the “functional remission of general schizophrenia” (frogs) scale: development and validation of...
TRANSCRIPT

Schizophrenia Research 113 (2009) 218–225
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres
The “Functional Remission of General Schizophrenia” (FROGS) scale:Development and validation of a new questionnaire
Pierre-Michel Llorca a, Christophe Lançon b, Sylvie Lancrenon c, Franck-Jean Bayle d, Hervé Caci e,Frédéric Rouillon f,g, Philip Gorwood f,g,⁎a Centre Hospitalier Universitaire, Clermont-Ferrand, Franceb CHU Sainte Marguerite, Department of Psychiatry, Marseille, Francec SYLIA-STAT, Bourg-la-Reine, Franced Sainte-Anne Hospital (SHU), Paris V-Descartes University, Paris, Francee CHU de Nice, Pôle Enfants-Adolescents, F-06200 Nice, Francef Sainte-Anne Hospital (CMME), Paris V-Descartes University, Paris, Franceg INSERM U675, Centre of Psychiatry and Neurosciences, Sainte-Anne Hospital, Paris, France
a r t i c l e i n f o
⁎ Corresponding author. CMME, Hopital Sainte-An100, rue de la santé, 75674 Paris Cedex 14, France. Tefax: +33 1 45 65 89 43.
E-mail address: [email protected] (P. G
0920-9964/$ – see front matter © 2009 Elsevier B.V.doi:10.1016/j.schres.2009.04.029
a b s t r a c t
Article history:Received 30 January 2009Received in revised form 27 April 2009Accepted 30 April 2009Available online 23 May 2009
Functional remission is an important treatment goal in schizophrenia, as independent livingand reintegration of patients into the community and the workplace is the ultimate goal of anytreatment. Nevertheless, assessing functional remission in schizophrenia is problematic, as itis a multifactorial and complex entity reflecting various aspects such as symptoms severity,personal skills and socio-cultural expectancies.The purpose of this study was to create and validate a novel scale for the evaluation offunctional remission in schizophrenia. Unlike previous scales, the scale was built on the basisof patients with few schizophrenia symptoms. The “Functional Remission of GeneralSchizophrenia” (FROGS) scale was developed using the expert consensus method following aMEDLINE and standard database search. Out of the 61 initially proposed, 19 items wereselected as gathering the core aspects of functional remission in schizophrenia detected inthe literature. The FROGS was then evaluated in 432 patients with DSM-IV criteria ofschizophrenia, all of them meeting the symptomatic remission criteria of Andreasen et al.[Andreasen, N.C., Carpenter, W.T., Kane, J.M., Lasser, R.A., Marder, S.R., Weinberger, D.R.,2005. Remission in schizophrenia: proposed criteria and rationale for consensus. Am.J. Psychiatry 162 441–449]. Total score was highly reliable. Exploratory factor analysis afteroblique rotation revealed that a three-factor solution was the most meaningful. On the basisof item content these three factors were labelled ‘Social Functioning,’ ‘Daily Life’ and‘Treatment.’ The FROGS total score can be used to measure a general construct for theevaluation of functional remission in schizophrenia.. Further work is required to measurethe acceptability, predictive validity, sensitivity to change, and stability of the factorstructure of the FROGS.
© 2009 Elsevier B.V. All rights reserved.
Keywords:FROGSEvaluationFunctional remissionMulticenter studySchizophreniaSocial functioningRecovery
ne (Paris Descartes),l.: +33 1 45 65 83 67;
orwood).
All rights reserved.
1. Introduction
Schizophrenia is a heterogeneous disease with a variableclinical course and outcome (Bromet and Fennig, 1999).Evolution of antipsychotic medication, psychosocial and voca-tional therapies over the past 10 years, and greater involvementof patients and their relatives in themanagementof the disease,

219P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
have led to more effective control of psychotic symptoms, withthe result that remission and recovery are now attainablegoals in a significant proportion of patients with schizophrenia(Andreasen et al., 2005; Kissling et al., 2005; Lasser et al., 2005,2007).
In 2005, the Remission in Schizophrenia Working Grouppublished the report of a consensus-standardised definitionof remission in schizophrenia (Positive and Negative Symp-toms Scale; PANSS) (Andreasen et al., 2005). The proposeddefinition of remission (low level of severity of 8 core symp-toms during at least 6 months) is in line with the conceptsof remission and recovery described for other psychiatricillnesses such as mood (Bakish, 2001; Frank et al., 1991;Keller, 2003) and anxiety (Ballenger, 2001; Sheehan, 2001)disorders.
Overall functioning and well being of a patient are usuallyconsidered as critical parameters to evaluate remission ofsymptoms, but should be distinguished (Fleischhacker et al.,2005) as symptomatic remission is not always accompaniedby improved social functioning (Mueser, 2000).
Schizophrenic patients with low functional competencerepresent a significant burden to their family and to societysince they are usually dependent on family members orassisted-living facilities for their daily care and are poorlyintegrated into the community. Achieving functional remis-sion is an important treatment goal allowing the reintegrationof patients into the community and the workplace, andreducing the social burden and health-care costs (Helldinet al., 2007). More relevant definitions of functional remissionand recovery in schizophrenia should be based on functionaloutcomes such as social functioning or work abilities. Asan outcome goal, functional remission should be attainable,easy to measure and should define an evolutionwhich can beperceived as important and positive by patients and theirfamilies.
