the journal of implant & advanced clinical dentistry - oct. 2015
TRANSCRIPT

Elkhadem et al
Background: to describe the con-cept and use of a simplified keyless guided implant placement system in partially and completely edentulous patients.
Methods: 89 implants were placed in 23 patients (7 complete, and 16 partial cases) using the universal simple guide kit. After CBCT and virtual implant planning, surgi-cal guides with c-shaped sleeves were con-structed. The implants were placed using flap or flapless approach according to the need for soft or hard tissue augmentation. The intra-operative complications, post-operative com-plains and implant survival rate were reported.
Results: All implants demonstrated insertion torque values greater than 30 Ncm. Only few post- operative complications were reported. 98.9% of the placed implants integrated.
Conclusions: The keyless partial guid-ance using the simple guide kit and c-shaped sleeves is a promising economic alterna-tive to conventional guided approach. Fur-ther investigations are required to evaluate its accuracy and long term success rates.
The Keyless Partially Guided Implant
Placement Protocol: Success Rate
and Complications
Amr Hosny Elkhadem, DDS, MSc1
1. Lecturer, Prosthodontics, Faculty of Oral & Dental medicine, Cairo University
Abstract
KEY WORDS: Computer-aided Implantology, surgical guide, open sleeve, tolerance
The Journal of Implant & Advanced Clinical Dentistry • 25

26 • Vol. 7, No. 8 • October 2015
INTRODUCTIONThe use of CT scans combined with computer software to plan implant cases has been pro-posed since the 1990s.1 The technique aims to provide correlation between the bone anat-omy and the desired tooth position allowing for predictable aesthetic and functional out-comes. Many authors refer to guided implant placement as a protocol that enhances the accuracy and safety of implant placement.2-4
Moreover, it allows for the minimally invasive flapless technique in many situations, which minimizes the intra-operative time, postopera-tive pain and postoperative complications.4,5
Despite of the aforementioned advan-tages the techniques is not popular among implant practitioners. This might be attributed to the higher cost and time required to plan the cases and fabricate the guides. Expensive guided implant kits with complex assortment are also mandatory.6 Additionally, the control over implant direction is usually achieved with a closed circular configuration with small drill tolerance. Using the relatively longer drills for guided systems through such closed configu-ration was always associated with accessibil-
ity problems in the posterior region for dentate patients. Such a small tolerance is manda-tory to provide accuracy, yet it is thought to block the passage of the irrigation and might cause increased incidence of implant fail-ure in dense bone and deep osteotomies7
Moreover, there is an uprising question related to the accuracy imposed by the mechan-ical tolerance of the machined components. To provide adequate precision of the guided sys-tems, a small gap of approximately 20 microns is provided between the main sleeve fixed in the guide and the removable, diameter spe-cific, keys. A similar tolerance gap is designed between the removable keys and the drills. The friction during repeated use of the keys and the drills increases the gap obviously which might contribute to increases linear and angu-lar deviation with these guided systems.8,9
When weighing the merits and demer-
Figure 1: The simple guide kit. (a) cortical drill, (b) 2.3 mm
starter drill, (c,d,e) 2.2 mm pilot drill with variable lengths,
(f) 2.8 mm intermediate drill.
Figure 2: Surgical guide with c-shaped sleeve establishing
3 mm facial openings for side approach of the drills.
Elkhadem et al

The Journal of Implant & Advanced Clinical Dentistry • 27
its of conventional guided systems one can understand why such protocol is not so pop-ular. Hence, there is a great need to pro-vide modification in the concept and design of guided surgical approach to overcome the drawbacks and maximize the benefits.
MATERIALS AND METHODSThe technique utilizes a simplified universal kit design (Simple guide kit, Dentis Co.-Ltd, Daegu, South Korea) and a modified C-shaped main sleeve. The kit design eliminates the removable keys used in conventional guided kits, and adopt the concept of guidance for the pilot and inter-mediate drills only. For all cases, the final drill-ing is done after removing the surgical guide using the conventional non-guided final drills.
