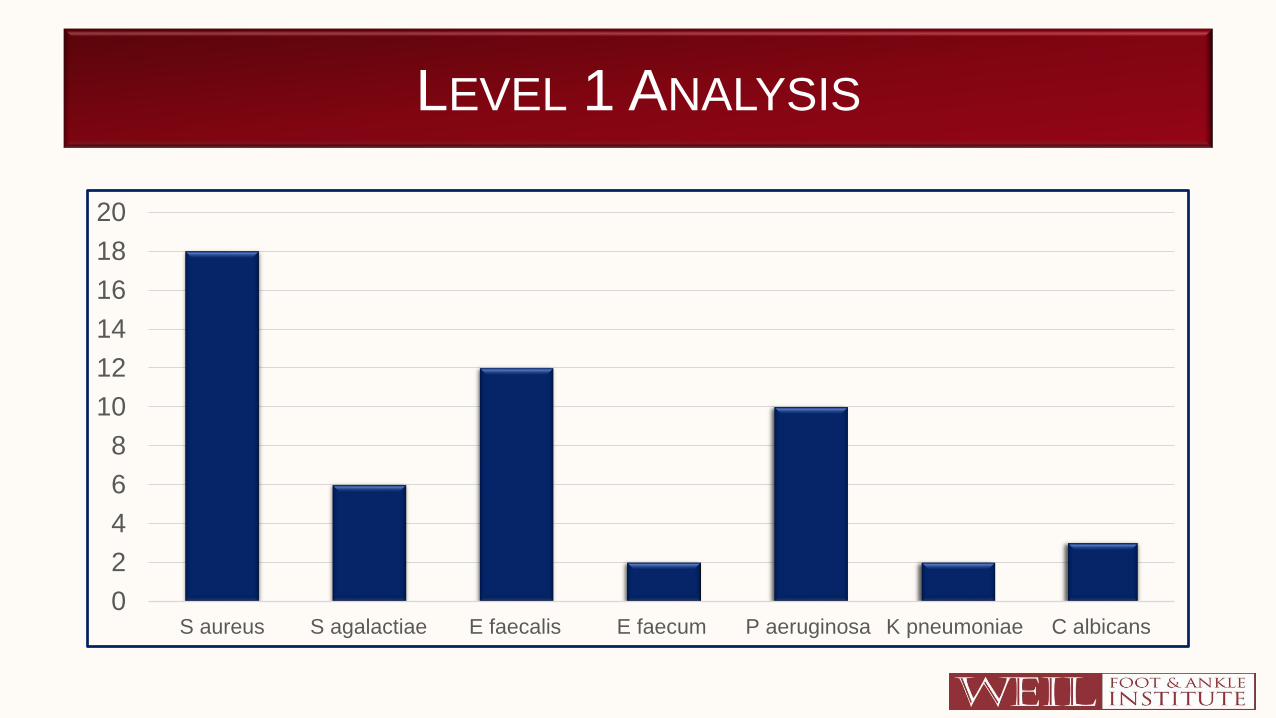
LEVEL 1 ANALYSIS
0
2
4
6
8
10
12
14
16
18
20
S aureus S agalactiae E faecalis E faecum P aeruginosa K pneumoniae C albicans
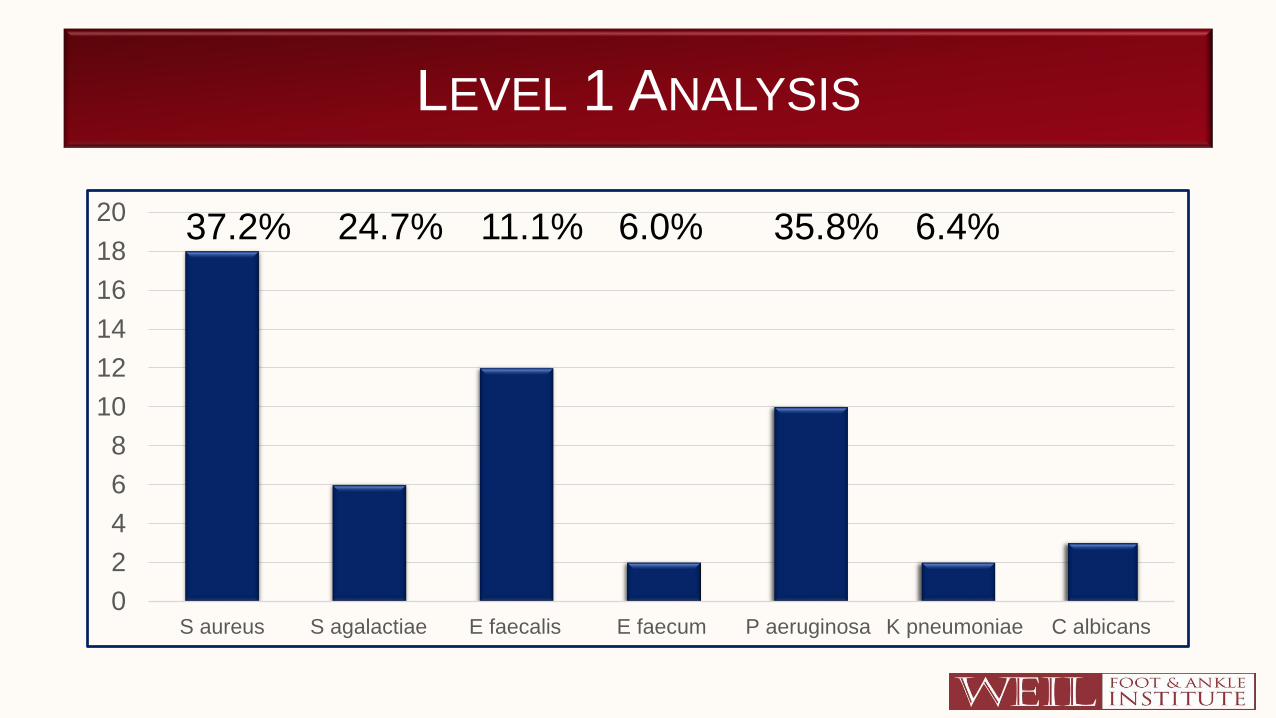