The concept of social functioning is nevertheless com-plex. It is essentially composed of the ability of a patient totake care of himself andmaintain daily activities, and requireinstrumental and social skills in order to manage in thecommunity.
A number of scales measuring social and independentfunctioning have been developed; as underlined by Brekke(1992), the different independent functioning scales can beclassified into two main categories: multidimensional, thatcapture several aspects of functioning and global, thatincorporate symptoms and role functioning into a singlemeasure.
In the first category, the Multidimensional Scale forIndependent Functioning (MSIF; Jaeger et al., 2003) wasdesigned to elicit and appropriately discriminate thedimensions of role responsibility, support and perfor-mance within work, education ad residential domains. Itcan be considered as a useful tool for research that can beused in different illnesses (e.g. bipolar disorder, Berns et al.,2007).
In the second category, the Personal and Social Perfor-mance Scale (PSP) (Morosini et al., 2000) was developed onthe basis of the social functioning component of the DSMIV, assessing patient's functioning in four main areas(socially useful activities, personal and social relationships,self-care and disturbing and aggressive behaviours) to
obtain a single score. This scale and others are generallypsychometrically sound (Schedule for the Assessment ofPsychiatric Disability (SAPD), Thara et al., 1988; GroningenSocial Disabilities Schedule (GSDS II), Wiersma et al., 1988;Life Skills Profile (LSP), Rosen et al., 1989; Social Function-ing Scale (SFS), Birchwood et al., 1990; MultinomahCommunity Ability Scale (MCAS), Barker et al., 1994;SCARF Social Functioning Index (SF1), Padmavati et al.,1995; Social-Adaptive Functioning Evaluation (SAFE), Har-vey et al., 1997; Independent Living Scale (ILSS), Wallaceet al., 2000; and Disability Assessment Schedule (DAS-II),WHO, 2000), but have a number of limitations. Amongthem, one could quote (1) imprecise terminology (mild,moderate…), (2) the absence of behavioural anchor points,(3) the lack of objective description of the degree ofimpairment, and (4) the inclusion of items that in factreflect clinical symptoms (Dickerson et al., 1996; Wallaceet al., 2000). The different domains that have to beevaluated, and their definitions, may also be discussed(Saraswat et al., 2006).
We set out to design a specific and simple scale for themeasurement of functional remission in schizophrenia,which would be suitable for use in clinical outcomestudies and patient evaluations. The FROGS (FunctionalRemission of General Schizophrenia) scale attempts toovercome the limitations of earlier scales in developingprecise definition of the different domains, with no itemevaluating symptoms. The present report includes twoparts: (1) the development of the scale, especially itemsgeneration and selection, and (2) the statistical validationof the FROGS in a sample of schizophrenic patientsfulfilling the criteria for symptomatic remission of Andrea-sen et al. (2005). This criterion was chosen as functionalremission is expected to be an important goal, especiallyin patients who already reached the symptomatic remis-sion level.
2. Development of the FROGS
2.1. Item generation and selection
The FROGS was developed using the expert consensusmethod (Delphi method) (Helmer, 1983). The panel of ex-perts was involved in criteria selection and design of theFROGS (and is listed in the Acknowledgment section).
Three stages were needed: (1) selection of functionaldimensions in the literature; (2) generation of relevant itemsreflecting the different domains; and (3) construction of thescale to measure functional aspects of remission.
In the first stage, the FROGS was constructed with ref-erence to a model of functional remission. Five domains thathave to be evaluated were proposed: ‘Daily Life,’ ‘Activities,’‘Quality of Adaptation,’ ‘Relationships’ and ‘Health and Treat-ment,’ as gathering the maximum of various items alreadyused in the literature.
The second stage involved a PubMed® and standarddatabase search for relevant articles on remission andmethods of measuring remission using key search para-meters ‘psychosis/schizophrenia’ and ‘social functioning,’‘disability,’ ‘relationships,’ ‘social activity,’ ‘rehabilitation’and ‘quality of life.’
