the islamic university- gaza report about nocardia spp. prepared by manal ghanem el-astal supervised...
Post on 20-Dec-2015
220 views
TRANSCRIPT
The Islamic University- GazaThe Islamic University- Gaza
Report about Nocardia sppReport about Nocardia spp..
Prepared by Prepared by Manal Ghanem El-AstalManal Ghanem El-Astal
Supervised bySupervised byDr. Abdelraouf A. ElmanamaDr. Abdelraouf A. Elmanama
2
Nocardia is a member of the family Actinomycetales
Actinomycetales
Actinomycetes Mycobacteria Streptomyces Nocardia
• Both Actinomyces and Nocardia are filmentous branching bacteria and
• were often confused with fungi before the fundemental differences between prokaryotes and eukaryotes were recognized.
• Actinomycetes anaerobic
• Nocardia is Strictly aerobic.
(Cont.)

Nocardia spp. Includes
• Nocardia asteroides
• Nocardia farcinica
• Nocardia nova
• Nocardia transvalensis
• Nocardia brasiliensis
• Nocardia caviae
• Nocardia otitidiscaviarum

Route of infection
• Nocardia spp. are soil saprophytes
• route of infection can be either 1. By inhalation
2. By direct cutaneous inoculation.

• 90% of nocardial infections are caused by inhalation of members of the N. asteroides group
Nocardia asteroides complexNocardia farcinica
Nocardia nova
• Other strains represent the remaining 10% of infections.
(Cont)

• N. brasiliensis is the most important in tropical areas.
• It is most often seen as a cutaneous infection • Can affect individuals with normal immune
function • 70% of cases of N. brasiliensis are seen in
immunocompromised individuals.
(Cont.)

Characteristics of Nocardia• Classically Gram +ve(may be variable)
• Strictly aerobic
• Filmentous
• Branching
• weakly acid –fast bacilli
• Have mycolic acid in cell wall.
• Nocardia has cells that are 1.0 µm wide and 1.0-2.0 µm long.

Identifecation of Nocardia in culture media• Types of samples
Sputum culture
Bronchoscopy
Lung biopsy
Skin biopsy
Brain biopsy

Nocardia can be difficult to isolate by culture
• Because of over growth by faster- growing nonpathgenic colonizers that may mask its presence.
• solid medium that uses paraffin as the sole source of carbon has been effective for isolating Nocardia spp. from contaminated clinical specimens.
Other types of media
• Sheep blood agar
• L.j medium
• Sabouraud dextrose agar (chloramphenicol should not be added)
Nocardia spp. inhibited by chloramphenicol
Rate of growth time to visible colonies
• May be 2- 4 days.
• May be 2- 4 weeks.
Diagnosis may be difficult . In the clinical laboratory, routine cultures may be
held for insufficient time to grow Nocardiae.

The colonial appearance of Nocardia spp. are extremely variable
• May be smooth and moist, or
• Have”mold- like” verrucous grey – white waxy,or
• powdery appearance from aerial hyphae.
• Nocardia colonies initially have a dry, wrinkled, chalk like appearance, adhere to the agar, and develop white to orange pigment over time.
• Nocardia colonies have very distinct,strong mildew oder that allow experienced microbiologists to suspect their presence.

• The colonies of N. brasiliensis (left) and N. caviae (right) pictured below show the wide range of colony appearance, even within the same species:

Nocardia with Gram stain and acid Fast stain
• Gram variable, with a “beeded”appearance of alternating G+ve and G+ve segments along a filments.
• However , Nocardia grown under suboptimal conditions sometimes appear uniformly Gram – negative.

(Cont.)
• Nocardia organisms are classically weakly modified acid-fast.
• This characteristic may help to distinguish Nocardia from negative Actinomyces (which is modified-acid-fast-negative).

(Cont.)
• Nocardia can occasionally appear modified-acid-fast-stain negative.
• Nocardia grown under suboptimal conditions will have retarded synthesis of mycolic acids in their cell wall that, in turn, compromises the ability of the organisms to retain Gram stain or modified-acid-fast stains.

Differentiation of Nocardia species
• Histologic appearance of Nocardia is similar to other Actinomycetes family members,
culture and biochemical testing is necessary for definitive
diagnosis/identification.

