the ins and outs of enteral nutrition gravity drip – many times forgotten martin k, ncp...
TRANSCRIPT
The Ins and Outs of Enteral NutritionKELLY GREEN CORKINS, MS, RD-AP, CSP, LDN, FAND
CLINICAL DIETITIAN III, LE BONHEUR CHILDREN’S HOSPITAL, MEMPHIS, TN
1

Disclosures
u Abbott Speakers Bureau – honoraria
(Not product related)
2

Objectives
u Provide information on the differences in enteral formula categories (polymeric or standard, peptide based, elemental, commercially prepared blenderized).
u Discuss the home made blenderized diet – advantages and disadvantages.
u Discuss ENFitu Describe common symptoms of formula intolerance
and other medical related reasons for intolerance.
3
The Ins
FORMULASBLENDERIZED TUBE FEEDINGSADMINISTRATION
4
Enteral Formula Regulation
u Considered Medical Foods by the United States Food and Drug Administration.
u “a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation.”
u Efficacy studies are not required.
u Pre-marketing review or approval is not required.
u Manufacturing is monitored and regulated.
5
Escuro NCP 2016;31(6):709-722Brown NCP 2015;30(1):72-85

Enteral Formulas(P) = Pediatric Product available
Standard/Polymeric (P)
Manufactured Blenderized (P)
Peptide based/Semi-elemental (P)
Elemental (P) Specialty
Diabetes/glucose intoleranceRenal (P)HepaticPulmonaryImmune modulating
6

Pediatric versus Adult Products
Pediatric Products:u 12% kcals from proteinu 34-43% kcals from fatu 45-57% kcals from
carbohydrateu Higher in calcium and vitamin D
Adult Products:u 16% kcals from proteinu 30% kcals from fatu 54-61% kcals from
carbohydrateu Higher in Folic Acid and Zinc
7

Composition of enteral formulas
u Proteinu Animal sources have a higher biological value than
plant sources.
u Intact, hydrolyzed, amino acid
u Fatu Essential Fatty Acids
u LCT versus MCT
Savino P, NCP 2018;33(1):90-98.Brown B, NCP 2015;30(1):72-85.
8

Composition of enteral formulas
u Carbohydrateu FODMAPs (fermentable fiber, oligosaccharides,
disaccharides, monosaccharides, and polyalcohols)u Fiber
u Soluble and Insoluble both arrive to the colon unchanged (not digested and absorbed)
u Insoluble does not dissolve in water and retains water making stools softer
u Prebiotic fiber is soluble and fermented in the colon and include FOS and inulin.
Savino P, NCP 2018;33(1):90-98.Brown B, NCP 2015;30(1):72-85.
9
Tube feeding Administration10
u Continuous infusion (pump)
u Intermittent/Cyclic feedings (pump)
u Bolus/Gavage (syringe)u Gravity Drip – many times forgotten
Martin K, NCP 2017;32(6):712-721

Pump Feedings
u Not as precise as we might assumeu Walker et al in Houston
u Compared actual volume of formula infused (container catching it, not human subjects) to pump rate and volume infused from the pump.
u The variable was hang height.
u They found: The volume deliver was less than what was calculated from the rate and from the volume the pump recorded. The higher the hang height the closer these numbers were, so hang height is a significant factor.
11
Walker NCP 2018;33(1):151-157

Choosing the Best Enteral Regimen12
Escuro AA, NCP, 2016;31(6):709-722/Reimbursement