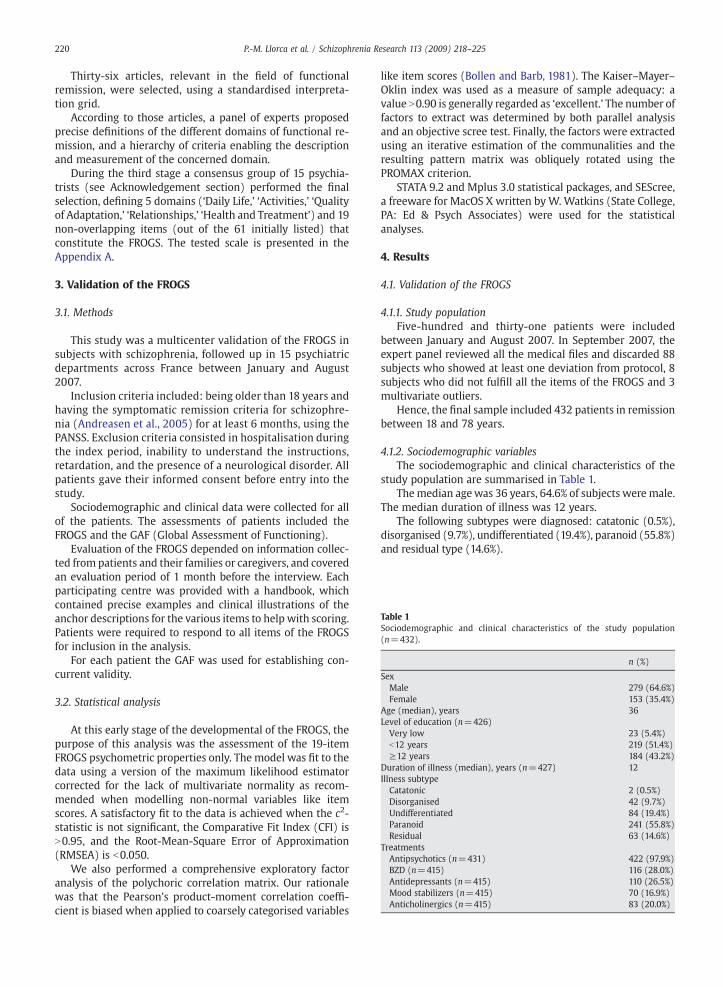
Table 1Sociodemographic and clinical characteristics of the study population(n=432).
n (%)
SexMale 279 (64.6%)Female 153 (35.4%)
Age (median), years 36Level of education (n=426)Very low 23 (5.4%)b12 years 219 (51.4%)≥12 years 184 (43.2%)
Duration of illness (median), years (n=427) 12Illness subtypeCatatonic 2 (0.5%)Disorganised 42 (9.7%)Undifferentiated 84 (19.4%)Paranoid 241 (55.8%)Residual 63 (14.6%)
TreatmentsAntipsychotics (n=431) 422 (97.9%)BZD (n=415) 116 (28.0%)Antidepressants (n=415) 110 (26.5%)Mood stabilizers (n=415) 70 (16.9%)Anticholinergics (n=415) 83 (20.0%)
220 P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
Thirty-six articles, relevant in the field of functionalremission, were selected, using a standardised interpreta-tion grid.
According to those articles, a panel of experts proposedprecise definitions of the different domains of functional re-mission, and a hierarchy of criteria enabling the descriptionand measurement of the concerned domain.
During the third stage a consensus group of 15 psychia-trists (see Acknowledgement section) performed the finalselection, defining 5 domains (‘Daily Life,’ ‘Activities,’ ‘Qualityof Adaptation,’ ‘Relationships,’ ‘Health and Treatment’) and 19non-overlapping items (out of the 61 initially listed) thatconstitute the FROGS. The tested scale is presented in theAppendix A.
3. Validation of the FROGS
3.1. Methods
This study was a multicenter validation of the FROGS insubjects with schizophrenia, followed up in 15 psychiatricdepartments across France between January and August2007.
Inclusion criteria included: being older than 18 years andhaving the symptomatic remission criteria for schizophre-nia (Andreasen et al., 2005) for at least 6 months, using thePANSS. Exclusion criteria consisted in hospitalisation duringthe index period, inability to understand the instructions,retardation, and the presence of a neurological disorder. Allpatients gave their informed consent before entry into thestudy.
Sociodemographic and clinical data were collected for allof the patients. The assessments of patients included theFROGS and the GAF (Global Assessment of Functioning).
Evaluation of the FROGS depended on information collec-ted from patients and their families or caregivers, and coveredan evaluation period of 1 month before the interview. Eachparticipating centre was provided with a handbook, whichcontained precise examples and clinical illustrations of theanchor descriptions for the various items to help with scoring.Patients were required to respond to all items of the FROGSfor inclusion in the analysis.
For each patient the GAF was used for establishing con-current validity.
3.2. Statistical analysis
At this early stage of the developmental of the FROGS, thepurpose of this analysis was the assessment of the 19-itemFROGS psychometric properties only. The model was fit to thedata using a version of the maximum likelihood estimatorcorrected for the lack of multivariate normality as recom-mended when modelling non-normal variables like itemscores. A satisfactory fit to the data is achieved when the c2-statistic is not significant, the Comparative Fit Index (CFI) isN0.95, and the Root-Mean-Square Error of Approximation(RMSEA) is b0.050.
We also performed a comprehensive exploratory factoranalysis of the polychoric correlation matrix. Our rationalewas that the Pearson's product-moment correlation coeffi-cient is biased when applied to coarsely categorised variables
like item scores (Bollen and Barb, 1981). The Kaiser–Mayer–Oklin index was used as a measure of sample adequacy: avalue N0.90 is generally regarded as ‘excellent.’ The number offactors to extract was determined by both parallel analysisand an objective scree test. Finally, the factors were extractedusing an iterative estimation of the communalities and theresulting pattern matrix was obliquely rotated using thePROMAX criterion.
STATA 9.2 and Mplus 3.0 statistical packages, and SEScree,a freeware for MacOS X written by W. Watkins (State College,PA: Ed & Psych Associates) were used for the statisticalanalyses.