The design and sequence of the simplified
kit is different from the regular guided implant drills (Fig 1). All drills are composed of cutting flutes and a smooth guiding shaft that is com-patible in size with the main sleeve of the surgi-cal guide with no removable key in between. The drilling sequences starts with a pointed drill for penetration of the cortical bone. A starter drill (2.3x8mm) is used to create an initial osteotomy inside the bone. This is followed by the use of pilot drills (2.2mm in diameter). The pilot drills have variable lengths according to the desired implant to be placed. As the pilot drill diameter is smaller than the initial osteotomy created by the starter drill, it will snap into the osteotomy engag-ing 8 mm of vertical bone height and part of its guiding shaft will engage the main sleeve of the guide. In all scenarios, a 2.8x8mm intermediate drill is used afterwards to prepare the coronal
Figure 3: Virtual implant planning for an edentulous case. Implants were placed in relation to the required prosthetic
position guided by the radio-opaque scan appliance.
Elkhadem et al
28 • Vol. 7, No. 8 • October 2015
8 mm of the osteotomy. As the osteotomy path is shaped the surgical guide is removed and the final drill of the conventional kit is used to cre-ate the final osteotomy shape. This is followed by inserting the implant in the conventional non guided fashion. Additionally, the surgical guide is designed with a c-shaped metal sleeve with a facial opening (Fig 2). The opening allows for side approach of the drills and unrestricted access of the coolant. In this report, 23 cases were oper-ated. 89 implants were installed in 7 completely edentulous and 16 partially edentulous cases.
COMPLETELY EDENTULOUS CASES
37 implants were installed in 7 completely edentulous cases (two mandibular and 5 max-illary) using this technique. Preparation started by duplicating the patient denture into radio-
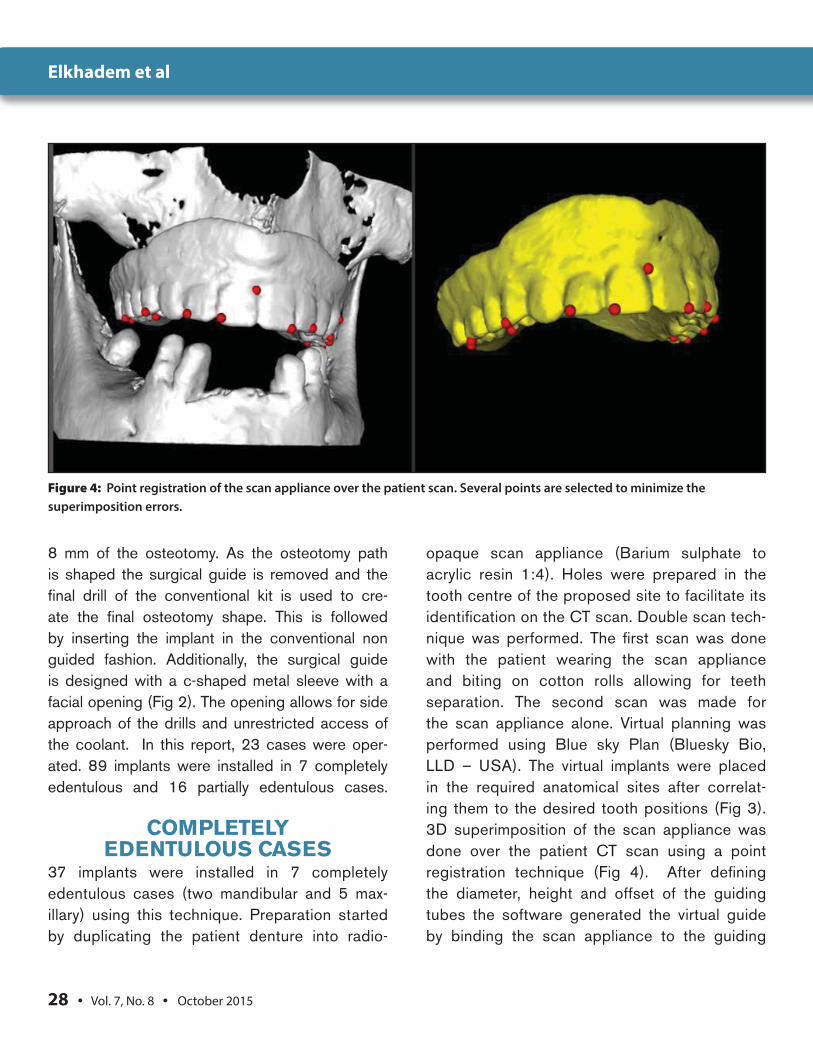
opaque scan appliance (Barium sulphate to acrylic resin 1:4). Holes were prepared in the tooth centre of the proposed site to facilitate its identification on the CT scan. Double scan tech-nique was performed. The first scan was done with the patient wearing the scan appliance and biting on cotton rolls allowing for teeth separation. The second scan was made for the scan appliance alone. Virtual planning was performed using Blue sky Plan (Bluesky Bio, LLD – USA). The virtual implants were placed in the required anatomical sites after correlat-ing them to the desired tooth positions (Fig 3). 3D superimposition of the scan appliance was done over the patient CT scan using a point registration technique (Fig 4). After defining the diameter, height and offset of the guiding tubes the software generated the virtual guide by binding the scan appliance to the guiding
Figure 4: Point registration of the scan appliance over the patient scan. Several points are selected to minimize the
superimposition errors.