What is a blenderized tube feeding (BTF)?
u Sometimes referred to as:u Pureed diet through gastrostomy tube (PDGT)
u Homemade tube feeding (HMTF)
u Real foods/Whole foods
u Home prepared foods are liquefied in a blender and given through a g-tube
u BTF can replace some of the feedings or all of the feedings
u Can be made using a commercial product as part of the recipe
u Some recipes use baby foods for increased consistency and eliminating the need for a high quality blender.
13
Martin NCP 2017;32(6):712-721.Vermilyea NCP 2016;31(1):59-67.
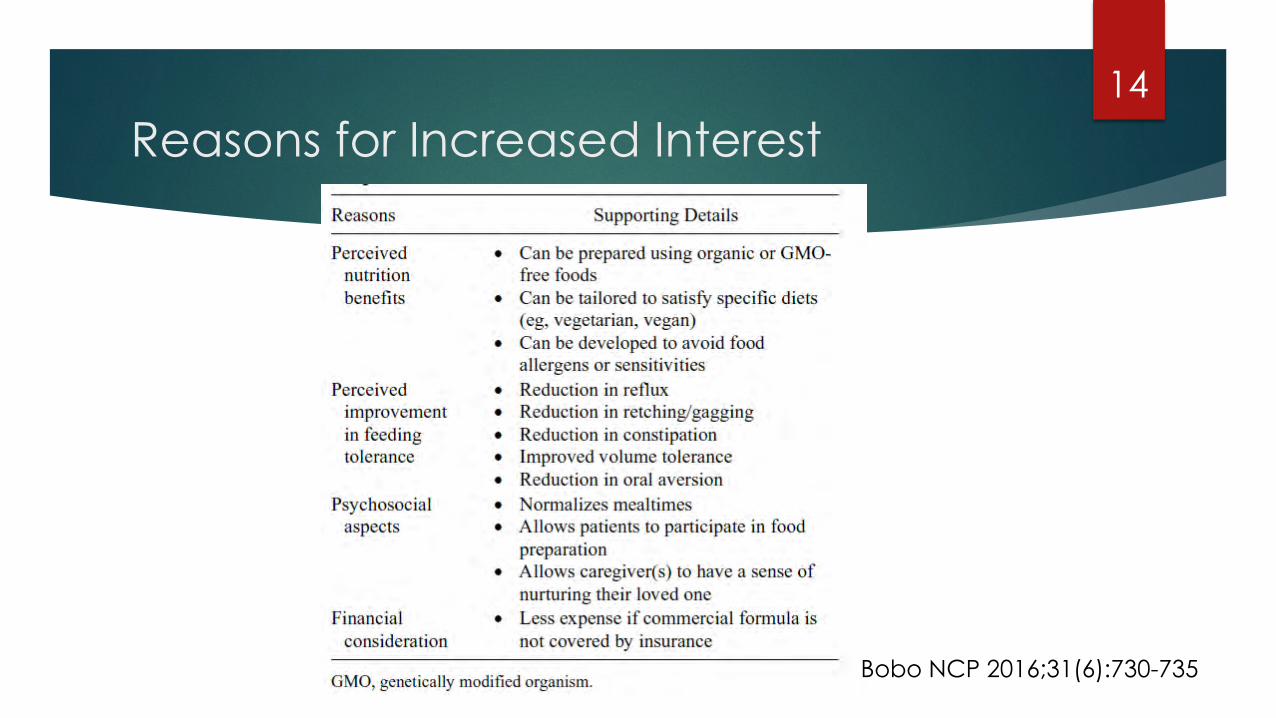
Reasons for Increased Interest14
Bobo NCP 2016;31(6):730-735

Why do Patients choose BTF?
u More naturalu Like eating what the family is eatingu Makes them feel normalu Better toleranceu Don’t like the ingredients in the commercial productsu Food allergies
Hurt RT et al, NCP, 2015;30(6):824-829.
15

Risks
u Microbial contaminationu Unbalanced nutrition/malnutrition – too much or too
littleu Tube clogging and increased wear on tubing
u What do the Enteral Nutrition Practice Recommendations say?u Suggest commercial products
u BTF requires additional attention to safe food handling and storage
Campbell, NCP, 2006; Hurt RT, NCP 2013; Bankhead R et al, JPEN, 2013
16

Who is appropriate for BTF?
u Medically stable on an enteral regimen at home
u Syringe, Bolus feedings or feedings with hang time less than 2 hours
u >10 French tube size (usually 14 French)
u Gastric feedings
u Appropriate growth or clearly able to meet needs with the diet
u Caregivers have a good working relationship with healthcare professionals, esp. a dietitian Bobo NCP 2016;31(6):730-735.
Vermilyea NCP 2016;31(1):59-67.Escuro NCP 2016;31(6):709-722.Brown NCP 2015;30(1):72-85.
17
u Motivated parents/caregivers
u Refrigerator, electricity, blender
u Volume tolerance
u Access to clean water and food
u > 8 months of age
u Able to meet fluid needs with flushes

Contraindications to BTF
u Less than 6 months of age
u Gastrostomy tube smaller than 10 French
u Jejuenostomy tube (or g-j-tube)
u Requires continuous feedings
u Immunocompromised
u Lack of resources/motivation/skills
u Significant malabsorption issues
18

Considerations
u Food borne illness (home versus hospital)u Safe preparation is crucial
u Nutrient variability
u Inconsistency in recipes/food quality
u Requires high level of commitment from the caregiver
u Higher viscosity (increased risk for tube occlusion)
u Increased osmolalityu Could contribute to adverse GI symptoms. (more research needed)
19
Vermilyea NCP 2016;31(1):59-67.Brown NCP 2015;30(1):72-85.