4. Results
4.1. Validation of the FROGS
4.1.1. Study populationFive-hundred and thirty-one patients were included
between January and August 2007. In September 2007, theexpert panel reviewed all the medical files and discarded 88subjects who showed at least one deviation from protocol, 8subjects who did not fulfill all the items of the FROGS and 3multivariate outliers.
Hence, the final sample included 432 patients in remissionbetween 18 and 78 years.
4.1.2. Sociodemographic variablesThe sociodemographic and clinical characteristics of the
study population are summarised in Table 1.Themedian agewas 36 years, 64.6% of subjects were male.
The median duration of illness was 12 years.The following subtypes were diagnosed: catatonic (0.5%),
disorganised (9.7%), undifferentiated (19.4%), paranoid (55.8%)and residual type (14.6%).
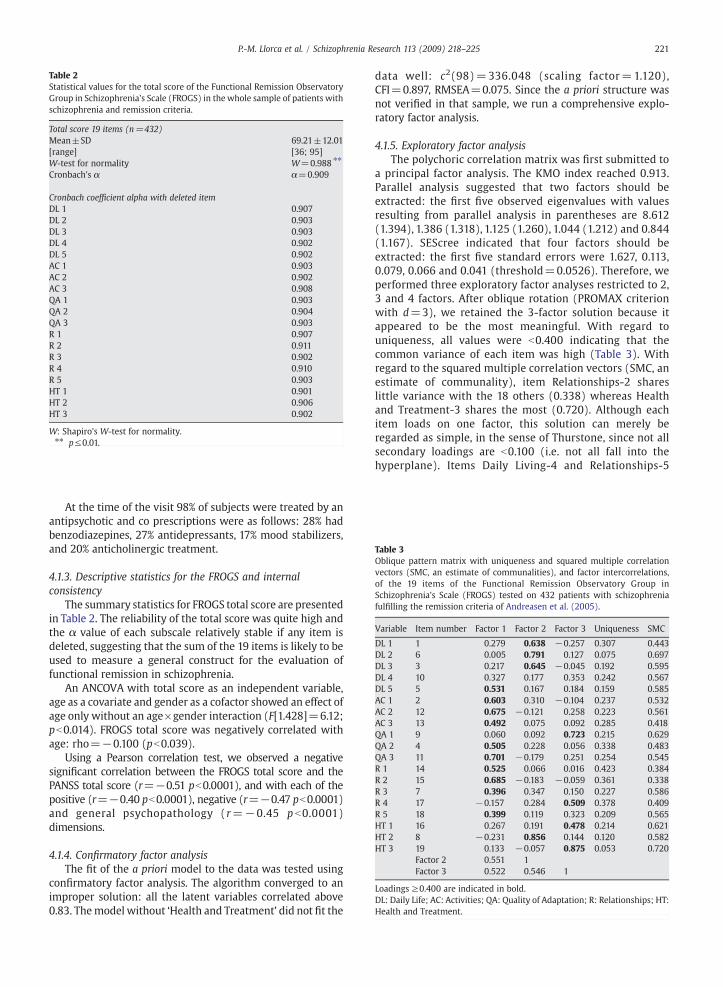
Table 3Oblique pattern matrix with uniqueness and squared multiple correlationvectors (SMC, an estimate of communalities), and factor intercorrelations,of the 19 items of the Functional Remission Observatory Group inSchizophrenia's Scale (FROGS) tested on 432 patients with schizophreniafulfilling the remission criteria of Andreasen et al. (2005).
Variable Item number Factor 1 Factor 2 Factor 3 Uniqueness SMC
DL 1 1 0.279 0.638 −0.257 0.307 0.443DL 2 6 0.005 0.791 0.127 0.075 0.697DL 3 3 0.217 0.645 −0.045 0.192 0.595DL 4 10 0.327 0.177 0.353 0.242 0.567DL 5 5 0.531 0.167 0.184 0.159 0.585AC 1 2 0.603 0.310 −0.104 0.237 0.532AC 2 12 0.675 −0.121 0.258 0.223 0.561AC 3 13 0.492 0.075 0.092 0.285 0.418QA 1 9 0.060 0.092 0.723 0.215 0.629QA 2 4 0.505 0.228 0.056 0.338 0.483QA 3 11 0.701 −0.179 0.251 0.254 0.545R 1 14 0.525 0.066 0.016 0.423 0.384R 2 15 0.685 −0.183 −0.059 0.361 0.338R 3 7 0.396 0.347 0.150 0.227 0.586R 4 17 −0.157 0.284 0.509 0.378 0.409R 5 18 0.399 0.119 0.323 0.209 0.565HT 1 16 0.267 0.191 0.478 0.214 0.621HT 2 8 −0.231 0.856 0.144 0.120 0.582HT 3 19 0.133 −0.057 0.875 0.053 0.720
Factor 2 0.551 1Factor 3 0.522 0.546 1
Loadings ≥0.400 are indicated in bold.DL: Daily Life; AC: Activities; QA: Quality of Adaptation; R: Relationships; HT:Health and Treatment.
Table 2Statistical values for the total score of the Functional Remission ObservatoryGroup in Schizophrenia's Scale (FROGS) in the whole sample of patients withschizophrenia and remission criteria.