(Cont.)
• The UPMC-Presbyterian Mycology Laboratory performs
petri-dish cultures with tap water agar (1%) to differentiate the Nocardias and other aerobic Actinomycete genera from the rapid growing mycobacteria.
• (The trace organic material found in tap water provides sufficient nutrients to support growth)

(Cont.)• Biochemical tests includes:1. hydrolysis of casein, tyrosine, and/or xanthine.
2. presence of urease.
3. utilization of rhamnose.
4. positive resistance to lysozyme, and
5. Catalase test.
(Cont.)
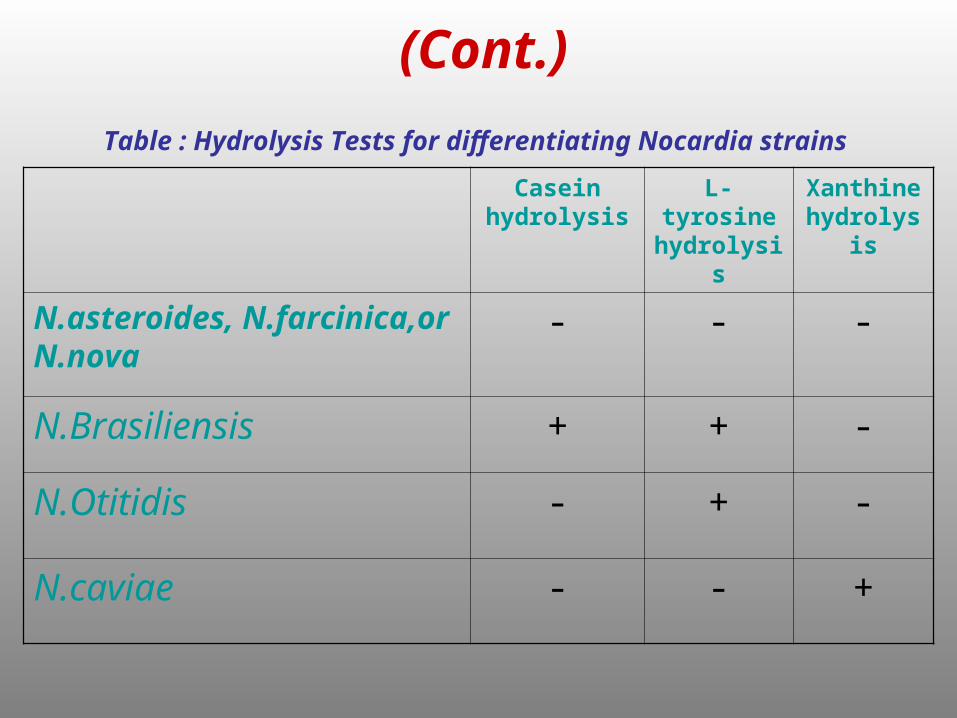
Table : Hydrolysis Tests for differentiating Nocardia strains
Casein hydrolysis
L-tyrosine hydrolysis
Xanthine hydrolysis
N.asteroides, N.farcinica,or N.nova
- - -
N.Brasiliensis + + -
N.Otitidis - + -
N.caviae - - +

(Cont.) Hydrolysis Pattern of casein
• N. brasiliensis (left, below) versus N. caviae (right, below).
• Generally, casein media is in the lower left, followed by L-tyrosine(upper left) and xanthine (upper right ).

(Cont.)
• An antibiotic susceptibility test may be performed for a more precise identification
• N. asteroides group (N. asteroides complex; N. farcinica; or N. nova) have the same hydrolysis test
(Cont.)
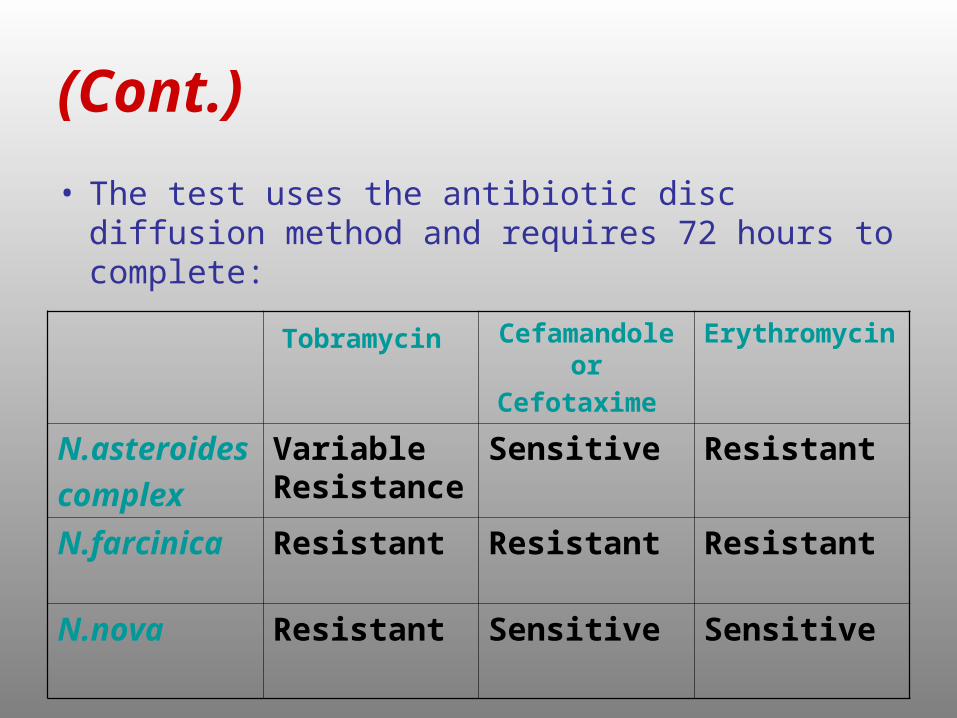
• The test uses the antibiotic disc diffusion method and requires 72 hours to complete:
Tobramycin Cefamandole
or Cefotaxime Erythromycin
N.asteroides
complex
Variable Resistance
Sensitive Resistant
N.farcinica Resistant Resistant Resistant
N.nova Resistant Sensitive Sensitive
In general, diagnostic factors are
• Catalase positive.
• Urease positive
• Filamentous morphology.
• Orange-red waxy wrinkled colonies.
• Poorly stained with Gram's stain.
• Have strong mildew odor
• Growth on blood agar