Potential Benefits
u Psycho-social needs metu Caregiver feels in control and food is nurturing
u Can participate in preparation of family meals
u “Eating” the same meal as everyone else
u Decreased reflux symptoms
u Decreased reports of constipation
u Provides phytochemicals and fibers not found in commercial products
u Improved retching and gagging with fundoplication
u May promote oral intake
20
There are no randomized controlled studies comparing BTF to formulas.

BTF
u Required 50% more calories on the BTF to maintain BMI
u BTF micronutrient was superior
u Significant decrease in vomiting and use of acid-suppressive agents
u Stool consistency and frequency was unchanged but stool softener increased
u Caregivers were more satisfied and would recommend it
21
Gallager NCP 2018;42(6):1046-1060.
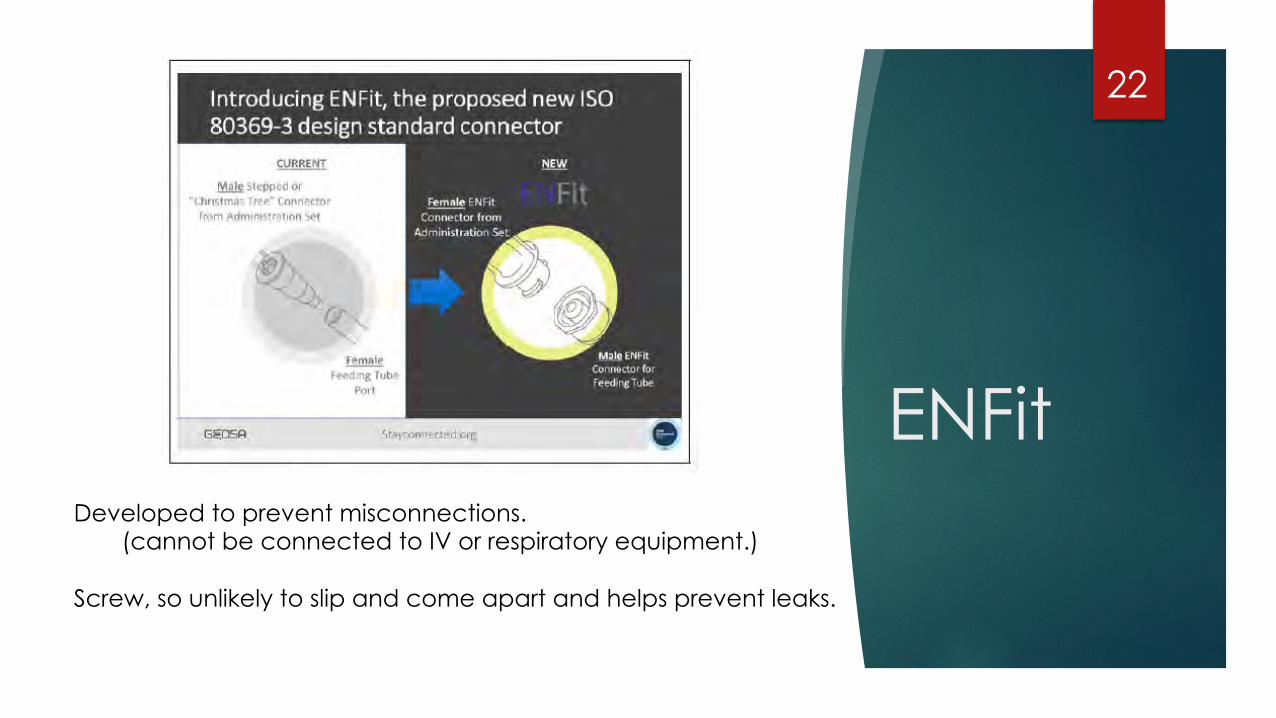
ENFit
22
Developed to prevent misconnections.(cannot be connected to IV or respiratory equipment.)
Screw, so unlikely to slip and come apart and helps prevent leaks.
ENFit - Challenges
u It is a small bore connector.
u Medication administration.
u Bacterial contamination – attention to cleaning.
u Blenderized Tube Feedingu Mundi and colleagues found that formula, size of tube, blender used,
and time of blending had more impact on the force needed to push the feeding through the tube than the connector used.
23
Guenter NCP 2016;31(6):769-772.Lord NCP 2018;33(1):16-38.Mundi JPEN 2018 – online first

The OutsDIARRHEACONSTIPATIONGASTRIC RESIDUALSREFLUX
24
Diarrhea
u Usually defined based on stool frequency and consistency, but no standard definition.
u It can cause:
u Electrolyte abnormalities
u Pressure sores
u Malnutrition (increased frequency of holding feedings)
25
Majid NCP 2012;27(2):252-260.