Total score 19 items (n=432)Mean±SD 69.21±12.01[range] [36; 95]W-test for normality W=0.988 ⁎⁎
Cronbach's α α=0.909
Cronbach coefficient alpha with deleted itemDL 1 0.907DL 2 0.903DL 3 0.903DL 4 0.902DL 5 0.902AC 1 0.903AC 2 0.902AC 3 0.908QA 1 0.903QA 2 0.904QA 3 0.903R 1 0.907R 2 0.911R 3 0.902R 4 0.910R 5 0.903HT 1 0.901HT 2 0.906HT 3 0.902
W: Shapiro's W-test for normality.⁎⁎ p≤0.01.
221P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
At the time of the visit 98% of subjects were treated by anantipsychotic and co prescriptions were as follows: 28% hadbenzodiazepines, 27% antidepressants, 17% mood stabilizers,and 20% anticholinergic treatment.
4.1.3. Descriptive statistics for the FROGS and internalconsistency
The summary statistics for FROGS total score are presentedin Table 2. The reliability of the total score was quite high andthe α value of each subscale relatively stable if any item isdeleted, suggesting that the sum of the 19 items is likely to beused to measure a general construct for the evaluation offunctional remission in schizophrenia.
An ANCOVA with total score as an independent variable,age as a covariate and gender as a cofactor showed an effect ofage only without an age×gender interaction (F[1.428]=6.12;pb0.014). FROGS total score was negatively correlated withage: rho=−0.100 (pb0.039).
Using a Pearson correlation test, we observed a negativesignificant correlation between the FROGS total score and thePANSS total score (r=−0.51 pb0.0001), and with each of thepositive (r=−0.40 pb0.0001), negative (r=−0.47 pb0.0001)and general psychopathology (r=−0.45 p b0.0001)dimensions.
4.1.4. Confirmatory factor analysisThe fit of the a priori model to the data was tested using
confirmatory factor analysis. The algorithm converged to animproper solution: all the latent variables correlated above0.83. Themodel without ‘Health and Treatment’ did not fit the
data well: c2(98)=336.048 (scaling factor=1.120),CFI=0.897, RMSEA=0.075. Since the a priori structure wasnot verified in that sample, we run a comprehensive explo-ratory factor analysis.
4.1.5. Exploratory factor analysisThe polychoric correlation matrix was first submitted to
a principal factor analysis. The KMO index reached 0.913.Parallel analysis suggested that two factors should beextracted: the first five observed eigenvalues with valuesresulting from parallel analysis in parentheses are 8.612(1.394), 1.386 (1.318), 1.125 (1.260), 1.044 (1.212) and 0.844(1.167). SEScree indicated that four factors should beextracted: the first five standard errors were 1.627, 0.113,0.079, 0.066 and 0.041 (threshold=0.0526). Therefore, weperformed three exploratory factor analyses restricted to 2,3 and 4 factors. After oblique rotation (PROMAX criterionwith d=3), we retained the 3-factor solution because itappeared to be the most meaningful. With regard touniqueness, all values were b0.400 indicating that thecommon variance of each item was high (Table 3). Withregard to the squared multiple correlation vectors (SMC, anestimate of communality), item Relationships-2 shareslittle variance with the 18 others (0.338) whereas Healthand Treatment-3 shares the most (0.720). Although eachitem loads on one factor, this solution can merely beregarded as simple, in the sense of Thurstone, since not allsecondary loadings are b0.100 (i.e. not all fall into thehyperplane). Items Daily Living-4 and Relationships-5

Table 4Oblique 3-factor solution (Cronbach's α).
Factor 1: 10 items(n=432)
Factor 2: 4 items(n=432)
Factor 3: 4 items(n=432)
Mean±SD 33.63±6.91 Mean±SD 16.22±2.77 Mean±SD 15.86±3.10[range] [14; 50] [range] [7; 20] [range] [6; 20]W-test W=0.993 ⁎ W-test W=0.947 ⁎⁎⁎ W-test W=0.946 ⁎⁎⁎Cronbach's α α=0.847 Cronbach's α α=0.764 Cronbach's α α=0.772
Cronbach coefficient alpha with deleted itemDL 5 0.826 DL 1 0.753 QA 1 0.679AC 1 0.827 DL 2 0.646 R 4 0.824AC 2 0.824 DL 3 0.698 HT 1 0.697AC 3 0.846 HT 2 0.725 HT 3 0.652QA 2 0.832QA 3 0.827R 1 0.837R 2 0.850R 3 0.828R 5 0.830
W: Shapiro's W-test for normality.Factor 1: Social Functioning (10 items): travel and communication (DL 5), personal activities (AC 1), social activities (AC 2), studying or work (AC 3), adaptation to stress and unforeseen circumstances(QA 2), self-esteem and sense of independence (QA 3), family, friends (R 1), love and sexual life (R 2), social network (R 3) and empathy and help for others (R 5).Factor 2: Daily life (4 items): personal care and appearance (DL 1), diet (DL 2), housekeeping (DL 3) and respect for biological rhythms (HT 2).Factor 3: Treatment (4 items):management of his illness and treatment (QA 1), absence of antisocial or violent behaviour (R 4), taking charge of personal health (HT 1) and functional impact ofthe secondary effects of treatment (HT 3).⁎ p≤0.05.⁎⁎⁎ p≤0.001.