LEVEL 1 ANALYSIS
0
2
4
6
8
10
12
14
16
18
20
S aureus S agalactiae E faecalis E faecum P aeruginosa K pneumoniae C albicans
37.2% 11.1%24.7% 6.0% 35.8% 6.4%
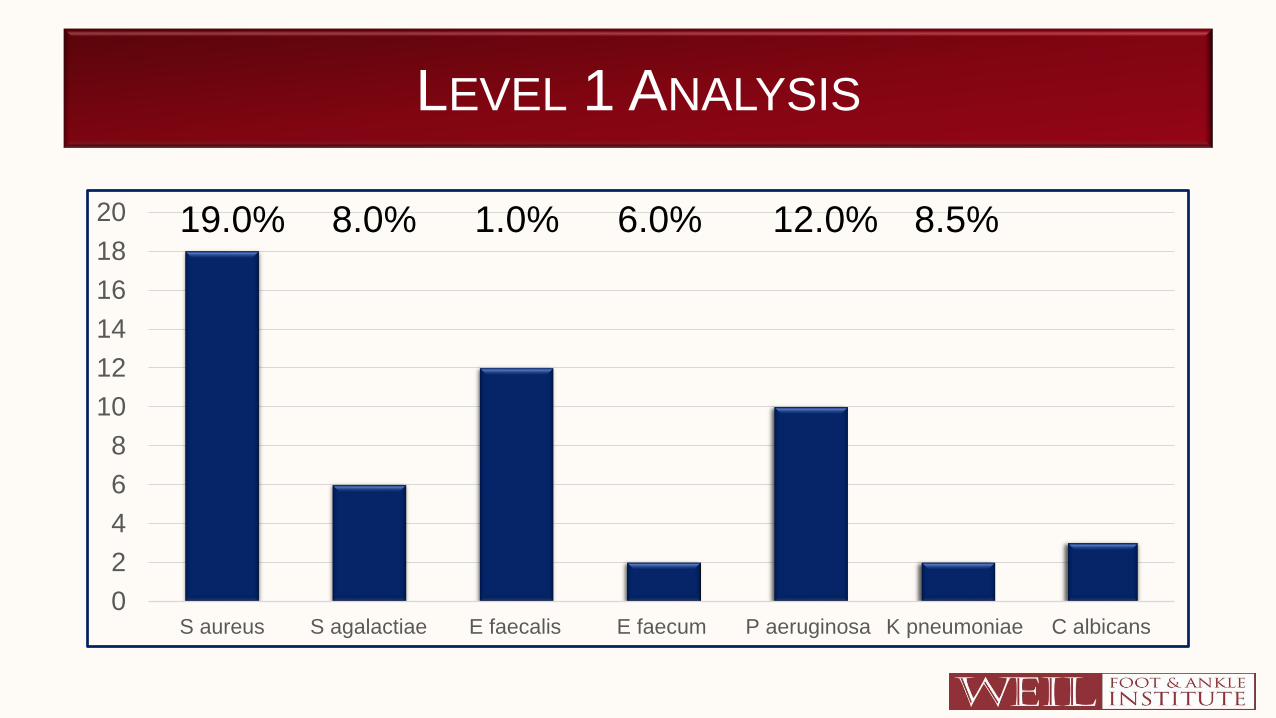
LEVEL 1 ANALYSIS
0
2
4
6
8
10
12
14
16
18
20
S aureus S agalactiae E faecalis E faecum P aeruginosa K pneumoniae C albicans
19.0% 1.0%8.0% 6.0% 12.0% 8.5%