Elkhadem et al

The Journal of Implant & Advanced Clinical Dentistry • 29
tubes. The STL file of the guide was fabricated using additive manufacturing. C-shaped sleeves were fixed in the surgical guide and the guid-ing tubes were opened facially opposite to the sleeve openings (Fig 2). The guide was fixed in the patient mouth with 3 fixation screws and the suggested drilling sequence was applied.
PARTIALLY EDENTULOUS CASES
52 implants in 16 partially edentulous cases (7 mandibular and 9 maxillary) were placed. Patient scanning protocol differed according to the number of missing teeth and the presence of metallic restorations. In cases with few miss-ing teeth and few or no metallic restoration, the patient received a CBCT with no scan appli-ance. The patient model was scanned using a laser scanner. When the patient had multiple missing teeth and /or numerous metallic resto-rations a scan appliance with radiopaque mark-ers was first prepared. The patient had a CBCT wearing the scan appliance. Afterwards, a CBCT for the patient model with the scan appli-
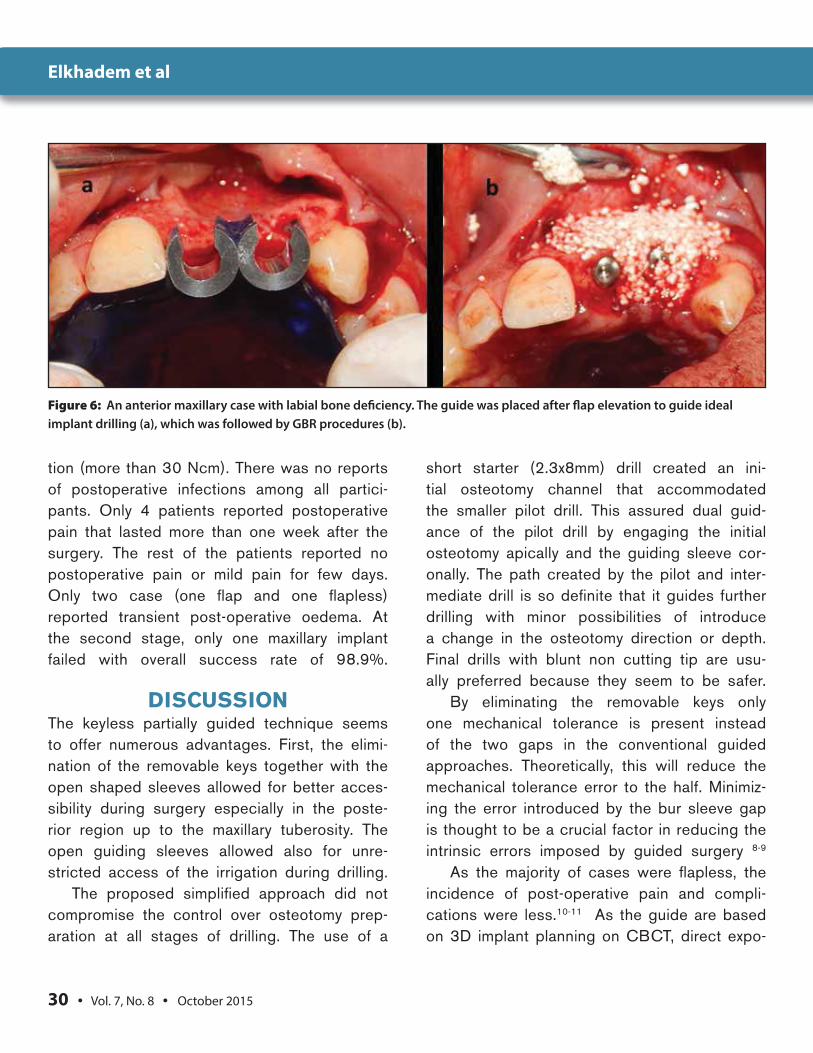
ance was made for superimposition purposes. Virtual planning was done after correlating the prosthetic position to the underlying bone anat-omy. When no scan appliance existed virtual tooth setting was utilized. When designing the guide, extension over the adjacent teeth as well as part of the palatal and lingual mucosa was required to assure proper stability. All cases not requiring grafting were done in a flapless man-ner (Fig 5). In cases requiring bone grafting a flap was first raised and the guide was then used for implant placement (Fig 6). When extra security was required to fix the guide in place light-cured flowable composite was used to tem-porarily bond the guide to the supporting teeth.
RESULTSNo major intra-operative complications or problems were reported in either flap or flap-less cases. In few cases the c-shaped sleeves were detached off the guide when contact-ing the drills. The sleeves were replaced and the procedure completed. All implants dem-onstrated acceptable implant stability at inser-
Figure 5: A bilateral flapless maxillary case. Plan was made to avoid enlarged sinus on the left side (a). The guide design
allowed implant placement at the tuberosity region (b).
Elkhadem et al
30 • Vol. 7, No. 8 • October 2015
Figure 6: An anterior maxillary case with labial bone deficiency. The guide was placed after flap elevation to guide ideal
implant drilling (a), which was followed by GBR procedures (b).
tion (more than 30 Ncm). There was no reports of postoperative infections among all partici-pants. Only 4 patients reported postoperative pain that lasted more than one week after the surgery. The rest of the patients reported no postoperative pain or mild pain for few days. Only two case (one flap and one flapless) reported transient post-operative oedema. At the second stage, only one maxillary implant failed with overall success rate of 98.9%.