222 P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
cross-load on factors 1 and 3, but under the arbitrarythreshold of 0.400.
On the basis of item content, the factors were labelled“Social Functioning,” “Daily Life” and “Treatment,” respec-tively (Table 4). They correlated above 0.50 indicating thatthey are not identical but share enough common variance tomake the hypothesis of a higher order factor viable.
In the factor treatment, the deletion of the “relationship”item 4 (absence of antisocial or violent behaviour) is associatedwith an increase of the α; despite the fact that antisocial andviolent behaviour have an effect on relationship, this mayindicate that this item explores another aspect of schizo-phrenia, for example being closer to symptomatology ratherthan functionality.
4.2. Concurrent validity
Using a Pearson correlation test, we observed a significantcorrelation between the GAF score and the total score of theFROGS (r=0.561, p=b .0001).
5. Discussion
The FROGS was designed and validated to measure sometheoretically sound components of functional remission inschizophrenia based on a comprehensive review of the lite-rature and expert consensus, and was then assessed in asample of more than 400 schizophrenic patients with symp-tomatic remission.
According to the inclusion criteria, the homogeneity of ourpatient sample, in terms of symptomatology (and especiallyremission), is a specific feature of our study, compared tovarious studies designed for the validation of other scales(Morosini et al., 2000, Jaeger et al., 2003, Saraswat et al.,2006).
The statistically significant correlation between the totalscore of the FROGS and the GAF in our sample confirms thefact that the new scale that we have developed is indeedassessing functioning in schizophrenic patients.
Validation of the FROGS in the 432 patients in PANSSremission from schizophrenia failed to confirm the a priori5-domain model although the FROGS total score was validand can be used to measure a general construct. Compre-hensive exploratory factor analysis resulted in the extractionof three factors that could be labelled on the basis of itemcontent: ‘Social Functioning,’ ‘Daily Life’ and ‘Treatment.’These factors are not identical but share enough commonvariance to make the hypothesis of a higher order factorviable.
The present results are similar to another recent reportdescribing the development of the Social OccupationalFunctioning Scale (Saraswat et al., 2006) for functionalremission. In this study, exploratory factor analysis alsorevealed a three-factor structure supporting the constructvalidity of the scale, namely ‘Adaptive Living Skills’ (includingactivities of daily living, instrumental living skills and workfunctioning), ‘Social Appropriateness’ (reflecting self-presen-tation) and ‘Interpersonal Skills’ (including communication

223P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
and interpersonal interaction As with our scale, the authorsconcluded that the SOFS total score was sufficient for clinicaluse.
The PSP was developed on the basis of the social func-tioning component of the DSM IV (Social and OccupationalFunctioning Assessment Scale) (Morosini et al., 2000). It iseasy to use as the rating instructions are rather simple andthe different areas to be evaluated are clearly specified.The four main areas explore: (a) socially useful activities(including work and studies); (b) personal and socialrelationships; (c) self-care; and (d) disturbing andaggressive behaviours. The three areas (a, b and c) areclose to the domains that we defined after comprehensiveexploratory factor analysis (respectively ‘Social Function-ing,’ ‘Daily Life’ and ‘Treatment’). It therefore confirms theclinical relevancy of the 3 dimensions we extracted.Nevertheless, the PSP still includes an evaluation ofsymptoms (and especially of unacceptable behaviourwith domain d) and their impact on functioning. Com-pared to PSP, the FROGS is the latter avoids an evaluationof symptoms and focuses on the different domains ofinterest, specifically in terms of functionality. The distinc-tion between symptomatology and functionality is alsoone of the purposes of the MSIF (Jaeger et al., 2003). Theauthors have chosen the areas work, education andresidential, and each of these domains is evaluated interms of role position, support and performance. Theabsence of evaluation of self-care is a choice that can bediscussed for schizophrenic patients. We may considerthat the MSIF evaluate “functioning” in a more global way,with less specificity for schizophrenia compared to theFROGS.
The FROGS gives a new assessment of social functioning,has the advantage of incorporating several accuratelydescribed domains and being organised excluding psycho-pathological symptoms. The three domains identified byexploratory factor analysis are clinically pertinent, concern-ing major elements of an independent life in a normalenvironment outside hospital. The quality of disease man-agement by the patient constitutes a crucial element forlong-term prognosis reinforcing the possibility to assess thisdimension in a scale devoted to functional remission inschizophrenia.
Descriptive analysis of each item, inter-item correlationmatrix and stability of Cronbach's α after removal of eachitem indicate that the 19 items should be kept. Never-theless, the factorial analysis was in favour of a differentstructure (with 3 instead of 5 domains) and showed thatone item is not specific of any of these three dimensions. Atthis stage of the developmental of the FROGS, we thoughtthat it might be premature to decide to exclude an item, asit is difficult to state if this item is having poor clarity (notwell understood, defined and/or described) versus poorvalidity (assessing a dimension not linked to functionalaspects of schizophrenia).
Following this preliminary study, it is now hoped toinvestigate the inter-rater reliability of the scale, the accept-ability and stability of the factorial structure of the FROGS, andits sensitivity to change.
More analyses may also give information on therelevance of items such as “absence of antisocial and violent
behaviour” in the evaluation of functional remission inschizophrenia.