LEVEL 2 ANALYSIS
56 genera
124 species
Average number of species per wound:
4.4 + 3.4 (range 1 – 15)
Median: 3

LEVEL 2 ANALYSIS
31%
67%
2%
Oxygen Status of Isolated Organisms
Aerobes
Anaerobic
Unknown

LEVEL 2 ANALYSIS
58%31%
3%1%
5%
1%
1%
Bacillus
Cocci
Coccibacillus
Curved/bent
Not reported
Variable
clusters of 8

LEVEL 2 ANALYSIS
Top performers Isolated Oxygen Status Gram Stain Shape
Staphylococcus 43 Facultative anaerobes Positive Cocci
Anaercoccus 37 Anaerobic Positive Cocci
Corynebacterium 36 Aerobic Positive Bacillus
Peptoniphilus 22 Anaerobic Positive Cocci
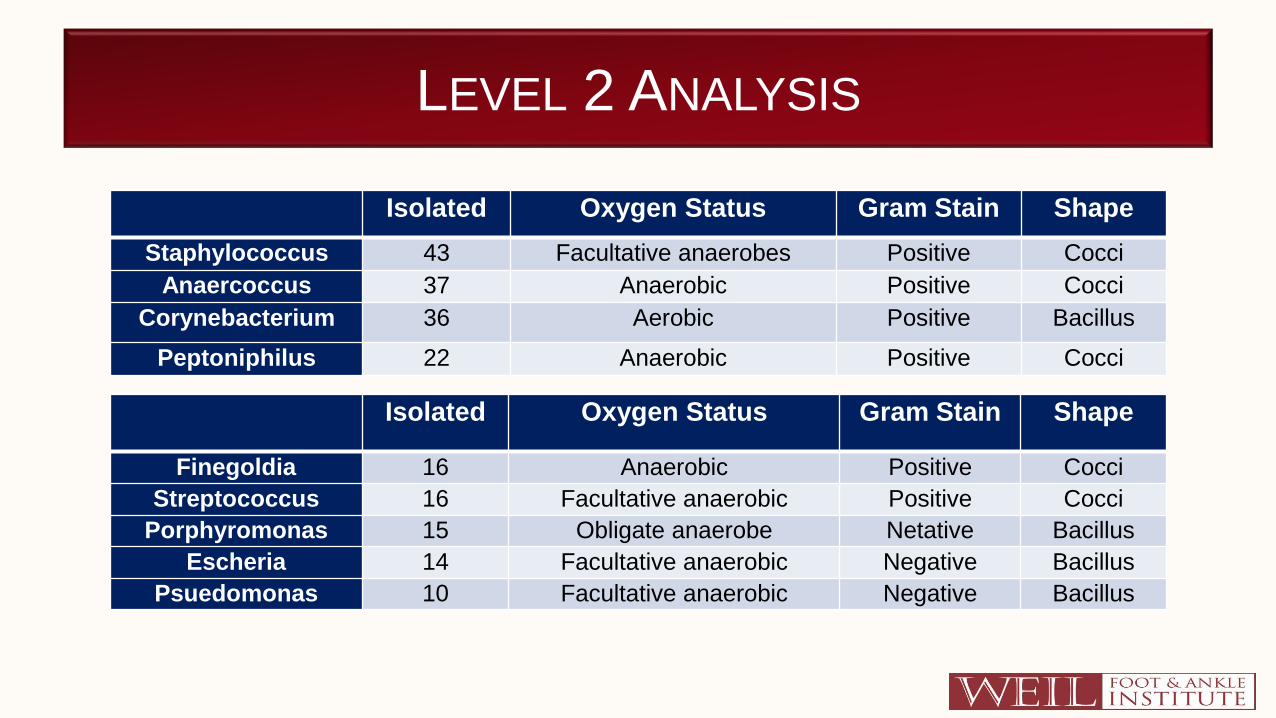
LEVEL 2 ANALYSIS
Isolated Oxygen Status Gram Stain Shape
Staphylococcus 43 Facultative anaerobes Positive Cocci
Anaercoccus 37 Anaerobic Positive Cocci
Corynebacterium 36 Aerobic Positive Bacillus
Peptoniphilus 22 Anaerobic Positive Cocci
Isolated Oxygen Status Gram Stain Shape
Finegoldia 16 Anaerobic Positive Cocci
Streptococcus 16 Facultative anaerobic Positive Cocci
Porphyromonas 15 Obligate anaerobe Netative Bacillus
Escheria 14 Facultative anaerobic Negative Bacillus
Psuedomonas 10 Facultative anaerobic Negative Bacillus
WHY SO MANY ANAEROBES?
LET’S TAKE A WALK BACK TO THAT BIOFILM THING

BIOCIDES VS BIOFILM
After 60 minutes of exposure
to bleach
Dying cells (green)
Alive cells (red)

COAGGREGATION AND SYMBIOTIC RELATIONSHIPS
Is it possible that bacteria live in
communities where certain bacteria
have symbiotic relationships with
others?
Aerobes live at surface
Anaerobes live a bit deeper
Oxygen penetrates biofilm 4 microns.

WHAT DOES ALL OF THIS MEAN?
In many ways, the clinical significance of this data is currently unclear.
Identified that there is a higher than previously thought level of anaerobic bacteria that is present in wound beds.
Variability of bacteria in biofilms and wound beds.
There may be a role for topical antibiotics that are aimed at all of the microbial species in the wound bed, rather than just one or two.

FUTURE STUDIES IN THIS AREA
Personalized/customized medicine based on genomics may be
the way of the future.
16S amplicon vs PCR vs plated culture study
Prospective study on customized topical medication and wound
outcomes

THANK YOU!
ERIN E KLEIN, DPM, MS
LOWELL WEIL, JR, DPM
ADAM E FLEISCHER, DPM