DISCUSSIONThe keyless partially guided technique seems to offer numerous advantages. First, the elimi-nation of the removable keys together with the open shaped sleeves allowed for better acces-sibility during surgery especially in the poste-rior region up to the maxillary tuberosity. The open guiding sleeves allowed also for unre-stricted access of the irrigation during drilling.
The proposed simplified approach did not compromise the control over osteotomy prep-aration at all stages of drilling. The use of a
short starter (2.3x8mm) drill created an ini-tial osteotomy channel that accommodated the smaller pilot drill. This assured dual guid-ance of the pilot drill by engaging the initial osteotomy apically and the guiding sleeve cor-onally. The path created by the pilot and inter-mediate drill is so definite that it guides further drilling with minor possibilities of introduce a change in the osteotomy direction or depth. Final drills with blunt non cutting tip are usu-ally preferred because they seem to be safer.
By eliminating the removable keys only one mechanical tolerance is present instead of the two gaps in the conventional guided approaches. Theoretically, this will reduce the mechanical tolerance error to the half. Minimiz-ing the error introduced by the bur sleeve gap is thought to be a crucial factor in reducing the intrinsic errors imposed by guided surgery 8-9
As the majority of cases were flapless, the incidence of post-operative pain and compli-cations were less.10-11 As the guide are based on 3D implant planning on CBCT, direct expo-
Elkhadem et al

The Journal of Implant & Advanced Clinical Dentistry • 31
sure of bone was not utilized unless soft and / or hard tissue augmentation was required. Moreover, conservative transmucosal drill-ing was used. Tissue punch was not used as there is no proven clinical advantage or impact on the implant success rate when com-pared to transmucosal drilling. On the con-trary, the increase in the size of the punched tissue is thought to increase the probing depth and crestal bone loss around implants.12
A debate exist about the accuracy of partial guidance in comparison to classical fully guided systems. While some practitioners might believe that guided final drilling and insertion signifi-cantly affect the accuracy others believe that guidance of the initial osteotomy provides suf-ficient guidance to the rest of the procedures. The clinical data regarding the survival rate and accuracy of partial versus full guidance is still sparse.13 Kuhl et al.14 evaluated the accu-racy of half versus fully guided techniques on cadaver model. They found no statistical sig-nificant difference between the two protocols. Yet, there is a need to conduct more clinical tri-als to evaluate the accuracy of both systems.