When those different psychometric properties of theFROGS will be well defined, such a tool will be useful toexplore the complex relation between symptoms and func-tionality. The specificity of the effect of the main clinicaldimensions of schizophrenia (i.e. positive, negative anddisorganization) on functionality also remains to be described.We will need to use the FROGS in a population of non-re-mitters to explore this aspect. Correlations between thedifferent factors of the PANSS (e.g. the five factors solutiondescribed by Lançon et al., 1998) and the 3 factors weidentified have also to be explored.
The relationship between functional remission, as definedwith our scale, and elements such as quality of life should alsobe investigated since there is a considerable overlap betweenthese two concepts.
In conclusion, the first operational consensus definition ofremission in schizophrenia based on symptomatic remissionwas published in 2005 (Andreasen et al., 2005), facilitatingthe evaluation of new treatment strategies. However, func-tional aspects of recovery such as improvement in cognitionand social functioning are also important when evaluatingremission and recovery. Our scale may be a step towardsdeveloping a consensual international definition of functionalremission in schizophrenia.
Role of funding sourceNone.
ContributorsPierre-Michel LLORCA contributed as a clinical investigator, as the
coordinator of the analyses.Christophe LANÇON contributed as a clinical investigator, and as the
coordinator of the medline review.Sylvie LANCERNON was responsible for the statistical analyses.Franck-Jean BAYLE contributed as a clinical investigator.Hervé CACI was in charge of the principal component analyses.Frédéric ROUILLON supervised the activity of the expertise group and
corrected the manuscript.Philip GORWOOD contributed as a clinical investigator, participated in
the analyses and organised the submission of the final manuscript.
Conflict of interestConsultancies, honoraria, paid expertise and grants were obtained by
authors (detailed list below), with no stock ownership, nor patent applica-tions, neither registrations.
PM Llorca (Bristol Myers-Squibb, Eli Lilly, Janssen & Janssen, Lundbeck,Servier, UCB-Pharma and Wyeth), C Lançon (Eli Lilly, Janssen & Janssenand Servier), S Lancrenon (Janssen & Janssen), F Baylé (Bristol-Myers-Squibb, Eli Lilly, Janssen & Janssen, Lundbeck, Servier, UCB-Pharma), HervéCaci (Janssen & Janssen), F Rouillon (Myers-Squibb, Eli Lilly, Janssen &Janssen, Lundbeck, Servier, UCB-Pharma and Wyeth) and P Gorwood(Myers-Squibb, Eli Lilly, Janssen & Janssen, Lundbeck, Servier, UCB-Pharma).
Acknowledgments
The authors express their gratitude to their colleagues who were deeplyinvolved in the literature review, the proposition of items and the recruitmentof patients: Alain Bottéro (Paris); Olivier Canceil (Paris); François-RégisCousin (St Germain en Laye); Michel Maron (Lille); Annie Navarre-Coulard(Dieppe); Jérôme Palazzolo (Nice); Marie-Noëlle Vacheron (Paris); GillesVidon (Saint-Maurice).
The study was performed with financial support from Janssen-Cilag, andconcerned the training of clinicians, and the organization of the meetings.The interpretation of data and the writing of the manuscript were madeindependently by the authors.

Appendix A. Instrument for the evaluation of “Functional Remission in General Schizophrenia” (FROGS) (guidelines available onrequest)
224 P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
References
Andreasen, N.C., Carpenter, W.T., Kane, J.M., Lasser, R.A., Marder, S.R.,Weinberger, D.R., 2005. Remission in schizophrenia: proposed criteria
and rationale for consensus. Am. J. Psychiatry 162, 441–449.Bakish, D., 2001. New standard of depression treatment: remission and fullrecovery. J. Clin. Psychiatry 62 (suppl. 26), 5–9.
Ballenger, J.C., 2001. Treatment of anxiety disorders to remission. J. Clin.Psychiatry 62 (suppl. 1), 5–9.
Barker, S., Barron, N., McFarlane, B.H., Bigelow, D.A., 1994. A communityability scale for chronically mentally ill consumers: 1. Reliability andvalidity. Community Ment. Health J. 30, 363–379.
Berns, S., Uzelac, S., Gonzalez, C., Jaeger, J., 2007. Methodological considerationsofmeasuring disability in bipolar disorder: validity of theMultidimensionalScale of Independent Functioning. Bipolar Disord. 9 (1–2), 3–10.
Birchwood, M., Smith, J., Cochrane, R., Wetton, S., Copestake, S., 1990. TheSocial Functioning Scale: the development and validation of a new scaleof social adjustment for use in family intervention programmes withschizophrenic patients. Br. J. Psychiatry 157, 853–859.
Bollen, K.A., Barb, K.H., 1981. Pearson's r and coarsely categorized measures.Am. Soc. Rev. 46, 232–239.
Brekke, J.S., 1992. An examination of the relationships among three outcomescales in schizophrenia. J. Nerv. Ment. Dis. 180 (3), 162–167.
Bromet, E.J., Fennig, S., 1999. Epidemiology and natural history of schizo-phrenia. Biol Psychiatry 46 (7), 869–870.