Sites and Sources of Nocardia
• Nocardia spp.found in the environment,
(In soil and in dust particles)
(as saprophytes)
• Nocardia not considered as normal human flora.

(Cont.)
Nocardia spp.usually occur:
• In recipients of bone marrow and organ transplants.
• In patients with leukemia, lymphoma, humeral or leukocyte defects
• After prolonged steroid therapy.
• In patients with connective tissue disorders, and
• In HIV / AIDS patients.

• Generally :
It occur in immunocompromised patients.

Virulence factors
• Nocrdia spp. grow in nonactivated macrophage, have intracellular growth, and have prenvention of phagolysosome fusion.

Pathogenesity and symptoms
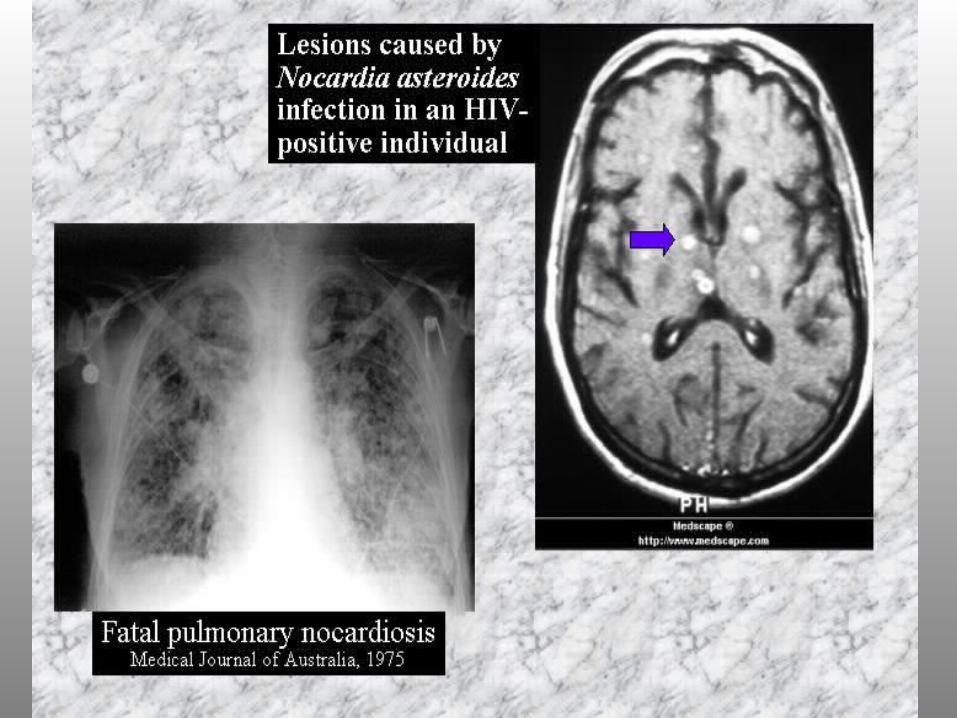
1. Pulmonary Nocardiosis:
”Lung involvement”
Caused by Nocardia asteroides group.
Symptoms include • Fever • Coughing blood • Weight loss• Night sweats, and • Chest pain

(Cont.)
2. Brain abscess:
Caused by Nocardia asteroides group.
Symptoms include • Headache • Lethargy• Confusion• Vomiting• Seizures, and • Sudden onset of neurologic problems.
(Cont.)3. Cutaneous Nocardiosis:
”Skin infection” “Myctoma”
Caused by Nocardia brasiliensis
Symptoms include • Pustules • Fever • Tender lymphadenitis in the regional lymph
nodes, and • May become chronically infected (myctoma) and
develop draining tracts

(Cont.)
4. Disseminated disease from Nocardia:
It may also involve • the kidneys• the joints • the heart • the eye, and • the bones.