CONCLUSIONThe use of the simplified partially guided key-less approach seems to be a promising alter-native to conventional guided surgery. The technique allowed easy access to the poste-rior region with efficient delivery of the irriga-tion during drilling. The use of a small economic universal kit might encourage many practitio-ners to utilize guided surgery. Further stud-ies are required to compare the accuracy and success rate versus the conventional guided techniques and manual techniques. ●
Correspondence:Dr. Amr Hosny Elkhademe-mail: [email protected] Address: 5 jasmine buildings zahraa elmaadi- Cairo – EgyptPostal code: 11435
DisclosureThe author reports no conflicts of interest with anything mentioned in this article.
References1. Verstreken K, Van Cleynenbreugel J, Martens K, Marchal G, van Steenberghe
D, Suetens P. An image-guided planning system for endosseous oral implants. IEEE Trans Med Imaging 1998;17(5):842-852.
2. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 1: diagnostics, imaging, and collaborative accountability. Int J Periodontics Restorative Dent 2006;26(3):215-221.
3. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 2: rapid-prototype medical modeling and stereolithographic drilling guides requiring bone exposure. Int J Periodontics Restorative Dent 2006;26(4):347-353.
4. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 3: stereolithographic drilling guides that do not require bone exposure and the immediate delivery of teeth. Int J Periodontics Restorative Dent 2006;26(5):493-499.
5. van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, et al. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. Clin Implant Dent Relat Res 2005;7 Suppl 1:S111-120.
6. Vercruyssen M, Hultin M, Van Assche N, Svensson K, Naert I, Quirynen M. Guided surgery: accuracy and efficacy. Periodontol 2000. 2014;66(1): 228-246.
7. Yong LT, Moy PK. Complications of computer-aided-design/computer-aided-machining-guided (NobelGuide) surgical implant placement: an evaluation of early clinical results. Clin Implant Dent Relat Res. 2008;10(3):123-127.
8. Cassetta M, Di Mambro A, Di Giorgio G, Stefanelli LV, Barbato E. The Influence of the Tolerance between Mechanical Components on the Accuracy of Implants Inserted with a Stereolithographic Surgical Guide: A Retrospective Clinical Study. Clin Implant Dent Relat Res. 2015;17(3):580-588.
9. Cassetta M, Di Mambro A, Giansanti M, Stefanelli LV, Cavallini C. The intrinsic error of a stereolithographic surgical template in implant guided surgery. Int J Oral Maxillofac Surg. 2013;42(2):264-75.
10. Hultin M1, Svensson KG, Trulsson M. Clinical advantages of computer-guided implant placement: a systematic review. Clin Oral Implants Res. 2012;23 Suppl 6:124-35.
11. Brodala N. Flapless surgery and its effect on dental implant outcomes. Int J Oral Maxillofac Implants 2009;24 Suppl:118-25.
12. Lee DH, Choi BH, Jeong SM, Xuan F, Kim HR, Mo DY. Effects of soft tissue punch size on the healing of peri-implant tissue in flapless implant surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(4):525-30.
13. Van Assche N, Vercruyssen M, Coucke W, Teughels W, Jacobs R, Quirynen M. Accuracy of computer-aided implant placement. Clin Oral Implants Res. 2012;23 Suppl 6:112-23
14. Kühl S, Zürcher S, Mahid T, Müller-Gerbl M, Filippi A, Cattin P. Accuracy of full guided vs. half-guided implant surgery. Clin Oral Implants Res. 2013;24(7):763-9.
Elkhadem et al