Dickerson, F., Boronow, J.J., Ringel, N., Parente, F.,1996. Neurocognitive deficits andsocial functioning in outpatients with schizophrenia. Schizophr. Res. 21 (2),75–83.
Fleischhacker, W.W., Rabinowitz, J., Kemmler, G., Eerdekens, M., Mehnert, A.,2005. Perceived functioning, well-being and psychiatric symptoms inpatients with stable schizophrenia treated with long-acting risperidonefor 1 year. Br. J. Psychiatry 187, 131–136.
Frank, E., Prien, R.F., Jarrett, R.B., Keller,M.B., Kupfer, D.J., Lavori, P.W., Rush, A.J.,Wesiman, M.M., 1991. Conceptualisation and rationale for consensusdefinition of terms in major depressive disorder. Remission, recovery,relapse and recurrence. Arch. Gen. Psychiatry 48, 851–855.
Harvey, P.D., Davidson, M., Mueser, K.T., Parrella, M., White, L., Powchik, P.,1997. Social-Adaptive Functioning Evaluation (SAFE): a rating scale forgeriatric psychiatric patients. Schizophr. Bull. 23, 131–145.
Helldin, L., Kane, J.M., Karilampi, U., Norlander, T., Archer, T., 2007. Remissionin prognosis of functional outcome: a new dimension in the treatment ofpatients with psychotic disorders. Schizophr. Res. 93 (1–3),160–168.
Helmer, O.,1983. Looking Forward: AGuide to Future Research. InSage, BeverleyHills, CA, p. 376.
Jaeger, J., Berns, S.M., Czobor, P., 2003. The multidimensional scale ofindependent functioning: a new instrument for measuring functionaldisability in psychiatric populations. Schizophr. Bull. 29 (1), 153–168.

225P.-M. Llorca et al. / Schizophrenia Research 113 (2009) 218–225
Keller, M.B., 2003. Past, present, and future directions for defining optimaltreatment outcome in depression: remission and beyond. JAMA 289 (23),3152–3160.
Kissling,W.,Heres, S., Lloyd, K., Sacchetti, E., Bouhours, P.,Medori, R., Llorca, P.M.,2005. Direct transition to long-acting risperidone — analysis of long-termefficacy. J. Psychopharmacol. 19 (suppl. 5), 15–21.
Lançon, C., Aghababian, V., Llorca, P.M., Auquier, P., 1998. Factorial structure ofthe Positive and Negative Syndrome Scale (PANSS): a forced five-dimensional factor analysis. Acta Psychiatr. Scand. 98 (5), 369–376 Nov.
Lasser, R.A., Bossie, C.A., Gharabawi, G.M., Kane, J.M., 2005. Remission inschizophrenia: results from a 1-year study of long-acting risperidoneinjection. Schizophr. Res. 77 (2–3), 215–227.
Lasser, R.A., Nasrallah, H., Helldin, L., Peuskens, J., Kane, J., Docherty, J., Tronco,A.T., 2007. Remission in schizophrenia: applying recent consensuscriteria to refine the concept. Schizophr. Res. 96 (1–3), 223–231.
Morosini, P.L., Magliano, L., Brambilla, L., Ugolini, S., Pioli, R., 2007.Development, reliability and acceptability of a new version of theDSM-IV Social and Occupational Functioning Assessment Scale (SOFAS)to assess routine social functioning. Acta Psychiatr. Scand. 101 (4), 323–329.
Mueser, K.T., 2000. Cognitive functioning, social adjustment and long termoutcome in schizophrenia. In: Sharma, T., Harvey, P. (Eds.), Cognition inSchizophrenia: Impairments, Importance and Treatment Strategies.InOxford University Press, New York, pp. 157–177.
Padmavati, R., Thara, R., Srinivasan, L., Kumar, S., 1995. SCARF SocialFunctioning Index. Indian J. Psychiatry 37 (4), 161–164.
Rosen, A., Hadzi-Pavlovic, D., Parker, G., 1989. The Life Skills Profile: ameasureassessing function and disability in schizophrenia. Schizophr. Bull. 15,325–337.
Saraswat, N., Rao, K., Subbakrishna, D.K., Gangadhar, B.N., 2006. The SocialOccupational Functioning Scale (SOFS): a brief measure of functionalstatus in persons with schizophrenia. Schizophr. Res. 81, 301–309.
Sheehan, D.V., 2001. Defining remission in generalized anxiety disorder:venlafaxine extended release comparative data. J. Clin. Psychiatry 62(19), 26–31.
Thara, R., Rajkumar, S., Valecha, V., 1988. The schedule for the assessment ofpsychiatric disability. Indian J. Psychiatry 30 (1), 47–53.
Wallace, C.J., Liberman, R.P., Tauber, R.,Wallace, J., 2000. The independent LivingSkills Survey: a comprehensive measure of the community functioningof severely and persistently mentally ill individuals. Schizophr. Bull. 26,631–658.
Wiersma, D., de Jong, A., Ormel, J., 1988. The Groningen Social DisabilitiesSchedule: development, relationship with I.C.I.D.H. and psychometricproperties. Int. J. Rehabil. Res. 11, 213–224.
World Health Organization (WHO), 2000. World Health OrganizationDisability Assessment Schedule (WHO DASII). World Health Organiza-tion, Geneva.