(Cont.)
• (about 90%) of cases of nocardiosis involves lung infection, brain abscess, or disseminated (wide spread) disease from Nocardia.
• The remaining 10% of cases are localized to the skin.
(Cont.)
• Nocardia asteroides is an important opprtunistic Pathogen in patients with malignancy or receiving immunosuppressive therapy and usually responsible for pulmonary infection.

(Cont.)
• Nocardia brasiliesis, is the primary pathgen in mycetoma but may occasionally found in disseminated disease, particularly in patients with poor host defense mechanism.
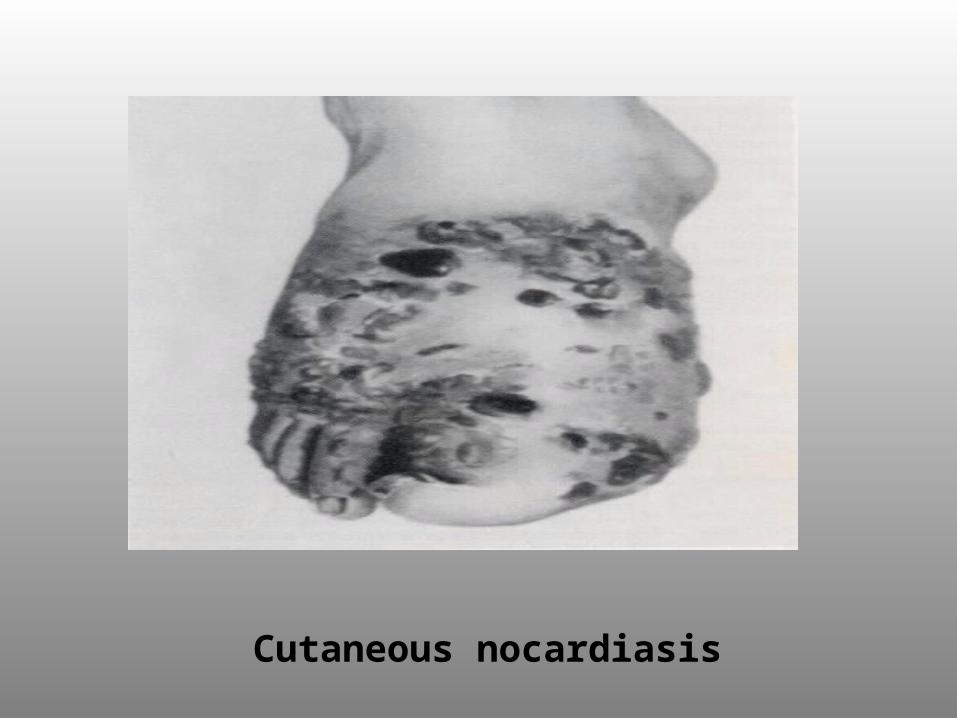
Cutaneous nocardiasis

Mode of transmission of disease
• Nocardia is found in soil.
• The inhalation of Nocardia spores usually initiates pulmonary nocardiosis.
• The skin form of nocardiosis is contracted through soil contamination of wounds.

(Cont.)
• There is no evidence for person to person transmission of Nocardia.
• Rarely nosocomial post surgical transmission occurs.

Risk factors
• While individuals with normal immune systems can acquired this infection, the main risk factors for nocardiosis are
• Weakened immune system or chronic lung disease.
• People on chronic steroid therapy, • Those with cancer, • Organ or bone marrow transplants, or • HIV / AIDS are at risk , and • Males (ratio male: female = 3:1).
Treatment• Nocardia are not susceptible to penicillin.
• The current drug of choice is sulfonamides.
• Long-term antibiotic therapy (usually with sulfonamides) for 6 months to a year (or longer depending on the individual and site involved) is needed to treat nocardia.
• Chronic suppressive therapy may be needed (prolonged, low-dose antibiotic therapy).
• In addition, in patients with abscesses caused by this infection, surgery may be required in order to ensure adequate drainage.

(Cont.)• The antimicrobial combination of
trimethoprim-sulfamethoxazole (TMP-SMX) is the drug of choice.
Howeverresistance to TMP-SMX is becoming more
common.(e.g. N. farcinica is more resistant TMP-SMX).• A new combination drug therapy
(sulfonamide, ceftriaxone, and amikacin) has shown promise for infections difficult to treat.

Prognosis for Nocardial infection• About 10% of cases of uncomplicated Nocardia
pneumonia are fatal.
• Prognosis depends on the sites involved.
• The fatality rates increase with disseminated disease, and brain abscess.
• In addition, the degree of impairment of the individual's immune system will affect the outcome.
عليكم السالم