Diarrhea - Evaluation
u Protocols are helpful.
u What type of diarrhea?u Motility, inflammatory, malabsorption, osmotic, secretory
u Recent changes in regimens?u Medications (sorbitol, antibiotics, antacids, laxatives, H2 blockers, stool softeners)
u Formula Composition
u Fiber – prebiotic fiber (FOS)
u Bacterial Contamination
26
Majid NCP 2012;27(2):252-260.Savino NCP 2018;33(1):90-98.

Constipation
u More frequent than diarrhea.u Associated with increased ICU stay, feeding
intolerance, and difficulty weaning from the vent.u Causes include:
u Medications (H2 Blockers)u Dehydrationu Decreased motility
27
Bittencourt NCP 2012;27(4):533-39.

Constipation - Fiber
u Soluble fibers reduce gastric emptying and are associated with decreasing cholesterol and triglyceride levels.
u Insoluble fiber:
u Increase fecal mass
u Promote optimal intestinal functioning/transit
u Prevent/decrease constipation
u Reduce laxative use
28
Bittencourt NCP 2012;27(4):533-39.

Gastric Residuals
u Time consumingu Increase risk of clogging the tubeu Increase risk of contaminating the feedingsu Electrolyte imbalances if not replacedu May result in holding feedings unnecessarily negatively
impacting nutrition status.
29
Lord NCP 2018;33(1):16-38.
What amount of residuals is significant?

Gastroesophageal Reflux
u Increased LES relaxationsu Increased intra-abdominal pressure u Delayed gastric emptying u Increased gastric acid secretion u Overeating/overfeeding –
ubolus too large/infused too fast
30
Summary
u Enteral formulas are safe and provide adequate nutrition but as professionals and consumers need to be aware of differences in each understanding that marketing can be misleading.
u BTF is a viable option for many home enteral nutrition recipients, but it is not appropriate for everyone and needs close monitoring by a registered dietitian and team.
u Enfit was developed to improve patient safety, yet we need to evaluate challenges associated with this change.
u Intolerances can happen and can be related to formula or may be secondary to many things.
31

References
u Hurt RT et al. Blenderized tube feeding use in adult home enteral nutrition patients: A cross-sectional study. NCP. 2015;30(6):824-829.
u Escuro AA, Hummell AC. Enteral Formulas in Nutrition Support Practice: Is there a better choice for you patient? NCP. 2016;31(6):709-722.
u Martin K, Gardner G. Home Enteral Nutrition: Updates, Trends and Challenges. NCP. 2017;32(6):712-721.
u Walker R et al. Hang height of enteral nutrition influences the delivery of enteral nutrition. NCP. 2017;33(1):151-157.
u Vermilyea S, Goh VL. Enteral feedings in children: Sorting out tubes, buttons, and formulas. NCP. 2016;31(1):59-67.
u Bobo E. Reemergence of blenderized tube feedings: Exploring the evidence. NCP. 2016;31(6):730-735.
32

References
u Gallagher K et al. Blenderized enteral nutrition diet study: feasibility, clinical, and microbiome outcomes of providing, blenderized feeds through a gastric tube in a medically complex pediatric population. NCP. 2018;42(6):1046-1060.
u Pentiuk SP, et al. Pureed by gastrostomy tube diet improves gagging and retching in children with fundoplication. JPEN. 2011;35:375-379.
u O’Flaherty T. Use of a pureed by gastrostomy tube (PBGT) diet to promote oral intake: review and case study. Support Line. 2015;37:21-23.
u Novak P et al. The use of blenderized tube feedings. ICAN. 2009;1(1):21-23.
u O’Flaherty et al. Calculating and preparing a pureed-by-gastrostomy-tube (PBGT) diet for pediatric patients with retching and gagging postfundoplication. ICAN. 2011;3(6):361-364.
33

References
u Lord LM. External access devices: types, function, care, and challenges. NCP 2018;33(1):16-38.
u Savino P. Knowledge of constituent ingredients in enteral nutrition formulas can make a difference in patient response to enteral feeding. NCP 2018;33(1):90-98.
u Bittencourt AF, Martins JR, Logullo L et al. Constipation is more frewuent than diarrhea in patients fed exclusively by enteral nutrition: results of an observational study. NCP 2012;27(4):533-539.
u Guenter P, Lyman B. ENFit enteral nutrition connectors: benefits and challenges. NCP 2016;31(6):769-772.
u Majid HA, Emery PW, Whelan K. Definitions, attitudes, and management practices in relation to diarrhea during enteral nutrition: A survey of patients, nurses and dietitians. NCP 2012;27(2):252-260.
34